 Ling Yin
Ling Yin Feng Liang2
Feng Liang2 Xin Wei
Xin Wei- 1Department of Obstetrics and Gynecology, The Affiliated Changsha Central Hospital, Hengyang Medical School, University of South China, Changsha, China
- 2Gynecology Department, The Reproductive Hospital of Guangxi Zhuang Autonomous Region, Nanning, China
- 3Gynecology Department, The First People’s Hospital of Nanning, Nanning, China
Background: Endometriosis is a multifaceted disorder with genetic, immune, inflammatory, and multifactorial origins. Vitamin B6 serves as a pivotal coenzyme in various metabolic pathways involving lipids, hemes, nucleic acids, proteins, and carbohydrates. Dysregulation or deficiency of vitamin B6 can perturb human physiology. However, the relationship between dietary vitamin B6 and endometriosis remains elusive. This study aims to explore how dietary intake of vitamin B6 is associated with the risk of endometriosis.
Methods: Using cross-sectional data from the National Health and Nutrition Examination Survey, we analyzed information from American women aged 20–54 years between 1999 and 2006. After adjusting for relevant covariates, multivariable logistic regression analysis was employed to evaluate correlations.
Results: A total of 4,453 women were included in the study. The multiple linear regression model revealed a positive association between dietary vitamin B6 intake and the risk of endometriosis, even after controlling for confounding variables. Compared to individuals with lower vitamin B6 consumption (Q1: <0.94 mg/day), the adjusted odds ratio (OR) values for dietary vitamin B6 intake and endometriosis in Q2 (0.95–1.39 mg/day), Q3 (1.40–1.99 mg/day), and Q4 (>1.90 mg/day) were 1.22 (95% CI: 0.88–1.69, p = 0.23), 1.22 (95% CI: 0.86–1.73, p = 0. 279), and 1.51 (95% CI, 1.01–2. 24, p = 0.04), respectively.
Conclusion: Our findings suggest a positive correlation between endometriosis and dietary vitamin B6 intake. Further investigations are imperative to establish a causal relationship between dietary vitamin B6 intake and endometriosis.
Introduction
Endometriosis is an inflammatory condition characterized by the ectopic growth of endometrial-like tissue outside the uterus, often affecting pelvic organs (1). It affects around 176 million women globally, leading to symptoms such as pelvic pain and infertility in 5–10% of cases (2). Those affected typically incur double the healthcare costs compared to unaffected individuals (3), making it a significant public health concern (4). Despite its impact, there is limited understanding of modifiable risk factors associated with its development.
Vitamin B6, a water-soluble vitamin found naturally in various foods, is involved in numerous metabolic processes as a coenzyme (5). It exists in three forms: pyridoxamine, pyridoxal, and pyridoxine, with pyridoxal-phosphate (PLP) being the active form. Vitamin B6 also plays a role in the immune and endocrine systems and has antioxidant properties (6, 7). Studies have suggested that vitamin B6 deficiency may increase the risk of various cancers, while adequate levels might reduce the risk, although findings are mixed (8–13). There is also evidence linking high doses of vitamin B6 with bone issues and other health concerns (14–16). Despite these associations, its potential protective effects against conditions like depression, cardiovascular disease, and cognitive decline remain unconfirmed (17–19).
The biological behaviors of endometriosis and malignancies, particularly in pathways regulating inflammation and cell proliferation, indicate a potential role for vitamin B6 in modulating these processes (20). Limited research has explored the relationship between dietary vitamin B6 and endometriosis. One study reported lower vitamin B6 levels in patients with advanced endometriosis (21). This study seeks to investigate the association between dietary vitamin B6 intake and endometriosis in a large sample of American women aged 20 to 54, aiming to offer new insights into potential preventive strategies.
Methods
Data source
The National Health and Nutrition Examination Survey (NHANES) and the National Center for Health Statistics (NCHS) played essential roles in collecting data for this investigation. We acquired data from three consecutive 2-year NHANES cycles conducted between 1999 and 2006, utilizing a nationally representative stratified sample through interviews and physical examinations. The NCHS Ethics Review Committee granted ethical approval, and all subjects provided signed informed consent.
Study design and population
The original dataset included 5,557 female participants. After excluding individuals with missing endometriosis-related information and those outside the age range of 20 to 54 years, our final study population comprised 4,453 women. Among them, 337 were diagnosed with endometriosis, while 4,116 were not. Exclusions were made for 991 pregnant women and 113 individuals lacking information on dietary vitamin B6 intake. Figure 1 provides a detailed illustration of the inclusion and exclusion process.
