
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr. , 24 July 2024
Sec. Clinical Nutrition
Volume 11 - 2024 | https://doi.org/10.3389/fnut.2024.1440185
This article is part of the Research Topic Vitamin D: From Pathophysiology to Clinical Impact, volume II View all 24 articles
 Miguel Angel Villasis-Keever1
Miguel Angel Villasis-Keever1 Jessie Nallely Zurita-Cruz2*
Jessie Nallely Zurita-Cruz2* Juan Garduño-Espinosa3
Juan Garduño-Espinosa3 Mardya López-Alarcón4
Mardya López-Alarcón4 Aly Sugey Barradas Vázquez4María Guadalupe Miranda-Novales1
Aly Sugey Barradas Vázquez4María Guadalupe Miranda-Novales1 Israel Parra-Ortega5
Israel Parra-Ortega5 Briseida López-Martinez5Heladia García1
Briseida López-Martinez5Heladia García1 Miguel Klünder-Klünder6
Miguel Klünder-Klünder6Introduction: Globally, up to 76.6% of the population may be affected by vitamin D (VD) deficiency, which has been linked to increased morbidity and mortality from COVID-19. This underscores the importance of further research into VD supplementation, particularly for health care workers, who are at higher risk due to indoor work environments and dietary challenges associated with shift schedules.
Objective: This study aimed to identify factors associated with VD deficiency in Mexican health care workers exposed to SARS-CoV-2.
Materials and methods: We conducted a cross-sectional study from June 2020 to January 2021 among frontline health care workers treating hospitalized COVID-19 patients. Blood samples were collected to measure 25-hydroxy VD levels via radioimmunoassay. We also assessed previous COVID-19 infection and comorbidities that could influence VD levels.
Results: The study included 468 health care workers. The median serum VD concentration was 16.6 ng/mL. VD deficiency was found in 69.4% (n = 325) of participants, while only 5.1% (n = 24) had normal levels. Those with type 2 diabetes (13.3 ng/mL vs. 17.1 ng/mL) or obesity (15.7 ng/mL vs. 17.1 ng/mL) had significantly lower VD levels than their counterparts (p < 0.001 and p = 0.049, respectively). No significant differences were found among participants with high blood pressure. Multivariate analysis revealed that type 2 diabetes was independently associated with VD deficiency.
Conclusion: There is a high prevalence of VD deficiency among health care workers, which is potentially linked to both personal health factors and occupational conditions.
Vitamin D (VD) deficiency poses a significant global health challenge, with research indicating a prevalence rate of up to 76.6%, underscoring substantial regional variability and the impact of diverse determinant factors (1). Certain occupational groups exhibit a heightened prevalence of VD deficiency. This issue is partly linked to limited sun exposure inherent to specific job roles, particularly those conducted predominantly indoors or within shift work schedules, including night shifts (2). Additionally, those working night or rotating shifts are prone to less healthy dietary patterns. This tendency is influenced by a lack of suitable nutritional options and restricted eating times due to long working hours, leading to diets high in ultra-processed foods, meats, fats, and alcoholic beverages (3). Such dietary habits, combined with the demands of shift work, may contribute to the development of digestive disorders, sleep disturbances, and comorbidities (4). These risk factors, including limited sun exposure, inadequate diet, and obesity, which are inherent to the health care profession, significantly contribute to VD deficiency (5, 6).
During the COVID-19 pandemic, populations in areas with a high prevalence of VD deficiency experienced increased morbidity and mortality related to COVID-19 infection. This finding supports further studies on the prevalence of VD deficiency and the benefits of VD supplementation across various pathologies, from cardiometabolic disorders to viral infections (7). During the pandemic, the working conditions of health care workers worsened, likely due to the increase in indoor activities—both work-related and personal—heightening the risk of VD deficiency (8).
VD affects various body systems beyond bone health, including the immune system, where it modulates immune responses; the cardiovascular system, which influences heart and blood vessel functions; the endocrine system, particularly insulin secretion and glucose metabolism; and the nervous system, which affects brain function and mental health. These roles highlight the importance of VD in overall health and disease prevention (9).
Therefore, this study aimed to identify factors associated with VD deficiency in Mexican health care workers exposed to SARS-CoV-2. This information may strengthen the importance of vitamin D supplementation in this high-risk group.
This cross-sectional study was carried out between June 2020 and January 2021 at four tertiary care hospitals treating COVID-19 patients in Mexico City. Participants were enrolled during the period from June 15 to December 15, 2020, encompassing the summer and fall seasons. The inclusion criteria were frontline health care workers who were hospitalized with COVID-19, who underwent confirmatory testing for SARS-CoV-2 due to suspected symptoms or due to having unprotected contact with a suspected case, and who had a blood test for 25-hydroxy vitamin D (25[OH]D) levels. The exclusion criteria included subjects who were already receiving VD or other vitamin supplements and those whose 25[OH]D samples were not processed.
