 Haoran Zhou
Haoran Zhou Tianshu Li1†
Tianshu Li1† Dongdong Zheng
Dongdong Zheng
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr. , 29 February 2024
Sec. Nutritional Epidemiology
Volume 11 - 2024 | https://doi.org/10.3389/fnut.2024.1365580
This article is part of the Research Topic Nutritional Status Assessment and its Links with Chronic Disease Prognosis and Surgical Outcomes View all 18 articles
Background: There is growing evidence that antioxidant-rich diets may prevent hyperlipidemia. However, the relationship between the Composite Dietary Antioxidant Index (CDAI) and hyperlipidemia is unclear. The CDAI is a composite score reflecting the antioxidant content of an individual’s diet, and this study aimed to investigate the relationship between CDAI and hyperlipidemia.
Methods: The study used the 2003–2018 National Health and Nutrition Examination Survey (NHANES) database for cross-sectional analyses and included 27,626 participants aged 20 years and older. The CDAI, which includes vitamins A, C, and E, zinc, selenium, and carotenoids, was calculated based on dietary intake reported in a 24-h recall interview. Hyperlipidemia was defined by the National Cholesterol Education Program (NCEP). Covariates included age, sex, race, education, marriage, household poverty-to-income ratio (PIR), glomerular filtration rate (eGFR), body mass index (BMI), energy, carbohydrates, total fat, cholesterol, smoking, alcohol consumption, hypertension, diabetes mellitus, coronary heart disease, and lipid-lowering medications. The association between CDAI and hyperlipidemia was explored through multiple logistic regression analyses and smoothed curve fitting. We also performed subgroup analyses and interaction tests to verify the relationship’s stability.
Results: After adjusting for potential confounders, CDAI was negatively associated with the risk of developing hyperlipidemia (OR 0.98, 95% CI 0.96–0.99, p < 0.01). The results of weighted regression models stratified by quartiles of CDAI (−8.664 ≤ Q1 ≤ −2.209, −2.209 < Q2 ≤ −0.002, −0.002 < Q3 ≤ 2.774, 2.774 < Q4 ≤ 124.284), fully adjusted for confounding variables, indicated that compared with the bottom quartile (Q1) of the CDAI, Q2, Q3, and Q4 of participants had a lower advantage ratio (Q2: OR 0.91, 95% CI 0.78–1.06, p < 0.21; Q3: OR 0.85, 95% CI 0.73–1.00, p < 0.05; and Q4: OR 0.77, 95% CI 0.64–0.94, p < 0.01), which was confirmed by a test for trend (p < 0.05). Smoothed curve fit analysis showed linearity (p for non-linear = 0.0912). In summary, there is a linear negative relationship between CDAI and the risk of developing hyperlipidemia. Subgroup analyses by age, sex, ethnicity, education level, marriage, tobacco status, alcoholic drinking, body mass index (BMI), hypertension, and diabetes did not indicate strong interactions.
Conclusion: In this large cross-sectional study, there was a linear negative association between CDAI and hyperlipidemia among US adults. Therefore increase antioxidant rich foods in your life as a prevention of hyperlipidemia.
Hyperlipidemia is a metabolic disorder in which there is an abnormally high level of lipids in the blood and is clinically classified as hypercholesterolemia, hypertriglyceridemia, mixed hyperlipidemia, and low HDL cholesterolemia, depending on the type of elevated lipoprotein (1, 2). Hyperlipidemia has been a widespread concern in Europe, America, and other developing countries. According to epidemiologic surveys, it was found that in the United States, about 12% of adults ≥20 years of age had total cholesterol levels higher than 240 mg/dL, and about 17% had high-density lipoprotein (HDL) cholesterol levels <40 mg/dL between 2015 and 2018 (3). Hyperlipidemia is one of the risk factors for several vascular diseases (4). Thus, it increases the risk of disease in the elderly (5). The prevalence of hyperlipidemia continues to grow as the world faces an increasingly aging population (6). Hyperlipidemia is associated with a variety of diseases such as stroke, diabetes, coronary heart disease, and other chronic diseases (7), severely reducing the quality of life, shortening the lifespan of the patients, and causing a substantial economic burden. Based on this fact, finding effective treatments to address this problem is essential.
Current research has identified the key to oxidative stress as reactive oxygen species (ROS), and the overproduction of ROS has been linked to pathological diseases such as obesity, insulin resistance, hyperglycemia, chronic inflammation and dyslipidemia (8–10). During physiological circumstances, ROS are readily modulated by counter-oxidants. However, counter-oxidants can be obtained in vivo and in vitro (11). When antioxidant deficiencies and malnutrition result in the body being more susceptible to oxidative stress, thus improving the risk of an adverse reaction (12). There is evidence of an association between hyperlipidemia and oxidative stress (13). Vitamin A (VA) as a dietary antioxidant, Wang et al. (14). In an intervention experiment in diabetic adipose rats, administration of VA for 8 weeks was able to improve fat metabolism to reduce hyperlipidemia. Vitamin E (VE) derives its antioxidant activity mainly from α-tocopherol and γ-tocopherol. In a study in children and adolescents, administration of micronutrients VE and VA was shown to reduce blood lipids through antioxidant properties (15). Administration of zinc alone in type 2 diabetic rats improved lipid levels (16), in addition to dietary zinc reducing oxidative stress (17). It is apparent that numerous studies have confirmed the effect of single antioxidants on hyperlipidemia, but the relationship between combined dietary antioxidant intake and hyperlipidemia still needs to be explored.
In recent years, the role of antioxidants has become prominent in global dietary patterns, and the impact of total nutritional antioxidant capacity on health has become increasingly common in all sectors (18). Dietary antioxidant supplementation through consuming fruits, vegetables, whole grains, nuts, and legumes has been suggested (19), and the intake of adequate antioxidants may help reduce the burden of oxidative stress (20). CDAI was proposed by Wright et al. (21) as a composite score reflecting antioxidant capacity of one’s diet, which includes vitamins A, C, and E, zinc, selenium, and carotenoids. Previous studies have found that CDAI improves heart failure, hypertension, depression, and atherosclerotic cardiovascular disease and reduces the risk of morbidity (18, 22–24). However, there are no studies on the relationship between CDAI and hyperlipidemia.
In this study, we explored the association between CDAI and hyperlipidemia for the first time using a large-sample cross-sectional design. Based on previous studies, it was hypothesized that there may be a negative association between CDAI and hyperlipidemia, intending to prevent hyperlipidemia and reduce the risk of its onset through diet, with important clinical implications.
The National Health and Nutrition Examination Survey (NHANES) is a United States population census intended to accurately estimate health and nutritional status, applying stratified, multistage, and probability sampling methods to obtain comprehensive data. This survey utilized a database of 80,312 participants from 8 cycles of NHANES in the United States from 2003 to 2018. After excluding participants with age < 20 years (n = 35,522) and missing or incomplete data on hyperlipidemia (n = 1871), CDAI (n = 7,890), and covariates (n = 7,403), we ultimately included 27,626 participants. Figure 1 shows a flow diagram of the entire sample selection process. The National Center for Health Statistics (NCHS) Ethics Review Committee approved the research, and all subjects signed an informed consent form.
