 Cira Ba1†
Cira Ba1† Chloé Marques
Chloé Marques Gianluca Severi
Gianluca Severi Francesca Romana Mancini
Francesca Romana Mancini- 1Université Paris-Saclay, UVSQ, Inserm, Gustave Roussy, CESP, Villejuif, France
- 2Department of Statistics, Computer Science, Applications “G. Parenti”, University of Florence, Florence, Italy
Western studies have shown a non-linear association between fish consumption and mortality, which might be explained by exposure to chemical contaminants. This study aims to explore the associations between fish consumption or omega-3 polyunsaturated fatty acids (n-3 PUFA) and mortality within the prospective E3N French cohort, and to investigate the role of dietary exposure to contaminants in these associations. In the E3N cohort composed of 72,585 women, we assessed fish consumption and n-3 PUFA intake through a food questionnaire sent in 1993. To estimate the dietary exposure to contaminants, we used the food contamination database of the second French total diet study. Cox proportional hazard models were used to estimate the association between fish, lean fish, fatty fish, and n-3 PUFA intake, with the risk of all-cause or cause-specific mortality. During the follow-up (1993–2014), 6,441 deaths were recorded. A U-shaped association was observed between fish consumption and all-cause mortality (Poverall_association = 0.017). A similar association was observed with lean fish consumption, while the non-linear association between fatty fish consumption or n-3 PUFA intake and all-cause mortality did not reach statistical significance. A non-linear association was observed between fish consumption and lung cancer mortality (Poverall_association = 0.005). A positive and linear association was observed between fatty fish consumption or n-3 PUFA intake and breast cancer mortality (HR [CI95%]: 1.07 [1.01–1.15] and 1.08 [1.01–1.15]). Our results remained unchanged when further adjusting on dietary exposure to contaminants. Our results showed a U-shaped association between fish consumption and all-cause mortality and suggest a notable role of lean fish consumption in this association, but no role of dietary exposure to contaminants. Further studies are needed to better clarify this U-shaped association and the different impacts of fatty and lean fish consumption on health.
1 Introduction
Fish has valuable nutritional qualities that make it a particularly interesting food from a nutritional point of view. The European Food Safety Authority (EFSA) recommends eating fish twice a week, including fatty fish (1). Fish is a source of proteins and essential micronutrients and constitutes a primary source of long-chain omega-3 polyunsaturated fatty acids (n-3 PUFA): eicosapentaenoic acid (EPA), docosapentaenoic acid (DPA) and docosahexaenoic acid (DHA) (2). A recent meta-analysis showed that n-3 PUFA were associated with a lower risk of developing major chronic diseases, including cardiovascular disease (CVD), coronary heart disease (CHD), and overall mortality (3). Previous epidemiological studies that have investigated the association between fish consumption and mortality risk generally indicate that consuming fish reduces the risk of mortality (4–6). However, findings from epidemiological studies remain heterogeneous. Several meta-analyses have identified a linear inverse or non-linear U-shaped association between fish consumption and the risk of all-cause mortality (3, 7), with variations observed based on geographical regions. Indeed, whereas some Asian studies showed a linear, inverse, and statistically significant association (6, 8), Western studies showed a non-linear U-shaped association that was not statistically significant (4, 5). It has been suggested that the shape of the association between fish consumption and mortality risk may depend on several factors, such as fish preparation methods (fried or not) (7), fat content (9, 10), or level of contamination from chemical substances (11, 12). Indeed, increased fish consumption may be linked to elevated risks of all-cause and cause-specific mortality, due to heightened exposure to chemical contaminants, such as heavy metals (methylmercury (MeHg), cadmium) and persistent organic pollutants (POPs; such as dioxins, polychlorobiphenyls (PCBs), polybrominated diphenyl ethers (PBDEs) (11–13). Exposure to environmental contaminants in fish might reduce the positive impacts of fish consumption and potentially elucidate the U-shaped associations observed in prior studies on all-cause mortality.
The present study aims to explore the association between fish consumption and all-cause and cause-specific mortality, along with the association between the intake of n-3 PUFA (EPA, DHA, and DPA) and all-cause and cause-specific mortality within the French E3N (Epidemiological Study on Women of the National Education) prospective cohort. As a secondary objective, this study will estimate the direct effect of fish on mortality by adjusting on dietary exposure to food chemical contaminants, namely POPs.
2 Materials and methods
2.1 E3N cohort
The E3N study launched in 1990 across mainland France is an ongoing prospective cohort that included 98,995 women aged from 40 to 65 years at enrolment, living in France, and insured by MGEN, a health insurance for workers of the French national education system. Anthropometric, lifestyle, and health characteristics were systematically gathered every 2 to 3 years through self-administered questionnaires. Only 3% of E3N women were lost to follow-up (14). All participants provided explicit consent for their involvement in this study, which received approval from the CNIL (the French National Commission for Data Protection and Privacy).
2.2 Ascertainment of mortality
Information regarding the vital status of participants was obtained from various databases, including health insurance records, postal services, municipal registries, physicians, and next of kin. Details about the causes of death were sourced from Inserm-CépiDC (French Epidemiology Center on the Medical Causes of Death). Causes of death were coded according to the ninth revision (ICD-9, death before 2000) and the tenth revision (ICD-10, death after 2000) of the International Classification of Diseases (ICD). Mortality by cause was defined as follows: ICD-9390–459 and ICD-10 I00-I99 for CVD; ICD-9140-208 and ICD-10 C00-C97 for cancer; ICD-9174 and ICD-10 C50 for breast cancer; ICD-9153, 154.0, 154.1 and ICD-10 C18-C20 for colorectal cancer; ICD-9162 and ICD-10 C33-C34 for lung cancer.
2.3 Dietary questionnaire
In the E3N cohort, dietary data were collected using a semi-quantitative food frequency questionnaire. This questionnaire comprising 208 food items was distributed in 1993 (third questionnaire, Q3). It consisted of two parts. The first part addressed the frequency of consumption (never, 1 to 3 times per month, or 1 to 7 times per week) and the quantity consumed of various food groups during 8 meal occasions over the past 12 months. The second part provided details about the specific food items included within each food group identified in the first part. The validity and reproducibility of this questionnaire were satisfied in a dedicated study, including for fish consumption (15).
The data collected through the dietary questionnaire were used to estimate the average daily consumption of foods and beverages in grams per day. Fish consumption was assessed using the dietary questionnaire sent in 1993. In addition to analysing the overall fish consumption, we also examined the intake of lean fish (cod, whiting, hake, pollock, ling, dab, sole, haddock, coley) and fatty fish (salmon, trout, sardines, mackerel, and canned tuna), which specific consumptions were specified in the second part of the dietary questionnaire.
Daily nutrient intakes were obtained from the French food composition table provided by the French Information Centre on Food Quality (CIQUAL) (16). The daily nutritional intake of n-3 PUFA predominantly found in fish (EPA, DHA, and DPA) were considered in the analysis.
2.4 Estimation of POPs dietary intake
Food contamination levels were obtained from food contamination data performed by the French Agency for Food, Environmental, and Occupational Health and Safety (ANSES) during the second French Total Diet Study (17), the most comprehensive French food contamination database.
In summary, a total of 20,280 food items were acquired from eight French regions between 2007 and 2009. This led to the creation of 1,352 composite samples that were prepared “as consumed” (including processes such as peeling and frying) for the analysis of over 400 food chemical contaminants, as detailed by Sirot et al. (18).
