 Anna-Maria Sapała1
Anna-Maria Sapała1 Wiktoria Staśkiewicz-Bartecka
Wiktoria Staśkiewicz-Bartecka Marek Kardas
Marek Kardas- 1Department of Dietetics and Food Science, Faculty of Science, Natural and Technical Sciences, Jan Długosz University in Częstochowa, Czestochowa, Poland
- 2Department of Food Technology and Quality Evaluation, Department of Dietetics, Faculty of Health Sciences in Bytom, Medical University of Silesia in Katowice, Zabrze, Poland
- 3Department of Health Sciences and Physical Culture, University of Applied Sciences in Nysa, Nysa, Poland
Background: Cardiovascular disease is a leading cause of death worldwide. The increase in patients with obesity and diabetes raises the risk of cardiovascular diseases. Proper eating habits and adequate nutritional knowledge play a key role in preventing and treating these conditions. This study aimed to evaluate the dietary habits, nutritional knowledge, and nutritional status of patients hospitalized in a cardiology department in Poland, including those with obesity or diabetes.
Methods: The study was conducted at St. Barbara Regional Specialized Hospital No. 5 in Sosnowiec from January to June 2021, involving 301 patients, 154 women (51.2%) and 147 men (48.8%), aged 29 to 87. Participants were assessed for BMI, NRS 2002 scale, morphology, biochemistry results, blood pressure, and examined for nutritional knowledge and habits using proprietary questionnaires. A proprietary scale was used to assess eating habits.
Results: Most cardiology patients were overweight or obese, with 80% exceeding the normal weight range. No significant gender differences were noted in malnutrition risk on the NRS 2002 scale. The study found patients rarely consumed recommended amounts of vegetables, fruits, legumes, whole grains, fish, and dairy products. Only 26.2% regularly ate a second breakfast, and just 9.3% chose water with meals. However, consumption of salty snacks, energy drinks, and alcohol was low. Biochemical and blood test analysis did not show significant differences between patients with diabetes, obesity, and others.
Conclusion: Most cardiology patients were overweight or obese, which poses a significant risk for further health complications, including cardiovascular diseases. Although patients with diabetes and/or obesity had better nutritional knowledge in some areas, this did not lead to healthier eating habits. The absence of significant differences in biochemical tests suggests that overall lifestyle and diet are crucial to cardiovascular health.
1 Introduction
The development of civilization and scientific and technological advances are resulting in an increase in the health consciousness of society and an improvement in the living conditions of many populations. At the same time, this development is accompanied by the development of many diseases, of which metabolic diseases are an increasing problem (1, 2). Obesity is a chronic metabolic disease characterized by increased body weight due to a significant increase in body fat. Its basis may be genetic, endocrine, and environmental factors, however, it is most often the result of an excessive energy supply with food (2, 3). Obesity is considered an epidemic, causing dysfunction and pathological conditions of organs and entire systems in the human body over time. These dysfunctions, if not taken care of by specialists, can lead to permanent disability and even indirectly to death (4). This is common, especially in highly developed countries in which the percentage of obese people is higher due to easier access to high-calorie products with high amounts of simple sugars and fat. However, it should be noted that obesity has become a pathogenic factor in the development of type 2 diabetes, hypertension, or depression also in low- and middle-income countries (4, 5). Abdominal obesity, often referred to as central obesity, is characterized by fat accumulation in the abdominal and trunk area. It is particularly dangerous because of its various associated health risks (5). Abdominal obesity is assessed indirectly by anthropometric measurements and indices and directly by MRI, body composition analysis, or CT scans. Methods for assessing abdominal obesity, along with criteria for diagnosis, are as follows: WHR (Waist Hip Ratio—an indicator of body fat distribution) ≥ 0.85 in women, ≥ 1.0 in men; WHtR (Waist to Height Ratio—waist-to-height ratio) ≥ 0.50; abdominal sagittal dimension ≥25,2 cm in women, ≥ 22,8 cm in men; waist circumference ≥ 80 cm in women, ≥ 94 cm in men and direct methods—tissue cross-sectional area at the level of the L4-L5 intervertebral space (6, 7).
In Europe, obesity rates are 10–27% in men and 10–38% in women, while in Poland, overweight or obesity affects more than 60 and 50% of the population, respectively. In contrast, abdominal obesity, which can occur in normal-weight individuals, affects 71% of women and 56% of men in Europe, while in Poland it affects 56% of men and 39% of women (8).
Carbohydrate metabolism disorders are one of the most important, and more difficult to treat, problems. The most common such disorder is type 2 diabetes, which has been declared an epidemic by the United Nations (UN) and the World Health Organization (WHO). It is noteworthy that it is the first and only disease whose cause is non-communicable and is attributed to an epidemic nature (9, 10). The disease, according to IDF statistics, affects 300 million people worldwide, however, as many as one-third do not receive treatment because they are unaware of the disease. Poland, like many other countries, is also struggling with this diabetes problem. A study showed that in the early 2000s, 5.6% of Poland’s population between the ages of 18 and 94 had diabetes, but the figure is still rising. Currently, 7% of men and 6% of women suffer from diabetes. Studies have recorded 2.17 million people with diabetes (1.22 million women and 0.96 million men). It is expected that by 2030 as much as 10% of the Polish population will have diabetes (10–12). Factors in the development of type 2 diabetes, are primarily improper eating habits, which include an inappropriate diet, poor in whole grains, vegetables, and fruits, while rich in saturated fatty acids, trans fats, and simple sugars. These factors are further reinforced by a lack of physical activity and chronic stress (10, 13–17).
The pre-diabetic state, in combination with the other elements of the metabolic syndrome, poses a serious threat to the patient’s health and even life. It is estimated that about 80–90% of patients struggling with diabetes are those who are simultaneously being treated for obesity, hypertension, as well as accompanying lipid disorders (12, 18).
Knowledge, attitudes, and practices related to nutrition play a key role in the prevention and treatment of obesity and metabolic diseases, such as type 2 diabetes and hypertension. Obesity, a global health issue, is often a result of poor dietary habits and lack of physical activity (14, 16). Research shows that nutritional education can significantly influence patient attitudes and behaviors, but knowledge alone does not always lead to improved health outcomes (15). Attitudes and motivation for change are equally important, though they may be hindered by external factors, such as access to healthy foods or social support. Regular adoption of healthy dietary habits can reduce the risk of complications related to obesity and diabetes, but maintaining these habits requires an integrated approach that includes education, behavioral support, and social reinforcement (15, 17).
The main objective of this study was to evaluate the dietary habits, nutritional knowledge, and nutritional status of patients hospitalized in the cardiology ward, taking into account the group of patients diagnosed with obesity or diabetes. It was hypothesized that hospitalized cardiac patients with obesity or diabetes show differences in eating habits and nutritional knowledge, which affect their nutritional status, compared to patients without these conditions.
2 Materials and methods
2.1 Study design
The study was conducted between January and June 2021. The site of the study was the Cardiology Department at the St. Barbara Regional Specialized Hospital No. 5 in Sosnowiec in Poland. Patients presented to the hospital with cardiovascular complaints (I00-I99, according to the International Classification of Diseases and Health Problems ICD-10). The study was conducted after obtaining permission from the department and approval from the Bioethics Committee of the Silesian Medical University in Katowice No. PCN/0022/KB/299/19/20 (approval date: 21.01.2020), patients invited to participate in the study were informed about the purpose of the study and expectations in accordance with the Declaration of Helsinki. Patients were included in the study after obtaining their verbal and written consent.
2.2 Study participants
The study group consisted of patients of the Cardiology Department at the St. Barbara Regional Specialized Hospital No. 5 in Sosnowiec. The group consisted of 301 patients, including 154 women (51.2%) and 147 men (48.8%), aged 29 to 87 years. Inclusion criteria for the study included (1) age over 18, (2) residence in the Silesian province, (3) diagnosis of cardiovascular disease, (4) stay in the Cardiology Department at the St. Barbara Regional Specialized Hospital No. 5 in Sosnowiec for at least 3 days, and (5) consent to the study. Exclusion criteria for the study included (1) the presence of mental disorders and other health conditions that prevented informed full and correct completion of the survey, and (2) incomplete completion of the survey.
