 Sonali Randhawa1
Sonali Randhawa1 Manisha Choudhury2*
Manisha Choudhury2* Devika Gali Choudhary3
Devika Gali Choudhary3 Ramnath Ballala4Shailendra Hegde5
Ramnath Ballala4Shailendra Hegde5 Priyanka Barman6
Priyanka Barman6 Vishal Dogra7
Vishal Dogra7- 1Health Systems Transformation Platform, New Delhi, India
- 2Department of Food Science and Nutrition, College of Community Science, Assam Agricultural University, Jorhat, India
- 3Piramal Foundation, Hyderabad, India
- 4Bharatiya Vikas Trust, Manipal, India
- 5Piramal Swasthya Management and Research Institute, Hyderabad, India
- 6National Institute of Food Technology, Entrepreneurship and Management, Thanjavur (NIFTEM), Guwahati, India
- 7Bill & Melinda Gates Foundation, New Delhi, India
The knowledge, attitude, and practices (KAP) of mothers and frontline health workers (FLWs) regarding optimal Infant and Young Child Feeding (IYCF) are essential for mitigating undernutrition and associated morbidities among under-five children. The study assessed the KAP of mothers (of children aged 0–60 months) and FLWs regarding recommended IYCF practices, the association of mother’s KAP with their demographic characteristics and children’s nutritional outcomes, and the prevalence of stunting, wasting, and underweight among children aged 0–60 months in five high-focus districts of Assam. Data were collected from 389 mothers, 456 children, and 138 FLWs using a standard method. Of the 389 mothers, 29% had good KAP scores, 42% scored average, and 29% had poor KAP scores regarding IYCF practices. The mean KAP score increased significantly with improvements in variables such as community, language, education level, monthly income, and living conditions (p < 0.01). Less than half of the children were stunted (40%), one-third were affected by wasting (28%), and approximately 43% were underweight. Children whose mothers had a KAP score of less than 40% were 2.05 times more likely to experience stunting (CI = 1.04–4.02) than those whose mothers scored above 60%. Similar findings were reported for wasting and underweight. Of the 138 FLWs, 56% had good KAP scores, 30% had average scores, and 14% had poor scores. There was a noticeable gap in the KAP of the mothers regarding IYCF practices compared to that of FLWs. A comprehensive intervention plan to improve feeding practices can enhance the nutritional status of under-five children.
1 Introduction
Malnutrition is a critical public health concern influencing child morbidity and mortality, accounting for one-third (35%) of global deaths and two-thirds (68%) of deaths among under-five children in India (1). Globally, 25% (approximately 159 million) of under-five children are stunted, 16% are underweight (101 million), and 11% are wasted (52 million). South Asia has 38% of children who are stunted and 33% who are wasted, with India contributing significantly: 32.1% of children are underweight and 35.5% are stunted, largely due to chronic undernutrition (2–4).
Although India’s infant mortality rate has decreased from 89 per 1,000 live births (in 1990) to 28 (in 2020) per 1,000 live births, progress in managing undernutrition remains unsatisfactory. For instance, the rate of wasting changed only marginally from 19.8% (NFHS 2005–2006) to 19.3% (NFHS 2019–21) in the last decade (2, 5, 6). In Assam, a northeastern Indian state, the indicators are even more concerning: 35.3% of under-five children are stunted, 32.8% are underweight, 21.7% are wasted, and 9.1% are severely wasted, reflecting a decline compared to the 2015–16 NFHS data (2, 7, 8). Key nutrition indicators for India, Assam, and globally are provided in Table 1.
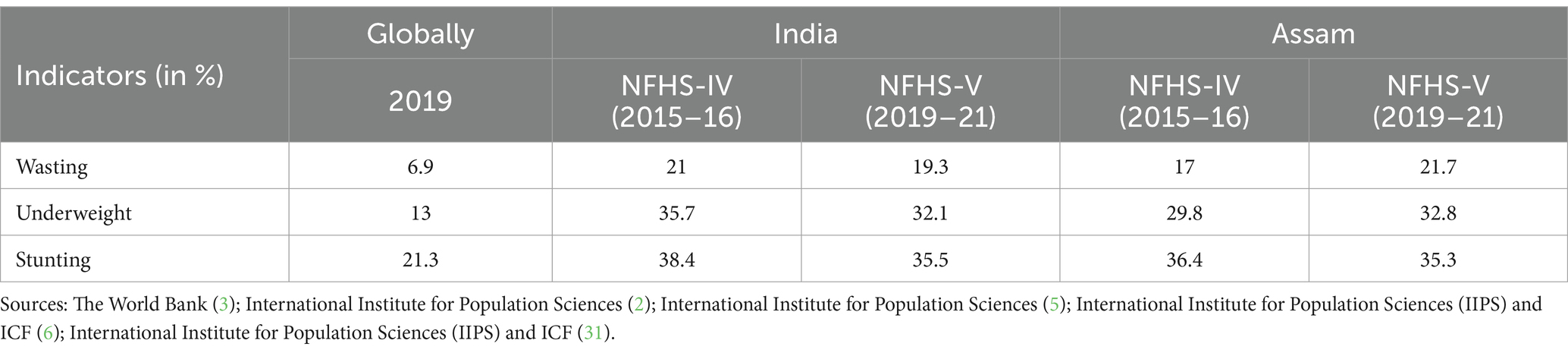
Table 1. Key nutrition indicators globally, in India, and in Assam.
