 Yiping Huang
Yiping Huang Wenyan Wang2
Wenyan Wang2 Jianxiang Jin
Jianxiang Jin
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Nutr. , 31 July 2024
Sec. Food Chemistry
Volume 11 - 2024 | https://doi.org/10.3389/fnut.2024.1428911
Background: The effect of polyphenol subclasses on prostate cancer (PCA) is controversial. Therefore, the purpose of this study was to investigate the relationship between polyphenol subclasses and PCA incidence.
Methods: From the establishment of the database to December 2023, a systematic search was conducted on PubMed, Web of Science, Embase, and Cochrane Library to identify relevant observational studies. The adjusted odds ratio (OR) and corresponding 95% confidence interval (95% CI) were used to assess the association.
Results: A total of 38 studies (11 were cohort studies and 27 were case–control studies), composing 824,933 participants, were included in this meta-analysis after excluding irrelevant records. The findings of the study revealed that men who consumed dietary polyphenols had a significantly higher risk of PCA compared to those who never or rarely consumed dietary polyphenols (OR = 1.01, p = 0.023), especially dietary flavonol (OR = 1.05, p = 0.042), flavanol (OR = 1.03, p = 0.026) and anthocyanin (OR = 1.06, p = 0.001). Neither total nor subclasses of dietary polyphenols have an effect on non-localized or high-grade PCA (OR = 1.01, p = 0.518). Dietary isoflavones tended to reduce the incidence of local or low-grade PCA, although there was no statistically significant difference (OR = 1.00, p = 0.081). Regarding serum/plasma polyphenol, total polyphenol (OR = 0.95, p = 0.002), genistein (OR = 0.92, p = 0.029) and enterolactone (OR = 0.92, p = 0.022) can reduce the incidence of PCA. No association was observed between total/subclasses of urinary polyphenols and PCA risk.
Conclusion: Polyphenols seem to generally increase the risk of PCA in the male population. The effect of polyphenols on PCA is affected by factors such as polyphenol subclasses, their forms (serum/plasma, urinary, dietary), and PCA-related factors (like PCA stage).
Systematic review registration: identifier: CRD42022322699.
Prostate cancer (PCA) is the most frequently diagnosed cancer among men in over half of the world’s countries and was the sixth leading cause of cancer mortality in 2020 (1). Nevertheless, the etiology of PCA has remained poorly understood compared to other common cancers (2). It is widely believed that both endogenous and exogenous factors may influence the occurrence of PCA. Established risk factors for PCA include advancing age (3), race (4), and a family history of PCA (5), all of which are non-modifiable. Numerous modifiable factors, such as smoking (6) and obesity (7), have also been implicated in the development of PCA. Among these factors, nutrition and lifestyle habits, which are more readily changeable, are considered potential avenues for effective cancer prevention strategies (8).
In recent years, Asian diets rich in plant polyphenols and estrogens, such as soybeans, have been associated with a reduced risk of PCA (9, 10). Polyphenols constitute a group of biologically active compounds widely distributed in plants and plant-based foods, including fruits, vegetables, tea leaves, coffee beans, wine, soybeans, lentils, and peanuts (11). They are primarily categorized into four subclasses: flavonoids (including isoflavones and coumestans), phenolic acids, lignans, and stilbenes (12). Among them, isoflavones and lignans have received the most attention in studies. Common isoflavones include daidzein, genistein, glycitein, formononetin, biochanin. Equol, a metabolite of daidzein produced by intestinal bacteria, has also been studied for its biological effects (13). Polyphenols can also be subdivided into many subclasses depending on the number of phenol units within their molecular structure, substituent groups, and the linkage type between phenol units (14).
Experimental studies (15, 16) conducted on cell lines and animal models (17, 18) have demonstrated that polyphenols possess antioxidative and anti-inflammatory effects. They can regulate androgen receptors and/or activate signaling pathway, induce cell cycle arrest and apoptosis, and inhibit the migratory and invasive capabilities of tumor cells. Consequently, they are expected to be used as chemo-preventive drugs for PCA (19). However, the evidence from epidemiological studies is still limited and vague. For example, (i) some studies [e.g., S. S. Strom et al. (20) and Yoshie Nagata et al. (21)] did not observe an association between polyphenol and PCA risk (p > 0.05); (ii) subgroup analyses of polyphenol subclasses, PCA stage, etc., showed a high degree of inconsistency across studies (22, 23); (iii) most published observational studies focus only on dietary isoflavones and lignans as polyphenols (24, 25), and the relationship between polyphenol content in serum or urine and PCA has shown inconsistent results. Hence, based on the aforementioned understanding, this study aims to conduct a systematic review and meta-analysis to examine the association between total/subclasses of polyphenols and PCA risk. Meanwhile, this study also hopes to help clinicians and public health personnel provide better prevention reference for the male population from the perspective of dietary habits.
This meta-analysis was conducted according to the Meta-Analysis of Observational Studies in Epidemiology (MOOSE) guidelines (26) and was registered on PROSPERO (CRD42024493149).
From the inception of the database until December 2023, a systematic search was conducted on electronic databases including PubMed, Web of Science, Embase, and the Cochrane Library to identify studies investigating the relationship between polyphenols and PCA risk. The search terms used were: “prostate cancer” and “polyphenol.” The following related terms were selected for the search: (“prostate cancer” OR “prostate neoplasm” OR “PCa” OR “prostatic carcinoma”) AND (“isoflavone” OR “daidzein” OR “genistein” OR “glycitein” OR “biochanin A” OR “formononetin” OR “flavonol” OR “flavanols” OR “flavones” OR “flavanones” OR “anthocyanins” OR “phytoestrogen” OR “polyphenol” OR “lignans” OR “equol” OR “enterolactone” OR “enterodiol” OR “flavonoids”). The reference lists of relevant articles were searched by 2 researchers to avoid omissions. When referring to duplicate literature, the original article was included if the study was published as an abstract and an original article. Also, if a study was continuously updated and reported, only the most recent or comprehensive articles were included. The population, intervention/exposure, comparison, outcome, and setting (PICOS) criteria were used to describe the research question.
Two researchers independently conducted a search to select studies from the database and reviewed the titles and abstracts of these articles to determine their eligibility for inclusion. When uncertainties arose, the full text was read or looked through for further selection. If necessary, authors are contacted to obtain additional information about their research. In instance of disagreement, discussions were held with a third researcher. When consensus could not be reached, the study was excluded.
Studies were considered for inclusion if they meet each of the following inclusion criteria: (i) the main exposure of the study was polyphenol and the outcome was a risk of PCA; (ii) a correlation between polyphenol and PCA risk was reported; (iii) the study provided usable outcome of polyphenol and PCA risk; (iv) the study is an observational study (cohort study, case–control study and cross-sectional study). At the same time, articles meeting one of the following exclusion criteria would be excluded: (i) the full text cannot be obtained; (ii) articles were not written in English; (iii) the study was conducted on PCA population and used mortality or recovery rate as the outcome; (iv) the study was published in duplicate; (v) the study had no reference value or control group.
The research data were extracted independently by two investigators, with disagreements arbitrated by a third researcher. The following information was extracted using a pre-determined data collection form: (i) authors; (ii) year of publication; (iii) country; (iv) research cohort; (v) study duration; (vi) follow-up period; (vii) number of PCA cases and participants; (viii) measurement tool; (ix) adjusting factors; (x) relevant data.
