 Amanuel Yosef Gebrekidan1*†
Amanuel Yosef Gebrekidan1*† Yordanos Sisay Asgedom1
Yordanos Sisay Asgedom1 Beshada Zerfu Woldegeorgis2
Beshada Zerfu Woldegeorgis2 Gizachew Ambaw Kassie1
Gizachew Ambaw Kassie1 Kirubel Eshetu Haile3
Kirubel Eshetu Haile3 Solomon Abrha Damtew1Ashenafi Teklay4
Solomon Abrha Damtew1Ashenafi Teklay4 Amare Demsie Ayele5
Amare Demsie Ayele5- 1School of Public Health, College of Health Sciences and Medicine, Wolaita Sodo University, Wolaita Sodo, Ethiopia
- 2Department of Internal Medicine, College of Health Sciences and Medicine, Wolaita Sodo University, Wolaita Sodo, Ethiopia
- 3School of Nursing, College of Health Sciences and Medicine, Wolaita Sodo University, Wolaita Sodo, Ethiopia
- 4Subuha Seasie Woreda Health Office, Edaga Hamus, Tigray, Ethiopia
- 5Department of Pediatrics and Child Health Nursing, School of Nursing, College of Medicine and Health Sciences and Specialized Hospital, University of Gondar, Gondar, Ethiopia
Background: Vitamin A supplementation every 4–6 months is an economical, rapid, and effective strategy to enhance vitamin A status and minimize child morbidity and mortality due to vitamin A deficiency in the long run. Therefore, this study was aimed at investigating the level as well as the factors influencing VAS status among children aged 6–59 months in Tanzania.
Methods: This analysis relied on data from the 2022 Tanzania Demographic and Health Survey (TDHS). The study used a weighted sample of 9,382 children aged 6–59 months. Given the effect of clustering and the binary character of the outcome variable, we employed a multilevel binary logistic regression model. The adjusted odds ratio (AOR) with a 95% confidence interval (CI) was used to determine statistical significance, considering the model with the lowest deviation that best fits the data.
Results: In this study, vitamin A supplementation among children aged 6–59 months was found to be 53.18% [95% CI: 52.17, 54.19]. Mother’s/caregiver’s working status; Working [AOR = 1.59, 95% CI: 1.34, 1.89], ANC follow-up [AOR = 1.71, 95%CI: 1.34, 2.2], and health facility delivery [AOR = 1.55, 95%CI: 1.25, 1.91] were individual-level factors associated with vitamin A supplementation. Whereas administrative zones of Western [AOR = 2.02, 95% CI: 1.16, 3.52], Southern highlands [AOR = 3.83, 95% CI: 2.02, 7.24], Southern administrative zone [AOR = 2.69, 95% CI: 1.37, 5.3], and South West highlands [AOR = 0.56, 95% CI: 0.33, 0.95] were community-level factors associated with vitamin A supplementation.
Conclusion: The proportion of VAS among children in Tanzania is low compared to UNICEF’s target of 80. Mother’s/caregiver’s working status, antenatal care, place of delivery, community-level media exposure, and administrative zones were significantly associated factors with vitamin A supplementation. Therefore, interventions should be designed to improve the uptake of VAS. Provision and promotion of ANC and institutional delivery and strengthening of routine supplementation are recommended to increase coverage of childhood vitamin A supplementation. Moreover, special focus should be given to regions in the south-western highlands.
Introduction
Vitamin A is an essential nutrient for several physiological functions throughout all stages of life. Vitamin A and its derivatives regulate a wide range of functions, including reproduction, embryogenesis, vision, growth, cellular differentiation and proliferation, epithelial cellular integrity maintenance, and immunological function, as well as the development of children, and it is typically gained through a nutritious diet (1, 2). The primary animal sources of vitamin A are liver, eggs, milk, and milk products. Plant foods high in provitamin A account for more than 80% of total vitamin A intake due to their low cost, widespread availability, and diversity. Fruits, roots, tubers, and leafy vegetables are the primary sources of vitamin A carotenoids. Among fruits, mangoes are an important source of vitamin A. Yellow or orange-sweet potatoes are high in provitamin A. Red palm oil also contains high levels of provitamin A carotenoids (3). Retinol is the primary circulating form of vitamin A in the blood and plasma (4). Vitamin A (VA) improves immune function and decreases mortality from measles, diarrhea, and other infections (5).
Vitamin A deficiency occurs when dietary intake of vitamin A is insufficient to meet physiological requirements (4). Vitamin A deficiency is the major cause of preventable childhood blindness, increasing the risk of death from common childhood diseases, including measles and diarrhea. Conversely, vitamin A deficiency can also be aggravated by high infection rates, particularly diarrhea and measles. It is widespread in low-income countries and a public health concern, particularly in Africa and Southeast Asia, but uncommon in developed countries (2, 4).
Vitamin A deficiency affects around 190 million preschool-aged children, the majority of whom live in Africa and Southeast Asia, and there is evidence linking it to severe acute malnutrition. If left untreated, vitamin A deficiency can lead to blindness, an increased risk of disease, and mortality from childhood infections (6). In 2013, the prevalence of vitamin A deficiency, considering data from 83 countries across the globe, was found to be 29% (7). Between 1991 and 2013, vitamin A deficiency decreased from 42 to 6% in East and Southeast Asia and Oceania, as well as from 21 to 11% in Latin America and the Caribbean. In 2013, Sub-Saharan Africa had the highest prevalence of vitamin A deficiency (48%), followed by South Asia (44%) (7). Vitamin A deficiency caused 94,500 fatalities from diarrhea and 11,200 deaths from measles, accounting for 1.7 percent of all deaths in children under 5 years old in low-and middle-income countries. More than 95% of the deaths occurred in sub-Saharan Africa and South Asia (7).
Different studies conducted in Tanzania have shown a varying degree of vitamin A deficiency. A study conducted to determine the effect of vitamin A deficiency on the anthropometric attributes of children in the Manyara and Shinyanga regions of Tanzania found that the prevalence of vitamin A deficiency among children aged 6–36 months was 69.5% (8). Another study conducted in Kikwawila and Kiberege wards, Tanzania, on primary schoolchildren aged 6–12 years showed that the magnitude of vitamin A deficiency was 34.71% (9).
On April 1, 2016, the United Nations (UN) General Assembly proclaimed 2016–2025 the United Nations Decade of Action on Nutrition. Led by World Health Organization and the Food and Agriculture Organization of the United Nations (FAO), the UN Decade of Action on Nutrition calls for policy action across six key areas, including aligning health systems to nutrition needs and providing universal coverage of essential nutrition interventions (10).
Vitamin A supplementation twice a year is linked to a clinically relevant reduction in morbidity, and it was found to reduce the risk of all-cause death by 12% when compared to the non-supplemented controls. Additionally, it will lead to a 12% reduction in deaths caused by diarrhea, a 15% reduction in the incidence of diarrhea, and a 50% reduction in the incidence of measles (7, 11). Therefore, supplementation with vitamin A every 4–6 months is an economical, rapid, and effective strategy to enhance vitamin A status and minimize child morbidity and mortality in the long run (2, 12). In many countries, vitamin A supplementation for newborns and children has been successfully combined with routine immunization programs and vaccination campaigns. Furthermore, delivering high-dose supplements to mothers at vaccination centers soon after birth provides an additional benefit to young infants through enriched breast milk (2).
