 Tagese Yakob1*
Tagese Yakob1* Eskinder Israel1
Eskinder Israel1 Begidu Yakob2
Begidu Yakob2 Mekdes Meshesha1
Mekdes Meshesha1 Endale Jambo1Tadewos Utalo3
Endale Jambo1Tadewos Utalo3 Awoke Abraham1
Awoke Abraham1- 1School of Public Health, College of Health Science and Medicine, Wolaita Sodo University, Sodo, Ethiopia
- 2Division of Nutrition, Maternal and Child Health Unit, Wolaita Zone Health Department, Sodo, Ethiopia
- 3Integrated Emergency Surgery and Obstetrics (IESO), Maternal and Child Health Unit, Bele Primary Hospital, Sodo, Ethiopia
Background: Globally, more than 815 million estimated people worldwide suffer from malnutrition or are unable to access enough food due to malnutrition. Conflict remains the single most fundamental factor contributing to chronic malnutrition in the conflict-affected areas. Developing a healthy and balanced dietary pattern is essential for school children because their habits in this period may last longer. Therefore, the current study aimed to assess dietary adequacy level and factors associated among school children in conflicts affected communities of southern Ethiopia.
Method and materials: A community-based cross-sectional study was conducted among 616 schoolchildren aged 6 to 12 years with their caregivers using a multistage sampling method. The data were collected by using a structured questionnaire. The data were collected and entered into Epi-data version 4.6.0.2 and exported to STATA software version 14 for analysis. Adequate dietary diversity was defined as the consumption of at least five food groups. Both bivariable and multivariable binary logistic regression were performed. A p-value less than 0.05 on multivariate logistic regression indicated a statistically significant association.
Results: The overall response rate of this study was 98.5%. The median [inter quartile range (IQR)] dietary diversity score of the studies was 4(3–5) with the prevalence of inadequate dietary diversity among the school children of current study was 59.4% (95% CI, 55.17–62.99). In this study, schoolchildren with no near-health care facility (AOR = 1.95, 95% CI; 1.35–2.82), a family size greater than five (AOR = 1.44, 95% CI; 1.01–2.05), and the absence of a family home garden (AOR = 1.55, CI: 1.35–1.83) were significantly associated with low dietary diversity in school children.
Conclusion: When compared with other studies, dietary diversity in the current study area was low. This emphasizes the need to encourage mothers to use family planning and implementing focused public health interventions, such school lunch programs and community gardening projects, to improve children’s nutritional outcomes and dietary diversity.
Background
World Health Organization (WHO) has reported that one in every two school-aged children suffers from hunger (1). Globally, more than 815 million estimated people worldwide suffer from malnutrition or are unable to access enough food due to malnutrition (2). In Africa, nearly 40% (60 million) school children had faced malnutrition (3).
Malnutrition is the leading and most important factor for morbidity and mortality among children worldwide (4). School age is an important period of children’s life that needs the right attention and their diversified diet intake are more momentous (5). Children are very prone to malnutrition due to many reasons, such as low dietary intake, food insecurity within the household, infectious diseases, and inadequate health care (6).
Due to their slow and steady growth pattern before puberty, school-aged children require a wide range of nutrient-dense foods that must be gradually adjusted in term of quantity and portion size to meet their rising energy needs (7). Ensuring their health through the use of protein, fat, vitamin, and minerals can better support their overall growth and development (8). For children, optimal nutrition is crucial for child brain development as well as normal physical and cognitive development (9, 10). Less recommended diet decreases the health and physical growth and negatively affects their cognitive and social skills (6, 10, 11).
Conflict remains the single most fundamental factor contributing for chronic malnutrition in the conflict affected areas (12, 13). The community will be unable to work for the agriculture and basic livelihood when there is intermittent conflict and have gross effect on the community wellbeing including children (13, 14).
The “zero hunger” Sustainable Development Goal (SDG) targets 2.1 and 2.2 aims to “ensure that everyone has access all years round healthy, nutritious, and sufficient food” and “put an end to all forms of malnutrition, including eradicating hunger (7). In Ethiopia, Ministry of Education is committed to the promotion of quality health and nutrition for school-age children who constitute more than 25% of the total population (15), and of whom a major portion suffer from alarming levels of ill health, nutritional deficiencies and morbidity. In response to this, Ethiopia Federal Ministry of Health (FMOH) has been striving to eradicate malnutrition and enable the health and nutrition status to be improved for a significant proportion of Ethiopia’s population, promoting healthy attitudes, knowledge and behaviors throughout their lifetime among school age children through compressive national School Health and Nutrition (SHN) strategy (16). Despite various studies have assessed the dietary diversity of school age children in different countries including Ethiopia, among general communities, none have explored in conflict-affected communities (17–19). Careful assessing and identifying this will improve school children’s nutritional status and significantly improve overall child’s development. Therefore, the current study aimed to assess dietary adequacy level and factors associated among school children in conflicts affected communities of southern Ethiopia.
Materials and methods
Study area, period, and design
A community-based cross-sectional study was conducted from 16th June to 23rd July 2023 in Konso zones, southern region of Ethiopia. The Konso Zone is one of the 12 zones in the southern region of Ethiopia. The Konso Zone is divided into five districts (Konso zuriya, Kena, Koleme, Karat city administration and Segen Zuriya) with an estimated total population of 359,998 and a total of 43 Kebeles. It is situated 595 km away from the capital city of Ethiopia, Addis Ababa. Konso shares a border with the northwest Alle zone’s Burji zone in the east, the northeastern Amaro zone’s Gardula zone in the north, the Ari zone in the southwest, and the Borena zone of Oromia in the south (20). Mixed farming, or the production of both crops and animals, is the primary source of household income in many districts. The main cabbage tree in the area is Moringa stenopetala, also known as Shelaqta’an in Konso. Fresh green leaves are used in everyday meals as a vegetable that is cooked and consumed, and they can also be sold for cash in the neighborhood market. This area in Ethiopia is impacted by intercommunal conflict (21).
Population, sample size calculation, and sampling procedure
All school-age children paired with their parents or caregivers in conflicts affecting the community of southern Ethiopia were the source population, and all school-age children were systematically selected from randomly sampled households with their parents or caregivers in the selected Keble. Only households with at least one school-age child aged between 6 and 12 years of age with their parent/caregiver’s pair were included in this study. Study participants who were sick during the previous week and who had a special ceremony on the day before data collection were excluded from the study.
The sample size was calculated based on the single population formula by Epi-data version 4.6.0.2 considering the following assumptions: P (proportion of dietary diversity practice among school-age children) = 58.3% of the studies conducted with school children in the Gurage Zone, Ethiopia (18); margin of error (d) = 5%; confidence level = 95%; n = (Za/2)2p (1−p)/d2; n = sample size = 373; and a multiplier design effect of 1.5 = 560. After considering a 10% non-response rate, the final sample size was 616.
Analogously, related studies (22, 23) have employed this methodology. Using a multistage simple random sampling technique, districts and kebeles within the study area were chosen. Four of the five districts—three rural districts and one district with an intentionally chosen karate city administration—were included in the study. Twelve kebeles (three in each) were chosen from these districts using a simple random sampling number. Next, in the chosen kebeles, every household was registered as a sampling frame. Ultimately, the sample size was distributed proportionally among the designated kebeles in the respective districts, and the respondents were selected through a computer-generated basic random sampling procedure.
Study variables
The dietary diversity score (DDS) was used as the outcome variable in this study. The independent variables were sociodemographic characteristics (age, maternal status, maternal and paternal education status, mother and father occupational status, child sex, child birth order, resident, family size, household head, household security), environmental characteristics (water source, type of water treatment, availability of latrine, hand washing practice), comorbidity of children (chronic disease conditions, acute illness for the last 2 weeks), and access-related characteristics (animal in household of their family, own farm land, media, presence of home garden, access to fruit/vegetables, time to reach health care from home, and access to healthcare services).