2.3 Research tools
2.3.1 Assessment of nutritional status
Nutritional status was assessed using the body mass index (BMI). The categorization was done according to the general findings of the WHO (World Health Organization): BMI <18.49 kg/m2—underweight, 18.5–24.99 kg/m2—normal weight, 25–29.99 kg/m2—overweight, 30–34.99 kg/m2 -obesity of the first degree, 35–39.99 kg/m2—obesity of II degree, >40 kg/m2—obesity of III degree (19).
2.3.2 NRS 2002 scale
Patients’ nutritional status was also assessed by analyzing nutritional status and disease severity using the Nutritional Risk Score (NRS 2002) scale. According to Kondrup et al. (2, 3), the NRS-2002 nutritional risk score is based on an assessment of the following three items: nutritional status, disease severity, and age. Patients receive 0 to 3 points for nutritional status and 0 to 3 points for disease severity. A score of 1 is added to patients aged 70 and older. The total score ranges from 0 to 7, and if the total score is 3 or more, the patient is classified as at risk of malnutrition according to the NRS-2002. Nutritional status in the NRS-2002 is assessed by three individual components: BMI, recent weight loss (5% in the past 1, 2, or 3 months), and food intake in the previous week. Information on food intake during the week before hospital admission was determined by the dietitian through an interview with the patient. Questions focusing on food intake before hospitalization were compared with normal intake. In addition, food intake was divided into 0–25%, 25–50%, and 50–75% of normal requirements (20, 21).
2.3.3 Assessment of dietary habits and nutritional knowledge
Individual face-to-face interviews were conducted by the researcher (nutritionist) to collect all relevant data from the study participants, including socio-demographic data (age, education level, place of residence) and lifestyle information. The study used a diagnostic survey method, within which a survey technique was applied. The author’s survey questionnaire consisted of a metric and two sections assessing dietary habits and knowledge.
The scope of the metric included questions on metric data such as gender, and age (determined by the year of birth and the year of the survey; environmental data: education; clinical data: diagnosed medical conditions, introduced diet). The author’s questionnaire examining the level of patients’ nutritional knowledge consisted of 19 closed-ended single-choice questions and two questions on self-assessment of their knowledge. The questionnaire examining patients’ eating habits included 9 closed-ended single-choice questions and a table of selected food products based on the FFQ-6 questionnaire (21). It assesses habitual consumption of food items over the past 12 months, divided into 6 levels of frequency. For each selected food item, respondents were able to indicate the frequency of their consumption by selecting one of the following options: (1) never, (2) once a month or less often, (3) several times a month, (4) several times a week, (5) daily or (6) several times a day.
A proprietary rating scale was used to assess the level of knowledge. Based on the questionnaire examining the level of nutritional knowledge and the answers given to questions 1–19, points were assigned: 0- incorrect answer, 1- correct answer. The total score for each patient and the percentage (%) against the maximum number of correct answers were then given. The level of knowledge was determined according to the following classification: Unsatisfactory 0–59%; Satisfactory 60–73%; Good 74–86%; Very good 87–100%.
A proprietary rating scale was used to assess the correctness of eating habits. Questions 1, 3, 6, 7, and 8 from Part I of the survey examining eating habits and all questions from Part II were evaluated. Based on the answers given in Part I, points were assigned: 0- incorrect answer, 1- correct answer. The answers to Part II, concerning the correctness of the frequency of consumption (never or seldom, once a month or less often, several times a month, several times a week, daily, several times a day) according to each food product, were assigned points: 0- answer may indicate incorrect eating habits, 1- correct answer. The total score for each patient and the percentage (W%) against the maximum number of correct answers were then given. The correctness of eating habits was determined according to the same classification as the level of nutritional knowledge.
2.3.4 Morphology, biochemical blood tests
Blood samples from all participants were taken after a 12-h overnight fast. These tests included leukocyte (WBC), erythrocyte (RBC), platelet (PLT), hemoglobin (Hgb), and hematocrit (Hct) levels. Biochemical results included fasting blood glucose (FG), total cholesterol (TC), triglycerides (TG) LDL cholesterol (LDL-C), and HDL cholesterol (HDL-C), as well as sodium (Na) and potassium (K). Uric acid (UA), creatinine (Cr), troponin (Troponin T) alanine aminotransferase (ALT), aspartate aminotransferase (AST), and creatine kinase (CK-MB) levels were also performed.
2.3.5 Blood pressure
Participants were in a sitting position for at least five minutes before blood pressure (BP) was assessed. A total of two trained nurses took two BP measurements for each participant (the same nurse took both measurements for a given participant) with a five-minute interval between measurements, according to Frese et al. (22). The mean value of each participant’s blood pressure calculated from the two measurements was used for the study.
2.4 Statistical analysis
Data were collected in MS Excel spreadsheet, MS Office 2013. Statistical analysis was performed using Statistica 2013, Stat Soft Poland. Measurable data were presented using measurable characteristics: mean (X) ± standard deviation (SD) median (M) and interquartile range (Rk). In the case of a symmetrical distribution, the mean was considered, while when the distribution was asymmetrical, the median value was interpreted. The Shapiro–Wilk test was used to assess the shape of the distribution. The analysis of differences in groups was conducted according to the number of groups and the shape of the distribution. In the case of two groups, the Student’s T-test or its non-parametric equivalent the Mann–Whitney U-test was used. For three or more groups, analysis of variance ANOVA or Kruskal-Wallis test was used, followed by multiple group analyses using post-hoc tests. Unmeasured data were presented as percentages. For analyses, significance tests of percentages within groups and χ2 tests of independence were used, taking into account corrections to the test (Yul’s test, Fischer’s test) depending on the expected numbers. In addition, correlation coefficients (Gamma, V Cramer) were provided to assess the strength of the relationship. In turn, to analyze the concordance of correct answers to questionnaire questions, Cochran’s Q test was performed. Wanting to assess the risk of metabolic syndrome, a logistic regression analysis was performed using the NRS 2002 level, age groups, and the results of morphological and biochemical blood tests. The level of statistical significance was set at p < 0.05.
3 Results
3.1 Characteristics of the study group
The study included 301 patients: 154 women (51.2%) and 147 men (48.8%), aged 29 to 87 years. They represented 5 age groups: under 50 (9.3%), 50–59 (12.6%), 60–69 (29.9%), 70–79 (36.9%) and over 80 (11.3%). Detailed information is presented in Table 1.