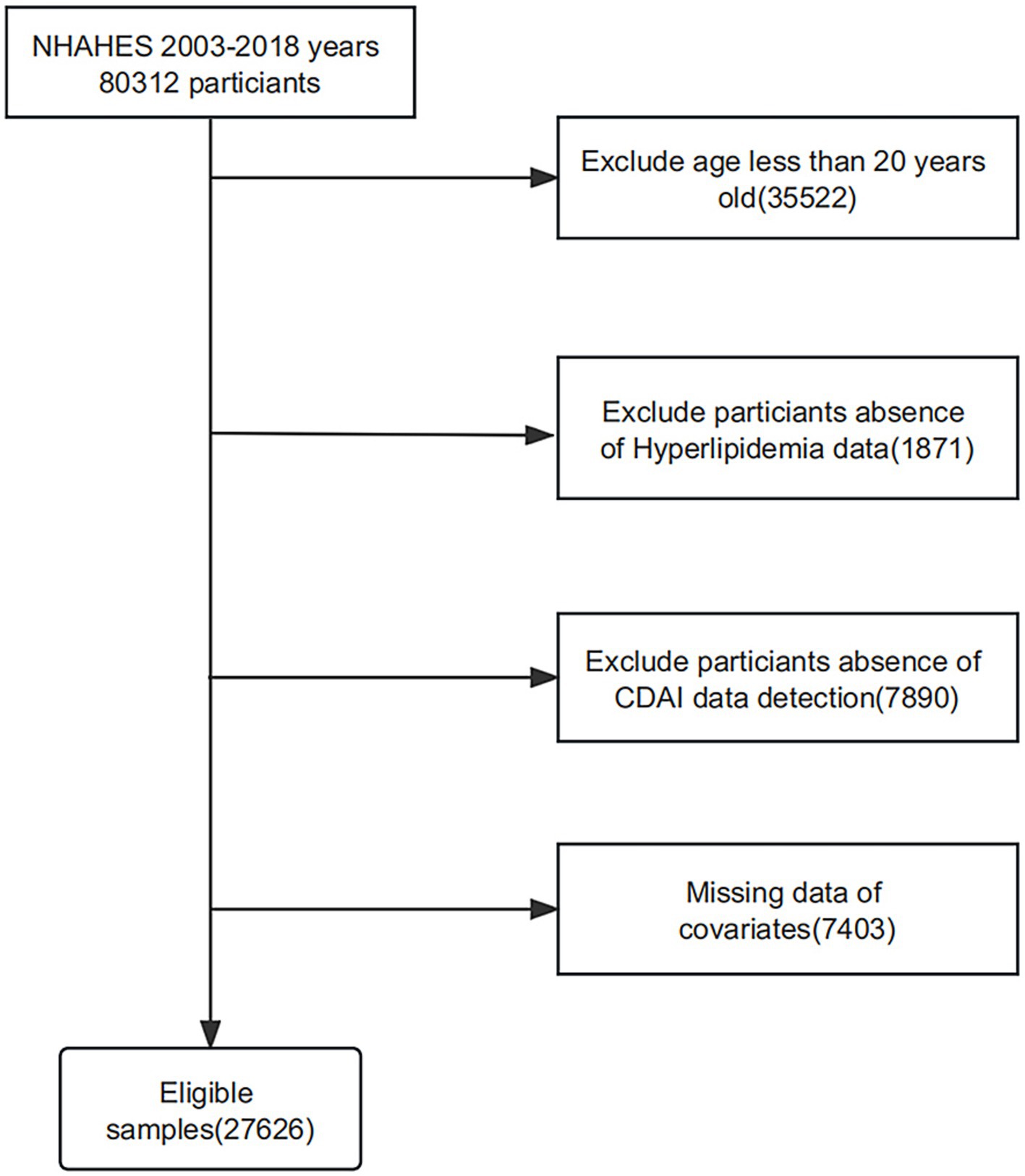
Figure 1. Flowchart depicting participant selection in the study.
During the NHANES survey, a professional statistician conducted two 24-h recall dietary interviews to collect information on the intake of nutritional antioxidants and other food components. The primary recollection interview was performed at the Mobile Screening Center, and the secondary recollection interview was obtained 3–10 days later through a telephone inquiry. Participants were asked to recall the specifics of all diets over 24 h, and dietary supplement intake, including dose, frequency, and duration, was determined (25). The Composite Dietary Antioxidant Index (CDAI) includes six dietary antioxidants: vitamins A, C, and E, zinc, selenium, and carotenoids. This dietary antioxidant access excludes antioxidants in nutritional supplements, medications, or drinking water. The CDAI was calculated by subtracting the mean and dividing by the standard deviation of an individual’s intake, and the results were as follows:
.
Relying on the National Cholesterol Education Program (NCEP) Adult Treatment Panel III (ATP-III), we estimated the Hyperlipidemia status. We defined Hyperlipidemia as (1) triglycerides (TG) ≥ 150 mg/dL (1.7 mmol/L), (2) total cholesterol (TC) ≥ 200 mg/dL (5.18 mmol/L), (3) low-density lipoprotein (LDL-C) ≥ 130 mg/dL (3.37 mmol/L), (4) high-density lipoprotein (HDL-C<), ≤40 mg/dL (1.04 mmol/L) for men or ≤ 50 mg/dL (1.30 mmol/L) for women, and (5) a participant that reported the use of lipid-lowering drugs was at the same time defined as having hyperlipidemia (3, 26–28). Hyperlipidemia was diagnosed if any of these five conditions were met.
Based on previous studies and confounders, we selected the following covariates including age, sex (male/female), race (Mexican American/other Hispanic/non-Hispanic white/non-Hispanic black/other race), educational attainment (less than 9th grade, 9th–11th grade, high school graduation, some college graduation, and college and beyond), marital status (married, widowed, divorced, separated, unmarried, living with a partner), and household poverty-to-income ratio (PIR, <1.3, 1.3–3.5, ≥3.5); income-to-poverty ratios were calculated based on the US Department of Health and Human Services (DHHS) Family Income Poverty Guidelines (29). Smoking was categorized as (1) non-smoking (2) former tobacco (3) current smoking. Alcohol consumption was categorized as (1) no alcohol consumption, (2) previous alcohol consumption, (3) mild alcohol consumption, (4) moderate alcohol consumption, (5) heavy alcohol consumption. Body mass index (BMI) is weight (Kg) divided by the square of height (m). The glomerular filtration rate (eGFR) was calculated based on the serum creatinine equation (30). Energy, carbohydrate, total fat, and cholesterol intake were determined by averaging dietary recall over 2 days; coronary artery disease and lipid-lowering medications were obtained by a questionnaire that recorded whether participants were told by a physician that they had coronary artery disease and were taking lipid-lowering medications. The definition of diabetes was sufficient to satisfy any of the following: (1) self-reported physician diagnosis of diabetes mellitus, (2) current use of glucose-lowering medications or insulin injections, an (3) randomized Blood glucose ≥11.1 mmol/L, (4) Glycated hemoglobin (HbA1c) level ≥ 6.5%, (5) Fasting blood glucose (FPG) level ≥ 7.0 mmol/L, and (6) 2-h OGTT blood glucose level ≥ 11.1 mmol/L. The definition of hypertension can be satisfied with any one of the following: (1) self-reported high blood pressure, (2) patients taking antihypertensive medication, (3) mean systolic blood pressure (SBP) ≥140 mmHg and/or mean diastolic blood pressure (DBP) ≥90 mmHg; detailed measurement procedures for all covariates are available at www.cdc.gov/nchs/nhanes/index.htm.
