
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr. , 11 September 2024
Sec. Clinical Nutrition
Volume 11 - 2024 | https://doi.org/10.3389/fnut.2024.1402625
 Claudia N. Orozco-González1,2
Claudia N. Orozco-González1,2 Roxana M. Marquez-Herrera1,3
Roxana M. Marquez-Herrera1,3 Fabiola Martín-del-Campo1,3
Fabiola Martín-del-Campo1,3 Laura Cortés-Sanabria1
Laura Cortés-Sanabria1 Mariana Villasana-Ballesteros1
Mariana Villasana-Ballesteros1 Alfonso M. Cueto-Manzano1*
Alfonso M. Cueto-Manzano1*Background: In dialysis patients, on the one hand unwillingness to change negative lifestyle patterns is associated with worse nutritional status and unhealthy lifestyle, whereas on the other, pica may be highly prevalent. However, it is not known whether pica is associated with unwillingness to change negative lifestyle behaviors, as well as with consumption of different types of foods. This study aimed to investigate this issue.
Methods: This is a cross-sectional study in dialysis patients. Lifestyle was assessed using the self-administered Instrument to Measure Lifestyle Questionnaire (IMEVID). Pica diagnosis was established according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. A food frequency questionnaire was performed and self-reported willingness to change was determined by a trans-theoretical model staging inventory.
Results: Compared with patients without pica, those with pica (particularly hard pica) had lower willingness to change unhealthy behavior in the case of diet (22% vs. 46% in precontemplation/contemplation stages, respectively) and exercise (43% vs. 62% in precontemplation/contemplation stages, respectively). Patients with hard pica had significantly (p < 0.05) lower scores in almost all dimensions of the lifestyle questionnaire than those in the no pica group: diet (23.9 vs. 26.8, respectively), physical activity (5.5 vs. 7, respectively), knowledge of disease (5.7 vs. 6.4, respectively), emotion management (6.6 vs. 8, respectively) and adherence to treatment (13.4 vs. 14.7, respectively), but not in the consumption of tobacco and alcohol. Compared to patients with no pica, those with hard pica ate vegetables and fruits less frequently, and dairy products, fried foods and soda more frequently.
Conclusions: Pica was more frequently observed in patients with lower willingness to change negative habits of diet and exercise, in those who had more unhealthy behaviors in diet, exercise and emotion management dimensions and adherence to treatment, as well as in those who ate less frequently healthful foods and more frequently unhealthy foods.
In patients with end-stage kidney disease (ESKD) on dialysis, unwillingness to change unhealthy lifestyle is associated with worse nutritional status, and with lower consumption of healthy foods and higher intake of unhealthy ones (1–5). Thus, to improve clinical outcomes and decrease complications, it is necessary to recognize the healthy lifestyle non-adherence risks and design tailored strategies to increase motivation and enhance changes of negative lifestyle.
On the other hand, pica, defined as the intake of a substance or object without calories or nutritional properties at least once a month (6), has been the subject of study by multiple disciplines; thus, it has been interpreted in multiple ways as an eating disorder, behavioral problem, symptom of mental illness, expression of nutrient deficiency, abandonment, neglect, poverty or hunger. Etiology of pica is not completely known; sometimes is regarded as a cause and sometimes a consequence (7–9). In patients without kidney disease, pica has been reported to have a 2.35-fold increased odds association with anemia and lower zinc concentrations in a recent meta-analysis (10). In iron deficiency, pagophagia appears to be common in United States, affecting 25% of patients, whereas geophagia is more common in the rest of the world (7); ice seems to be the most common pica item (87%) in non-pregnant women and children (8).
However, in patients with CKD less information is available (11–13), and ice pica was the most frequently found (46%), followed by the soil pica (29%) (14).
Scarce data have been published regarding the association between pica and nutritional variables; in patients without kidney disease, pica was associated with worse nutritional status (15–17); more recently, it has been associated with unmet macronutrient and calorie requirements in patients with ESKD (14). Notwithstanding, it is not known whether pica is associated with the patient's willingness to make positive lifestyle changes and the intake of healthy or unhealthy foods.
Therefore, the present study was aimed to investigate the association between the presence of pica and the willingness to change negative lifestyle behaviors in patients on dialysis, as well as the consumption of different types of foods.