In our study, we were focused on POPs. In particular, dietary intakes of non-dioxin-like PCBs (NDL-PCBs, continuous, ng/day), dioxins added to dioxin-like PCBs (dioxins + DL-PCBs continuous, TEQ, pg/day), and PBDEs (continuous, ng/day) were included in the analyses.
The estimation of participant’s dietary intake of those POPs was carried out by merging the E3N database containing food consumption levels and the ANSES database containing food contamination levels as detailed in the study of Mancini et al. (19). For each participant, the average daily dietary intake of each POP was obtained by summing, for each food item, the product of the average daily quantity consumed of that food item by the level of contamination of that food item with the POP of interest. Then, the dietary intake of each group of POPs (dioxins, DL-PCBs, NDL-PCBs, or PBDEs) was obtained by adding up the dietary intake of each congener. For this study, 17 dioxin congeners, six NDL-PCBs congeners, 12 DL-PCBs congeners, and eight PBDEs congeners were included in the analysis (Supplementary Table 1). To limit the overestimation of POPs intakes, we estimated those intakes according to the lower bound (LB) scenario, in which non-detected values were replaced by zero.
2.5 Assessment of other covariates
In order to respect temporality, covariates measured in several E3N questionnaires were selected in the second questionnaire (Q2) sent in 1992 to precede the dietary questionnaire (sent in 1993) which focused on the last 12 months dietary consumptions. We included physical activity measured at Q3 as it was not collected at Q2.
The adjustment variables were selected based on the literature and based on a directed acyclic graph (DAG; Supplementary Figure 1). The following covariates were included in the analyses: birth cohort (≤1930; (1930–1935]; (1935–1940]; (1940–1945]; >1945), education level (<12 years, 12 to 14 years, >14 years), smoking status at Q2 (never smoker; former smoker; current smoker), body mass index (BMI) at Q2 (continuous, kg/m2, derived from height and weight), menopausal status combined with recent use (within the past year) of menopausal hormone therapy (MHT) at Q2 (premenopausal; menopausal with recent MHT use; menopausal without recent MHT use; menopausal with missing data on MHT use), physical activity at Q3 (continuous, metabolic equivalents of task-hours/week (MET-h/week)), total energy intake excluding alcohol consumption at Q3 (continuous, kcal/day), alcohol consumption at Q3 (continuous, g of ethanol/day), red and processed meat consumption at Q3 (continuous, g/day), fruits and vegetables consumption at Q3 (continuous, g/day), and dairy products consumption at Q3 (continuous, g/day).
2.6 Study population
This study included all participants who had completed the dietary questionnaire sent in June 1993, totalling 74,522 women. For this analysis, we excluded participants with extreme energy intake to mitigate over-reporting or under-reporting (n = 1,491). In other words, participants with energy intake-to-requirements ratios in the bottom or top 1% of the distribution were excluded. Energy requirements were estimated using the basal metabolic rate (BMR) multiplied by the level of physical activity. To calculate BMR, we used the Schofield equation based on age, sex, and weight (20). Additionally, we excluded women who did not complete subsequent questionnaires after this dietary questionnaire (n = 446).
Our study population for all-cause mortality comprised 72,585 women. Subsequently, women with unknown causes of death (n = 169) were excluded, resulting in a study population of 72,416 women for analyses on cancer or cardiovascular disease mortality. Finally, for analyses on mortality by specific cancer type, women with unknown primary locations of cancer were also excluded (n = 178), resulting in a study population of 72,238 participants. The flow chart is presented in the Supplementary Figure 2.
2.7 Statistical analyses
2.7.1 Descriptive analyses
The characteristics at baseline of the study population were described (mean and standard deviation for continuous variables, frequencies and proportions for categorical variables) for the total population and within each quartile group of fish consumption (in g/day). Spearman rank correlation tests between dietary exposure to POPs and fish consumption were also performed (Supplementary Table 2).
2.7.2 Main analyses
Cox proportional hazard regression models, with age as the time scale, were employed to estimate Hazard Ratios (HR) and their 95% confidence intervals (CI). In the Cox models, fish consumption (in g/day), lean fish consumption (in g/day), fatty fish consumption (in g/day), and n-3 PUFA intake (sum of EPA, DPA, and DHA in g/day) were analysed separately as the primary exposure variables, treated as both a continuous and categorical variable, with the smallest quartile group serving as the reference. The outcomes of interest were the following: all-cause mortality, CVD mortality, cancer mortality, and mortality from specific types of cancer (breast, lung, and colorectal). To account for the role of total energy intake in the association between n-3 PUFA intake and the risk of mortality, we applied the energy adjustment residual method which consisted of substituting the n-3 PUFA intake main exposure variable with the residuals of the regression between n-3 PUFA intake and total energy intake (21).
Participants were followed from their age at Q3 response until the age at the first observed event, being the end of the follow-up (November 17, 2014), the date of death, or the date of completion of the last questionnaire, whichever occurred first. Furthermore, for analyses on specific causes of mortality, causes other than those of interest were censored at the date of death.
Five models were developed for each of the 4 main exposure variables (fish consumption, lean fish consumption, fatty fish consumption, and n-3 PUFA intake). Model 1 was unadjusted with age as the time scale. Model 2 was adjusted for the following covariates: birth cohort, education level, smoking status, BMI, menopausal status combined with recent use of MHT, physical activity, total energy intake excluding alcohol consumption, alcohol consumption, red and processed meat consumption, fruits and vegetables consumption, and dairy products consumption. We performed additional analyses further adjusting Model 2 for dietary intake of POPs: Model 3 was adjusted for dietary intake of dioxins added to DL-PCBs (TEQ, pg/day), Model 4 for dietary intake of NDL-PCBs (ng/day), and Model 5 for dietary intake of PBDEs (ng/day).
Restricted cubic spline (RCS) regression was used to assess dose–response relationships for all continuous variables and to examine deviations from linearity. If the linearity test was not respected (i.e., if the p-value of the non-linearity test was under 0.10), the continuous variable was considered non-linear, and RCS was used to model this variable. In these models, the number of knots for the main exposure variable was determined using the smallest Akaike information criterion (AIC) between three test models: 3 knots (at the 10th, 50th, and 90th percentiles), 4 knots (at the 5th, 35th, 65th, and 95th percentiles), and 5 knots (at the 5th, 27.5th, 50th, 72.5th, and 95th percentiles). For continuous covariates, 4 knots (at the 5th, 35th, 65th, and 95th percentiles) were used by default, as recommended by Harell (22). When the main exposure variable was linear, it was divided by its standard deviation to obtain estimates of the HRs for the increase of one standard deviation.
We imputed covariates with less than 5% of missing values with the median for continuous variables and with the modal category for categorical variables. We created an “unknown value” category when there were more than 5% missing values (only for menopausal status and recent MHT use).
A p-value less than 5% was considered statistically significant. We used SAS 9.4 software to build the database and R software version 4.1.0 to perform statistical analyses.
2.7.3 Sensitivity analyses
In order to assess the impact of a potential reverse causation bias, we ran Model 2 after having included a 5-year exposure lag and excluded all cases and participants censored during the first 5 years of follow-up.
3 Results
3.1 General characteristics
The average follow-up was 19.0 years (standard deviation: 4.1). During the follow-up, 6,441 women died, including 896 due to CVD and 3,473 due to cancer (of which 953 due to breast cancer, 364 due to lung cancer, and 317 due to colorectal cancer).
Table 1 describes the baseline characteristics of the study population overall and according to quartile groups of fish consumption. The baseline characteristics of the study population according to quartile groups of n-3 PUFA are described in Supplementary Table 3.