The World Health Organization (WHO) recommends optimal Infant and Young Child Feeding (IYCF) practices to ensure adequate child growth and development. These recommendations include initiating breastfeeding within 1 h of birth, exclusive breastfeeding for the first 6 months and continuing for 2 years or more, and providing nutritionally adequate, age-appropriate complementary feeding after 6 months (9–11). Although the IYCF practices in India have improved, they remain below optimal standards. In Assam, only 49.1% of newborns are breastfed in a timely manner and 63.8% are exclusively breastfed for the first 6 months (5).
Optimal breastfeeding could reduce under-five mortality rates by 13–19%, with an additional 6% reduction from complementary feeding (9, 12, 13). Breastfeeding also offers benefits to mothers by lowering health risks and delaying the return of fertility (14). However, women in rural areas are often found lacking appropriate knowledge and compliance with IYCF practices, which places children at risk for adverse health outcomes (15–17). Cultural and traditional feeding practices, including poor attitudes and unhealthy IYCF practices by primary caregivers, also hinder child development (18, 19).
To address these challenges, the National Institution for Transforming India (NITI) Aayog launched the ‘Aspirational Districts Transformation (ADT)’ program in 2018, targeting 115 underperforming districts across 24 states (20). The program focuses on health, nutrition, education, and various other sectors to track and improve outcomes. The Piramal Foundation also supported its implementation in 25 aspirational districts (including 5 in Assam) to enhance health and nutrition indicators.
1.1 Objectives
In our study, we assessed the following: (i) the knowledge, attitude, and practices (KAP) of mothers (of children aged 0–60 months) regarding recommended IYCF practices and their association with demographic characteristics and children’s nutritional outcomes; (ii) prevalence of stunting, wasting, and underweight among 0–60-months-old children; and (iii) the KAP of frontline workers (FLWs) regarding recommended IYCF practices in five districts of Assam.
2 Materials and methods
2.1 Study settings
The study was conducted in five high-focus, aspirational districts of Assam, namely Baksa (population: 988,247; health blocks: 6); Barpeta (population: 1,772,211; health blocks: 7); Darrang (population: 996,915; health blocks: 4); Dhubri (population: 2,069,000; health blocks: 7), and Goalpara (population: 1,057,927; health blocks: 6) (21). These districts have poor nutrition indicators, with high rates of stunting (48.5% in Dhubri) and underweight prevalence (37.8% in Dhubri), compared to the state averages (stunting: 35.3%; underweight: 32.8%) and national averages (stunting: 35.5%; underweight: 32.1%) (5, 7, 8). The key nutrition indicators for all five districts are provided in Table 2, based on the NFHS-5 (2019–21) data.

Table 2. Key nutrition indicators of all five aspirational districts of Assam.
2.2 Sampling method and sample size
A cross-sectional study was conducted over 3 months, from April to June 2019. A multi-stage sampling technique was employed for the selection of the participants. In the first stage, a total of 10 blocks, 2 blocks from each of the 5 districts, were randomly selected to ensure adequate representation of the districts. In the second stage, 10 villages per block that conduct regular Village Health Sanitation and Nutrition Days (VHSNDs) were randomly selected. In the third stage, the sample population attending the VHSNDs and fulfilling the inclusion criteria was selected. The sample size of mothers and children was calculated using Open Epi version 3.01. Among the five districts, Dhubri recorded the highest prevalence of children under 3 years of age who were breastfed within 1 h of birth (57.9%) (8). Considering this prevalence, a design effect of 1.5, a precision of 5%, and a non-response rate of 10%, we calculated a sample of 398 mothers to obtain statistically significant results. Similarly, we estimated a sample size of 440 for children aged 0–60 months using a 26.2% prevalence of underweight from Barpeta (7). A total of 94 VHSNDs across the 10 health blocks were visited to collect data from 389 mothers, 456 children, and 138 frontline workers.
