
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr. , 11 November 2024
Sec. Nutritional Epidemiology
Volume 11 - 2024 | https://doi.org/10.3389/fnut.2024.1423658
 Živa Lavriša1,2*
Živa Lavriša1,2* Igor Pravst1,2,3
Igor Pravst1,2,3 Sanja Krušič1
Sanja Krušič1 Neža Hren1
Neža Hren1 Nadan Gregorič4,5
Nadan Gregorič4,5 Irena Hren6
Irena Hren6 Barbara Koroušić Seljak7
Barbara Koroušić Seljak7 Hristo Hristov1,8
Hristo Hristov1,8Background: Older adults living in nursing homes (NHs) are considered a vulnerable population in terms of nutrition. The aim of the present study was to explore the usual intake of energy, macronutrients, and specific food groups, along with offers in the NH menus on a nationally representative sample of Slovenian NH residents and compare dietary patterns with the established recommendations.
Methods: The study was conducted as part of a cross-sectional NutriCare study on 317 residents (65–101 years) from 20 Slovenian NHs in 9 health regions. Relatively independent residents were selected using quota sampling by sex and age. Data collection involved interviews and anthropometric measurements. Usual dietary intake was assessed by a multiple-source method from two 24-h dietary recalls and food frequency questionnaires. Adherence of dietary intake to the recommendations and dietary composition of NH menus were assessed. The Mini Nutritional Assessment (MNA) was used to explore nutritional status.
Results: Notable variability in energy and macronutrient intakes was observed with some participants showing intakes below and others above the recommended values. A high prevalence of BMI > 30 kg/m2 was observed in 39% of participants, indicating potential discrepancies between total energy intake and expenditure. The usual intake of fat was 36% of total energy intake (TEI). The intake of foods of animal origin exceeded dietary guidelines. Intake of carbohydrates (46% TEI in men and 47% TEI in women) as well as dietary fibre (20 g/day for both sexes) was below recommendations. A scarce intake of fruits, vegetables, and cereals was observed. In total, 40% of men and 35% of women had usual daily protein intakes lower than 1 g/kg of body weight. The protein content of breakfast and dinner could be improved. NH residents consumed little food from outside NH. The usual nutrient and food group intakes of residents reflected the NH menu offers.
Conclusion: The study results on the usual intake of energy, macronutrients, specific food groups, and offers in the NH menus indicate the potential for optimisation. According to the World Health Organisation, the prevalence of BMI > 30 kg/m2 is notable and warrants attention. Careful meal planning and regular monitoring of the nutritional status of NH residents should be considered.
The global trend of an ageing population reflects a major demographic shift, characterized by an unprecedented increase in the proportion of older individuals. Addressing the needs of this population is crucial for the future overall wellbeing of society and assuring the quality of life in older years. The World Health Organisation (WHO) predicts that by 2050, the proportion of older adults, 12% of the global population in 2015, will nearly double (1). Along with these predictions, studies aiming at understanding the nutritional status of this population have gained additional focus recently.
In terms of nutrition, older adults are being recognised as a vulnerable population group, with institutionalised individuals being particularly exposed (2). An adequate intake of essential nutrients and physical activity play a major role in maintaining health of the older adults (3). Insufficient intake of nutrients increases the risk of developing health complications and loss of independence (4). The term “malnutrition” describes a lack of proper nutrition, which refers to energy, macronutrient, and micronutrient deficiencies, as well as excesses or imbalances (5). Studies report high rates of malnutrition among institutionalised older adults, which include nursing home (NH) residents (6, 7). However, the demographic structure of NH residents can vary notably. In Slovenia, for example, the structure of NH residents ranges from bed-bound, very ill, with mobility or cognitive impairment to those who are relatively independent, with low-level care requirements, who are characteristically closer to community-dwelling population or residential home inhabitants. The health characteristics of NH residents therefore have a high impact on their care requirements.
Major concerns in the nutrition of older adults are low energy and protein intake, often leading to malnutrition (8). One of the causes for the lower intake of nutrients can be also decreased appetite, which is common among older adults. In older age, one of the top priorities is maintaining muscle mass to prevent sarcopenia and frailty, which is achieved mainly through adequate protein intake and physical activity (9). The current European Society for Clinical Nutrition and Metabolism (ESPEN) guidelines for geriatrics state a daily protein intake of at least 1 g/kg body weight with up to 2 g/kg body weight/day considered appropriate based on individual health status (10). Despite this, in Europe, many institutionalised older adults have much lower daily protein intakes, which compromise muscle integrity and overall health (11). Attention should also be given to fat intake, with the recommended level set at 30% of daily energy intake (12), yet studies indicate that older adults often exceed this limit (13). Additionally, dietary fibre intake is generally inadequate across all population groups in Europe (14), with older adults particularly benefiting from a daily intake of at least 25 g to alleviate issues such as constipation (15). In NHs, many residents suffer from chronic disease and frailty (16); therefore, it is important that nutritional status is monitored and meals are carefully planned in order to support health and assist in slowing or preventing further decline, which is a burden for individuals and society and also increases care costs.
Gathering data on nutrient intakes is essential to provide valuable insights into the dietary habits of NH residents. NH meals are centrally planned, and residents rely almost entirely on NHs to provide their daily meals. Epidemiological data on NH residents’ nutrition is therefore invaluable for menu planning and aiding policymakers in developing targeted interventions and guidelines to improve the nutrition of older adults in such settings. It is important for NH staff to be familiar with the nutritional challenges of older adults living in NHs and to be trained to intervene effectively, as this is not always the case (17).
The epidemiological data on nutrition in NH in Europe is quite scarce. In Slovenia, there has been no comprehensive epidemiological study investigating the diets of NH residents. In the scope of the NutriCare project, this was addressed nationwide on a representative sample of NH residents. The aim of the present study was to explore the usual dietary intake of energy and macronutrients, as well as the consumption of specific food groups, among NH residents, and compare dietary patterns with the established recommendations. Additionally, the offers in the NH menus were explored.
This cross-sectional study was conducted as a part of the Slovenian National Research Project NutriCare, which focuses on dietary challenges among nursing home residents. The data was collected in June 2022, September 2022 (10 NHs), December 2022, January 2023, and February 2023 (10 NHs) to include both summer and winter seasons. Ethical approval for the study was obtained from the National Medical Ethics Committee (0120-531/2021/13) on 4.5.2022. The study was registered on clinicaltrials.gov (NCT05389618) (18).
The study was conducted in all 9 health regions, as defined by Slovenian National Institute for Public Health (19). The data on the residential demographic structure of all NH in Slovenia was obtained from the Ministry of Labour, Family, Social Affairs, and Equal Opportunities and used for the selection of NH for this study. Both public NHs and private NHs (with public concession) were included. A total of 20 NHs were included, with at least one from each region. First, the largest NH in each region was invited, while other(s) from the same region were selected using simple randomisation. If the largest regional NH declined participation, an alternative NH was selected using randomisation. The target sample size was set at a minimum of 300 participants, and quota sampling was conducted based on sex and age groups, following the approach used in the EFSA-funded nationally representative dietary survey SI. Menu (20), which included a subsample of community-dwelling older adults (but excluding NH residents). The final sample included N = 387 subjects (response rate 54%), representing more than 2% of the population in NHs (in the year 2022 Slovenian NH had altogether 17,939 residents aged 65+ years). For reference, similar national studies in other countries were commonly performed on smaller study samples (21, 22). It should be noted that the study sample was not intended to include bedbound, cognitively, or mentally impaired persons, who also reside in NHs. The study sample was selected from a relatively independent NH subpopulation, requiring low-level care (care category I–IIIa) and being able to give informed consent, which presents more than 80% of the population living in NHs in Slovenia.