The quality of cohort and case–control studies was assessed based on the Newcastle-Ottawa Quality Assessment Scale (NOS), which consists of three quality parameters: selection (4 points), comparability (2 points) and outcomes (3 points). A score of 7 or above indicates high quality.
The primary purpose of this study was to explore the relationship between polyphenols and the incidence of PCA. The secondary purpose was to investigate the relationship between the incidence of PCA and polyphenol subclasses (e.g., isoflavones, daidzein, genistein), different forms of polyphenols and PCA (e.g., serum/plasma polyphenol, urinary polyphenol, dietary polyphenol), and the association between polyphenol and different PCA subtypes (e.g., advanced PCA, localized PCA). The results, after adjusting for relevant confounding factors were uniformly used for the analysis of the data from the included articles.
The Stata software version 12 (StataCorp, College Station, Texas, USA) was used to analyze the data. The study used odds ratio (OR) with 95% confidence intervals (95% CI) to evaluate the relationship between polyphenol and the incidence of PCA. The chi-square test was used to determine heterogeneity, with I2 values <30% indicating low heterogeneity, I2 values between 30 and 60% indicating moderate heterogeneity, and I2 values >60% indicating high heterogeneity. Due to the potential heterogeneity among the included studies, a random-effects model was used to improve the credibility of the results. When more than ten studies were included (27, 28), sensitivity analysis and a publication bias test were performed to evaluate the stability and reliability of the results. Publication bias was assessed using Begg’s test, and a two-tailed P-test was used to determine statistical significance, with a p-value of less than 0.05 considered statistically significant.
The established retrieval strategy from electronic databases yielded a total of 3,716 records. No additional articles were identified through other sources. After removing duplicates, 2,491 records remained. Subsequently, investigators eliminated 2,136 irrelevant publications after browsing their titles, abstracts, and keywords, leaving 355 articles for full-text review. Among these, 317 articles were eliminated due to reasons such as being non-observational studies (n = 144), duplicate publications (n = 86), not exploring the risk of PCA (n = 64), lack of available data for extraction (n = 18), and not being published in English (n = 5). As a result of these factors, 38 articles (13, 20–25, 29–59) comprising 824,933 participants met the inclusion criteria. Figure 1 shows the flow diagram of the selection of articles.
Figure 1. A schematic flow for the selection of articles included in this meta-analysis.
Each included observational study in this meta-analysis was assessed across 8 dimensions using the NOS checklist. In cohort studies, 90.9% were of high quality (NOS score ≥ 7), while in case–control studies, 92.6% were deemed high quality (NOS score ≥ 7). The assessment of risk of bias is recorded in Supplementary Tables S2, S3.
Of the 38 included studies, 11 were cohort studies (795,570 participants and 24,236 PCA cases) and 27 were case–control studies (29,363 controls and 12,888 PCA cases). All studies were published between 1999 and 2023, with follow-up times ranging from 3.5 to 17.3 years. Among them, 15 studies were conducted in Europe, 13 in Asia, and 10 in America. Regarding age at recruitment, 2 studies did not specify an upper age limit, 1 study did not set a lower age limit, and 1 study lacked accessible data. The median age for analysis ranged from 39.3 to 72.5 years, with data lacking in 5 studies. For data collection and evaluation of relevant exposure factors, 31 studies used questionnaires, 15 used blood samples, 4 used interviews, and 2 used urine samples. Additionally, 34.2% of the studies employed a combination of two methods for data evaluation. The adjustment for potential confounding factors varied among the studies, with common parameters including age, geographical area, physical activity, body mass index, family history of PCA, total energy intake, smoking, and alcohol consumption. Tables 1, 2 contain detailed characteristics of the included studies.
Table 1. Characteristics of included observational studies in the meta-analysis.
Table 2. Characteristics of included observational studies in the meta-analysis.
Twenty-seven studies recorded data on the risk of PCA associated with total intake of dietary polyphenols. The analysis indicated that men who consumed dietary polyphenols had a significantly higher risk of PCA than those who never or rarely consumed dietary polyphenol (OR = 1.01, p = 0.023) with moderate heterogeneity (I2 = 41.0%). In other words, dietary polyphenol intake was found to be harmful for the male population, increasing PCA risk. Additionally, cohort studies (OR = 1.01, p < 0.001) and case–control studies (OR = 1.01, p = 0.089) have consistently concluded that the consumption of dietary polyphenol increases the risk of PCA in men. The detailed data are contained in Table 3.
Table 3. Effects of dietary polyphenol subclasses on PCA incidence.
Different dietary polyphenol subclasses exhibit varying effects on PCA. The results indicated that dietary flavonol intake (OR = 1.05, p = 0.042), dietary flavanol intake (OR = 1.03, p = 0.026), and dietary anthocyanin intake (OR = 1.06, p = 0.001) were associated with an increased incidence of PCA, with statistically significant differences observed. However, dietary isoflavone (OR = 1.00, p = 0.818), genistein (OR = 0.98, p = 0.107), daidzein (OR = 1.00, p = 0.822), glycitein (OR = 0.98, p = 0.229), biochanin A (OR = 0.98, p = 0.592), formononetin (OR = 0.99, p = 0.641), coumestrol (OR = 0.97, p = 0.223), flavonoids (OR = 1.02, p = 0.082), flavone (OR = 1.02, p = 0.456), flavanone (OR = 1.01, p = 0.583), phytoestrogen (OR = 0.91, p = 0.084), lignan (OR = 0.96, p = 0.364) and other polyphenols (OR = 1.02, p = 0.626) did not show a significant effect on PCA, that was, these were not an observable risk factor for PCA in men. The detailed data are contained in Table 3.
For non-localized or high-grade PCA, data from 8 studies on the intake of dietary polyphenol subclasses and PCA risk were available. The analysis revealed that total dietary polyphenol intake had no effect on the occurrence of PCA (OR = 1.01, p = 0.518). Additionally, intake of all dietary polyphenol subclasses showed no significant relationship with PCA risk, including genistein (OR = 0.97, p = 0.565), daidzein (OR = 0.94, p = 0.287), glycitein (OR = 0.99, p = 0.867), isoflavone (OR = 1.07, p = 0.233), flavonoids (OR = 1.00, p = 0.861), flavonols (OR = 1.01, p = 0.728), flavanol (OR = 0.99, p = 0.618), flavones (OR = 1.01, p = 0.847), flavanones (OR = 1.01, p = 0.538), and anthocyanidins (OR = 1.01, p = 0.474). The detailed data are contained in Table 4.