This is a cross-sectional study of ESKD patients from a tertiary health-care teaching hospital. Patients in the living donor kidney transplant program were included if they were on dialysis at least 6 months, >18 years old, with any cause of kidney disease and granted their verbal informed consent. They were excluded if had pregnancy, breast feeding, previous transplant, any evidence of infection, or mental illness. Schizophrenia, intellectual disability, organic mental problems, and severe anxious or depressive disorders are specifically excluded before patients enter in our transplant program. This study adhered to the Declaration of Helsinki and was approved by the Local Committee of Research and Ethics (No. R-2016-1301-95).
Socio-demographical and clinical variables were obtained from interview and clinical files; weight was measured just after hemodialysis session. A flow chart showing procedures once the patients were included in the study is shown in Figure 1. Lifestyle was evaluated by the self-administered Instrument to Measure Diabetic Lifestyle Questionnaire (IMEVID) (18), which is made up of 25 items evaluating seven domains: nutrition, physical activity, tobacco consumption, alcohol consumption, emotion management, disease knowledge, and therapeutic adherence. Each item has three possible response options (individualized for each domain), with ratings of 0, 2 and 4 points; total score is 0–100, the higher the score the healthier the lifestyle. IMEVID questionnaire was first developed for diabetes mellitus; thus, the disease knowledge, emotion and adherence domains were modified to consider kidney disease instead of diabetes.
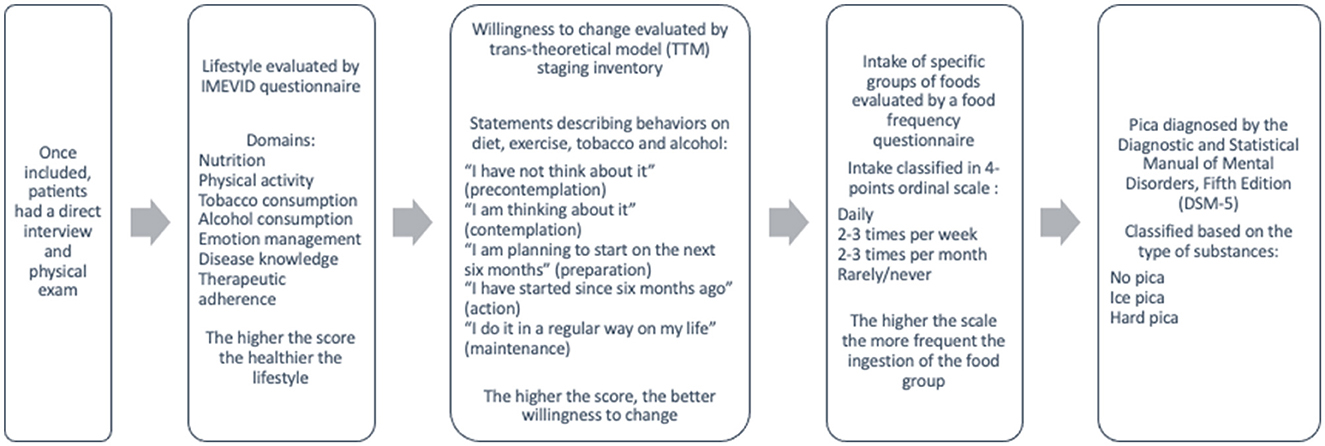
Figure 1. Flow chart of the study procedures.
Diagnosis of pica was established according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) (6) and was classified based on the type of ingested substances as: no pica, ice pica, and hard pica (i.e., starch, soil, clay, grass, paper, or other pica) (6). Of note, only the compulsive ice intake (recognition of intake without thirst) was classified as pica.
A food frequency questionnaire was performed in all patients to evaluate the intake of specific groups of foods; frequency intake answers were classified in a 4-points ordinal scale from never/rarely to daily; the higher the scale the more frequent the ingestion of the food group.
