 Wei Sun
Wei Sun Yuchao Wang1†
Yuchao Wang1† Yinshi Liu
Yinshi Liu Chen Xu
Chen Xu Daqing Sun
Daqing Sun
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr. , 18 July 2024
Sec. Clinical Nutrition
Volume 11 - 2024 | https://doi.org/10.3389/fnut.2024.1404400
Background: Oxidative stress is acknowledged as a pivotal factor in the intricate pathophysiological processes and pathogenesis of constipation. Modifying dietary patterns can elevate in vivo antioxidant biomarker levels, consequently mitigating oxidative stress. The Composite Dietary Antioxidant Index (CDAI) provides a dependable scoring mechanism for quantifying the potential antioxidant capacity of diets. The association between CDAI levels and the risk of constipation remains uncertain.
Purpose: To investigate the potential correlation between CDAI and constipation, aiming to improve constipation management through dietary guidance.
Methods: A total of 11,165 adults aged ≥20 years, drawn from the 2005–2010 National Health and Nutrition Examination Survey, were enrolled in this cross-sectional study. We evaluated the correlation between CDAI levels and the risk of constipation through three weighted logistic regression models. Restricted cubic spline (RCS) analysis was employed to assess nonlinear trends, and stratified analyses were conducted.
Results: After adjusting for all confounding variables, the findings revealed an association between CDAI and constipation [OR = 0.937; 95% CI (0.892, 0.984), p = 0.012]. Moreover, individuals in the highest quartile of CDAI demonstrated a 40.1% lower likelihood of experiencing constipation compared to those in the lowest quartile [OR = 0.599; 95% CI (0.382, 0.939), p = 0.027]. The RCS analysis indicated a linear relationship between CDAI and constipation (P-non-linear =0.1016). Subgroup analysis by gender revealed a negative correlation in the male population [OR = 0.871; 95% CI (0.801, 0.947), p = 0.002], with men in the highest CDAI quartile exhibiting a 59.8% lower likelihood of experiencing constipation compared to those in the lowest quartile [OR = 0.402; 95% CI (0.206, 0.787), p = 0.010]. Furthermore, alterations in selenium [OR = 0.997; 95% CI (0.995, 1.000), p = 0.039] per milligram were independently linked to constipation. In a gender subgroup analysis of a single antioxidant, changes per milligram of vitamin E [OR = 0.904; 95% CI (0.838 to 0.975), p = 0.011] among males were independently associated with constipation.
Conclusion: The fully adjusted model showed a correlation between CDAI and constipation and a significant correlation in quartiles. Meanwhile, subgroup analysis by gender showed that CDAI was negatively associated with constipation in the male population. Moreover, the findings of this study imply that investigations into antioxidant diets should be contextualized within dietary patterns.
Constipation represents a widespread concern afflicting individuals across all age groups (1). It is commonly described as bowel movements that are infrequent or difficult (2). This imposes a significant health burden on patients, significantly impacting their quality of life and mental health (3). Within the community, the median prevalence of constipation among adults is 16%., This prevalence increases significantly among older individuals, reaching 33.5% among adults aged 60 to 101 years (4, 5). Its prevalence is greater among non-Caucasian populations, inpatients, and women; the median prevalence ratio in women to men is 1.5:1 (6). Constipation is a multifactorial disorder with common risk factors such as genetic predisposition, socioeconomic status, parental education, lifestyle, medications, and depression (7, 8). Among them, lifestyle is a more controllable risk factor, especially the relationship between dietary composition and constipation. Recent research indicates that levels of oxidative stress have increased in both constipated patients and animal models (9). Moreover, multiple studies have demonstrated an imbalance of oxidative stress in the intestines of constipated patients (10, 11). Diet plays a crucial role in providing exogenous antioxidants, effectively increasing the levels of endogenous antioxidant biomarkers in the body, thereby alleviating oxidative stress (12, 13). Vitamins A or carotenoids, along with vitamins C and E, as well as other antioxidants, are believed to ameliorate constipation by thwarting cellular damage induced by oxidative stress. Recently, studies have reported that soluble fiber and trace elements, such as selenium, magnesium, and phosphorus, have been thought to reduce the risk of constipation (8, 14–16), while high saturated fat or relatively low energy intake in women are associated with an increased risk (17, 18). Therefore, research by adjusting the level of antioxidants in the diet offers hope for the prevention and control of constipation.
the Composite Dietary Antioxidant Index (CDAI) is a comprehensive score used to assess an individual’s total dietary antioxidant capacity (TAC), which is based on various dietary vitamins and minerals with antioxidant properties, such as vitamins A, C, and E, as well as minerals like selenium and zinc (19, 20). The CDAI serves as a tool to quantify the potential antioxidant capacity of one’s daily diet (21). Existing literature suggests that CDAI is negatively correlated with osteoporosis (22), hypertension (23), depression (20), and cardiovascular disease mortality (24). Furthermore, it is also associated with specific inflammatory biomarkers such as IL-1β and TNFα (25), which are known to be elevated in constipated populations (26). Additionally, there is a noteworthy bimodal distribution observed in constipation and oxidative balance, contingent upon gender disparities (27). Currently, the relationship between CDAI and constipation remains unexplored. Therefore, we conducted a cross-sectional study using data from the National Health and Nutrition Examination Survey (NHANES) from 2005 to 2010. NHANES is a comprehensive representative survey of the U.S. populace, aimed at investigating the possible link between CDAI and the occurrence of constipation, with the objective of enhancing its management through dietary guidance.
NHANES is a major program conducted by the National Center for Health Statistics (NCHS) to collect nationally representative health data concerning the broader population of the United States. NHANES employs a sophisticated multistage stratified probability sampling method, conducting an annual cross-sectional survey on approximately 5,000 individuals. These surveys have been biennially published since 1999. To ensure a representative sample, NHANES deliberately oversamples specific subgroups of the population. Thus, during data analysis, we considered sample weights to correct for differences in the probability of different selections, to compensate for possible underrepresentation of eligible populations, and to adjust for non-coverage and non-response. The NHANES protocol received approval from the NCHS Research Ethics Review Board, and all participants provided informed consent. The NHANES survey data, comprehensive survey operation manuals, consent documents, and brochures for each survey period were made publicly accessible on the NHANES website.1
In this study, we integrated survey data from the years 2005–2006, 2007–2008, and 2009–2010, as these three cycles included the most comprehensive Bowel Health Questionnaire (BHQ) to date. The data analyzed in this paper were exclusively extracted from adults aged ≥20 years. Participants with colorectal cancer or pregnancy were excluded from the study, as were those with missing covariate data. Ultimately, a total of 11,165 participants were included in the analysis. The process of patient selection is depicted using a flowchart, as illustrated in Figure 1.
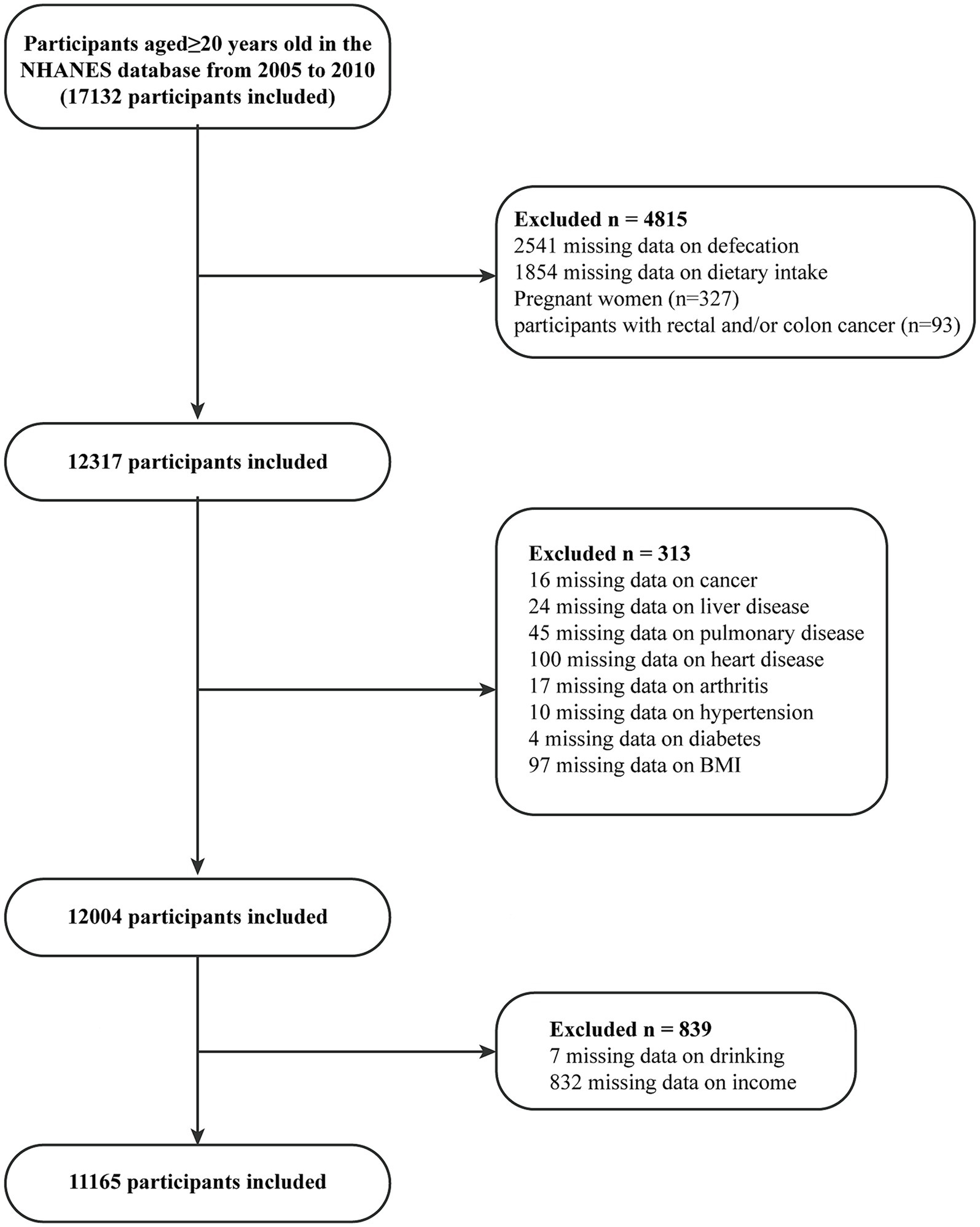
Figure 1. Flowchart depicting participant selection in the study.