The coverage of vitamin A supplementation for children aged 6–59 months rose from 30% in 2008–2009 to 72% in 2014 worldwide (13). Even though the importance of vitamin A supplementation is proven, the coverage and utilization of vitamin A supplementation are still below target in most countries. A United Nations International Children’s Emergency Fund (UNICEF) report in 2018 shows that in 2016, only 64% of children in need in priority countries received two doses of vitamin A; yet, more than 141 million children were left behind, making them vulnerable to disease and death (13). According to data from Nutrition International, 167 million under-five children received two doses of vitamin A in 2021, and 80% of those who need vitamin A supplements in developing countries were reached (11). The 2016 Tanzania Demographic and Health Survey (TDHS) and the 2018 Tanzania nutrition survey showed that the coverage of vitamin A supplementation among 6–59 month-old children was 41 and 63.8%, respectively (14, 15). A UNICEF report in 2022 indicates a two doses of vitamin A coverage was 90% in Tanzania, which indicates a 6 % reduction compared to 96% coverage in 2021 (16). Despite this, previous studies have shown that the national VAS coverage is based on a tally-sheet system, which can estimate vitamin A supplementation 30% higher than the actual coverage. Additionally, there are factors, including health worker measurement errors in summarizing the count sheets and underestimating target population statistics, that indicate the need for nation-wide representative studies (17).
Different studies associate different factors with the uptake of vitamin A supplementation, both at the individual level and at the community level. Age of the mother, educational status of the mother, mother’s occupation, and household wealth status were frequently mentioned as individual-level sociodemographic factors (18–21). Maternal obstetric factors such as antenatal care, place of delivery, and postnatal care were found to be significantly associated with vitamin A supplementation (18, 20, 21). The age of the child is described as a child-related characteristic associated with vitamin A supplementation (18–20). Region (area) and residence were found to be factors associated with vitamin A supplementation at a community level (18–20).
Although there is evidence on the level of VAS in Tanzania, the majority of the evidence is derived from government reports, and available studies either utilized data from the previous demographic and health surveys conducted or were conducted on a small scale and cannot represent the whole country, with an additional lack to identify national-level factors.
Therefore, this study was aimed at using the most recent 2022 Tanzania Demographic and Health Survey and Malaria Indicator Survey (2022 TDHS-MIS) data to investigate the level as well as the factors influencing VAS status among children aged 6–59 months in Tanzania, aiming to provide current information on the national-level VAS and its determinants, facilitating evidence-based decision-making.
Materials and methods
Study design and study area
We conducted a secondary data analysis study by using cross-sectional designed data from the 2022 Tanzania Demographic and Health Survey and Malaria Indicator Survey (2022 TDHS-MIS). Tanzania is organized into 31 regions; 26 in mainland Tanzania and 5 in Zanzibar (22). According to the 2022 population and housing census of Tanzania, the country has a total of 61.7 million population of which 59,851,347 reside in mainland Tanzania while 1,889,773 reside in Zanzibar. Of the total population, 40.2 million and 21.5 million people reside in rural and urban areas, respectively. Out of the total population, 31.7 million were females while the remaining 30 million were males (23). The 2022 Tanzania Demographic and Health Survey and Malaria Indicator Survey (2022 TDHS-MIS) is the seventh in a series of Demographic and Health Surveys (DHS) in Tanzania, carried out through the DHS Program. Previous DHSs were conducted in 1991–1921, 1996, 1999, 2004–2005, 2010, and 2015–2016. The 2022 TDHS-MIS aims to give current and credible information on population and health matters (22). To achieve this, a nationally representative sample of 16,354 households were chosen for the survey (22). Tanzania was divided into nine zones to evaluate spatial differences in population indicators. The Reproductive and Child Health Section of the Ministry of Health uses this classification scheme, despite the fact that these zones are not formal administrative areas. Grouping regions into zones results in larger denominators and smaller sampling errors for indicators at the zonal level (22).
Data source, population and sampling procedure
This study was based on the recent 2022 TDHS-MIS, which is conducted to update health and health-related indicators. The 2022 TDHS-MIS sample design involved two stages and included estimates for the entire country, urban and rural areas in Tanzania Mainland, and Zanzibar (22). The first stage involved selecting sampling points (clusters) from enumeration areas (EAs) identified for the 2012 Tanzania Population and Housing Census (2012 PHC). EAs were chosen with a probability proportional to their size within each sampling stratum. A total of 629 clusters were identified. Of the 629 EAs, 211 were from urban areas and 418 from rural areas (22). The second stage involved selecting 26 households from each cluster, resulting in a total sample size of 16,354 for the 2022 TDHS-MIS. Prior to the main survey, all selected EAs underwent household listing operations, and households were selected from each cluster using a systematic sampling (22).
This study used data from interviewed women with under-five children (TZKR data). The investigation comprised 9,382 weighted sample children aged 6–59 months.
Study variables and measurement
This study’s dependent variable was vitamin A supplementation among children aged 6–59 months within the previous 6 months before the survey. It was assessed by reviewing the integrated child health card, which includes immunization and growth monitoring information, as well as the mother’s spoken response, to determine if they have received vitamin A supplementation within the past 6 months. Because of the hierarchical nature of the DHS data, we evaluated individual and community-level variables as independent variables. Individual-level variables such as sociodemographic and economic variables, child-related characteristics, and a mother’s/caregiver’s obstetric characteristics were considered individual-level independent variables. The sociodemographic and economic variables included were the mother’s/caregiver’s age, the sex of the household head, marital status, mother’s/caregiver’s educational level, husband’s/partner’s educational level, mother’s/caregiver’s occupation, husband’s/partner’s occupation, and wealth index. The wealth index of households receives scores based on the number and types of consumer goods they own, including televisions, bicycles, or cars, as well as dwelling qualities like sources of drinking water, bathroom facilities, and flooring materials. These scores are calculated using principal component analysis. National wealth quintiles are calculated by assigning a household score to each household member, ranking each person based on their score, and splitting the distribution into five equal categories, each representing 20% of the population. It was categorized as poorest, poorer, middle, richer, and richest (22).