After obtaining approval from NH management to conduct the study in the selected NHs, they provided an anonymous list of residents, including data on their care category, age, and sex. Based on predefined quota requirements for age groups (65–80 and over 80 years) and sex (men and women), each NH contributed to the quotas according to their resident composition and the number of residents in the selected care categories. Using simple computer-generated randomisation, and considering the size of the NH and the quota requirements, at least 36 participants, distributed by age and sex, were invited from each NH. Those who accepted the invitation to the study and signed an informed consent form were enrolled. The inclusion criteria were as follows: participants aged 65 years or older, have lived in an NH for at least 3 months before joining the study, and fall into care categories I., II., or III.A (indicating they require little or no personal assistance and are not severely cognitively impaired). Additionally, participants should be able to feed themselves independently or with minimal help and must have signed informed consent. The exclusion criteria were acute illness, being a dialysis patient, having a temporary special diet/ fasting at the time of the study visit, being unable to be weighed by the usual weighing scale or chair weighing scale, not being a full-time resident of an NH, and being in isolation due to COVID-19 measures.
Data was collected from the selected NHs during two study visits, which took place at least 7 days apart. The interviews and anthropometric measurements were performed by the trained researchers. At the first visit, data on age, sex, year of birth, and care category were taken from the NH records and medical records; data on disease and disease history, as well as data on the medications used, were collected. Anthropometric and body composition measurements were also taken. A general questionnaire, adopted and modified from the SI.Menu study (20), was used in the interviews to assess sociodemographic and health status, including eating habits, food allergies, and use of non-prescription drugs and food supplements. Participants were questioned on their physical activity using the International Physical Activity Questionnaire (IPAQ), and the scores were calculated using an established methodology (23). Dietary habits were assessed by two 24-h dietary recall (24HDR) and food frequency questionnaires (FFQ). The first 24HDR was performed on the first visit and on the second visit, the second 24HDR was performed. The participating NHs provided recipes with the ingredients amounts and meal portion amounts for all served meals on each of the 2 days that were questioned in the 24HDR. Additionally, 13 NHs provided these data for 7 days. Data on chronic disease were provided by the NH nurses from participants’ medical records.
Data on dietary intake was collected by 24HDR for two non-consecutive days, at least 7 days apart, according to the EFSA guidelines (24). In each NH, the data were collected in one season and both weekdays and weekends were considered, depending on the day of the study visit. For assistance, the NH menus with all dishes and portion sizes for the day of questioning were available, so the interviewers helped the participants recall the dishes on the menu and questioned them on any additional food, beverage, or supplements they consumed on that day. Recording of the consumed amounts of reported foods was supported using portion sizes in the daily menu of particular NH and a picture book (25), which was previously developed and used for the national dietary study SI.Menu. The picture book contains different food products and common dishes, accompanied by six portion sizes. For each reported food, it was also coded whether it was provided by the NH or not (i.e., for foods purchased by individual volunteers, provided by their relatives, etc.). The 24HDR was complemented with the FFQ to collect the data on the frequency of consumption of specific food categories in the past year, enabling us to model usual intakes (26). Altogether, 43 different food categories were included according to the food categorisation system and adopted and modified by Haubrock et al. (27) and the DGE Nutrition Circle (28). For each food category, daily frequencies of consumption were calculated based on the reported consumption frequency (e.g., 3× weekly). For some food categories (milk and dairy products, bread, and cereal products), recommendations for respective food subcategories were aggregated.
The data on dietary intake was analysed using the Open Platform for Clinical Nutrition (29), a web tool, which includes a Slovenian database with nutrient contents of generic and some branded foods (30). The OPEN Platform consists of nutritional composition data for different foods and recipes and allows the input of new recipes. All foods and beverages, reported in the 24HDR, were assigned to the OPEN Platform to obtain nutrient composition data to calculate daily nutrient intakes. The recipes for the dishes on the menu of each of the participating NHs were inputted into the OPEN platform, which assisted in the correct calculation of nutritional composition also for more complex dishes consumed. Nutrients were calculated for foods as prepared for consumption (e.g., cooked pasta).
Participants, who did not report both 24HDR (n = 7), were not included in the present study because we were not able to calculate their usual dietary intakes. Under- and over-reporting was assessed using the Goldberg method (31). This method assesses the plausibility of participants’ reported energy intake by comparing it to their estimated basal metabolic rate (BMR) and physical activity level (PAL) to evaluate if the reported energy intake aligns with the expected energy expenditure for such a population. The assigned PAL for the population in this study was 1.3, reflecting that the participants mostly exhibited very low physical activity levels, with many being mostly sedentary and some being wheelchair-bound (32). The BMR was estimated according to the Katch–McArdle equation (33) considering lean body mass (LBM). For participants with missing lean body mass data (n = 53), we estimated the BMR based on the linear association between values, calculated by two Katch McArdle equations, one considering LBM and the other anthropometric parameters (33) to enable the inclusion of these participants in the analytic sample. Cut-offs, calculated using the Goldberg method, considering a 95% confidence interval were 0.96 and 1.76; 27 under- and 27 over-reporters were excluded.
At the first study visit, height and weight were measured using the Seca 799 medical scale (Seca GmbH, Hamburg, Germany). Waist, hip, arm, and calf circumferences were measured using a soft measuring tape. Body composition was estimated using a Bodystat Multiscan 5,000 multifrequency bioelectrical impedance monitor (Bodystat, Isle of Man, Ireland). This device measures bioelectrical impedance by transmitting mild electrical current (800 μA) across a spectrum of frequencies (5–500 kHz) throughout the subject’s body via four electrodes. Two of the electrodes are positioned on the right hand and two on the right foot. Participants with cardiac pacemakers and those who were unable to get into the position suitable for performing measurements were excluded from this analysis. Bioimpedance techniques have been widely used for estimating body composition due to their non-invasiveness, portability, ease of use, and relatively low operation costs, compared to other techniques (34), such as the MRI and DXA methods (35). Body composition was estimated from the equations used in the Geriatric mode of Bodystat Multiscan 5,000 operation. The estimated lean body mass was further used for the estimation of participants’ BMR. Physical activity was assessed using the short form of the International Physical Activity Questionnaire (IPAQ) (23).
Usual daily dietary intakes were calculated from the two 24HDR and FFQ. The Multiple Source Method (MSM) was used for modelling variations in the intake distribution between and within days and individuals (27). Such a modelling approach enables the estimation of usual daily intake by correcting variations in food and nutrient intake of an individual by considering the FFQ data, which provide information on long-term dietary habits. FFQ frequencies were obtained by converting the reported frequency of consumption of specific food categories to daily frequencies (e.g., foods consumed twice per week had a daily frequency of 2/7). Participants recorded as true non-consumers reported they never eat foods from specific food categories.
The data on usual intakes of energy, nutrients, and food groups were presented as mean with standard deviation (SD) and median/quartiles or as numbers and percentages per day, for each sex. Usual daily mean (UDM) energy and protein intake were presented in kJ/kg or g/kg body weight, respectively. For statistical analyses, STATA (version 17.0; StataCorp LLC, College Station, TX, USA) and IBM SPSS Version 27 (IBM SPSS, IBM Corp., Armonk, NY) were used.