All data in this study were statistically analyzed using the R language (version 4.3.1) and followed the guidelines established by the Centers for Disease Control and Prevention (CDC). We weighted the data in the data analysis, applying mean ± standard deviation for continuous variables and frequency (percentage) for categorical variables. Differences between categorical variables were analyzed using the chi-square test, while continuous variables conforming to normal distribution were tested with the weighted Student’s t-test; otherwise, they were tested with the Man-Whitney u-test. The correlation between CDAI and hyperlipidemia was studied using multifactor logistic regression modeling. CDAI was transformed into categorical variables by quartiles, and the linear trend test and p-value of the trend were calculated to determine the consistency of the relationship. Three models were constructed for this research: Model 1, a crude model without adjusting for any variables; Model 2, adjusted for sex, age, and race; and Model 3, which continued to change for education, marriage, PIR, eGFR, BMI, energy, carbohydrates, total fat, cholesterol, smoking, alcohol, hypertension, diabetes mellitus, coronary artery disease, and lipid-lowering medications based on Model 2. Smoothed curve fitting was applied to explore further whether there was a linear relationship between CDAI and hyperlipidemia. In addition, to investigate whether there were interactions and stability between subgroups, we performed subgroup-stratified analyses for age, gender, race, education level, marriage, smoking status, alcohol consumption, BMI, hypertension, and diabetes mellitus. A p-value of below 0.05 was recognized as statistically significant.
This research included 27,626 participants, with a mean age of 47.42 ± 0.24 years, of which 51.23% were female and 48.77% were male. Baseline characteristics of participants by CDAI quartiles are shown in Table 1, differences between quartiles were statistically significant (p < 0.05) for age, sex, race, education, marriage, PIR, smoking, alcohol consumption, BMI, eGFR, energy, carbohydrates, total fat, cholesterol, hypertension, diabetes mellitus, coronary artery disease, and use of lipid-lowering drugs. Compared to Q1, Q4 tended to be younger, male, non-Hispanic white, with lower BMI, better economic standard, and higher education status. Non-smoking and mild alcohol consumption had greater levels of CDAI. The higher the CDAI level, the more energy, carbohydrates, total fat, and cholesterol they consume. Hypertension, diabetes mellitus, coronary heart disease, and hyperlipidemia decreased with increasing CDAI.
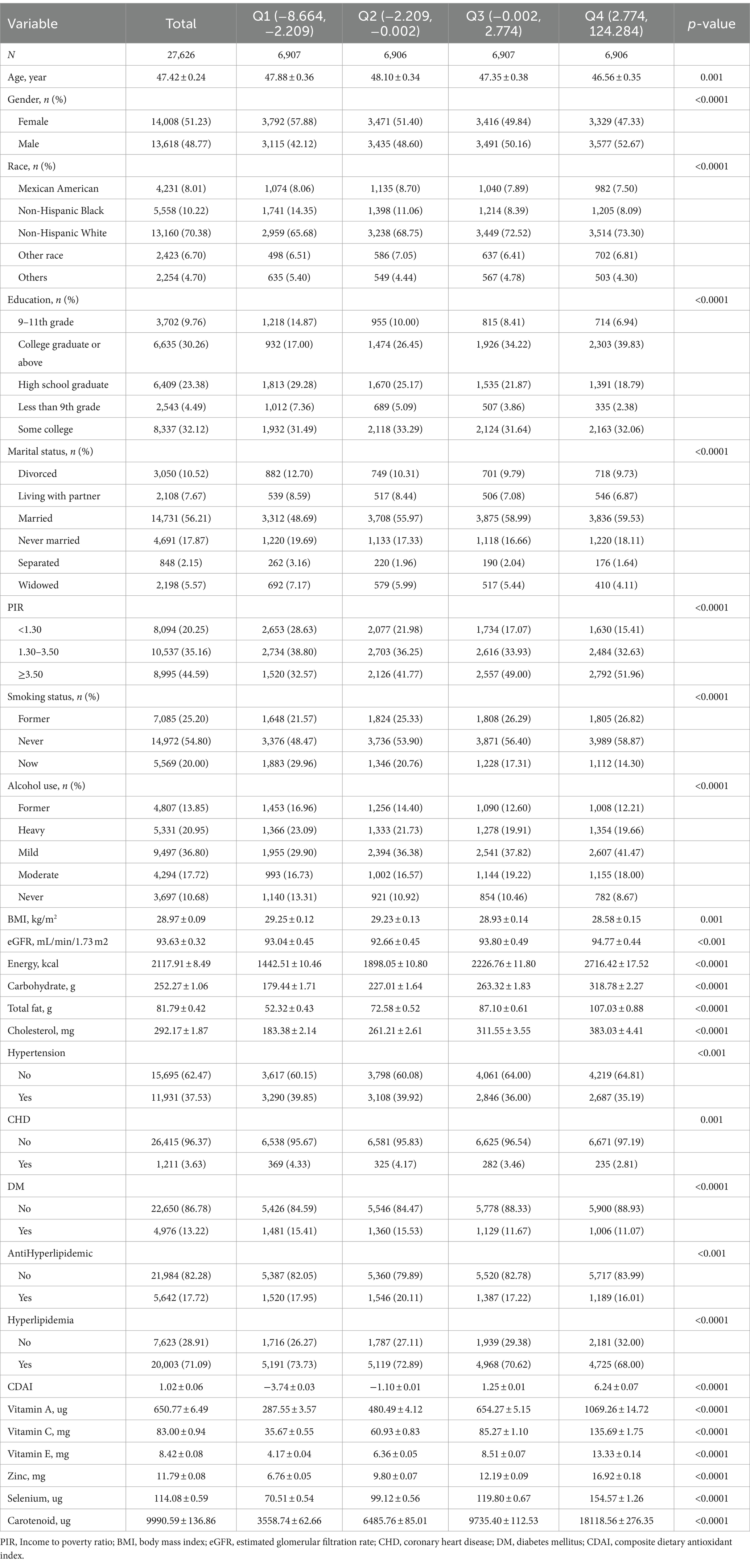
Table 1. The characteristics of participants.
The multivariate logistic regression model, as shown in Table 2, demonstrates the correlation between CDAI and the risk of hyperlipidemia. In model 3, CDAI scores were negatively associated with the risk of developing hyperlipidemia (OR 0.98, 95% CI 0.96–0.99). This negative correlation was more pronounced in participants with a lower predominance ratio of hyperlipidemia than in Q1 according to quartile stratification in Q2 (OR 0.91, 95% CI 0.78–1.06), Q3 (OR 0.85, 95% CI 0.73–1.00), and Q4 (OR 0.77, 95% CI 0.64–0.94) and was also confirmed by a test of trend in each model using Q1 as control this (p < 0.05). We also used smoothed curve fitting to assess the association between the two; as shown in Figure 2, the correlation between CDAI and hyperlipidemia was negative and linear (p for non-linear = 0.0912).