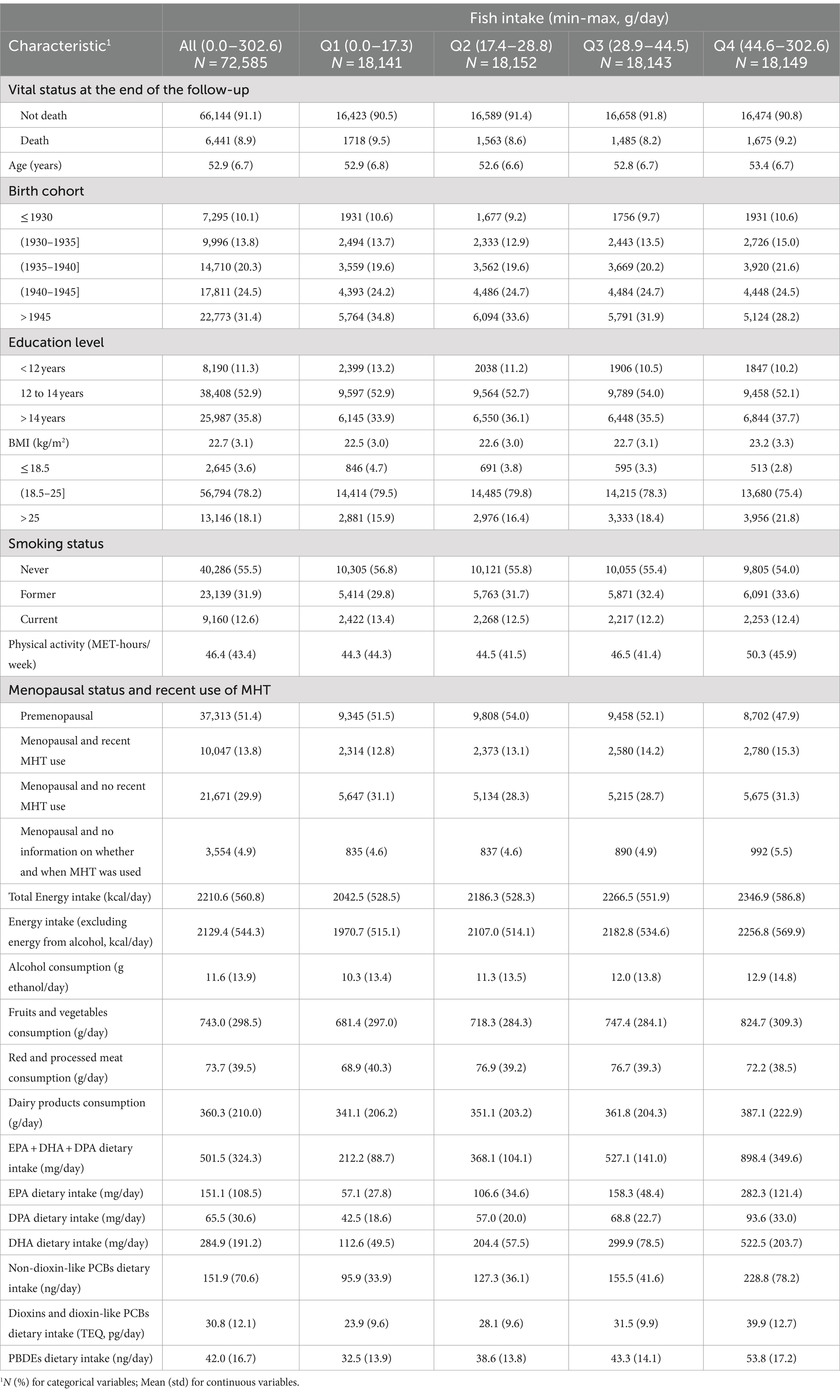
Table 1. Baseline characteristics of the study population overall and among each quartile group of fish intake in the E3N cohort (N = 72,585).
Overall, the average intake of fish was 34.0 g/day: 20.5 g/day of lean fish and 13.5 g/day of fatty fish. Regarding nutrient consumption, the average total intake of n-3 PUFA was 501.5 mg/day (standard deviation: 324.3), with a predominance of DHA (284.9 mg/day, standard deviation: 191.2), compared to EPA (151.1 mg/day, standard deviation: 108.5) and DPA (65.5 mg/day, standard deviation: 30.6).
Furthermore, a higher fish consumption (>44.6 g/day), compared to less than 17.3 g/day of fish consumption, corresponded to a higher dietary intake of POPs with an average intake of 228.8 vs. 95.9 ng/day for NDL-PCBs, 39.9 vs. 23.9 TEQ pg/day for dioxins and DL-PCBs, and 53.8 vs. 32.5 ng/day of PBDEs.
3.2 Fish consumption or n-3 PUFA intake and mortality
In Model 2, the analysis revealed a U-shaped association between fish consumption and all-cause mortality (P overall association = 0.017; Table 2 and Figure 1A). The use of spline functions highlighted a reduction in the risk of all-cause mortality when fish consumption increased from 0 to 40 g/day, and then an inversion of the trend (Figure 1A). The association was also non-linear but not statistically significant between fish consumption and CVD mortality (P overall association = 0.281) and cancer mortality (P overall association = 0.179). The association between fish consumption and breast cancer mortality as well as colorectal cancer mortality was linear but not statistically significant (respectively, HR [CI95%]: 1.05 [0.98–1.13] and HR [CI95%]: 0.93 [0.81–1.06]). The analyses also revealed a statistically significant non-linear association between fish consumption and lung cancer mortality (P overall association = 0.005; Table 2 and Supplementary Figure 3).