To obtain the adherence of usual intakes to the recommendations, energy and nutrient intakes were compared to the national reference values, which were adopted from the D-A-CH reference values for energy and nutrient intake (12) and the ESPEN guidelines on clinical nutrition for geriatrics (10). The proportions of the participants with usual intakes below or above the recommended values were calculated. Adherence to the intake of the recommended daily amounts of specific food groups was also presented, according to DGE Nutrition Circle criteria (28). In the case of food categories, for which the recommended amounts referred to weekly consumption (e.g., meat and eggs), these were converted to recommended daily amounts and presented accordingly.
Altogether, 13 NHs also provided daily menus for 7 consecutive days, while 7 NHs provided daily menus for 2 non-consecutive days. However, four daily menus were excluded from the analysis due to their total energy deviating more than two standard deviations from the mean. In total, 108 daily NH menus were included in the analyses of the offered menus in NHs. We modelled the daily macronutrient content data provided by NHs to estimate the macronutrient composition in daily menus and main meals, offered by all NHs. For this purpose, we used linear mixed model analysis with the random effect of NHs on intercepts. Additionally, the generalised linear mixed-effects model analysis was employed to explore differences in main meals to contain at least 25 g of protein among (1) NHs, and (2) main meals (breakfast, lunch, and dinner). We looked at both NHs with random effects on the intercepts set on the type of meal and main meals with random effects of NHs on intercepts.
Altogether, 378 participants were included in the NutriCare study. For nutrition assessment, seven participants were excluded due to incomplete data on 24HDR and FFQ, and 54 were classified as mis-reporters using the Goldberg method and were excluded from further analysis. The final sample for the present study therefore included 317 participants. The characteristics of the participants are presented in Table 1. The participants’ flowchart is presented in Supplementary Table 3.
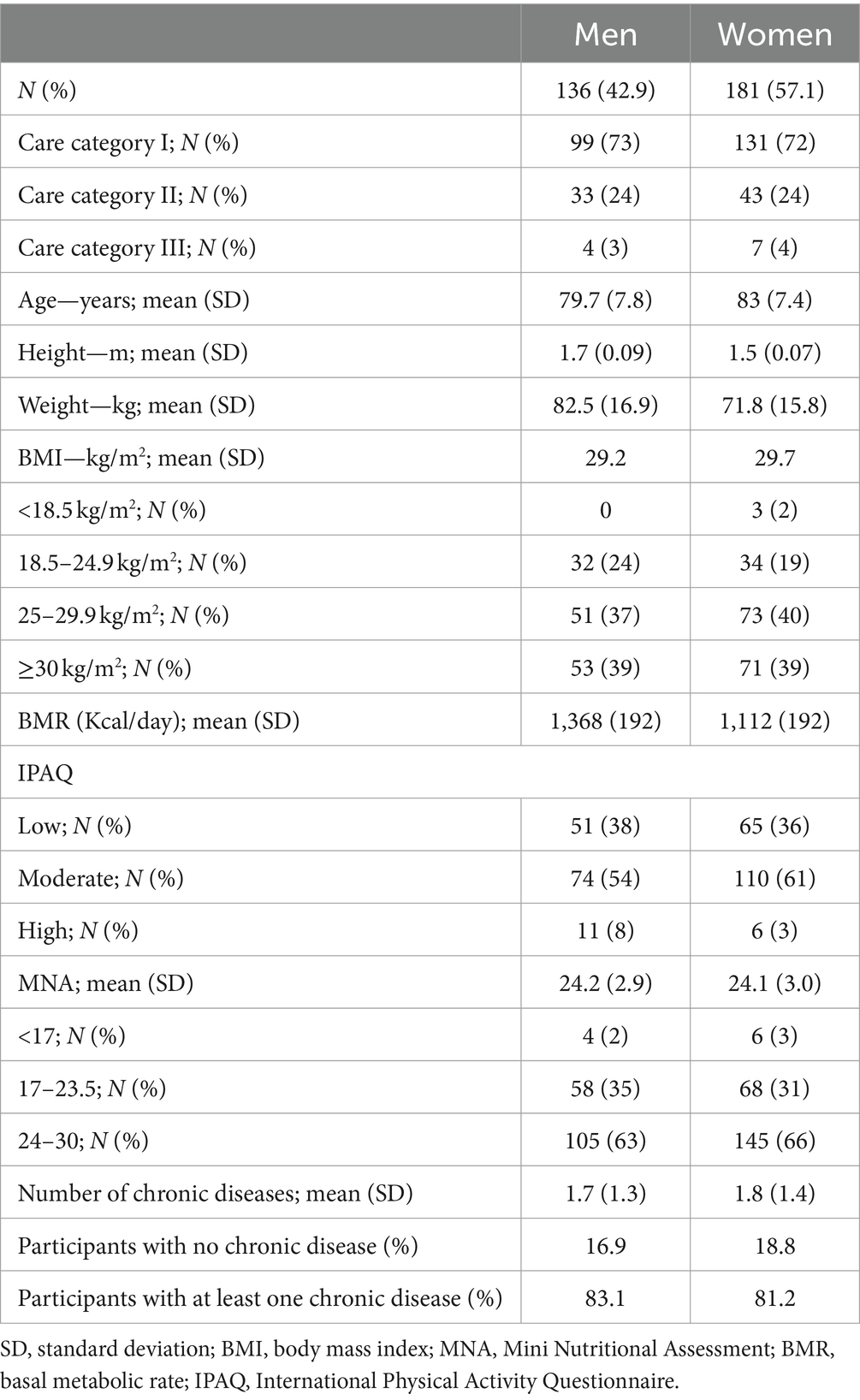
Table 1. Characteristics of participants in the NutriCare study (Slovenia, 2022–2023).
Table 2 presents the descriptive statistics of the usual daily dietary intake of participants. Wide UDM energy intake ranges were observed in both sexes; however, at least half of the population in both sexes had UDM energy intakes below 30 kcal/kg body weight, which is recommended by the ESPEN (10). On the other hand, a high prevalence of high BMI was observed (Table 1).

Table 2. Descriptive statistics of usual daily dietary intakes in men and women nursing home residents in the NutriCare study (Slovenia, 2022–2023).
Daily carbohydrate intake below the recommended 50% of daily energy intake was observed in 81% of men and 66% of women (Table 3). Low mean dietary fibre intake was observed, which was approximately 20 g daily for both sexes (Table 2). Less than 20% of the participants had dietary fibre intakes of at least 25 g daily (Table 3). Approximately 90% of the participants had fat intakes above 30% of total daily energy intake (Table 3).