Data from health care workers without COVID-19 were obtained from a previous clinical trial registered at ClinicalTrials.gov (#NCT04535791), and these data were used to analyze the efficacy and safety of VD supplementation in preventing SARS-CoV-2 infection (10).
Participants were divided into two groups: those with VD deficiency (25[OH]D levels <20 ng/mL) and those without (25[OH]D levels ≥20 ng/mL) (11).
As previously described (10), all participants underwent simultaneous serum sampling for 25[OH]D determination and RT–PCR COVID-19 testing, which occurred as part of the RCT selection process. Anthropometric measurements and blood pressure assessments were performed on the participants. Obesity was defined as a body mass index (BMI) >30. Previous diagnoses of type 2 diabetes (T2D) and high blood pressure (HBP) were recorded as comorbidities. HBP was defined as a persistent elevation of blood pressure above systolic pressure ≥ 140 mmHg or diastolic pressure ≥ 90 mmHg (12), and T2D was defined as fasting plasma glucose levels >126 mg/dL or 2-h values in the oral glucose tolerance test of >200 mg/dL (13). A subject was classified as having a positive SARS-CoV-2 infection if they presented a positive real-time polymerase chain reaction (RT–PCR) test.
The protocol was approved by the institutional review boards of the Instituto Mexicano del Seguro Social (CNIS # R-2020-785-090) and Hospital Infantil de Mexico Federico Gómez (HIM-2020-045). All participants provided written informed consent after the procedures were explained according to the protocol.
The 25(OH)D concentrations were determined at the Hospital Infantil de Mexico Clinical Laboratory using the Abbot brand chemiluminescence technique with Architect 1,000 equipment. According to the serum levels, a VD deficiency was defined as <20 ng/mL, VD insufficiency was defined as 20–29.99 ng/mL, and a normal level was defined as >30 ng/mL (11, 14).
Using the Kolmogorov–Smirnov test, it was determined that the quantitative variables did not have a Gaussian distribution, so they are presented as median with their respective 95% confidence intervals (95% CIs). Qualitative variables are expressed as proportions and frequencies.
Patients were categorized into two groups: those with and without VD deficiency. VD levels were compared across participants based on their comorbidities and type of personnel. Additionally, serum VD concentrations were compared among factors that could influence levels, such as obesity, T2D, HBP, age, and sex.
To assess differences between groups, we applied the Mann–Whitney U test or Kruskal-Wallis for quantitative variables and the chi–square test for qualitative variables.
Multiple logistic regression analysis was conducted to determine the associations of VD levels with age, male sex, HBP, T2D, and obesity. All the statistical analyses were performed using STATA version 12.0.
Among the 590 potential candidates for inclusion, 122 were excluded: 72 did not meet the inclusion criteria, 18 had samples that were not processed for serum vitamin D levels, and 32 were health care workers who declined to participate. Among the 468 health care workers included, the median age was 40 years, and there was a predominance of female participants (65.4%). Nursing was the most common type of personnel (35.5%), followed by doctors (20.5%) and laboratory personnel (17.7%).
As shown in Table 1, 197 (42.1%) participants had one or more comorbidities, and HBP was the most common (n = 145, 31.0%). In total, 151 patients were positive for SARS-CoV-2 (32.3%).