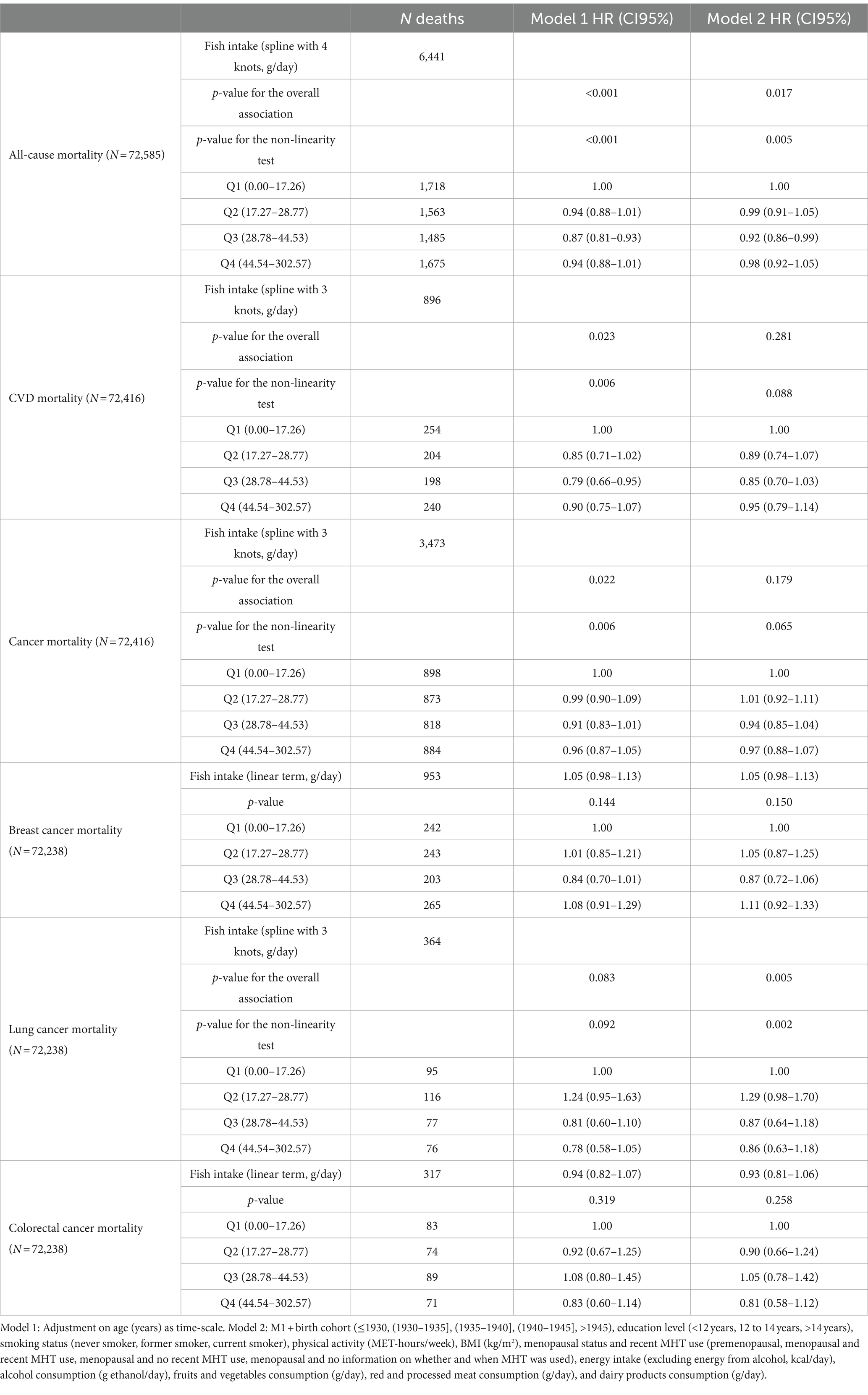
Table 2. Hazard ratios (CI95%) estimated by Cox multivariable regression models for the association between fish consumption and mortality risk in the E3N cohort.
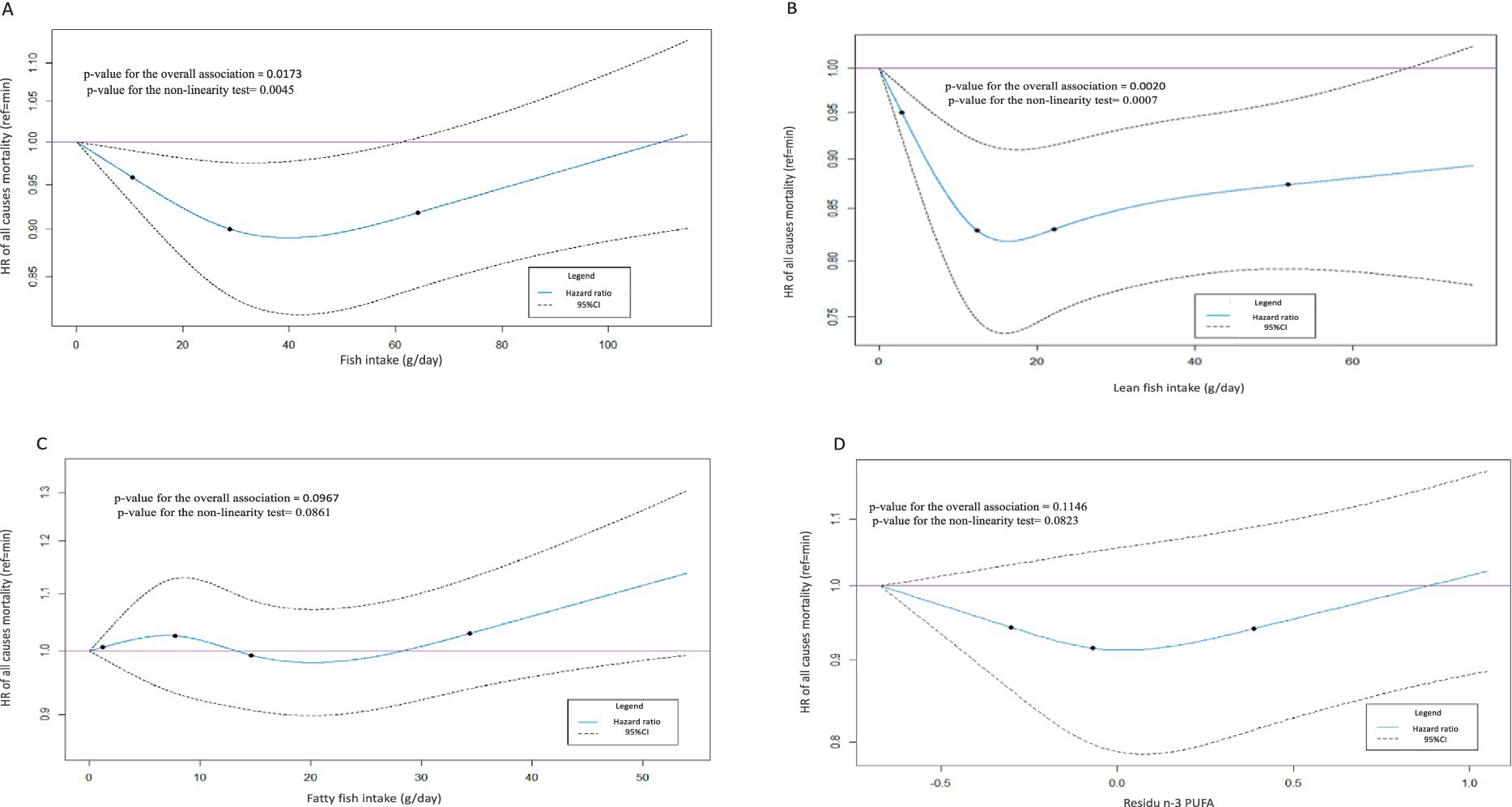
Figure 1. Restricted cubic splines of Model 2 of fish consumption (A), lean fish consumption (B), fatty fish consumption (C), and n-3 PUFA intake residuals (D) in association with all-cause mortality risk in the E3N cohort (N = 72,585). The minimum value of the main exposure variable is taken as reference. Solid lines indicate HR and dashed lines indicate 95% CI. The points represent percentiles as follows: 3 knots at the 10th, 50th, and 90th percentiles or 4 knots at the 5th, 35th, 65th, and 95th percentiles.
The analysis of the association between lean fish consumption and the risk of all-cause mortality in Model 2 revealed a statistically significant non-linear association (P overall association = 0.002), with a reduction of the risk when lean fish consumption increased up to 18 g/day after which a plateau was observed (Table 3 and Figure 1B). The associations between lean fish consumption and all other causes of death were not statistically significant (Table 3).