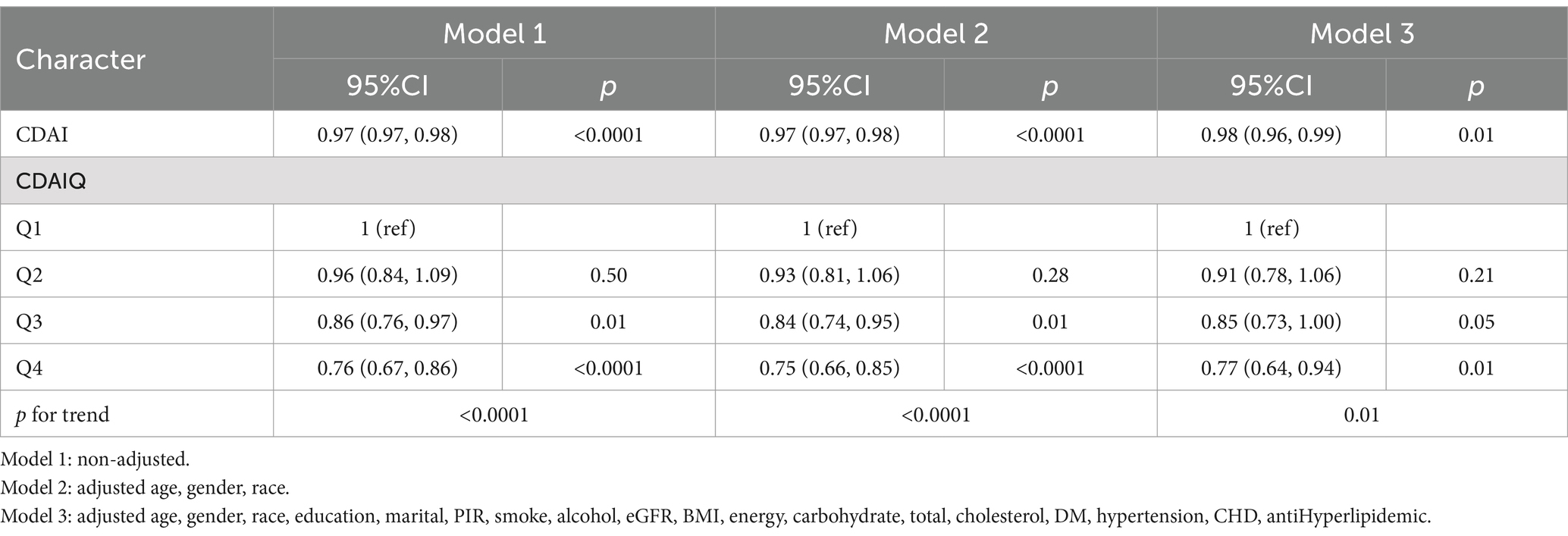
Table 2. The association between CDAI and hyperlipidemia.
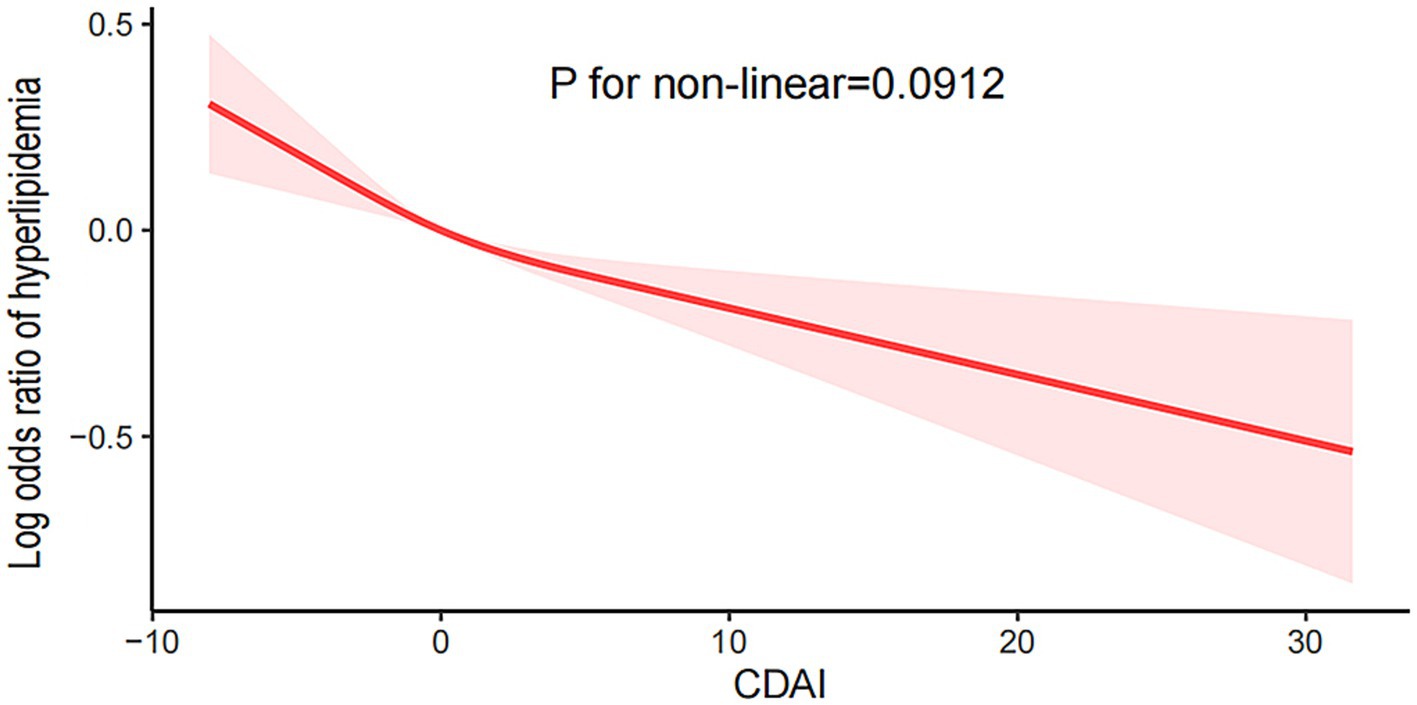
Figure 2. The smooth curve fitting analysis of CDAI and hyperlipidemia.
As shown in Figure 3, we stratified age, gender, race, education level, marriage, smoking status, alcohol consumption, BMI, hypertension, and diabetes to explore the stability of the relationship between CDAI and hyperlipidemia and the presence or absence of interaction. In subgroup analyses, no significant interactions were found between CDAI and these stratified variables (p > 0.05), and the relationship was very stable.
