 Ana Merino Sánchez-Cañete1*
Ana Merino Sánchez-Cañete1* Concepción Marina López Cárdenes1
Concepción Marina López Cárdenes1 Saioa Vicente Santamaría1
Saioa Vicente Santamaría1 José Ramón Gutiérrez Martínez2Marta Suárez González2
José Ramón Gutiérrez Martínez2Marta Suárez González2 María Álvarez Merino2
María Álvarez Merino2 David González Jiménez2
David González Jiménez2- 1Cystic Fibrosis Unit, Department of Pediatrics, University Hospital Ramón y Cajal, Madrid, Spain
- 2Cystic Fibrosis Unit, University Hospital Central de Asturias, Oviedo, Spain
Background: When people with cystic fibrosis (PwCFs) are treated with cystic fibrosis transmembrane conductance regulator protein modulator (CFTRm), it leads to changes in body composition. An easy, non-invasive, and reproducible method to assess this is by means of electrical bioimpedance measurement, which complements the information provided by the already-known anthropometric parameters.
Methods: Seventeen adults with cystic fibrosis in treatment with elexacaftor–tezacaftor–ivacaftor (ETI) were recruited for a prospective, longitudinal, single-center study over 12 months. Study variables included weight, body mass index (BMI), and body composition by bioelectrical impedance analysis (BIA) [including fat mass (FM) and fat-free mass (FFM)].
Results: At 12 months, there was an increase in overweight patients (5.9% vs. 23.5%) and a statistically significant increase in BMI at 6 and 12 months. An increase in FM and FFM was observed at 12 months. The increase was greater in FM (95% CI) from a baseline of 1.77% (0.00–3.54; p = 0.050) at 6 months and 2.64% (0.48–4.81; p = 0.020) at 12 months.
Conclusion: After treatment with ETI, there was an increase in weight, BMI, and FM more than FFM in PwCF. These changes would be confirmed in long-term studies to improve nutritional management.
1 Introduction
Since European Medicines Agency (EMA) approved elexacaftor–tezacaftor–ivacaftor (ETI) for people with cystic fibrosis (PwCF) in 2020, the improvement in lung function and the decrease in sweat chloride have been superior to that demonstrated in PwCF treated with previous generations of cystic fibrosis transmembrane conductance regulator protein modulator (CFTRm) (1–3).
Improvements in anthropometric and body composition changes appear to be observed (1, 4–6) regarding a special interest as a better nutritional status is associated with improved quality of life, survival (7), and lung function in cystic fibrosis (CF) (5, 8).
In recent years, the nutritional status of patients has been defined by anthropometric parameters such as weight, height, and body mass index (BMI). Using new methods, such as bioelectrical impedance analysis (BIA), allows us to complete the information on body composition in a non-invasive, valid, and safe way for PwCF (9, 10).
In our study, we analyzed the anthropometric and body composition changes observed in a cohort of PwCF over 18 years of age with CF and undergoing treatment with ETI.
2 Methods
2.1 Study design and outcome variables
We designed a prospective, longitudinal study in a single CF Unit. PwCF data were collected before ETI initiation and at 6 and 12 months post-treatment. The clinical research ethics committee of the participating hospital approved the study. Informed consent was obtained from all subjects. We included adult patients who were 18 years or older. The mandatory requirements were that all the participants were diagnosed with CF, and the genotype had at least one F508del mutation. All participants initiated triple therapy with ETI at the time of the study, regardless of prior treatment with CFTRm. The exclusion criteria were patients with only baseline bioimpedance measurement without subsequent follow-up and patients with incomplete data and PwCF who had to stop treatment at some point during the study.
2.2 Anthropometric measures
Regarding the anthropometric parameters used, they were classified into four groups according to their BMI according to WHO guidelines: underweight (<18.5 kg/m2), adequate weight (18.5–24.9 kg/m2), overweight (25–29.9 kg/m2), or obese (≥30 kg/m2). In addition, we follow the recommendations of the Cystic Fibrosis Foundation and according to The European Society for Clinical Nutrition and Metabolism (ESPEN) guidelines 2024 for patients with CF: Women maintain a BMI of at least 22 kg/m2 and men a BMI of at least 23 kg/m2.