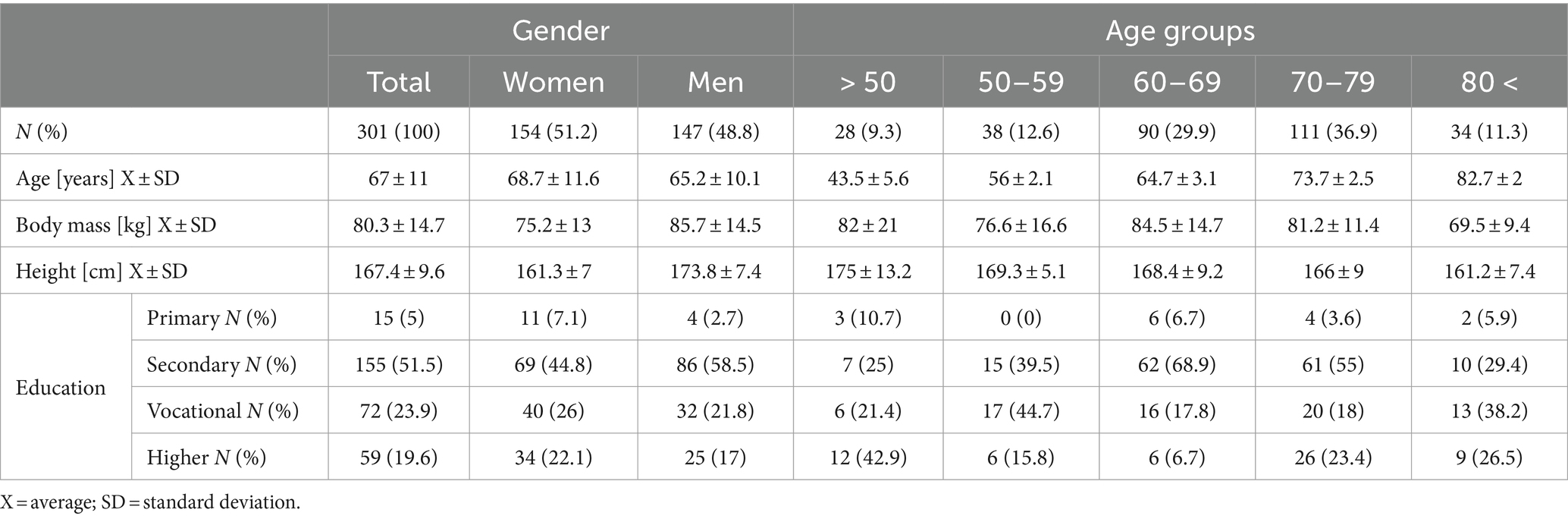
Table 1. Characteristics of the study group by gender and age.
More than half of the cardiac patients studied were found to have obesity or diabetes (52.8%). There were no differences in the incidence of diabetes and obesity according to gender. However, there were differences in incidence according to age, those in the 70–79 age group were more likely to have diabetes and obesity (p < 0.01; p < 0.001). Details are shown in Table 2.
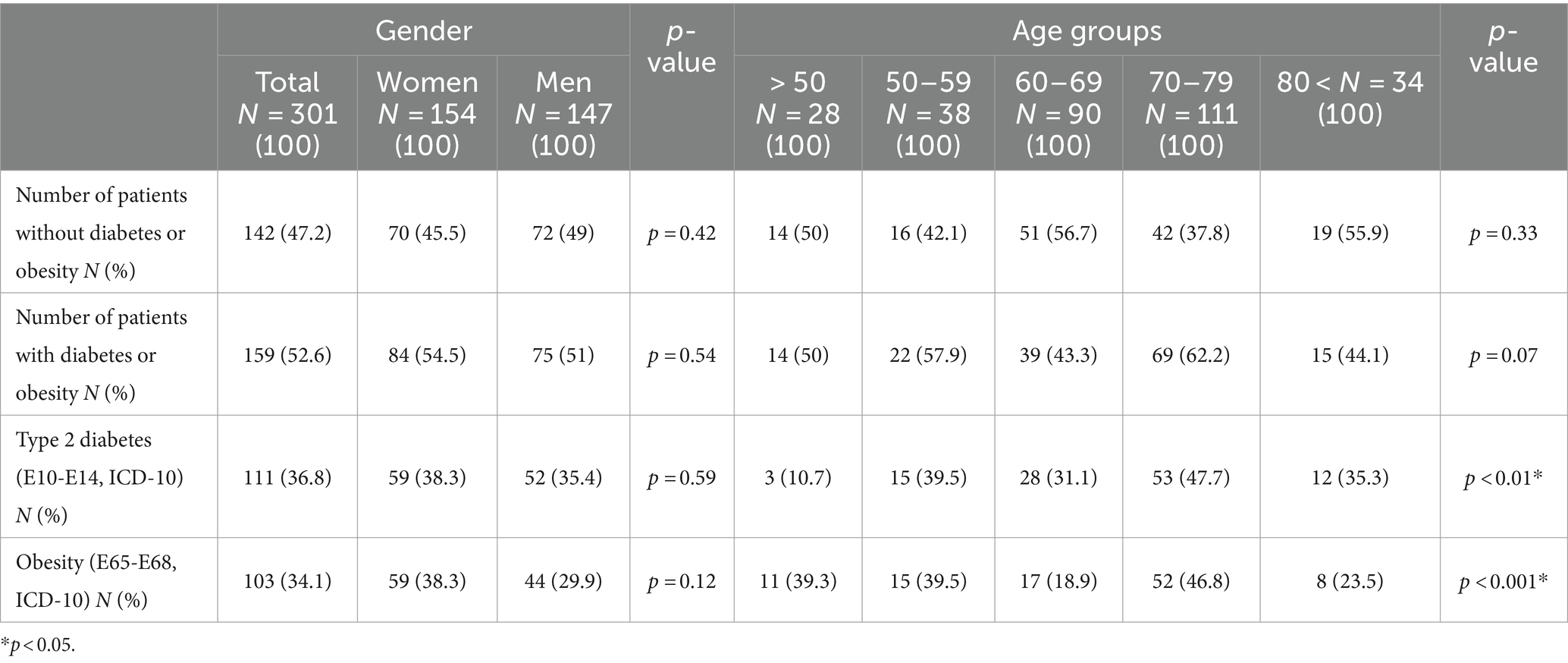
Table 2. Characteristics of the study group concerning the incidence of diabetes and obesity.
3.2 BMI and NRS-2000
More than three-fourths of the study subjects (80%) showed above-normal body weight as interpreted by the BMI index. Obesity of the 1st and 2nd degree particularly affected women 27.9 and 14.9%, respectively. By age, grade I obesity was most common among those in the 70–79 age range (26.1%), while grade II obesity was most common among those aged 60–69 (24.4%). Details of the anthropometric data are shown in Table 3. There was no significant group variation by gender, age, or diagnosis of obesity or diabetes in the frequency of diagnosed nutritional level risk as measured by the NRS index (Table 4).
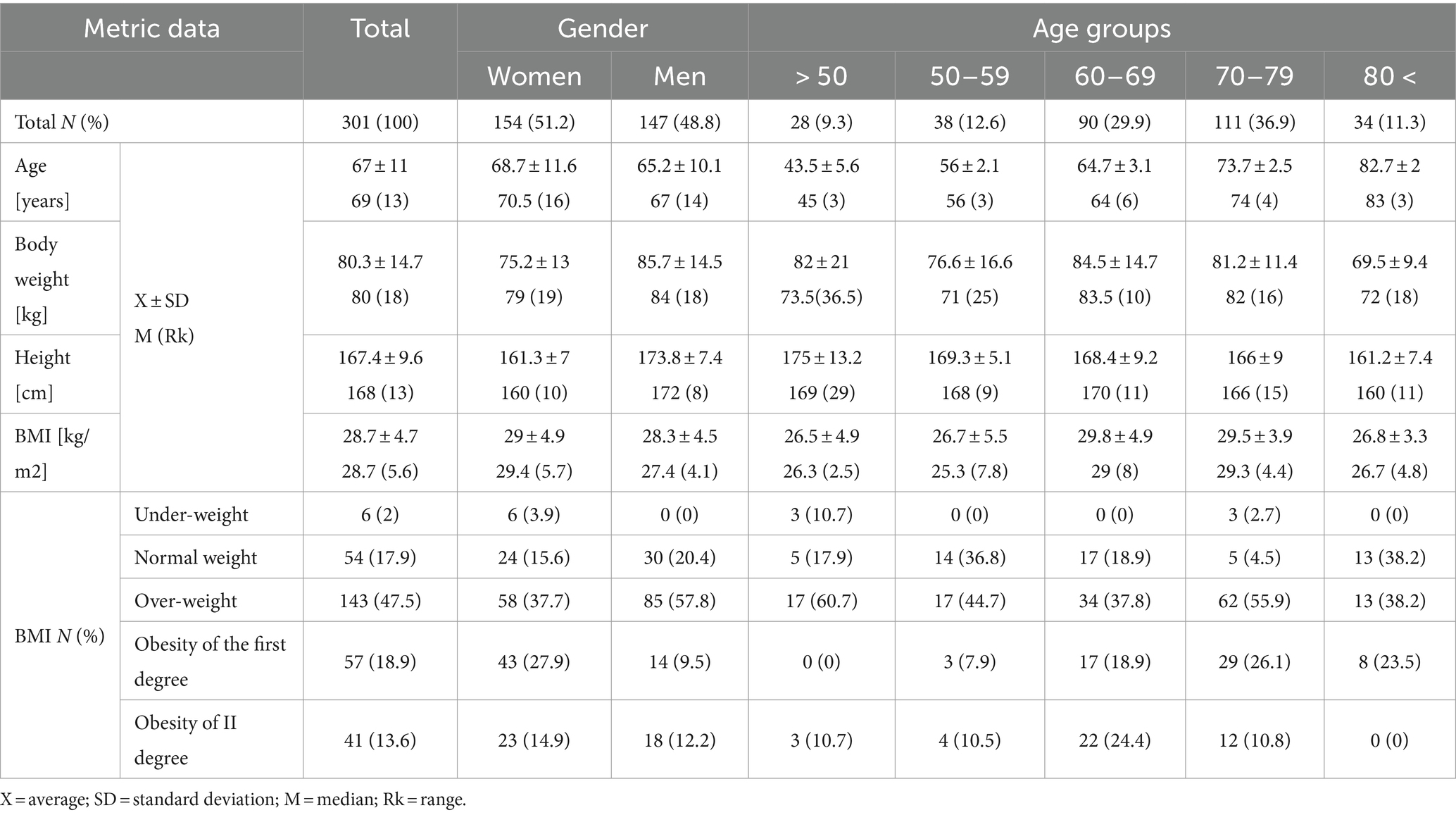
Table 3. Anthropometric data of patients in the study group.