Independent variables under the child-related characteristics include the child’s age and the sex of the child, whereas independent variables under mother’s/caregiver’s obstetric characteristics include parity; parity was categorized as low parity if the mother or caregiver has never given birth or gave birth once; multiparous if the mother or caregiver gave two up to four births; and grand multiparous if the mother or caregiver gave five or more births. Antenatal care (ANC) was assessed if a woman with a live birth or a stillbirth in the last 2 years received antenatal care from a skilled provider for the most recent birth (24). The place of delivery of the child was categorized as home if the child was delivered at places other than a health facility and as a health facility if the child was delivered at a health facility (25); and number of under-five children in the household, were used as independent variables. The community-level variables were residence, administrative zones and community-level media exposure. Administrative zones: Tanzania was divided into nine zones to evaluate spatial differences in population indicators. The Reproductive and Child Health Section of the Ministry of Health uses this classification scheme, despite the fact that these zones are not formal administrative areas. Grouping regions into zones results in larger denominators and smaller sampling errors for indicators at the zonal level. The administrative zones were classified as main land Tanzania (8 zones): Western zone: Tabora, Kigoma; Northern zone: Kilimanjaro, Tanga, Arusha; Central zone: Dodoma, Singida, Manyara; Southern Highlands zone: Iringa, Njombe, Ruvuma; Southern zone: Lindi, Mtwara; Southwest Highlands zone: Mbeya, Rukwa, Katavi, Songwe; Lake zone: Kagera, Mwanza, Geita, Mara, Simiyu, Shinyanga; Eastern zone: Dar es Salaam, Pwani, Morogoro; and Zanzibar (1 zone): Zanzibar zone: Kaskazini Unguja, Kusini Unguja, Mjini Magharibi, Kaskazini Pemba, Kusini Pemba (22). Community media exposure was classified as “yes” if they had access to all three media (read a newsletter, listen to a radio, and watch television) at least once a week, and “no” if they had no media exposure (25).
Data processing and analysis
The data were analyzed in Stata version 14 (StataCorp, United States) following the eligibility check. A multilevel analysis was carried out. The model’s eligibility was determined by calculating the Intra-class Correlation Coefficient (ICC), and a model with ICC more than 10% was selected for multilevel analysis. In this study, the ICC was 18.2%. Because the data were hierarchical (individuals were nested within communities), a two-level mixed-effects logistic regression model was fitted to estimate both the individual and community level variables (fixed and random effect) on vitamin A supplementation status, and the log of the probability of VAS was modeled using the formula below (26):
In this equation, i and j represent individual and community units, while X and Z represent individual and community-level variables, respectively. Πij represents the probability of vitamin A supplementation for the ith 6–59 months aged child in the jth community. The (β) will be the fixed coefficients. The intercept (β0) represents the probability of Vitamin A supplementation in the absence of predictors; the random effect (μj) represents the effect of the community on VAS for the jth community, whereas eij represents random errors at the individual level. Assuming each community has a unique intercept (β0) and fixed coefficient (β), we can account for clustered data and variances between communities (26).
After being weighted with sampling weight, primary sampling unit, and strata to account for the sampling design and restore survey representativeness. Because the outcome variable was binary, we used a multilevel binary logistic regression model to investigate the associated factors of Vitamin A supplementation. Because DHS data are hierarchical, under five children are nested inside clusters, and subjects within the same cluster may have comparable characteristics with those in another cluster, so breaching the independence and equal variance criteria. As a result, an advanced multilevel cumulative logit model was applied to account for cluster heterogeneity. To quantify the extent of cluster variation in Vitamin A supplementation status, four models for multilevel binary logistic regression analysis were developed. These models included a null model with no explanatory factors. The second model was modified for individual-level factors, and the third for community-level variables. The fourth model was fitted simultaneously with variables at the individual and community levels. To find the best-fitted model for the data, model fitness was assessed using deviance [−2Log-Likelihood Ratio (LLR)], with the model with the lowest deviation being the most appropriate. In the bivariable multilevel binary logistic regression model, variables having a p-value ≤0.2 were considered for the multivariable analysis. The multivariable analysis gave an adjusted odds ratio (AOR) with a 95% confidence interval (CI). Variables with a p-value <0.05 were identified as significantly associated factors.
Measures of variation (random-effects) were reported using ICC, median odds ratio (MOR), and proportionate change in variance (PCV) to compare variations between clusters. The ICC measures the similarity of observations within a cluster, while MOR assesses unexplained cluster heterogeneity (26). MOR is defined as the median odds ratio between the highest and lowest risk areas when two areas are chosen at random (26). In this study, MOR demonstrates how much the residential cluster influences an individual’s likelihood of vitamin A supplementation. The proportionate change in variance (PCV) calculates the overall variation caused by both individual-level and area-level components in a multilevel model (26).
Ethical consideration
Our study did not require ethical approval or participant agreement because it was a secondary analysis of publicly available survey data from the MEASURE DHS program. However, the 2022 TDHS-MIS questionnaires and survey protocol were approved and authorized by the Medical Research Council of Tanzania and the Zanzibar Health Research Institute. The ICF’s Internal Review Board also reviewed the study. The dataset was retrieved from the Demographic and Health Survey program website1 after receiving consent to use it. Furthermore, the dataset did not include any personally identifiable information, such as names or household numbers (identifiers).
Results
Socio-demographic characteristics of respondents
The study included a weighted sample of 9,382 mothers/caregivers with children aged 6–59 months (Table 1). The mean age of the mothers was 27.79 (SD ± 7.04) years, with the majority (78.83%) of the household heads being male. Nearly one-third (32.39%) of mothers are not working, and 22.85% of households fall into the poor wealth index (Table 1).
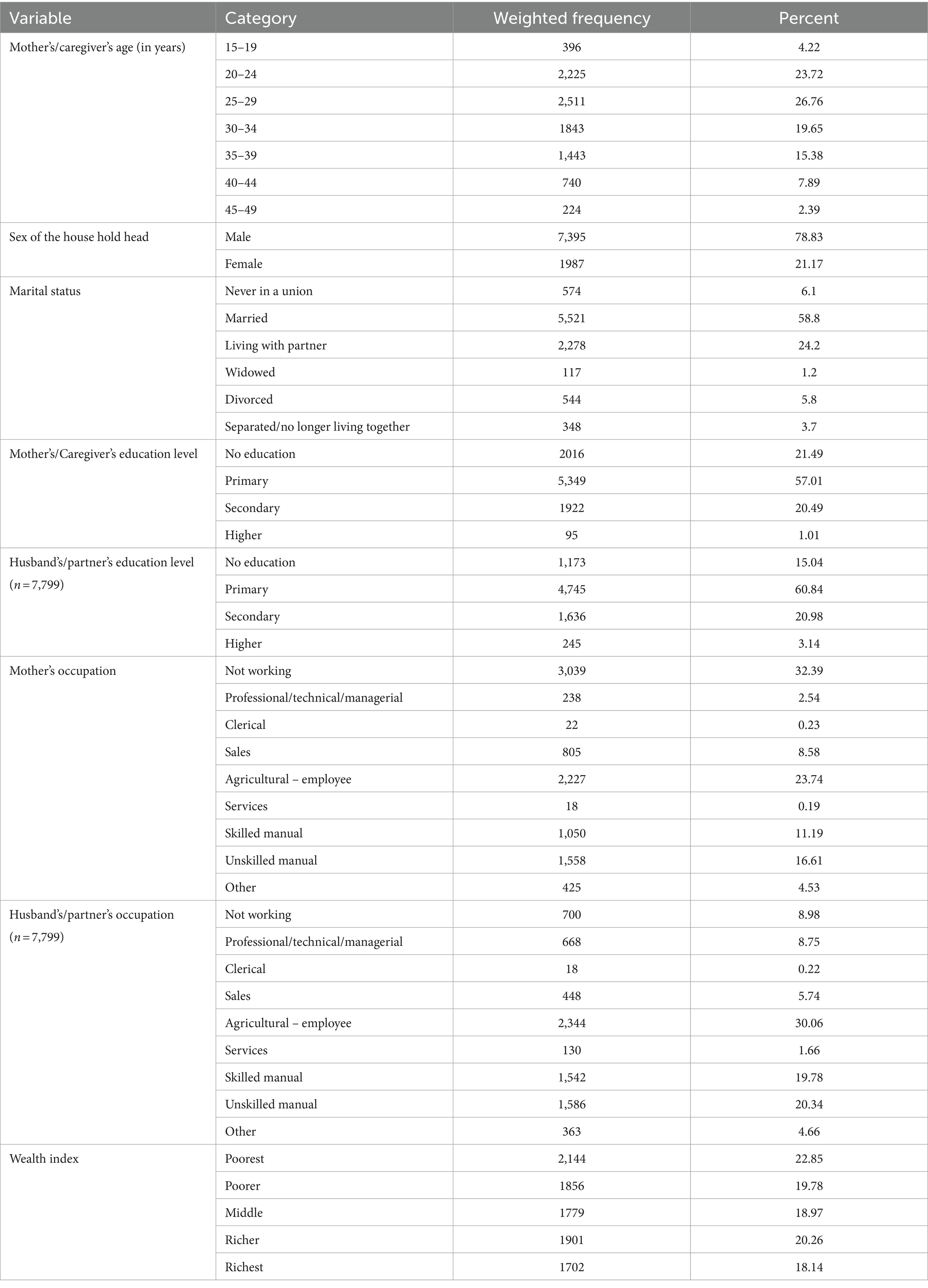
Table 1. Sociodemographic and economic characteristics of study participants who have children aged 6–59 months in Tanzania.