2.3 Body composition assessment
Body composition was studied with a BIA AKERN 101 device (Akern, Montachiello, Pisa, Italy). The study was carried out with the subjects lying supine on a stretcher with their arms separated from the trunk by 30° and their legs separated by 45°. Four electrodes (Biatrodes, Akern) were placed on the extremities, two on the right hand and another two on the right foot, with a 4–5-cm space between them. These were connected by wire to the device, thus providing the resistance and reactance values. These data, together with the subject’s weight and height, age, sex, ethnicity, and physical activity, were entered into the device’s accompanying software (BODYGRAM PLUS, Akern), and the values of FM, FFM, and total body water (TBW) were recorded.
2.4 Statistical analysis
Study data were collected and managed using REDCap (11) electronic data capture tools hosted at Sociedad Española de Gastroenterología, Hepatología y Nutrición Pediátrica (SEGHNP).1 The technical support was made by the AEG REDCap Support Unit, shared with Asociación Española de Gastroenterología (AEG).
Descriptive statistics were performed on demographic, clinical, and body composition data. Shapiro–Wilk test was used to assess normality. Paired Student’s t-test was used to compare pre- and post-ETI values for all variables where the normality assumption was met. Statistical analysis was performed with STATA software, version 13.1. A statistically significant result was considered to be p < 0.05.
3 Results
3.1 Participant baseline characteristics
Finally, seventeen patients with baseline body impedance values and at least one other at 6 or 12 months were recruited. The ages were between 20 and 47 years, with a mean of 32.2 years old, without differences in sex. More than half of the participants (55.9%) were homozygous for the F508del mutation, and 88.2% were on enzyme replacement therapy (ERT) for pancreatic insufficiency.
3.2 Anthropometric and body composition parameters
During follow-up, patients presented a statistically significant increase in mean BMI (paired Student’s t-test): 0–6 months 0.77 (CI 95%: 0.19–1.36) kg/m2 (p = 0.013); 6–12 months 0.59 (CI 95%: 0.13–0.92) kg/m2 (p = 0.013); and 0–12 months 1.29 (CI 95%: 0.56–2.04) kg/m2 (p = 0.002).
According to WHO BMI guidelines, there was an increase in overweight (25–29.9 kg/m2) patients after 12 months on ETI (p = 0.083, McNemar’s test), being 5.9% (1/17 patients) of patients at baseline vs. 23.5% (4/17 patients) after 12 months of study.
Regarding the BMI nutritional target according to the CF Foundation and ESPEN 2024 guidelines, two patients reached the BMI recommendations for improving respiratory parameters (FEV1): At baseline, 8 patients (41%) had a BMI of at least 22 in women and 23 in men, and at 12 months of treatment, 10 patients had at least this BMI.
There was a significant increase in patient weight after 12 months of ETI (60.5 ± 9.3 vs. 64.20 ± 10.88, p = 0.001, paired Student’s t-test) and a significant increase in FM (kg) in the same interval (9.51 ± 4.46 vs. 12.00 ± 4.83, p = 0.006, paired Student’s t-test).
Table 1 summarizes the main data with the changes in body impedance.