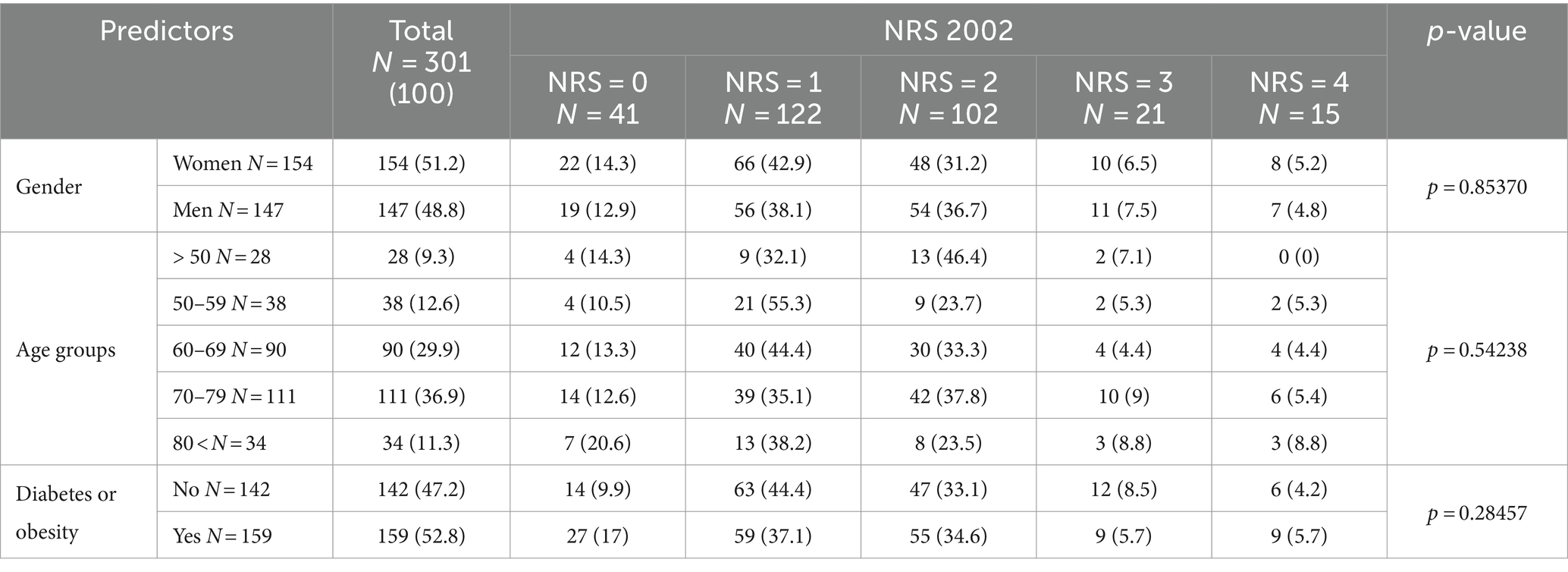
Table 4. Analysis of nutritional status risk using the NRS-2002 index.
3.3 Nutrition knowledge
The results of the patient’s nutritional knowledge survey were mixed. Patients with diabetes and/or obesity had better knowledge of the source of dietary protein (84.3% vs. 66.9%), the function and source of dietary fiber (52.8% vs. 37.3% and 52.2% vs. 48.6%, respectively), the function of iron (63.5% vs. 42.3%), and the source of vitamin C (71.7% vs. 58.5%). Patients who were not diagnosed with these entities did better on questions about dietary sources of calcium (81.8% vs. 57.1%). Among all respondents, respondents gave the most correct answers in questions about the source of protein (76.1%), the source of calcium (69.8%), and the source of vitamin C (65.4%). The exact results are shown in Table 5.
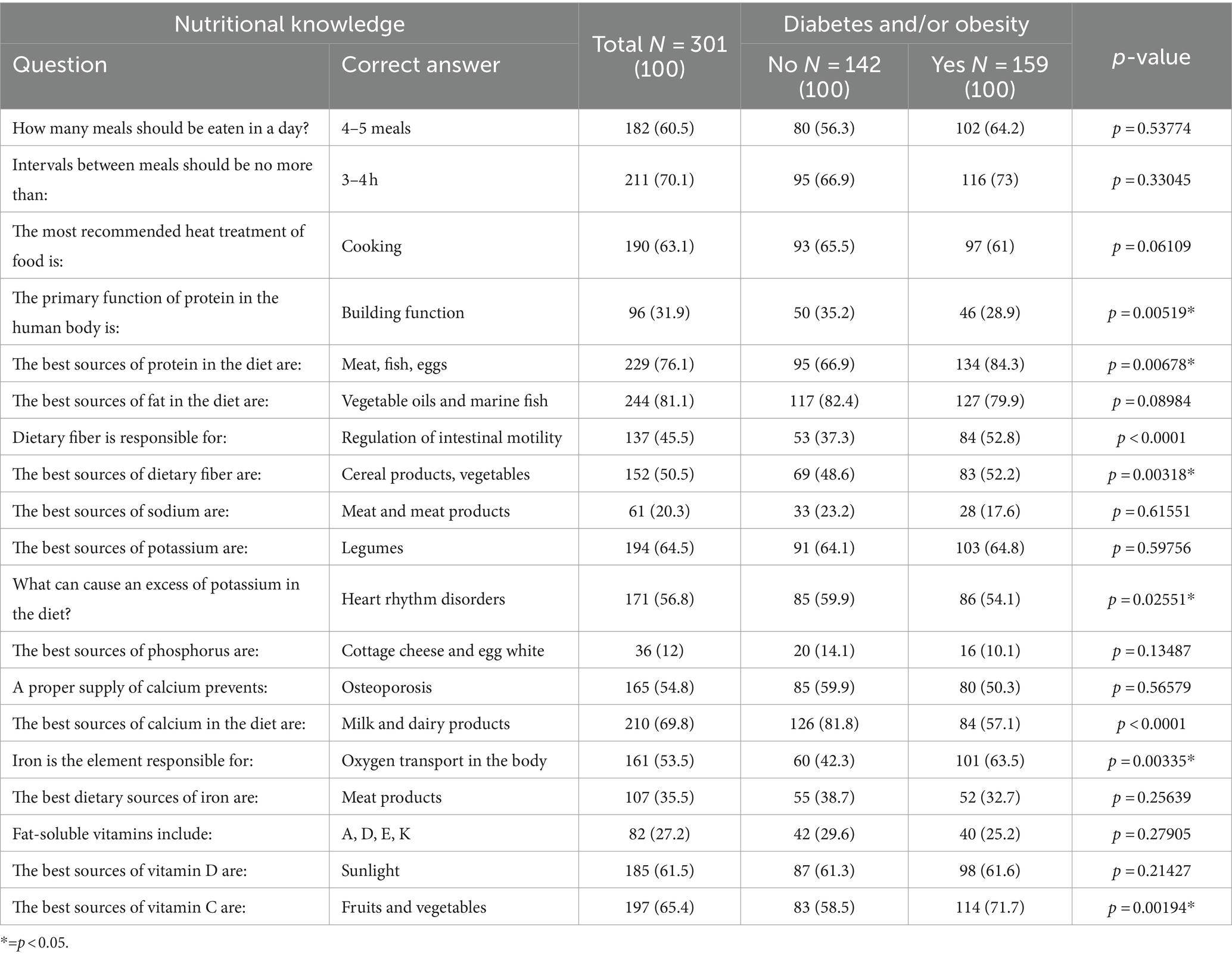
Table 5. Respondents’ nutritional knowledge.