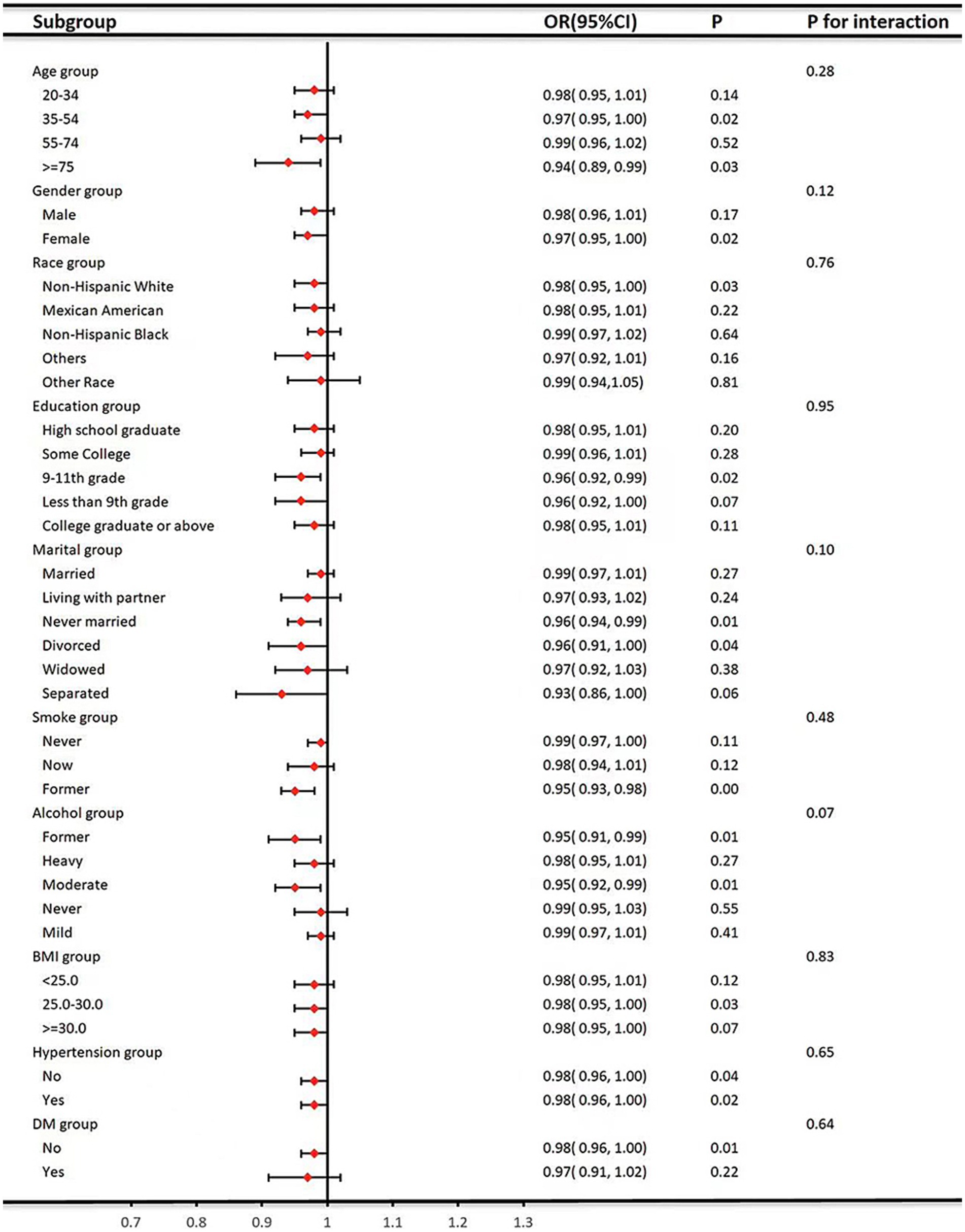
Figure 3. Subgroup analysis for the association between CDAI and hyperlipidemia.
The study analyzed the most representative US population data and, after adjusting for several covariates, found that CDAI was negatively associated with the prevalence of hyperlipidemia in the population, which confirms our hypothesis. These results suggest that appropriate dietary modification and increased antioxidant intake can help prevent and treat hyperlipidemia. Although previous studies have demonstrated the effect of dietary antioxidants such as VA, VE, and zinc on hyperlipidemia, most of them applied a single class of antioxidants for correlation analysis and did not consider them in combination. However, the intake of a single antioxidant is difficult to achieve in the daily diet, and it is more likely that a wide range of foods and a wide range of antioxidants will be consumed. In addition, there is no single antioxidant component in foods that are rich in multiple antioxidants. Therefore, there is a need to investigate the relationship between combined dietary antioxidant intake and hyperlipidemia.
Oxidative stress plays a vital role in hyperlipidemia. Wu et al. (31) found that the substrates of G. frondosa decreased glutathione (GSH) and catalase activity, increased GSH peroxidase activity, inhibited oxidative stress, and increased bile acid synthesis to improve hypercholesterolemia. Feng et al. (32) administered hawthorn fructofuranic acid (HFA) to rats. Found that activation of Nrf2/HO-1 signaling pathway could inhibit oleic acid (OA)-induced oxidative damage in a hepatocellular carcinoma cell line (HepG2), which in turn reduced oxidative stress damage in rats, effectively reduced triglyceride and cholesterol levels, attenuated hepatic steatosis and intervened in hyperlipidemia. Pretreatment with M. charantia polysaccharides for 25 days in a rat model was found to inhibit oxidative stress via nuclear factor κB (NF-kB), lowering lipid indices, and consequently ameliorating hyperlipidemia (33). Ji et al. (34) further found that consumption of propolis by rabbits with hypercholesterolemia lowered the lipid levels and enhanced antioxidant activity by a mechanism which may be the inhibition of the TLR4-mediated NF- κB signaling pathway. Puerarin was found to reduce ROS production and increase antioxidant capacity by modulating the phosphorylated Jun N-terminal kinase (JNK)/phosphorylated c-Jun protein/cholesterol 7a-hydroxylase (CYP7A1) pathway in mouse liver, which in turn inhibited hyperlipidemia (35). Fan et al. (36) used baicalein to intervene in hyperlipidemic rats and showed results of enhanced activation of PI3K/AKT and activation of Nrf2, thereby increasing the expression of HO-1 and NQO1, inhibiting oxidative stress and preventing hyperlipidemia. Honey pretreatment given to rats before feeding them a high-fat diet was found to be able to attenuate oxidative stress and exert anti-hyperlipidemia effects more significantly by inhibiting 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase (37). Antunes et al. (38) experimented with different combinations of phenolic compounds from purple grape bark, both in vitro and in vivo, and all of the results showed an antioxidant effect, thereby reducing hypercholesterolemia. Administration of p-coumaric acid (p-CA) in mouse experiments revealed an increase in the expression of Nrf2, HO-1, glutathione peroxidase (Gpx), and superoxide dismutase (SOD-1), which in turn exerted an antioxidant and potentially therapeutic effect in the treatment of hyperlipidemia (39). In conclusion, inhibition of oxidative stress, which can treat hyperlipidemia, is the same as the conclusions of cross-sectional studies on the relationship between CDAI and hyperlipidemia.