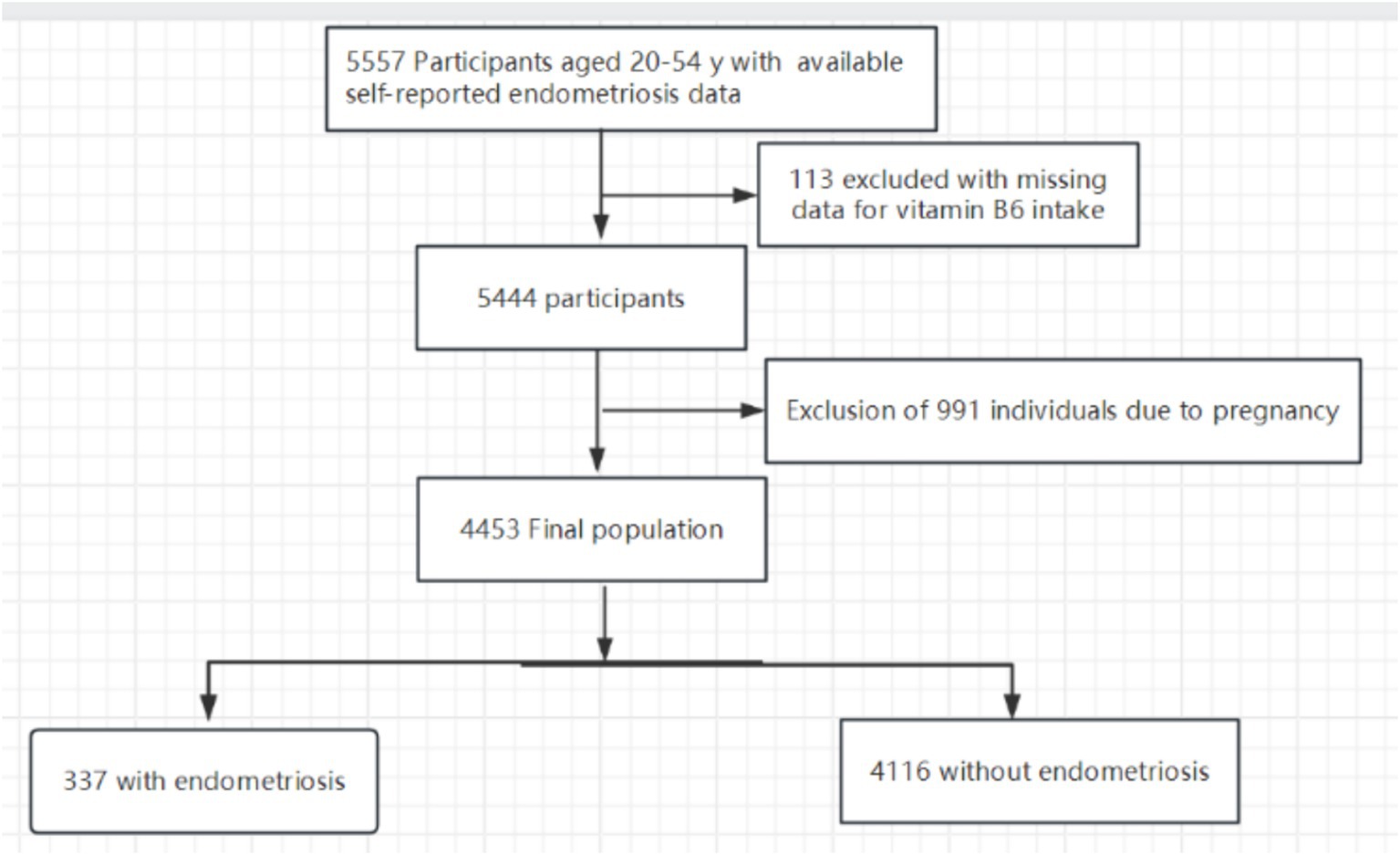
Figure 1. The study’s flow diagram.
Participants and definition
We determined endometriosis based on participants’ responses to a specific question in the reproductive health questionnaire: “Has a doctor or other health professional ever diagnosed you with endometriosis?” We categorized those who answered affirmatively as patients. Professional interviewers assessed dietary vitamin B6 consumption during the NHANES dietary survey, a component of the “What We Eat in America” survey, conducted at the Mobile Examination Center (MEC) using a 24-h recall method. The NHANES computer-assisted dietary interview (CADI) system recorded participants’ food and beverage intake from the 24 h preceding the interview.
According to the study procedure, we randomly assigned participants to data collection sessions that occurred in the morning, afternoon, or evening. We determined dietary vitamin B6 and nutrient consumption using the US Department of Agriculture Survey Nutrients Database and the University of Texas Food Intake Analysis System. We excluded pharmaceuticals and dietary supplements from the nutritional calculations. We conducted two 24-h dietary recall interviews, followed by a phone interview 3 to 10 days later. We selected the first interview, conducted in person at the MEC, for analysis, as the 24-h recall method is the most commonly used in large-scale surveys (22).
Measurements
In our study, we considered a wide range of covariates sourced from the literature (23–25), including Age, marital status, race/ethnicity, education level, family income, smoking status, physical activity, BMI, alcohol consumption, use of birth control pills, high blood pressure, diabetes, coronary heart disease, chronic bronchitis, caloric consumption, total fat intake, total cholesterol intake, and usage of nutritional supplements. We categorized race and ethnicity into Non-Hispanic White, non-Hispanic Black, Mexican American, and other races. We classified marital status as either living with a partner or living alone. We stratified educational attainment into three levels: fewer than 9, 9 to 12 years, and more than 12 years. We assessed family income using the Poverty Income Ratio (PIR) and categorized it into low, medium, and high income, based on ranges from 1.3 to 3.5, according to the US government’s Agriculture report (26). We dichotomized smoking status into smokers and never smokers (those who have smoked fewer than 100 cigarettes in total). Alcohol drinking status was determined by the survey question, “In any 1 year, have you had at least 12 drinks of any type of alcoholic beverage?” Participants who answered “yes” were defined as alcohol drinkers. We divided physical activity levels into three categories: unable to perform physical activity, moderate (defined as at least 10 min of movement within the previous 30 days resulting in light perspiration or a mild to moderate increase in respiration or heart rate), and vigorous (at least 10 min of activity within the last 30 days resulting in profuse sweating or an increased heart rate). The determination of previous disease (high blood pressure, diabetes, coronary heart disease and chronic bronchitis) was based on the inquiry in the questionnaire of whether the doctor had been informed of the condition in the past.
Prior to the MEC interview, participants completed a food recall questionnaire in order to get 24-h nutritional data, including macronutrient profiles and calorie intake. Additionally, details regarding medications, including dietary supplements consumed within the preceding month, were documented.
Statistical analyses
In this study, we conducted a secondary analysis of publicly available datasets and used descriptive statistics to characterize continuous variables (mean/SD or median/IQR) and proportions (%) for categorical variables. We assessed group differences using Kruskal-Wallis tests and one-way analyses of variance. We employed logistic regression models to explore the relationship between dietary vitamin B6 intake and endometriosis across three models. Model 1 adjusted for sociodemographic (age, race/ethnicity, education level, family income and marital status); Model 2 was adjusted for Model 1 plus BMI, smoking status, vigorous activity, moderate activity, alcohol consumption, birth control pills taken, high blood pressure, diabetes, coronary heart disease and chronic bronchitis; and Model 3 was adjusted for Model 2 plus calorie consumption, total fat consumption, total cholesterol consumption and dietary supplements taken. These models aimed to comprehensively address potential confounding factors and to enhance our understanding of the relationship between dietary vitamin B6 intake and endometriosis.