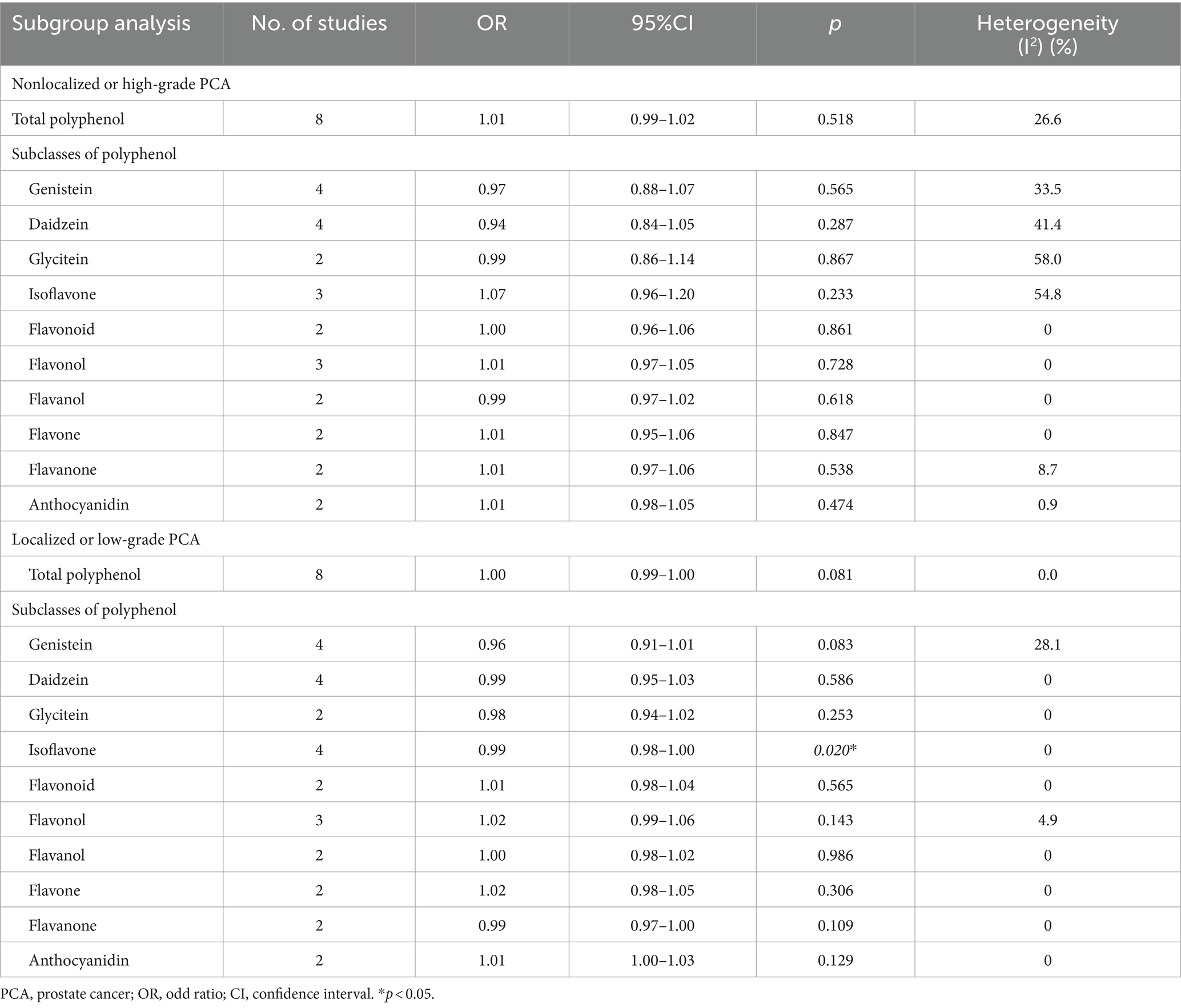
Table 4. Effects of dietary polyphenol subclasses on different PCA stage incidence.
For localized or low-grade PCA, data from 8 studies on the intake of dietary polyphenol subclasses and PCA risk were analyzed. The analysis showed that total dietary polyphenol had no effect on the occurrence of PCA (OR = 1.00, p = 0.081). Subgroup analysis revealed that dietary intake of genistein (OR = 0.96, p = 0.083), daidzein (OR = 0.99, p = 0.586), glycitein (OR = 0.98, p = 0.253), flavonoids (OR = 1.01, p = 0.565), flavonols (OR = 1.02, p = 0.143), flavanols (OR = 1.00, p = 0.986), flavones (OR = 1.02, p = 0.306), flavanones (OR = 0.99, p = 0.109), and anthocyanidins (OR = 1.01, p = 0.129) have no effect on PCA incidence, with slight heterogeneity. However, dietary isoflavone intake was found to reduce the incidence of PCA (OR = 0.99, p = 0.020), with statistically significant differences. The detailed data are contained in Table 4.
Fourteen studies investigated the effect of serum/plasma polyphenols on PCA risk and twelve studies provided data on serum/plasma polyphenol subclasses. The results indicate that total serum/plasma polyphenol can reduce the incidence of PCA in the male population (OR = 0.95, p = 0.002). Among them, serum/plasma genistein (OR = 0.92, p = 0.029) and enterolactone (OR = 0.92, p = 0.022) showed statistically significant protective effects against PCA, while serum/plasma daidzein (OR = 0.91, p = 0.053), glycitein (OR = 0.87, p = 0.095), equol (OR = 1.02, p = 0.733), and isoflavone (OR = 1.01, p = 0.708) has no significant effect on PCA. The detailed data are presented in Table 5.
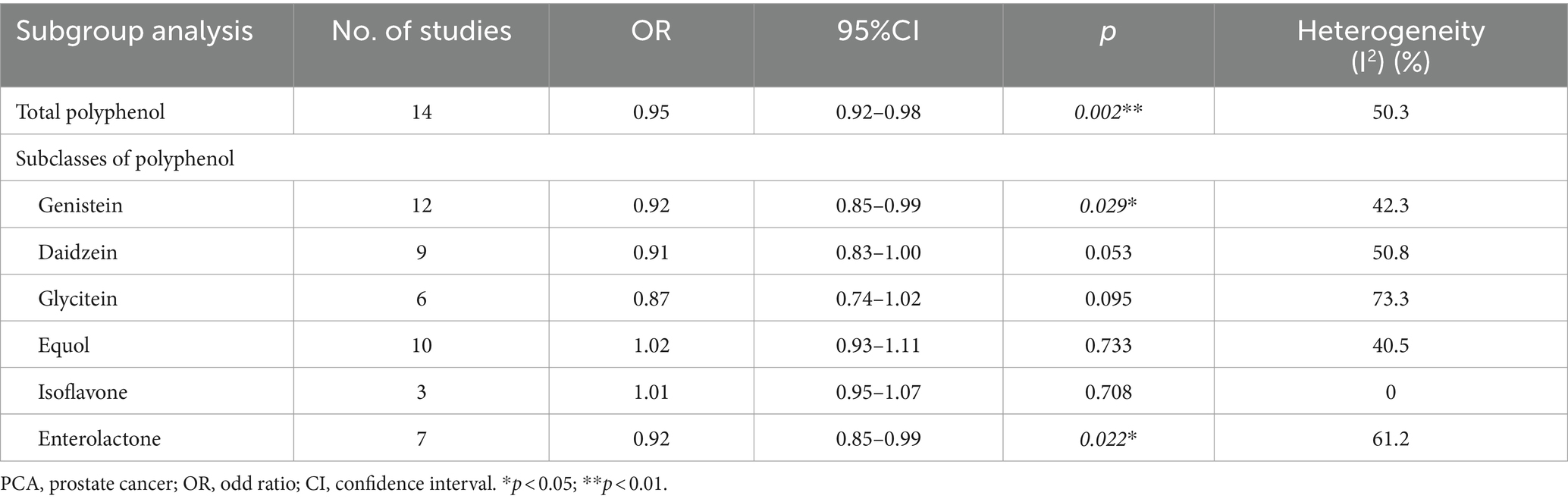
Table 5. Effects of serum/plasma polyphenol subclasses on PCA incidence.