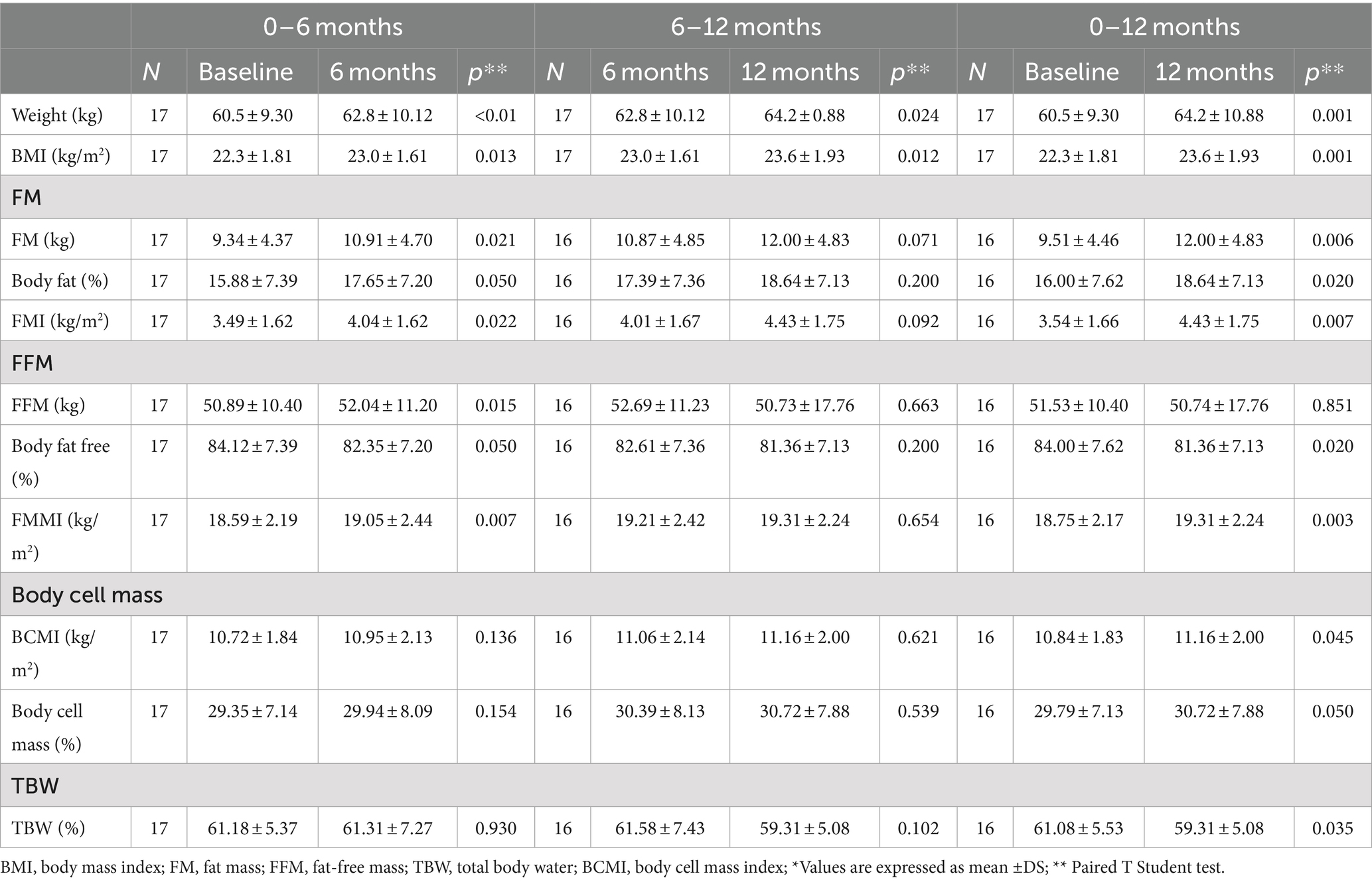
Table 1. Anthropometric and body composition parameters.
We observed an increase in total FM and FFM compared with basal values; however, in proportion, there is a greater increase in the percentage of FM compared to FFM (paired Student’s t-test): Mean 1.77 (IC 95%: 0.00–3.54; p = 0.050) between 0 and 6 months and 2.64 (IC 95%: 0.48–4.81; p = 0.020) between 0 and 12 months (Figure 1). We do not find differences in FM and FFM percentages between 6 and 12 months. Figure 1 shows the changes in FM at baseline, 6 months, and 12 months of the study.