According to previous studies, bowel habits were assessed using the Bristol Stool Form Scale (BSFS), which consists of illustrated and textual descriptions of seven types of stools. Participants were instructed to review the cards and subsequently indicate the number associated with the stool type they typically or most commonly experience to researchers. “Constipation” was defined as type 1 (separate hard lumps, like nuts) or type 2 (sausage-like, but lumpy). As in other NHANES publications, normal stool consistency is defined as types 3, 4, and 5 of the BSFS. To compare the definition of constipation based on stool characteristics with other definitions, we also assessed bowel frequency through the following question from the questionnaire: “How many times do you usually have bowel movements in a week?.” Responses ranged from once a week to 70 times a week. The results of bowel frequency were separated into two categories: those having fewer than three bowel movements per week (constipation), and those with three or more bowel movements per week (non-constipation) (14, 18).
NHANES employs non-consecutive 24-h dietary recall to collect participants’ food intake data. The initial dietary recall is conducted at a Mobile Examination Center (MEC), while the second interview takes place via telephone 3 to 10 days later. The daily average antioxidant intake is calculated based on the dietary recall data from these 2 days, and all participants’ CDAI levels are computed using a modified version developed by Wright et al. (14). The CDAI is computed as the sum of the daily average intake of zinc, selenium, carotenoids, vitamins A, C, and E, which is initially standardized by subtracting the mean and then dividing by their standard deviation (SD):
In order to reduce potential confounding biases in the analysis, we selected covariates based on previous research and clinical rationale. The chosen covariates comprise age, gender, race, education level, family poverty income ratio (PIR), body mass index (BMI), whether they perform vigorous physical activity, smoking status, alcohol consumption, diabetes status, hypertension status, arthritis status, heart disease status, lung disease status, liver disease status, cancer status, dietary fiber intake, total fat and protein intake, carbohydrate intake and water intake. Detailed measurement procedures can be found on https://www.cdc.gov/nchs/nhanes.
Due to the complex nationwide sampling design, we only considered 2-year dietary weights (WTDR2D), sampling units (SDMVPSU), and strata (SDMVSTRA) in all analyses. In this instance, new 6-year weights can be calculated by dividing the 2-year weights by 3. A descriptive analysis was performed for all participants. Continuous data were analyzed using means and standard deviations (SD), while categorical variables were expressed as percentages (%). The chi-square test was employed for categorical variables, whereas the t-test was utilized for continuous variables (such as age). The relationship between constipation and CDAI was analyzed using logistic regression models. Three different models, including both unadjusted and multivariable-adjusted models, were employed: Model I (without adjusting for any covariates), Model II (adjusted for gender, age, and race), Model III(adjusted for Model II plus education level, PIR, vigorous physical activity, BMI, diabetes, hypertension, arthritis, heart disease, lung disease, liver disease, cancer, and other covariates). Statistical significance was determined by comparing adjusted odds ratios (ORs) to 1.0 and its 95% confidence intervals (CIs). All statistical analyses were performed using R version 4.2.1(R Foundation for Statistical Computing, Vienna, Austria; http://www.r-project.org), and the statistical significance threshold was ascertained by a two-sided p-value of <0.05.
This study analyzed a total of 11,165 eligible participants. Table 1 showcases the baseline characteristics of the study cohort stratified by quartiles of CDAI, unveiling notable disparities across diverse demographic and lifestyle factors including gender, race, education level, family poverty income ratio (PIR), vigorous physical activity, smoking status, alcohol consumption, diabetes, pulmonary disease, dietary fiber intake, total fat intake, protein intake, carbohydrate intake, and moisture intake (p < 0.001). Particularly noteworthy is the observation that individuals in the uppermost quartile of CDAI were predominantly between 40 to 60 years of age male, of non-Hispanic White ethnicity, possessed higher levels of education, exhibited greater economic prosperity, maintained a BMI within the range of 25 to 30, participated in vigorous physical activity, refrained from smoking and consuming alcohol. Additionally, a notable correlation was identified between CDAI quartiles and constipation even in the absence of covariate adjustment (p < 0.001).
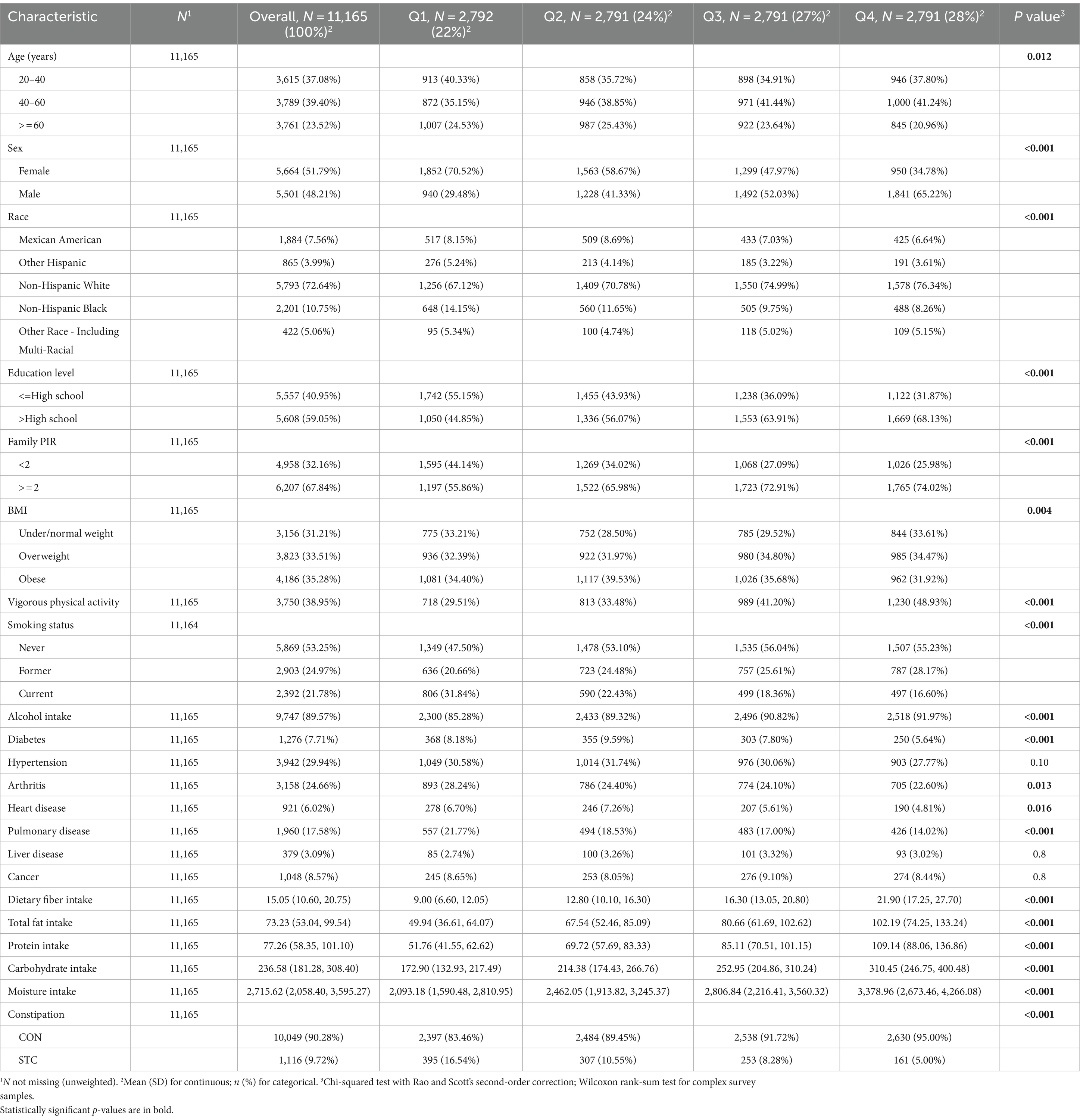
Table 1. Demographic characteristics stratified by Quartile of CDAI (n = 11,165).