Four studies explored the effect of urinary polyphenol on PCA risk, and detailed data on urinary polyphenol subclasses were available from four studies. The results showed that total urinary polyphenol had no significant influence on PCA risk (OR = 0.98, p = 0.184). Meanwhile, none of the urinary polyphenol subclasses demonstrated a significant effect on the occurrence of PCA in the male population, including genistein (OR = 0.97, p = 0.253), daidzein (OR = 0.99, p = 0.682), glycitein (OR = 1.00, p = 0.985), isoflavone (OR = 0.97, p = 0.523), enterolactone (OR = 0.97, p = 0.291), and equol (OR = 0.90, p = 0.406). The detailed data are contained in Table 6.
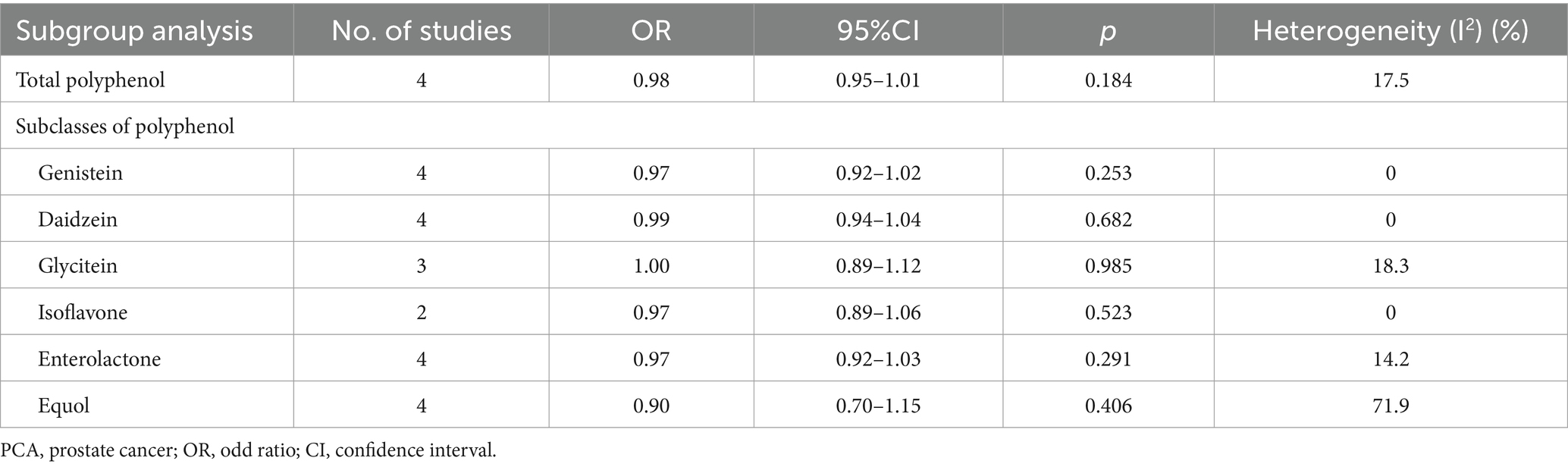
Table 6. Effects of urinary polyphenol subclasses on PCA incidence.
Begg’s test was used to estimate publication bias. The results of Begg’s test indicated the absence of publication bias among the included articles (p > 0.05). Sensitivity analysis was performed to assess whether individual studies affected the overall results. The results indicated that the analysis was relatively stable.
This study found that men who consumed dietary polyphenols had a significantly higher risk of PCA compared to those who never or rarely consumed dietary polyphenols, especially dietary flavonols, flavanols and anthocyanins. While total polyphenols and their subclasses did not show an effect on non-localized or high-grade PCA, dietary isoflavones were found to reduce the incidence of localized or low-grade PCA. For serum/plasma polyphenols, total polyphenol intake, as well as genistein and enterolactone, were associated with a reduced incidence of PCA. No significant association was observed between total or subclasses of urinary polyphenols and PCA risk.
Due to the diverse array of polyphenol types (60), there is no unified mechanism to explain the impact of polyphenol on the incidence of PCA. Researchers generally believe that polyphenols found in blood and urine originate from dietary intake, which mainly includes isoflavones, genistein, daidzein, glycitein, formononetin, and biochanin A, which are present in soy, soy-based foods and legumes (61, 62). The biological mechanisms underlying the effects of polyphenol on the human body have been proposed in the past decade. The prevailing perspective suggests that polyphenols exert their potential health effects due to their structural similarity to estrogen (63), which allows them to bind to estrogen receptors and produce both anti-estrogenic and estrogenic effects (55). Additionally, polyphenols can also induce significant cellular changes, particularly through the RAS-MAPK signaling pathways, which may promote the proliferation and metastasis of PCA cells (26). Consequently, polyphenols play various roles in gene regulation, cancer biology, and treatment (64).
According to previous studies, androgen levels significantly influence prostate health, and long-term exposure to androgens or increased cellular response to androgens is a key risk factor for PCA (65). Exogenous polyphenol intake can reduce testosterone production in the testes through a negative feedback mechanism, thereby exerting anti-androgenic effects (66). On the one hand, plant estrogens found in polyphenols can bind to a large number of estrogen receptors in prostate tissue, exerting an antagonistic effect on androgens, thereby regulating tumor cell proliferation and apoptosis, inhibiting angiogenesis and tumor metastasis (67, 68). On the other hand, the intake of flavonoids, a type of polyphenol that is not classified as phytoestrogens, may lead to disruptions in the human endocrine system and induce cellular stress (65, 69). Additionally, exogenous supplementation of phytoestrogens can alter hormone metabolism, potentially converting these hormones into androgens, which may lead to an increase in circulating androgens and reactive oxygen species, increasing the risk of the prostate cancer (70).
Researchers have not reached a unified conclusion on the balance and interaction between these two effects. However, the interplay of genetics, gene–environment interactions (such as race), and specific nutrient exposures can provoke diverse cellular effects, influencing PCA susceptibility (27, 71, 72). The varying degrees of impact observed across different studies can be attributed to background factors that influence the susceptibility of PCA through population-specific gene–environment interactions (73, 74). This may explain why our study found that consuming dietary polyphenols, flavanols, and anthocyanins increases the risk of PCA, while other studies (57, 75) have reported that dietary polyphenols may reduce the risk of PCA. Additionally, research indicates that as PCA progresses, mutations or epigenetic silencing of DNA repair genes in cancer cells can affect their sensitivity to hormone therapy, potentially leading to the progression of tumors from hormone-dependent to hormone-independent (76). This is a crucial issue in the management of advanced-stage cancer (77). This may explain why dietary polyphenol intake has a protective effect on localized or low-grade PCA, while its effect on non-localized or high-grade PCA is not significant.
Most serum/plasma and urinary polyphenols are metabolites of dietary polyphenols produced by gut microbiota, mainly including equol and enterolactone (78). The impact of these polyphenols on the human body is largely related to the polymorphisms associated with individual differences in gut microbiota and their effects on the formation of active metabolites (78, 79). Previous studies have suggested that the polyphenolic metabolite equol, being an estrogenic compound, may be more active than daidzein (80). However, due to individual differences, daidzein is only metabolized to form equol in a portion of the population. Similarly, lignans, a type of polyphenol, can only be converted into enterolactone and enterodiol by the gut microbiota in a portion of the population (63, 81). Different types of polyphenols exhibit distinct absorption and metabolic characteristics in the body. For example, flavonoid polyphenols may have higher bioavailability compared to phenolic acid polyphenols (14, 27). These differences in chemical composition might lead to variations between dietary polyphenols and serum/plasma polyphenol levels. Individual dietary habits, lifestyle choices, and health status also influence polyphenol absorption and metabolism. Factors such as smoking, alcohol consumption, exercise, and medication use can impact polyphenol metabolism and serum/plasma levels (23, 28, 29). Therefore, owing to the complexity of the human diet and the different confounding factors controlled for in various studies, we should be cautious about the conclusions drawn on the impact of polyphenol subclasses on PCA, as any bias may cause changes in the results. Further research is needed to explore how polyphenolic compounds interact with specific genes and how these interactions influence cancer risk and progression, particularly considering the potential differences in their effects among diverse populations.