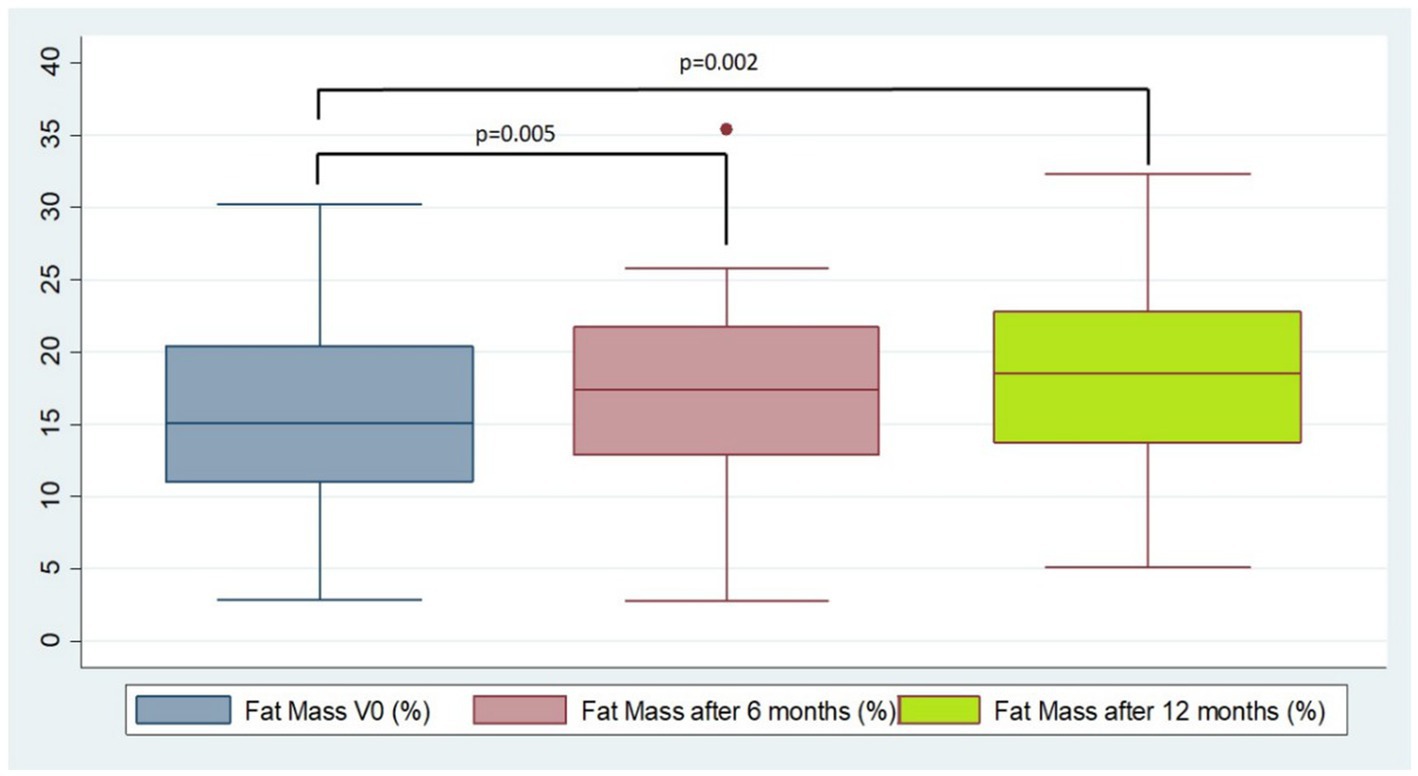
Figure 1. Percentage of fat mass (FM) at baseline at 6 months and 12 months.
4 Discussion
Observational studies (1, 4) have already shown improvements in lung function and reductions of sweat chloride but also a significant change in body composition (5–7).
In this context, there is growing interest in body composition changes that occur after the initiation of ETI, which have been increasing (12). A study by King et al. already evidenced these changes in a cohort of adults on Ivacaftor treatment (1). In addition, if we look at the German Cystic Fibrosis Registry 2022 (13), we can see a change in the trend in the BMI of patients. In this registry, an increase in the percentage of patients reaching the optimal BMI (women 22–23.9 kg/m2 and men 23.0–24.9 kg/m2) can be observed between 2010 and 2022, at the time of the start of CFTR modulators (13). As in our study, an increase in BMI, defined as overweight by WHO (14), was observed in the age groups of patients included in our study and between the years corresponding to the start of CFTR modulators.