When asked about sources of nutritional knowledge, men were more likely to indicate that a dietician was the source of their knowledge relative to women’s indications (p = 0.005), while women were more likely to indicate literature and magazines (p = 0.001). Analyzing the sources of knowledge in the age groups studied showed that those aged 60–69 were significantly more likely to indicate that a nutritionist was their source of knowledge (p = 0.0001). In contrast, those aged 70–79 were significantly more likely to indicate a doctor. The Internet was the primary source of information for those under 50, with 67.9% indicating this response (p = 0.01). Detailed information is shown in Figure 1.

Figure 1. Respondents’ sources of nutritional knowledge by age (n=301).
3.4 Eating habits
Respondents were mostly characterized by incorrect eating habits. Only 26.2% of respondents always eat a second breakfast, and 44.3% of them choose fruit for this meal. A disturbing result is that only 9.3% of the subjects, including 15.7% with obesity and/or diabetes and only 2.1% without these diseases, chose water as a beverage for their meal. It is noteworthy, however, that almost ¾ of patients, regardless of the diagnosed disease entity, are wary of overeating at night (Table 6). The study of dietary habits in terms of frequency of intake of selected nutrients was divided into food groups such as cereal products, dairy products and eggs, meat products and fish, vegetables and grains, fruits, fats, beverages, and sweets. Detailed results including the above groups are shown in Table 7.
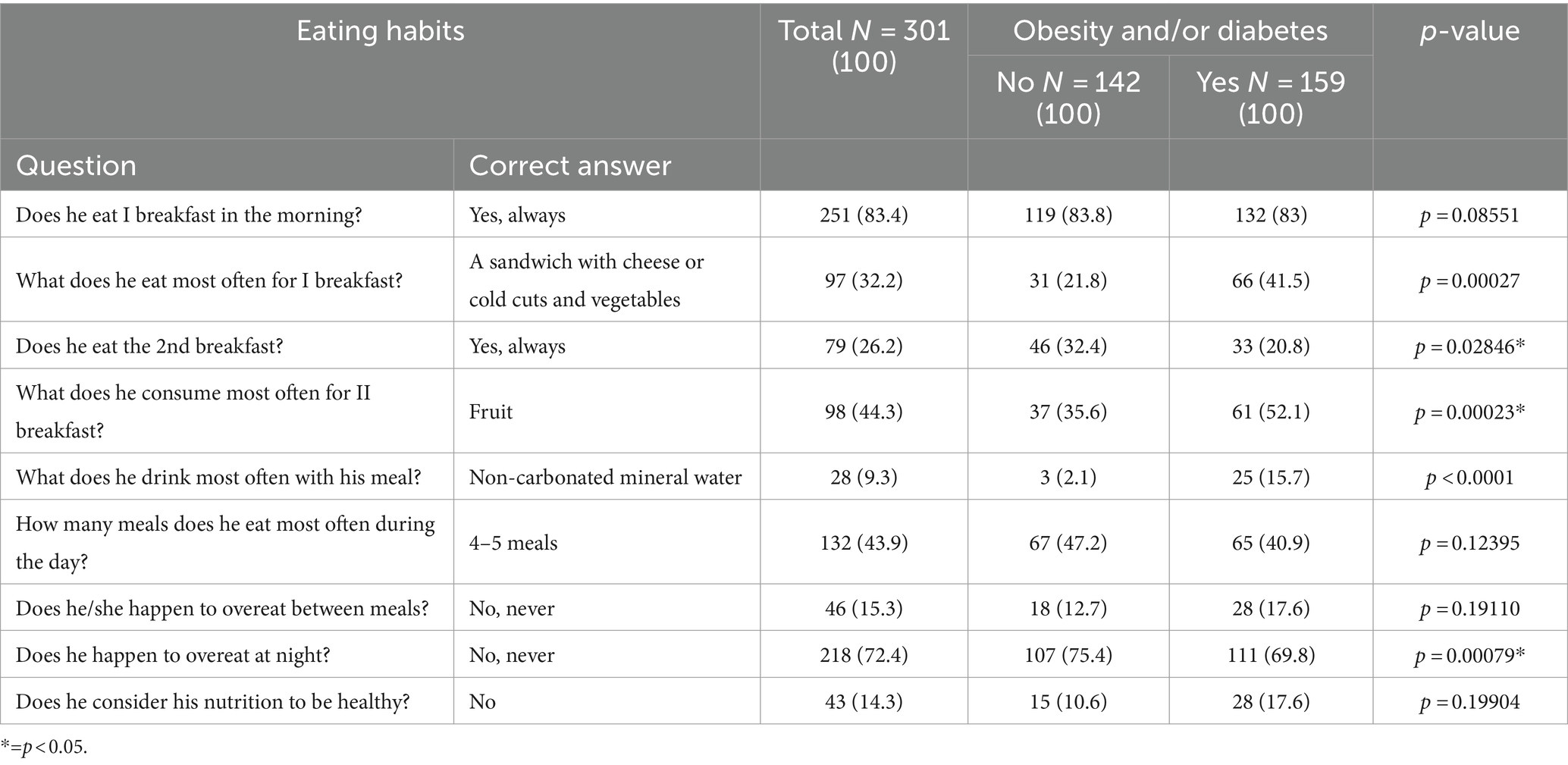
Table 6. Eating habits of respondents.