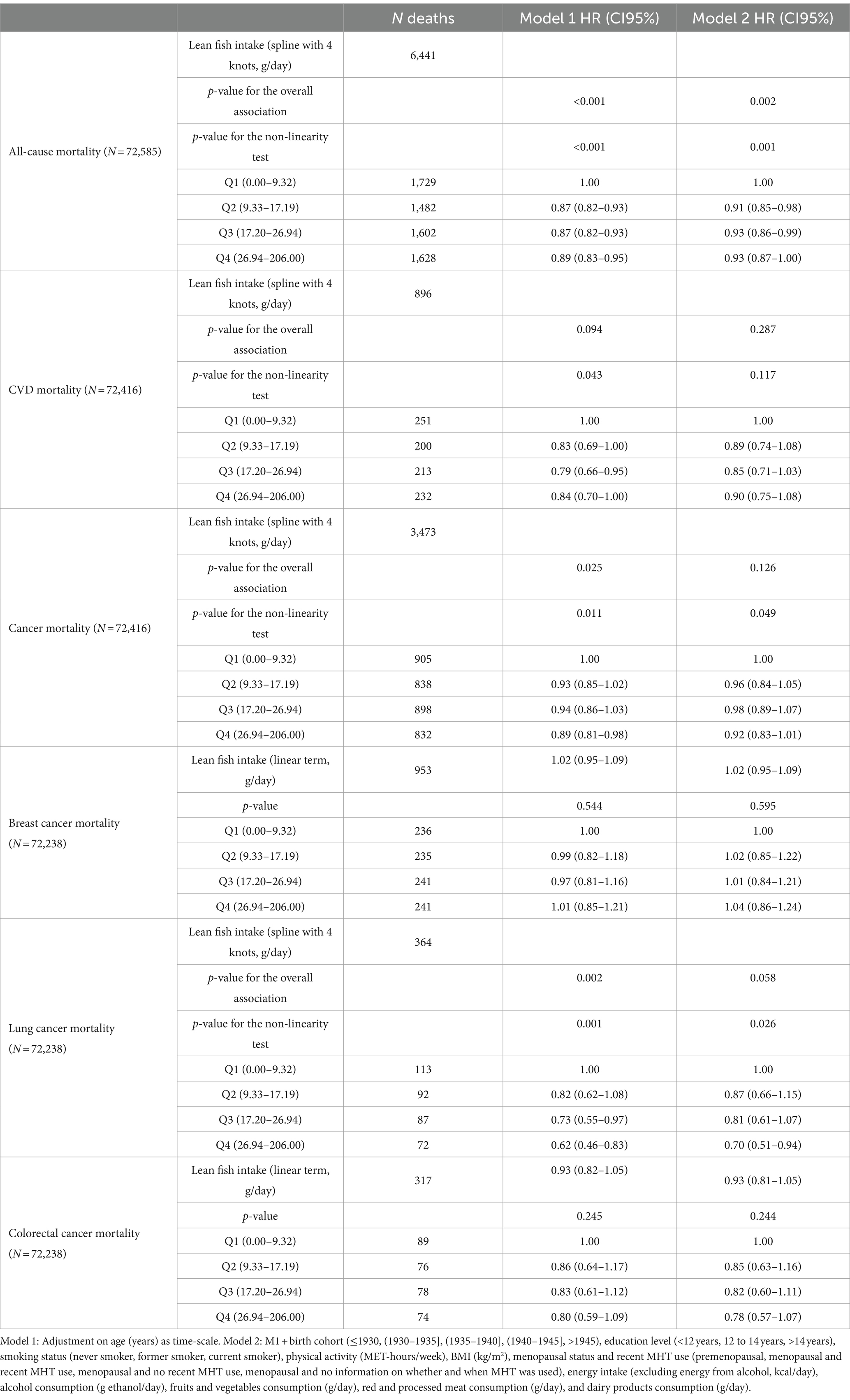
Table 3. Hazard ratios (CI95%) estimated by Cox multivariable regression models for the association between lean fish consumption and mortality risk in the E3N cohort.
For fatty fish consumption, the association with all-cause mortality was non-linear although not statistically significant (P overall association = 0.097; Table 4 and Figure 1C). A non-linear and statistically significant association was identified for fatty fish consumption in relation to cancer mortality (P overall association = 0.035), while a positive, linear and statistically significant association was observed between fatty fish consumption and breast cancer mortality (HR [CI95%]: 1.07 [1.01–1.15]). The associations between fatty fish consumption and all other causes of death were not statistically significant (Table 4).
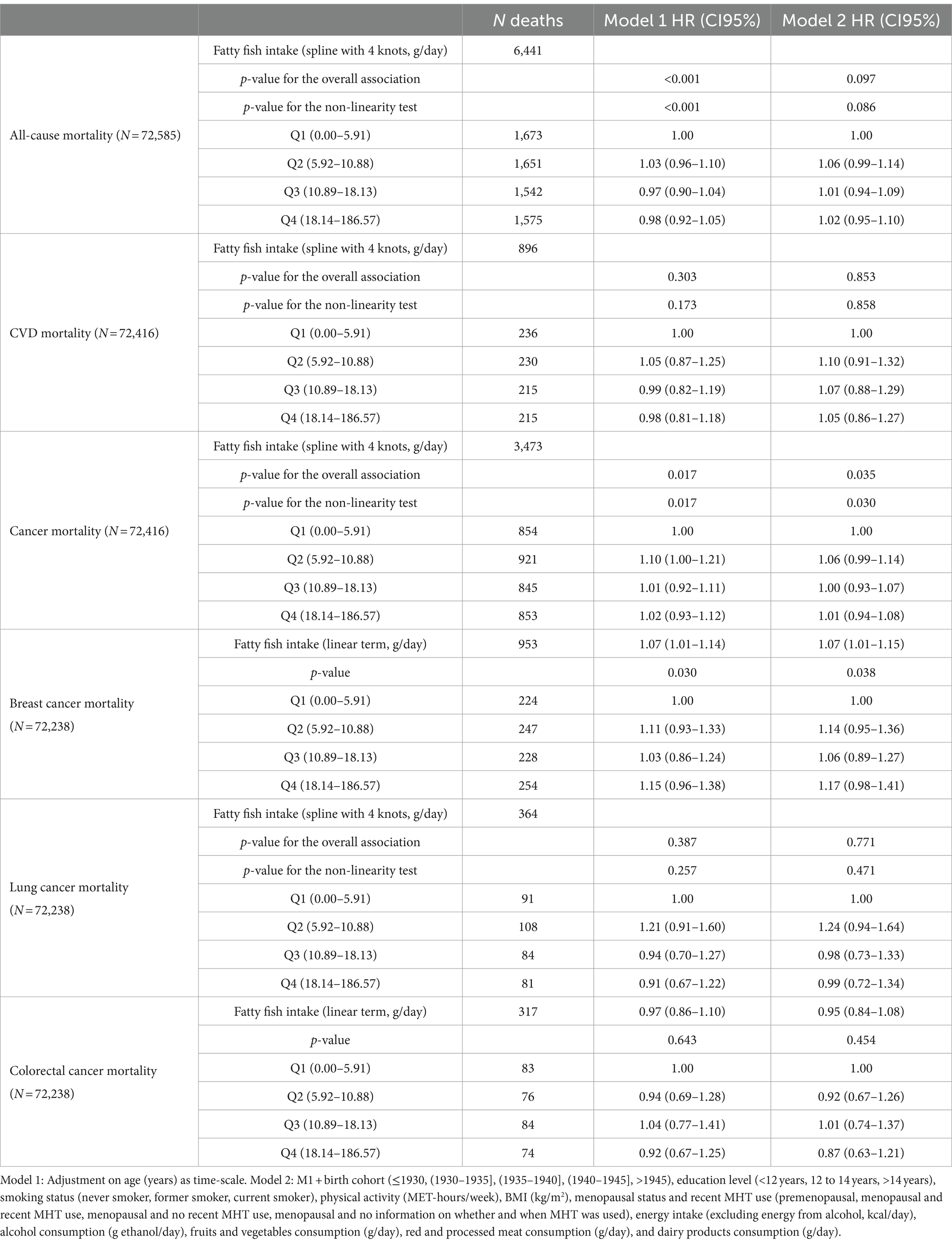
Table 4. Hazard ratios (CI95%) estimated by Cox multivariable regression models for the association between fatty fish consumption and mortality risk in the E3N cohort.