Most published meta-analyses have predominantly focused on dietary isoflavones and equol in polyphenols and their effects on PCA, while neglecting to explore the relationship between other polyphenol subclasses and polyphenol levels in serum and urine with PCA. Studies such as Yukiko Sugiyama et al. (82) and Catherine C. Applegate et al. (83) may have consequently overestimated their findings and lacked reliability due to this narrow focus. In addition, Jinjing He et al.’s study (84) investigated the relationship between phytoestrogens and PCA risk, but only included isoflavones, genistein, daidzein, and ligans, without further extraction and analysis of the impact of other polyphenol subclasses on PCA risk. Therefore, caution should be exercised when drawing conclusions due to incomplete data extraction and a lack of consistency among the included studies.
Although this meta-analysis provides comprehensive and objective conclusions, it is important to acknowledge several potential limitations. First, variations in study design, study population, sample size, risk assessments, and adjustments for related confounding factors among the included studies may introduce bias and reduce the confidence of the conclusions. To address this, a random-effects model was utilized to evaluate the effect of polyphenols on PCA. Additionally, significant heterogeneity exists in the lifestyle habits and geographical locations of the study population. To mitigate this, relevant data were selected for statistical analysis, and adjustments were made for a maximum number of potential confounding factors to enhance the accuracy of the conclusions. Second, although most studies utilized questionnaires and blood samples to assess polyphenol intake, accurately measuring the specific intake of compounds remains challenging, and deviations in intake assessment may have occurred during data collection. Third, not all trials provided subgroup data, such as data on PCA type and intake subgroups, making it difficult to conduct certain subgroup analyses. Therefore, large-scale observational studies are needed to further validate the relevant conclusions.
Despite its limitations, this meta-analysis possesses several strengths. Firstly, to our knowledge, this study is the first meta-analysis to categorize extracted data by different forms of polyphenols or polyphenol subclasses (dietary, blood, and urine) and to perform subgroup analyses to comprehensively explore the potential effect of total polyphenols and their subclasses on different types of PCA. Secondly, this study included a large number of observational studies, encompassing over 800,000 participants across Europe, Asia, and America. The large observational population increases the reliability and validity of the conclusions of this study. In summary, this meta-analysis provides meaningful insights that may offer a new reference for PCA prevention in the male population.
From the perspective of clinical dietary recommendations, this study suggests that for healthy men, clinicians or nutritionists might consider appropriately reducing the recommendation of foods rich in polyphenols, especially those high in flavanols, flavones, and anthocyanins, such as onions, berries, and kale. For patients with early-stage or localized prostate cancer, this study suggests that clinicians or nutritionists might recommend foods rich in isoflavones, such as soybeans, chickpeas, and kudzu root. However, current research does not provide specific recommended intake levels for different populations. Future clinical studies with larger sample sizes and detailed data are needed to further explore the relationship between polyphenols and prostate cancer.
This study identified that men who consumed dietary polyphenols had a significantly higher risk of PCA compared to those who rarely or never consumed them, particularly with respect to dietary flavonols, flavanols, and anthocyanins. However, neither total dietary polyphenols nor their subclasses showed an effect on non-localized or high-grade PCA, while dietary isoflavones appeared to reduce the incidence of localized or low-grade PCA. Regarding serum/plasma polyphenols, total polyphenols, genistein, and enterolactone demonstrated potential in reducing the incidence of PCA. Conversely, no association was observed between total or subclass urinary polyphenols and PCA risk. Considering these limitations, further large-scale prospective cohort studies are warranted to validate these findings.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
YH: Data curation, Writing – original draft, Writing – review & editing. WW: Data curation, Investigation, Methodology, Resources, Writing – review & editing. JJ: Software, Validation, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2024.1428911/full#supplementary-material
PCA, Prostate cancer; MOOSE, The meta-analysis of observational studies in epidemiology; PICOS, The population, intervention, comparison, outcome and setting criteria; NOS, Newcastle-Ottawa quality assessment scale checklist; OR, Odds ratio; CI, Confidence interval
1. Sung, H, Ferlay, J, Siegel, RL, Laversanne, M, Soerjomataram, I, Jemal, A, et al. Global Cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660
2. He, H, Xie, B, and Xie, L. Male pattern baldness and incidence of prostate cancer: a systematic review and meta-analysis. Medicine (Baltimore). (2018) 97:e11379. doi: 10.1097/MD.0000000000011379
3. Vietri, MT, D'Elia, G, Caliendo, G, Resse, M, Casamassimi, A, Passariello, L, et al. Hereditary prostate Cancer: genes related, target therapy and prevention. Int J Mol Sci. (2021) 22:3753. doi: 10.3390/ijms22073753
4. Siegel, DA, O'Neil, ME, Richards, TB, Dowling, NF, and Weir, HK. Prostate cancer incidence and survival, by stage and race/ethnicity-United States, 2001–2017. MMWR Morb Mortal Wkly Rep. (2020) 69:1473–80. doi: 10.15585/mmwr.mm6941a1
5. Barber, L, Gerke, T, Markt, SC, Peisch, SF, Wilson, KM, Ahearn, T, et al. Family history of breast or prostate Cancer and prostate Cancer risk. Clin Cancer Res. (2018) 24:5910–7. doi: 10.1158/1078-0432.CCR-18-0370
6. Jochems, SHJ, Fritz, J, Häggström, C, Järvholm, B, Stattin, P, and Stocks, T. Smoking and risk of prostate Cancer and prostate Cancer death: a pooled study. Eur Urol. (2023) 83:422–31. doi: 10.1016/j.eururo.2022.03.033
7. Saha, A, Kolonin, MG, and DiGiovanni, J. Obesity and prostate cancer – microenvironmental roles of adipose tissue. Nat Rev Urol. (2023) 20:579–96. doi: 10.1038/s41585-023-00764-9