Furthermore, we investigated potential modifiers of the association between dietary vitamin B6 intake and endometriosis by incorporating variables such as family income (low vs. medium or high), marital status (living with a partner vs. living alone), smoking status, and dietary supplements taken. We assessed heterogeneity among subgroups using multivariate logistic regression and examined interactions between subgroups and dietary vitamin B6 intake through likelihood ratio testing. To ensure the robustness of our findings, we conducted sensitivity analyses by excluding participants with extreme energy intake, defined as consuming less than 500 or more than 5,000 kcal per day. This meticulous approach aimed to assess the consistency and reliability of our results under different conditions, thereby enhancing the validity of the study outcomes.
We determined the sample size based on available data, without conducting a priori statistical power assessments. We performed statistical analyses using R 3.3.2 and Free Statistics Software 1.5 (27). We conducted a comprehensive descriptive study on all individuals. For hypothesis testing, we utilized a two-tailed analysis, considering a significance level of 0.05 for determining statistical significance. This widely accepted threshold ensures standard confidence levels for interpreting results and drawing meaningful conclusions from the analyses.
Results
Baseline characteristics
Table 1 presents the essential characteristics of the 4,453 participants in the study. Among the sample, 337 individuals (7. 57%) received a diagnosis of endometriosis, and 2,820 (63.92%) were classified as overweight. A total of 1741 participants (39.10%) reported being smokers, while 2099 (47.14%) acknowledged the use of dietary supplements. Regarding age distribution, 2,378 participants (53.40%) were below 40 years old, 1,424 (31.98%) were between 40 and 50 years old, and 651 (14.62%) were above 50 years old. Notably, dietary vitamin B6 intake appeared higher in individuals who used dietary supplements, engaged in moderate exercise, were aged under 40, had a BMI below 25, had an education level exceeding 12 years, did not smoke, and lived with a partner or had a higher income. These baseline characteristics provide an overview of the diversity within the study population and establish the foundation for subsequent analyses exploring the association between these factors and endometriosis.
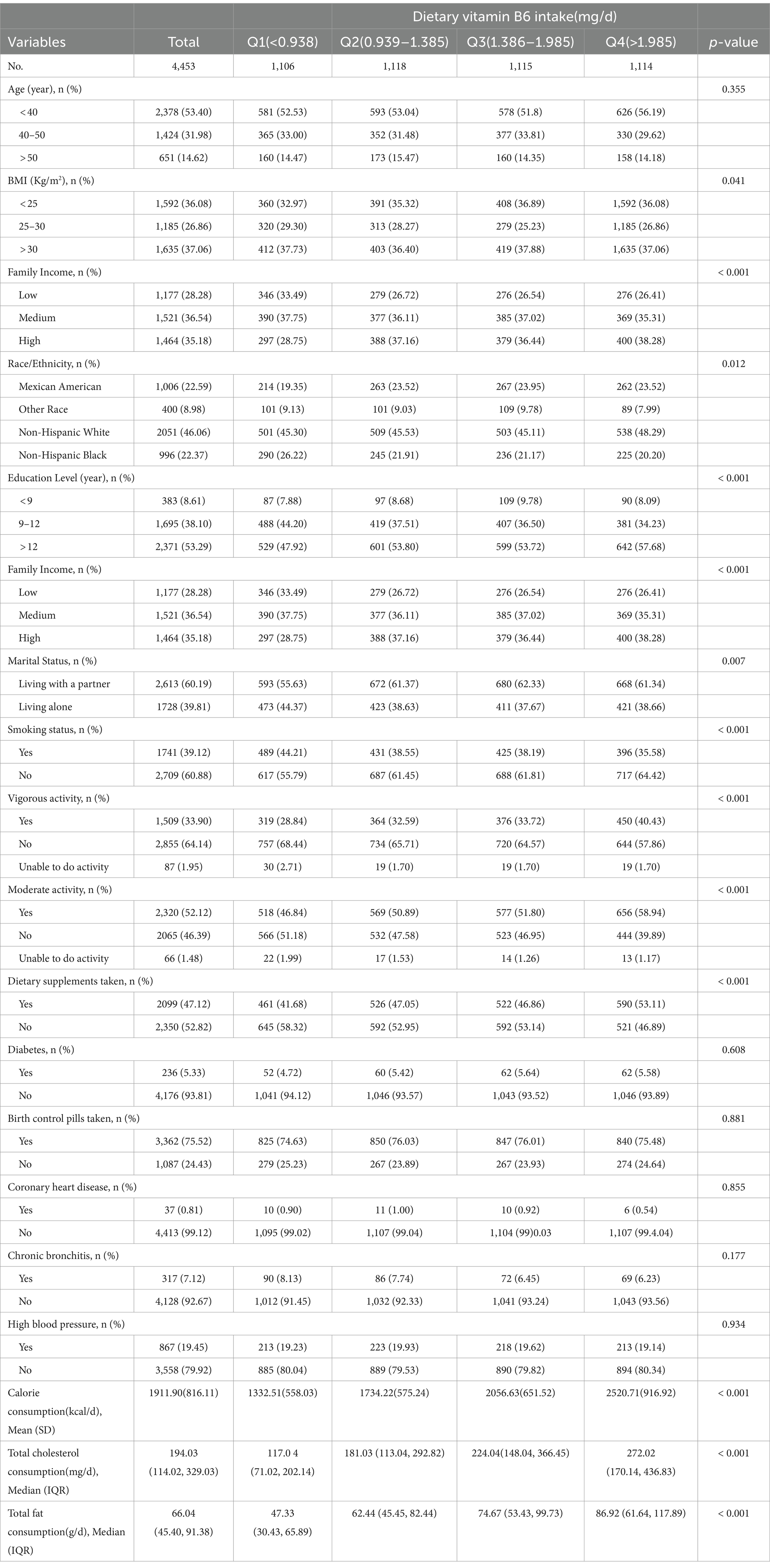
Table 1. Population characteristics by categories of dietary vitamin B6 intake.