Mothers/caregivers obstetrics related characteristics
Out of the total 9,382 included mothers/caregivers, 55.29% are multiparous, while 29.54% are grand multiparous. Out of 4,612 mothers who were asked for antenatal care follow-up, 89.4 had ANC follow-up, and the majority, 81.2%, delivered their last child in a health facility. More than half, or 52.48%, of the households have two to three under five children in their houses (Table 2).
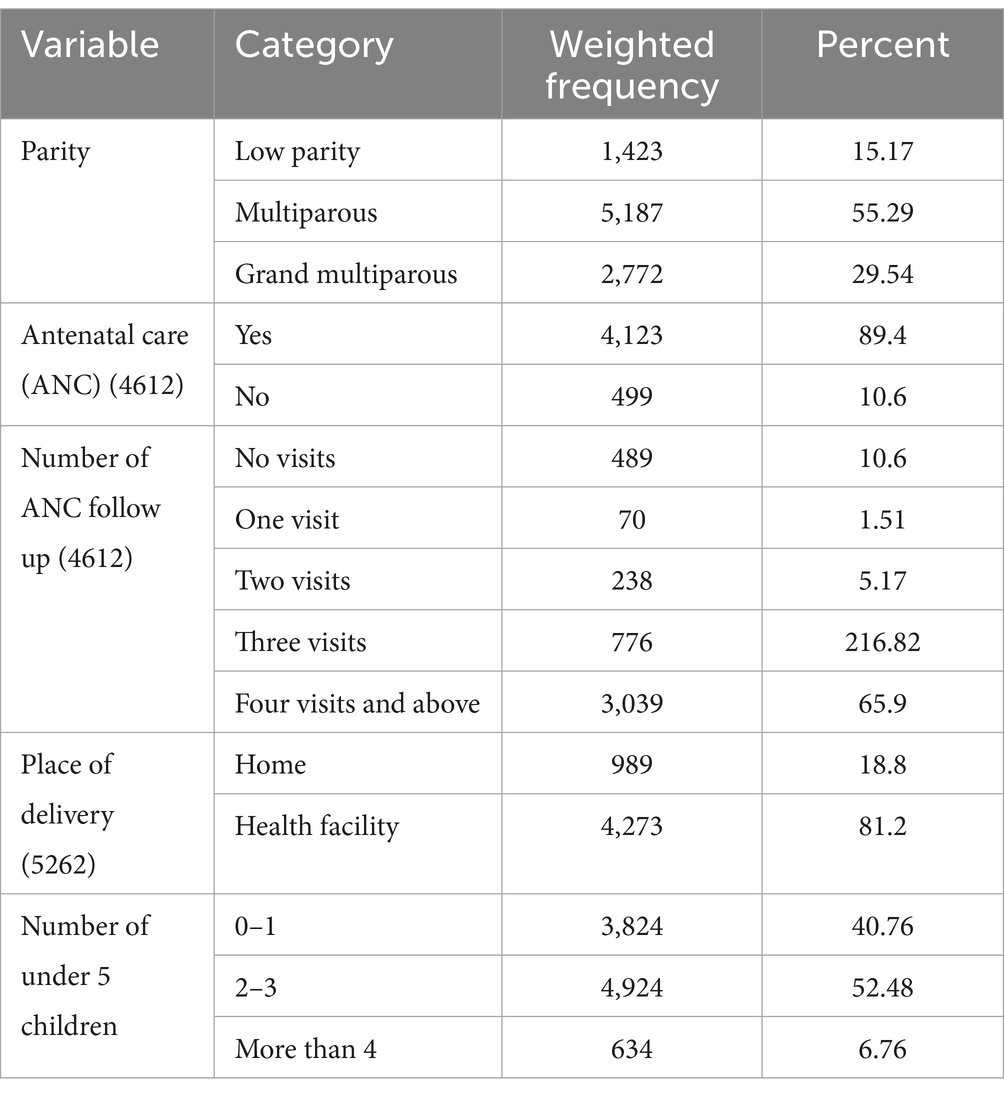
Table 2. Obstetrics-related characteristics of respondent mothers/caregivers who have children aged 6–59 months in Tanzania.
Child characteristics
The mean age of the children was 32.07 (standard deviation ±15.69) months, with 50.88% being male (Table 3).
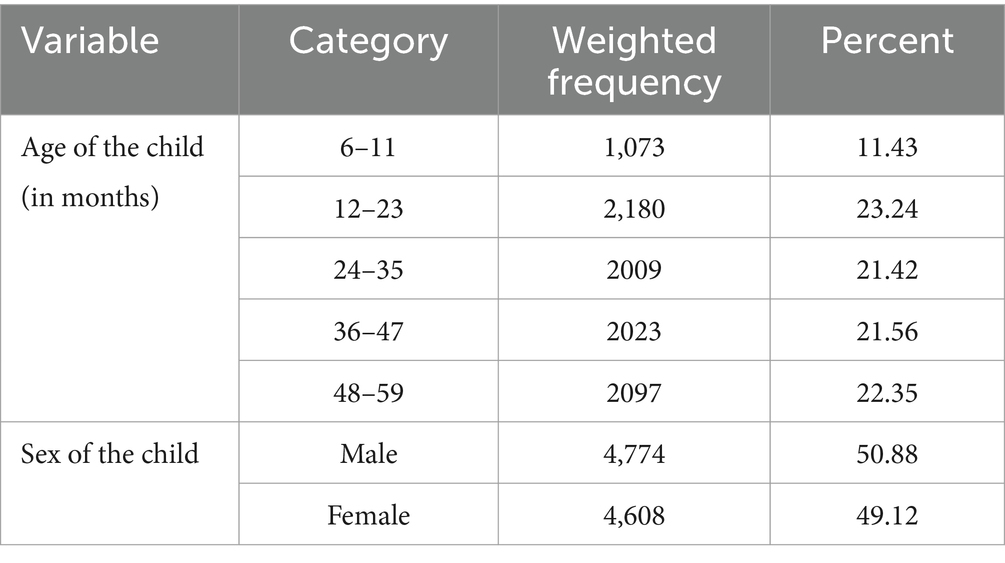
Table 3. Child-related characteristics among study participants aged 6–59-month-old children in Tanzania.
