 Masahiko Okubo1
Masahiko Okubo1 Motoyoshi Morishita2Tomoko Odani3Hideo Sakaguchi4Takeshi Kikutani5
Motoyoshi Morishita2Tomoko Odani3Hideo Sakaguchi4Takeshi Kikutani5 Shoichiro Kokabu6*†
Shoichiro Kokabu6*†- 1Department of Dentistry and Oral Surgery, Ongata Hospital, Hachioji, Tokyo, Japan
- 2Department of Physical Therapy, Faculty of Rehabilitation, Reiwa Health Sciences University, Fukuoka, Japan
- 3Department of Dentistry, Kawaguchi Cupola Rehabilitation Hospital, Kawaguchi, Saitama, Japan
- 4Department of Dentistry, Ryohoku Hospital, Hachioji, Tokyo, Japan
- 5Division of Clinical Oral Rehabilitation, Nippon Dental University Graduate School of Life Dentistry, Iidabashi, Tokyo, Japan
- 6Division of Molecular Signaling and Biochemistry, Kyushu Dental University, Kitakyushu, Japan
The world’s population is aging. Pneumonia is the leading cause of death among the older adults, with aspiration pneumonia being particularly common. Aspiration pneumonia is caused by a decline in swallowing function. Causes can include age-related sarcopenia of swallowing muscles, cognitive decline, cerebrovascular and other diseases or even changes in individual taste preference. Currently, the main treatment approach for dysphagia is resistance training of swallowing-related muscles. This approach has not been effective and establishment of novel methods are required. In this review, we introduce and discuss the relationship between taste, taste preference, carbonation and swallowing function. Taste and preference improve swallowing function. Recently, it has been shown that a carbonated beverage that combines the functionality of a thickening agent, the appeal of taste, and the stimulation of carbonation improves swallowing function. This may be very useful in the recovery of swallowing function. It is important to note that deliciousness is based not only on taste and preference, but also on visual information such as food form. Umami taste receptors are expressed not only in taste buds but also in skeletal muscle and small intestine. These receptors may be involved in homeostasis of the amino acid metabolic network, i.e., the process of amino acid ingestion, intestine absorption, and storage in skeletal muscle. Proper stimulation of umami receptors in organs other than taste buds may help maintain nutritional status and muscle mass. Umami receptors are therefore a potential therapeutic target for dysphagia.
1 Introduction
Throughout life, the ability to eat well and savor a meal remains one of the most important factors in pursuing happiness. Therefore, developing proper swallowing functions in childhood and maintaining them throughout life is essential.
In 2017, 1.13 million people over the age of 70 (261/100,000) died from secondary community-acquired pneumonia (CAP), a 9% increase in that mortality rate over the past 30 years (1). CAP in the elderly population frequently stems from aspiration pneumonia (AP). Aspiration pneumonia has been proposed as a physiologic phenomenon caused by aspiration due to the age-related decline in swallowing function and cough reflex (2). Furthermore, stroke and prolonged bed rest have been identified as risk factors for aspiration. However, there are still no uniform global diagnostic criteria for aspiration pneumonia. Certain cultures regard and treat aspiration pneumonia in cases of obvious aspiration associated with head and neck cancer or stroke. However, those associated with senility are not considered for active intervention. The proportion of aspiration pneumonia among pneumonia cases that result in hospitalization increases with age, and non-aspiration pneumonia is less common among older adults (3, 4). In other words, aspiration pneumonia poses a significant challenge that must be addressed to ensure healthy longevity in today’s aging society worldwide.
In this review, we would like to discuss the role of taste sensation in swallowing motor functions, their disorders, and the functions of taste receptors expressed outside the oral mucosa. We can examine strategies for overcoming swallowing disorders, paving the way for a healthy and fulfilling life throughout our entire lifespan.
2 Population aging worldwide and dysphagia/aspiration pneumonia
Swallowing disorders are characterized and classified by the following: [1] Inability to form a bolus of food in the oral cavity and to transport the bolus to the pharynx. [2] Misdirection of food and fluid in the pharynx, causing it to enter the trachea instead of the esophagus. [3] Inability to get rid of food or liquid accidentally entering the trachea by coughing (5).