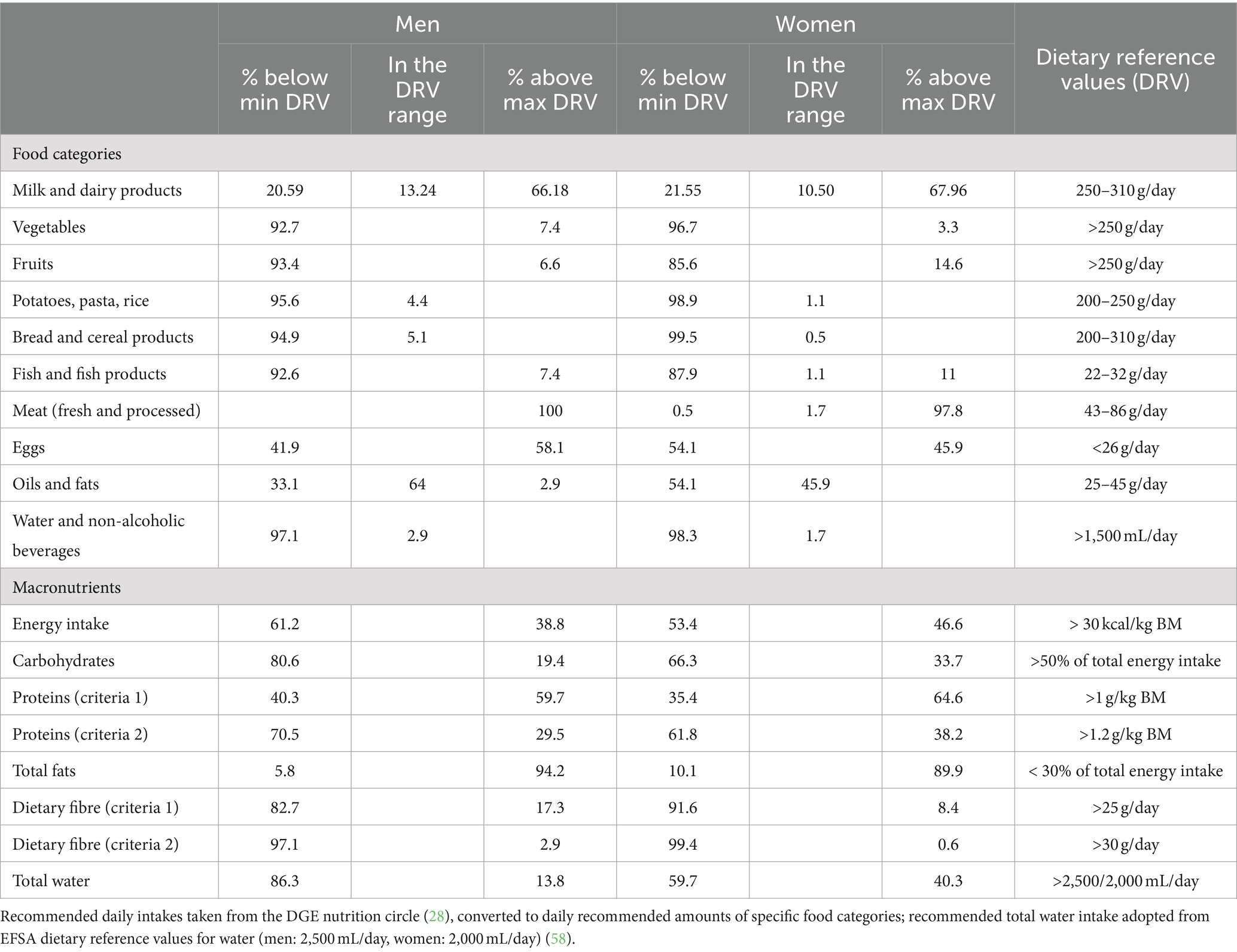
Table 3. Proportions of men and women nursing home residents meeting reference values for specific food categories, energy, and macronutrients in the NutriCare study (Slovenia, 2022–2023).
The UDM protein intake was 1.1 g/kg body weight for men and 1.2 g/kg body weight for women (Table 2). However, as presented in Table 4, 40% of men and 35% of women do not meet the minimum daily reference protein intake of 1 g/kg body weight. Given the high prevalence of chronic diseases among the NH residents, the recommended daily protein intake according to ESPEN (10) would be closer to 1.2 g/kg body weight. The median intake of 1.1 g/kg body weight for both sexes suggests that more than 50% of participants have suboptimal daily protein intakes (Table 2). In fact, 70% of men and 62% of women had usual daily protein intakes below this threshold (Table 3). A high range of UDM protein intakes was noticed in both sexes, from 0.5 g/kg body weight to more than 2 g/kg body weight, indicating a high variability of UDM protein intakes per kg body weight among participants (Table 2).
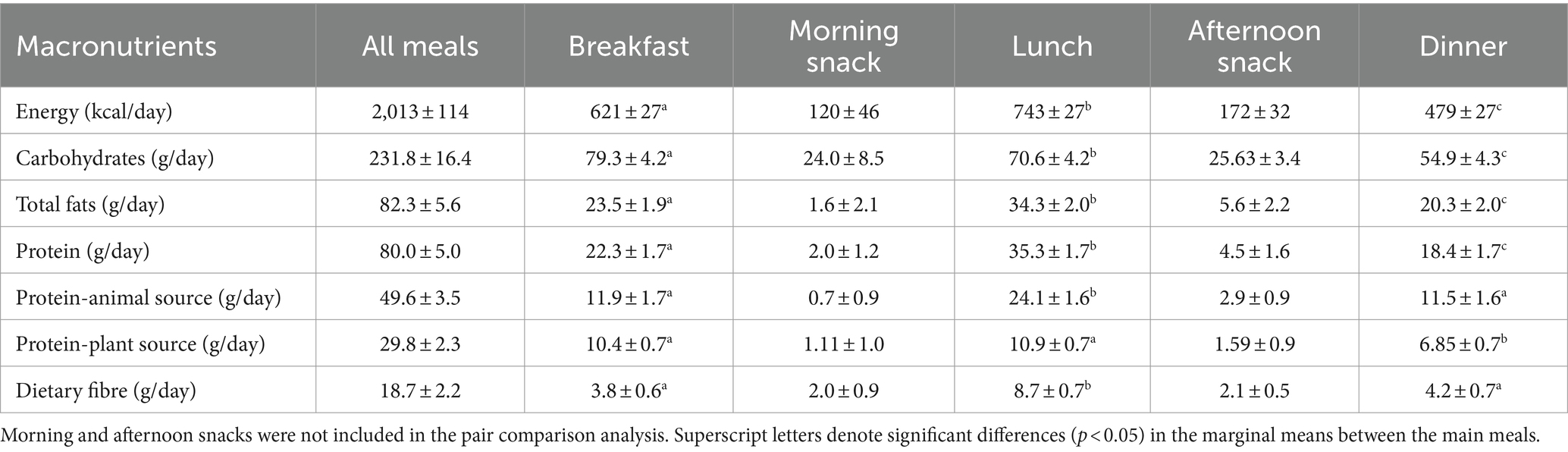
Table 4. Linear mixed model mean (CI) estimates of macronutrient composition of daily meals served in nursing homes in the NutriCare study (Slovenia, 2022–2023).
Looking into the food categories and their amounts consumed among the NH residents, Table 3 and Supplementary Table 1 show that according to the dietary reference values, particularly meat was consumed in excess amounts; 100% of men and 98% of women exceeded the maximum reference value of 86 g meat daily, with a mean daily amount of 137 and 114 g, respectively. On the other hand, at least 85% of women and more than 90% of men did not meet the recommended daily intakes for fruit, vegetables, potatoes, pasta, rice, bread, cereal products, and fish.