Operational definition
The dietary diversity score was defined as the total count of different food groups irrespective of the amount consumed by children in the 24-h period preceding the survey by 24-h dietary recall method. It was developed using the mother’s recollection of the food groups the child had consumed in the 24 h prior to the survey. A 10 food groups were reported by mothers as being consumed by the child: (1) cereals, roots and tubers; (2) Legumes/pulse; (3) Dairy products (milk, yogurt, cheese); (4) Flesh foods; (5) Eggs; (6) Vitamin-A rich fruits and vegetables; (7) Other fruits and vegetables; (8) nut and seeds; (9) meat and meat products and (10) other meat products (18, 24, 25) and each food groups response options were ‘yes, consumed’ (score 1) and ‘no, not consumed’ (score 0). These were added up to create child DDS, which range from 0 to 7. The outcome variable (diet diversity) was measured by inadequate/adequate. A child is considered having poor/inadequate/diet diversity when he/she eats less than four types of food groups per day (within 24 h) (26). Finally, those children who categorized adequate/meet the minimum/dietary diversity score were coded as “1” and those who categorized inadequate/did not meet minimum/dietary diversity score were coded as “0” for regression analysis.
Household security (hanger scale) was categorized into three levels based on the FANTA recommendation (24, 27).
Near-health care facility: at least health facility should be within 5 km from communities’ inhabitant or 1 h walking distance from living house to health facility.
School age: children aged 6–12 years were included (18).
Data collection tools and quality control
The data were collected via face-to-face interviews using pretested validated food frequency questionnaires adapted from related literature (5, 6, 17–19, 23, 28, 29). It was collected from caregivers by allowing them to freely recall the type of food items they feed their children within the last 24 h.
The data collectors were trained before the data collection for 2 days on how to ask questions and code answers. Close supervision was provided by the investigators and the assigned supervisors. Any quest related to clarity, ambiguity, incompleteness, or misunderstanding was resolved on the day following the next day. Pretests were performed on 5% of the sample nearby city called Kelle and necessary amendments like spelling and appropriate word selection were done. The questionnaire was prepared in English, translated to the local language and checked for consistency by translating it back to English by those who were well-oriented with the stated languages. All finalized data collection forms were checked for completeness and clarity before and during data management, storage and analysis.
Data processing and analysis
The data were entered into Epi-data version 4.6.0.2 and exported to STATA software version 14 for analysis. Before the analysis of the data, the variables were recoded to facilitate analysis. Descriptive statistics such as the frequency for all variables and median with interquartile range (IQR) some specific variable were computed. Multicollinearity regression coefficient based was checked by the help of variance inflation factor based on value of VIF <10 that updates no collinearity among independent predictors. Binary logistic regression was performed to examine the association of each independent variable with the outcome variable. Variables with p-value <0.25 in the bivariable analysis were selected and included in the final multivariable logistic regression analysis. Multivariate logistic regression was performed to identify the independent predictors of outcome variable. Associated variable was tested at 95% of CI and summarized by using AOR and any variable with p-value <0.05 in the final model was taken as statistically significant. Model fitness was checked by using Hosmer and Lemeshow’s test, with a p-value greater than 0.05 indicating a fitted regression model (that was p-value = 0.905). After checking for multi-collinearity, the associations between dependent and independent variables were measured using odds ratio (OR) with 95% confidence interval (CI) at p-value <0.05. Finally, the results of the study are presented in the form of text, tables, and figures.
Results
Sociodemographic characteristics of the respondents
The overall response rate of this study was 98.5%. Majority of households (91.1%) household head was fathers. Nearly half (45.9%) of the heads of household were aged 20–29 years. A significant percentage of mothers (72.3%) were housewives and about 58.3% had no formal education. About nearly two-third, (62.4%) of fathers were farmers/herdsmen, and greater than one-third, 255 (42.0%) of fathers had completed primary school. More than half of the school children (325, 53.5%) were male, nearly two-thirds, 370 (60.1%) of the school children were aged 6–8 years, and more than one-third, 246 (40.5%) of the children were intermediate birth order. The majority, 530 (87.3%) of study participants were living in rural areas (Table 1).
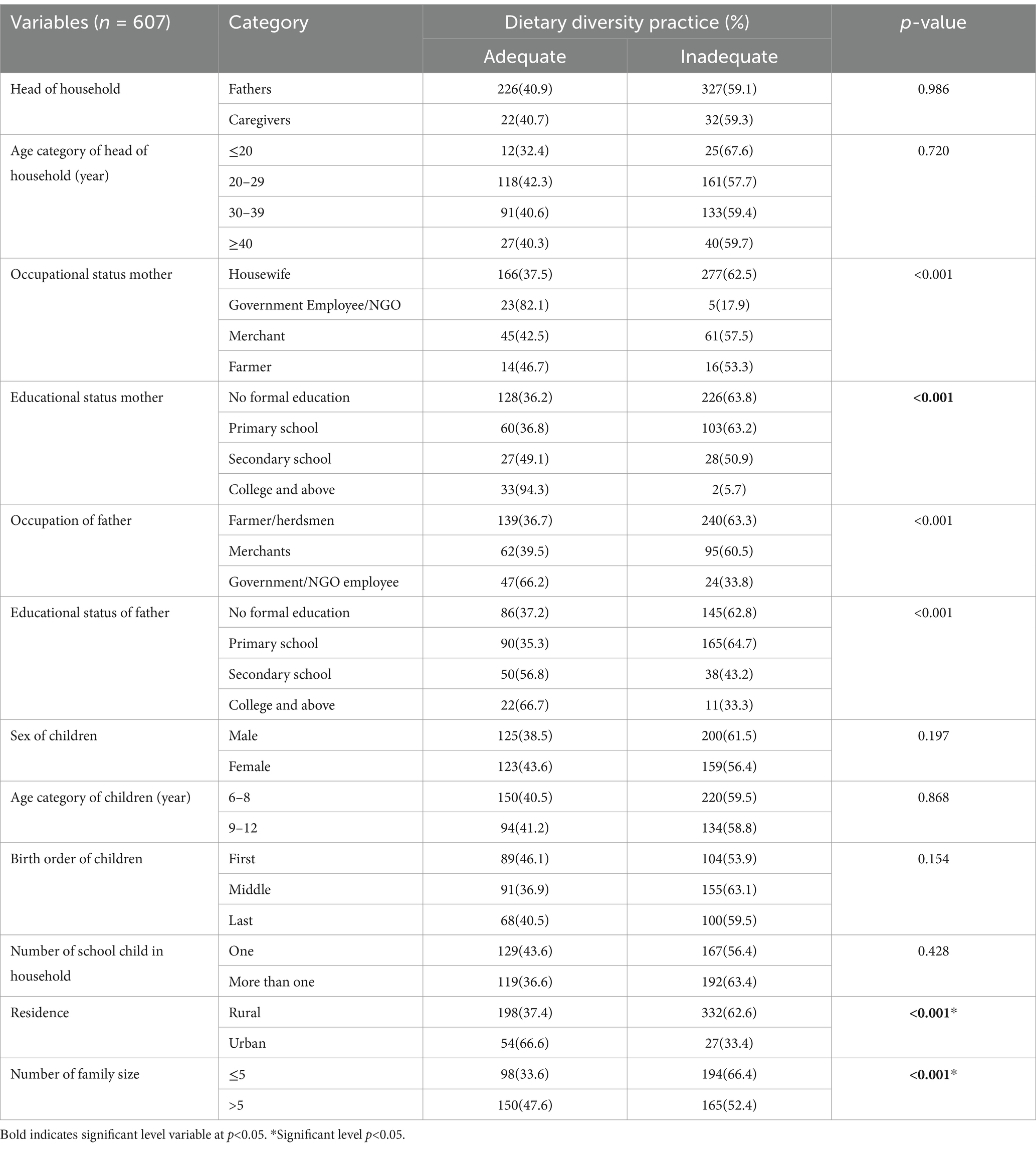
Table 1. Sociodemographic characteristics of respondents in conflict-affecting communities in the southern region of Ethiopia, 2023.