Self-reported willingness to change was determined by selecting a trans-theoretical model (TTM) staging inventory that includes statements reflecting the five stages of change (19). TTM proposes that persons are at varying points of willingness (or readiness) to adopt a specified health-related practice and move about a sequence of stages along a continuum of behavioral change. Participants select the statement that best describes their current behaviors on diet, exercise, tobacco and alcohol from the following 5-points ordinal scale options: (1) “I have not think about it” (precontemplation), (2) “I am thinking about it” (contemplation), (3) “I am planning to start on the next six months” (preparation), (4) “I have started since 6 months ago” (action), and (5) “I do it in a regular way on my life” (maintenance). The higher the score, the better willingness to change (20).
Data are shown as mean ± SD or median (25th to 75th percentiles) when dimensional variables had parametric or nonparametric distribution, respectively, or as percentage in the case of nominal variables. Comparisons between groups (no pica, ice pica and hard pica) were performed by ANOVA or Kruskal Wallis tests for dimensional variables, as appropriate: in the case of nominal variables, comparison analysis was done by means of χ2 or Fisher exact tests, as appropriate. Cronbach's alpha was calculated to assure internal consistency of the modified lifestyle questionnaire (IMEVID), a value above 0.7 was considered as adequate. A p < 0.05 was accepted as significant.
Four-hundred patients were studied. In the whole sample, mean age was 28 years, 280 (70%) were male, 76% had an unknown cause of kidney disease and only four patients had diabetes mellitus (three in the no pica group and one in the ice pica group). Pica was present in 42% of patients: 46% had ice pica, 29% soil, 14% two substances, 5% red brick, 3% paper, 2% soap, and 1% cattle pasture. Main sociodemographical, clinical and laboratory results are shown in Table 1.
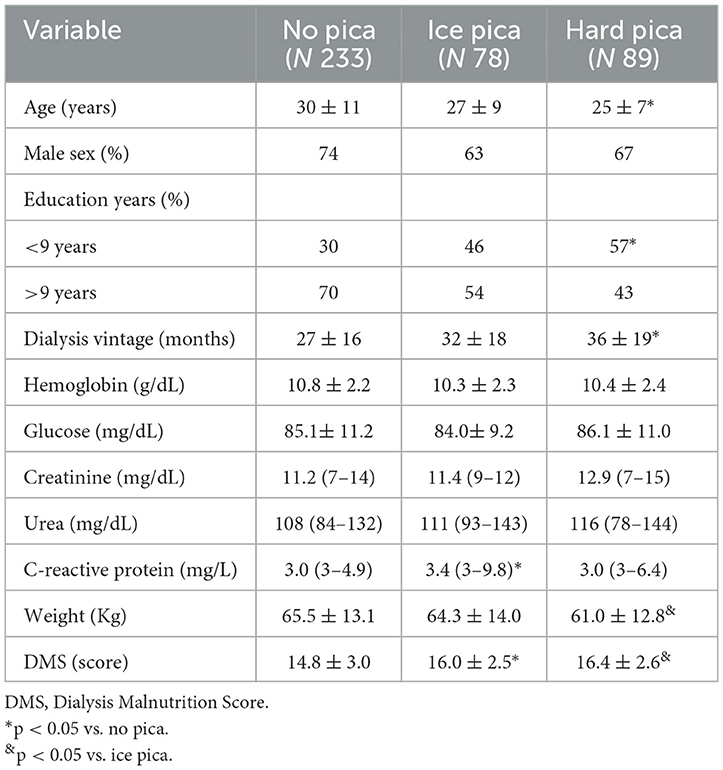
Table 1. Comparison of sociodemographic, clinical and biochemical variables according to the type of pica.
Results of willingness to change lifestyle behavior according to the presence of pica are shown in Figure 2. Patients with pica (particularly hard pica) had lower willingness to change behavior in the case of diet and exercise: a higher frequency were in the contemplation and a lower frequency in the action stages compared to patients in the no pica group. Noteworthy, most of patients reported themselves in the action and maintenance stages regarding tobacco and alcohol consumption without differences between groups.