Relationship between dietary vitamin B6 intake and endometriosis
Table 2 illustrates the relationships between dietary vitamin B6 intake and endometriosis. Univariate analysis revealed significant associations, indicating correlations between dietary vitamin B6 intake, age, race, family income, education level, use of birth control pills, high blood pressure, chronic bronchitis, and the use of dietary supplements with the presence of endometriosis. These findings underscore a complex interplay between dietary factors, demographic variables, and lifestyle choices influencing the occurrence of endometriosis. Subsequent multivariate analyses will further dissect these associations to elucidate the independent contributions of each factor to the risk of endometriosis.
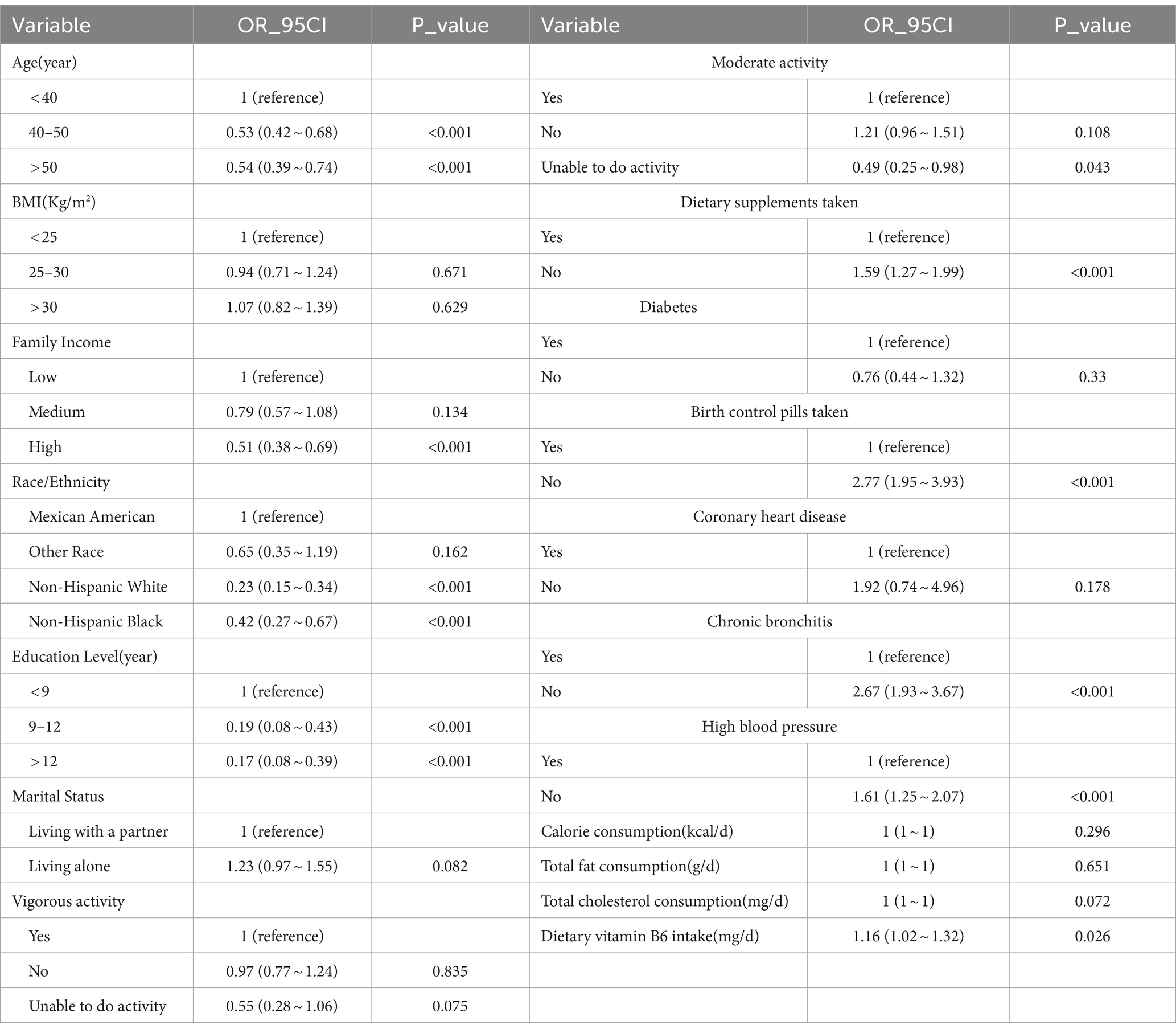
Table 2. Association of covariates and endometriosis risk.
Compared to individuals with lower vitamin B6 consumption (Q1 < 0.94 mg/day), the adjusted odds ratio (OR) values for dietary vitamin B6 intake and endometriosis in Q2 (0.95–1.39 mg/day), Q3 (1.40–1.99 mg/day), and Q4 (>1.99 mg/day) were 1.22 (95% CI: 0.88–1.69, p = 0.24), 1.22 (95% CI: 0.86–1.73, p = 0. 279), and 1.51 (95% CI: 1.01–2. 24, p = 0.04), respectively (Table 3).