However, to our knowledge, there are currently no studies using BIA to assess body composition in PwCF on ETI. Our study observed an increase in weight Z-score and BMI. Both were significant at 6 and 12 months of treatment. Of note is the increase in overweight patients with possible short- and long-term consequences. Similarly, studies such as that of Granados et al. also show a significant increase in weight (7, 15).
However, a BMI in the appropriate range according to reference values does not necessarily imply an adequate body composition (8, 10, 16–18). This is the case in Engelen et al. where BMI could not estimate FFM depletion in more than half of the patients. Furthermore, if not well matched to body composition, the appropriate BMI value in CF is constantly changing (15, 17–20). In this respect, our results support the conclusion of similar studies. If we compare these values with those of the population in the study by King et al., the population has a similar BMI (22.3 vs. 23.3 k/m2); however, our sample has a lower percentage of FM (15.9 vs. 23.6) and a higher percentage of FFM (84.1 vs. 76.4).
Therefore, it is important to highlight patients who, despite having a normal weight (kg), have a BMI (kg/m2) in the obese range with a high percentage of FM and low FFM as it is related to worse lung function. In percent when compared to overweight and obese PwCF (18).
Therefore, we consider that this study can be a reference point for studying body composition by this method in PwCF treated with ETI.
Regarding body composition, several studies have shown changes in body compartments (15, 19, 20). There appears to be a tendency for rapid weight and BMI gain during the first months of therapy. These initial changes and subsequent stabilization have been specifically studied with the onset of ETI and assessed with different methods, such as dual-energy X-ray absorptiometry (DXA) (7). It is of interest to extend studies explaining this rapid initial improvement and to assess the stabilization of anthropometric parameters and their relationship with changes in lung capacity. Both in our study and in King et al., there was a significant increase in weight at the expense of FM in the first 6 months. However, after 2 years of follow-up in the ivacaftor-treated cohort, weight and FM have attenuated with the stabilization of FFM (1). In our study, following the cohort for a shorter period (12 months), weight and FM continue to increase significantly, with a slight depletion of FFM.
The increase in weight and the fat component in the cohort of patients has been previously attempted to be explained in patients treated with ivacaftor (21, 22). However, it is not known whether this mechanism is exclusively due to CFTRm (23, 24).
There are studies assessing body composition changes after initiation of ETI using methods such as DXA or after using one or a combination of two CFTR modulators (1, 7). However, our study provides the first insight into the body composition behavior of patients using BIA in the first months of treatment with ETI. Sustained improvement in these results would be expected with continued treatment. However, these preliminary data and results must be confirmed over the next few months of treatment.
The study’s limitations are the small sample size and the lack of a control group. Furthermore, it is a short-term study, and the results obtained are early changes. In addition, factors that could influence body composition, such as physical activity and dietary intake, have not been included in the analysis. Finally, our body composition data are presented as percentages and kilograms, although the use of values for resistance and reactance is preferred by ESPEN guidelines 2024.
However, if larger studies confirm these results, it may lead to a change in the approach to these patients. It will be important to emphasize nutritional therapy, individualization, and monitoring of body composition from the start of therapy.
5 Conclusion
The initiation of treatment with CFTR modulators has led to a change in the management of CF. In general, anthropometric changes are reflected in weight gain, which in the first 6 months reflects an increase in both FM and FFM, both of which are significant. It would be interesting to analyze the evolution of these parameters in the long term to verify the stabilization of the parameters and improve the nutritional approach.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
This study protocol was reviewed and approved by “Comité Ético de la Investigación con Medicamentos” (CEIm) from Ramón y Cajal University Hospital, at the meeting held on 13/01/2022 Cerficate# 425. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants' legal guardians/next of kin because all participants gave their informed consent verbally before enrolling in the study, after detailed information from the researchers.