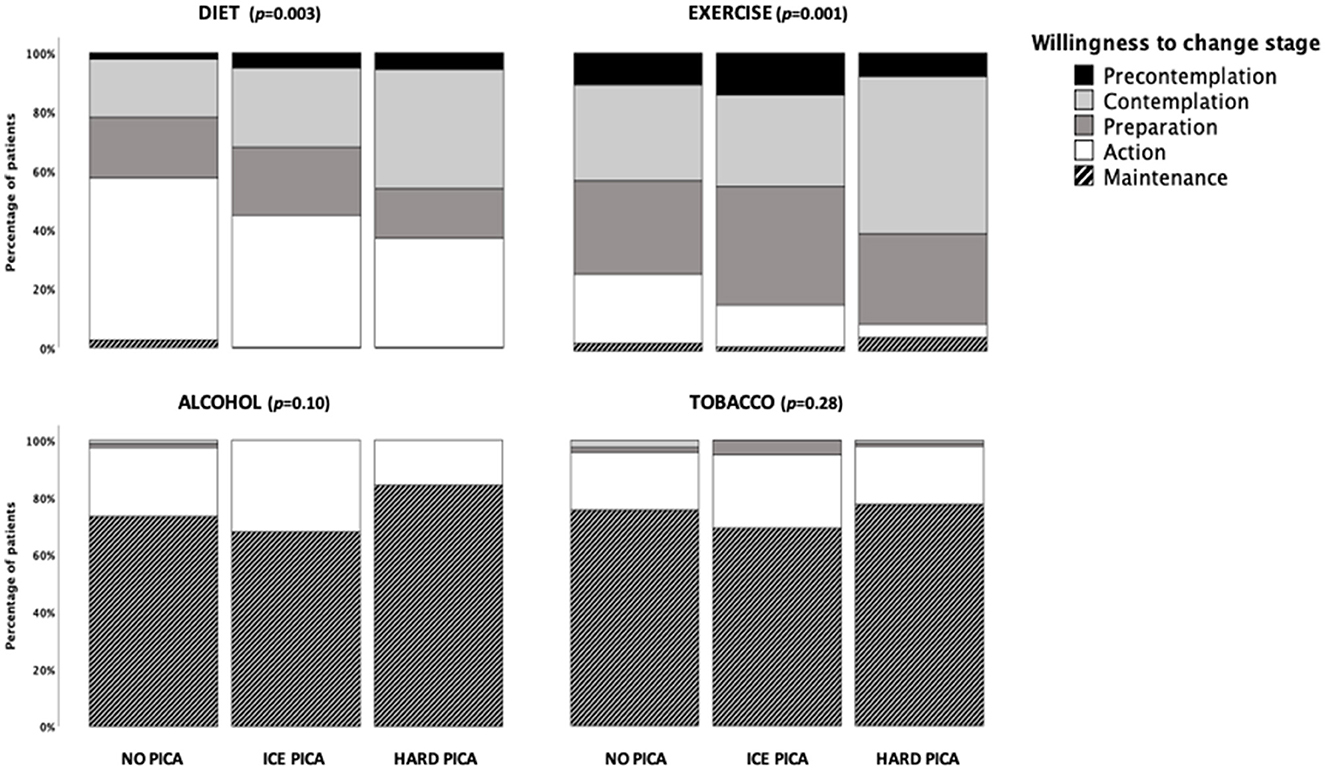
Figure 2. Results of the willingness to change lifestyle behavior according to the presence of pica.
Regarding lifestyle evaluation (Table 2), it was observed that patients with hard pica had lower scores in all dimensions (and consequently in the total score), except for tobacco and alcohol consumption, compared to patients without pica. Similarly, patients with ice pica scored significantly lower compared to the no pica group in total score, and in the emotion management and adherence to treatment dimensions. The hard pica group also had lower knowledge of disease score compared to patients with ice pica.