The results from the linear mixed effects models determining the available macronutrient composition in daily menus and the mean comparison analysis of the meal composition using the random effect of NHs on intercepts are presented in Table 4. The mean modelled energy content of daily NH menus was 2.013 ± 114 kCal. Approximately one-third of energy intake was from breakfast, a third from lunch, a quarter from dinner, and the rest from snacks. The mean amount of protein per meal was the highest for lunch (35.5 ± 1.7 g) and the lowest for dinner (18.4 ± 1.7 g). The dominating source of protein was animal protein, which was most noted in lunch and was significantly higher than in breakfast and dinner. Breakfast and lunch had similar content of plant-sourced proteins, while at dinner, it was significantly lower. The mean daily amount of meat and meat products offered in NH menus was 167 g, which was well above the recommendations (Supplementary Table 2). On the other hand, the total mean daily amounts of fruits and vegetables on NH menus were below 400 g. The foods, consumed from outside sources (not offered through NH menus) presented approximately 1% of daily energy consumption. These were mostly coffee, soft drinks, sweets, and fruit.
Although the analysis of UDM energy intakes among NH residents might suggest a generally satisfactory state, a closer examination revealed considerable variability within the population, which was also evident in UDM macronutrient intakes. A notable concern arises from the fact that the mean BMI of participants exceeded 29 kg/m2 in both sexes, with approximately 40% of participants having a BMI > 30 kg/m2, indicating obesity according to the World Health Organisation (WHO) criteria (36). Although meta-analyses did not show a significant link between increased mortality and overweight in older adults, going beyond a BMI of 28 kg/m2 put a considerable proportion of participants at risk (37). The high prevalence of obesity highlights an important health issue, supposedly originating mainly in imbalances in dietary intake and physical activity. Due to the predominantly sedentary lifestyles of NH residents, the introduction of suitable physical activity is crucial for maintaining their functionality and independence and preventing various diseases, particularly sarcopenic obesity (38). In this population, low BMI and malnutrition are serious concerns, but our study did not find them to be significant issues based on the MNA results (only 3% of malnourished participants), probably mainly due to the characteristics of our study sample (39), which included residents in need of low-level care.
The distribution proportions of UDM macronutrient intakes indicate an opportunity to better align with the established recommendations for macronutrient intake. In older adults, adequate protein intake is crucial for maintaining muscle mass, which tends to decline during this stage of life (40). As shown in Table 3, daily protein intakes were not optimal for many participants. For example, 40% of men and 35% of women failed to meet even the lowest threshold for daily protein intake (1 g/kg BM), compared to 40% of community-dwelling Slovenian older men and 21% of women (20). This could also be related to the variations in body weight of the participants. As dietary protein intakes should be individually adjusted, considering health and nutritional status, the “one-fits-all” approach could hardly suit all NH residents’ protein requirements. This is particularly pronounced in those with higher body weight. In such cases, the recommended protein daily intake (e.g., >1.2 g/kg BM) could be difficult to achieve in practice, especially through communal meals alone, as the protein quantities required could be very high. On the other hand, such high protein quantities could pose a risk for some residents, for example, those with kidney failure. This highlights the importance of monitoring the nutritional status of NH residents and employing individual approaches.
A substantial proportion of the total energy intake (TEI) was shown to be derived from fats, indicating that daily menus, offered in NH exhibit an excessive fat content (37% of energy intake). Less than 10% of NH residents had appropriate daily fat intakes up to 30% of daily energy intake, with men being more exposed. This can be linked to the high consumption of meat and dairy products among NH residents. High dietary fat intakes and imbalances in the type of consumed fats should not be overlooked, as this can potentially influence various health outcomes in older adults, including cognitive function (41), metabolic syndrome (42), and risk of fractures (43). Regarding the fact that approximately 13% of TEI was from saturated fats, balancing meals by including more unsaturated fats would be beneficial. Considering the high prevalence of individuals with high BMI in our sample, more attention should be paid to the fat content of the meals, particularly the type of fats contained in the meals.
Suboptimal carbohydrate and fibre intakes were noted. Inadequate intake of less-refined carbohydrates is associated with low dietary fibre intake, observed in more than 80% of men and 90% of women who consume dietary fibre below the daily threshold of 25 g (10). Generally, the UDM fibre intakes in our study were even lower than in Slovenian community-dwelling older adults (44), where 77% of men and 65% of women had UDM fibre intakes below 25 g. It should be noted that 25 g of dietary fibre daily is the lowest threshold for normal laxation (45), while the optimal daily intake would be 30 g. Regarding the fact that older adults, particularly institutionalised, often have constipation issues (46), it would be crucial to adjust dietary fibre intakes to support normal laxation. For example, it has been shown that dietary fibre intervention in NH residents led to the discontinuation of laxative use in more than half of the users and significantly improved their overall wellbeing (46). Adding more fruits and vegetables to the diet could support this, as currently, approximately 90% of participants do not meet the daily recommendations for these food groups, which is set at >250 g/day (28). Moreover, a higher intake of wholegrain bread and cereal products would be a positive addition to their daily diet and fibre intake.
Adequate hydration was found to be a problem, especially among men. In older adults, this is often a concern, as many of them do not feel thirsty, have incontinence issues, or simply forget to drink. NH residents should regularly be offered drinks and encouraged to consume fluids by NH staff (47).
UDM macronutrient intakes of the participants reflected what we found in the analysis of NH menus. In general, the menus were not optimally balanced (Table 4). As NH residents consume little food from outside sources, NH meals should well suit their dietary needs. Our findings showed that the NH menus failed to provide a balanced macronutrient intake to meet the needs of the NH residents optimally, even though Slovenia has implemented recommendations for meal planning in NHs already in the year 2020 (48). The main issue observed was that the NH daily menus were excessive in fat (37% energy—estimated) and rather scarce in quality carbohydrates (46% energy—estimated), affecting the adequate daily intake of fibre. If, for various reasons, daily protein intakes in NH residents cannot be individually adjusted, meals should at least contain the recommended amount of protein (25–30 g protein per meal) (11, 48). Breakfast and dinner had a particularly low protein content, with a mean below 25 g. We observed significant differences in the likelihood of reaching a minimum of 25 g protein per meal between main meals (F = 37.7; df = 2; p < 0.001) as well as between NHs (F = 1.8; df = 19; p = 0.017).
The observed macronutrient intakes essentially mirrored the consumption patterns of specific food groups. The general impression was that NH menus should try to focus on introducing more foods of plant origin. The menus were heavy on foods of animal origin, especially dairy products and meat, but lacked vegetables, fruits, and cereals to balance the nutrient intakes. Although meat is an important source of good quality protein and micronutrients, replacing some of the animal protein and introducing more foods of plant origin, including legumes and nuts, could not only add to the protein content of meals but also add more less-refined carbohydrate sources and dietary fibre to the existing meals, contributing to more balanced diets (49). Foods of animal origin can also be high in fat, which is unfavourable for a healthy diet. Higher dietary fibre intake could be achieved by replacing refined grains, such as white bread and pasta, with whole grains. Meals could include more vegetable side dishes and salads, as well as fruits. Furthermore, reducing the use of foods high in saturated fat by offering leaner cuts of meat, limiting high-fat dairy, and using plant-based oils such as olive oil for cooking would help lower the overall fat content and its quality, which is particularly important given the BMIs observed in this sample. By introducing such changes, NH staff could create more balanced menus that better address the observed discrepancies and promote healthier dietary patterns.