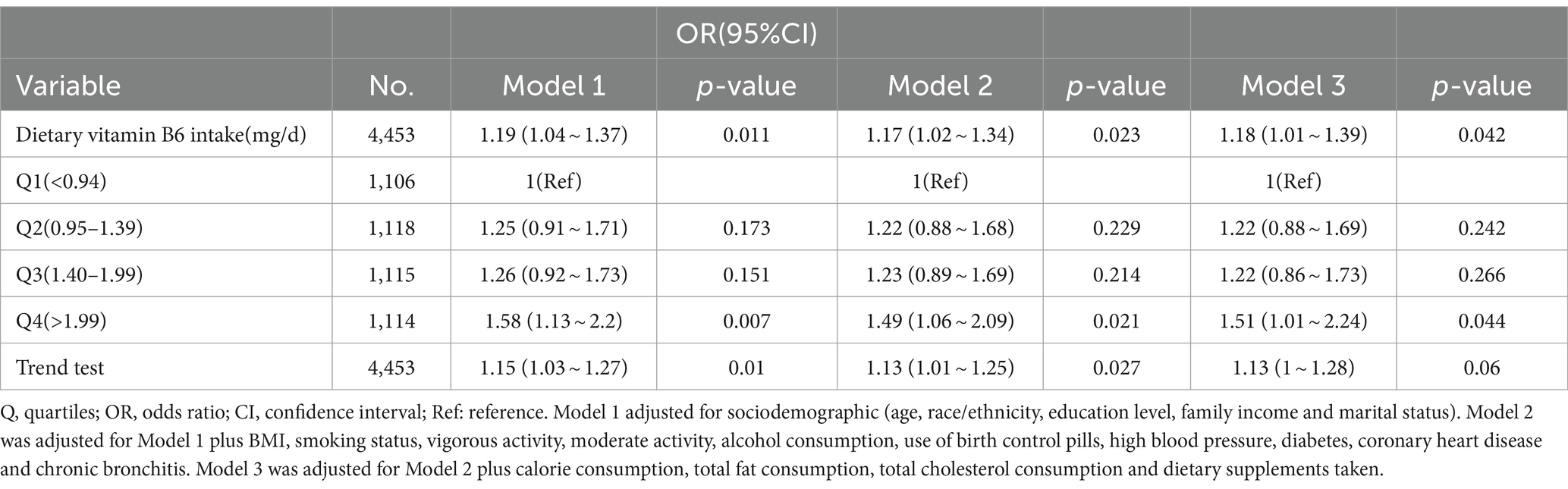
Table 3. Association between dietary vitamin B6 intake and endometriosis.
Stratified analyses based on additional variables
In a thorough examination of various subgroups, stratified analyses were conducted to assess potential effect modifications on the relationship between dietary vitamin B6 intake and endometriosis (refer to Figure 2). Notably, no significant interactions were identified in any subgroups, whether stratified by age, BMI, marital status, family income, smoking status, education level, or dietary supplements taken. These results suggest that the observed association between dietary vitamin B6 intake and endometriosis remains consistent across diverse demographic and lifestyle factors, reinforcing the robustness of the findings.
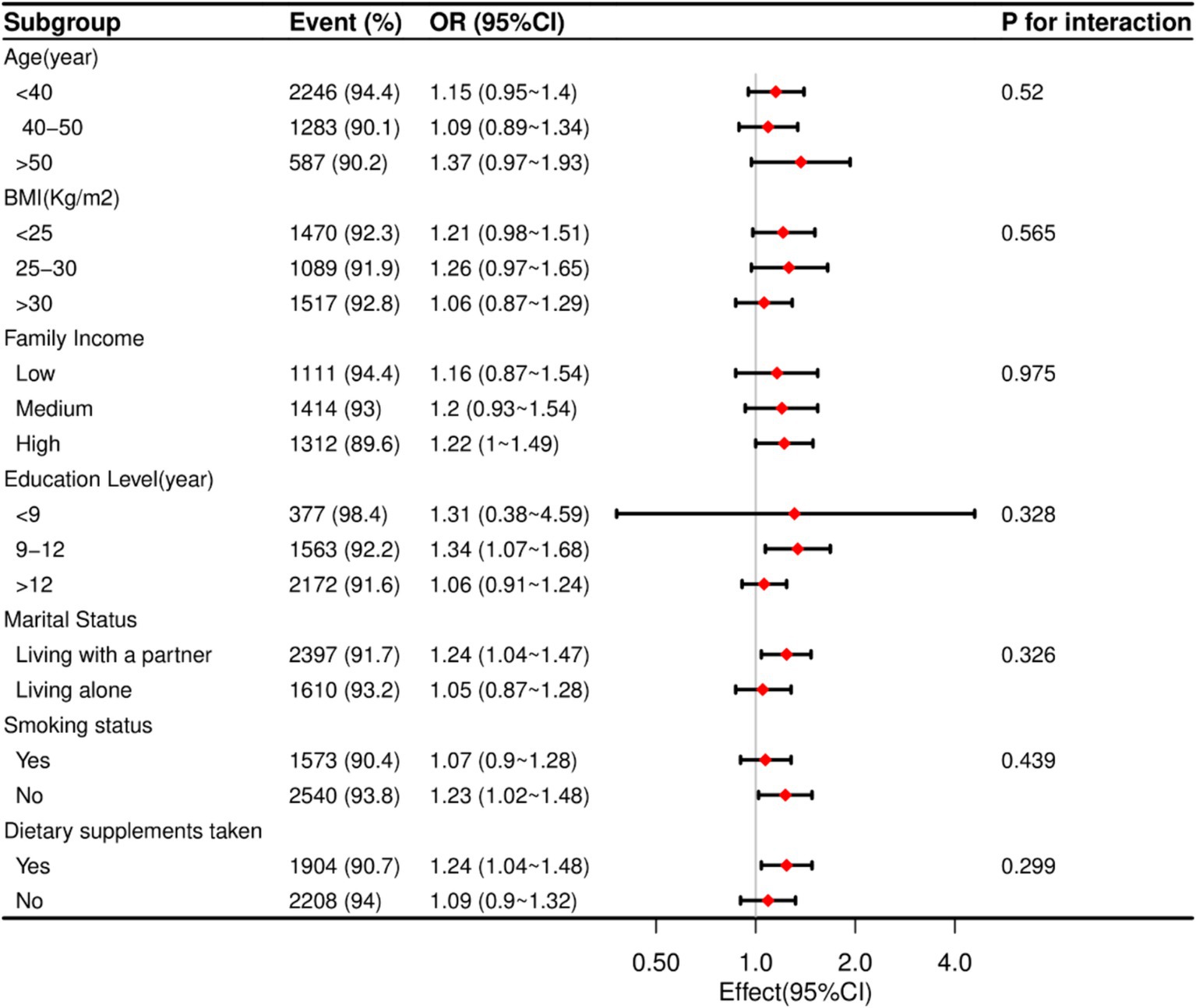
Figure 2. The relationship between dietary vitamin B6 intake and endometriosis according to basic features. Except for the stratification component itself, each stratification factor was adjusted for all other variables (age, marital status, race/ethnicity, education level, family income, BMI, vigorous activity, moderate activity, dietary supplements taken and smoking status).