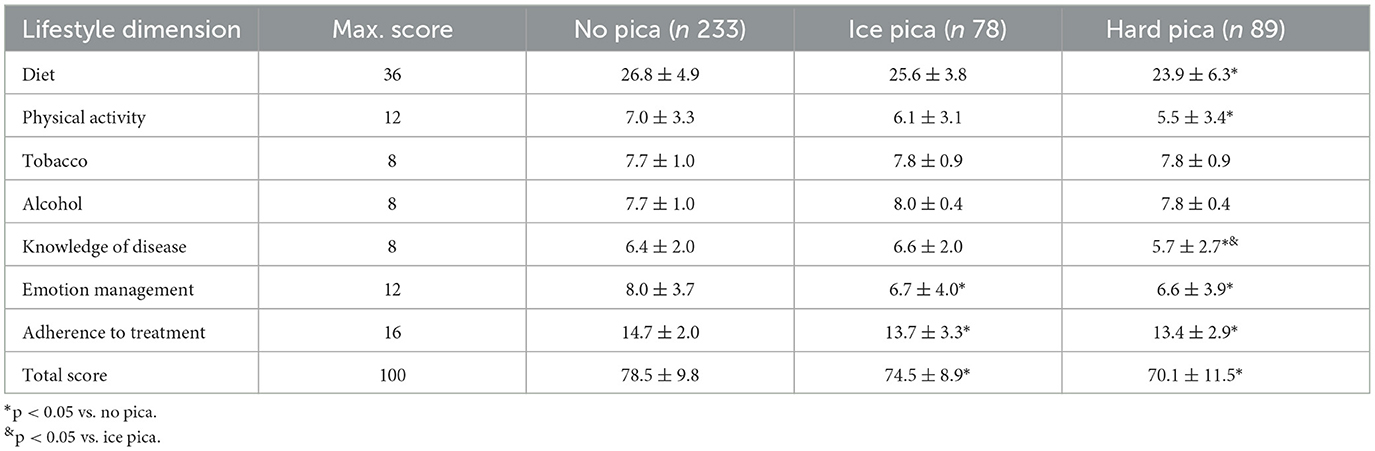
Table 2. Comparison of healthy lifestyle domains scores according to the presence of pica.
Analysis of food consumption frequency is shown in Table 3. Compared to patients with no pica, those with hard pica ate vegetables and fruits less frequently, whereas they ate dairy products, fried foods and soda more frequently, although the latter was significantly different only compared to patients with ice pica. Patients with ice pica consumed less frequently fish and more frequently processed meat compared to patients in the no pica group. No differences were observed between groups in legumes, tortillas, bread, pork, beef meat, chicken, egg and sugar intake frequency.

Table 3. Comparison of food consumption frequency according to the type of pica.
To our knowledge, this is the first study evaluating the association of the presence of pica with willingness to change lifestyle behaviors and food consumption in patients on dialysis. This study lays the groundwork for this under-evaluated aspect among ESKD patients.
In the current study, pica was found more frequently at younger ages, in those with a lower level of education and a longer duration of dialysis, which is consistent with other studies (11–13). It is possible that consumption of non-nutritive substances is more frequent in younger patients and with a lower educational level due to the lack of concern about its negative consequences. On the other hand, it is not completely clear why patients with ice pica had higher serum CRP; however, the mutual reinforcement between fluid overhydration and inflammation cannot be discarded (21). Overhydration was not investigated in depth in this study, although it was observed that weight was higher in patients with ice pica; inflammation in the presence of pica deserves to be considered in further investigations.
Patients with hard pica displayed lower willingness to change negative habits in diet and exercise behaviors than those without pica. The willingness to take actions for the control of medical conditions is a crucial component for successful self-management; the better readiness to change negative habits has higher self-management practices, dietary problem-solving skills, and lower barriers (22); once patients improved one lifestyle behavior, they may increase confidence in their ability to overcome barriers and achieve healthy lifestyle, increasing the probability to change other unhealthy behavior (23, 24). Interestingly, patients in all groups reported high willingness to change tobacco and alcohol consumption, with more frequent action and maintenance stages. The reason for this latter finding was not specifically investigated nor the temporality of the event (i.e., when the tobacco and alcohol consumption cessation started), but it is possible that being in a transplantation program could be partially implicated.
When comparing the lifestyle scores, patients with pica had lower results in diet, physical activity, knowledge of disease, emotion management and adherence to treatment, besides the overall score, compared to patients without pica. These results are in concordance with those of the willingness to change, as patients with the lowest willingness also had the worst habits in terms of diet and exercise, and all the groups had high scores for tobacco and alcohol consumption reflecting healthy habits in these latter aspects. In adults, pica is associated with pregnancy, intellectual disability, psychotic disorders and recurrent or masked depression (25, 26). The exact nature of the overlapping phenomenology is unclear, although hypotheses include shared neurological pathology (brain volume loss, temporal lobe injury, and neurotransmitter abnormalities), learned behavior, and coping mechanisms (symptoms that begin after stress) (27). Although many of these aspects were excluded in this study, it cannot be ruled out the participation of some of them in a subtle way, for example depression, or alteration in coping skills; this is an issue that deserve further investigation.