Table 2 illustrates the weighted logistic regression models depicting the relationship between CDAI and constipation. In models I, II, and III, there is a negative association between CDAI and constipation [OR = 0.858; 95% CI (0.830, 0.886); p < 0.001; OR = 0.894; 95% CI (0.864, 0.925); p < 0.001; OR = 0.937; 95% CI (0.892, 0.984); p = 0.012], suggesting that each unit increase in CDAI is associated with a decreased likelihood of constipation. Following the categorization of CDAI into quartiles, individuals in the highest quartile exhibited a 40.1% reduced likelihood of experiencing constipation in contrast to those in the lowest quartile [OR = 0.599; 95% CI (0.382, 0.939); p = 0.027]. The restricted cubic splines (RCS) of Figure 2 reveal a linear correlation between CDAI and constipation (non-linear p = 0.1016). Table 2 displays the results of stratified analysis conducted according to gender differences. In male patients, CDAI demonstrates a negative association with constipation [OR = 0.871; 95% CI (0.801, 0.947); p = 0.002]. Moreover, males in the highest quartile of CDAI exhibit a 59.8% reduced likelihood of experiencing constipation compared to those in the lowest quartile [OR = 0.402; 95% CI (0.206, 0.787); p = 0.010]. In models I and II, a significant association between CDAI and constipation in female patients was observed (p < 0.001); however, after adjusting for all confounding factors, no correlation was found between CDAI and constipation in female patients (p > 0.05).
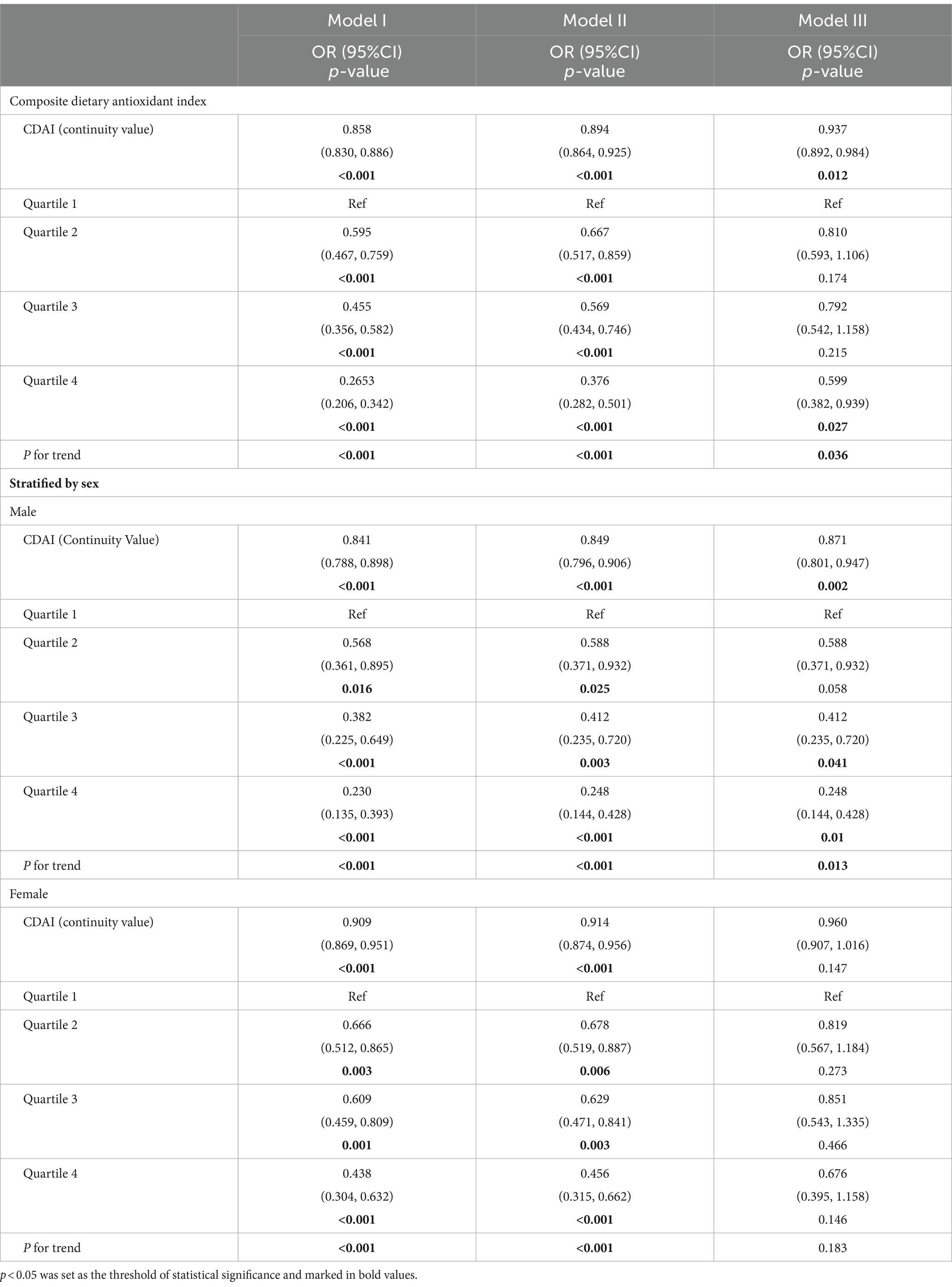
Table 2. The association between composite dietary antioxidant index and constipation.
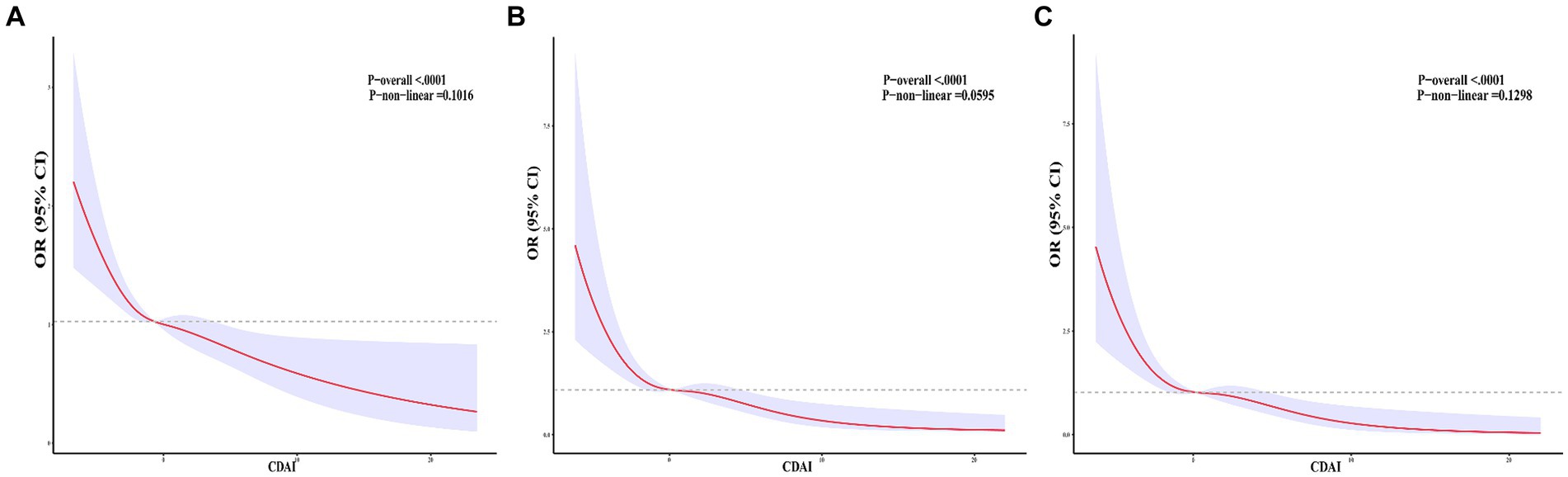
Figure 2. Correlations between CDAI and constipation. (A) A linear correlation between CDAI and constipation. (B) A linear relationship between CDAI and male patients with constipation. (C) A linear relationship between CDAI and female patients with constipation.
We conducted further analysis to examine the relationship between six antioxidant components of CDAI and constipation. As depicted in Table 3, all six antioxidant components were observed to be negatively associated with constipation in models I and II. Nonetheless, following adjustment for all variables, selenium exhibited an independent association with constipation, with an odds ratio of 0.997 [95% CI (0.995, 1.000); p = 0.039] per milligram increase. Among men, change per milligram of vitamin E (OR = 0.9039; [95% CI (0.995, 1.000); p = 0.039]) was independently associated with constipation risk after adjusting for all variables; however, this association was not observed in women. To delve deeper into the nonlinear dose–response relationship between antioxidant components and constipation, we constructed restricted cubic splines (RCS) for six antioxidant components (vitamins A, C, E, carotenoids, zinc, and selenium) and their association with constipation in Figure 3. The analysis using RCS revealed nonlinear dose–response relationships between carotenoids (non-linear p = 0.019), vitamin A (non-linear p = 0.001), and vitamin C (non-linear p = 0.030) levels and the prevalence of constipation. Simultaneously, we conducted a gender-stratified analysis to elucidate the dose–response relationship between the six antioxidants and constipation among participants of varying genders (Figures 4, 5).