Environmental characteristics of the respondents
Greater than one-third, 241 (39.7%) of the study participants used communal water. The majority (505, 83.1%) had access to water near their residence area, and more than one-third (33.9%) of the respondents did not use any type of water treatment. Greater than two-thirds (77.3%) of the respondents had a toilet. Overall, 454 (74.8%) practiced hand washing either before or after eating or before or after food processing (Table 2).
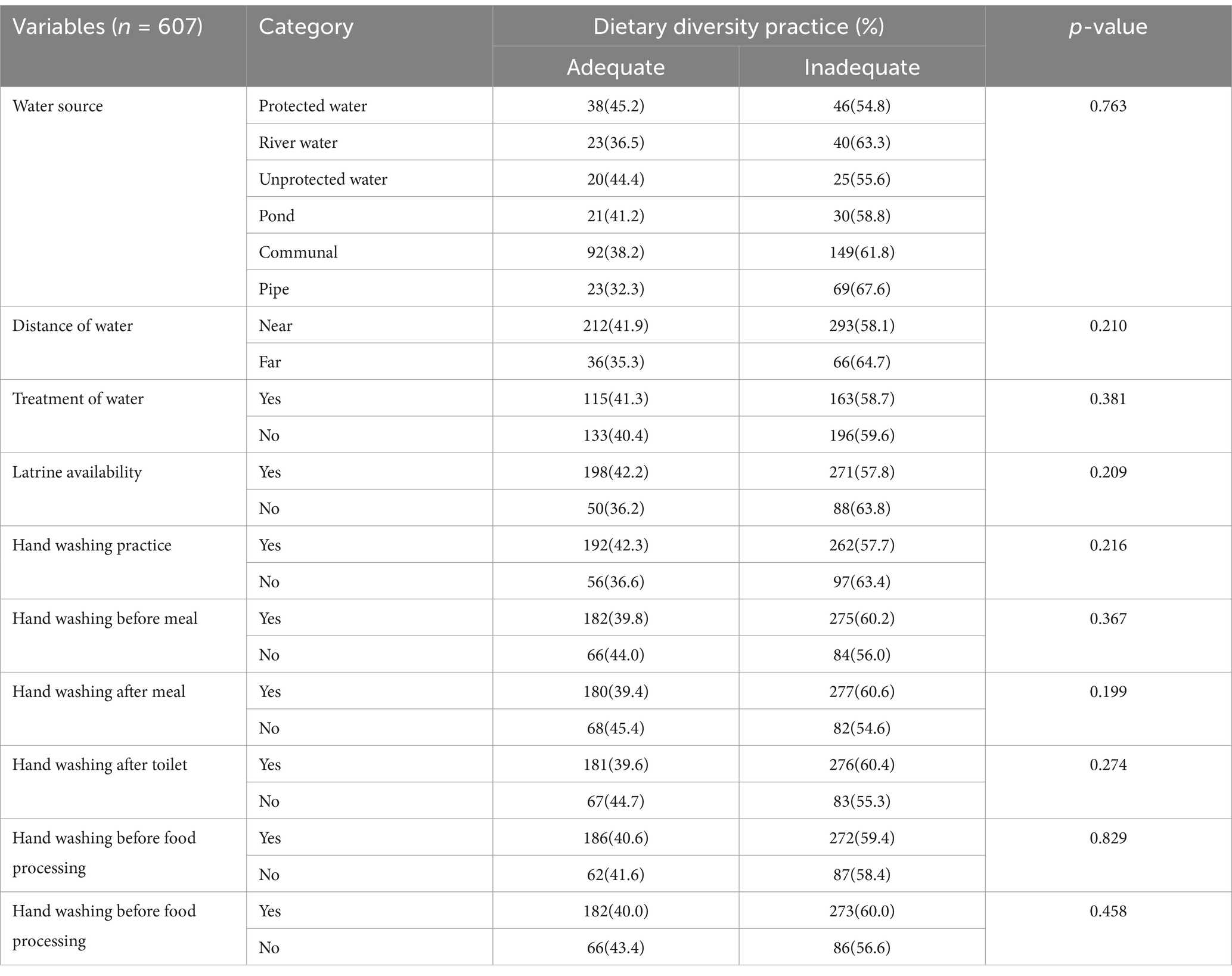
Table 2. Environmental characteristics of respondents in conflict affecting communities in the southern region of Ethiopia, 2023.
Comorbid conditions of the school children
Of the total school children, 96 (23.6%) had chronic diseases. Overall, 78 (18.8%) of the school-aged children had fever 2 weeks prior to data collection. Of these, 25 (32.1%) had related diarrheal disease, and 24 (30.7%) had upper respiratory tract infections (Table 3).
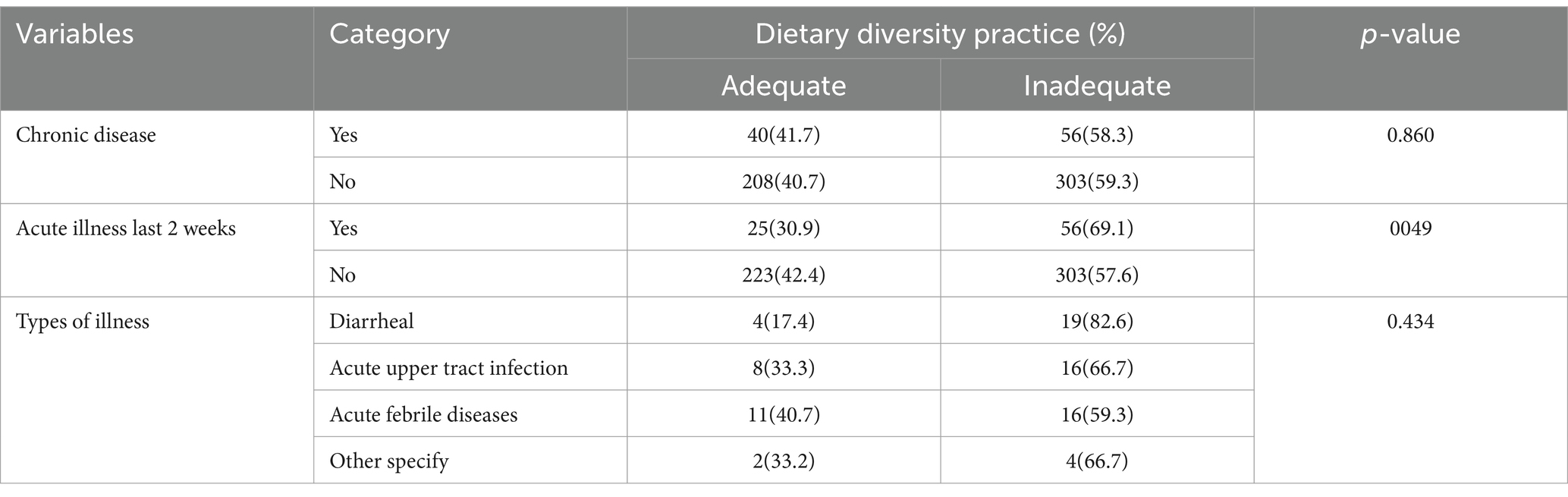
Table 3. Comorbidity conditions of schoolchildren in conflict affecting communities in the South Region, Ethiopia, in 2023.