The reason why patients with hard pica eat vegetables and fruits less frequently, and dairy products, fried foods and soda more frequently, is not completely clear. Previous studies described the presence of pica and the ingestion of some substances but not of specific foods (14, 28–33). Thus, it was interesting in this study that the presence of pica was associated with frequent ingestion of unhealthy food and decreased ingestion of healthful one.
Adequate nutritional status is ideal for patients on dialysis, as it has been repeatedly shown that protein-energy wasting is associated with increased morbidity and mortality (28). However, achieving this goal is not easy nor frequent due to the intricated etiology of protein-energy wasting in this kind of patients. Diet interventions are very complex, and frequently require multiple individualized dietary restrictions, making more difficult patient's understanding and adherence (29). It has been demonstrated that pica (14) and the unwillingness to change unhealthy patterns are independently associated with a higher prevalence of malnutrition (1). Thus, the confluence of such factors, as well as the ingestion of unhealthy foods requires the participation of a multidisciplinary team, including renal dietitians, psychologists, social workers, and physicians. In addition, selection of foods must consider patient's culture, economy and preferences.
Unfortunately, exercise is not part of the standard clinical care, and is associated with multiple barriers, such as lack of motivation, inadequate equipment and training, fatigue, presence of multiple comorbidities and risks for complications and side effects, psychological alterations, lack of information, among others (30). This could explain why few patients of all groups were in the habit of including physical activity in their routinary life (31); however, such a finding was more apparent in patients with hard pica. Whether these factors are present individually or in conjunction, or in different degree, is not completely clear, but members of the healthcare team should have a more active role recommending physical activity (32, 33).
Main limitation of the present work is the cross-sectional design that allow us to establish association but not causality. Therefore, it cannot be established whether pica is cause or consequence of unwillingness to change negative habits, the presence of an unhealthy lifestyle or the consumption of certain foods. Other limitation may be that the frequency of consumption was summarized as group of foods and not detailed with specific foods. For example, beef meat included different types and cuts of meat, which we recognize they are not the same. However, as a first approximation, our results are very interesting and set up the basis for future prospective studies on a topic not deeply addressed before.
In conclusion, the presence of pica was more frequently observed in patients with lower willingness to change their negative habits in the case of diet and exercise, in those who had more unhealthy behaviors in the diet, exercise and emotion management dimensions and lower adherence to treatment, as well as in those who ate less frequently healthful foods and more frequently unhealthy foods.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Local Committee of Research and Ethics (No. R-2016-1301-95), Hospital de Especialidades, CMNO. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
CO-G: Conceptualization, Formal analysis, Methodology, Writing – original draft, Writing – review & editing, Data curation, Investigation. RM-H: Investigation, Writing – review & editing. FM: Formal analysis, Investigation, Writing – review & editing. LC-S: Writing – review & editing. MV-B: Investigation, Writing – review & editing. AC-M: Conceptualization, Formal analysis, Methodology, Resources, Supervision, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Orozco-González CN, Cortés-Sanabria L, Márquez-Herrera RM, Martín-Del-Campo-López F, Gómez-García EF, Rojas-Campos E, et al. Willingness to change diet and exercise behavior is associated with better lifestyle in dialysis patients close to a kidney transplant. Clin Nutr. (2022) 47:277–82. doi: 10.1016/j.clnesp.2021.11.032
2. Lafranca JA, IJzermans JN, Betjes MG, Dor FJ. Body mass index and outcome in renal transplant recipients: a systematic review and meta-analysis. BMC Med. (2015) 13:111. doi: 10.1186/s12916-015-0387-3
3. Zimbudzi E, Lo C, Ranasinha S, Kerr PG, Polkinghorne KR, Teede H, et al. The association between patient activation and self-care practices: a crosssectional study of an Australian population with comorbid diabetes and chronic kidney disease. Health Expect. (2017) 20:1375e84. doi: 10.1111/hex.12577
4. Ahmadi SF, Zahmatkesh G, Streja E, Molnar MZ, Rhee CM, Kovesdy CP, et al. Body mass index and mortality in kidney transplant recipients: a systematic review and meta-analysis. Am J Nephrol. (2014) 40:315e24. doi: 10.1159/000367812
5. Wissing KM, Pipeleers L. Obesity, metabolic syndrome and diabetes mellitus after renal transplantation: prevention and treatment. Transplant Rev. (2014) 28:37e46. doi: 10.1016/j.trre.2013.12.004
6. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM V). (2013). Arlington, VA: Editorial Medica Panamericana SA de CV (Spanish Edition). Fifth Edition.