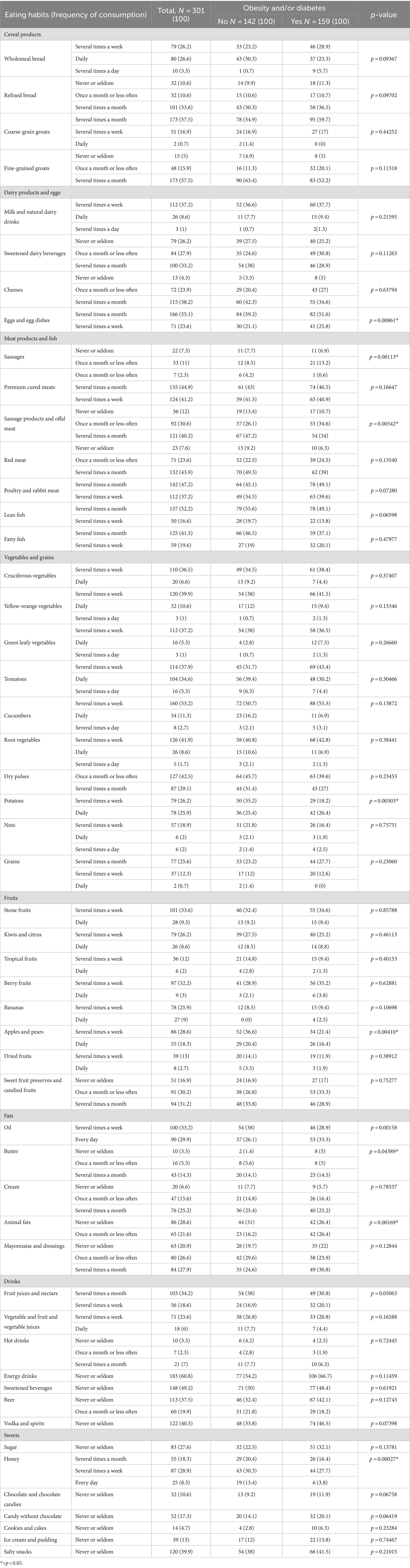
Table 7. Frequency of consumption of selected products by respondents.
3.5 Biochemistry and blood pressure
There was not much variation in the levels of blood biochemical parameters among the groups classified by BMI. The presence of obesity and/or diabetes generally did not affect the variation in levels of blood biochemical parameters. The results were not statistically significant. Detailed information is presented in Table 8.
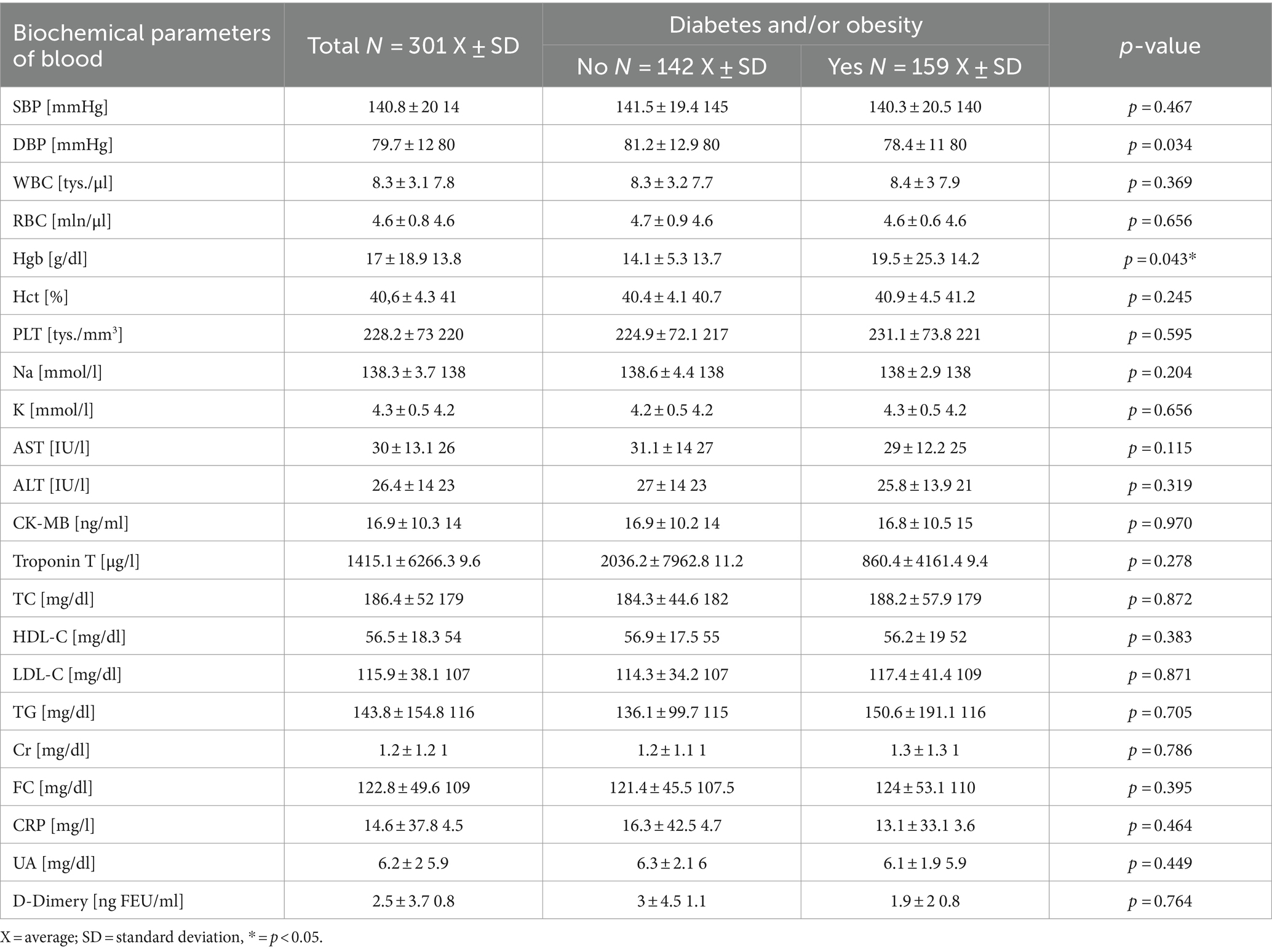
Table 8. Analysis of blood pressure and blood biochemistry results.
4 Discussion
The purpose of this study was to evaluate and analyze in detail the knowledge, behavior, and eating habits of patients hospitalized in the cardiology department with diagnosed diabetes or obesity, taking into account the results of morphological and biochemical tests and their nutritional status. The study included 301 patients hospitalized in the Cardiology Department of a hospital in the Silesian province. A survey technique based on proprietary questionnaires and available methods of assessing nutritional status was used. The study was conducted from January to June 2021 with the approval of the hospital director.
The hypothesis was that people with diabetes or obesity would show differences in diet and nutrition knowledge, which would affect their nutritional status compared to those without these conditions. The results of the study showed that more than 65% of overweight or obese respondents scored either sufficient or good on the nutrition knowledge questionnaire. In comparison, only 24.1% of those with a normal BMI scored other than inadequate. These results suggest that overweight individuals have greater nutritional awareness, although this does not always translate into healthy eating habits.
Respondents declared eating mainly 4–5 meals a day, and most of them, regardless of the type of health ailment, had breakfast every day, choosing most often a cheese or ham sandwich and tea. The highest daily consumption of wholemeal baked goods was declared by overweight and obese respondents. Similar results were obtained by Stefanska et al. (23)-in their study, about 32% of obese people declared daily consumption of wholemeal products. The study by Pielak et al. (24) showed that both rye bread and wheat bread are consumed with the same frequency, while diet, health-promoting, and crisp bread are far less popular among the surveyed consumers. Comparing the data concerning obesity and diabetes, it can be concluded that the results in all groups are similar.
Analysis of the weekly consumption of dairy products did not show particularly high consumption of these products in the diet of the subjects—the results oscillated around 37%. The relationship between the consumption of dairy products and eggs and the occurrence of obesity or diabetes could not be established. A comparison of data on the consumption of different types of meat showed that the respondents consumed lean fish, poultry, and red meats to a similar extent while avoiding organ meats and sausage products. This was also confirmed by a study conducted in Wroclaw in 2010 (25). The results showed that for 54% of women and 36% of men with hypertension, the presence of fat in the food items in question was of great importance when purchasing meat and meat products.
Regardless of the diagnosis of diabetes or obesity, patients were most likely to choose cucumber, root, and leafy vegetables. In comparison, the results of a study conducted during training at the Biaton Health Academy by Wlodarek and Glabska showed that patients with diabetes t. 2 were most likely to eat tomatoes, carrots, and cabbage (26). Regardless of BMI and prevalent diseases, the least frequently chosen products daily are nuts, pulses, and grains. The same results were presented in a study by Drywiew and Kuć (27), which proved the low consumption of legumes by elderly people living in rural areas.