2.3 Study participants
Inclusion criteria: All women residing in the aforementioned five aspirational districts of Assam, primigravida and multigravida women, and mothers with children aged 0–60 months, who attended the VHSNDs in the selected villages. It also included female FLWs who were involved in community health, such as Accredited Social Health Activists (ASHA) or Anganwadi workers, who conducted the VHSNDs and consented to participate in the study. Exclusion criteria: Mothers or FLWs who refused to participate in the study were excluded, even if they satisfied the inclusion criteria.
2.4 Study variables
Outcome variables: The primary outcome variable (s) were the knowledge, attitude, and practices (KAP) of the mothers regarding infants and young child feeding practices. The interview schedule included 43 questions to assess the knowledge (13), attitude (10), and practices (20), based on the WHO infant and child feeding guidelines (11). If a person answered all questions correctly, they were awarded 43 scoring points. The total KAP score was categorized as good (correct answers ≥60%), average (correct answers between 40 and 59%), and poor (correct answers <40%) (22). The knowledge questions were scored with one point for correct answers and zero for wrong or uncertain responses, with a score range from 13 to 0. Individuals with more than seven correct answers (≥60%) were considered to have good knowledge of IYCF, while those with seven or fewer correct answers were considered to have poor knowledge. Attitude was assessed using a Likert scale ranging from −2 (strongly disagree) to +2 (strongly agree), with a total score ranging from a maximum of +20 to a minimum of −20. An attitude score greater than 11 (≥60%) was considered good, while a score of 11 or less was considered poor. For practices, the score range was from a maximum of +20 to a minimum of 0, with one point awarded for correct responses and zero for wrong or uncertain responses. Practices were classified as good with a score greater than 11 and as poor with a score of 11 or less. Anthropometric measurements were recorded to assess nutritional outcomes among the children aged 0–60 months, including (i) wasting (weight-for-height below −2 SD), (ii) stunting (height-for-age below −2 SD), and (iii) underweight (weight-for-age below −2 SD).
Predictor variables: Predictor variables were selected based on our previous knowledge of the factors affecting the knowledge, attitude and practices of the mothers regarding IYCF practices, such as sociodemographic variables (family size, socioeconomic status, religion, etc.) and environmental conditions (sanitation, drinking water, etc.).
2.5 Data collection
Data collection was conducted using an interviewer-administered, structured, and semi-structured interview schedule, along with an existing validated questionnaire on Infant Young and Child Feeding practices by the World Health Organization. This questionnaire was translated into the native language of the respondents to gather relevant sociodemographic characteristics, as well as the knowledge, attitude and practices of the mothers regarding IYCF. Trained staff collected anthropometric measurements of the children’s weight (kg), height (cm), and mid-upper arm circumference (MUAC) (cm). The interview schedule was pretested among 15 respondents before administering it for the data collection. These samples were not included in the main data analysis. The data obtained from the participants were kept confidential and anonymous.
2.6 Data analysis
The data analysis was conducted using licensed IBM SPSS statistics version 25 (23). All categorical variables were presented as frequencies and percentages, and all continuous variables were presented as mean ± standard deviation. The association between the demographic features and the mean knowledge, attitude, and practices scores was analyzed using one-way ANOVA to determine the level of significance. A p-value of less than 0.05 was considered statistically significant. The internal consistency of the mothers’ responses to the questions on knowledge, attitude, and practices regarding IYCF practices was assessed using Cronbach’s alpha reliability coefficient. A reliability coefficient of 0.70 or higher was considered “acceptable.” The association between stunting (below −2 SD), wasting (below −2 SD), and underweight (below −2 SD) and the mother’s KAP was assessed using the odds ratio (24, 25).
2.7 Ethical approval
The Institutional Ethics Committee of Piramal Swasthya Management and Research Institute (PSMRI) approved the study (IEC Study Ref No: PSMRI/2019/12). The purpose of the study was explained to participants and the Participant Information Sheet was provided in the native language of the respondent (Assamese for the study). The signed informed consent was obtained before enrolling the participants into the study.
3 Results
A total of 389 mothers with children aged 0–60 months participated in the study. The mean age of the mothers was 25.5 (± 5.1) years. The majority (70%) of the mothers were from the Muslim community, and more than half of them (54%) had completed schooling up to high school (class 10). The mean family size was 5.8 members (± 3.5), with an average monthly earning of INR 11,591 (± 6,611). Only one-fifth (22%) lived in pucca houses, and almost all households (97%) had access to a toilet, either kaccha or sanitary. The sociodemographic characteristics of the mothers are provided in Table 3.