Access-related characteristics of the respondents
The majority, 527 (86.8%) of study participant had animals in the household of their family, and a significant number of households, 424 (69.8%), had their own farmland. The majority, 524 (86.3%) of their households had access to any type of media. Greater than one-third, (469, 77.3%) of the participants had home gardens and nearly two-thirds, (386, 63.6%) had access to fruits/vegetables. Nearly two-third, 357 (58.8%) of the respondents were near the market to their living house, and nearly half, (323, 53.2%) had access to healthcare services within ≤1 h (Table 4).
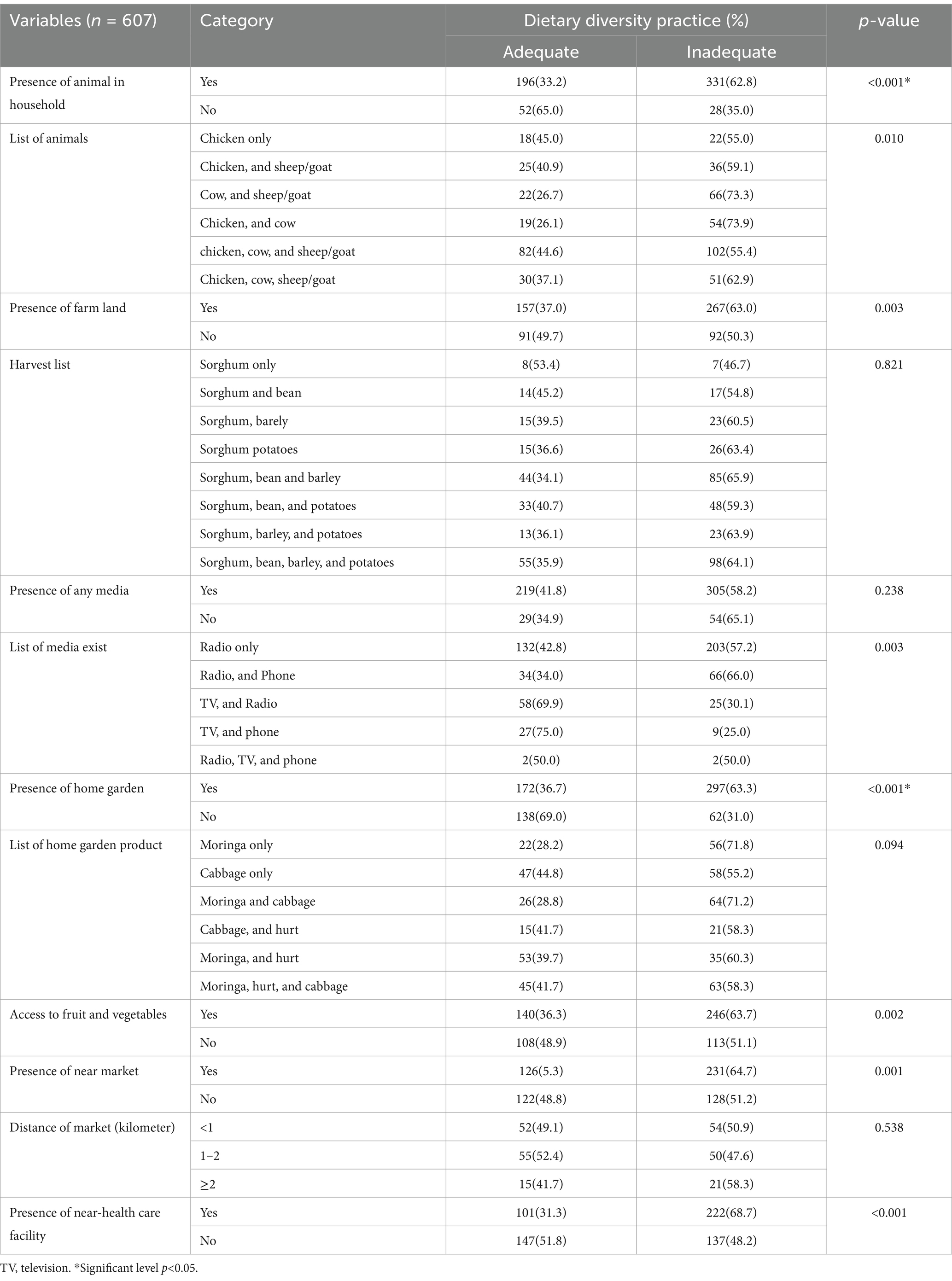
Table 4. Access-related characteristics of school-aged children in conflict-affecting communities in the South Region, Ethiopia, in 2023.
Household food security
About 42.3% of respondents were secured with food access scales. In the past 4 weeks, 46.7% were worried about household food shortages, 48.6% could not eat the kinds of foods they preferred, 40.3% ate a limited variety of foods, 39.2% ate some foods that truly did not want to eat, 37.5% ate a smaller meal than you felt, 46.8% ate a fewer meal a day, 36.2% went to sleep at night hungry and 33.1% went a whole day and night eating nothing (Table 5).
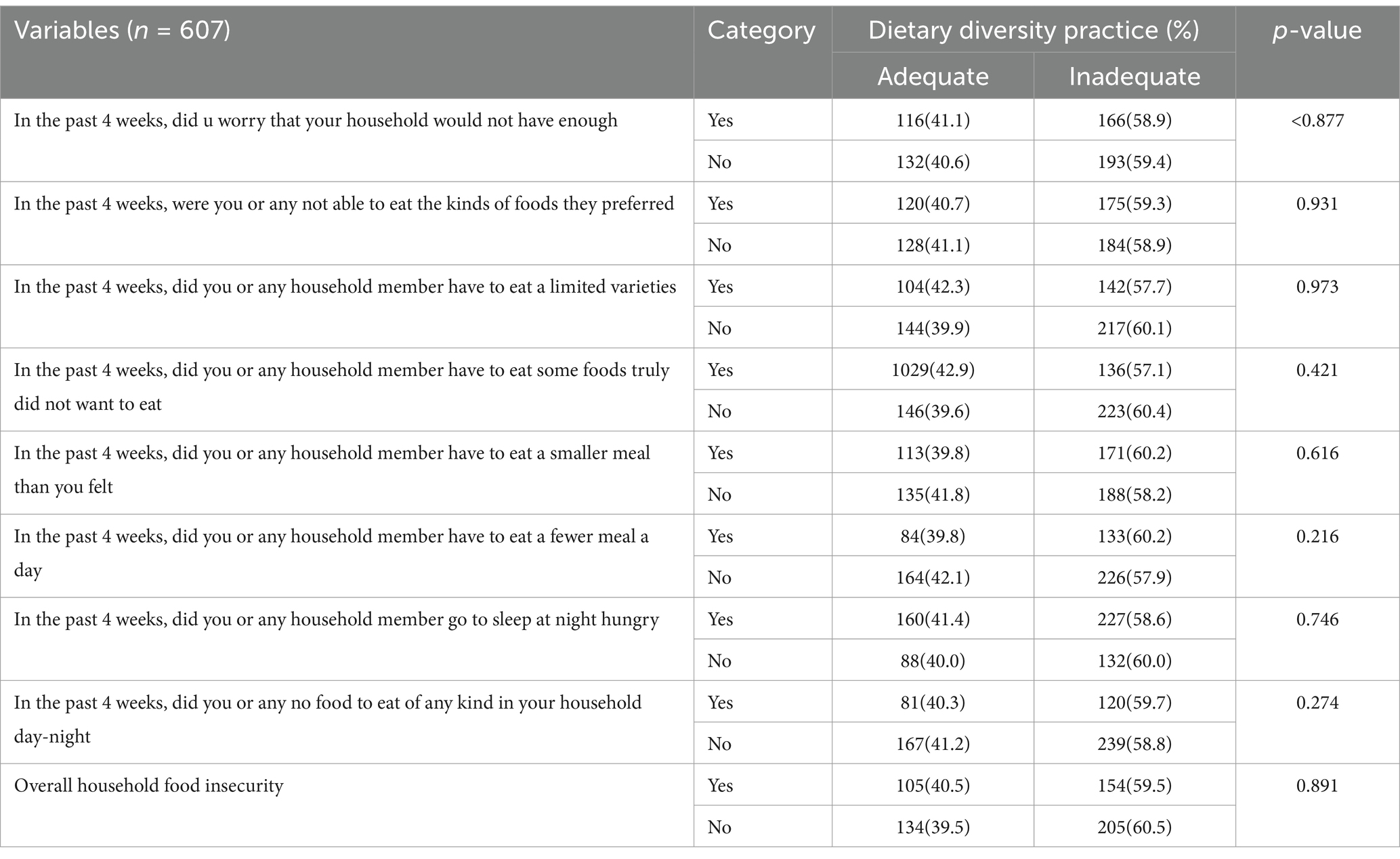
Table 5. Household food insecurity of respondents in conflict affecting communities in the South Region, Ethiopia, 2023.