The analysis of the association between n-3 PUFA intake residuals and the risk of all-cause mortality in Model 2 showed a non-linear and not statistically significant association (P overall association = 0.115; Table 5 and Figure 1D). A statistically significant, positive and linear association was revealed between n-3 PUFA intake residuals and the risk of breast cancer mortality (HR [CI95%]: 1.08 [1.01–1.15]). The associations between n-3 PUFA intake residuals and all other causes of death were not statistically significant (Table 5).

Table 5. Hazard ratios (CI95%) estimated by Cox multivariable regression models for the association between n-3 PUFA intake residuals and mortality risk in the E3N cohort.
Results remained virtually unchanged for the four exposure variables in relation to all outcomes tested when further adjusting Model 2 for dietary intake of dioxins and DL-PCBs (Model 3), NDL-PCBs (Model 4), or PBDEs (Model 5; Supplementary Tables 4–7).
3.3 Sensitivity analyses
Similar results to those of the main analyses were observed for the association between fish consumption and all-cause mortality after having included a 5-year exposure lag and excluded 1,663 participants who died or were censored during the first 5 years of follow-up (data not shown).
4 Discussion
This study allowed us to identify a non-linear (U-shaped) association between fish consumption and the risk of all-cause mortality. Indeed, the association between fish consumption and all-cause mortality was inverse up to consumption of 40 g/day: at this consumption level, the risk of all-cause mortality was reduced by around 10% compared to women whom did not consume fish. After this threshold, an inversion of the trend was observed. A similar but stronger association was observed when considering lean fish consumption, while the association between fatty fish consumption or n-3 PUFA intake with all-cause mortality risk was always non-linear but did not reach statistical significance. Interestingly, when observing results for cause-specific mortality risk, a non-linear association between fish consumption was observed in relation to lung cancer mortality, while a positive and linear association was observed between fatty fish consumption or n-3 PUFA intake with respect to breast cancer mortality.
In line with our finding, a meta-analysis similarly identified a U-shaped association between fish consumption and the mortality risk in studies conducted within Western countries (7). To explain the U-shape observed in the association between fish consumption and the risk of all-cause mortality, it had been hypothesised that dietary exposure to POPs could attenuate the beneficial health effects of fish consumption. Indeed, in some studies, the complex interaction between POPs and diet was reported, for example highlighting that POPs have the potential to disrupt the metabolism of beneficial nutrients (23–25). Nevertheless, the results obtained in our study do not allow us to confirm this hypothesis since our results remain virtually unchanged after adjusting the models for dioxins and DL-PCBs, NDL-PCBs, or PBDEs dietary intake. On the other hand, based on this study, no conclusion concerning the role played by other possible contaminants present in fish can be driven. Indeed, the form of association observed in our study could still be explained by the presence of other contaminants such as heavy metals (mercury, cadmium), polycyclic aromatic hydrocarbons (mainly in smoked fish), organochlorine pesticides, and per-and poly fluor alkylated substances.
Moreover, divergent results have been observed among studies conducted in different geographical regions. Several Asian studies have reported an inverse and linear association between fish consumption and all-cause mortality (6, 8, 26, 27). This discrepancy could be explained by geographical variations of n-3 PUFA and POPs in fish (28, 29). It could also be explained by differences in fish preparation methods between the populations studied. Depending on the region, people in Asian countries tend to eat fish either raw, steamed, or sauteed, whereas frying may be more common in Europe (30). The study by Gadiraju et al. shows that frying food causes oxidative degradation, leading to the formation of oxidised compounds and, consequently, an alteration in nutritional properties (31). In addition, a prospective Australian study showed that consumption of non-fried fish was inversely associated with the risk of CVD mortality in women (HR [CI95%]: 0.64 [0.45–0.91]), whereas total fish consumption was not (32). These data suggest that the method of cooking fish, particularly deep-fried fish, could have an impact on the beneficial effects of fish consumption, making it an important subject for future research aimed at elucidating the potential factors that explain these differences.
Concerning cause-specific mortality risk, in agreement with our results, an inverse association between fish consumption and lung cancer incidence has been reported in a meta-analysis including 20 studies (33). On the other hand, the relationship between fish consumption and breast cancer incidence has not yet been fully elucidated and conflicting results have been observed, with some studies suggesting that high consumption of fatty fish is associated with a reduced risk for breast cancer (34, 35), while others observing a positive association between fatty fish consumption and breast cancer (36). Finally, in contrast to many previous studies (37–39), our analyses did not highlight any statistically significant effect on CVD mortality neither due to fish consumption (nor lean, nor fatty) nor to n-3 PUFA intake.
4.1 Strengths and limitations
Several limitations need to be considered when interpreting the results of the present study. Firstly, the generalisability of our results should be treated with caution. Indeed, the E3N cohort is composed of middle-aged French women working for the French national education system, which are leaner and with a higher education level (40), therefore not representative of the French general population. Moreover, concerning the comparison of fish consumption across European countries, some authors concluded that substantial variations exist (41). In addition, food intake is assessed using a self-administered questionnaire, which is subject to misestimation. It is recognised that dietary questionnaires can be affected by social desirability bias and memory bias due to difficulties in recalling food consumption over the last 12 months. These biases can lead to errors in the measurement of fish consumption, n-3 PUFA intake, and exposure to POPs. Nevertheless, the exclusion of energy outliers allows us to take account of under-and over-reporting. Moreover, due to lack of information, we did not consider fish cooking methods in our study, which might have impacted the results. In addition, the questionnaire was completed at baseline, assuming that dietary habits remained unchanged over time. Variations in dietary habits could increase exposure misclassification. However, we assume that the diets of middle-aged women varied little over time as suggested by Thorpe et al. (42). Furthermore, even though we have many adjustment variables, we cannot exclude the presence of residual and unmeasured confounding in the estimation of our associations. Finally, we cannot exclude that the fish contamination levels with POPs have varied between the time when the food consumption data were collected in the E3N cohort (1993) and when the food contamination levels were assessed (2007 and 2009), leading to a possible misclassification of POPs dietary intakes. However, as POPs are persistent in the environment, their concentration in food items varies slowly overtime. Moreover, even if there is a decrease in food items in the time elapsed, POPs are ubiquitous in the environment, so we can assume that this decrease is comparable in all food items, leading to a good classification of participants between them.
Nevertheless, this study presents several strengths. To our knowledge, this is the first epidemiological study to analyse the association between fish consumption and mortality risk, taking into account the dietary exposure to several POPs, highly present in fish. Moreover, to better characterise the effect of fish consumption on health, in the present study it was also possible to make the distinction in the consumption of lean and fatty fish, identified according to lipid content, and to explore the effect of n-3 PUFA intake. In addition, thanks to the long follow-up available in the E3N cohort and the large number of participants, it was possible to investigate the long-term effects of fish consumption and n-n-3 PUFA intake in relation to mortality while ensuring high statistical power. Furthermore, the availability of extensive data on causes of death enabled us to study associations between fish consumption and n-3 PUFA intake, and different specific causes of mortality. Finally, the study population has a low rate of loss to follow-up and a low proportion of missing data, reflecting the quality of the data available in the E3N cohort allowing to adjust for many potential confounding factors.