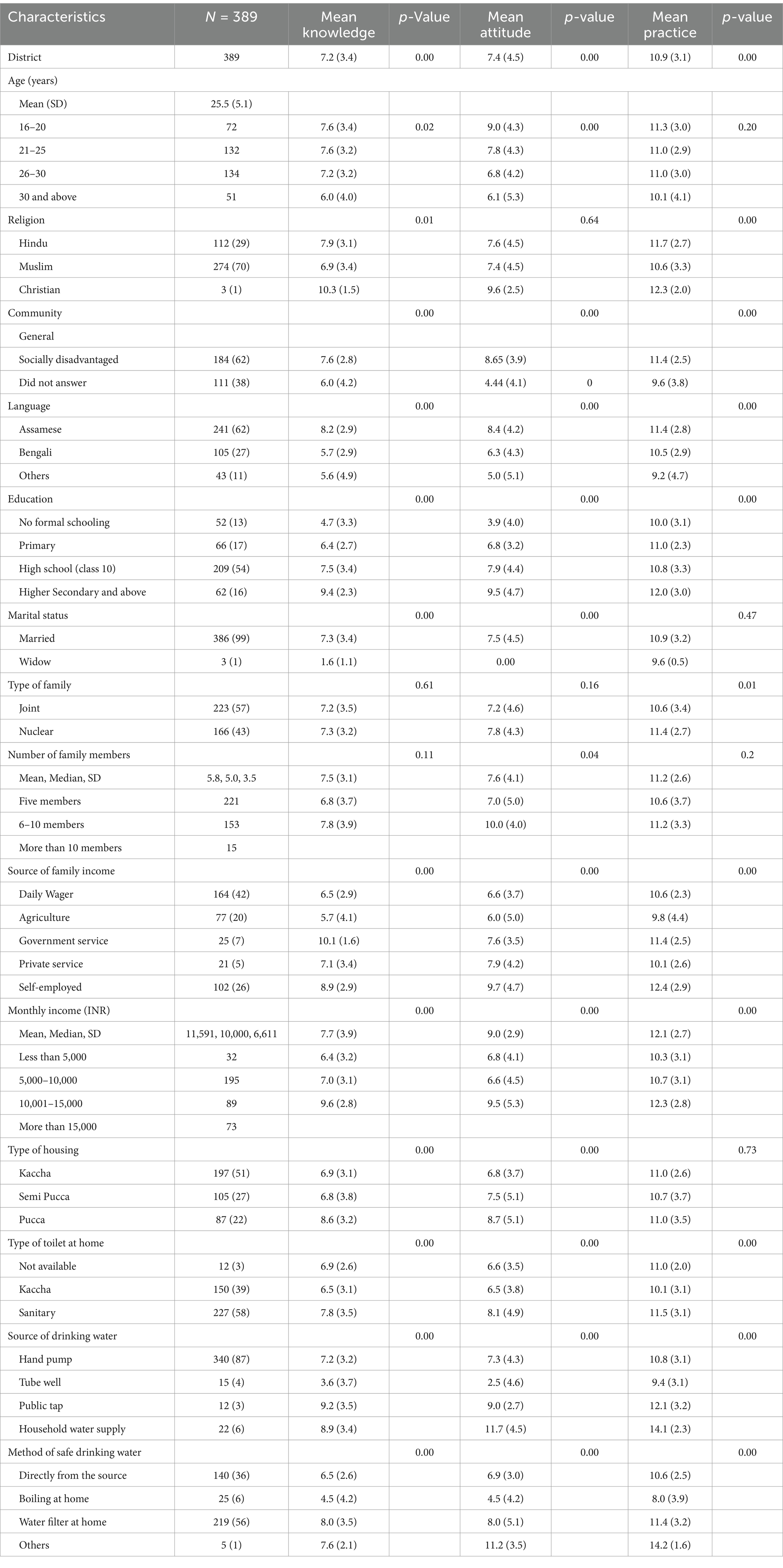
Table 3. Comparison of the sociodemographic characteristics of the mothers with the mean KAP scores.
The Cronbach’s alpha reliability coefficient was in the range of 0.81 (knowledge), 0.84 (attitude), and 0.63 (practices). The overall reliability coefficient for the 43 questions on the mothers’ KAP regarding IYCF was 0.89. Of the 389 participants, 112 (29%) had good knowledge, attitude, and practices, whereas 162 (42%) had average KAP and the remaining 115 (29%) had poor KAP regarding IYCF practices. The mean KAP scores increased significantly with improvements in variables such as community, language, education level, source of family income, monthly income, type of toilet at home, source of drinking water, and method of safe drinking water (p < 0.01). A comparison of the sociodemographic characteristics of the mothers with the mean KAP scores is provided in Table 3.