Dietary diversity practice
The median (IQR) dietary diversity score of the participants was 4 (3–5). The prevalence of study participants with inadequate dietary diversity in this study was 59.4% (95% CI, 55.17–62.99). Flesh food (9.9%) was the food group least consumed by the school-age children, and cereals, roots and tubers (90.1%) were the most consumed food group by the school-age children (Figures 1, 2).
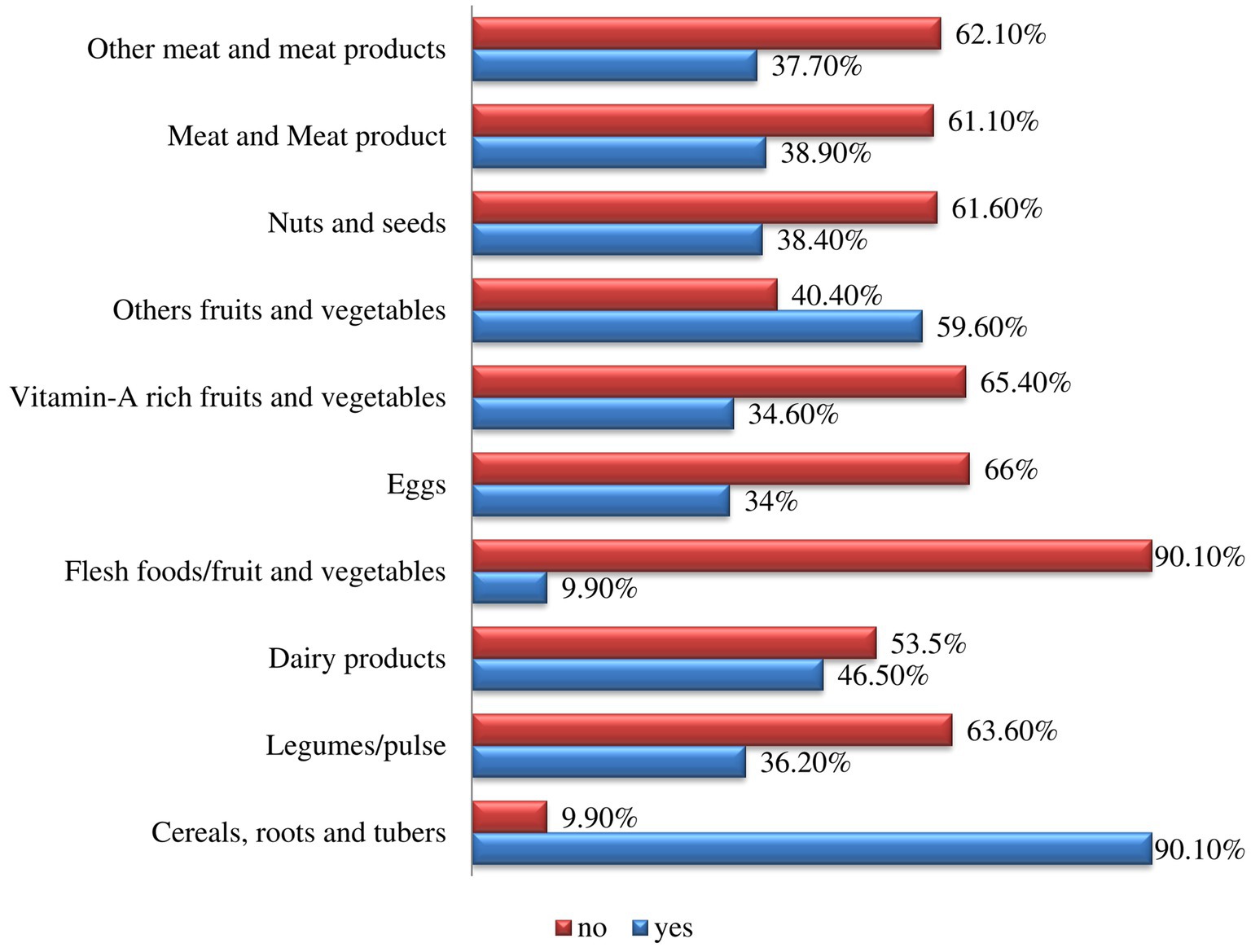
Figure 1. A 10 food group dietary diversity measured using the 24-h recall method for schoolchildren in conflict-affecting communities in the southern region of Ethiopia in 2023.
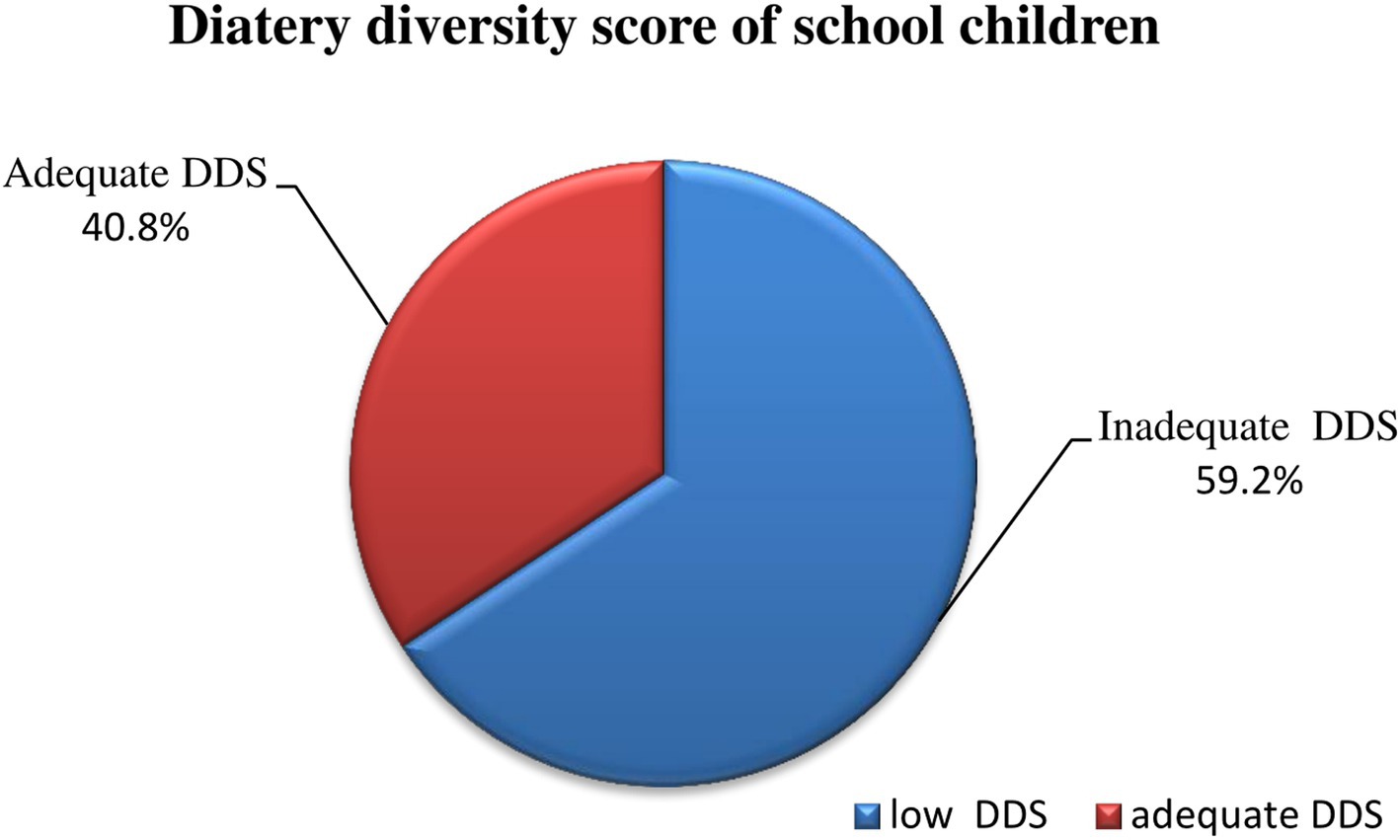
Figure 2. Measure of dietary diversity practices of schoolchildren in conflict affecting communities in the South Region, Ethiopia, in 2023.