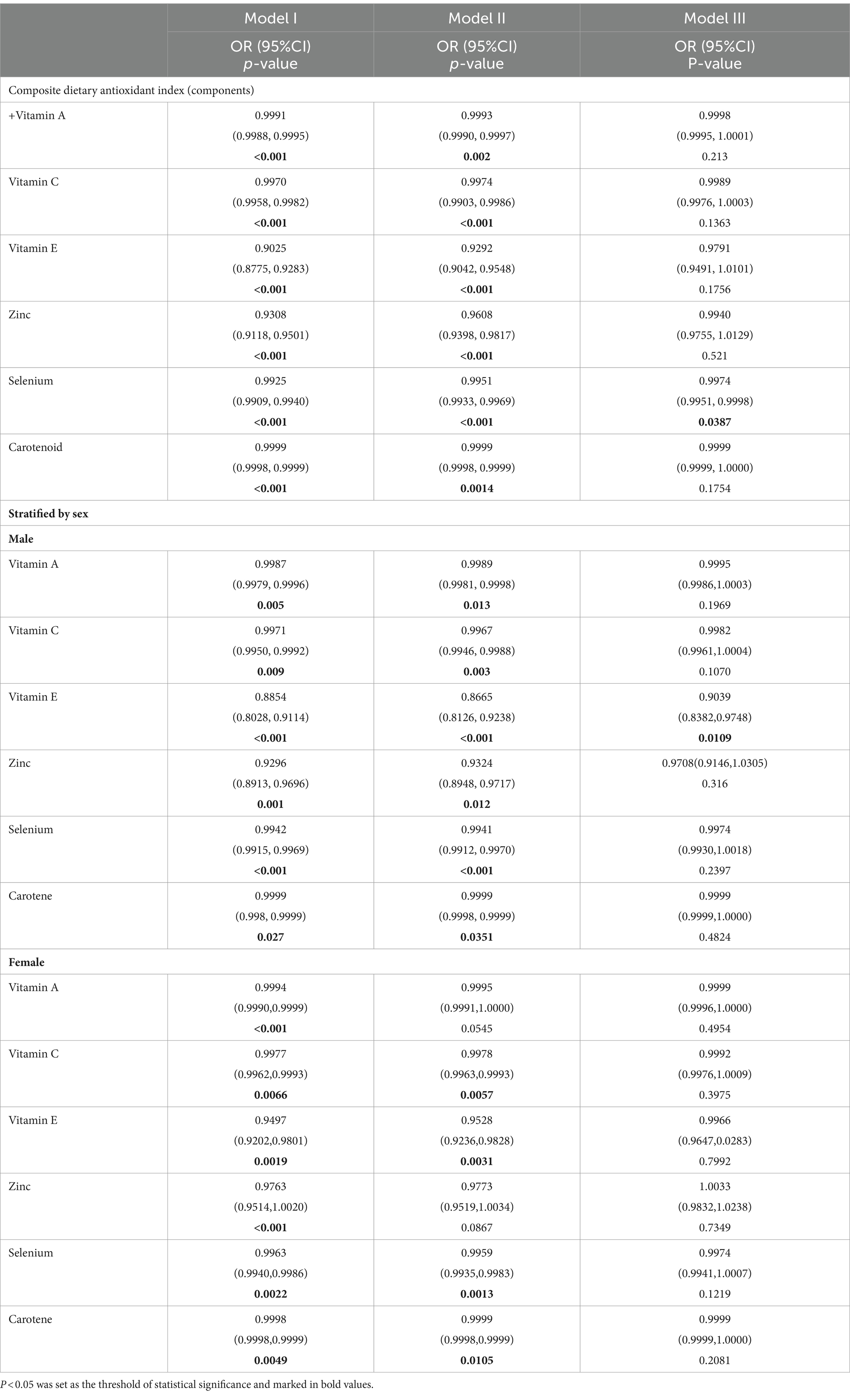
Table 3. The association between composite dietary antioxidant index (components) and constipation.
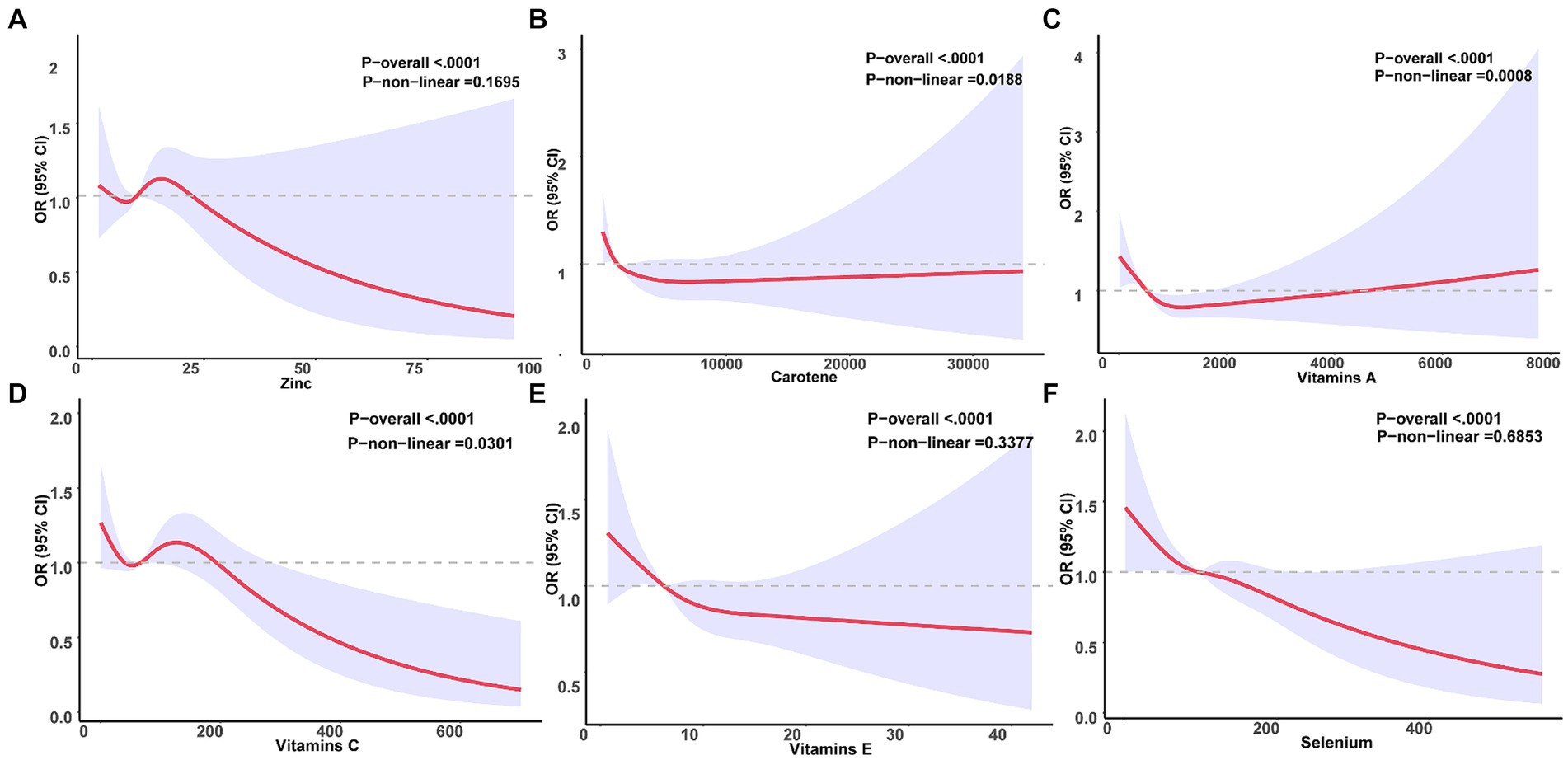
Figure 3. Relationship between six antioxidant components and constipation. A nonlinear correlation was observed between Carotene (B), Vitamin A (C), and Vitamin C (D) and the incidence of constipation. Conversely, a linear relationship was identified between Zinc (A), Vitamin E (E), and Selenium (F) and constipation.