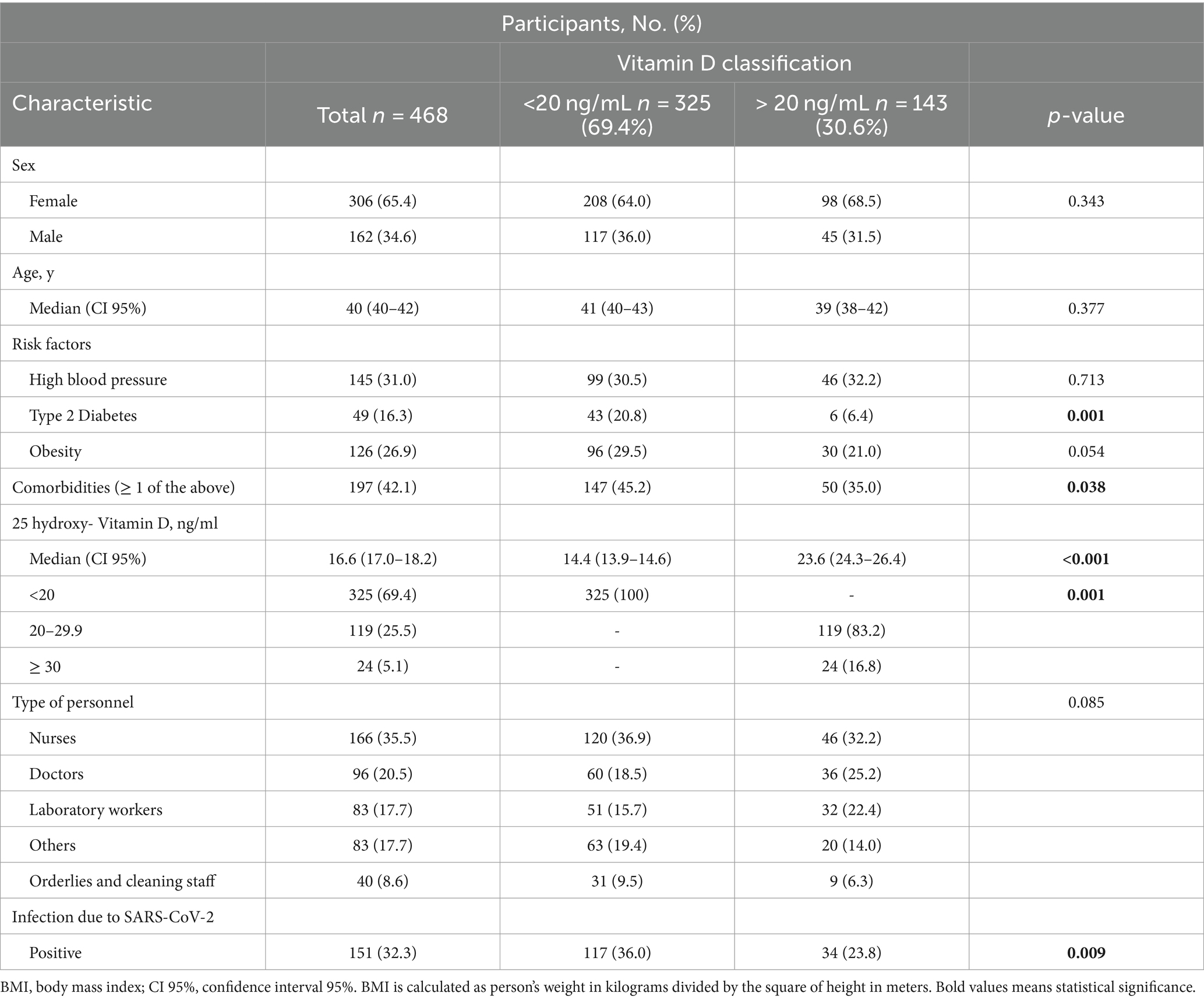
Table 1. General characteristics of the health-care workers included.
The distribution of VD levels is shown in Figure 1; the median VD level among all health care workers was 16.6 ng/mL (95% CI 17.0–18.2 ng/mL). Among the 24 health care workers with sufficient VD levels, the median age was 39 years (95% CI: 38–46). Of these, 4.2% (n = 1) had DM2, 37.5% (n = 9) had hypertension, and 20.8% (n = 5) were obese.
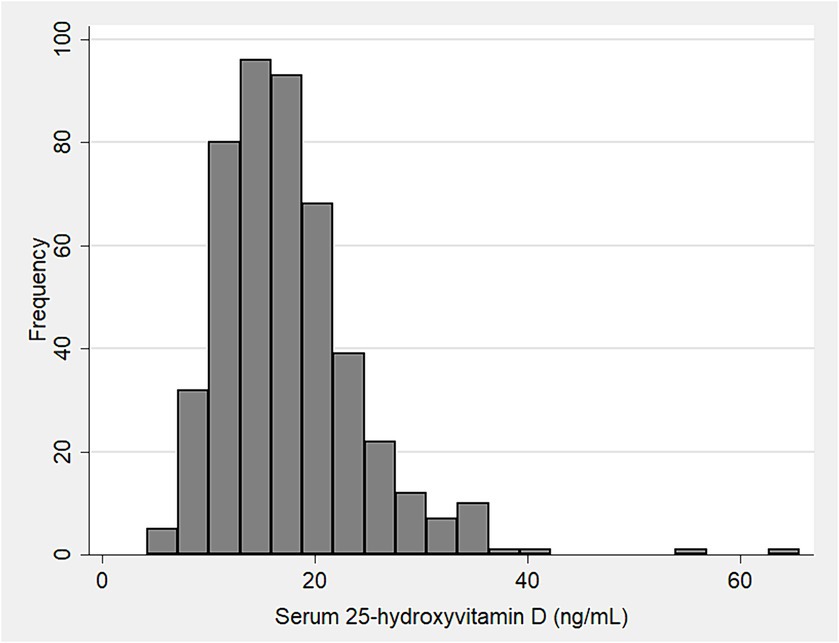
Figure 1. Histogram showing the distribution of serum 25-hydroxy vitamin D levels in 468 health-care workers.