8. Ballon-Landa, E, and Parsons, JK. Nutrition, physical activity, and lifestyle factors in prostate cancer prevention. Curr Opin Urol. (2018) 28:55–61. doi: 10.1097/MOU.0000000000000460
9. Perdana, NR, Mochtar, CA, Umbas, R, and Hamid, AR. The risk factors of prostate Cancer and its prevention: a literature review. Acta Med Indones. (2016) 48:228–38. doi: 10.3389/fonc.2023.1203791
10. Ajdžanovic, V, Filipovic, B, Miljic, D, Mijatovic, S, Maksimovic-Ivanic, D, Miler, M, et al. Prostate cancer metastasis and soy isoflavones: a dogfight over a bone. EXCLI J. (2019) 18:106–26. doi: 10.17179/excli2018-1836
11. Pérez-Jiménez, J, Neveu, V, Vos, F, and Scalbert, A. Identification of the 100 richest dietary sources of polyphenols: an application of the phenol-explorer database. Eur J Clin Nutr. (2010) 64:S112–20. doi: 10.1038/ejcn.2010.221
12. Durazzo, A, Lucarini, M, Souto, EB, Cicala, C, Caiazzo, E, Izzo, AA, et al. Polyphenols: a concise overview on the chemistry, occurrence, and human health. Phytother Res. (2019) 33:2221–43. doi: 10.1002/ptr.6419
13. Reger, MK, Zollinger, TW, Liu, Z, Jones, JF, and Zhang, J. Dietary intake of isoflavones and coumestrol and the risk of prostate cancer in the prostate, lung, colorectal and ovarian Cancer screening trial. Int J Cancer. (2018) 142:719–28. doi: 10.1002/ijc.31095
14. Di Lorenzo, C, Colombo, F, Biella, S, Stockley, C, and Restani, P. Polyphenols and human health: the role of bioavailability. Nutrients. (2021) 13:273. doi: 10.3390/nu13010273
15. Costea, T, Nagy, P, Ganea, C, Szöllősi, J, and Mocanu, MM. Molecular mechanisms and bioavailability of polyphenols in prostate Cancer. Int J Mol Sci. (2019) 20:1062. doi: 10.3390/ijms20051062
16. Stewart, KL, and Lephart, ED. Overview of BPH: symptom relief with dietary polyphenols, vitamins and phytochemicals by nutraceutical supplements with implications to the prostate microbiome. Int J Mol Sci. (2023) 24:5486. doi: 10.3390/ijms24065486
17. Pejčić, T, Tosti, T, Džamić, Z, Gašić, U, Vuksanović, A, Dolićanin, Z, et al. The polyphenols as potential agents in prevention and therapy of prostate diseases. Molecules. (2019) 24:3982. doi: 10.3390/molecules24213982
18. Lall, RK, Syed, DN, Adhami, VM, Khan, MI, and Mukhtar, H. Dietary polyphenols in prevention and treatment of prostate cancer. Int J Mol Sci. (2015) 16:3350–76. doi: 10.3390/ijms16023350
19. Ahmad, N, Qamar, M, Yuan, Y, Nazir, Y, Wilairatana, P, and Mubarak, MS. Dietary polyphenols: extraction, identification, bioavailability, and role for prevention and treatment of colorectal and prostate cancers. Molecules. (2022) 27:2831. doi: 10.3390/molecules27092831
20. Strom, SS, Yamamura, Y, Duphorne, CM, Spitz, MR, Babaian, RJ, Pillow, PC, et al. Phytoestrogen intake and prostate cancer: a case-control study using a new database. Nutr Cancer. (1999) 33:20–5.
21. Nagata, Y, Sugiyama, Y, Fukuta, F, Takayanagi, A, Masumori, N, Tsukamoto, T, et al. Relationship of serum levels and dietary intake of isoflavone, and the novel bacterium Slackia sp. strain NATTS with the risk of prostate cancer: a case-control study among Japanese men. Int Urol Nephrol. (2016) 48:1453–60. doi: 10.1007/s11255-016-1335-7
22. Kurahashi, N, Iwasaki, M, Sasazuki, S, Otani, T, Inoue, M, and Tsugane, S. Soy product and isoflavone consumption in relation to prostate cancer in Japanese men. Cancer Epidemiol Biomarkers Prev. (2007) 16:538–45. doi: 10.1158/1055-9965.EPI-06-0517
23. Wang, Y, Stevens, VL, Shah, R, Peterson, JJ, Dwyer, JT, Gapstur, SM, et al. Dietary flavonoid and proanthocyanidin intakes and prostate cancer risk in a prospective cohort of US men. Am J Epidemiol. (2014) 179:974–86. doi: 10.1093/aje/kwu006
24. Geybels, MS, Verhage, BA, Arts, IC, van Schooten, FJ, Goldbohm, RA, and van den Brandt, PA. Dietary flavonoid intake, black tea consumption, and risk of overall and advanced stage prostate cancer. Am J Epidemiol. (2013) 177:1388–98. doi: 10.1093/aje/kws419
25. Sawada, N. Risk and preventive factors for prostate cancer in Japan: the Japan public health center-based prospective (JPHC) study. J Epidemiol. (2017) 27:2–7. doi: 10.1016/j.je.2016.09.001
26. Stroup, DF, Berlin, JA, Morton, SC, Olkin, I, Williamson, GD, Rennie, D, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. JAMA. (2000) 283:2008–12. doi: 10.1001/jama.283.15.2008
27. Li, S, Gu, L, Shen, Z, Mao, D, Khadaroo, PA, and Su, H. A meta-analysis of comparison of proximal gastrectomy with double-tract reconstruction and total gastrectomy for proximal early gastric cancer. BMC Surg. (2019) 19:117. doi: 10.1186/s12893-019-0584-7
28. Gu, L, Huang, X, Li, S, Mao, D, Shen, Z, Khadaroo, PA, et al. A meta-analysis of the medium-and long-term effects of laparoscopic sleeve gastrectomy and laparoscopic roux-en-Y gastric bypass. BMC Surg. (2020) 20:30. doi: 10.1186/s12893-020-00695-x
29. Knekt, P, Kumpulainen, J, Järvinen, R, Rissanen, H, Heliövaara, M, Reunanen, A, et al. Flavonoid intake and risk of chronic diseases. Am J Clin Nutr. (2002) 76:560–8. doi: 10.1093/ajcn/76.3.560
30. Greenlee, H, White, E, Patterson, RE, and Kristal, AR. Supplement use among cancer survivors in the vitamins and lifestyle (VITAL) study cohort. J Altern Complement Med. (2004) 10:660–6. doi: 10.1089/acm.2004.10.660
31. Mursu, J, Nurmi, T, Tuomainen, TP, Salonen, JT, Pukkala, E, and Voutilainen, S. Intake of flavonoids and risk of cancer in Finnish men: the Kuopio Ischaemic heart disease risk factor study. Int J Cancer. (2008) 123:660–3. doi: 10.1002/ijc.23421
32. Park, SY, Murphy, SP, Wilkens, LR, Henderson, BE, and Kolonel, LN. Legume and isoflavone intake and prostate cancer risk: the multiethnic cohort study. Int J Cancer. (2008) 123:927–32. doi: 10.1002/ijc.23594
33. Sawada, N, Iwasaki, M, Yamaji, T, Shimazu, T, Inoue, M, and Tsugane, S. Soy and isoflavone consumption and subsequent risk of prostate cancer mortality: the Japan public health center-based prospective study. Int J Epidemiol. (2020) 49:1553–61. doi: 10.1093/ije/dyaa177
34. Almanza-Aguilera, E, Guiñón-Fort, D, Perez-Cornago, A, Martínez-Huélamo, M, Andrés-Lacueva, C, Tjønneland, A, et al. Intake of the Total, classes, and subclasses of (poly) phenols and risk of prostate Cancer: a prospective analysis of the EPIC study. Cancers (Basel). (2023) 15:4067. doi: 10.3390/cancers15164067
35. Kolonel, LN, Hankin, JH, Whittemore, AS, Wu, AH, Gallagher, RP, Wilkens, LR, et al. Vegetables, fruits, legumes and prostate cancer: a multiethnic case-control study. Cancer Epidemiol Biomarkers Prev. (2000) 9:795–804.