Analyzing the results, it can be concluded that apples are the most consumed fruits daily. This is understandable, as they are available all year round, relatively cheap, and firmly rooted in Polish culinary tradition. Dried and candied fruits were chosen on average once a month or less often. Daily consumption of butter was declared by all respondents, regardless of the diagnosed disease entity. Consumption of mayonnaise and dressings was limited to a few times a month, which is a positive surprise considering the high energy value of these products. Similar results were obtained by Pilska (28), whose study of a representative group of Poles showed that butter was the most commonly consumed type of fat, followed by canola oil, margarine, olive oil, and sunflower oil.
All respondents unanimously avoided the consumption of sweetened and energy drinks—more than 60% never or seldom included them in their diet. This fact is a positive but unsurprising development. The respondents are mainly people aged 50 to 80 and older, who did not use these types of drinks during the acquisition of their eating habits (childhood and adolescence), so it was likely that the percentage of consumption of these products would be low. During the daily period, hot beverages are the most popular, with the majority of respondents declaring that they consume them daily or drink them even several times a day. Different results are presented in the study by Witanowska et al. (29), according to which the respondents are most likely to drink mineral water (83%), followed by fruit juices and sweet drinks. However, it is important to note the negligible consumption of energy drinks, both in this analysis and in our study.
Respondents also avoided the consumption of alcoholic beverages, with the highest consumption of wine, drinks, vodka, and spirits declared as “never” or “seldom” and “once a month” or less often. Analyzing the consumption of sweets, all respondents most often reached for chocolates, chocolate products, cookies, cakes, ice cream, puddings, and non-chocolate candies several times a month, with the percentage of consumption of each category of items being similar in all groups.
Summarizing the respondents’ knowledge and eating habits, it can be concluded that they vary depending on the topic addressed, but are generally incorrect about the diagnosed disease entity. Similar results were obtained in a study by Bieniek-Walenda et al. (30), who assessed the level of nutritional knowledge of patients after acute coronary syndrome hospitalized in a cardiology department. A good level of nutritional knowledge concerned only 6.9% of the subjects.
Analyzing dietary habits and the effect of diet on glycemic variability in patients with type 1 diabetes, a study by Koperska et al. (31) observed that, except for too little consumption of vegetables and too much consumption of fatty acids, the diet of respondents was satisfactory and following recommendations. Diet significantly influenced the variability of glycemic results, and properly planned nutrition was conducive to achieving the intended therapeutic goals. A study by Izycka et al. (32) on the diet of another group of patients, i.e., patients diagnosed with non-alcoholic steatohepatitis, showed that the vast majority of respondents, as in the author’s study, were eating incorrectly. Mistakes consisted mainly of consuming too many products rich in saturated fatty acids and simple sugars.
The results of assessing the dietary habits of patients with cardiovascular disease in the study by Mikulska et al. (33) were similar to those of the authors. The subjects also consumed excessive amounts of foods rich in fat and simple sugars, and insufficient amounts of foods containing dietary fiber, vegetables, legumes, nuts and fish. Similar to our results, the study also reported insufficient water intake. In conclusion, regardless of the diagnosed disease, the level of knowledge and eating habits of the public is inadequate, and it is necessary to introduce broad-based nutrition education.
Tests on the levels of biochemical parameters and patients’ blood counts, as well as the respondents’ blood pressure and their NRS, did not correlate with the occurrence of diabetes and/or obesity. Different results were obtained by Lewandowski et al. (34), who compared blood morphology studies with selected biochemistry results in elderly patients. This study showed that the onset of inflammation and associated changes in biochemistry affect the morphology of responders.
One of the main strengths of the study is the large number of respondents, which increases the representativeness of the results and allows for more reliable conclusions about the dietary habits and nutritional status of patients with cardiovascular disease. The use of the FFQ questionnaire provides accurate results on the frequency of product consumption, which allows for a detailed analysis of eating habits. In addition, a detailed questionnaire assessing the level of patients’ nutritional knowledge makes it possible to evaluate their awareness of diet and its impact on health. The survey took into account both clinical data (e.g., blood pressure, morphological and biochemical blood test results) and information on dietary habits, which allows a broad assessment of the impact of diet on patients’ health. It should be mentioned that the study was conducted in a hospital setting allowed direct assessment of patients’ health status and provided greater control over the quality of the data collected.
However, the study also has some weaknesses. Limiting the survey to a single institution may limit the ability to generalize the results to a broader population of patients with cardiovascular disease. There is also a risk of potential respondent error, as with surveys there is always the possibility that respondents may not answer honestly or accurately, which may affect the reliability of the results. In addition, the measurement of dietary habits and nutritional status was conducted only once, which does not allow for analysis of changes over time.
5 Conclusion
Analysis of the results obtained allows us to propose conclusions that the body weight and BMI value of the majority of respondents indicated overweight or obesity, and these results varied by gender, age, and the presence of diseases. There was no increased risk of malnutrition and no variation in the prevalence of malnutrition levels using the NRS 2002 scale. In addition, the respondents’ level of knowledge was inadequate and varied. Several abnormalities in dietary behavior and habits were found, in particular: a low level of consumption of vegetables and fruits, pulses, nuts and grains, whole grain cereal products, fish and milk, and dairy products, as well as a markedly insufficient intake of water. On the positive side, there was a low intake of salty snacks, sweetened energy drinks, and alcohol. There were no differences in the respondents’ eating behavior and habits in the context of the diagnosed disease entity. In addition, the vast majority of respondents had a diagnosed metabolic disease, co-morbidities were also common, and analysis of biochemical and blood count results showed some abnormalities, but these results did not vary by gender, age, BMI, and NRS scale.
The study results clearly indicate significant clinical and public health implications. Clinically, the inappropriate body weight of the majority of patients with cardiovascular diseases significantly increases the risk of cardiovascular complications. Although patients with diabetes and obesity possess better nutritional knowledge, this does not always translate into healthy dietary habits, highlighting the need for education that effectively changes behaviors. From a public health perspective, these findings emphasize the necessity of spreading nutritional education throughout society, especially among high-risk groups, and implementing educational programs and policies that promote healthy eating. Early dietary intervention based on solid knowledge could significantly reduce the risk of developing chronic diseases, thereby improving the overall health of the population.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Bioethics Committee of the Silesian Medical University in Katowice no. PCN/0022/KB/299/19/20 (approval date: 21.01.2020). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
A-MS: Conceptualization, Data curation, Formal analysis, Methodology, Software, Writing – original draft. WS-B: Methodology, Project administration, Writing – review & editing. EG-N: Conceptualization, Validation, Visualization, Writing – review & editing. MK: Funding acquisition, Investigation, Resources, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Lemieux, I, and Després, JP. Metabolic syndrome: past, present and future. Nutrients. (2020) 12:3501. doi: 10.3390/nu12113501
2. Fisher, L, Polonsky, WH, Perez-Nieves, M, Desai, U, Strycker, L, and Hessler, D. A new perspective on diabetes distress using the type 2 diabetes distress assessment system (T2-DDAS): prevalence and change over time. Direct. (2022) 36:108256. doi: 10.1016/j.jdiacomp.2022.108256
3. Litwin, M, and Kułaga, Z. Obesity, metabolic syndrome, and primary hypertension. Pediatr Nephrol. (2021) 36:825–37. doi: 10.1007/s00467-020-04579-3
4. Bryl, W, and Pupek-Musialik, D. Obesity of children and adolescents – epidemiology, consequences and prevention. Guide for GPs. (2006) 9:91–5.