In today’s aging society, aspiration pneumonia due to dysphagia in older adults is becoming an increasing problem (6). Older adults over 65 years old account for two-thirds of those affected by dysphagia (7). In the United States, aspiration pneumonia was reported as the underlying cause of death in an average of 17,616 cases per year, representing 30.1% of all aspiration pneumonia-related deaths. Individuals aged 75 and over accounted for 76.0% of deaths from aspiration pneumonia, with an age-adjusted rate ratio of 161.0 (CI 160.5–161.5) (8). Maintaining oral hygiene and swallowing function is important in preventing aspiration pneumonia (9).
3 Swallowing and skeletal muscle
Various muscles are involved in swallowing movements. They include the masticatory muscles, the tongue, and the perifacial muscles involved in mastication movements. They include the supralaryngeal muscles involved in elevating the larynx. The sublingual muscles support the hyoid bone, and the pharyngeal contractile muscles increase swallowing pressure. However, this is not the only cause of dysphagia, as poor posture with aging, such as hunchback and neck anteflexion, can lead to compensatory use of muscles needed for swallowing, resulting in secondary dysphagia (10).
Although sarcopenia is a disease characterized by generalized muscle loss, muscle weakness, and loss of physical function, the muscles associated with swallowing do not seem to lose muscle mass and strength like other muscles. These muscles, except the geniohyoid muscle, are actively engaged in respiration, even at rest, under the control of the respiratory center. Therefore, it has been thought that disuse muscle atrophy is unlikely to occur in the muscles associated with swallowing (11). In contrast, there are reports of accelerated muscle atrophy of the tongue and diaphragm in patients with aspiration pneumonia (12), and studies show that muscle atrophy occurs in the respiratory muscles and muscles associated with swallowing (13).
Various types of training are available to improve swallowing function, including resistance training of swallowing-related muscles (14–16) and neuroelectrical stimulation therapy (17).
4 Taste receptors and skeletal muscle
The Tas1R family (Tas1r1, Tas1r2, and Tas1r3) are G protein-coupled receptors that sense sweet taste in the Tas1r2/Tas1r3 complex and umami taste in the Tas1r1/Tas1r3 complex as taste receptors. Recent studies have revealed that the Tas1R family members function as nutrient sensors in tissues other than the oral mucosa (18).
Skeletal muscle is one of the largest organs in the human body, accounting for approximately 40% of body mass. With age, skeletal muscle mass tends to decrease, leading to a condition known as sarcopenia. Sarcopenia is characterized by muscle weakness and decreased physical activity capacity, which can significantly impact the quality of life for older adults. Since muscle is a central organ that takes up and consumes sugar and fatty acids from the blood, its maintenance is considered essential for preventing metabolic-related diseases such as obesity and diabetes (19).
Satellite cells are muscle stem cells that provide a regenerative capacity to skeletal muscle. Aged skeletal muscles have an impaired regenerative capacity which can contribute to physical incapacitation. Aged skeletal muscles fail to retain stem cell quiescence (20–22). Muscle stem cell number and the functionality decline with aging (20–25). The process of autophagy, which involves the degradation of long-lived proteins and damaged organelles in lysosomes, has been implicated in the aging of different model organisms (22, 26–29). Maintenance of skeletal muscle mass also relies on the balance between anabolic and catabolic processes. Protein degradation in skeletal muscle cells is essentially mediated by the activity of two conserved pathways: the ubiquitin proteasomal pathway and the autophagic/lysosomal pathway (30). The ubiquitin-proteasomal pathway is responsible for the turnover of the majority of soluble and myofibrillar muscle proteins (31, 32). Autophagy also plays an important role in the degradation of skeletal muscle (33).