There was no difference in VD levels according to age or sex, nor by type of health personnel (Figure 2A). However, when comparing between participants with and without VD deficiency (Table 1), a smaller proportion of doctors (18.5% vs. 25.5%) and laboratory workers (15.7% vs. 22.4%) had VD deficiency compared to nurses (36.9% vs. 32.2%), but this difference was not statistically significant. By contrast, participants with T2D and other comorbidities had a statistically higher frequency of VD deficiency (p < 0.05), as shown in Table 1.
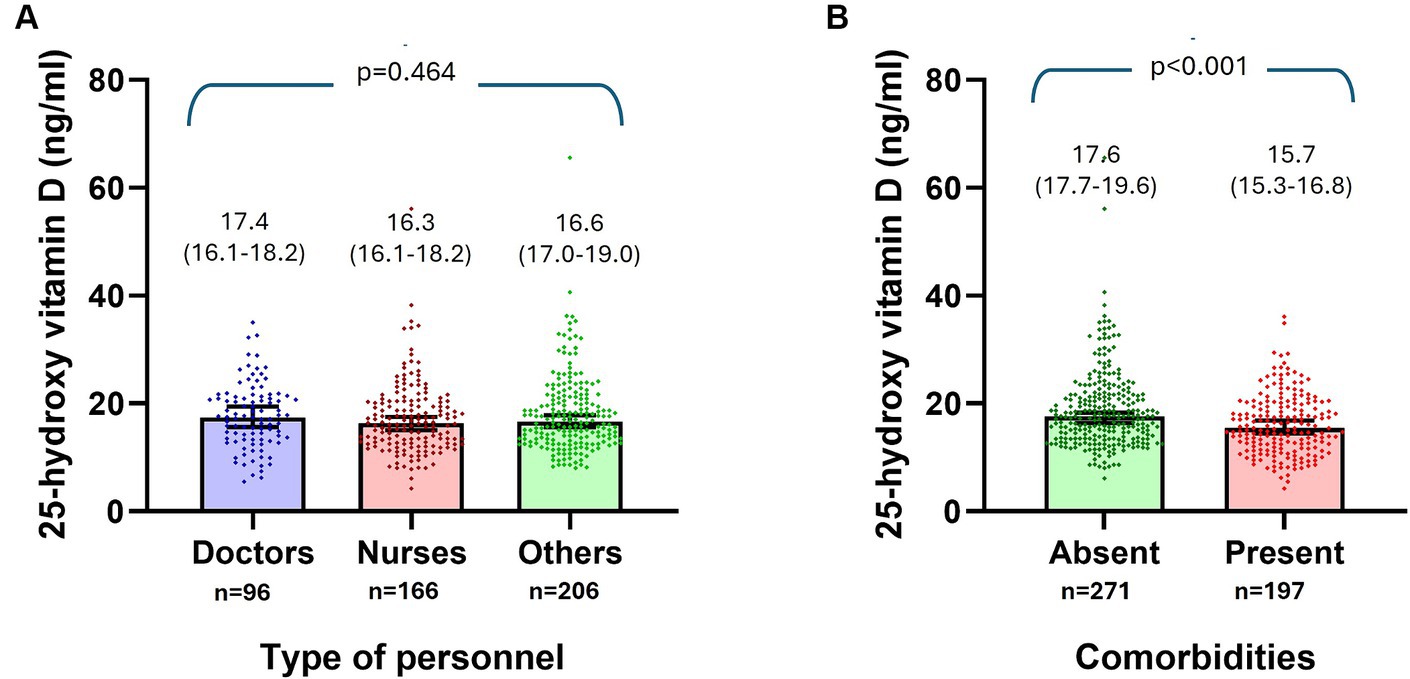
Figure 2. Comparison of serum levels of 25-hydroxy vitamin D (ng/ml) according to the type of personnel (A), and by the presence or not of comorbidities (B).
Serum VD concentrations were also compared among patients according to factors that could influence serum levels. Subjects with T2D (13.3 ng/mL vs. 17.1 ng/mL, p < 0.001), obesity (15.7 ng/mL vs. 17.1 ng/mL, p = 0.047), and comorbidities (15.7 ng/mL vs. 17.6 ng/mL, p < 0.001) had lower VD levels than those without these factors (Figure 2B). No significant differences were found among participants with HBP (Table 2).