Similar issues in macronutrient and food group composition of dietary intakes of NH residents have been also highlighted in previous studies (50, 51). The main issues of concern were usually low energy and protein intake (22, 52, 53) and also high fat and low dietary fibre intakes (50, 54, 55). However, when comparing and interpreting results from different studies, it is important to be cautious due to the differences in the methodology of data collection and analysis. Although similar methods are used for the assessment of dietary intakes—usually 24HDR or food diaries, many studies report habitual (short term) dietary intakes, while in our study, usual dietary intakes were reported, which reflect long-term dietary habits. Regardless of methodological differences, the observed trends in nutrient intakes often point in the same direction, as mentioned above. As NH residents almost completely rely on NH provision of food, more attention should be paid to include more beneficial food groups currently lacking in their diet.
The importance of including qualified professionals, such as dietitians and clinical nutrition experts, in the multidisciplinary NH teams has been continuously highlighted (56, 57). Only a comprehensive approach and individual monitoring could efficiently combat malnutrition and related preventable health problems in the NH population. Unfortunately, nutrition professionals are currently rarely actively included in the care of Slovenian NH residents. To deliver high-quality care in NHs and avoid additional costs associated with poor nutrition among residents, addressing this issue should be a top priority. In any case, the nutritional status of NH residents should be monitored using established tools, such as the MNA and the Global Leadership Initiative on Malnutrition (GLIM) (58) criteria to identify emerging nutrition-related issues to act promptly and appropriately.
The present study was the first nationally representative study focussed on investigating the nutrition of NH residents in Slovenia. It is one of the few studies comprehensively addressing the nutrition of the older adults in long-term residential institutions with national representativeness. The cross-sectional study design allowed for a snapshot of dietary patterns among this vulnerable population focussing on usual macronutrient intakes and the consumption of various food groups. Most of the studies on the nutrition of NH residents used only the MNA for the assessment of nutritional status, without using tools that allow the estimation of usual dietary intakes. The present study included relatively independent NH residents requiring low-level care, who well-presented most of the Slovenian NH population and were not bedbound. Such a population is characteristically closer to community-dwelling older adults or those living in residential homes; however, the latter is not very common in Slovenia. NH population with low-level care requirements allows for the implementation of improvement strategies to practice, maintain health, and prevent or delay advancing in care assistance. The latter is linked to health decline and the loss of independence, which causes significantly higher costs of care and staff requirements (59). The findings present valuable insights that could assist in further meal planning and areas for potential improvement with the aim of providing better care for older adults. A limitation that should be considered is that not all the NHs provided daily menus for the whole week; therefore, for mean macronutrient meal composition analysis, weights were used. Another limitation is that physical activity was assessed using self-reported IPAQ scores, which should be interpreted with caution. For a more specific assessment of the physical activity, objective methods should be employed such as accelerometers or pedometers. These devices would provide more reliable data, minimising the subjective inaccuracies that accompany self-reporting.
Future studies should explore challenges in achieving the proper nutritional status of distinct subgroups of NH residents, such as those with specific diseases or feeding-related difficulties with the aim to optimise their nutrition according to the specific requirements. The variations in NH menus among NHs across the country could also be assessed. Additionally, interventions that could improve nutrient status, health, and quality of life should be explored. Furthermore, given that NHs facilitate communal meals, there is a need to investigate optimal strategies for accommodating the diverse dietary requirements of residents within a communal dining framework.
The results of the present study showed that the diet of Slovenian NH residents could be improved. Notable variability in macronutrient intakes was observed; men were found particularly at risk for an imbalanced diet. The prevalence of high BMI reflects the discrepancies between energy intake and expenditure. The diets of NH residents were high in fats and foods of animal origin (meat and dairy) and low in less-refined carbohydrates and dietary fibre, due to insufficient intake of fruits, vegetables, and cereals. The protein content of meals could be enhanced, especially for breakfast and dinner. NH residents consume little food from sources outside the NH, and their macronutrient and food group intakes well reflect the composition of menus served in NHs. Careful menu planning and monitoring of the nutritional status of NH residents should be implemented to avoid health complications and higher care costs. Qualified staff capable of implementing individualised, tailored nutritional monitoring and interventions is needed to ensure optimal care for NH.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Slovenian National Medical Ethics Committee. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
ŽL: Writing – review & editing, Writing – original draft, Supervision, Resources, Project administration, Methodology, Funding acquisition, Formal analysis. IP: Writing – review & editing, Methodology, Funding acquisition, Conceptualization. SK: Writing – review & editing, Formal analysis. NH: Writing – review & editing, Formal analysis. NG: Writing – review & editing, Methodology. IH: Writing – review & editing, Methodology. BK: Writing – review & editing, Formal analysis. HH: Writing – review & editing, Methodology, Formal analysis, Conceptualization.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. The project NutriCare: “Dietary challenges in the population of nursing homes’ residents” Z3-3213 was funded by the Slovenian Research and Innovation Agency. Additional funding was provided within the research programme P3-0395 “Nutrition and Public Health,” funded by the Slovenian Research and Innovation Agency.
We are grateful to all participants, who enabled the conduction of the study. We acknowledge the support of all NutriCare researchers and students who helped in the study conduct, particularly Kim Bratkič, Tjaša Perko, Kaja Krajnc, Ana Poročnik, Maja Cokan, Špela Goljuf, Monika Húdeková, Matej Štebih, Tilen Sernc, Neja Hranjec, Lara Dobaj, Jasna Verdnik, Gregor Potrebuješ, Patricija Kunstek, and Karmen Klemenc (Nutrition Institute, Slovenia). We are grateful for the support of the participating nursing homes staff and management, particularly Alenka Milojica, Ana Štefančič, Martina Demojzes, Valerija Volk, Dijana Glavaš, Katarina Cijan, Manca Kovač Likar, Aleš Kovač, Nataša Slejko, Lilijana Deržek, Jožica Hudžar, Andreja Bogdan, Katarina Rakuša, Hermina Smole, Dragica Čas, Jana Starc, Sabina Avsec, Martina Martinčič, Vojvodić Biljana, and Tomaž Teran. We would like to also thank Dorothee Volkert and Doris Eglseer for providing useful suggestions for the design of the study protocol.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2024.1423658/full#supplementary-material
1. WHO (2018). Ageing and health. Available at: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (Accessed October 14, 2024).
2. Donini, LM, Scardella, P, Piombo, L, Neri, B, Asprino, R, Proietti, A, et al. Malnutrition in elderly: social and economic determinants. J Nutr Health Aging. (2013) 17:9–15. doi: 10.1007/s12603-012-0374-8
3. Pirlich, M, and Lochs, H. Nutrition in the elderly. Best Pract Res Clin Gastroenterol. (2001) 15:869–84. doi: 10.1053/bega.2001.0246
4. Zhao, W, Ukawa, S, Okada, E, Wakai, K, Kawamura, T, Ando, M, et al. The associations of dietary patterns with all-cause mortality and other lifestyle factors in the elderly: an age-specific prospective cohort study. Clin Nutr. (2019) 38:288–96. doi: 10.1016/j.clnu.2018.01.018
5. WHO (2020). Malnutrition 2020. Available at: https://www.who.int/news-room/questions-and-answers/item/malnutrition (Accessed October 14, 2024).