Tas1r1 and Tas1r3, are highly expressed in muscle relative to other tissues (34). We reported that myogenic regulatory factor (MRF)s regulate the expression of Tas1r3 (35). Overexpression of MyoD and Myogenin induces murine Tas1r3 promoter activity. ChIP analysis demonstrated that MyoD and Myogenin bind to the endogenous murine Tas1r3 promoter and increase mRNA levels of endogenous Tas1r3 in murine myoblasts. We demonstrated that the expression of Tas1r1 also increased during myogenesis in a cell culture model (36). These findings are further supported by the observation that Tas1r1 and Tas1r3 are endogenously expressed in skeletal muscle tissue. The skeletal muscle Tas1r3 knockout mice exhibit decreased activity of the mammalian target of rapamycin complex 1 (mTORC1) and a higher frequency of autophagy (34), suggesting that umami receptor function is critical to detecting nutrient status since skeletal muscle is the main source of stored amino acid during times of amino acid deprivation (37). For these reason, we hypothesized that disorder of signaling through Umami receptor is involved in pathogenesis of skeletal muscle related diseases including sarcopenia and swallowing disorders.
5 Rehabilitation, nutrition, and taste
Adequate nutrition is essential for enhancing the effectiveness of rehabilitation through strength training, and the concept of rehabilitation nutrition is gaining increasing recognition (38). The importance of the trinity of rehabilitation, nutrition, and oral management for sarcopenic dysphagia in older adults is emphasized (39). Taste is essential to sustain life, and its primary function is to facilitate the intake of essential nutrients and the rejection of harmful substances. Umami receptors are expressed on epithelial cells in the small intestine. Glutamate stimulation via umami receptors in the small intestine is essential for maintaining the normal turnover of small intestinal epithelial cells (40). Insufficient umami stimulation of umami receptors in the small intestine can lead to impaired nutrient absorption from the small intestine. To ensure optimal nutrient intake, it is necessary to study the sense of taste and the regulatory mechanism of nutrient absorption via taste receptors in the intestinal tract.
6 Swallowing function and sense of taste and preferences
Swallowing function is known to be influenced by individual preferences. High temporal resolution fMRI studies show that taste, smell, and visual sensations stimulated by highly palatable foods, such as popcorn and chocolate, activate areas of the cerebral cortex associated with swallowing (sensorimotor area, insular cortex, cingulate gyrus, prefrontal cortex) (41). Taste stimuli alter the swallowing reflex. Taste, particularly acidity, increases swallowing pressure and suprahyoid muscle activity (42–44). Other reports indicate that salty and sweet stimuli increase swallowing pressure and suprahyoid muscle activity (43–45). However, foods with intense sour or salty flavors that directly trigger swallowing are considered problematic regarding taste and palatability (43). Conversely, there is a positive correlation between taste and swallowing function. Salty and sweet stimuli are more effective than no-taste stimuli in increasing swallowing pressure and supratrochlear muscle activity (42, 44, 45). A study involving young, healthy subjects compared the ease of swallowing foods with the five basic tastes (sweet, salty, sour, bitter, and umami) against tasteless foods. Sweet and tasteless foods exhibited slightly better swallowing acceptability than by sour and bitter foods (46). Investigations involving healthy adult male volunteers have shown that cortical swallowing pathways are similarly modulated by both sweet and bitter stimuli (46). This study implies the existence of a close interaction between taste perception and swallowing activity via the central nervous system.
7 Swallowing function-carbonation and taste
Swallowing movements are not merely simple muscle contractions; rather, they are controlled by various nerves. Stimulating these sensory nerves is important for maintaining their functionality and overcoming swallowing dysfunction. Using carbonated beverages as a stimulatory modality has recently garnered attention for its efficacy in enhancing swallowing movements. Carbonated water increases muscle activity during swallowing more than plain water (47), and the higher gas volume of carbonated water increases tongue pressure (48). In addition to its effect on muscle activity, carbonated water improves pharyngeal clearance with significantly faster pharyngeal transit time compared to normal liquids (49). Furthermore, carbonated water supports the shortening of tablet transit time during tablet swallowing (50). Furthermore, carbonated water is less likely to be aspirated or left in the pharynx than non-carbonated liquids in patients with central nervous system disease (51, 52). We and other laboratories have reported that thickened carbonic acid further improves swallowing function (53, 54).