Factors affecting school-age children’s dietary diversity practices
All the independent variables were analyzed via logistic regression with the dependent variable of school children’s dietary diversity practices to analyze their associations. Nine variables were significantly associated with school dietary diversity according to binary logistic regression (p-value ≤0.25) and were entered into the multiple logistic regression analysis. There was a significant association between the following variables: educational level of the father, residence, number of family members, birth order, time to reach health care from home, fruit/vegetable access, presence of a home garden, presence of an animal, and presence of a market resident area.
In this study, schoolchildren who were not at a health care facility were 1.95 times higher odds of having inadequate diet diversity than were their counterparts (AOR = 1.95, 95% CI; 1.35–2.82). Schoolchildren with family sizes greater than five were 1.44 times higher odds of having inadequate diet diversity than their counterparts were (AOR = 1.44, 95% CI; 1.01–2.05). School children with no family home garden were 1.55 times higher odds of having inadequate diet diversity [AOR = 1.55, CI: (1.35–2.03)], which was significantly associated with inadequate dietary diversity in the study area (p-value <0.05) (Table 6).
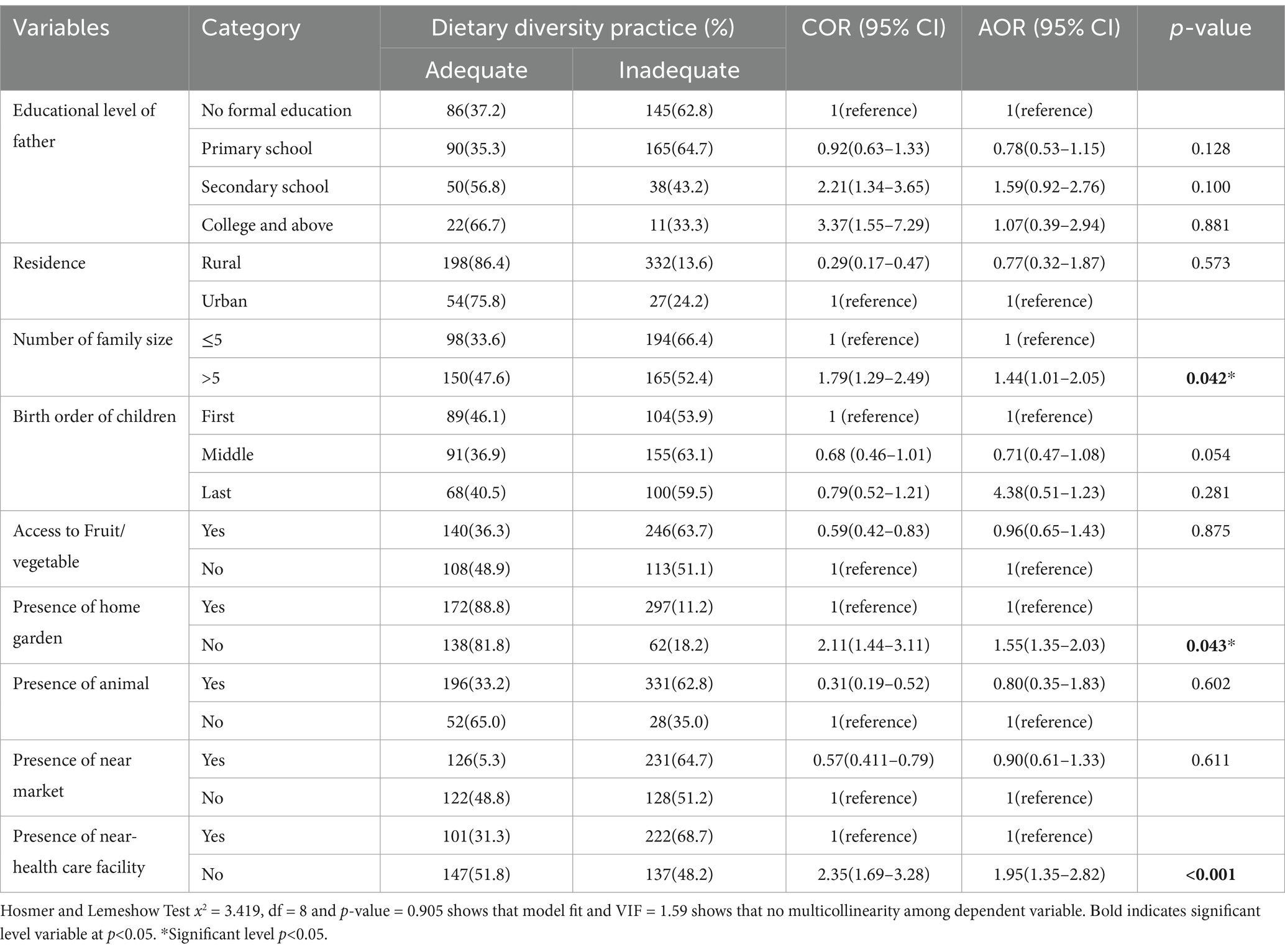
Table 6. Bivariable and multivariable logistic regression analysis of factors associated with school children in conflict affecting communities in the southern region of Ethiopia in 2023.
Discussion
This community-based study assessed dietary diversity and its predictors among school-age children in the southern region of Ethiopia. The median (IQR) dietary diversity score of the participants was 4 (3–5), and the prevalence of inadequate dietary diversity among the schoolchildren in this study was 59.4% (95% CI, 55.17–62.99). This finding was lower than that reported in a previous study (30), which was 19.2%, and a study conducted in India (31). This variation might be due to the variation of food groups included, environmental and cultural differences between study settings. The results of our study align with those of a study conducted in the Gurage Zone, southern Ethiopia (58.3%) (18). This might due to similarity socioeconomic characteristic of both study setting. However, the results of this study were better than those of studies conducted in the EDHS (10.8%) (32), Merawi town, Amhara region, Ethiopia (8%) (25), Sinan districts (13%) (33), the Gonder Zone (16.2%) (34), the Mirab Abaya district in the southern region of Ethiopia (34.3%) (35) and the Wolaita Sodo region (43.2%) (36). Possible explanations for these variations could be the sociocultural, economic, and geographical differences between the study area and the referenced places. Further, this might be because a significant number of participants in the study area had animals in the household of their family, their own farmland and access to fruit/vegetables may have affected their dietary practices compared with those in other studies.