6. Verbrugghe, M, Beeckman, D, Van Hecke, A, Vanderwee, K, Van Herck, K, Clays, E, et al. Malnutrition and associated factors in nursing home residents: a cross-sectional, multi-Centre study. Clin Nutr. (2013) 32:438–43. doi: 10.1016/j.clnu.2012.09.008
7. Bell, CL, Lee, AS, and Tamura, BK. Malnutrition in the nursing home. Curr Opin Clin Nut Metabolic Care. (2015) 18:17–23. doi: 10.1097/MCO.0000000000000130
8. Agarwal, E, Miller, M, Yaxley, A, and Isenring, E. Malnutrition in the elderly: a narrative review. Maturitas. (2013) 76:296–302. doi: 10.1016/j.maturitas.2013.07.013
9. Morley, JE, Argiles, JM, Evans, WJ, Bhasin, S, Cella, D, Deutz, NE, et al. Nutritional recommendations for the management of sarcopenia. J Am Med Dir Assoc. (2010) 11:391–6. doi: 10.1016/j.jamda.2010.04.014
10. Volkert, D, Beck, AM, Cederholm, T, Cruz-Jentoft, A, Goisser, S, Hooper, L, et al. ESPEN guideline on clinical nutrition and hydration in geriatrics. Clin Nutr. (2019) 38:10–47. doi: 10.1016/j.clnu.2018.05.024
11. Deutz, NE, Bauer, JM, Barazzoni, R, Biolo, G, Boirie, Y, Bosy-Westphal, A, et al. Protein intake and exercise for optimal muscle function with aging: recommendations from the ESPEN expert group. Clin Nutr. (2014) 33:929–36. doi: 10.1016/j.clnu.2014.04.007
12. D-A-CH (2020) Reference values DACH 2020. Available from: https://www.sge-ssn.ch/grundlagen/lebensmittel-und-naehrstoffe/naehrstoffempfehlungen/dachreferenzwerte/.
13. ter Borg, S, Verlaan, S, Hemsworth, J, Mijnarends, DM, Schols, JMGA, Luiking, YC, et al. Micronutrient intakes and potential inadequacies of community-dwelling older adults: a systematic review. Br J Nutr. (2015) 113:1195–206. doi: 10.1017/S0007114515000203
14. Stephen, AM, Champ, MM-J, Cloran, SJ, Fleith, M, Van Lieshout, L, Mejborn, H, et al. Dietary fibre in Europe: current state of knowledge on definitions, sources, recommendations, intakes and relationships to health. Nutr Res Rev. (2017) 30:149–90. doi: 10.1017/S095442241700004X
15. Emmanuel, A, Mattace-Raso, F, Neri, MC, Petersen, K-U, Rey, E, and Rogers, J. Constipation in older people: a consensus statement. Int J Clin Pract. (2017) 71:e12920. doi: 10.1111/ijcp.12920
16. Onder, G, Vetrano, DL, Marengoni, A, Bell, JS, Johnell, K, and Palmer, K. Accounting for frailty when treating chronic diseases. Eur J Intern Med. (2018) 56:49–52. doi: 10.1016/j.ejim.2018.02.021
17. Suominen, MH, Sandelin, E, Soini, H, and Pitkala, KH. How well do nurses recognize malnutrition in elderly patients? Eur J Clin Nutr. (2009) 63:292–6. doi: 10.1038/sj.ejcn.1602916
18. Nutrition institute (2022). Dietary challenges in the population of nursing homes' residents (NUTRICARE) Available at: https://classic.clinicaltrials.gov/ct2/show/NCT05389618?id=NCT05389618&draw=2&rank=1 (Accessed October 14, 2024).
19. NIJZ (2022). Regije 2021. Available at: https://www.nijz.si/sl/regije (Accessed October 14, 2024).
20. Gregorič, M, Hristov, H, Blaznik, U, Koroušić Seljak, B, Delfar, N, and Pravst, I. Dietary intakes of Slovenian adults and elderly: design and results of the National Dietary Study SI.Menu 2017/18. Nutrients. (2022) 14:3618. doi: 10.3390/nu14173618
21. Doumit, JH, Nasser, RN, and Hanna, DR. Nutritional and health status among nursing home residents in Lebanon: comparison across gender in a national cross sectional study. BMC Public Health. (2014) 14:629. doi: 10.1186/1471-2458-14-629
22. Ongan, D, and Rakıcıoğlu, N. Nutritional status and dietary intake of institutionalized elderly in Turkey: a cross-sectional, multi-center, country representative study. Arch Gerontol Geriatr. (2015) 61:271–6. doi: 10.1016/j.archger.2015.05.004
23. Lee, PH, Macfarlane, DJ, Lam, TH, and Stewart, SM. Validity of the international physical activity questionnaire short form (IPAQ-SF): a systematic review. Int J Behav Nutr Phys Act. (2011) 8:1–11. doi: 10.1186/1479-5868-8-115
24. EFSA. Guidance on the EU menu methodology. EFSA J. (2014) 12:3944. doi: 10.2903/j.efsa.2014.3944
25. Gregorič MTF, V.; Gabrijelčič Blenkuš, M. (2013). Slikovno Gradivo s Prikazom Velikosti Porcij: Inštitut za varovanje zdravja Republike Slovenije. Available at: https://www.nijz.si/sites/www.nijz.si/files/publikacije-datoteke/slikovno_gradivo_s_prikazom_velikosti_porcij.pdf (Accessed October 14, 2024).
26. Dodd, KW, Guenther, PM, Freedman, LS, Subar, AF, Kipnis, V, Midthune, D, et al. Statistical methods for estimating usual intake of nutrients and foods: a review of the theory. J Am Diet Assoc. (2006) 106:1640–50. doi: 10.1016/j.jada.2006.07.011
27. Haubrock, J, Nöthlings, U, Volatier, JL, Dekkers, A, Ocké, M, Harttig, U, et al. Estimating usual food intake distributions by using the multiple source method in the EPIC-Potsdam calibration study. J Nutr. (2011) 141:914–20. doi: 10.3945/jn.109.120394
28. Oberritter, H, Schäbethal, K, Von Ruesten, A, and Boeing, H. The DGE nutrition circle—presentation and basis of the food-related recommendations from the German nutrition society (DGE). Ernahrungs-Umschau. (2013) 60:24–9.
29. IJS (2010). OPKP - odprta platforma za klinično prehrano. Available from: www.opkp.si. [Accessed Janury 01, 2015].
30. Korošec, M, Golob, T, Bertoncelj, J, Stibilj, V, and Seljak, BK. The Slovenian food composition database. Food Chem. (2013) 140:495–9. doi: 10.1016/j.foodchem.2013.01.005
31. Goldberg, GR, Black, AE, Jebb, SA, Cole, TJ, Murgatroyd, PR, Coward, WA, et al. Critical evaluation of energy intake data using fundamental principles of energy physiology: 1. Derivation of cut-off limits to identify under-recording. Eur J Clin Nutr. (1991) 45:569–81. doi: 10.1038/sj.ijo.0801376
32. Shetty, P. Energy requirements of adults. Public Health Nutr. (2007) 8:994–1009. doi: 10.1079/PHN2005792
33. McArdle, WD, Katch, FI, and Katch, VL. Exercise Physiology. Med Sci Sports Exerc. (1991) 23:1403. doi: 10.1249/00005768-199112000-00013
34. Mulasi, U, Kuchnia, AJ, Cole, AJ, and Earthman, CP. Bioimpedance at the bedside. Nutr Clin Pract. (2015) 30:180–93. doi: 10.1177/0884533614568155
35. Müller, MJ, Braun, W, Pourhassan, M, Geisler, C, and Bosy-Westphal, A. Application of standards and models in body composition analysis. Proc Nutr Soc. (2015) 75:181–7. doi: 10.1017/S0029665115004206
36. WHO (2010). A healthy lifestyle - WHO recommendations/. Available at: https://www.who.int/europe/news-room/fact-sheets/item/a-healthy-lifestyle---who-recommendations (Accessed October 14, 2024).