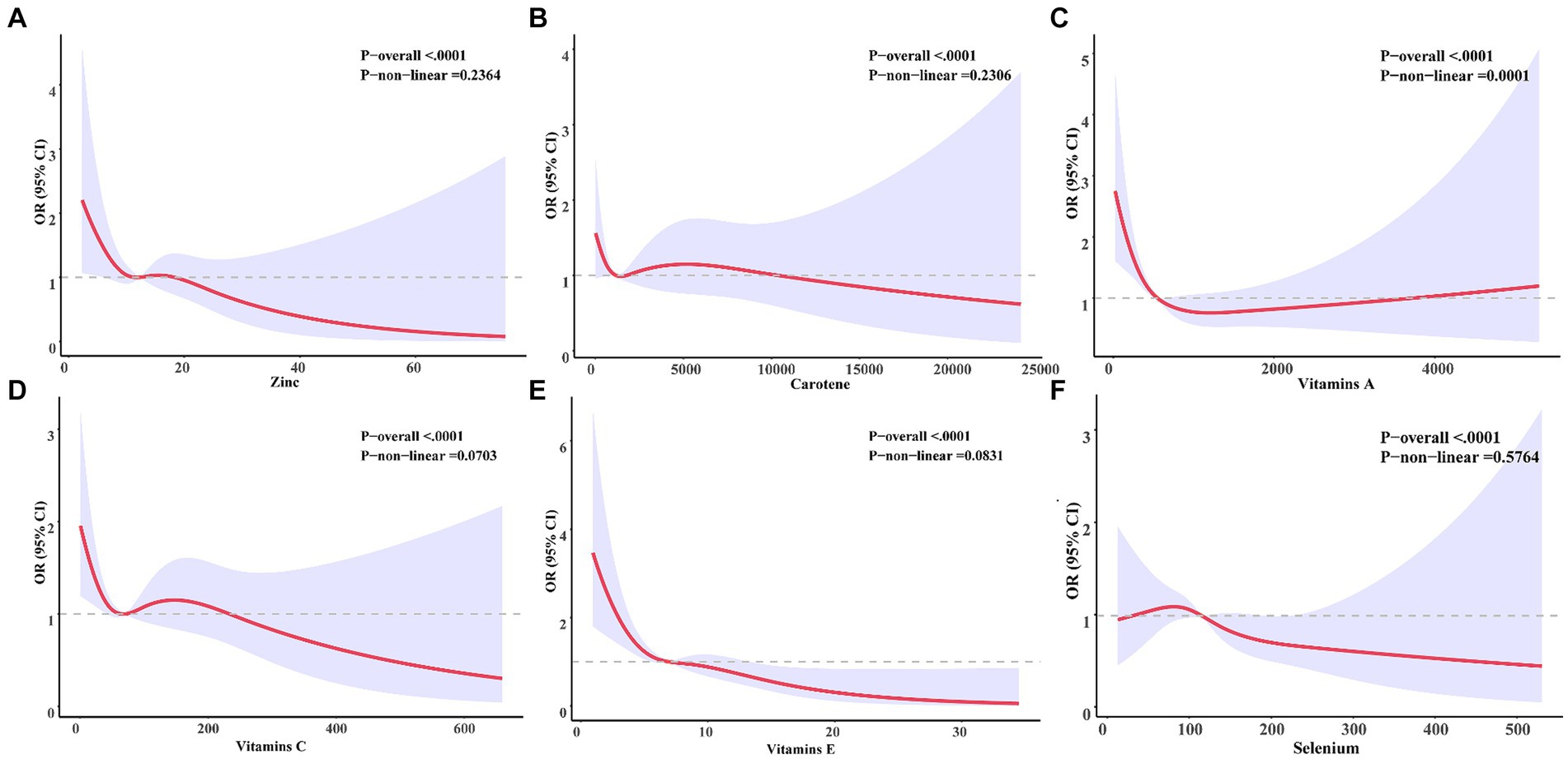
Figure 4. Six antioxidants were associated with a dose–response relationship to constipation in male participants. Zinc (A), Carotene (B), Vitamin A (C), Vitamins C (D), Vitamins D (E), Selenium (F).
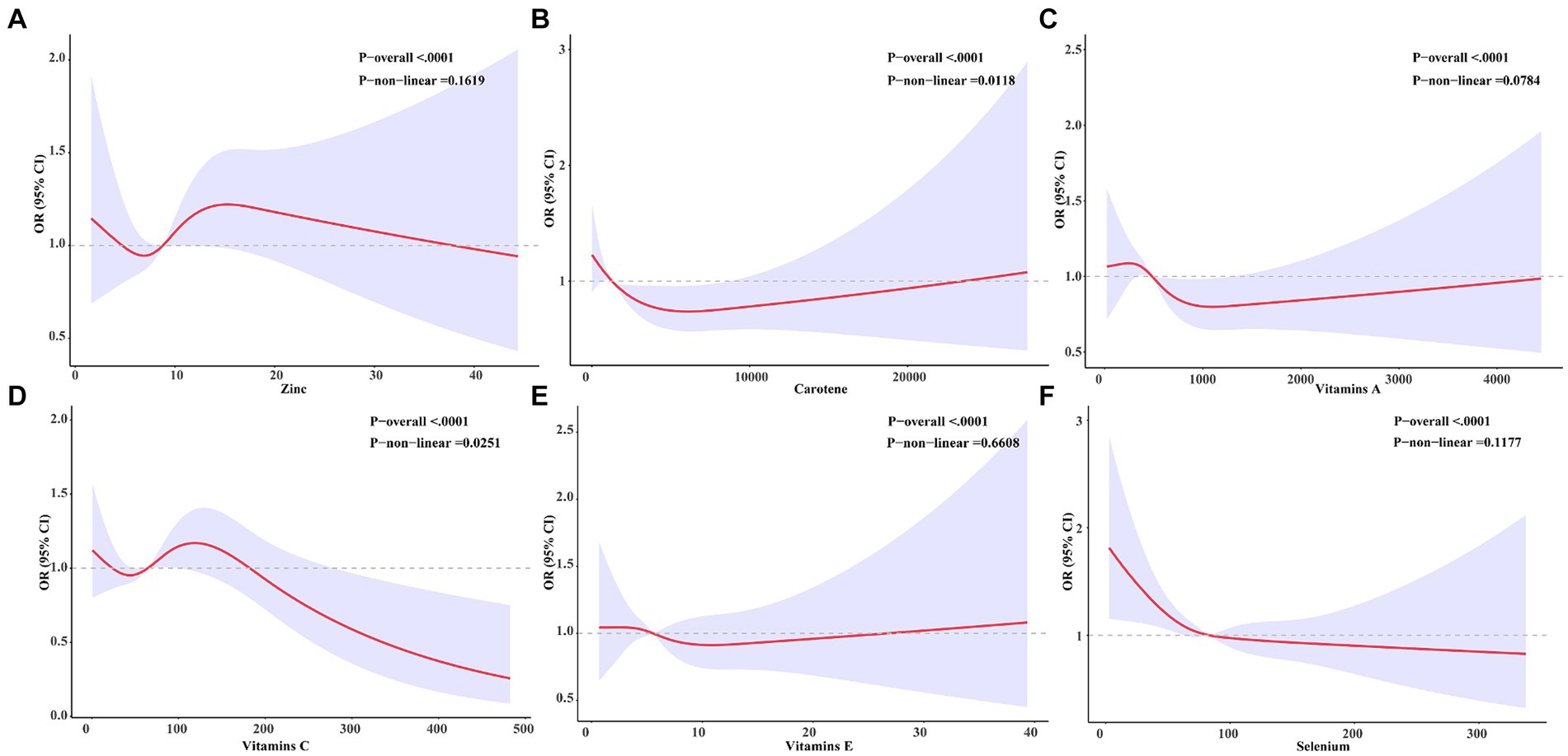
Figure 5. Six antioxidants were associated with a dose–response relationship to constipation in female participants. Zinc (A), Carotene (B), Vitamin A (C), Vitamins C (D), Vitamins D (E), Selenium (F).
Stratified analysis was performed based on age, gender, race, BMI, education, family PIR, diabetes, cancer, hypertension, and activity. Forest plots of Figure 6 were generated, which demonstrates a persistent negative correlation between CDAI and the risk of constipation. Simultaneously, we noted that among men, the inverse association between CDAI and constipation risk was notably significant among younger participants and those of non-Hispanic White ethnicity. A similar trend was observed among women. No significant interaction was detected between these variables (all p for interaction >0.05; Figures 7, 8).