This study also found that the prevalence of hypertension, diabetes mellitus, and coronary heart disease decreased progressively with increasing CDAI. Previous analyses of the NHANES database found that the prevalence of hypertension, coronary heart disease, and diabetes mellitus were negatively correlated with CDAI (18, 23, 40), which is consistent with our findings. Control variables such as energy, carbohydrates, total fat, and cholesterol, which may affect the results of the study, were added to the previous ones. In addition, instead of using the traditional Dietary Antioxidant Quality Score (DAQS) for assessing dietary antioxidant indices in this study, the more accurate CDAI was used for correlation analyses because of its applied advantages and validity proved in epidemiological studies.
Diet is essential in treating hyperlipidemia by containing antioxidants that reduce oxidative stress damage and promote health (41). Antioxidants are biologically active compounds that neutralize free radicals and reduce oxidative damage (42). Although there are no studies on the relationship between CDAI and hyperlipidemia, the use of dietary antioxidant properties to intervene in hyperlipidemia has become a hot research topic. The vitamins (A, D, and E) and carotenoids in CDAI are fat-soluble and vitamin C is water-soluble, which is relevant for absorption, transport and action. Feeding a VA-rich (52 mg/kg) diet for 20 weeks in hypercholesterolemic obese rats increased plasma lecithin cholesterol acyltransferase activity and expression of ATP-binding cassette transporter protein A1, which, in turn, led to normalization of plasma HDL-C levels (43). Vitamin C (VC) is an essential nutrient for humans and the effect of administration is highly dose dependent (44), maximizing neutrophil concentration, reducing ROS production and inhibiting LDL-C oxidation through dietary intake (45, 46). Kumar et al. (47) administered VC (0.5 g/kg) once daily for 30 days in a male rat model of hyperlipidemia. It showed a decrease in triglycerides, cholesterol, ROS, malondialdehyde (MDA), and reduced GSH, the mechanism of which may be to prevent hyperlipidemia by inhibiting oxidative stress and maintaining redox balance. In a randomized double-blind crossover study, VC (1,000 mg) in combination with dietary nitrates given to untreated hypercholesterolemic subjects for 4 weeks was found to reduce oxidized low-density lipoprotein (oxLDL), triglycerides and inhibit oxidative stress by increasing the total plasma NO metabolites (48). Selenium was able to maintain the anti-oxidative stress function of glutathione peroxidation and selenoprotein P (49). Guo et al. (50) fed selenium nanoparticles (SeNPs) 50 μg/d in apolipoprotein E-deficient (ApoE) mice, and showed that it was able to alleviate hyperlipidemia in ApoE mice by regulating cholesterol metabolism through antioxidant selenoenzymes/selenoproteins and reducing oxidative stress, and additionally metabolomics selenium-enriched kiwifruit was also found to be able to treat hyperlipidemia (51). Carotenoids (Crt) act as antioxidants in lipid-rich environments (52), mainly through (i) electron transfer between free radicals (R-) and Crt, leading to the formation of Crt radical cation (Crt-+) or Crt radical anion (Crt-); and (ii) radical adducts (R-), leading to the formation of Crt radical cation (Crt-+) or Crt radical anion (Crt-). (-); (ii) radical adduct formation (RCrt-); and (iii) hydrogen atom transfer leading to neutral Crt radicals (Crt-) three pathways to scavenge free radicals, which can also effectively scavenge ROS and play an antioxidant role (53). Lycopene, a water-soluble carotenoid, intervenes in hyperlipidemia by down-regulating oxidative stress induced by the preprotein convertase Bacillus subtilis protease/kexin type 9 (PCSK-9) targeting lipopolysaccharide (LPS) (54). This study concluded that the difference between single serum antioxidant and hyperlipidemia was statistically significant, and the more intake, the greater the CDAI and the lower the prevalence of hyperlipidemia, which is in line with the results of the above study.
The following four limitations exist in this research. First, the study was a cross-sectional analysis, and we could not determine a causal relationship between CDAI and hyperlipidemia. Second, since the population studied was Americans, special people such as minors were omitted. Third, some unknown covariates may affect the relationship between CDAI and the risk of hyperlipidemia. Fourth, CDAI data are self-reported and will be subject to recall bias.
There is a linear negative association between CDAI and the risk of hyperlipidemia. Therefore, intake of foods rich in CDAI components, which are mainly rich in VC and VE, may reduce the risk of hyperlipidemia. In the future, prospective studies and basic experiments are needed to further explore the mechanism of action, tap into the diet of each component of CDAI to exclude the effect of individual variability, and additionally explore the relationship between more antioxidants in the diet and hyperlipidemia to guide the diet. Living with balanced nutrition, reasonable diet, strengthening physical exercise, improving body metabolism, strengthening hyperlipidemia prevention and reducing the occurrence of the disease.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by The Research Ethics Review Board at the National Center for Health Statistics (NCHS). The patients/participants provided their written informed consent to participate in this study. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
HZ: Data curation, Formal analysis, Methodology, Software, Validation, Writing – original draft, Writing – review & editing. TL: Conceptualization, Data curation, Formal analysis, Methodology, Writing – review & editing. JL: Conceptualization, Methodology, Visualization, Writing – review & editing. DZ: Formal analysis, Software, Visualization, Writing – review & editing. JY: Conceptualization, Methodology, Validation, Visualization, Writing – review & editing. XZ: Data curation, Supervision, Visualization, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work was supported by Natural Science Foundation of Shandong Province, Youth Program (no. ZR2023QH119) and Shandong Traditional Chinese Medicine Science and Technology Development Program (no. Q-2022051).