5 Conclusion
Our study is the first to evaluate the impact of fish consumption, making a distinction between lean and fatty fish, and of n-3 PUFA intake on the risk of all-cause and cause-specific mortality while considering the potential role of dietary exposure to several chemical contaminants. The results highlight a U-shaped association between fish consumption and the risk of all-cause mortality and suggest that consumption of lean fish is the main driver of this association. Further studies are needed to better clarify this non-linear association and the differences between lean and fatty fish in order to provide scientific evidence necessary to develop precise dietary recommendations to the general population.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: sensitive data, available upon request. Requests to access these datasets should be directed to ZnJhbmNlc2NhLm1hbmNpbmlAZ3VzdGF2ZXJvdXNzeS5mcg==.
Ethics statement
The studies involving humans were approved by CNIL (the French National Commission for Data Protection and Privacy). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
CB: Conceptualization, Formal analysis, Investigation, Methodology, Validation, Writing – original draft, Writing – review & editing. CM: Conceptualization, Investigation, Methodology, Supervision, Validation, Writing – original draft, Writing – review & editing. PF: Methodology, Writing – original draft, Writing – review & editing. XR: Writing – original draft, Writing – review & editing. GS: Writing – original draft, Writing – review & editing. FM: Conceptualization, Investigation, Methodology, Supervision, Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work was realised with the data of the E3N cohort of the Inserm and supported by the Mutuelle Générale de l’Education Nationale (MGEN), the Gustave Roussy Institute, and the French League against Cancer for the constitution and maintenance of the cohort. This work has benefited from State aid managed by the National Research Agency under the program “Investment in the future” bearing the reference ANR-10-COHO-0006 as well as subsidy from the Ministry of Higher Education, Research and Innovation for public service charges bearing the reference n°2103586016. This work was also supported by a doctoral funding from the Paris-Saclay University Doctoral School of Public Health EDSP.
Acknowledgments
The authors express their gratitude to all the women who have participated in the E3N cohort, and they extend their appreciation to all members of the E3N study group.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. EFSA. Opinion of the scientific committee on a request from EFSA related to a harmonised approach for risk assessment of substances which are both genotoxic and carcinogenic. EFSA J. (2005) 3:1–31. doi: 10.2903/j.efsa.2005.282
2. Kalmijn, S, van Boxtel, MPJ, Ocké, M, Verschuren, WMM, Kromhout, D, and Launer, LJ. Dietary intake of fatty acids and fish in relation to cognitive performance at middle age. Neurology. (2004) 62:275–80. doi: 10.1212/01.WNL.0000103860.75218.A5
3. Jiang, H, Wang, L, Wang, D, Yan, N, Li, C, Min, W, et al. Omega-3 polyunsaturated fatty acid biomarkers and risk of type 2 diabetes, cardiovascular disease, Cancer, and mortality. Clin Nutr. (2022) 41:1798–807. doi: 10.1016/j.clnu.2022.06.034
4. Bellavia, A, Larsson, SC, and Wolk, A. Fish consumption and all-cause mortality in a cohort of Swedish men and women. J Intern Med. (2017) 281:86–95. doi: 10.1111/joim.12545
5. Engeset, D, Braaten, T, Teucher, B, Tilman Kühn, HB, Bueno-de-Mesquita, ML, Agudo, A, et al. Fish consumption and mortality in the European prospective investigation into Cancer and nutrition cohort. Eur J Epidemiol. (2015) 30:57–70. doi: 10.1007/s10654-014-9966-4
6. Takata, Y, Zhang, X, Li, H, Gao, Y-T, Yang, G, Gao, J, et al. Fish intake and risks of Total and cause-specific mortality in 2 population-based cohort studies of 134, 296 men and women. Am J Epidemiol. (2013) 178:46–57. doi: 10.1093/aje/kws584
7. Jayedi, A, Shab-Bidar, S, Eimeri, S, and Djafarian, K. Fish consumption and risk of all-cause and cardiovascular mortality: a dose-response meta-analysis of prospective observational studies. Public Health Nutr. (2018) 21:1297–306. doi: 10.1017/S1368980017003834
8. Wang, MP, Neil Thomas, G, Ho, SY, Lai, HK, Mak, KH, and Lam, TH. Fish consumption and mortality in Hong Kong Chinese--the LIMOR study. Ann Epidemiol. (2011) 21:164–9. doi: 10.1016/j.annepidem.2010.10.010
9. Giosuè, A, Calabrese, I, Lupoli, R, Riccardi, G, Vaccaro, O, and Vitale, M. Relations between the consumption of fatty or lean fish and risk of cardiovascular disease and all-cause mortality: a systematic review and Meta-analysis. Adv Nutr. (2022) 13:1554–65. doi: 10.1093/advances/nmac006
10. Hengeveld, LM, Praagman, J, Beulens, JWJ, Brouwer, IA, van der Schouw, YT, and Sluijs, I. Fish consumption and risk of stroke, coronary heart disease, and cardiovascular mortality in a Dutch population with low fish intake. Eur J Clin Nutr. (2018) 72:942–50. doi: 10.1038/s41430-018-0190-2
11. Bergkvist, C, Berglund, M, Glynn, A, Julin, B, Wolk, A, and Åkesson, A. Dietary exposure to polychlorinated biphenyls and risk of myocardial infarction in men — a population-based prospective cohort study. Environ Int. (2016) 88:9–14. doi: 10.1016/j.envint.2015.11.020
12. Wennberg, M, Bergdahl, IA, Stegmayr, B, Hallmans, G, Lundh, T, Skerfving, S, et al. Fish intake, mercury, long-chain n-3 polyunsaturated fatty acids and risk of stroke in northern Sweden. Br J Nutr. (2007) 98:1038–45. doi: 10.1017/S0007114507756519
13. Salonen, JT, Seppänen, K, Nyyssönen, K, Korpela, H, Kauhanen, J, Kantola, M, et al. Intake of mercury from fish, lipid peroxidation, and the risk of myocardial infarction and coronary, cardiovascular, and any death in eastern Finnish men. Circulation. (1995) 91:645–55. doi: 10.1161/01.CIR.91.3.645
14. Clavel-Chapelon, Françoise and for the E3N Study Group. Cohort profile: the French E3N cohort study. Int J Epidemiol. (2015) 44:801–9. doi: 10.1093/ije/dyu184
15. Liere, V, Marti, J, Lucas, F, Clavel, F, Slimani, N, and Villeminot, S. Relative validity and reproducibility of a French dietary history questionnaire. Int J Epidemiol. (1997) 26:128S–1136S. doi: 10.1093/ije/26.suppl_1.S128
16. ANSES (2013). Table de Composition Nutritionnelle Des Aliments Ciqual. 2013. Available at: https://ciqual.anses.fr/ (Accessed March 11, 2024).
17. ANSES (2011). Second French Total Diet Study (TDS 2) report 2 pesticide residues, Additives, Acrylamide and Polycyclic Aromatic Hydrocarbons. Expert Report. Available at: https://www.anses.fr/en/system/files/PASER2006sa0361Ra2EN.pdf (Accessed March 11, 2024).