37. Winter, JE, MacInnis, RJ, Wattanapenpaiboon, N, and Nowson, CA. BMI and all-cause mortality in older adults: a meta-analysis. Am J Clin Nutr. (2014) 99:875–90. doi: 10.3945/ajcn.113.068122
38. Reiter, L, Bauer, S, Traxler, M, Schoufour, JD, Weijs, PJ, Cruz-Jentoft, A, et al. Effects of nutrition and exercise interventions on persons with Sarcopenic obesity: an umbrella review of Meta-analyses of randomised controlled trials. Curr Obes Rep. (2023) 12:250–63. doi: 10.1007/s13679-023-00509-0
39. van Nie-Visser, NC, Meijers, J, Schols, J, Lohrmann, C, Bartholomeyczik, S, Spreeuwenberg, M, et al. Which characteristics of nursing home residents influence differences in malnutrition prevalence? An international comparison of the Netherlands. Germany Austria Br J Nutr. (2013) 111:1129–36. doi: 10.1017/S0007114513003541
40. Moore, DR. Keeping older muscle “young” through dietary protein and physical activity. Adv Nutr. (2014) 5:599S–607S. doi: 10.3945/an.113.005405
41. Cao, GY, Li, M, Han, L, Tayie, F, Yao, SS, Huang, Z, et al. Dietary fat intake and cognitive function among older populations: a systematic review and meta-analysis. J Prev Alzheimers Dis. (2019) 6:204–11. doi: 10.14283/jpad.2019.9
42. Julibert, A, Bibiloni, MM, Mateos, D, Angullo, E, and Tur, JA. Dietary fat intake and metabolic syndrome in older adults. Nutrients. (2019) 11:1901. doi: 10.3390/nu11081901
43. Mozaffari, H, Djafarian, K, Mofrad, MD, and Shab-Bidar, S. Dietary fat, saturated fatty acid, and monounsaturated fatty acid intakes and risk of bone fracture: a systematic review and meta-analysis of observational studies. Osteoporos Int. (2018) 29:1949–61. doi: 10.1007/s00198-018-4540-7
44. Seljak, BK, Valenčič, E, Hristov, H, Hribar, M, Lavriša, Ž, Kušar, A, et al. Inadequate intake of dietary fibre in adolescents, adults, and elderlies: results of Slovenian representative SI. Menu study. Nutrients. (2021) 13:3826. doi: 10.3390/nu13113826
45. Agostoni, C, Bresson, J-L, Fairweather Tait, S, Flynn, A, Golly, I, Korhonen, H, et al. Scientific opinion on dietary reference values for carbohydrates and dietary fibre. EFSA J. (2010) 8:1462. doi: 10.2903/j.efsa.2010.1462
46. Sturtzel, B, and Elmadfa, I. Intervention with dietary fiber to treat constipation and reduce laxative use in residents of nursing homes. Ann Nutr Metab. (2008) 52:54–6. doi: 10.1159/000115351
47. Wotton, K, Crannitch, K, and Munt, R. Prevalence, risk factors and strategies to prevent dehydration in older adults. Contemp Nurse. (2008) 31:44–56. doi: 10.5172/conu.673.31.1.44
48. Zelenik, D, Fajdiga, T. V., Gabrijelčič, B. M., Hovnik, K. M., Jevšjak, K., Kurbus, A., et al. (2020). Smernice za izvajanje prehranske oskrbe v domovih za starejše. Available at: https://www.nijz.si/sites/www.nijz.si/files/publikacije-datoteke/smernice_za_izvajanje_prehranske_oskrbe_v_domovih_za_starejse.pdf (Accessed October 14, 2024).
49. Carballo-Casla, A, Sotos-Prieto, M, García-Esquinas, E, A Struijk, E, Caballero, FF, Calderón-Larrañaga, A, et al. Animal and vegetable protein intake and malnutrition in older adults: a multicohort study. J Nut Health Aging. (2024) 28:100002. doi: 10.1016/j.jnha.2023.100002
50. Fernández-Barrés, S, Martín, N, Canela, T, García-Barco, M, Basora, J, Arija, V, et al. Dietary intake in the dependent elderly: evaluation of the risk of nutritional deficit. J Hum Nutr Diet. (2016) 29:174–84. doi: 10.1111/jhn.12310
51. Aytekin Sahin, G, and Caferoglu, Z. The food service quality and its effects on nutritional status in nursing home residents. Clin Nut ESPEN. (2022) 47:233–9. doi: 10.1016/j.clnesp.2021.12.004
52. Woods, JL, Walker, KZ, Iuliano-Burns, S, and Strauss, BJ. Malnutrition on the menu: nutritional status of institutionalised elderly Australians in low-level care. J Nut Health Aging. (2009) 13:693–8. doi: 10.1007/s12603-009-0199-2
53. Vikstedt, T, Suominen, MH, Joki, A, Muurinen, S, Soini, H, and Pitkälä, KH. Nutritional status, energy, protein, and micronutrient intake of older service house residents. J Am Med Dir Assoc. (2011) 12:302–7. doi: 10.1016/j.jamda.2010.12.098
54. Nowson, C, Sherwin, A, McPhee, J, Wark, J, and Flicker, L. (2003). Energy, protein, calcium, vitamin D and fibre intakes from meals in residential care establishments in Australia.
55. Rodríguez-Rejón, AI, Ruiz-López, MD, and Artacho, R. Dietary intake and associated factors in long-term care homes in Southeast Spain. Nutrients. (2019) 11:266. doi: 10.3390/nu11020266
56. Agarwal, E, Marshall, S, Miller, M, and Isenring, E. Optimising nutrition in residential aged care: a narrative review. Maturitas. (2016) 92:70–8. doi: 10.1016/j.maturitas.2016.06.013
57. Stahl, J, Hauser, C, Simon, M, Valenta, S, Favez, L, and Zúñiga, F. Institutional factors associated with residents’ malnutrition in nursing homes: a cross-sectional study. J Am Med Dir Assoc. (2023) 24:1074–81. doi: 10.1016/j.jamda.2023.02.010
58. Cederholm, T, Jensen, GL, Correia, M, Gonzalez, MC, Fukushima, R, Higashiguchi, T, et al. GLIM criteria for the diagnosis of malnutrition - a consensus report from the global clinical nutrition community. Clin Nutr. (2019) 38:1–9. doi: 10.1016/j.clnu.2018.08.002
Keywords: older adults, nursing home residents, dietary intake, macronutrient intake, protein, energy, dietary fibre
Citation: Lavriša Ž, Pravst I, Krušič S, Hren N, Gregorič N, Hren I, Koroušić Seljak B and Hristov H (2024) Nutrition among nursing home residents: results from the NutriCare study. Front. Nutr. 11:1423658. doi: 10.3389/fnut.2024.1423658
Edited by:
Kathleen L. Hefferon, Cornell University, United StatesReviewed by:
Gerd Faxén Irving, Karolinska Institutet (KI), SwedenCopyright © 2024 Lavriša, Pravst, Krušič, Hren, Gregorič, Hren, Koroušić Seljak and Hristov. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Živa Lavriša, eml2YS5sYXZyaXNhQG51dHJpcy5vcmc=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.