Of the 456 children aged 0–60 months whose anthropometric measurements were taken, 52% were male individuals and 48% female individuals, with a mean age of 20 (±15) months, an average weight of 8.7 (±2.9) kg, and a mean length of 73 (±15) cm. Approximately less than half of the children were stunted (40%, 185/456), one-third had wasting (28%, 127/456), and approximately 43% were underweight (43%, 96/456), all below −2 standard deviations, according to the WHO standards. The nutritional status of the children (0–60 months) is provided in Table 4.
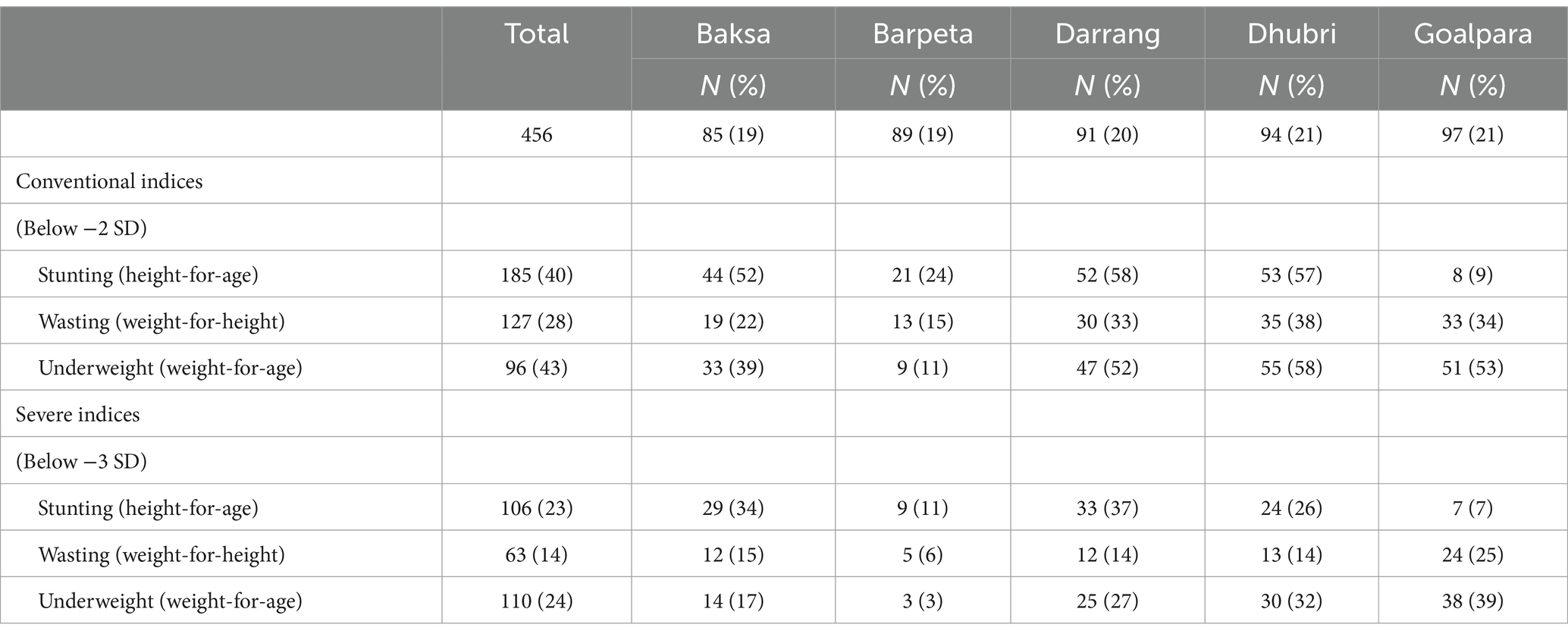
Table 4. Nutritional status of the children (0–60 months).
The odds of developing stunting, wasting, and underweight among the children aged 0–60 months increased as their mother’s knowledge, attitude and practices regarding appropriate IYCF practices declined. The odds of the children developing stunting were 2.05 (CI = 1.04–4.02) times higher when their mothers’ KAP score regarding IYCF optimal practices was less than 40%, compared to those whose mothers scored more than 60%. Similar findings were reported for wasting (OR = 2.01, 0.93–4.35) and underweight (OR = 2.93, 1.47–5.85) for the mother whose KAP score was less than 40% compared to those who scored more than 60%. The association between the children’s stunting, wasting, and underweight and the mothers’ KAP score is provided in Table 5.