7. Borgna-Pignatti C, Zanella S. Pica as a manifestation of iron deficiency. Expert Rev Hematol. (2016) 9:1075–80. doi: 10.1080/17474086.2016.1245136
8. Barton JC, Barton JC, Bertoli LF. Pica associated with iron deficiency or depletion: clinical and laboratory correlates in 262 non-pregnant adult outpatients. BMC Blood Disord. (2010) 10:9. doi: 10.1186/1471-2326-10-9
9. Young SL, Khalfan SS, Farag TH, Kavle JA, Ali SM, Hajji H, et al. Association of pica with anemia and gastrointestinal distress among pregnant women in Zanzibar, Tanzania. Am J Trop Med Hyg. (2010) 83:144–51. doi: 10.4269/ajtmh.2010.09-0442
10. Miao D, Young SL, Golden CD. A meta-analysis of pica and micronutrient status. Am J Hum Biol. (2015) 27:84–93. doi: 10.1002/ajhb.22598
11. Ward P, Kutner NG. Reported pica behavior in a sample of incident dialysis patients. J Ren Nutr. (1999) 9:14–20. doi: 10.1016/S1051-2276(99)90017-1
12. Katsoufis CP, Kertis M, McCullough J, Pereira T, Seeherunvong W, Chandar J, et al. Pica: an important and unrecognized problem in pediatric dialysis patients. J Ren Nutr. (2012) 22:567–71. doi: 10.1053/j.jrn.2011.10.038
13. Stillman MA. The Incidence of Pica in a Sample of Dialysis Patients. (2008). Available at: https://www.semanticscholar.org/paper/e69ed135058df5827e8fa1a5e5ba1dcab0d73866 (accessed September 01, 2024).
14. Orozco-González CN, Cortés-Sanabria L, Cueto-Manzano AM, Corona-Figueroa B, Martínez-Ramírez HR, López-Leal J, et al. Prevalence of pica in patients on dialysis and its association with nutritional status. J Ren Nutr. (2019) 29:143–8. doi: 10.1053/j.jrn.2018.08.002
15. Ali SA, Hassan AA, Adam I. History of pica, obesity, and their associations with anemia in pregnancy: a community-based cross-sectional study. Life. (2023) 13:2220. doi: 10.3390/life13112220
16. Din ZU, Pervez L, Amir A, Abbas M, Khan I, Iqbal Z, et al. Parasitic infections, malnutrition and anemia among preschool children living in rural areas of Peshawar, Pakistan. Nutr Hosp. (2018) 35:1145–52. doi: 10.20960/nh.1685
17. Papini NM, Bulik CM, Chawner SJ, Micali N. Prevalence and recurrence of pica behaviors in early childhood: findings from the ALSPAC birth cohort. medRxiv [Preprint] 2023.06.04.23290951. (2023). doi: 10.1101/2023.06.04.23290951
18. López-Carmona JM, Ariza-Andraca CR, Rodríguez-Moctezuma JR, Munguía-Miranda C. Construcción y validación inicial de un instrumento para medir el estilo de vida en pacientes con diabetes mellitus tipo 2. Salud Publica Mex. (2003) 45:259–68. doi: 10.1590/S0036-36342003000400004
19. Fried TR, Redding CA, Martino S, Paiva A, Iannone L, Zenoni M, et al. Increasing engagement in advance care planning using a behaviour change model: Study protocol for the STAMP randomised controlled trials. BMJ Open. (2018) 8:e025340. doi: 10.1136/bmjopen-2018-025340
20. Klusmann V, Gow AJ, Robert P, Oettingen G. Using theories of behavior change to develop interventions for healthy aging. J Gerontol B Psychol Sci Soc Sci. (2021) 76:S191–205. doi: 10.1093/geronb/gbab111
21. Dekker MJE, van der Sande FM, van den Berghe F, Leunissen KML, Kooman JP. Fluid overload and inflammation axis. Blood Purif. (2018) 45:159–65. doi: 10.1159/000485153