36. Stattin, P, Adlercreutz, H, Tenkanen, L, Jellum, E, Lumme, S, Hallmans, G, et al. Circulating enterolactone and prostate cancer risk: a Nordic nested case-control study. Int J Cancer. (2002) 99:124–9. doi: 10.1002/ijc.10313
37. Lee, MM, Gomez, SL, Chang, JS, Wey, M, Wang, RT, and Hsing, AW. Soy and isoflavone consumption in relation to prostate cancer risk in China. Cancer Epidemiol Biomarkers Prev. (2003) 12:665–8.
38. Ozasa, K, Nakao, M, Watanabe, Y, Hayashi, K, Miki, T, Mikami, K, et al. Serum phytoestrogens and prostate cancer risk in a nested case-control study among Japanese men. Cancer Sci. (2004) 95:65–71. doi: 10.1111/j.1349-7006.2004.tb03172.x
39. McCann, SE, Ambrosone, CB, Moysich, KB, Brasure, J, Marshall, JR, Freudenheim, JL, et al. Intakes of selected nutrients, foods, and phytochemicals and prostate cancer risk in western New York. Nutr Cancer. (2005) 53:33–41. doi: 10.1207/s15327914nc5301_4
40. Hedelin, M, Klint, A, Chang, ET, Bellocco, R, Johansson, JE, Andersson, SO, et al. Dietary phytoestrogen, serum enterolactone and risk of prostate cancer: the cancer prostate Sweden study (Sweden). Cancer Causes Control. (2006) 17:169–80. doi: 10.1007/s10552-005-0342-2
41. Low, YL, Taylor, JI, Grace, PB, Mulligan, AA, Welch, AA, Scollen, S, et al. Phytoestrogen exposure, polymorphisms in COMT, CYP19, ESR1, and SHBG genes, and their associations with prostate cancer risk. Nutr Cancer. (2006) 56:31–9. doi: 10.1207/s15327914nc5601_5
42. Heald, CL, Ritchie, MR, Bolton-Smith, C, Morton, MS, and Alexander, FE. Phyto-oestrogens and risk of prostate cancer in Scottish men. Br J Nutr. (2007) 98:388–96. doi: 10.1017/S0007114507700703
43. Bosetti, C, Bravi, F, Talamini, R, Parpinel, M, Gnagnarella, P, Negri, E, et al. Flavonoids and prostate cancer risk: a study in Italy. Nutr Cancer. (2006) 56:123–7. doi: 10.1207/s15327914nc5602_1
44. Nagata, Y, Sonoda, T, Mori, M, Miyanaga, N, Okumura, K, Goto, K, et al. Dietary isoflavones may protect against prostate cancer in Japanese men. J Nutr. (2007) 137:1974–9. doi: 10.1093/jn/137.8.1974
45. Ward, H, Chapelais, G, Kuhnle, GG, Luben, R, Khaw, KT, and Bingham, S. Lack of prospective associations between plasma and urinary phytoestrogens and risk of prostate or colorectal cancer in the European prospective into Cancer-Norfolk study. Cancer Epidemiol Biomarkers Prev. (2008) 17:2891–4. doi: 10.1158/1055-9965.EPI-08-0335
46. Kurahashi, N, Iwasaki, M, Inoue, M, Sasazuki, S, and Tsugane, S. Plasma isoflavones and subsequent risk of prostate cancer in a nested case-control study: the Japan public health center. J Clin Oncol. (2008) 26:5923–9. doi: 10.1200/JCO.2008.16.8807
47. Lewis, JE, Soler-Vilá, H, Clark, PE, Kresty, LA, Allen, GO, and Hu, JJ. Intake of plant foods and associated nutrients in prostate cancer risk. Nutr Cancer. (2009) 61:216–24. doi: 10.1080/01635580802419756
48. Travis, RC, Spencer, EA, Allen, NE, Appleby, PN, Roddam, AW, Overvad, K, et al. Plasma phyto-oestrogens and prostate cancer in the European prospective investigation into Cancer and nutrition. Br J Cancer. (2009) 100:1817–23. doi: 10.1038/sj.bjc.6605073
49. Park, SY, Wilkens, LR, Franke, AA, Le Marchand, L, Kakazu, KK, Goodman, MT, et al. Urinary phytoestrogen excretion and prostate cancer risk: a nested case-control study in the multiethnic cohort. Br J Cancer. (2009) 101:185–91. doi: 10.1038/sj.bjc.6605137
50. Ward, HA, Kuhnle, GG, Mulligan, AA, Lentjes, MA, Luben, RN, and Khaw, KT. Breast, colorectal, and prostate cancer risk in the European prospective investigation into Cancer and nutrition-Norfolk in relation to phytoestrogen intake derived from an improved database. Am J Clin Nutr. (2010) 91:440–8. doi: 10.3945/ajcn.2009.28282
51. Jackson, MD, McFarlane-Anderson, ND, Simon, GA, Bennett, FI, and Walker, SP. Urinary phytoestrogens and risk of prostate cancer in Jamaican men. Cancer Causes Control. (2010) 21:2249–57. doi: 10.1007/s10552-010-9648-9
52. Sawada, N, Iwasaki, M, Inoue, M, Sasazuki, S, Yamaji, T, Shimazu, T, et al. Plasma testosterone and sex hormone-binding globulin concentrations and the risk of prostate cancer among Japanese men: a nested case-control study. Cancer Sci. (2010) 101:2652–7. doi: 10.1111/j.1349-7006.2010.01721.x
53. Travis, RC, Allen, NE, Appleby, PN, Price, A, Kaaks, R, Chang-Claude, J, et al. Prediagnostic concentrations of plasma genistein and prostate cancer risk in 1,605 men with prostate cancer and 1,697 matched control participants in EPIC. Cancer Causes Control. (2012) 23:1163–71. doi: 10.1007/s10552-012-9985-y
54. Sugiyama, Y, Nagata, Y, Fukuta, F, Takayanagi, A, Masumori, N, Tsukamoto, T, et al. Counts of Slackia sp. strain NATTS in intestinal flora are correlated to serum concentrations of equol both in prostate cancer cases and controls in Japanese men. Asian Pac J Cancer Prev. (2014) 15:2693–7. doi: 10.7314/APJCP.2014.15.6.2693
55. Wu, Y, Zhang, L, Na, R, Xu, J, Xiong, Z, Zhang, N, et al. Plasma genistein and risk of prostate cancer in Chinese population. Int Urol Nephrol. (2015) 47:965–70. doi: 10.1007/s11255-015-0981-5
56. Russo, GI, Di Mauro, M, Regis, F, Reale, G, Campisi, D, Marranzano, M, et al. Association between dietary phytoestrogens intakes and prostate cancer risk in Sicily. Aging Male. (2018) 21:48–54. doi: 10.1080/13685538.2017.1365834
57. Reale, G, Russo, GI, Di Mauro, M, Regis, F, Campisi, D, Giudice, AL, et al. Association between dietary flavonoids intake and prostate cancer risk: a case-control study in Sicily. Complement Ther Med. (2018) 39:14–8. doi: 10.1016/j.ctim.2018.05.002
58. Ghanavati, M, Clark, CCT, Bahrami, A, Teymoori, F, Movahed, M, Sohrab, G, et al. Dietary intake of polyphenols and total antioxidant capacity and risk of prostate cancer: a case-control study in Iranian men. Eur J Cancer Care. (2021) 30:e13364. doi: 10.1111/ecc.13364
59. Galván-Portillo, M, Vázquez-Salas, RA, Hernández-Pérez, JG, Blanco-Muñoz, J, López-Carrillo, L, and Torres-Sánchez, L. Dietary flavonoid patterns and prostate cancer: evidence from a Mexican population-based case-control study. Br J Nutr. (2021) 127:1695–1703. doi: 10.1017/S0007114521002646