Author contributions
AS-C: Conceptualization, Investigation, Methodology, Visualization, Writing – original draft. CL: Investigation, Methodology, Visualization, Writing – original draft. SV: Conceptualization, Methodology, Project administration, Resources, Validation, Writing – review & editing. JG: Investigation, Visualization, Writing – review & editing. MS: Investigation, Visualization, Writing – review & editing. MÁ: Investigation, Visualization, Writing – review & editing. DG: Conceptualization, Data curation, Formal analysis, Project administration, Validation, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
1. ^ www.seghnp.org
References
1. King, SJ, Tierney, AC, Edgeworth, D, Keating, D, Williams, E, Kotsimbos, T, et al. Body composition and weight changes after ivacaftor treatment in adults with cystic fibrosis carrying the G551 D cystic fibrosis transmembrane conductance regulator mutation: a double-blind, placebo-controlled, randomized, crossover study with open-label extension. Nutrition. (2021) 85:111124. doi: 10.1016/j.nut.2020.111124
2. De la Hoz, D, Villamil Osorio, M, and Restrepo-Gualteros, SM. Cystic fibrosis transmembrane conductance regulator modulators: present and future in cystic fibrosis treatment. A review. Arch Argent Pediatr. (2019) 117:e131–6. doi: 10.5546/aap.2019.eng.e131
3. Borowitz, D, Lubarsky, B, Wilschanski, M, Munck, A, Gelfond, D, Bodewes, F, et al. Nutritional status improved in cystic fibrosis patients with the G551D mutation after treatment with Ivacaftor. Dig Dis Sci. (2016) 61:198–207. doi: 10.1007/s10620-015-3834-2
4. Nichols, DP, Paynter, AC, Heltshe, SL, Donaldson, SH, Frederick, CA, Freedman, SD, et al. Clinical effectiveness of Elexacaftor/Tezacaftor/Ivacaftor in people with cystic fibrosis: a clinical trial. Am J Respir Crit Care Med. (2022) 205:529–39. doi: 10.1164/rccm.202108-1986OC
5. Soltman, S, Hicks, RA, Naz Khan, F, and Kelly, A. Body composition in individuals with cystic fibrosis. J Clin Transl Endocrinol. (2021) 26:100272. doi: 10.1016/j.jcte.2021.100272
6. Calella, P, Valerio, G, Brodlie, M, Taylor, J, Donini, LM, and Siervo, M. Tools and methods used for the assessment of body composition in patients with cystic fibrosis: a systematic review. Nutr Clin Pract. (2019) 34:701–14. doi: 10.1002/ncp.10247
7. Granados, A, Chan, CL, Moheet, A, Vigers, T, Arbeláez, AM, and Larson, OK. The impact of elexacaftor/tezacaftor/ivacaftor on body composition in a small cohort of youth with cystic fibrosis. Pediatr Pulmonol. (2023) 58:1805–11. doi: 10.1002/ppul.26388
8. Alvarez, JA, Ziegler, TR, Millson, EC, and Stecenko, AA. Body composition and lung function in cystic fibrosis and their association with adiposity and normal-weight obesity. Nutrition. (2016) 32:447–52. doi: 10.1016/j.nut.2015.10.012
9. Beaumesnil, M, Chaillou, E, Wagner, AC, Rouquette, A, Audran, M, and Giniès, JL. Composition corporelle des patients mucoviscidosiques–comparaison de 3 techniques de mesure: anthropométrie, absorptiométrie biphotonique et impédancemétrie. Arch Pédiatr. (2011) 18:370–5. doi: 10.1016/j.arcped.2011.01.008
10. Kuriyan, R. Body composition techniques. Indian J Med Res. (2018) 148:648–58. doi: 10.4103/ijmr.IJMR_1777_18
11. Harris, PA, Taylor, R, Thielke, R, Payne, J, Gonzalez, N, and Conde, JG. Research electronic data capture (REDCap)—a metada-ta-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. (2009) 42:377–81. doi: 10.1016/j.jbi.2008.08.010
12. Goetz, DM, and Savant, AP. Review of CFTR modulators 2020. Pediatr Pulmonol. (2021) 56:3595–606. doi: 10.1002/ppul.25627
13. Nährlich, L, Burkhart, M, and Wosniok, J. German cystic fibrosis registry. Annual report 2022. Mukoviszidose eV (2023). 26 p.