Sensitivity analysis
Furthermore, after excluding individuals with extreme energy intake, the dataset comprised 4,375 individuals, and the association between dietary vitamin B6 intake and endometriosis remained robust. Compared to individuals with lower vitamin B6 consumption (<0.96 mg/day), and after adjustments for age, race, education level, smoking status, dietary supplements taken, vigorous activity, moderate activity, marital status, family income, and BMI, the adjusted odds ratio (OR) values for dietary vitamin B6 intake and endometriosis in Q2 (0.96–1.39 mg/day), Q3 (1.40–2.05 mg/day), and Q4 (>2.05 mg/day) were 1.26 (95% CI: 0.91–1.73, p = 0.16), 1.27 (95% CI: 0.92–1.75, p = 0.15), and 1.61 (95% CI: 1.14–2.26, p = 0.01), respectively (Supplementary Table S1).
Discussion
In this comprehensive cross-sectional study involving American adults, a noteworthy and previously unexplored positive correlation between endometriosis and dietary vitamin B6 intake was identified. Upon stratified analysis, these associations were found to be more significant among patients from high-income families, with 9–12 years of education, living with a partner, non-smokers, and those eligible for dietary supplements. Endometriosis has been frequently linked to inflammation (28), and evidence from studies suggested that women who have the disease exhibited greater levels of both systemic and localized inflammation. This led to the hypothesis that antioxidants, including vitamin B6, may contribute to the modulation of endometriosis, given its roles as an antioxidant regulator. This finding suggested a possible association between dietary factors and endometriosis, indicating a need for further research to explore this relationship in detail.
Given the observed correlation, it is essential to delve deeper into the specific biochemical mechanisms by which Vitamin B6 may influence endometriosis, particularly through its antioxidant and anti-inflammatory effects. Vitamin B6, present in forms such as pyridoxine, pyridoxal, and pyridoxamine, along with their phosphorylated derivatives, is known for its potent antioxidant properties, particularly in scavenging reactive oxygen species (ROS) (7, 29). This function is crucial in managing conditions like endometriosis, characterized by chronic inflammation and oxidative stress. The active form, pyridoxal 5′-phosphate (PLP), is vital in the transsulfuration pathway, where it helps convert homocysteine into cysteine, a precursor for the synthesis of glutathione (30). Glutathione, a key antioxidant, neutralizes ROS, thus protecting cells from oxidative damage and maintaining a balanced redox state (31, 32).
In endometriosis, elevated ROS levels lead to cellular damage, such as lipid peroxidation, DNA damage, and protein oxidation, which exacerbate inflammation in endometrial tissues (31). Vitamin B6 contributes to reducing oxidative stress and inflammation by promoting glutathione production, thereby mitigating these damaging effects (32, 33). This antioxidant defense and regulation of inflammation are crucial in controlling the progression and symptoms of endometriosis.
Additionally, research indicates that sufficient levels of Vitamin B6 can lower pro-inflammatory cytokines like IL-6 and TNF-α, which are significant mediators in inflammatory responses and are linked to worsening chronic inflammatory conditions (34). This anti-inflammatory property of Vitamin B6 suggests its potential therapeutic use in not only endometriosis but also other inflammatory diseases, such as rheumatoid arthritis and cardiovascular disorders (35).
Moreover, the enhancement of glutathione activity by Vitamin B6 underscores its role in maintaining cellular redox balance, which is essential for preventing oxidative damage and managing inflammation in chronic diseases (36). Studies have shown that Vitamin B6 supplementation can improve markers of oxidative stress and reduce inflammation, demonstrating its protective effects against cellular damage (37). In summary, Vitamin B6 is integral in supporting glutathione synthesis and modulating inflammatory responses, offering potential benefits in managing chronic inflammatory diseases like endometriosis. Further research is necessary to fully understand these mechanisms and develop effective therapeutic applications.
Our study possessed several strengths. Firstly, it was the first research explicitly examining the association between dietary vitamin B6 consumption and endometriosis. We identified a positive correlation between dietary vitamin B6 intake and endometriosis, and these results remained robust after conducting multiple regression and sensitivity analyses. Our study had several limitations, though. Firstly, because of the cross-sectional design, we were unable to prove directionality or causation. The existence of unmeasured variables may have added confounding effects even when possible confounders were carefully adjusted for in the logistic regression model. Interestingly, our model included several dietary parameters in an attempt to reduce confounding effects. Secondly, it was still challenging to measure the complete body’s vitamin B6 status precisely. We had inherent constraints in measuring vitamin B6 consumption because we relied on dietary questionnaires and 24-h memory. Because self-reported dietary data were prone to recall bias, they could not provide accurate assessments of a person’s overall vitamin B6 level. The accuracy of these assessments could be improved in the future by adopting more advanced approaches for assessing vitamin B6 levels. Thirdly, the study’s unique emphasis on citizens of the US meant that conclusions should be extrapolated with caution to other populations. Our results may not have been as broadly applicable as they could be due to the distinctive lifestyle and demographic characteristics of the US. Therefore, to confirm and broaden the applicability of our findings, carefully planned multicenter controlled studies including a variety of populations are essential. In conclusion, although our investigation illuminated the complex correlation between vitamin B6 intake in the diet and endometriosis, the limitations we found emphasized the necessity for additional study to fully comprehend this link and its wider consequences.
Conclusion
In this study, we identified a positive association between dietary vitamin B6 intake and the risk of endometriosis among American women aged 20 to 54 years. The findings suggest that higher dietary intake of vitamin B6 may be linked to an increased risk of developing endometriosis, particularly in women with specific sociodemographic characteristics. This study adds to the growing body of evidence highlighting the potential role of diet in the pathogenesis of endometriosis. However, given the observational nature of this study, further research is warranted to explore the underlying mechanisms and to establish causal relationships. Future studies should also consider a broader range of populations and utilize longitudinal designs to validate these findings and examine the long-term effects of dietary vitamin B6 on endometriosis risk.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
Ethical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and the institutional requirements.