Community level characteristics
The majority of the study participants (72.63%) reside in urban areas, with more than one-third (34.22%) living in the Lake Administrative Zone. More than half of the households (59.85%) have no media exposure (Table 4).
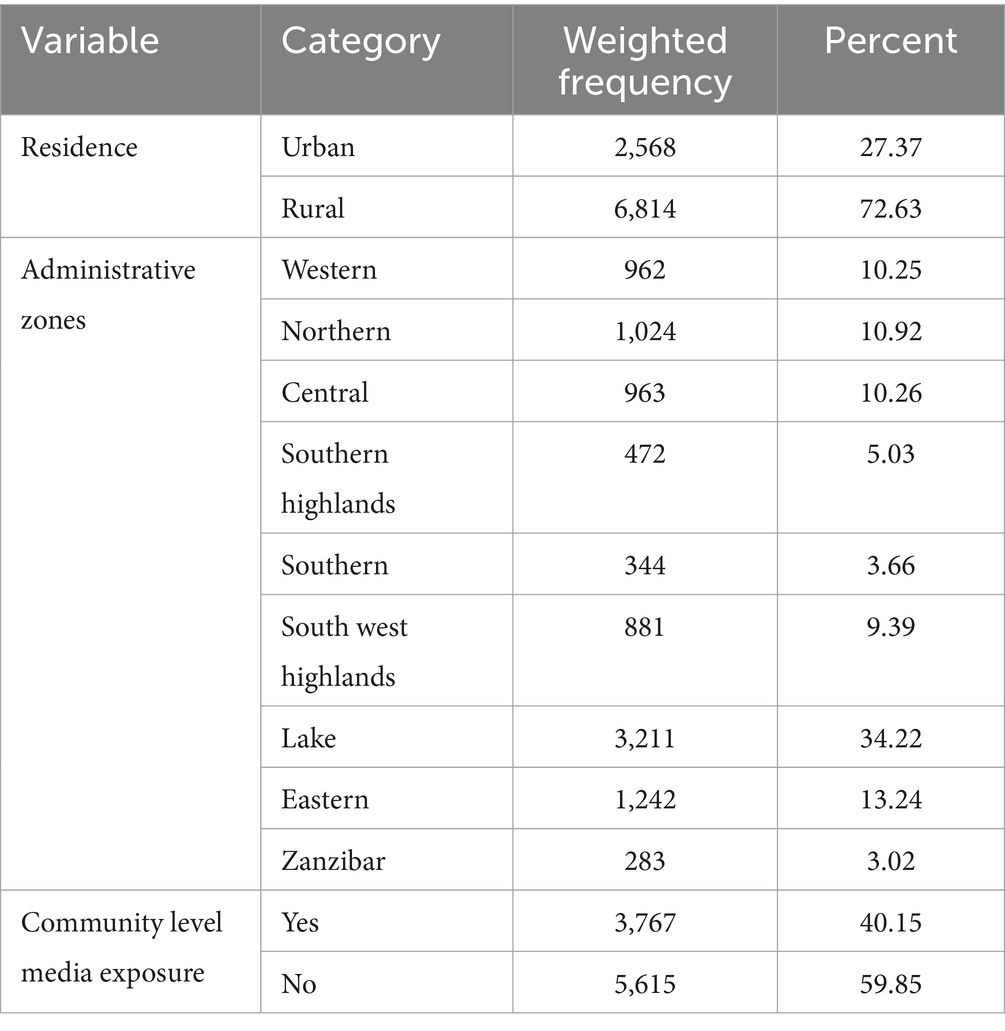
Table 4. Community-level characteristics of study participants who have children aged 6–59 months in Tanzania.
Vitamin A supplementation uptake among children aged 6–59 months in Tanzania
The overall uptake of vitamin A supplementation in Tanzania among children aged 6–59 months in the last 6 months prior to the survey was 53.18% [95% CI: 52.17, 54.19] (Figure 1).
Figure 1. Proportion of vitamin A supplementation status among 6–59-month-old children in Tanzania.
Random effect analysis (measures of variation)
Null model (model 1)
This model is intercept-only, with no predictors. We used the Likelihood Ratio to determine if the multilevel binary logistic regression model was more significant than the single-level binary logistic regression model. The LR test findings were statistically significant (p < 0.01), showing that the multilevel binary logistic regression model best fit the single-level binary logistic regression analysis. As a result of the LR test, a multilevel binary logistic regression model was used to identify factors associated with vitamin A supplementation. Four random effects models were fitted, and the final model was chosen based on the lowest deviation value.
The null model’s ICC was 18.12%, indicating that 18.12% of the overall variability in Vitamin A supplementation uptake was due to cluster variation. Furthermore, the median odds ratio (MOR) for vitamin A supplementation uptake was 1.92, indicating variance between clusters. Those children aged 6–59 months in the cluster with higher vitamin A supplementation status had a 1.92 times higher likelihood of vitamin A supplementation than those in the cluster with lower vitamin A supplementation status. The best-fit model was selected based on the lowest deviation value (4751.16) (Table 5).