As one of the reasons why carbonated beverages improve swallowing, H2CO3 produced by carbonic anhydrase IV in saliva from CO2 dissolved in carbonated beverages stimulates nociceptors in the oral mucosa and activates the trigeminal nerve (55). In addition, the carbonic acid in carbonated water splits into bicarbonate and hydrogen ions, and the hydrogen ions stimulate the facial nerve via acid-sensitive taste receptors (56). Stimulation with capsaicin improves swallowing function (57).
Capsaicin-induced improvement of swallowing involves TRPV1 at the nerve terminal. ASIC3 is a receptor expressed at nerve endings similar to TRPV1. The ASIC3 receptor has been implicated in the effects of carbonic acid stimulation on swallowing (58).
In contrast, there are reports that swallowing only carbonated water can worsen the penetration-aspiration scale (PAS) and videofluoroscopic dysphagia scale (VDS) (59, 60). This is thought to be influenced by preference and taste (Please see preceding paragraph).
8 Swallowing and food forms
The available forms of food intake are frequently restricted due to poor swallowing functions. However, even if dysphagia-adjusted diets, such as kizami or paste diets, are suitable for the remaining swallowing functions, these dysphagia-adjusted diets do not maintain the original food form and may decrease the patient’s desire to eat (61). Sight and smell control appetite (62). Other laboratories reported that the arrangement of coloring, smell, and flavor could increase food intake and improve nutritional status, while dysphagia-adjusted diets serve as food form (63–65). Eating well brings a sense of spiritual richness and satisfaction, and it helps establish and maintain social relationships and communication. Because social activities are often limited for older adults, meals are a major recreation component.
Yoshihara et al. (66) reported a positive correlation between appetite and quality of life in a study of an elderly community in Japan. Eating food that is not tasty solely for sustenance can be a disagreeable experience. Meals should be enjoyable to consume in terms of flavor and presentation. Older individuals exhibit different eating patterns compared to young children just starting to learn regarding food. Older individuals have had the pleasure of enjoying many delicious meals throughout their lives. The purpose of a meal extends beyond simply fulfilling nutritional and energy needs. The European Pressure Ulcer Advisory Panel’s guidelines for pressure ulcer prevention and treatment include considerations for appetizing food with attractive presentations (67).
9 Discussion
Thus, swallowing function is closely related not only to mastication and pharyngeal muscle contraction but also to various stimulus inputs (Figure 1). Therefore, simple muscle training may not be sufficient to treat dysphagia. This review focused on swallowing functions regarding taste and taste receptors. Maintaining swallowing functions and taking adequate nutrients are necessary to maintain swallowing functions. On the contrary, poor nutritional status naturally leads to a decline in swallowing function. This is indeed a chicken and egg situation between “swallowing” and “nutrition.”