60. Adjakly, M, Ngollo, M, Dagdemir, A, Judes, G, Pajon, A, Karsli-Ceppioglu, S, et al. Prostate cancer: the main risk and protective factors-epigenetic modifications. Ann Endocrinol (Paris). (2015) 76:25–41. doi: 10.1016/j.ando.2014.09.001
61. Ganry, O. Phytoestrogens and prostate cancer risk. Prev Med. (2005) 41:1–6. doi: 10.1016/j.ypmed.2004.10.022
62. Hedelin, M, Bälter, KA, Chang, ET, Bellocco, R, Klint, A, Johansson, JE, et al. Dietary intake of phytoestrogens, estrogen receptor-beta polymorphisms and the risk of prostate cancer. Prostate. (2006) 66:1512–20. doi: 10.1002/pros.20487
63. Zhang, HY, Cui, J, Zhang, Y, Wang, ZL, Chong, T, and Wang, ZM. Isoflavones and prostate Cancer: a review of some critical issues. Chin Med J. (2016) 129:341–7. doi: 10.4103/0366-6999.174488
64. Sohel, M, Sultana, H, Sultana, T, Mamun, AA, Amin, MN, Hossain, MA, et al. Chemotherapeutic activities of dietary phytoestrogens against prostate Cancer: from observational to clinical studies. Curr Pharm Des. (2022) 28:1561–80. doi: 10.2174/1381612828666220601153426
65. Mahmoud, AM, Yang, W, and Bosland, MC. Soy isoflavones and prostate cancer: a review of molecular mechanisms. J Steroid Biochem Mol Biol. (2014) 140:116–32. doi: 10.1016/j.jsbmb.2013.12.010
66. Rizzo, J, Min, M, Adnan, S, Afzal, N, Maloh, J, Chambers, CJ, et al. Soy protein containing Isoflavones improves facial signs of Photoaging and skin hydration in postmenopausal women: results of a prospective randomized double-blind controlled trial. Nutrients. (2023) 15:4113. doi: 10.3390/nu15194113
67. Canivenc-Lavier, MC, and Bennetau-Pelissero, C. Phytoestrogens and health effects. Nutrients. (2023) 15:317. doi: 10.3390/nu15020317
68. Vitale, DC, Piazza, C, Melilli, B, Drago, F, and Salomone, S. Isoflavones: estrogenic activity, biological effect and bioavailability. Eur J Drug Metab Pharmacokinet. (2013) 38:15–25. doi: 10.1007/s13318-012-0112-y
69. Jungbauer, A, and Medjakovic, S. Phytoestrogens and the metabolic syndrome. J Steroid Biochem Mol Biol. (2014) 139:277–89. doi: 10.1016/j.jsbmb.2012.12.009
70. Ramírez-de-Arellano, A, Pereira-Suárez, AL, Rico-Fuentes, C, López-Pulido, EI, Villegas-Pineda, JC, and Sierra-Diaz, E. Distribution and effects of estrogen receptors in prostate Cancer: associated molecular mechanisms. Front Endocrinol. (2021) 12:811578. doi: 10.3389/fendo.2021.811578
71. Mateo, J, Carreira, S, Sandhu, S, Miranda, S, Mossop, H, Perez-Lopez, R, et al. DNA-repair defects and Olaparib in metastatic prostate Cancer. N Engl J Med. (2015) 373:1697–708. doi: 10.1056/NEJMoa1506859
72. Parker, C, Castro, E, Fizazi, K, Heidenreich, A, Ost, P, Procopio, G, et al. Prostate cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. (2020) 31:1119–34. doi: 10.1016/j.annonc.2020.06.011
73. Rebbeck, TR. Prostate Cancer genetics: variation by race, ethnicity, and geography. Semin Radiat Oncol. (2017) 27:3–10. doi: 10.1016/j.semradonc.2016.08.002
74. Messina, M. Soy and health update: evaluation of the clinical and epidemiologic literature. Nutrients. (2016) 8:754. doi: 10.3390/nu8120754
75. Porter, MP, Stanford, JL, and Lange, PH. The distribution of serum prostate-specific antigen levels among American men: implications for prostate cancer prevalence and screening. Prostate. (2006) 66:1044–51. doi: 10.1002/pros.20417
76. Carruba, G. Estrogen and prostate cancer: an eclipsed truth in an androgen-dominated scenario. J Cell Biochem. (2007) 102:899–911. doi: 10.1002/jcb.21529
77. Nakai, S, Fujita, M, and Kamei, Y. Health promotion effects of soy Isoflavones. J Nutr Sci Vitaminol (Tokyo). (2020) 66:502–7. doi: 10.3177/jnsv.66.502
78. Wang, Q, Li, H, Tao, P, Wang, YP, Yuan, P, Yang, CX, et al. Soy isoflavones, CYP1A1, CYP1B1, and COMT polymorphisms, and breast cancer: a case-control study in southwestern China. DNA Cell Biol. (2011) 30:585–95. doi: 10.1089/dna.2010.1195
79. Daily, JW, Ko, BS, Ryuk, J, Liu, M, Zhang, W, and Park, S. Equol decreases hot flashes in postmenopausal women: a systematic review and Meta-analysis of randomized clinical trials. J Med Food. (2019) 22:127–39. doi: 10.1089/jmf.2018.4265
80. Hullar, MA, Lancaster, SM, Li, F, Tseng, E, Beer, K, Atkinson, C, et al. Enterolignan-producing phenotypes are associated with increased gut microbial diversity and altered composition in premenopausal women in the United States. Cancer Epidemiol Biomarkers Prev. (2015) 24:546–54. doi: 10.1158/1055-9965.EPI-14-0262
81. Corona, G, Kreimes, A, Barone, M, Turroni, S, Brigidi, P, Keleszade, E, et al. Impact of lignans in oilseed mix on gut microbiome composition and enterolignan production in younger healthy and premenopausal women: an in vitro pilot study. Microb Cell Factories. (2020) 19:82. doi: 10.1186/s12934-020-01341-0
82. Sugiyama, Y, Masumori, N, Fukuta, F, Yoneta, A, Hida, T, Yamashita, T, et al. Influence of isoflavone intake and equol-producing intestinal flora on prostate cancer risk. Asian Pac J Cancer Prev. (2013) 14:1–4. doi: 10.7314/APJCP.2013.14.1.1
83. Applegate, CC, Rowles, JL, Ranard, KM, Jeon, S, and Erdman, JW. Soy consumption and the risk of prostate Cancer: an updated systematic review and Meta-analysis. Nutrients. (2018) 10:40. doi: 10.3390/nu10010040
Keywords: prostate cancer, polyphenol subclasses, phytoestrogen, risk assessment, meta-analysis
Citation: Huang Y, Wang W and Jin J (2024) Association between polyphenol subclasses and prostate cancer: a systematic review and meta-analysis of observational studies. Front. Nutr. 11:1428911. doi: 10.3389/fnut.2024.1428911
Edited by:
Hock Eng Khoo, Guilin University of Technology, ChinaReviewed by:
Shi-Hui Cheng, University of Nottingham Malaysia Campus, MalaysiaCopyright © 2024 Huang, Wang and Jin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jianxiang Jin, amhqanhpYW5nQHRvbS5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.