Author contributions
LY: Conceptualization, Methodology, Writing – original draft. FL: Data curation, Formal analysis, Methodology, Software, Writing – original draft. BX: Data curation, Formal analysis, Resources, Software, Writing – review & editing. YS: Data curation, Formal analysis, Methodology, Software, Writing – review & editing. LC: Data curation, Formal analysis, Methodology, Software, Writing – review & editing. XW: Data curation, Formal analysis, Methodology, Validation, Visualization, Writing – review & editing. WT: Conceptualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2024.1407099/full#supplementary-material
References
1. Zondervan, KT, Becker, CM, Koga, K, Missmer, SA, Taylor, RN, and Vigano, P. Endometriosis. Nat Rev Dis Primers. (2018) 4:9. doi: 10.1038/s41572-018-0008-5
2. Giampaolino, P, Della Corte, L, Foreste, V, Barra, F, Ferrero, S, and Bifulco, G. Dioxin and endometriosis: a new possible relation based on epigenetic theory. Gynecol Endocrinol. (2020) 36:279–84. doi: 10.1080/09513590.2019.1698024
3. Soliman, AM, Surrey, ES, Bonafede, M, Nelson, JK, Vora, JB, and Agarwal, SK. Health care utilization and costs associated with endometriosis among women with Medicaid insurance. J Manag Care Spec Pharm. (2019) 25:566–72. doi: 10.18553/jmcp.2019.25.5.566
4. Agarwal, SK, Chapron, C, Giudice, LC, Laufer, MR, Leyland, N, Missmer, SA, et al. Clinical diagnosis of endometriosis: a call to action. Am J Obstet Gynecol. (2019) 220:354.e1–e12. doi: 10.1016/j.ajog.2018.12.039
5. Vrolijk, MF, Hageman, GJ, van de Koppel, S, van Hunsel, F, and Bast, A. Inter-individual differences in pharmacokinetics of vitamin B6: a possible explanation of different sensitivity to its neuropathic effects. Pharma Nutrit. (2020) 12:100188. doi: 10.1016/j.phanu.2020.100188
6. Hellmann, H, and Mooney, S. Vitamin B6: a molecule for human health? Molecules. (2010) 15:442–59. doi: 10.3390/molecules15010442
7. Zhang, P, Suda, T, Suidasari, S, Kumrungsee, T, Yanaka, N, and Kato, N. Novel preventive mechanisms of vitamin B6 against inflammation, inflammasome, and chronic diseases In: VB Patel, editor. Molecular Nutrition. US: Academic Press (2020). 283–99.
8. Gylling, B, Myte, R, Schneede, J, Hallmans, G, Haggstrom, J, Johansson, I, et al. Vitamin B-6 and colorectal cancer risk: a prospective population-based study using 3 distinct plasma markers of vitamin B-6 status. Am J Clin Nutr. (2017) 105:897–904. doi: 10.3945/ajcn.116.139337
9. Kayashima, T, Tanaka, K, Okazaki, Y, Matsubara, K, Yanaka, N, and Kato, N. Consumption of vitamin B6 reduces colonic damage and protein expression of HSP70 and HO-1, the anti-tumor targets, in rats exposed to 1,2-dimethylhydrazine. Oncol Lett. (2011) 2:1243–6. doi: 10.3892/ol.2011.370
10. Windebank, AJ, Low, PA, Blexrud, MD, Schmelzer, JD, and Schaumburg, HH. Pyridoxine neuropathy in rats: specific degeneration of sensory axons. Neurology. (1985) 35:1617–7.
11. Meyer, HE, Willett, WC, Fung, TT, Holvik, K, and Feskanich, D. Association of High Intakes of vitamins B6 and B12 from food and supplements with risk of hip fracture among postmenopausal women in the Nurses’ health study. JAMA Netw Open. (2019) 2:e193591. doi: 10.1001/jamanetworkopen.2019.3591
12. Li, Z, Zhang, S, Wan, L, Song, X, Yuan, D, Zhang, S, et al. Vitamin B6 as a novel risk biomarker of fractured ankles. Medicine. (2021) 100:e27442. doi: 10.1097/MD.0000000000027442
13. Badawy, AA. Pellagra and alcoholism: a biochemical perspective. Alcohol Alcohol. (2014) 49:238–50. doi: 10.1093/alcalc/agu010
14. Inubushi, T, Takasawa, T, Tuboi, Y, Watanabe, N, Aki, K, and Katunuma, N. Changes of glucose metabolism and skin-collagen neogenesis in vitamin B6 deficiency. Biofactors. (2005) 23:59–67. doi: 10.1002/biof.5520230201
15. Vilter, RW, Mueller, JF, Glazer, HS, Jarrold, T, Abraham, J, Thompson, C, et al. The effect of vitamin B6 deficiency induced by desoxypyridoxine in human beings. J Lab Clin Med. (1953) 42:335–57.