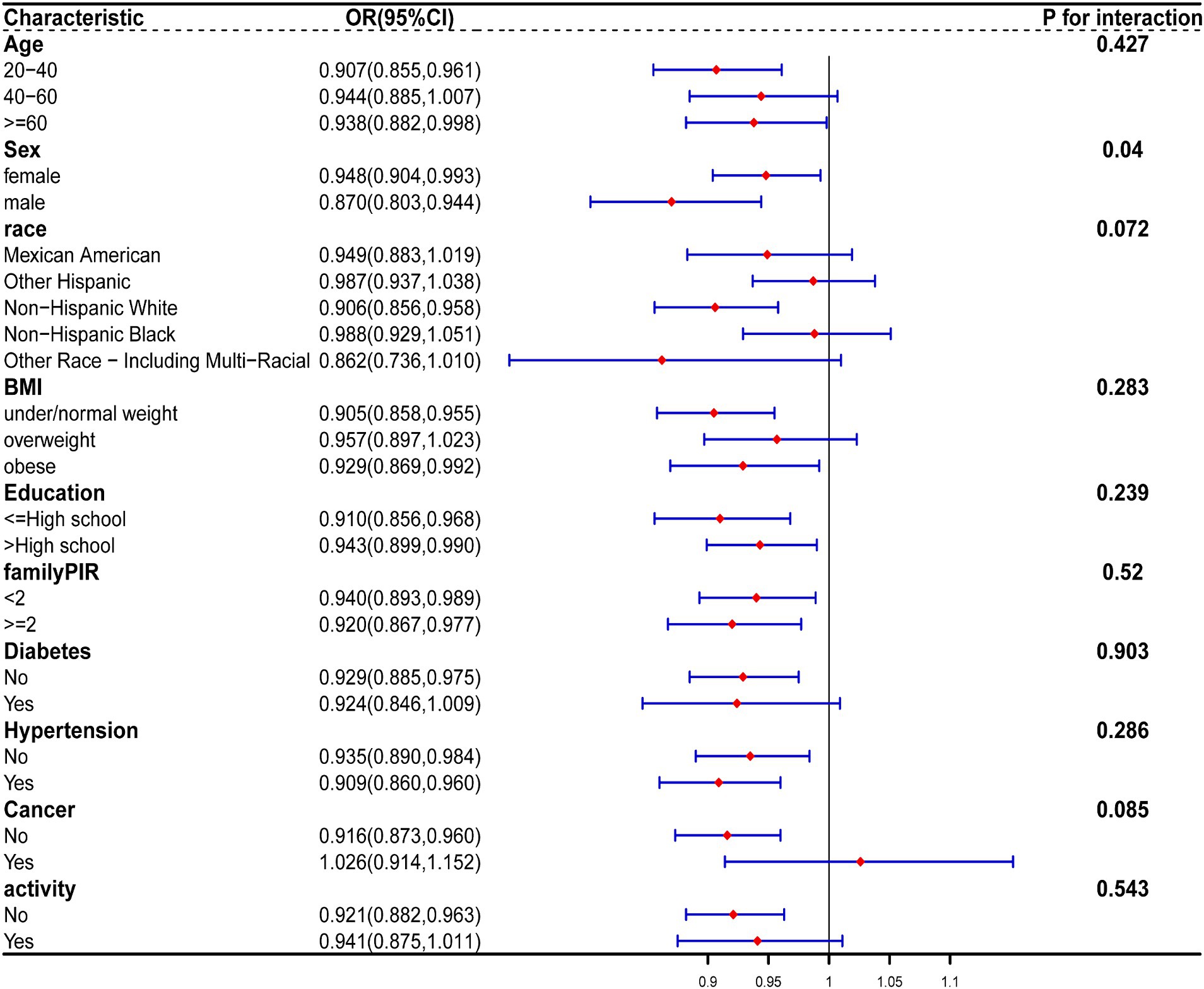
Figure 6. The relationship between CDAI and covariates was assessed by weighted stratified and interaction analysis. The covariates include age, race, BMI, educational levels, smoking, PIR, diabetes, hypertension, cancer, and vigorous physical activity.
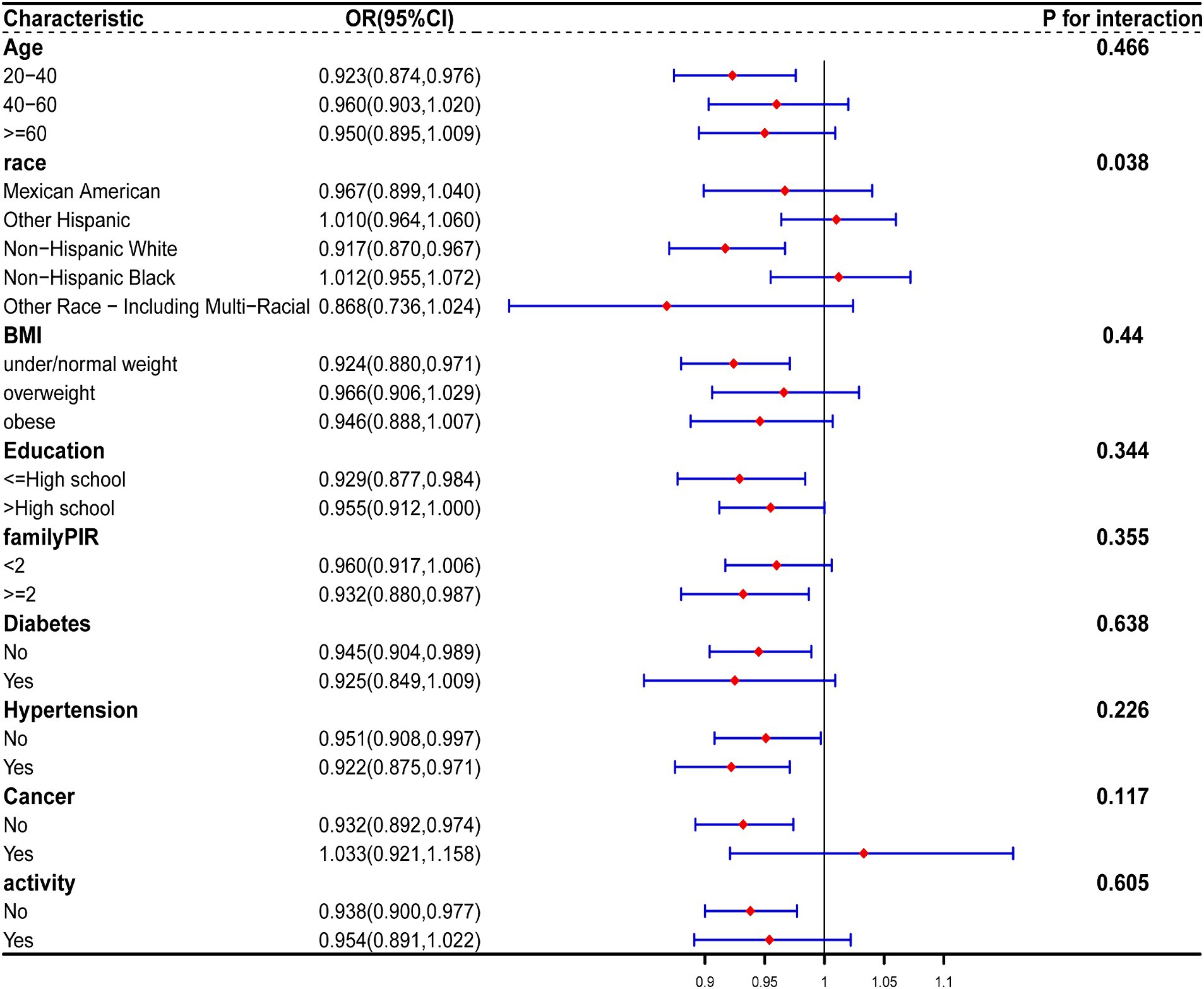
Figure 7. The relationship between CDAI and covariates in men was assessed by weighted stratified and interaction analysis. The covariates include age, race, BMI, educational levels, smoking, PIR, diabetes, hypertension, cancer, and vigorous physical activity.
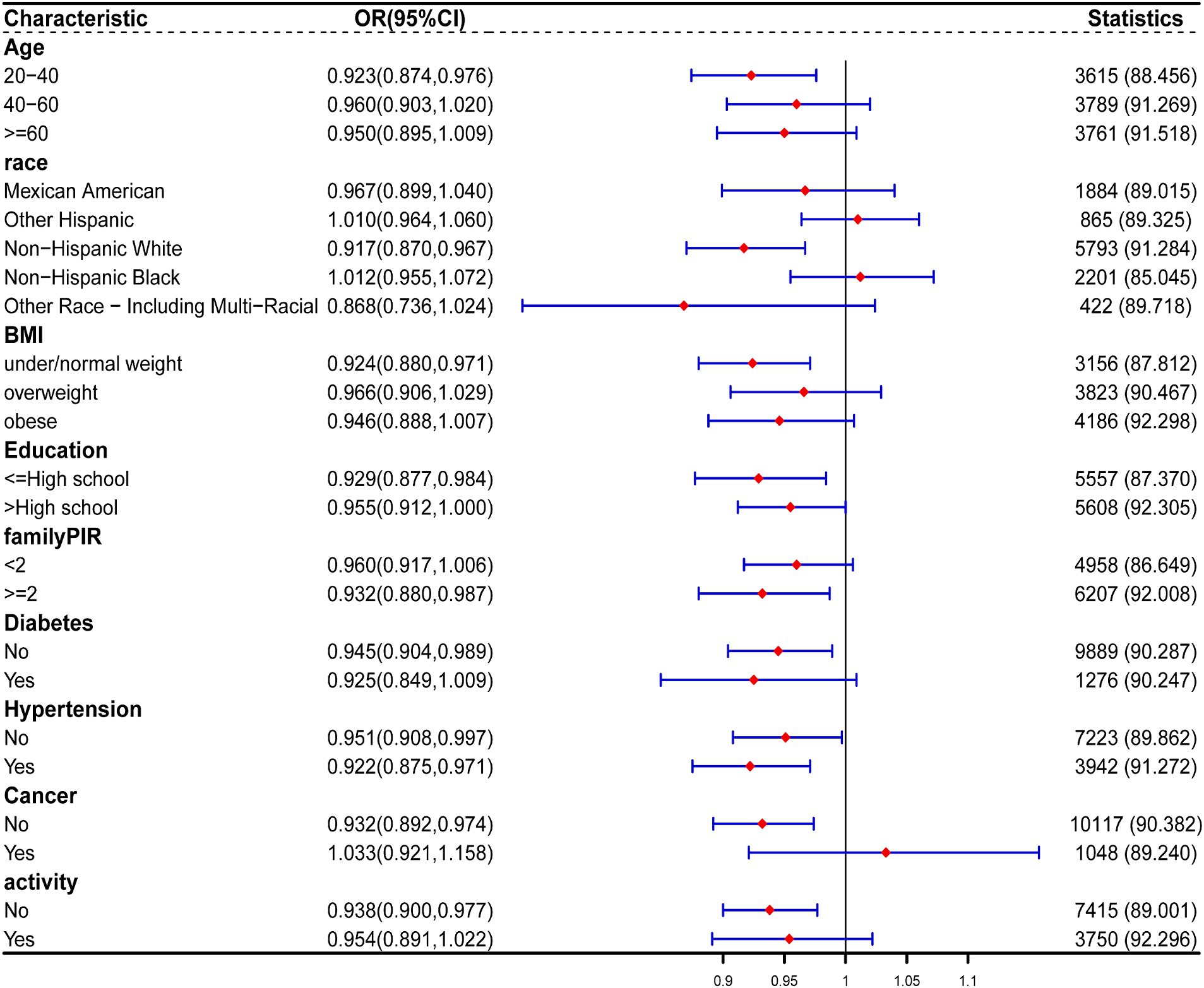
Figure 8. The relationship between CDAI and covariates in women was assessed by weighted stratified and interaction analysis. The covariates include age, race, BMI, educational levels, smoking, PIR, diabetes, hypertension, cancer, and vigorous physical activity.