The study revealed that children from extended families were 1.44 times higher odds of having inadequate diet diversity (AOR = 1.44, 95% CI; 1.01–2.05). A study carried out in the Gurage Zone in southern Ethiopia provided evidence in favor of this finding (18). This might be due number of family size increase related with increase demand of recommended diet and later it may lead deficit of recommended diet at household level. Additionally it explained as the equitable distribution of food among household members according to their physiological needs is essential, as one strategy for mitigating global malnutrition is making food more accessible at home. Our research revealed that a sizable average family size exists because a significant proportion of households had two or more school-age children. Given that the total fertility rate in the country is approximately 4.6 (37), ensuring equitable food distribution within households is crucial for addressing marginalized and nutritionally vulnerable populations.
According to this study, there was a 1.95-fold increase in the probability of being close to a health care facility (AOR = 1.95, 95% CI; 1.35–2.82) for every schoolchildren with diverse diets. This comparable with study conducted in Southwest Nigeria (38–40). Further, this study also supports finding from Nepal (29), which revealed that declining dietary diversity was significantly and negatively correlated with household spending and community infrastructure (hospital presence) [lowest versus highest household expenditure quintile, less developed (without hospital) versus more developed communities (29)]. This explained by that evident that people’s intention to feed varied food to their children arises when the awareness and directive of an attitude allows the person to practice those particular health behaviors. Thus, enhancing the educational level of caregivers, particularly people responsible for primary care of the child coupled with conducive environments such as physical and economical access to food, is important (41). Further, this might be explained that, if there are no access health settings and thus limited food options.
School children with no family home garden were 1.55 times higher odds of having inadequate diet diversity [AOR = 1.55, CI: (1.35–2.03)], which was significantly associated with a p-value <0.05 in the study area. This finding is consistent with an analogous study conducted in the South Gondar Zone, Northwest Ethiopia (23) and in Nepal, it revealed that access to home gardens was positively correlated with high dietary diversity and negatively correlated with low dietary diversity and that home gardens have high levels of species diversity as research findings suggest that rural households with home gardens have a greater probability of transitioning from a medium dietary diversity status (42). This could be because home gardeners have the ability to gather excess food from their farms to substitute for foods that are in short supply or non-existent at home. There ought to be a wide range of food available in home gardens. A varied family diet is the result of the diversity of plants in the garden (43). Furthermore, it explained as growing fruits, vegetables, and other crops at home allows you to have access to a wide range of food that might not be found in store. In both rural and urban locations, home gardens make it simple to obtain fresh vegetables and animal products (44). Strengthen of the current the study were use of large sample size and multistage sampling method for representativeness of the sample. Whereas the limitations of current study were socioeconomic variable that may be associated with dietary diversity, such as household income were not addressed and as its nature of a cross-sectional study inference of causality is not allowed. There may be recall bias related to dietary intake information, even though; great attention was given to the study procedures; including the process of training and close supervision throughout the study period.
Conclusion
When compared with other studies, dietary diversity in the current study area was low. A lack of proximity to a health care facility, a family size greater than five, and an absence of a family home garden were determinants of inadequate dietary diversity. A health extension platform should be used to raise awareness of the issue of inadequate dietary diversity in the area, and backyard vegetation should be improved. In addition to nutritional counseling for caregivers and the household as a whole, enhanced behavioral change programs should be implemented through community health agents, agricultural extension workers, and volunteers. The encouragement and maintain healthy program with Strong stakeholders’ collaboration is compulsory to improve healthy eating and to address family planning needs. Together with the rural roads authority, local government should support the local market and trade business that facilitates the development of market linkages. Such enterprises and initiatives would potentially communities to exchange their food commodities, which may help to increase their purchasing power and their dietary diversity status. Further, to address variable not covered in current study, a longitudinal study design is advised.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the institutional review board of the College of Health Science and Medicine, Wolaita Sodo University. The study was conducted following the relevant guidelines, regulation, and principles of the Helsinki Declaration. Furthermore, official permission letter was obtained from the Konso Zone Health Department and the respective woreda health offices. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin. Also Verbal and written informed consent was obtained from the respondents after they explained the purpose and objective of the study. The confidentiality of the participants in the study was considered. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
TY: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. EI: Writing – original draft, Writing – review & editing. BY: Conceptualization, Writing – original draft, Writing – review & editing. MM: Validation, Visualization, Writing – original draft, Writing – review & editing. EJ: Software, Writing – original draft, Writing – review & editing. TU: Visualization, Writing – original draft, Writing – review & editing. AA: Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. McLean, E, Cogwell, M, Egil, I, Wojdyla, D, and De Benoist, B. Worldwide prevalence of anaemia, WHO vitamin and mineral nutrition information system, 1993–2005. Public Health Nutr. (2008) 12:444–54. doi: 10.1017/S1368980008002401
2. Food and Agriculture Organization of United Nations (FAO). Schools–the beginning of the end of malnutrition Zero Hunger. Rome, Italy: FAO (2018).
3. Buhl, A. Global child nutrition foundation; University of Washington, School of Public Health Meeting nutritional needs through school feeding: a snapshot of four African nations. (2010). 40 p.
5. Leyna, GH, Mmbaga, EJ, Mnyika, KS, Hussain, A, and Klepp, K-I. Food insecurity is associated with food consumption patterns and anthropometric measures but not serum micronutrient levels in adults in rural Tanzania. Public Health Nutr. (2010) 13:1438–44. doi: 10.1017/S1368980010000327
6. Bundy, DA, Shaeffer, S, Jukes, M, Beegle, K, Gillespie, A, Drake, L, et al. School based health and nutrition programs. Dis Control Priorities Dev Ctries. (2016) 30:1091.
7. FAO. The state of food security and nutrition in the world Rome, Italy: FAO: Minister of education. (2019). 239 p.
8. Alamgir, K, Sami, UK, Salahuddin, K, Syed, Z, Naimatullah, KB, and Manzoor, K. Nutritional complications and its effects on human health. J Food Sci Nutr. (2018) 1:17–20.
9. Akubuilo, UC, Iloh, KK, Onu, JU, Iloh, ON, Ubesie, AC, and Ikefuna, AN. Nutritional status of primary school children: association with intelligence quotient and academic performance. Clin Nutr ESPEN. (2020) 40:208–13. doi: 10.1016/j.clnesp.2020.09.019
10. Peters, LW, Kok, G, Ten Dam, GT, Buijs, GJ, and Paulussen, TG. Effective elements of school health promotion across behavioral domains: a systematic review of reviews. BMC Public Health. (2019) 9:182. doi: 10.1186/1471-2458-9-182
11. Laxmi, BEK, Keshab, D, Rachana, S, Deepak Kumar, K, Anna Mia, E, and Luai Awad, A. Survival on antiretroviral treatment among adult HIV-infected patients in Nepal: a retrospective cohort study in far-western region, 2006–2011. BMC Infect Dis. (2013) 13:1471–2334.
12. Raleigh, C, Choi, HJ, and Kniveton, D. The devil is in the details: an investigation of the relationships between conflict, food price and climate across Africa. Glob Environ Chang. (2015) 32:187–99. doi: 10.1016/j.gloenvcha.2015.03.005
13. Sassi, M, and Thakare, H. Conflict and child malnutrition: a systematic review of the emerging quantitative literature. Curr Nutr Rep. (2022) 11:1–8. doi: 10.1007/s13668-021-00386-w
14. Maxwell, D. Famine early warning and information systems in conflict settings: challenges for humanitarian metrics and response. Confl Res Program. (2019) 2019:30.