14. World Health Organization. A healthy lifestyle-WHO recommendations (2010). Available at: https://www.who.int/europe/news-room/fact-sheets/item/a-healthy-lifestyle---who-recommendations (Accessed October 6, 2024).
15. Proud, D, and Duckers, J. Weight a minute: exploring the effect on weight and body composition after the initiation of elexa-caftor/tezacaftor/ivacaftor in adults with CF. J Cyst Fibros. (2023) 22:847–50. doi: 10.1016/j.jcf.2023.06.002
16. Achamrah, N, Colange, G, Delay, J, Rimbert, A, Folope, V, Petit, A, et al. Comparison of body composition assessment by DXA and BIA according to the body mass index: a retrospective study on 3655 measures. PLoS One. (2018) 13:e0200465. doi: 10.1371/journal.pone.0200465
17. Cystic Fibrosis Foundation. Nutritional basics. Available at: https://www.cff.org/managing-cf/nutritional-basics (Accessed October 5, 2024).
18. Wilschanski, M, Munck, A, Carrion, E, Cipolli, M, Collins, S, Colombo, C, et al. ESPEN-ESPGHAN-ECFS guideline on nutrition care for cystic fibrosis. Clin Nutr. (2024) 43:413–45. doi: 10.1016/j.clnu.2023.12.017
19. Engelen, MPKJ, Schroder, R, Van Der Hoorn, K, Deutz, NEP, and Com, G. Use of body mass index percentile to identify fat-free mass depletion in children with cystic fibrosis. Clin Nutr. (2012) 31:927–33. doi: 10.1016/j.clnu.2012.04.012
20. Chula De Castro, JA, Lima, TRD, and Silva, DAS. Body composition estimation in children and adolescents by bioelectrical impedance analysis: a systematic review. J Bodyw Mov Ther. (2018) 22:134–46. doi: 10.1016/j.jbmt.2017.04.010
21. Hart, N, Tounian, P, Clément, A, Boulé, M, Polkey, MI, Lofaso, F, et al. Nutritional status is an important predictor of diaphragm strength in young patients with cystic fibrosis. Am J Clin Nutr. (2004) 80:1201–6. doi: 10.1093/ajcn/80.5.1201
22. Bailey, J, Rozga, M, McDonald, CM, Bowser, EK, Farnham, K, Mangus, M, et al. Effect of CFTR modulators on anthropometric parameters in individuals with cystic fibrosis: an evidence analysis center systematic review. J Acad Nutr Diet. (2021) 121:1364–1378.e2. doi: 10.1016/j.jand.2020.03.014
23. Schwarzenberg, SJ, Vu, PT, Skalland, M, Hoffman, LR, Pope, C, Gelfond, D, et al. Elexacaftor/tezacaftor/ivacaftor and gastro-intestinal outcomes in cystic fibrosis: report of promise GI. J Cyst Fibros. (2023) 22:282–9. doi: 10.1016/j.jcf.2022.10.003
Keywords: cystic fibrosis, body composition, nutritional status, bioelectrical impedance, CFTR modulators
Citation: Merino Sánchez-Cañete A, López Cárdenes CM, Vicente Santamaría S, Gutiérrez Martínez JR, Suárez González M, Álvarez Merino M and González Jiménez D (2024) Increased fat mass and obesity risk after elexacaftor–tezacaftor–ivacaftor therapy in young adults with cystic fibrosis. Front. Nutr. 11:1477674. doi: 10.3389/fnut.2024.1477674
Edited by:
Lenycia De Cassya Lopes Neri, University of Pavia, ItalyReviewed by:
Matias Epifanio, Pontifical Catholic University of Rio Grande do Sul, BrazilRenata Guirau, State University of Campinas, Brazil
Copyright © 2024 Merino Sánchez-Cañete, López Cárdenes, Vicente Santamaría, Gutiérrez Martínez, Suárez González, Álvarez Merino and González Jiménez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ana Merino Sánchez-Cañete, YW5hLm1lcmluby5zY0BnbWFpbC5jb20=