Our study’s fully adjusted model III revealed a negative association between CDAI and constipation. Additionally, individuals in the highest quartile of CDAI exhibited a 40.1% reduced likelihood of constipation in comparison to those in the lowest quartile. Nevertheless, subgroup analysis by gender uncovered a negative correlation between CDAI and constipation among males. Males in the highest quartile of CDAI demonstrated a 60% reduced likelihood of constipation compared to their counterparts in the lowest quartile. However, female patients exhibited no association with constipation in the fully adjusted model. Following adjustment for all confounding factors, selenium emerged as a potential independent component associated with constipation. Dose–response analysis indicated a linear relationship between CDAI and constipation.
To the best of our knowledge, our study represents the first cross-sectional investigation exploring the correlation between CDAI levels and constipation. Based on the above, we launched dietary and lifestyle management serves as a primary strategy for preventing and treating constipation. We suggest additional research in this area.
Oxidative stress denotes an imbalance between antioxidants and prooxidants, leading to subsequent tissue and organ damage. The accumulation of reactive oxygen species (ROS) can result in the oxidation of DNA, proteins, carbohydrates, and lipids, which leads to cellular apoptosis and organ dysfunction. However, increasing evidence supports oxidative stress as an important precipitating factor for constipation. Inhibiting oxidative stress can maintain redox homeostasis, thereby alleviating constipation (13, 28). The dietary antioxidant capacity bears significant potential in predicting adult health outcomes (29). Previous studies have demonstrated that crude polysaccharides from Cistanche deserticola may alleviate constipation by attenuating oxidative stress to safeguard intestinal neurons (13). Findings from NHANES also indicate an association between low dietary fiber and fluid intake and constipation (30). Several individual components exhibiting antioxidant activity have been investigated for their potential role in constipation in preclinical experiments, including kale (31), a green kiwifruit powder (32), and dragon fruit oligosaccharide (33). Clinical studies have found that prune juice containing sorbitol, pectin, and polyphenol may alleviate constipation (34). The dietary quality has been demonstrated to exhibit a significant relationship with constipation (35). Thus, our study may further bolster the link between antioxidant intake and diet-related constipation. Gender differences also play an important role in the balance of antioxidants (36). Despite the mounting evidence implicating antioxidants in constipation, the influence of gender on the outcomes remains uncertain. A recent study has shown that increasing intake of lycopene can improve intestinal function in men (37), providing further support for the existence of gender differences, as demonstrated by our research. Elevating CDAI levels is inclined to afford protection against constipation symptoms in males but not in females, mirroring the higher prevalence of constipation among females. Furthermore, our further analysis of antioxidant components shows a negative correlation between selenium and constipation. Nutrients and components are consumed in combination and may interact with each other in complex ways (28). The association between individual components and diseases may be difficult to explore and explain (12). Moreover, previous research has mainly focused on individual antioxidants, but the current trend is increasingly recognizing the importance of diet as a whole (13). Consequently, prudence should be exercised when interpreting the effects of individual antioxidant components on diseases.
A notable strength of this study lies in its utilization of NHANES data, acquired through a stratified multistage probability sampling approach, thereby augmenting the reliability and representativeness of the investigation. Furthermore, we accounted for potential confounders, such as gender, age, race, education level, family PIR, BMI, activity level, smoking, and drinking, in our analyses to minimize the effects of confounding variables. However, this study does have some limitations. Firstly, recall-based questionnaire assessment may introduce measurement errors and inaccuracies when assessing antioxidant components. Secondly, bias is inevitable in cross-sectional studies. Moreover, despite adjusting for certain potential confounders, we cannot completely disregard the potential influence of other confounding variables.
In conclusion, we observed that CDAI acts as a protective factor against constipation in males. Patients with high levels of CDAI tend to have a lower incidence of constipation. There is a linear relationship between the CDAI level and the constipation risk. In addition, we also found that changes per milligram of selenium were independently associated with constipation, and changes per milligram of vitamin E in men were independently associated with constipation. Therefore, We suggest further exploration of antioxidants within dietary patterns and advise careful interpretation of the effects of individual antioxidant components. Furthermore, given the potential of diet as a modifiable intervention with significant health implications, continued exploration in this area is crucial, especially through larger-scale prospective cohort studies.
Publicly available datasets were analyzed in this study. This data can be found at: https://www.cdc.gov/nchs/nhanes/index.htm.
The studies involving humans were approved by NCHS IRB/ERB Protocol Number: NHANES 2011–2012 (Protocol #2011–17); NHANES 2013–2014 (Continuation of Protocol #2011–17). The patients/participants provided their written informed consent to participate in this study. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
WS: Formal analysis, Methodology, Writing – original draft, Conceptualization, Writing – review & editing, Data curation, Validation, Visualization. YW: Methodology, Writing – review & editing, Conceptualization, Data curation. LH: Writing – review & editing, Visualization. YL: Writing – review & editing, Methodology. HL: Writing – review & editing, Formal analysis. YT: Writing – review & editing, Formal analysis. ZJ: Writing – review & editing, Formal analysis. DS: Funding acquisition, Project administration, Resources, Writing – review & editing, Supervision. CX: Project administration, Writing – review & editing, Supervision.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This research was funded by the General Program of the National Natural Science Foundation of China, grant nos. 82070554 and 81770537; the Major Scientific and Technological Special Project for Public Health in Tianjin, grant no. 21ZXGWSY00080; the Tianjin Medical University General Hospital Clinical Research Program, grant no. 22ZYYLCCG06.
We want to acknowledge the participants and investigators of the National Health and Nutrition Examination Surveys. In addition, we are grateful for Figdraw; the graphic summary was drawn by Figdraw (https://www.figdraw.com).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Brenner, DM, Corsetti, M, Drossman, D, Tack, J, and Wald, A. Perceptions, definitions, and therapeutic interventions for occasional constipation: a Rome working group consensus document. Clin Gastroenterol Hepatol. (2024) 22:397–412. doi: 10.1016/j.cgh.2023.08.044
2. Higgins, PDR, and Johanson, JF. Epidemiology of constipation in North America: a systematic review. Am J Gastroenterol. (2004) 99:750–9. doi: 10.1111/j.1572-0241.2004.04114.x
3. Belsey, J, Greenfield, S, Candy, D, and Geraint, M. Systematic review: impact of constipation on quality of life in adults and children. Aliment Pharmacol Ther. (2010) 31:938–49. doi: 10.1111/j.1365-2036.2010.04273.x
4. Bharucha, AE, Locke, GR, Zinsmeister, AR, Seide, BM, McKeon, K, Schleck, CD, et al. Differences between painless and painful constipation among community women. Am J Gastroenterol. (2006) 101:604–12. doi: 10.1111/j.1572-0241.2006.00435.x
5. Mugie, SM, Benninga, MA, and Di Lorenzo, C. Epidemiology of constipation in children and adults: a systematic review. Best Pract Res Clin Gastroenterol. (2011) 25:3–18. doi: 10.1016/j.bpg.2010.12.010
6. Kinnunen, O. Study of constipation in a geriatric hospital, day hospital, dold people’s home and at home. Aging Clin Exp Res. (1991) 3:161–70. doi: 10.1007/BF03323997
7. Forootan, M, Bagheri, N, and Darvishi, M. Chronic constipation: a review of literature. Medicine (Baltimore). (2018) 97:e10631. doi: 10.1097/MD.0000000000010631
8. Bharucha, AE, and Wald, A. Chronic constipation. Mayo Clin Proc. (2019) 94:2340–57. doi: 10.1016/j.mayocp.2019.01.031
9. Wang, JY, Wang, YL, Zhou, SL, and Zhou, JF. May chronic childhood constipation cause oxidative stress and potential free radical damage to children? Biomed Environ Sci. (2004) 17:266–72.