18. Sirot, V, Guérin, T, Volatier, J-L, and Leblanc, J-C. Dietary exposure and biomarkers of arsenic in consumers of fish and shellfish from France. Sci Total Environ. (2009) 407:1875–85. doi: 10.1016/j.scitotenv.2008.11.050
19. Mancini, FR, Praud, D, Fervers, B, and Boutron-Ruault, M-C. Estimation of the dietary exposure to chemical compounds in the French E3N prospective cohort: a study protocol. Food Addit Contam Part A. (2020) 37:39–47. doi: 10.1080/19440049.2019.1678772
20. Schofield, WN. Predicting basal metabolic rate, new standards and review of previous work. Hum Nutr Clin Nutr. (1985) 39:5–41.
21. Willett, WC, Howe, GR, and Kushi, LH. Adjustment for Total energy intake in epidemiologic studies. Am J Clin Nutr. (1997) 65:1220S–8S. doi: 10.1093/ajcn/65.4.1220S
22. Harrell, F. Regression modeling strategies: with applications to linear models, logistic regression, and survival analysis, Springer Series in Statistics. New York: Springer-Verlag (2001).
23. Cano-Sancho, G, and Casas, M. Interactions between environmental pollutants and dietary nutrients: current evidence and implications in epidemiological research. J Epidemiol Community Health. (2020) 75:108–13. doi: 10.1136/jech-2020-213789
24. Ibrahim, MM, Fjære, E, Lock, E-J, Naville, D, and Amlund, H. Chronic consumption of farmed Salmon containing persistent organic pollutants causes insulin resistance and obesity in mice. PLoS One. (2011) 6:e25170. doi: 10.1371/journal.pone.0025170
25. Li, X, Wang, M, Yang, Y, Lei, B, Ma, S, and Yingxin, Y. Influence of nutrients on the bioaccessibility and Transepithelial transport of Polybrominated diphenyl ethers measured using an in vitro method and Caco-2 cell monolayers. Ecotoxicol Environ Saf. (2021) 208:111569. doi: 10.1016/j.ecoenv.2020.111569
26. Lee, JE, McLerran, DF, Betsy Rolland, Y, Chen, EJ, Grant, RV, Inoue, M, et al. Meat intake and cause-specific mortality: a pooled analysis of Asian prospective cohort studies 123. Am J Clin Nutr. (2013) 98:1032–41. doi: 10.3945/ajcn.113.062638
27. Yamagishi, K, Iso, H, Date, C, Fukui, M, Wakai, K, Kikuchi, S, et al. Fish, Omega-3 polyunsaturated fatty acids, and mortality from cardiovascular diseases in a Nationwide Community-based cohort of Japanese men and women the JACC (Japan collaborative cohort study for evaluation of Cancer risk) study. J Am Coll Cardiol. (2008) 52:988–96. doi: 10.1016/j.jacc.2008.06.018
28. Fonseca, VF, Duarte, IA, Matos, AR, Reis-Santos, P, and Duarte, B. Fatty acid profiles as natural tracers of provenance and lipid quality indicators in illegally sourced fish and bivalves. Food Control. (2022) 134:108735. doi: 10.1016/j.foodcont.2021.108735
29. Nicklisch, SCT, Bonito, LT, Sandin, S, and Hamdoun, A. Geographic differences in persistent organic pollutant levels of yellowfin tuna. Environ Health Perspect. (2017) 125:067014. doi: 10.1289/EHP518
30. Djoussé, L, Petrone, AB, and Michael Gaziano, J. Consumption of fried foods and risk of heart failure in the physicians’ health study. J Am Heart Assoc Cardiovas Cerebrovas Dis. (2015) 4:e001740. doi: 10.1161/JAHA.114.001740
31. Gadiraju, TV, Yash Patel, J, Gaziano, M, and Djoussé, L. Fried food consumption and cardiovascular health: a review of current evidence. Nutrients. (2015) 7:8424–30. doi: 10.3390/nu7105404
32. Owen, AJ, Magliano, DJ, O’Dea, K, Barr, ELM, and Shaw, JE. Polyunsaturated fatty acid intake and risk of cardiovascular mortality in a low fish-consuming population: a prospective cohort analysis. Eur J Nutr. (2016) 55:1605–13. doi: 10.1007/s00394-015-0979-x
33. Song, J, Hong, S, Wang, B-l, Zhou, Y-y, and Guo, L-L. Fish consumption and lung Cancer risk: systematic review and Meta-analysis. Nutr Cancer. (2014) 66:539–49. doi: 10.1080/01635581.2014.894102
34. Engeset, D, Alsaker, E, Lund, E, Welch, A, Khaw, K-T, Clavel-Chapelon, F, et al. Fish consumption and breast Cancer risk. The European prospective investigation into Cancer and nutrition (EPIC). Int J Cancer. (2006) 119:175–82. doi: 10.1002/ijc.21819
35. Terry, P, Rohan, TE, Wolk, A, Maehle-Schmidt, M, and Magnusson, C. Fish consumption and breast Cancer risk. Nutr Cancer. (2002) 44:1–6. doi: 10.1207/S15327914NC441_1
36. Stripp, C, Overvad, K, Christensen, J, Thomsen, BL, Olsen, A, Møller, S, et al. Fish intake is positively associated with breast Cancer incidence rate. J Nutr. (2003) 133:3664–9. doi: 10.1093/jn/133.11.3664
37. Jiang, L, Wang, J, Xiong, K, Lei, X, Zhang, B, and Ma, A. Intake of fish and marine N-3 polyunsaturated fatty acids and risk of cardiovascular disease mortality: a Meta-analysis of prospective cohort studies. Nutrients. (2021) 13:2342. doi: 10.3390/nu13072342
38. Kapoor, B, Kapoor, D, Gautam, S, Singh, R, and Bhardwaj, S. Dietary polyunsaturated fatty acids (PUFAs): uses and potential health benefits. Curr Nut Rep. (2021) 10:232–42. doi: 10.1007/s13668-021-00363-3
39. Zheng, S, Qiu, M, Wu, JHY, Pan, X-f, Liu, X, Sun, L, et al. Long-chain Omega-3 polyunsaturated fatty acids and the risk of heart failure. Therap Adv Chron Dis. (2022) 13:20406223221081616. doi: 10.1177/20406223221081616
40. Clavel-Chapelon, F, van Liere, MJ, Giubout, C, Niravong, MY, Goulard, H, Le Corre, C, et al. E3N, a French Cohort Study on Cancer Risk Factors. E3N Group. Etude Epidémiologique Auprès de Femmes de l’Education Nationale. Europ J Cancer Prevent. (1997) 6:473–8. doi: 10.1097/00008469-199710000-00007
41. Welch, AA, Lund, E, Amiano, P, Dorronsoro, M, Brustad, M, Kumle, M, et al. Variability of fish consumption within the 10 European countries participating in the European investigation into Cancer and nutrition (EPIC) study. Public Health Nutr. (2002) 5:1273–85. doi: 10.1079/PHN2002404
Keywords: fish, omega 3, mortality, persistent organic pollutant, women, cohort
Citation: Ba C, Marques C, Frenoy P, Ren X, Severi G and Mancini FR (2024) Association between fish consumption and mortality in the E3N French women’s cohort. Front. Nutr. 11:1462710. doi: 10.3389/fnut.2024.1462710
Edited by:
Anne Marie Minihane, University of East Anglia, United KingdomReviewed by:
Stine Marie Ulven, University of Oslo, NorwayHussein N. Yassine, University of Southern California, United States
Copyright © 2024 Ba, Marques, Frenoy, Ren, Severi and Mancini. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chloé Marques, Y2hsb2UubWFycXVlc0BndXN0YXZlcm91c3N5LmZy
†These authors have contributed equally to this work and share first authorship