15. Summary and Statistical Report of the 2007. Population and housing census, central statistics agency (CSA). Ethiopia: Addis Ababa (2008).
16. The Federal Democratic Republic of Ethiopia; National school health and nutrition strategy, Addis abeba, Ethiopia: Central Statistical Agency (2012)
17. Nithya, DJ, and Bhavani, RV. Do dietary diversity indices reflect the nutritional status of school aged children? Indian J Nutr Diet. (2016) 53:405. doi: 10.21048/ijnd.2016.53.4.8399
18. Abdu Oumer, BA. Determinants of dietary adequacy among school age children in Guraghe zone, southern Ethiopia. Int J Public Health Sci. (2019) 8:211–8. doi: 10.11591/ijphs.v8i2.18365
19. Legesse, ML, Abuhay, T, and Haile, Y. Factors associated with dietary diversity among children of agro pastoral households in Afar regional state, northeastern Ethiopia. Acad J Ped Neonatol. (2017) 5:555715.
20. CSA. Population size by sex, area and density by region, zone and Wereda Addis Ababa. Ethiopia: United States Agency for International Development (2013).
21. USAID. Ethiopia south Omo zone conflict assessment Washington, D.C., U.S: Journal of Food Security, United States (2021). 9 p.
22. Rakotonirainy, NH, Razafindratovo, V, Remonja, CR, Rasoloarijaona, R, Piola, P, Raharintsoa, C, et al. Dietary diversity of 6- to 59-month-old children in rural areas of Moramanga and Morondava districts. PLoS One. (2018) 13:e0200235. doi: 10.1371/journal.pone.0200235
23. Girma Nega, ME, Teferi, Degnet, and Nana, Amanuel, W Rigbe, Michael,. Dietary diversity and associated factors among rural households in South Gondar zone, Northwest Ethiopia feed the future – Research award. Journal of Food Security, United States (2015).
24. FANTA. Developing and validating simple indicators of dietary quality and energy intake of infants and young children in developing countries: summary of findings from analysis of 10 data sets. Working group on infant and young children feeding indicators; food and nutrition technical assistance (FANTA) project, academy for educational Development. J Med Physiol Biophys. (2006) 21:29–34.
25. Tewabe, T, Belachew, A, Miskir, Y, and Mekuria, G. Dietary diversity among school age children in Merawi town, Amhara region, Ethiopia, 2018: a community based cross sectional study. Arch Public Health. (2020) 78:2. doi: 10.1186/s13690-019-0384-7
26. WHO, UNICEF, IFPRI, UC Davis, USAID, FANTA, Macro International. Indicators for assessing infant and young child feeding practices In: Conclusions of a consensus meeting held 6–8 2007. Washington, DC, USA: WHO (2008).
27. Gedle, D, Mekuria, G, Kumera, G, Eshete, T, Feyera, F, and Ewunetu, T. Food insecurity and its associated factors among people living with HIV/AIDS receiving anti-retroviral therapy at Butajira hospital. Southern Ethiopia: Nutrition & Food Sciences (2015). 05 p.
28. Herrador, Z, Perez-Formigo, J, Sordo, L, Gadisa, E, Moreno, J, Benito, A, et al. Low dietary diversity and intake of animal source foods among school aged children in Libo Kemkem and Fogera districts, Ethiopia. PLoS One. (2015) 10:e0133435. doi: 10.1371/journal.pone.0133435
29. Abizari, AR, Azupogo, F, Nagasu, M, Creemers, N, and Brouwer, ID. Seasonality affects dietary diversity of schoolage children in northern Ghana. PLoS One. (2017) 12:e0183206. doi: 10.1371/journal.pone.0183206
30. AC2 S-PCaP. An assessment of dietary diversity and nutritional status of preschool children. Austin J Nutri Food Sci. (2014) 2:2381–8980.
31. Nithya, DJ, and Bhavani, RV. Factors which may limit the value of dietary diversity and its association with nutritional outcomes in preschool children in high burden districts of India. Asia Pac J Clin Nutr. (2018) 27:413–20.
32. Aemro, M, Mesele, M, Birhanu, Z, and Atenafu, A. Dietary diversity and meal frequency practices among infant and young children aged 6–23 months in Ethiopia: a secondary analysis of Ethiopian demographic and health survey 2011. J Nutr Met. (2013) 2013:782931:1–8. doi: 10.1155/2013/782931
33. Temesgen, H, Yeneabat, T, and Teshome, M. Dietary diversity and associated factors among children aged 6–23 months in SinanWoreda, Northwest Ethiopia: a cross-sectional study. BMC Nutr. (2018) 4:5. doi: 10.1186/s40795-018-0214-2
34. Nega, G, Endris, M, Teferi, D, Nana, AW, and Michael, R. Northwest Ethiopia: dietary diversity and associated factors among rural households in South Gondar zone. Journal of Food Security, United States (2015).
35. Misker, D, Misker, B, and Ayele, G. House hold dietary diversity and associated factors in Mirab Abaya wereda southern Ethiopia 2016; community based cross sectional study. Diver Equal Health Care. (2016) 13:293–6. doi: 10.21767/2049-5471.100065
36. Sagaro, GG, and Alemayehu, M. Dietary diversity and associated factors among infants and young children in Wolaita zone, southern Ethiopia. Sci J Clin Med. (2017) 6:53–9. doi: 10.11648/j.sjcm.20170604.12
37. EDHS. Ethiopia demographic and health survey in nutritional status of children I. Ethiopia: Central Statistical Agency Addis Ababa (2016).
38. Otekunrin, OA, Otekunrin, OA, Ayinde, IA, Sanusi, RA, Onabanjo, OO, and Ariyo, O. Dietary diversity, environment and health-related factors of under-five children: evidence from cassava commercialization households in rural South-West Nigeria. Environ Sci Pollut Res Int. (2021) 29:19432–46. doi: 10.1007/s11356-021-17221-y
39. Martin-Prevel, YBE, Taosoba, S, Castan, F, and Coulibaly, D. The 2008 food price crisis negatively affected household food security and dietary diversity in urban Burkina Faso. J Nutr Educ Behav. (2012) 142:1748–55.
40. Morseth, MS, Grewal, NK, Kaasa, IS, Hatloy, A, Barikmo, I, and Henjum, S. Dietary diversity is related to socioeconomic status among adult Saharawi refugees living in Algeria. BMC Public Health. (2017) 17:621. doi: 10.1186/s12889-017-4527-x
41. ACF, I. Food security and livelihood assessment; a practical guide, F.S.A. livelihood ACF international (2010). 92 p.
42. Taruvinga, A, Muchenje, V, and Mushunje, A. Determinants of rural household dietary diversity: the case of Amatole and Nyandeni districts, South Africa. Int J Dev Sustain. (2013) 2:2233–47.
43. Ajah, AI, Agera, SIN, and Ejembi, SE. Prospects of the contribution of home gardens to food security in our households. J Res Forest Wildlife Environ. (2013) 5:23–7.
Keywords: dietary diversity, nutrition, conflict affecting, school-age children, southern Ethiopia
Citation: Yakob T, Israel E, Yakob B, Meshesha M, Jambo E, Utalo T and Abraham A (2025) Dietary diversity and its associated factors among school children in conflict affected communities of southern Ethiopia. Front. Nutr. 11:1462178. doi: 10.3389/fnut.2024.1462178
Edited by:
Fentaw Wassie Feleke, Woldia University, EthiopiaReviewed by:
Ayenew Negesse, Debre Markos University, EthiopiaGetachew Sale Mezgebu, Hawassa University, Ethiopia
Copyright © 2025 Yakob, Israel, Yakob, Meshesha, Jambo, Utalo and Abraham. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tagese Yakob, eWl0YWd1akBnbWFpbC5jb20=