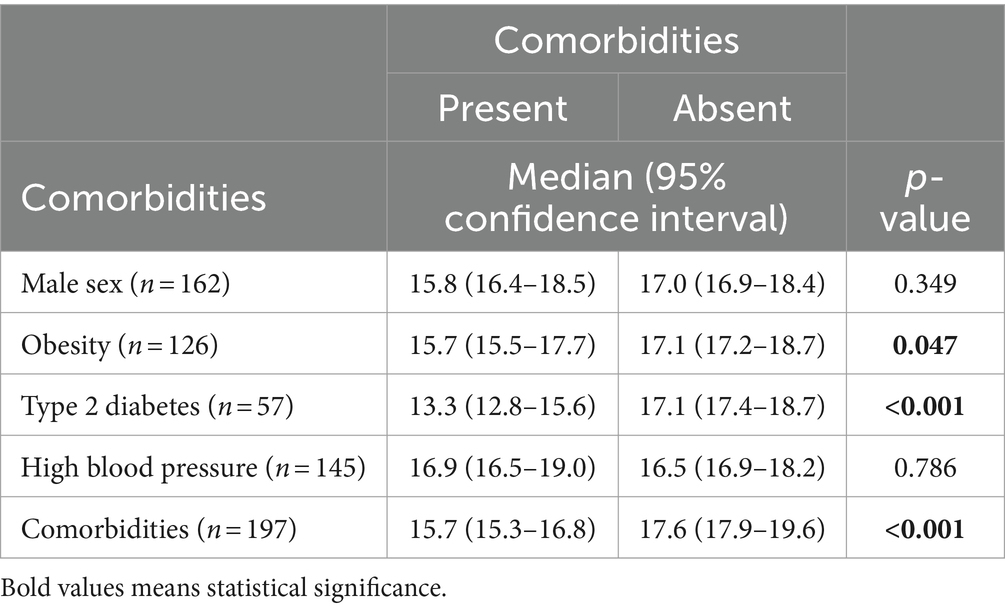
Table 2. Comparison of serum levels of 25-hydroxy vitamin D (ng/ml) according to the characteristics of healthcare workers.
According to the multivariate analysis, T2D (OR 3.40, CI 95%: 1.43 to 8.05, p = 0.005) was associated with VD deficiency, adjusted for age, sex, the presence of obesity, and HBP (Table 3).
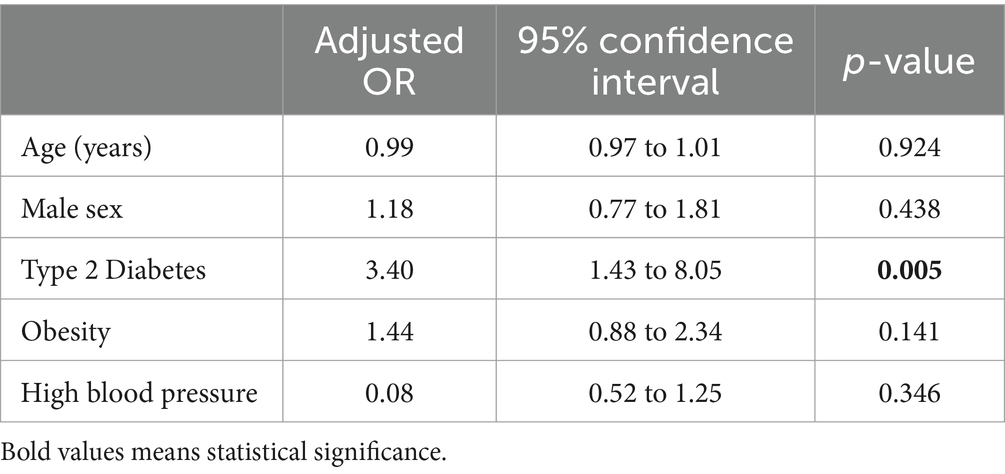
Table 3. Logistic regression analysis to identify factors related to deficiency vitamin D.