The author thanks the staff and the participants of the NHANES study for their valuable contributions.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Hill, MF, and Bordoni, B. Hyperlipidemia In: StatPearls. Treasure Island, FL: StatPearls Publishing (2022)
3. Han, Y, Jiang, X, Qin, Y, Zhao, Y, Zhang, G, and Liu, C. A cross-sectional study exploring the relationship between the dietary inflammatory index and hyperlipidemia based on the National Health and Nutrition Examination Survey (2005-2018). Lipids Health Dis. (2023) 22:140. doi: 10.1186/s12944-023-01908-x
4. Chen, YQ, Zhao, SP, and Zhao, YH. Efficacy and tolerability of coenzyme A vs pantethine for the treatment of patients with hyperlipidemia: A randomized, double-blind, multicenter study. J Clin Lipidol. (2015) 9:692–7. doi: 10.1016/j.jacl.2015.07.003
5. Mozaffarian, D, Benjamin, EJ, Go, AS, Arnett, DK, Blaha, MJ, Cushman, M, et al. Heart disease and stroke statistics–2015 update: A report from the American Heart Association. Circulation. (2015) 131:e29–e322. doi: 10.1161/cir.0000000000000152
6. Yusuf, S, Hawken, S, Ounpuu, S, Dans, T, Avezum, A, Lanas, F, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the inter heart study): case-control study. Lancet. (2004) 364:937–52. doi: 10.1016/s0140-6736(04)17018-9
7. Yan, S, Luo, W, Lei, L, Zhang, Q, and Xiu, J. Association between serum Klotho concentration and hyperlipidemia in adults: a cross-sectional study from NHANES 2007-2016. Front Endocrinol (Lausanne). (2023) 14:1280873. doi: 10.3389/fendo.2023.1280873
8. Padgett, LE, Broniowska, KA, Hansen, PA, Corbett, JA, and Tse, HM. The role of reactive oxygen species and proinflammatory cytokines in type 1 diabetes pathogenesis. Ann N Y Acad Sci. (2013) 1281:16–35. doi: 10.1111/j.1749-6632.2012.06826.x
9. Forrester, SJ, Kikuchi, DS, Hernandes, MS, Xu, Q, and Griendling, KK. Reactive oxygen species in metabolic and inflammatory signaling. Circ Res. (2018) 122:877–902. doi: 10.1161/CIRCRESAHA.117.311401
10.Čolak, E, and Pap, D. The role of oxidative stress in the development of obesity and obesity-related metabolic disorders. J Med Biochem (2021);40:1–9. doi: 10.5937/jomb0-24652
11. Wu, D, Wang, H, Wang, W, Qing, C, Zhang, W, Gao, X, et al. Association between composite dietary antioxidant index and handgrip strength in American adults: Data from National Health and Nutrition Examination Survey (NHANES, 2011-2014). Front Nutr. (2023) 10:1147869. doi: 10.3389/fnut.2023.1147869
12. Liu, Z, Ren, Z, Zhang, J, Chuang, CC, Kandaswamy, E, Zhou, T, et al. Role of ROS and nutritional antioxidants in human diseases. Front Physiol. (2018) 9:477. doi: 10.3389/fphys.2018.00477
13. Masenga, SK, Kabwe, LS, Chakulya, M, and Kirabo, A. Mechanisms of oxidative stress in metabolic syndrome. Int J Mol Sci. (2023) 24:7898. doi: 10.3390/ijms24097898
14. Wang, T, Tang, X, Hu, X, Wang, J, and Chen, G. Reduction in the dietary VA status prevents type 2 diabetes and obesity in Zucker diabetic fatty rats. Biomol Ther. (2022) 12:528. doi: 10.3390/biom12040528
15. Chakrabarti, A, Eiden, M, Morin-Rivron, D, Christinat, N, Monteiro, JP, Kaput, J, et al. Impact of multi-micronutrient supplementation on lipidemia of children and adolescents. Clin Nutr. (2020) 39:2211–9. doi: 10.1016/j.clnu.2019.09.010
16. Sadri, H, Larki, NN, and Kolahian, S. Hypoglycemic and hypolipidemic effects of leucine, zinc, and chromium, alone and in combination, in rats with type 2 diabetes. Biol Trace Elem Res. (2017) 180:246–54. doi: 10.1007/s12011-017-1014-2
17. Barman, S, and Srinivasan, K. Attenuation of oxidative stress and cardioprotective effects of zinc supplementation in experimental diabetic rats. Br J Nutr. (2017) 117:335–50. doi: 10.1017/S0007114517000174
18. Zhang, J, Lu, X, Wu, R, Ni, H, Xu, L, Wu, W, et al. Associations between composite dietary antioxidant index and estimated 10-year atherosclerotic cardiovascular disease risk among U.S. adults. Front Nutr. (2023) 10:1214875. doi: 10.3389/fnut.2023.1214875
19. Aune, D. Plant foods, antioxidant biomarkers, and the risk of cardiovascular disease, cancer, and mortality: a review of the evidence. Adv Nutr. (2019) 10:S404–21. doi: 10.1093/advances/nmz042
20. Mirmiran, P, Hosseini-Esfahani, F, Esfandiar, Z, Hosseinpour-Niazi, S, and Azizi, F. Associations between dietary antioxidant intakes and cardiovascular disease. Sci Rep. (2022) 12:1504. doi: 10.1038/s41598-022-05632-x
21. Wright, ME, Mayne, ST, Stolzenberg-Solomon, RZ, Li, Z, Pietinen, P, Taylor, PR, et al. Development of a comprehensive dietary antioxidant index and application to lung cancer risk in a cohort of male smokers. Am J Epidemiol. (2004) 160:68–76. doi: 10.1093/aje/kwh173
22. Ma, Y, Liu, J, Sun, J, Cui, Y, Wu, P, Wei, F, et al. Composite dietary antioxidant index and the risk of heart failure: A cross-sectional study from NHANES. Clin Cardiol. (2023) 46:1538–43. doi: 10.1002/clc.24144
23. Wu, M, Si, J, Liu, Y, Kang, L, and Xu, B. Association between composite dietary antioxidant index and hypertension: insights from NHANES. Clin Exp Hypertens. (2023) 45:2233712. doi: 10.1080/10641963.2023.2233712
24. Zhao, L, Sun, Y, Cao, R, Wu, X, Huang, T, and Peng, W. Non-linear association between composite dietary antioxidant index and depression. Front Public Health. (2022) 10:988727. doi: 10.3389/fpubh.2022.988727
25. Kantor, ED, Rehm, CD, du, M, White, E, and Giovannucci, EL. Trends in dietary supplement use among US adults from 1999-2012. JAMA. (2016) 316:1464–74. doi: 10.1001/jama.2016.14403
26. Chen, X, Zhou, M, Yan, H, Chen, J, Wang, Y, and Mo, X. Association of serum total 25-hydroxy-vitamin D concentration and risk of all-cause, cardiovascular and malignancies-specific mortality in patients with hyperlipidemia in the United States. Front Nutr. (2022) 9:971720. doi: 10.3389/fnut.2022.971720
27. Zhang, Y, Liu, W, Zhang, W, Cheng, R, Tan, A, Shen, S, et al. Association between blood lead levels and hyperlipidemiais: Results from the NHANES (1999-2018). Front Public Health. (2022) 10:981749. doi: 10.3389/fpubh.2022.981749
28. Mahemuti, N, Jing, X, Zhang, N, Liu, C, Li, C, Cui, Z, et al. Association between systemic immunity-inflammation index and hyperlipidemia: a population-based study from the NHANES (2015-2020). Nutrients. (2023) 15:1177. doi: 10.3390/nu15051177
29. Abdalla, SM, Yu, S, and Galea, S. Trends in cardiovascular disease prevalence by income level in the United States. JAMA Netw Open. (2020) 3:e2018150. doi: 10.1001/jamanetworkopen.2020.18150
30. Levey, AS, Stevens, LA, Schmid, CH, Zhang, Y(L), Castro, AF III, Feldman, HI, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. (2009) 150:604–12. doi: 10.7326/0003-4819-150-9-200905050-00006
31. Wu, WT, Hsu, TH, Chen, WL, Yang, CK, and Lo, HC. Polysaccharides of Grifola frondosa ameliorate oxidative stress and hypercholesterolaemia in hamsters fed a high-fat, high-cholesterol diet. J Pharm Pharmacol. (2022) 74:1296–306. doi: 10.1093/jpp/rgac031
32. Feng, Y, Gao, S, Zhu, T, Sun, G, Zhang, P, Huang, Y, et al. Hawthorn fruit acid consumption attenuates hyperlipidemia-associated oxidative damage in rats. Front Nutr. (2022) 9:936229. doi: 10.3389/fnut.2022.936229
33. Raish, M. Momordica charantia polysaccharides ameliorate oxidative stress, hyperlipidemia, inflammation, and apoptosis during myocardial infarction by inhibiting the NF-κB signaling pathway. Int J Biol Macromol. (2017) 97:544–51. doi: 10.1016/j.ijbiomac.2017.01.074
34. Ji, C, Pan, Y, Xu, S, Yu, C, Ji, J, Chen, M, et al. Propolis ameliorates restenosis in hypercholesterolemia rabbits with carotid balloon injury by inhibiting lipid accumulation, oxidative stress, and TLR4/NF-κB pathway. J Food Biochem. (2021) 45:e13577. doi: 10.1111/jfbc.13577
35. Ma, JQ, Ding, J, Zhao, H, and Liu, CM. Puerarin attenuates carbon tetrachloride-induced liver oxidative stress and hyperlipidaemia in mouse by JNK/c-Jun/CYP7A1 pathway. Basic Clin Pharmacol Toxicol. (2014) 115:389–95. doi: 10.1111/bcpt.12245
36. Fan, H, Ma, X, Lin, P, Kang, Q, Zhao, Z, Wang, L, et al. Scutellarin prevents nonalcoholic fatty liver disease (NAFLD) and hyperlipidemia via PI3K/AKT-dependent activation of nuclear factor (erythroid-derived 2)-like 2 (Nrf2) in rats. Med Sci Monit. (2017) 23:5599–612. doi: 10.12659/msm.907530
37. Erejuwa, OO, Akpan, JL, Uwaezuoke, NJI, Nwobodo, NN, Ezeokpo, BC, Erhiano, E, et al. Effects of honey on postprandial hyperlipidemia and oxidative stress in Wistar rats: role of HMG-CoA reductase inhibition and antioxidant effect. Niger J Physiol Sci. (2018) 33:129–38.