22. Knight H, Stetson B, Krishnasamy S, Mokshagundam SP. Diet self-management and readiness to change in underserved adults with type 2 diabetes. Prim Care Diab. (2015) 9:219–25. doi: 10.1016/j.pcd.2014.09.007
23. Karloh M, Matias TS, de Oliveira JM, de Lima FF, Araújo Pinheiro DH, Barbosa GB, et al. Breaking barriers to rehabilitation: the role of behavior change theories in overcoming the challenge of exercise-related behavior change. Braz J Phys Ther. (2023) 27:100574. doi: 10.1016/j.bjpt.2023.100574
24. Young I, Reimer D, Greig J, Meldrum R, Turgeon P, Waddell L. Explaining consumer safe food handling through behavior-change theories: a systematic review. Foodborne Pathog Dis. (2017) 14:609–22. doi: 10.1089/fpd.2017.2288
25. Fields VL, Soke GN, Reynolds A, Tian LH, Wiggins L, Maenner M, et al. Pica, autism, and other disabilities. Pediatrics. (2021) 147:e20200462. doi: 10.1542/peds.2020-0462
26. Fekih-Romdhane F, Cheour M. A rare case report of teen-onset pica in a female patient with a clinical high risk for psychosis. Early Interv Psychiatry. (2022) 16:808–11. doi: 10.1111/eip.13214
27. Schnitzler E. The neurology and psychopathology of pica. Curr Neurol Neurosci Rep. (2022) 22:531–6. doi: 10.1007/s11910-022-01218-2
28. Sabatino A, Cuppari L, Stenvinkel P, Lindholm B, Avesani CM. Sarcopenia in chronic kidney disease: what have we learned so far? J Nephrol. (2021) 34:1347–72. doi: 10.1007/s40620-020-00840-y
29. Kalantar-Zadeh K, Tortorici AR, Chen JL, Kamgar M, Lau WL, Moradi H, et al. Dietary restrictions in dialysis patients: is there anything left to eat? Semin Dial. (2015) 28:159–68. doi: 10.1111/sdi.12348
30. Griva K, Lai AY, Lim HA, Yu Z, Foo MW, Newman SP, et al. Non-adherence in patients on peritoneal dialysis: a systematic review. PLoS ONE. (2014) 9:e89001. doi: 10.1371/journal.pone.0089001
31. Volaklis K, Mamadjanov T, Meisinger C. Sedentary behavior and kidney function in adults: a narrative review. Wien Klin Wochenschr. (2021) 133:144–52. doi: 10.1007/s00508-020-01673-2
32. Jhamb M, McNulty ML, Ingalsbe G, Childers JW, Schell J, Conroy MB, et al. Knowledge, barriers and facilitators of exercise in dialysis patients: a qualitative study of patients, staff and nephrologists. BMC Nephrol. (2016) 17:192. doi: 10.1186/s12882-016-0399-z
Keywords: pica, CKD, dialysis, willingness to change, diet, lifestyle, exercise
Citation: Orozco-González CN, Marquez-Herrera RM, Martín-del-Campo F, Cortés-Sanabria L, Villasana-Ballesteros M and Cueto-Manzano AM (2024) Pica is associated with lower willingness to change negative habits of diet and exercise, inadequate lifestyle, and less healthful food consumption in dialysis. Front. Nutr. 11:1402625. doi: 10.3389/fnut.2024.1402625
Received: 18 March 2024; Accepted: 28 August 2024;
Published: 11 September 2024.
Edited by:
Claudia Saunders, Federal University of Rio de Janeiro, BrazilReviewed by:
Kona Chowdhury, Gonoshathaya Samaj Vittik Medical College, BangladeshCopyright © 2024 Orozco-González, Marquez-Herrera, Martín-del-Campo, Cortés-Sanabria, Villasana-Ballesteros and Cueto-Manzano. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alfonso M. Cueto-Manzano, YV9jdWV0b19tYW56YW5vQGhvdG1haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.