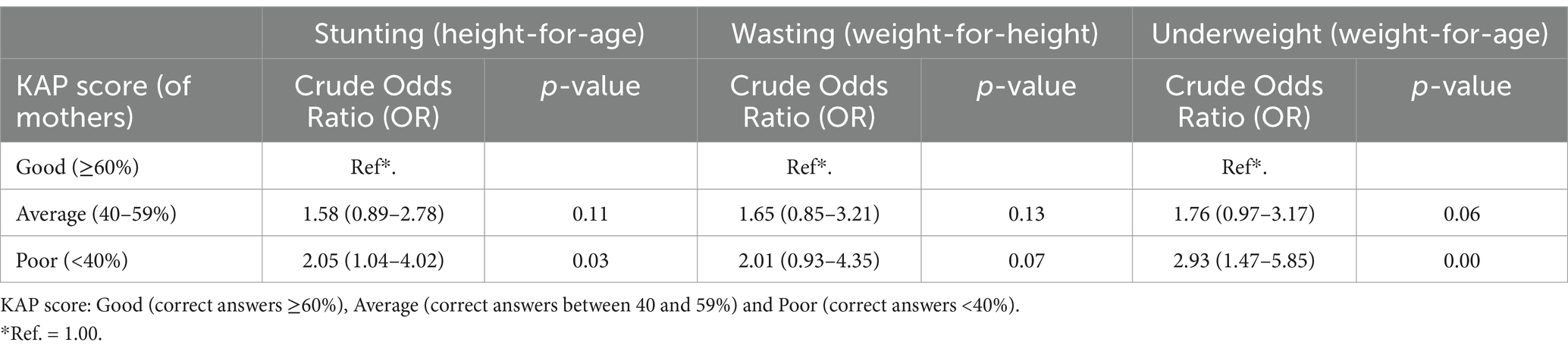
Table 5. Association between stunting, wasting, and underweight (below −2 SD) in the children (aged 0–60 months) and the KAP score of their mothers (N = 259).
Of the total 138 FLWs, only 56% had good KAP scores regarding IYCF, followed by 30% with average scores and 14% with poor scores. Of the 389 mothers, 29% displayed good KAP scores, 42% had average scores, and 29% had poor scores. The KAP scores of the mothers and FLWs regarding IYCF practices are presented in Figure 1. It could be seen that the KAP of the FLWs and mothers varied widely. Despite 56% of the FLWs demonstrating good knowledge of IYCF practices, it appeared that only 29% of the mothers received this knowledge from the FLWs. Except for Baksa and Barpeta, the other three districts, where the minority population is high, showed a significant difference between the KAP of the FLWs and the mothers. Specifically, in Darrang, the difference was 26% for the FLWs and 8% for the mothers; in Dhubri, it was 44% for the FLWs and 17% for the mothers; and in Goalpara, it was 60% for the FLWs and 17% for the mothers.

Figure 1. KAP scores of the mothers and FLWs regarding IYCF practices.
4 Strengths and limitations
There is a lack of literature on the knowledge, attitude, and practices of mothers regarding Infant and Young Child Feeding in Assam. The strength of the study lies in the fact that we collected a sample from five different districts of Assam, which are high-priority and aspirational and have some of the poorest child nutritional indicators. There are 115 aspirational districts in India based on the composite index score (18). The findings of the present study may be applicable to other districts with similar poor health and nutrition indicators but may not be generalized to other districts of Assam.
There is a possibility of recall bias among the older mothers. The study findings will be useful for redesigning the mode of imparting programs or languages used in delivering nutrition interventions and behavior change interventions. In addition, the study provides insights into the association between a child’s nutritional outcomes and the mother’s KAP regarding IYCF practices, considering sociodemographic, maternal, and sanitation factors.
5 Conclusion
There is a noticeable gap in the overall knowledge, attitude and practices of the mothers of children aged 0–60 months regarding appropriate IYCF practices. These are high-priority districts in the state of Assam, with the highest levels of undernutrition, especially stunting. The present study highlights that nutritional information regarding IYCF practices is influenced by the education, language, living conditions, and economic status of the caregiver and has a positive impact on the health status of children (26–29). Despite having good knowledge, a mother may have a poor attitude toward following standard IYCF practices.
Suggestions: There is an urgent need for strategic information, education, and communication (IEC) activities focusing on social and behavioral change communication (SBCC) to improve both acute and chronic outcomes of childhood nutrition. It is important to note that, although the entire family was involved in the process of child feeding, none of the members were aware of the recommended guidelines. Extensive awareness interventions for all family members, along with primary caregivers, regarding IYCF practices are essential. The SBCC program for interfaith leaders had some success in bringing about a change in the community’s acceptance of health programs (30). The same strategy can be used to educate family members alongside mothers. Teenage pregnancy is also one of the key concerns in Assam. Specific interventions targeting adolescent girls should be explored to bridge the gaps in IYCF practices. The involvement of community health workers at the peripheral level is crucial for conducting continued sensitization workshops.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by The Institutional Ethics Committee of Piramal Swasthya Management and Research Institute (PSMRI) approved the study (IEC Study Ref No: PSMRI/2019/12). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
SR: Conceptualization, Formal analysis, Writing – original draft. MC: Data curation, Investigation, Methodology, Supervision, Writing – review & editing. DC: Writing – review & editing. RB: Writing – review & editing. SH: Supervision, Writing – review & editing. PB: Writing – review & editing, Validation. VD: Formal analysis, Resources, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. The study was funded by the Piramal Foundation, a not-for-profit organization. This was part of the Aspirational Districts Transformation (ADT) program under the National Institution for Transforming India (NITI) Aayog, Government of India initiative.