10. Hajji, N, Wannes, D, Jabri, MA, Rtibi, K, Tounsi, H, Abdellaoui, A, et al. Purgative/laxative actions of Globularia alypum aqueous extract on gastrointestinal-physiological function and against loperamide-induced constipation coupled to oxidative stress and inflammation in rats. Neurogastroenterol Motil. (2020) 32:e13858. doi: 10.1111/nmo.13858
11. Yao, Z, Fu, S, Ren, B, Ma, L, and Sun, D. Based on network pharmacology and gut microbiota analysis to investigate the mechanism of the laxative effect of Pterostilbene on Loperamide-induced slow transit constipation in mice. Front Pharmacol. (2022) 13:913420. doi: 10.3389/fphar.2022.913420
12. Aleksandrova, K, Koelman, L, and Rodrigues, CE. Dietary patterns and biomarkers of oxidative stress and inflammation: a systematic review of observational and intervention studies. Redox Biol. (2021) 42:101869. doi: 10.1016/j.redox.2021.101869
13. Jiang, H-Y, Ma, R-A, Ji, F-L, Liu, Y, Wang, B, Fu, S-Q, et al. Structure characterization of polysaccharides from Cistanche deserticola and their neuroprotective effects against oxidative stress in slow transit constipation mice. Int J Biol Macromol. (2024) 260:129527. doi: 10.1016/j.ijbiomac.2024.129527
14. Wang, C, Zhang, L, and Li, L. Association between selenium intake with chronic constipation and chronic diarrhea in adults: findings from the National Health and nutrition examination survey. Biol Trace Elem Res. (2021) 199:3205–12. doi: 10.1007/s12011-020-02451-x
15. Zhang, L, Du, Z, Li, Z, Yu, F, and Li, L. Association of dietary magnesium intake with chronic constipation among US adults: evidence from the National Health and nutrition examination survey. Food Sci Nutr. (2021) 9:6634–41. doi: 10.1002/fsn3.2611
16. Zhao, X, Wang, L, and Quan, L. Association between dietary phosphorus intake and chronic constipation in adults: evidence from the National Health and nutrition examination survey. BMC Gastroenterol. (2023) 23:24. doi: 10.1186/s12876-022-02629-8
17. Taba Taba Vakili, S, Nezami, BG, Shetty, A, Chetty, VK, and Srinivasan, S. Association of high dietary saturated fat intake and uncontrolled diabetes with constipation: evidence from the National Health and nutrition examination survey. Neurogastroenterol Motil. (2015) 27:1389–97. doi: 10.1111/nmo.12630
18. Yang, S, Wu, X-L, Wang, S-Q, Guo, X-L, Guo, F-Z, and Sun, X-F. Association of Dietary Energy Intake with Constipation among men and Women: results from the National Health and nutrition examination survey. Front Nutr. (2022) 9:856138. doi: 10.3389/fnut.2022.856138
19. Yu, YC, Paragomi, P, Wang, R, Jin, A, Schoen, RE, Sheng, LT, et al. Composite dietary antioxidant index and the risk of colorectal cancer: findings from the Singapore Chinese health study. Int J Cancer. (2022) 150:1599–608. doi: 10.1002/ijc.33925
20. Zhao, L, Sun, Y, Cao, R, Wu, X, Huang, T, and Peng, W. Non-linear association between composite dietary antioxidant index and depression. Front Public Health. (2022) 10:727. doi: 10.3389/fpubh.2022.988727
21. Wright, ME. Development of a comprehensive dietary antioxidant index and application to lung Cancer risk in a cohort of male smokers. Am J Epidemiol. (2004) 160:68–76. doi: 10.1093/aje/kwh173
22. Li, S, and Zeng, M. The association between dietary inflammation index and bone mineral density: results from the United States National Health and nutrition examination surveys. Ren Fail. (2023) 45:200. doi: 10.1080/0886022X.2023.2209200
23. Wu, M, Si, J, Liu, Y, Kang, L, and Xu, B. Association between composite dietary antioxidant index and hypertension: insights from NHANES. Clin Exp Hypertens. (2023) 45:712. doi: 10.1080/10641963.2023.2233712
24. Wang, L, and Yi, Z. Association of the Composite dietary antioxidant index with all-cause and cardiovascular mortality: a prospective cohort study. Front Cardiovasc Med. (2022) 9:930. doi: 10.3389/fcvm.2022.993930
25. Luu, HN, Wen, W, Li, H, Dai, Q, Yang, G, Cai, Q, et al. Are dietary antioxidant intake indices correlated to oxidative stress and inflammatory marker levels? Antioxid Redox Signal. (2015) 22:951–9. doi: 10.1089/ars.2014.6212
26. Zhang, X, Chen, S, Zhang, M, Ren, F, Ren, Y, Li, Y, et al. Effects of fermented Milk containing Lacticaseibacillus paracasei strain Shirota on constipation in patients with depression: a randomized, double-blind. Placebo Control Trial Nutrients. (2021) 13:2238. doi: 10.3390/nu13072238
27. McCrea, GL, Miaskowski, C, Stotts, NA, Macera, L, and Varma, MG. A review of the literature on gender and age differences in the prevalence and characteristics of constipation in North America. J Pain Symptom Manag. (2009) 37:737–45. doi: 10.1016/j.jpainsymman.2008.04.016
28. Choi, K, Chen, J, Mitra, S, and Sarna, SK. Impaired integrity of DNA after recovery from inflammation causes persistent dysfunction of colonic smooth muscle. Gastroenterology. (2011) 141:1293–1301.e3. doi: 10.1053/j.gastro.2011.06.074
29. Nascimento-Souza, MA, Paiva, PG, Martino, HSD, and Ribeiro, AQ. Dietary total antioxidant capacity as a tool in health outcomes in middle-aged and older adults: a systematic review. Crit Rev Food Sci Nutr. (2017) 58:905–12. doi: 10.1080/10408398.2016.1230089
30. Markland, AD, Palsson, O, Goode, PS, Burgio, KL, Busby-Whitehead, J, and Whitehead, WE. Association of low Dietary Intake of Fiber and liquids with constipation: evidence from the National Health and nutrition examination survey. Am J Gastroenterol. (2013) 108:796–803. doi: 10.1038/ajg.2013.73
31. Nishimoto, Y, Salim, F, Yamauchi, Y, Mori, Y, Murakami, S, Suzuki, A, et al. Kale improves bowel movements in constipated women and affects some intestinal microbes and metabolites: a pilot study. Front Nutr. (2023) 10:683. doi: 10.3389/fnut.2023.1247683
32. Goya-Jorge, E, Bondue, P, Gonza, I, Laforêt, F, Antoine, C, Boutaleb, S, et al. Butyrogenic, bifidogenic and slight anti-inflammatory effects of a green kiwifruit powder (kiwi FFG®) in a human gastrointestinal model simulating mild constipation. Food Res Int. (2023) 173:113348. doi: 10.1016/j.foodres.2023.113348
33. Khuituan, P, K-da, S, Bannob, K, Hayeeawaema, F, Peerakietkhajorn, S, Tipbunjong, C, et al. Prebiotic oligosaccharides from dragon fruits alter gut motility in mice. Biomed Pharmacother. (2019) 114:108821. doi: 10.1016/j.biopha.2019.108821
34. Koyama, T, Nagata, N, Nishiura, K, Miura, N, Kawai, T, and Yamamoto, H. Prune juice containing sorbitol, pectin, and polyphenol ameliorates subjective complaints and hard feces while normalizing stool in chronic constipation: a randomized placebo-controlled trial. Am J Gastroenterol. (2022) 117:1714–7. doi: 10.14309/ajg.0000000000001931
35. Liu, Q, Kang, Y, and Yan, J. Association between overall dietary quality and constipation in American adults: a cross-sectional study. BMC Public Health. (2022) 22:1971. doi: 10.1186/s12889-022-14360-w
36. Kamper, EF, Chatzigeorgiou, A, Tsimpoukidi, O, Kamper, M, Dalla, C, Pitychoutis, PΜ, et al. Sex differences in oxidant/antioxidant balance under a chronic mild stress regime. Physiol Behav. (2009) 98:215–22. doi: 10.1016/j.physbeh.2009.05.011
Keywords: antioxidant, dietary complex antioxidant index, constipation, National Health and Nutrition Examination Survey, oxidative stress
Citation: Sun W, Wang Y, Han L, Liu Y, Liu H, Tong Y, Jiang Z, Xu C and Sun D (2024) Association between different composite dietary antioxidant indexes and constipation in American male adults: a cross-sectional study. Front. Nutr. 11:1404400. doi: 10.3389/fnut.2024.1404400
Edited by:
Musheerul Hassan, Ilia State University, GeorgiaReviewed by:
Gulzar Ahmed Rather, Sathyabama Institute of Science and Technology, IndiaCopyright © 2024 Sun, Wang, Han, Liu, Liu, Tong, Jiang, Xu and Sun. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Daqing Sun, c2RxY2hyaXMyMDE5QHRtdS5lZHUuY24=; Chen Xu, eGMxOTgxMjlAMTYzLmNvbQ==;
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.