The high prevalence of VD deficiency among Mexican health care workers exposed to SARS-CoV-2 observed in our study is alarming, with 69.4% showing low serum levels. This rate is significantly higher than that seen in the general population but aligns with findings from studies on high-risk occupational groups and individuals with conditions such as obesity and diabetes (2, 15). This rate of VD deficiency, which is higher than the global average of 50%, underscores the severity of the issue. In the Americas, the prevalence of VD deficiency has reached 77% (16). Specifically, in Mexico, the National Health and Nutrition Survey 2006 (ENSANUT) reported a VD deficiency and insufficiency rate of 30% in adults, with Mexico City (area where this study was developed) showing a higher rate than other regions, at 43.1% (17). During the first year of the COVID-19 pandemic, health care workers faced long hours (which reduced sun exposure) and a shortage of medications (including cholecalciferol) and consumed low levels of VD-rich foods, leading to increased rates of VD deficiency. It is crucial to maintain optimal VD concentrations, which, according to the Society of Endocrinology, should be above 30 ng/mL (14, 18). Our findings are similar to those recently reported by Ito et al.; they conducted a study to examine the prevalence of VD deficiency among healthcare workers following the onset of the COVID-19 pandemic (19). They identified that 9.2% of the subjects had adequate VD levels, whereas our data revealed that only 5.1% had adequate VD levels (>30 ng/mL).
Studies focusing on VD deficiency across different occupational and health risk groups have documented varying prevalence rates. For instance, shift workers and indoor workers experience similar trends of VD deficiency due to comparable environmental and work conditions that limit sun exposure, with deficiency rates between 78 and 80% compared to 48% for outdoor workers (2, 20). Recent studies have reported that the prevalence of VD deficiency among health care workers ranges from 45 to 51% (19, 21). These trends, observed across occupations with limited outdoor activity, highlight the occupational risk associated with VD deficiency. These findings emphasize the critical role of occupational factors in VD levels, suggesting that regular screening for VD levels in high-risk occupational groups should be considered in clinical practice guidelines and public health initiatives to prevent adverse health outcomes linked to VD deficiency.
Health care workers often endure prolonged periods indoors with limited exposure to natural sunlight, which is the primary source necessary for synthesizing VD in the skin. This issue is compounded in roles that involve night shifts or extensive indoor duties. The deficiency in VD is due to low UVB exposure and a secondary decrease in vitamin synthesis in the skin with aging (22, 23), as the precursor to VD, 7-dehydrocholesterol, decreases by approximately 50% between the ages of 20 and 80 (23).
Obesity and diabetes merit particular attention among the factors that influence VD levels. The literature presents contradictory results regarding the impact of obesity on VD deficiency (24). However, VD deficiency becomes more apparent in obese patients when diabetes mellitus is also present. A study conducted by Atia et al. (25) revealed that the prevalence of VD deficiency was significantly greater in individuals with prediabetes than in those without prediabetes (38.5% vs. 25.5%). In obese individuals, VD tends to be sequestered within adipose tissue, reducing its availability in the bloodstream. This biological trapping of VD in fat cells diminishes its overall active circulation (26). In the context of diabetes, the disease’s impact on renal function and liver enzymes can interfere with the hydroxylation processes that are essential for the vitamin’s activation. High glucose levels, which are common in diabetes, may further impair these processes, complicating the metabolic pathway required for converting VD to its active form (27, 28). These interconnected mechanisms highlight a compounded risk where occupational and personal health factors converge, leading to increased vulnerability to VD deficiency.
Study limitations include the inability to specify the work schedules of the included workers, as shifts varied during the pandemic. The study did not analyze the seasons during which participants were included; however, only non-winter seasons, namely, summer and autumn, were considered; winter, which is associated with decreased serum VD levels, was not included. The major limitation was the cross-sectional study design, which could not establish a causal relationship between VD deficiency and modifying factors such as obesity and diabetes.
Given the high prevalence of VD deficiency among health care workers, particularly those with prolonged indoor exposure and minimal sunlight, it is imperative to routinely evaluate serum VD levels. For health care workers, especially those positive for SARS-CoV-2, the benefits of VD supplementation could extend beyond correcting the deficiency—it might also enhance immune response capabilities against viral infections. Considering the broader implications, maintaining adequate vitamin D levels is crucial for infectious disease prevention and general health maintenance within health care settings.