Acknowledgments
The authors are grateful to the field staff of Piramal Foundation for their support during data collection, coordination, and other field-level activities while conducting the survey in the aspirational districts of Assam. The authors also thank Piramal Foundation for their financial and technical support. In addition, the authors would like to thank the participants who took part in the study, without whom the research would not have been possible.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. India State-Level Disease Burden Initiative Malnutrition Collaborators. The burden of child and maternal malnutrition and trends in its indicators in the states of India: the global burden of disease study 1990–2017. Lancet Child Adolescent Health. (2019) 3:855–70. doi: 10.1016/s2352-4642(19)30273-1
2. International Institute for Population Sciences. National Family Health Survey - 5, 2019-21 India fact sheet In: Ministry of Health and Family Welfare (2020). Available at: https://mohfw.gov.in/sites/default/files/NFHS-5_Phase-II_0.pdf
3. The World Bank. Prevalence of underweight, weight for age (% of children under 5). (2019). Available at: https://data.worldbank.org/indicator/SH.STA.MALN.ZS (Accessed January 09, 2024).
4. United Nations Children’s Fund. Improving child nutrition: the achievable imperative for global Progress. In Division of Communication, UNICEF. (2013).
5. International Institute for Population Sciences. National Family Health Survey 5: State and districts of Assam: Compendium of fact sheets - Assam, India In: Ministry of Health and Family Welfare (2021). Available at: https://nhm.assam.gov.in/documents-detail/national-family-health-survey-5-2019-20
6. International Institute for Population Sciences. National Family Health Survey (NFHS -4), 2015-16: India In: Ministry of Health and Family Welfare (2017). Available at: https://www.nfhsiips.in/nfhsuser/nfhs4.php
7. International Institute for Population Sciences. National Family Health Survey - 5: District fact sheet: Barpeta, Assam In: Ministry of Health and Family Welfare (2021) Available at: https://mohfw.gov.in/sites/default/files/NFHS-5_Phase-II_0.pdf
8. International Institute for Population Sciences. National Family Health Survey - 5: District fact sheet: Dhubri, Assam In: Ministry of Health and Family Welfare (2021) Available at: https://nhm.assam.gov.in/sites/default/files/swf_utility_folder/departments/nhm_lipl_in_oid_6/menu/document/dhubri_1.pdf
9. Patel, DV, Bansal, SC, Nimbalkar, AS, Phatak, AG, Nimbalkar, SM, and Desai, RG. Breastfeeding practices, demographic variables, and their association with morbidities in children. Adv Prev Med. (2015) 2015:1–9. doi: 10.1155/2015/892825
10. Tessema, M, Belachew, T, and Ersino, G. Feeding patterns and stunting during early childhood in rural communities of Sidama South Ethiopia. Pan Afr Med J. (2013) 14:75. doi: 10.11604/pamj.2013.14.75.1630
11. World Health Organization. Infant and young child feeding. Model Chapter for textbooks for medical students and allied health professionals. (2011). Available at: https://www.who.int/publications/i/item/9789241597494 (Accessed December 12, 2023).
12. Kushwaha, KP, Sankar, J, Sankar, MJ, Gupta, A, Dadhich, JP, Gupta, YP, et al. Effect of peer counselling by mother support groups on infant and young child feeding practices: the Lalitpur experience. PLoS One. (2014) 9:e109181. doi: 10.1371/journal.pone.0109181
13. Saaka, M. Relationship between mothers’ nutritional knowledge in childcare practices and the growth of children living in impoverished rural communities. J Health Popul Nutr. (2014) 32:237–48.