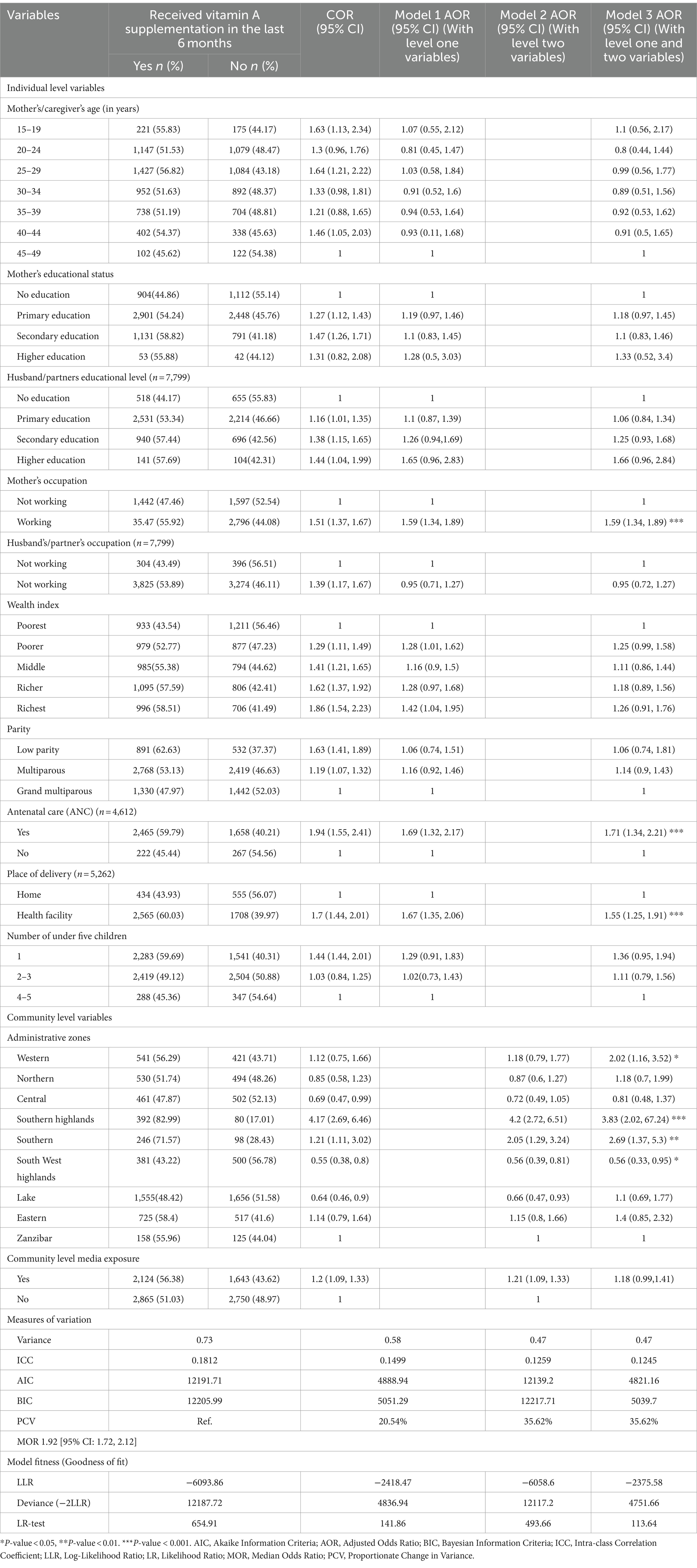
Table 5. Multilevel analysis of factors associated with vitamin A supplementation uptake among children aged 6–59 months in Tanzania.
Factors associated with vitamin A supplementation among children aged 6–59 months in Tanzania
Bivariable analysis was used to identify candidate variables for the multilevel multivariable mixed-effect binary logistic regression. As a result, mother’s/caregivers age, mother’s/caregiver’s educational status, husband’s educational status, mother’s/caregiver’s occupation, husband’s/partner’s occupation, wealth index, parity, ANC, place of delivery, number of under-five children, administrative zones, and community-level media exposure were associated with vitamin A supplementation. In the multilevel multivariable mixed effect binary logistic regression model, mother’s/caregiver’s occupation, ANC, place of delivery, and administrative zones were found to be statistically significant factors associated with vitamin A supplementation among 6–59-month-old children in Tanzania. The odds of having vitamin A supplementation among children with mother’s/caregiver’s who were working (employed) were found to be 1.59 times [AOR = 1.59, 95% CI: 1.34, 1.89], higher compared to those children with mother’s/caregiver’s who were not working. Children with mother’s/caregiver’s who had ANC follow-up were 1.71 times more likely [AOR = 1.71, 95%CI: 1.34, 2.22] to be vitamin A supplemented than those children with mother’s/caregiver’s who had no ANC follow-up. Children who were born in health facilities had 1.55 times more odds [AOR = 1.55, 95% CI: 1.25, 1.91] to be vitamin A supplemented than those children who were delivered at home. Regarding administrative zones, children living in Western, Southern highlands, and Southern administrative zones were 2.02 times [AOR = 2.02, 95% CI: 1.16, 3.52], 3.83 times [AOR = 3.83, 95% CI: 2.02, 7.24], and 2.69 times [AOR = 2.69, 95% CI: 1.37, 5.3] more likely to be vitamin A supplemented than children living in Zanzibar. Meanwhile, the odds of vitamin A supplementation in children living in the South West highlands were 44% less compared to children Zanzibar (Table 5).
Discussion
This study aimed at using the most recent 2022 Tanzania Demographic and Health Survey and Malaria Indicator Survey (2022 TDHS-MIS) data to investigate the level as well as the factors influencing VAS uptake among children aged 6–59 months in Tanzania. The study showed that only 53.18% [95% CI: 52.17, 54.19] of children aged 6–59 months had taken vitamin A supplementation in Tanzania. After adjusting for individual and community-level factors, mother’s/caregiver’s occupation, ANC, place of delivery of the current child, administrative zones, and community-level media exposure were significantly associated with vitamin A supplementation among children aged 6–59 months.
In this study, 53.18% of children have taken VAS, this finding is higher than studies conducted in Ethiopia among children aged 6–23 months reporting a vitamin A supplementation status of 47.2 and 43.4% (18, 25) and a study conducted in Guinea with a reported VAS status of 42% among children aged 6–59 months (27). This might be due to the difference in study population, in which this study considered children aged 6–59 months while the later studies took children aged 6–23 months. To the contrary, this study showed the status of vitamin A supplementation in Tanzania is below UNICEF’s target of 80%, a UNICEF report in 2022, which indicates a two-dose vitamin A supplementation coverage of 90% in Tanzania, and Tanzania’s 2018 nutrition survey report of 63.8% (13, 15, 16). These discrepancies might be attributed to the national VAS coverage based on a tally-sheet system, which can estimate vitamin A supplementation 30% higher than the actual coverage. Recent government data significantly overestimates VAS coverage. The huge difference in coverage percentages could be attributed to a number of factors, including health worker measurement errors in summarizing the count sheets and underestimating target population statistics (17, 28). It underscores the necessity to conduct representative population-based coverage surveys to supplement and validate tally-sheet estimations.
It was also found to be lower compared to a study conducted by including 23 Sub-Saharan countries that reported 59.4% vitamin A supplementation status (19). The possible explanation for this finding might be the difference in sociodemographic and economic status between these countries. This finding indicates Tanzania is lagging behind UNICEF’s target and the average of its fellow sub-Saharan countries, emphasizing the amount of work needed to reach the 80% target. Moreover, the finding of this study also revealed that the prevalence of VAS in Tanzania is lower than the reported prevalences of VAS in studies conducted in India and Pakistan among children aged 6–59, with reported nation coverages of 60.5 and 68.5%, respectively. The possible explanation for this difference could be the socioeconomic differences between the countries (29, 30).
This study identified significant individual and community-level factors that are associated with vitamin A supplementation. The odds of vitamin A supplementation among children aged 6–59 months with mother’s/caregiver’s who were working (employed) was found to be higher compared to those 6–59-month-old children with mother’s/caregiver’s who were not working. This finding is supported by a study conducted in Ethiopia where micronutrient uptake was found to be higher among children with mothers who had work compared to those with mothers who were not working, and a study about vitamin A supplementation among preschool children in Ethiopia (20, 25). The finding was also in line with studies conducted in Nigeria, Guinea and a multilevel analysis of 20 sub-Saharan African countries, where children with working mothers were found to be more likely to receive VAS than those without work (19, 27, 31). This might be explained as working mothers may have greater access to information about the benefits of VAS from colleagues at work or through community mobilization activities (20, 27).