In conclusion, the frequency of low VD values is high among health care workers, and TD2 was a significant risk factor associated with these values. This study underscores the urgent need for systematic VD deficiency screening and tailored VD supplementation strategies. Such measures are crucial not only for the health of individual workers but also for supporting the operational integrity and resilience of health care systems facing ongoing public health challenges.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by The protocol was approved by the institutional review boards of the Instituto Mexicano del Seguro Social (CNIS # R-2020-785-090) and Hospital Infantil de Mexico Federico Gómez (HIM-2020-045). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
MV-K: Conceptualization, Funding acquisition, Supervision, Validation, Writing – review & editing. JZ-C: Data curation, Formal analysis, Investigation, Writing – original draft, Writing – review & editing. JG-E: Funding acquisition, Supervision, Writing – review & editing. ML-A: Resources, Supervision, Writing – review & editing. AB: Data curation, Investigation, Writing – review & editing. MM-N: Formal analysis, Investigation, Writing – review & editing. IP-O: Formal analysis, Investigation, Writing – review & editing. BL-M: Investigation, Writing – review & editing. HG: Writing – review & editing, Investigation. MK-K: Funding acquisition, Supervision, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work was supported by a Mexican Federal Funds Grant (HIM 2020/131).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Cui, A, Zhang, T, Xiao, P, Fan, Z, Wang, H, and Zhuang, YE. Global and regional prevalence of vitamin D deficiency in population-based studies from 2000 to 2022: a pooled analysis of 7.9 million participants. Front Nutr. (2023) 10:1070808. doi: 10.3389/fnut.2023.1070808
2. Sowah, D, Fan, X, Dennett, L, and Hagtvedt, RSS. Vitamin D levels and deficiency with different occupations: a systematic review. BMC Public Health. (2017) 17:519. doi: 10.1186/s12889-017-4436-z
3. Wolska, A, Stasiewicz, B, Kaźmierczak-Siedlecka, K, Ziętek, M, Solek-Pastuszka, J, Drozd, A, et al. Unhealthy food choices among healthcare shift workers: a cross-sectional study. Nutrients. (2022) 14:4327. doi: 10.3390/nu14204327
4. Nea, FM, Kearney, J, Livingstone, MB, Pourshahidi, LK, and Corish, CAE. Dietary and lifestyle habits and the associated health risks in shift workers. Nutr Res Rev. (2015) 28:143–66. doi: 10.1017/S095442241500013X
5. Vranić, L, Mikolašević, I, and Milić, SE. Vitamin D deficiency: consequence or cause of obesity? Medicine. (2019) 55:541. doi: 10.3390/medicina55090541
6. Wu, SE, and Chen, WL. Moderate sun exposure is the Complementor in insufficient vitamin D consumers. Front Nutr. (2022) 9:832659. doi: 10.3389/fnut.2022.832659
7. Mariani, J, Giménez, VMM, Bergam, I, Tajer, C, Antonietti, L, Inserra, F, et al. Association between vitamin D deficiency and COVID-19 incidence, complications, and mortality in 46 countries: an ecological study. Health Secur. (2021) 19:302–8. doi: 10.1089/hs.2020.0137
8. Funaki, T, Sanpei, M, Morisaki, N, and Mizoue, TYK. Serious vitamin D deficiency in healthcare workers during the COVID-19 pandemic. BMJ Nutr Prev Heal. (2022) 5:134–6. doi: 10.1136/bmjnph-2021-000364
9. Carlberg, C, Raczyk, M, and Zawrotna, NE. Vitamin D: a master example of nutrigenomics. Redox Biol. (2023) 62:102695. doi: 10.1016/j.redox.2023.102695
10. Villasis-Keever, MA, López-Alarcón, MG, Miranda-Novales, G, Zurita-Cruz, JN, Barrada-Vázquez, AS, González-Ibarra, J, et al. Efficacy and safety of vitamin D supplementation to prevent COVID-19 in frontline healthcare workers. A randomized clinical trial. Arch Med Res. (2022) 53:423–30. doi: 10.1016/j.arcmed.2022.04.003
11. Holick, MF, Binkley, NC, Bischoff-Ferrari, HA, Gordon, CM, Hanley, DA, Heaney, RP, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. (2011) 96:1911–30. doi: 10.1210/jc.2011-0385
12. Unger, T, Borghi, C, Charchar, F, Khan, NA, Poulter, NR, Prabhakaran, D, et al. 2020 International Society of Hypertension global hypertension practice guidelines. J Hypertens. (2020) 38:982–1004. doi: 10.1097/HJH.0000000000002453