14. Collaborative Group on Hormonal Factors in Breast Cancer. Breast cancer and breastfeeding: collaborative reanalysis of individual data from 47 epidemiological studies in 30 countries, including 50302 women with breast cancer and 96973 women without the disease. Lancet. (2002) 360:187–95. doi: 10.1016/S0140-6736(02)09454-0
15. Masare, MS, Soyam, G, and Hiwarkar, PA. A cross-sectional study of determinants and impact of breastfeeding and complementary feeding practices on nutritional status and common illnesses among infants in urban slum. Int J Res Med Sci. (2017) 5:4563–6. doi: 10.18203/2320-6012.ijrms20174597
16. Tariqujjaman, M, Hasan, MM, Mahfuz, M, Hossain, M, and Ahmed, T. Association between mother’s education and infant and young child feeding practices in South Asia. Nutrients. (2022) 14:1514. doi: 10.3390/nu14071514
17. Assefa, DG, Woldesenbet, TT, Molla, W, Zeleke, ED, and Simie, TG. Assessment of knowledge, attitude and practice of mothers/caregivers on infant and young child feeding in Assosa Woreda, Assosa zone, Benshangul Gumuz region, Western Ethiopia: a cross-sectional study. Arch Public Health. (2021) 79:1–10. doi: 10.1186/s13690-021-00690-5
18. Demilew, YM. Factors associated with mothers’ knowledge on infant and young child feeding recommendation in slum areas of Bahir Dar City, Ethiopia: cross sectional study. BMC Res Notes. (2017) 10:191. doi: 10.1186/s13104-017-2510-3
19. Lutter, CK, Daelmans, BMEG, De Onis, M, Kothari, MT, Ruel, MT, Arimond, M, et al. Undernutrition, poor feeding practices, and low coverage of key nutrition interventions. Pediatrics. (2011) 128:e1418–27. doi: 10.1542/peds.2011-1392
20. Government of India. Transformation of aspirational districts. Vikaspedia, Ministry of Electronics and Information Technology Initiative. (2018). Available at: https://vikaspedia.in/social-welfare/rural-poverty-alleviation-1/transformation-of-aspirational-districts (Accessed December 14, 2023).
21. Census Population. Population census. (2011). Available at: https://www.census2011.co.in/ (Accessed January 09, 2024).
22. Mahanta, LB, Choudhury, M, Borthakur, S, Bhagabati, R, and Gogoi, P. Can communication media improve the KAP status of frontline health workers? A cross-sectional study on MCH indicators from Assam, India. South East Asia J Public Health. (2015) 5:57–64. doi: 10.3329/seajph.v5i2.28314
24. StataCorp, LLC. STATA Base reference manual: release 15 (revision 1) A Stata Press Publication (2017). Available at: https://www.stata.com/manuals17/r.pdf
25. Taber, KS. The use of Cronbach’s alpha when developing and reporting research instruments in science education. Res Sci Educ. (2018) 48:1273–96. doi: 10.1007/s11165-016-9602-2
26. Chattopadhyay, D, Chakraborty, S, Dasgupta, A, and Das, N. Infant and young child feeding perceptions and practices among mothers in a rural area of West Bengal, India. Ann Med Health Sci Res. (2013) 3:370–5. doi: 10.4103/2141-9248.117955
27. Malhotra, N. Inadequate feeding of infant and young children in India: lack of nutritional information or food affordability? Public Health Nutr. (2013) 16:1723–31. doi: 10.1017/S1368980012004065
28. Meshram, II, Mallikharjun Rao, K, Balakrishna, N, Harikumar, R, Arlappa, N, Sreeramakrishna, K, et al. Infant and young child feeding practices, sociodemographic factors and their association with nutritional status of children aged <3 years in India: findings of the National Nutrition Monitoring Bureau survey, 2011-2012. Public Health Nutr. (2019) 22:104–14. doi: 10.1017/S136898001800294X
29. Chatterjee, K, Sinha, RK, Kundu, AK, Shankar, D, Gope, R, Nair, N, et al. Social determinants of inequities in under-nutrition (weight-for-age) among under-5 children: a cross sectional study in Gumla district of Jharkhand, India. Int J Equity Health. (2016) 15:1–9. doi: 10.1186/s12939-016-0392-y
30. Aruldas, K, Khan, M, and Hazra, A. Increasing appropriate complementary feeding in rural Uttar Pradesh. J Fam Welf. (2010) 56:51–6.
Keywords: IYCF practices, knowledge, attitude, practices, undernutrition, aspirational districts, Assam
Citation: Randhawa S, Choudhury M, Choudhary DG, Ballala R, Hegde S, Barman P and Dogra V (2024) Influence of mothers’ and frontline health workers’ knowledge, attitude, and practices on infant and young child feeding and child nutrition: a cross-sectional study in aspirational districts of Assam, India. Front. Nutr. 11:1413867. doi: 10.3389/fnut.2024.1413867
Edited by:
Alexandru Rusu, Biozoon Food Innovations GmbH, GermanyReviewed by:
Abiola O. Oduwole, University of Lagos, NigeriaTeresa Abbattista, Senigallia Hospital, Italy
Copyright © 2024 Randhawa, Choudhury, Choudhary, Ballala, Hegde, Barman and Dogra. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Manisha Choudhury, bWFuaXNoYS5jaG91ZGh1cnlAYWF1LmFjLmlu