Additionally, children with mother’s/caregiver’s who had ANC follow-up were more likely to be vitamin A supplemented than those children with mother’s/caregiver’s who had no ANC follow-up. This is also reported in studies conducted in Ethiopia (18, 20, 25, 32) and Nigeria (21). Moreover, children aged 6–59 months who were born in health facilities had a greater odd of being vitamin A supplemented than those children aged 6–59 months who were delivered at home. This finding is similar to a study conducted in Ethiopia and Nigeria, which found that health facility delivery increases the odds of VAS uptake (21, 32). The possible explanations might be that mothers who had ANC follow-up and health facility delivery may have received information, education, knowledge, and counseling from healthcare experts regarding the needs and importance of vitamin A supplementation (18, 21, 25). This underlines that strengthening pregnancy-related contact with health facilities is predicted to lead to increased usage of health services later on.
Regarding administrative zones, children aged living in the Western, Southern, and South West highlands were 2.05 times, 3.64 times, and 2.84 times more likely to be vitamin A supplemented than children living in Zanzibar. Meanwhile, the odds of vitamin A supplementation in children living in the South West Highlands were 44% less compared to children living in Zanzibar. The possible reasons might be that the regions with the highest prevalences of VAS were Njombe (91%) and Iringa (90%), which are both found in the southern highlands, while the regions with the lowest prevalences of VAS were Simiyu (19%) and Rukwa (20%), which are located in the South West highlands administrative zones. Further research is needed to understand the possible causes of variation among administrative zones.
Limitations
Even though this study used a weighted pooled nationally representative TDHS survey in Tanzania with a sample size large enough to detect the true effect of the independent variables as well as the use of multilevel binary logistic regression analysis to achieve credible estimates and standard errors, the study cannot establish a causal association between vitamin A supplementation and independent variables due to the use of a cross-sectional study design. Furthermore, due to its reliance on respondents’ answers, the study might be affected by social desirability and recall biases.
Conclusion
In general, the proportion of VAS among children in Tanzania is low compared to UNICEF’s target of 80%, with only one in two children taking vitamin A supplementation. This finding’s prevalence of VAS falls below the UNICEF 2022 report for Tanzania and Tanzania’s 2018 nutrition survey report, implying that the problem may be masked by recent reports of high coverage and that the situation is far from reality. Mother’s/caregiver’s working status, antenatal care, and place of delivery were positively associated individual-level factors with VAS. Besides, residing in the western, southern, and south-west highlands of Tanzania were found to be community-level factors associated with VAS. Therefore, interventions should be designed to improve the uptake of VAS among children whose mothers are currently not working. Provision and promotion of ANC and institutional delivery and strengthening of routine supplementation are recommended to increase coverage of childhood vitamin A supplementation, as ANC and institutional delivery were found to be positive factors affecting VAS. Moreover, special focus should be given to regions in the south-western highlands, and additional studies are necessary to investigate the root causes of regional variations in VAS.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found here: https://dhsprogram.com.
Ethics statement
The studies involving humans were approved by Medical Research Council of Tanzania and the Zanzibar Health Research Institute. The ICF’s Internal Review Board also reviewed the study. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
AG: Conceptualization, Formal analysis, Software, Supervision, Writing – original draft, Writing – review & editing. YA: Formal analysis, Software, Writing – original draft, Writing – review & editing. BW: Formal analysis, Software, Writing – original draft, Writing – review & editing. GK: Formal analysis, Software, Writing – original draft, Writing – review & editing. KH: Formal analysis, Software, Writing – original draft, Writing – review & editing. SD: Formal analysis, Software, Writing – original draft, Writing – review & editing. AT: Formal analysis, Software, Writing – original draft, Writing – review & editing. AA: Formal analysis, Software, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
We would like to thank the measure TDHS program for providing the datasets.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
AIC, Akaike Information Criteria; ANC, Antenatal Care; AOR, Adjusted Odds Ratio; BIC, Bayesian Information Criteria; CI, Confidence Interval; COR, Crude Odds Ratio; CSA, Central Statistical Agency; DHS, Demographic and Health Survey; EA, Enumeration Areas; LLR, Log-Likelihood Ratio; LR, Likelihood Ratio; MOR, Median Odds Ratio; PCV, Proportionate Change in Variance; TDHS, Tanzania Demographic and Health Survey; TDHS-MIS, Tanzania Demographic and Health Survey and Malaria Indicator Survey; ICC, Intra-class Correlation Coefficients; UNICEF, United Nations International Children’s Emergency Fund; USA, United States of America; VA, Vitamin A; VAS, Vitamin A supplements; WHO, World Health Organization.
Footnotes
References
1. Bar-El Dadon, S, and Reifen, R. Vitamin A and the epigenome. Crit Rev Food Sci Nutr. (2017) 57:2404–11. doi: 10.1080/10408398.2015.1060940
2. World Health Organization . Vitamin A supplementation 2023. Available at: https://www.who.int/teams/immunization-vaccines-and-biologicals/essential-programme-on-immunization/integration/linking-with-other-health-interventions/vitamin-a (accessed March 20, 2024)
3. Codjia, G . Food sources of vitamin A and provitamin A specific to Africa: an FAO perspective. Food Nutr Bull. (2001) 22:357–60. doi: 10.1177/156482650102200403
4. World Health Organization . Vitamin A deficiency. Available at: https://www.who.int/data/nutrition/nlis/info/vitamin-a-deficiency (accessed March 20, 2024)
5. Wirth, JP, Petry, N, Tanumihardjo, SA, Rogers, LM, McLean, E, Greig, A, et al. Vitamin A supplementation programs and country-level evidence of vitamin A deficiency. Nutrients. (2017) 9:190. doi: 10.3390/nu9030190
6. World Health Organization . Vitamin A supplementation in children 6–59 months of age with severe acute malnutrition 2023. Available at: https://www.who.int/tools/elena/interventions/vitamina-sam (accessed March 20, 2024)
7. Stevens, GA, Bennett, JE, Hennocq, Q, Lu, Y, De-Regil, LM, Rogers, L, et al. Trends and mortality effects of vitamin A deficiency in children in 138 low-income and middle-income countries between 1991 and 2013: a pooled analysis of population-based surveys. Lancet Glob Health. (2015) 3:e528–36. doi: 10.1016/S2214-109X(15)00039-X
8. Ndau, E, Mosha, T, Horton, S, and Laswai, H. Influence of vitamin A status on the anthropometric attributes of children aged 6-36 months in Tanzania. Tanzania J Agric Sci. (2018) 16
9. Mrimi, EC, Palmeirim, MS, Minja, EG, Long, KZ, and Keiser, J. Malnutrition, anemia, micronutrient deficiency and parasitic infections among schoolchildren in rural Tanzania. PLoS Negl Trop Dis. (2022) 16:e0010261. doi: 10.1371/journal.pntd.0010261
10. World Health Organization . Malnutrition 2024. Available at: https://www.who.int/news-room/factsheets/detail/malnutrition/ (accessed March 25, 2024)
11. Nutrition International . Improving child survival rates with twice-yearly vitamin A supplementation 2023. Available at: https://www.nutritionintl.org/project/vitamin-a-supplementation/ (accessed March 25, 2024)
12. Imdad, A, Mayo-Wilson, E, Haykal, MR, Regan, A, Sidhu, J, Smith, A, et al. Vitamin A supplementation for preventing morbidity and mortality in children from six months to five years of age. Cochrane Database Syst Rev. (2022) 2022:CD008524. doi: 10.1002/14651858.CD008524.pub4
13. UNICEF . Coverage at a crossroads: new directions for vitamin A supplementation programmes 2018. Available at: https://data.unicef.org/resources/vitamin-a-coverage/ (accessed March 26, 2024)
14. Ministry of Health CD, Gender, Elderly and Children (MoHCDGEC) [Tanzania, Mainland] MoHMZ, National Bureau of Statistics (NBS), Office of the Chief, Government Statistician (OCGS) aI . Tanzania Demographic and Health Survey and Malaria Indicator Survey (TDHS-MIS) 2015–16. Dar es Salaam, Tanzania, and Rockville, Maryland, USA: ICF (2016).