38. Antunes, KA, Monteiro-Alfredo, T, Cunha, JSM, Espindola, PPT, Oliveira, AS, Ramalho de Oliveira, CF, et al. Spondias purpurea L. bark extract protects against oxidative stress and reduces hypercholesterolemia in mice fed high-fat diet. Oxidative Med Cell Longev. (2022) 2022:1–13. doi: 10.1155/2022/3046483
39. Shen, Y, Song, X, Li, L, Sun, J, Jaiswal, Y, Huang, J, et al. Protective effects of p-coumaric acid against oxidant and hyperlipidemia-an in vitro and in vivo evaluation. Biomed Pharmacother. (2019) 111:579–87. doi: 10.1016/j.biopha.2018.12.074
40. Chen, X, Lu, H, Chen, Y, Sang, H, Tang, Y, and Zhao, Y. Composite dietary antioxidant index was negatively associated with the prevalence of diabetes independent of cardiovascular diseases. Diabetol Metab Syndr. (2023) 15:183. doi: 10.1186/s13098-023-01150-6
41. Wang, H, and Chen, Y. Relationship between composite dietary antioxidant index and aging. Healthcare (Basel). (2023) 11:2722. doi: 10.3390/healthcare11202722
42. Aleksandrova, K, Koelman, L, and Rodrigues, CE. Dietary patterns and biomarkers of oxidative stress and inflammation: A systematic review of observational and intervention studies. Redox Biol. (2021) 42:101869. doi: 10.1016/j.redox.2021.101869
43. Prashanth, A, Jeyakumar, SM, Giridharan, NV, and Vajreswari, A. Vitamin A-enriched diet modulates reverse cholesterol transport in hypercholesterolemic obese rats of the WNIN/Ob strain. J Atheroscler Thromb. (2014) 21:1197–207. doi: 10.5551/jat.22186
44. Zeng, Q, Zhao, L, Meng, C, Zhao, X, Liu, Y, Shi, R, et al. Prophylactic and therapeutic effects of different doses of vitamin C on high-fat-diet-induced non-alcoholic fatty liver disease in mice. Biomed Pharmacother. (2020) 131:110792. doi: 10.1016/j.biopha.2020.110792
45. Moser, MA, and Chun, OK. Vitamin C and heart health: a review based on findings from epidemiologic studies. Int J Mol Sci. (2016) 17:1328. doi: 10.3390/ijms17081328
46. Institute of Medicine (US). Panel on Dietary Antioxidants and Related Compounds. Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium, and Carotenoids. Washington, DC: National Academies Press (2000).
47. Kumar, R, and Rizvi, SI. Vitamin C improves inflammatory-related redox status in hyperlipidemic rats. Indian J Clin Biochem. (2023) 38:512–8. doi: 10.1007/s12291-022-01070-8
48. Basaqr, R, Skleres, M, Jayswal, R, and Thomas, DT. The effect of dietary nitrate and vitamin C on endothelial function, oxidative stress and blood lipids in untreated hypercholesterolemic subjects: A randomized double-blind crossover study. Clin Nutr. (2021) 40:1851–60. doi: 10.1016/j.clnu.2020.10.012
49. Xia, Y, Hill, KE, Li, P, Xu, J, Zhou, D, Motley, AK, et al. Optimization of selenoprotein P and other plasma selenium biomarkers for the assessment of the selenium nutritional requirement: a placebo-controlled, double-blind study of selenomethionine supplementation in selenium-deficient Chinese subjects. Am J Clin Nutr. (2010) 92:525–31. doi: 10.3945/ajcn.2010.29642
50. Guo, L, Xiao, J, Liu, H, and Liu, H. Selenium nanoparticles alleviate hyperlipidemia and vascular injury in ApoE-deficient mice by regulating cholesterol metabolism and reducing oxidative stress. Metallomics. (2020) 12:204–17. doi: 10.1039/c9mt00215d
51. He, K, Gao, Q, Su, J, Shang, H, Meng, X, Jiang, S, et al. Gut microbiome and metabolomics study of selenium-enriched kiwifruit regulating hyperlipidemia in mice induced by a high-fat diet. J Agric Food Chem. (2023) 71:20386–401. doi: 10.1021/acs.jafc.3c00108
52. Yabuzaki, J. Carotenoids database: structures, chemical fingerprints and distribution among organisms. Database. (2017) 2017:bax0004. doi: 10.1093/database/bax0004
53. Fiedor, J, and Burda, K. Potential role of carotenoids as antioxidants in human health and disease. Nutrients. (2014) 6:466–88. doi: 10.3390/nu6020466
Keywords: CDAI, hyperlipidemia, relationship, a cross-sectional study, NHANES
Citation: Zhou H, Li T, Li J, Zheng D, Yang J and Zhuang X (2024) Linear association of compound dietary antioxidant index with hyperlipidemia: a cross-sectional study. Front. Nutr. 11:1365580. doi: 10.3389/fnut.2024.1365580
Edited by:
Wei-Cai Zeng, Sichuan University, ChinaReviewed by:
Karine C. M. Sena-Evangelista, Federal University of Rio Grande do Norte, BrazilCopyright © 2024 Zhou, Li, Li, Zheng, Yang and Zhuang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jie Yang, c3VtdXpoZXlhbmdqaWVAMTYzLmNvbQ==; Xin Zhuang, emh1YW5neGluMTk3MkAxMjYuY29t
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.