5. Seravalle, G, and Grassi, G. Obesity and hypertension. Pharmacol Res. (2017) 122:1–7. doi: 10.1016/j.phrs.2017.05.013
6. Suliga, E . Otyłość brzuszna – metody oceny, przyczyny występowania, implikacje zdrowotne. Studia Medyczne. (2012) 27:65–71. doi: 10.5114/ms.2012.27253
7. Browning, LM, Hsieh, SD, and Ashwell, M. A systematic review of waist-to-height ratio as a screening tool for the prediction of cardiovascular disease and diabetes: 0·5 could be a suitable global boundary value. Nutr Res Rev. (2010) 23:247–69. doi: 10.1017/S0954422410000144
8. Jarosz, M., Szponar, L., and Rychlik, E. Nadwaga, otyłość, niedożywienie w Polsce. Otyłość, żywienie, aktywność fizyczna, zdrowie Polaków. Instytut Żywności i Żywienia. Warszawa, (2006); pp. 45–114.
9. KAISER, AB, ZHANG, N, and der PLUIJM, WV. Global prevalence of type 2 diabetes over the next ten years (2018-2028). Diab Abstr. (2018) 67:1. doi: 10.2337/db18-202-LB
10. Małecki, MT . Obesity – insulin resistance – type 2 diabetes mellitus. Kardiol Pol. (2006) 64, 10, 6:561–6.
11. Rajewski, P, Waleśkiewicz, K, and Dobosz, K. Analiza składowych zespołu metabolicznego według IDF u kobiet z cukrzycą typu 2. Family Med Prima Care Rev. (2008) 10:624–6.
12. Wondmkun, YT . Obesity, insulin resistance, and type 2 diabetes: associations and therapeutic implications. Diab Metab Syndr Obes. (2020) 13:3611–6. doi: 10.2147/DMSO.S275898
13. Kahn, R, Buse, J, Ferrannini, E, and Stern, MAmerican Diabetes AssociationEuropean Association for the Study of Diabetes. The metabolic syndrome: time for a critical appraisal. Joint statement from the American Diabetes Association and the European Association for the Study of diabetes. Diabetes Care. (2005) 28:2289–304. doi: 10.2337/diacare.28.9.2289
14. Galicia-Garcia, U, Benito-Vicente, A, Jebari, S, Larrea-Sebal, A, Siddiqi, H, Uribe, KB, et al. Pathophysiology of type 2 diabetes mellitus. Int J Mol Sci. (2020) 21:6275. doi: 10.3390/ijms21176275
15. Mirkarimi, K . Effectiveness of nutritional education on nutritional behavior and anthropometric indexes among patients with hypertension based on the health promotion model. Int J Health Promot Educ. (2024) 1–16. doi: 10.1080/14635240.2024.2334875
16. Follow-up report on the diagnosis of diabetes mellitus. Diabetes Care. (2003) 26:3160–7. doi: 10.2337/diacare.26.11.3160
17. Henning, RJ . Type-2 diabetes mellitus and cardiovascular disease. Futur Cardiol. (2018) 14:491–509. doi: 10.2217/fca-2018-0045
19. Jarosz, M. Diagnozowanie zaburzeń stanu odżywienia, w praktyce lekarskiej i pielęgniarskiej. Instytut Żywności i Żywienia. Warszawa, (2010); pp. 2–22.
20. Kondrup, J, Allison, SP, Elia, M, Vellas, B, and Plauth, MEducational and Clinical Practice Committee, European Society of Parenteral and Enteral Nutrition (ESPEN). ESPEN guidelines for nutrition screening 2002. Clin Nutr. (2003) 22:415–21. doi: 10.1016/S0261-5614(03)00098-0
21. Niedzwiedzka, E, Wadolowska, L, and Kowalkowska, J. Reproducibility of a non-quantitative food frequency questionnaire (62-item FFQ-6) and PCA-driven dietary pattern identification in 13–21-year-old females. Nutrients. (2019) 11:2183. doi: 10.3390/nu11092183
22. Frese, EM, Fick, A, and Sadowsky, HS. Blood pressure measurement guidelines for physical therapists. Cardiopulm Phys Ther J. (2011) 22:5–12. doi: 10.1097/01823246-201122020-00002
23. Stefańska, E, Ostrowska, L, Czapska, D, and Karczewski, J. Consumption frequency of selected groups of food products among obese subjects. Bromat Chem Toksykol. (2008) 51:716–9.
24. Pielak, M, Olubiec-Opatowska, E, Czarniecka-Skubina, E, and Jaworska, D. Contemporary trends in the consumption of selected cereal products. Przemysł Spożywczy. (2018) 72:6. doi: 10.15199/65.2018.6.5
25. Szczepańska, E, and Brończyk-Puzoń, A. Evaluation of nutritional habits of obese patients qualified for bariatric surgery. Medycyna ogólna i Nauki o Zdrowiu. (2014) 20:330–4. doi: 10.5604/20834543.1124667
26. Włodarek, D, and Głąbksa, D. Vegetables and fruits consumption by individuals with diabetes mellitus type 2. Diabetologia Praktyczna. (2010) 11:6.
27. Drywień, ME, and Kuć, A. Specyfika zachowań żywieniowych osób starszych pochodzących ze środowiska wiejskiego. Kosmos. (2019) 68:303–10. doi: 10.36921/kos.2019_2544
28. Pilska, M . Wiedza i postrzeganie tłuszczów a zwyczaje żywieniowe polskich konsumentów produktów do smarowania pieczywa. Archives de médecine et de chirurgie pratiques. (2020) 122:148–63. doi: 10.15193/zntj/2020/122/329
29. Witanowska, J, Warmuz-Wancisiewicz, A, Wójcik, J, Nowak, U, and Jarecka, B. Eating habits in selected population of developmental age. In: Human health in ontogenesis – biomedical and psychosocial aspects. 1st ed, Poland: Biomed Aspects Katowice (2020) 141–149.
30. Bieniek-Walenda, J, Brończyk-Puzoń, A, and Jagielski, P. Ocena poziomu wiedzy żywieniowej za pomocą kwestionariusza komPAN pacjentów po ostrym zespole wieńcowym hospitalizowanych na oddziale kardiologii inwazyjnej. Doniesienie wstępne. Folia Cardiol. (2020) 15:1–5. doi: 10.5603/FC.2020.0012
31. Koperska, A, and Rogowicz-Frontczak, A. Ocena sposobu żywienia oraz wpływ diety na zmienność glikemii u chorych na cukrzycę typu 1 leczonych za pomocą osobistej pompy insulinowej. Forum Zaburzeń Metabolicznych. (2022) 13:9–18. doi: 10.5603/FZM.2022.0002
32. Iżycka, I, and Moszak, M. Ocena wartości energetycznej i odżywczej diety oraz sposobu odżywiania pacjentów ze stłuszczeniową chorobą wątroby. Forum Zaburzeń Metabolicznych. (2021) 12:115–23. doi: 10.5603/FZM.2021.0015
33. Mikulska, A, Grzelak, T, Pelczyńska, M, and Czyżewska, K. Ocena nawyków żywieniowych pacjentów z chorobami układu sercowo-naczyniowego. Forum Zaburzeń Metabolicznych. (2019) 10:142–51. doi: 10.5603/FZM.2019.0023
Keywords: dietary habits, nutritional knowledge, nutritional status, cardiological patients, obesity, diabetes
Citation: Sapała A-M, Staśkiewicz-Bartecka W, Grochowska-Niedworok E and Kardas M (2024) Dietary habits, nutritional knowledge, and nutritional status among cardiological patients, including those with obesity and diabetes. Front. Nutr. 11:1455236. doi: 10.3389/fnut.2024.1455236
Edited by:
Ying Xin, Jilin University, ChinaReviewed by:
Xiaowen Wang, Harvard University, United StatesMd Kamruzzaman, Islamic University, Bangladesh
Copyright © 2024 Sapała, Staśkiewicz-Bartecka, Grochowska-Niedworok and Kardas. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wiktoria Staśkiewicz-Bartecka, d3N0YXNraWV3aWN6QHN1bS5lZHUucGw=