15. Ministry of Health CD, Gender, Elderly and Children (MoHCDGEC) [Tanzania, Mainland] MoHMZ, Tanzania Food and Nutrition Centre (TFNC), National Bureau of Statistics (NBS), Office of the Chief Government Statistician (OCGS) [Zanzibar] and UNICEF . Tanzania National Nutrition Survey using SMART Methodology (TNNS) 2018. Dar es Salaam, Tanzania (2018).
16. UNICEF . Key demographic indicators 2022. Available at: https://data.unicef.org/country/tza/ (accessed March 26, 2024)
17. Nyhus Dhillon, C, Subramaniam, H, Mulokozi, G, Rambeloson, Z, and Klemm, R. Overestimation of vitamin A supplementation coverage from district tally sheets demonstrates importance of population-based surveys for program improvement: lessons from Tanzania. PLoS One. (2013) 8:e58629. doi: 10.1371/journal.pone.0058629
18. Amare, T, Sime, T, Legese, GL, and Alemu, MB. A multilevel analysis of factors associated with vitamin A supplementation among children aged 6–35 months in Ethiopia. Front Public Health. (2023) 11:1052016. doi: 10.3389/fpubh.2023.1052016
19. Berde, AS, Bester, P, and Kruger, IM. Coverage and factors associated with vitamin A supplementation among children aged 6–59 months in twenty-three sub-Saharan African countries. Public Health Nutr. (2019) 22:1770–6. doi: 10.1017/S1368980018004056
20. Haile, D, Biadgilign, S, and Azage, M. Differentials in vitamin A supplementation among preschool-aged children in Ethiopia: evidence from the 2011 Ethiopian demographic and health survey. Public Health. (2015) 129:748–54. doi: 10.1016/j.puhe.2015.03.001
21. Dahiru, T, Liman, KH, Bashir, S, Suleiman, N, Zambuk, Z, Mu’azu, M, et al. Determinants of vitamin A uptake in Nigeria: the role of contextual factors. Journal of advances in medicine and medical. Research. (2018) 25:1–4. doi: 10.9734/JAMMR/2018/38536
22. Ministry of Health (MoH) [Tanzania Mainland] MoHMZ, National Bureau of, Statistics (NBS) OotCGSO, and ICF . Tanzania Demographic and Health Survey and Malaria Indicator Survey 2022 Final Report. Rockville, Maryland, USA: ICF. 2022 p.
23. The United Republic of Tanzania (URT) MoFaP, Tanzania, National Bureau of Statistics and President’s Office – Finance and Planning Oot, Chief Government Statistician Z . The 2022 population and housing census: administrative units population distribution report. Tanzania: Ministry of Finance and Planning, National Bureau of Statistics, Presidents’ Office – Finance and Planning Office of the Chief Government Statistician. (2022).
24. Croft, TN, Allen, CK, and Zachary, BW. Guide to DHS statistics. Rockville, Maryland, USA: ICF (2023). Available at: https://www.dhsprogram.com/pubs/pdf/DHSG1/Guide_to_DHS_Statistics_DHS-8.pdf
25. Gebremedhin, T, Aschalew, AY, Tsehay, CT, Dellie, E, and Atnafu, A. Micronutrient intake status and associated factors among children aged 6–23 months in the emerging regions of Ethiopia: a multilevel analysis of the 2016 Ethiopia demographic and health survey. PLoS One. (2021) 16:e0258954. doi: 10.1371/journal.pone.0258954
26. Hox, J, Moerbeek, M, and Van de Schoot, R. Multilevel analysis: Techniques and applications. New York: Routledge (2017).
27. Abdoulaye, S, Fatoumata Sekou, K, Sadou, S, Alpha Oumar, D, Jean Konan, K, Mamadou Oury, B, et al. Factors associated with vitamin A supplementation in children aged 6–59 months in Guinea: secondary analysis of 2018 demographic and health survey data. World J Public Health. (2024) 9:43–8.
28. Masanja, H, Schellenberg, JA, Mshinda, HM, Shekar, M, Mugyabuso, JKL, Ndossi, GD, et al. Vitamin A supplementation in Tanzania: the impact of a change in programmatic delivery strategy on coverage. BMC Health Serv Res. (2006) 6:142. doi: 10.1186/1472-6963-6-142
29. Kaustubh, B . Vitamin A supplementation among 9-59 month old children in India: geospatial perspectives and implications for targeted coverage. BMJ Glob Health. (2022) 7:e007972. doi: 10.1136/bmjgh-2021-007972
30. Changezi, F, and Lindberg, L. Socio-economic determinants of vitamin A intake in children under 5 years of age: evidence from Pakistan. J Hum Nutr Diet. (2017) 30:615–20. doi: 10.1111/jhn.12450
31. Aremu, O, Lawoko, S, and Dalal, K. Childhood vitamin A capsule supplementation coverage in Nigeria: a multilevel analysis of geographic and socioeconomic inequities. TheScientificWorldJOURNAL. (2010) 10:452878:1901–14. doi: 10.1100/tsw.2010.188
Keywords: Tanzania, Tanzania Demographic and Health Survey, vitamin A supplementation (VAS), multi-level analysis, under five children
Citation: Gebrekidan AY, Asgedom YS, Woldegeorgis BZ, Kassie GA, Haile KE, Damtew SA, Teklay A and Ayele AD (2024) Vitamin A supplementation status and associated factors among children aged 6–59 months in Tanzania: a multi-level analysis. Front. Nutr. 11:1422805. doi: 10.3389/fnut.2024.1422805
Edited by:
C. P. Yadav, ICMR-National Institute of Cancer Prevention and Research, IndiaReviewed by:
Ekta Gupta, National Institute of Cancer Prevention and Research (ICMR), IndiaJaspreet Kaur, Indian Council of Medical Research (ICMR), India
Kakoli Borkotoky, Indian Council of Medical Research (ICMR), India
Syed Shah Hussain, National Institute of Malaria Research (ICMR), India
Copyright © 2024 Gebrekidan, Asgedom, Woldegeorgis, Kassie, Haile, Damtew, Teklay and Ayele. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Amanuel Yosef Gebrekidan, YW1hbnVlbHlvc2VmNzdAZ21haWwuY29t; YW1hbnVlbHlvc2VmQHdzdS5lZHUuZXQ=
†ORCID: Amanuel Yosef Gebrekidan, http://orcid.org/0000-0003-0960-3759