13. American Diabetes Association . 2. Classification and diagnosis of diabetes:standards of medical Care in Diabetes—2020. Diabetes Care. (2020) 43:S14–31. doi: 10.2337/dc20-S002
14. Amrein, K, Scherkl, M, Hoffmann, M, Neuwersch-Sommeregger, S, Köstenberger, M, Tmava Berisha, A, et al. Vitamin D deficiency 2.0: an update on the current status worldwide. Eur J Clin Nutr. (2020) 74:1498–513. doi: 10.1038/s41430-020-0558-y
15. da Silva, TBP, Luiz, MM, Delinocente, MLB, Steptoe, A, de Oliveira, C, and Alexandre, TDSE. Is abdominal obesity a risk factor for the incidence of vitamin D insufficiency and deficiency in older adults? Evidence from the ELSA study. Nutrients. (2022) 14:4164. doi: 10.3390/nu14194164
16. Contreras-Manzano, A, Villalpando, S, and Robledo-Pérez, RE. Vitamin D status by sociodemographic factors and body mass index in Mexican women at reproductive age. Salud Publ Mex. (2016) 59:518–25. doi: 10.21149/8080
17. Flores, M, Sánchez-Romero, LM, Macías, N, Lozada, A, Díaz, E, and Barquera, S E. Concentraciones séricas de vitamina D en niños, adolescentes y adultos mexicanos. (2006) Available at: https://www.insp.mx/images/stories/Centros/cinys/Docs/111202_ReporteVitaminaD.pdf
18. Prietl, B, Treiber, G, Pieber, TRAK, and Amrein, K. Vitamin D and immune function. Nutrients. (2013) 5:2502–21. doi: 10.3390/nu5072502
19. Ito, A, Yamamoto, S, Oshiro, Y, Inamura, N, Nemoto, T, Tan, T, et al. Vitamin D deficiency during the coronavirus disease 2019 (COVID-19) pandemic among healthcare workers. Clin Nutr ESPEN. (2024) 60:210–6. doi: 10.1016/j.clnesp.2024.02.005
20. Martelli, M, Salvio, G, Santarelli, L, and Bracci, ME. Shift work and serum vitamin D levels: a systematic review and Meta-analysis. Environ Res Public Health. (2022) 19:8919. doi: 10.3390/ijerph19158919
21. Phelan, J, Thangamuthu, A, Muthumeenal, S, Houston, K, Everton, M, Gowda, S, et al. Vital D: a modifiable occupational risk factor of UK healthcare workers. PLoS One. (2024) 19:e0296247. doi: 10.1371/journal.pone.0296247
22. Grant, WB, Lahore, H, McDonnell, SL, Baggerly, CA, French, CB, Aliano, JL, et al. Evidence that vitamin D supplementation could reduce risk of influenza and COVID-19 infections and deaths. Nutrients. (2020) 12:988. doi: 10.3390/nu12040988
23. Biesalski, HK . Vitamin D deficiency and co-morbidities in COVID-19 patients – a fatal relationship? Nfs J. (2020) 20:10–21. doi: 10.1016/j.nfs.2020.06.001
24. Lima-Martínez, MM, Arrau, C, Jerez, S, Paoli, M, González-Rivas, JP, Nieto-Martínez, R, et al. Relationship between the Finnish diabetes risk score (FINDRISC), vitamin D levels, and insulin resistance in obese subjects. Prim Care Diabetes. (2017) 11:94–100. doi: 10.1016/j.pcd.2016.11.001
25. Atia, T, Abdelzaher, MH, Nassar, SA, Gafar, HH, Husseini, MAM, Kaabi, AMY, et al. Investigating the relationship between vitamin-D deficiency and glycemia status and lipid profile in nondiabetics and prediabetics in Saudi population. Medicine. (2023) 102:e36322. doi: 10.1097/MD.0000000000036322
26. Piccolo, BD, Hall, LM, Stephensen, CB, Gertz, ER, and van Loan, MD. Circulating 25-Hydroxyvitamin D concentrations in overweight and obese adults are explained by sun exposure, skin reflectance, and body composition. Curr Dev Nutr. (2019) 3:nzz065. doi: 10.1093/cdn/nzz065
27. Wang, H, Chen, W, Li, D, Yin, X, Zhang, X, Olsen, N, et al. Vitamin D and chronic diseases. Aging Dis. (2017) 8:346–53. doi: 10.14336/AD.2016.1021
Keywords: 25-hydroxy vitamin D, vitamin D deficiency, health care worker, obesity, type 2 diabetes
Citation: Villasis-Keever MA, Zurita-Cruz JN, Garduño-Espinosa J, López-Alarcón M, Barradas Vázquez AS, Miranda-Novales MG, Parra-Ortega I, López-Martinez B, García H and Klünder-Klünder M (2024) Factors associated with vitamin D deficiency in health care workers exposed to SARS-CoV-2: a cross-sectional study. Front. Nutr. 11:1440185. doi: 10.3389/fnut.2024.1440185
Edited by:
Francesca Gorini, National Research Council (CNR), ItalyReviewed by:
Antonio Neme, National Autonomous University of Mexico, MexicoCopyright © 2024 Villasis-Keever, Zurita-Cruz, Garduño-Espinosa, López-Alarcón, Barradas Vázquez, Miranda-Novales, Parra-Ortega, López-Martinez, García and Klünder-Klünder. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jessie Nallely Zurita-Cruz, enVyaXRham5AaG90bWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.