16. Hsu, CC, Cheng, CH, Hsu, CL, Lee, WJ, Huang, SC, and Huang, YC. Role of vitamin B6 status on antioxidant defenses, glutathione, and related enzyme activities in mice with homocysteine-induced oxidative stress. Food Nutr Res. (2015) 59:25702. doi: 10.3402/fnr.v59.25702
17. Aisen, PS, Schneider, LS, Sano, M, Diaz-Arrastia, R, van Dyck, CH, Weiner, MF, et al. High-dose B vitamin supplementation and cognitive decline in Alzheimer disease: a randomized controlled trial. JAMA. (2008) 300:1774–83. doi: 10.1001/jama.300.15.1774
18. Okereke, OI, Cook, NR, Albert, CM, Van Denburgh, M, Buring, JE, and Manson, JE. Effect of long-term supplementation with folic acid and B vitamins on risk of depression in older women. Br J Psychiatry. (2015) 206:324–31. doi: 10.1192/bjp.bp.114.148361
19. Zhang, DM, Ye, JX, Mu, JS, and Cui, XP. Efficacy of vitamin B supplementation on cognition in elderly patients with cognitive-related diseases. J Geriatr Psychiatry Neurol. (2017) 30:50–9. doi: 10.1177/0891988716673466
20. Laganà, AA-O, Salmeri, FM, Ban Frangež, H, Ghezzi, F, Vrtačnik-Bokal, E, and Granese, R. Evaluation of M1 and M2 macrophages in ovarian endometriomas from women affected by endometriosis at different stages of the disease. Gynecol Endocrinol. (2020) 36:441–4. doi: 10.1080/09513590.2019.1683821
21. Cirillo, M, Coccia, ME, Petraglia, F, and Fatini, C. Role of endometriosis in defining cardiovascular risk: a gender medicine approach for women’s health. Hum Fertil (Camb). (2022) 25:745–53. doi: 10.1080/14647273.2021.1919764
22. Foster, E, Lee, C, Imamura, F, Hollidge, SE, Westgate, KL, Venables, MC, et al. Validity and reliability of an online self-report 24-h dietary recall method (Intake24): a doubly labelled water study and repeated-measures analysis. J Nutr Sci. (2019) 8:e29. doi: 10.1017/jns.2019.20
23. Liu, HA-O, Wang, L, Chen, C, Dong, ZA-O, and Yu, S. Association between dietary niacin intake and migraine among American adults: National Health and nutrition examination survey. Nutrients. (2022) 14:3052. doi: 10.3390/nu14153052
24. Xiao, Q, Cai, B, Yin, A, Huo, H, Lan, K, Zhou, G, et al. L-shaped association of serum 25-hydroxyvitamin D concentrations with cardiovascular and all-cause mortality in individuals with osteoarthritis: results from the NHANES database prospective cohort study. BMC Med. (2022) 20:308. doi: 10.1186/s12916-022-02510-1
25. Zhang, YY, Qiu, HB, and Tian, JW. Association between vitamin D and hyperuricemia among adults in the United States. Front Nutrit. (2020) 7:592777. doi: 10.3389/fnut.2020.592777
26. Agriculture ArRSUDo. What We Eat in America: Data Tables. (2024). Available from: https://www.ars.usda.gov/northeast-area/beltsville-md-bhnrc/beltsville-human-nutrition-research-center/food-surveys-research-group/docs/wweia-data-tables/ (Accessed March 20, 2024).
27. Yang, Q, Zheng, J, Chen, W, Chen, X, Wen, D, Chen, W, et al. Association between preadmission metformin use and outcomes in intensive care unit patients with sepsis and type 2 diabetes: a cohort study. Front Med (Lausanne). (2021) 8:640785. doi: 10.3389/fmed.2021.640785
28. Symons, LK, Miller, JE, Kay, VR, Marks, RM, Liblik, K, Koti, M, et al. The Immunopathophysiology of endometriosis. Trends Mol Med. (2018) 24:748–62. doi: 10.1016/j.molmed.2018.07.004
29. Vrolijk, MF, Opperhuizen, A, Jansen, E, Hageman, GJ, Bast, A, and Haenen, G. The vitamin B6 paradox: supplementation with high concentrations of pyridoxine leads to decreased vitamin B6 function. Toxicol In Vitro. (2017) 44:206–12. doi: 10.1016/j.tiv.2017.07.009
30. Matxain, JM, Padro, D, Ristila, M, Strid, Å, and Eriksson, LA. Evidence of high• OH radical quenching efficiency by vitamin B6. J Phys Chem B. (2009) 113:9629–32. doi: 10.1021/jp903023c
31. Abramiuk, M, Mertowska, P, Frankowska, K, Świechowska-Starek, P, Satora, M, Polak, G, et al. How can selected dietary ingredients influence the development and progression of endometriosis? Nutrients. (2024) 16:154. doi: 10.3390/nu16010154
32. Arab, A, Karimi, E, Vingrys, K, Kelishadi, MR, Mehrabani, S, and Askari, G. Food groups and nutrients consumption and risk of endometriosis: a systematic review and meta-analysis of observational studies. Nutr J. (2022) 21:58. doi: 10.1186/s12937-022-00812-x
33. Roshanzadeh, G, Jahanian Sadatmahalleh, SA-O, Moini, A, Mottaghi, A, and Rostami, F. The relationship between dietary micronutrients and endometriosis: a case-control study. Int J Reproductive BioMed. (2023) 21:333. doi: 10.18502/ijrm.v21i4.13272
34. Back, E, and Biesalski, HK. Vitamin B6 In: S Offermanns and W Rosenthal, editors. Encyclopedia of molecular pharmacology. Berlin, Heidelberg: springer (2008). 1290–1.
35. Ueland, PM, McCann, A, Midttun, O, and Ulvik, A. Inflammation, vitamin B6 and related pathways. Mol Asp Med. (2017) 53:10–27. doi: 10.1016/j.mam.2016.08.001
36. Rosenberg, J, Ischebeck, T, and Commichau, FM. Vitamin B6 metabolism in microbes and approaches for fermentative production. Biotechnol Adv. (2016) 35:31–40. doi: 10.1016/j.biotechadv.2016.11.004
Keywords: endometriosis, vitamin B6, NHANES, cross-sectional study, dietary intake
Citation: Yin L, Liang F, Xie B, Su Y, Cheng L, Wei X and Tian W (2024) Association between dietary vitamin B6 intake and endometriosis risk: evidence from the national health and nutrition examination survey. Front. Nutr. 11:1407099. doi: 10.3389/fnut.2024.1407099
Edited by:
Siddika Yalcin, Hacettepe University, TürkiyeReviewed by:
Ruijie Xie, German Cancer Research Center (DKFZ), GermanyMarzieh Saei Ghare Naz, Shahid Beheshti University of Medical Sciences, Iran
Copyright © 2024 Yin, Liang, Xie, Su, Cheng, Wei and Tian. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wencai Tian, MjAyMjAwMTIxQHNyLmd4bXUuZWR1LmNu