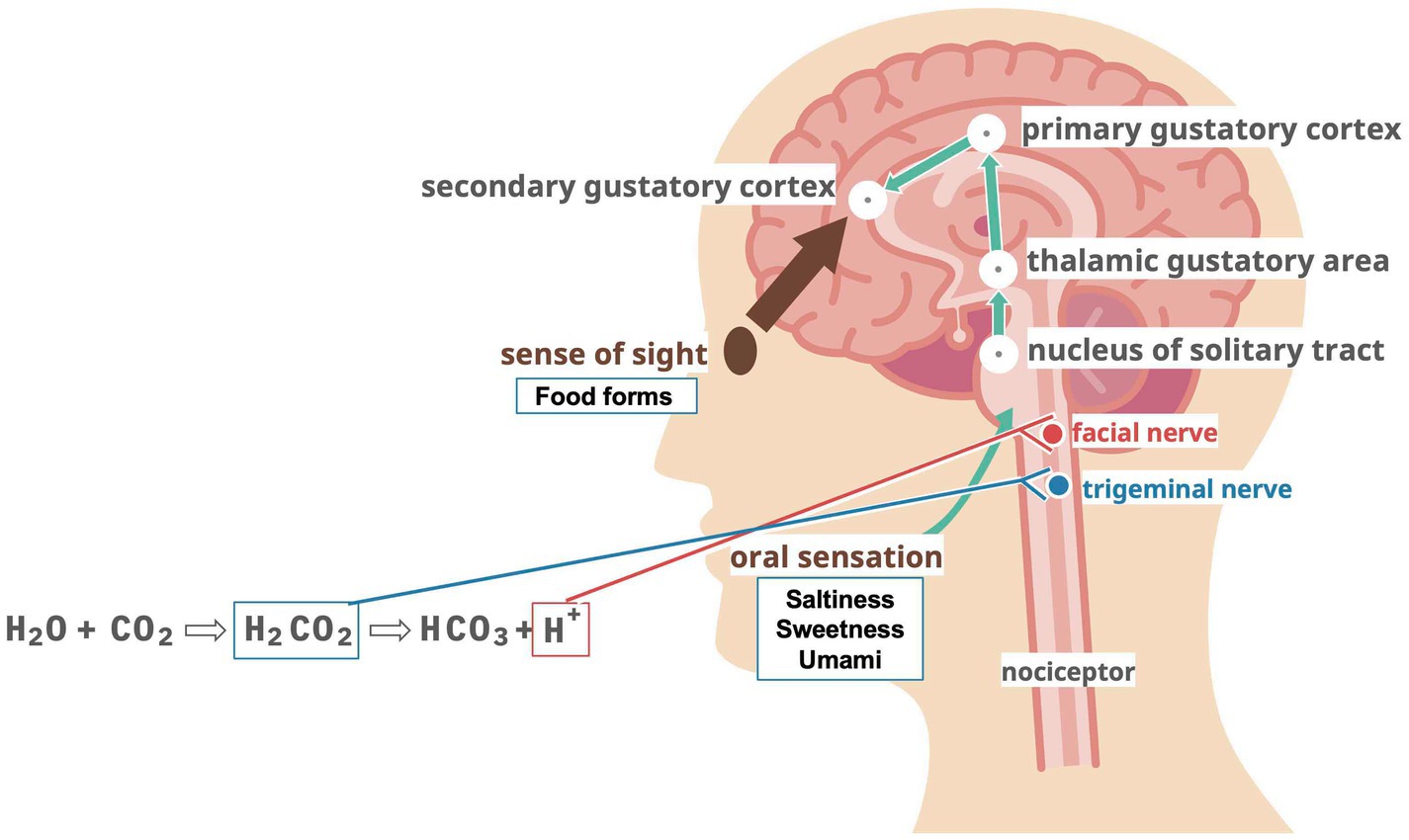
Figure 1. Hypothesized mechanisms of action for taste, vision, and carbonic acid stimulation.
Amino acids (proteins) in food are received by umami receptors (Tas1r1/Tas1r3) in the taste buds of the oral mucosa. These amino acids (proteins) are recognized as “delicious” taste sensations and are actively absorbed after digestion and stored in skeletal muscles as myofiber proteins. Muscle fibers are depleted during starvation, and amino acids are released into the bloodstream (37). In sarcopenia, this amino acid network (Figure 2) may be disrupted, leading to the breakdown of skeletal muscle proteins. This releases more amino acids that are taken up, causing a decrease in skeletal muscle mass and function. On the other hand, Tas1r3 knockout does not alter amino acid concentrations due to compensatory increases of other amino acid transporters (34). In addition to this, there are several issues that need to be resolved before deciding the function of taste receptor in skeletal muscle. For example, do Tas1r1 and Tas1r3 form a heteromeric complex in muscle cells similar to in taste bud cells? What is the ligand for taste receptors when they function as amino acid sensors in skeletal muscle? Careful in vivo experimental analysis focusing on skeletal muscle metabolism will be required to address these issues.
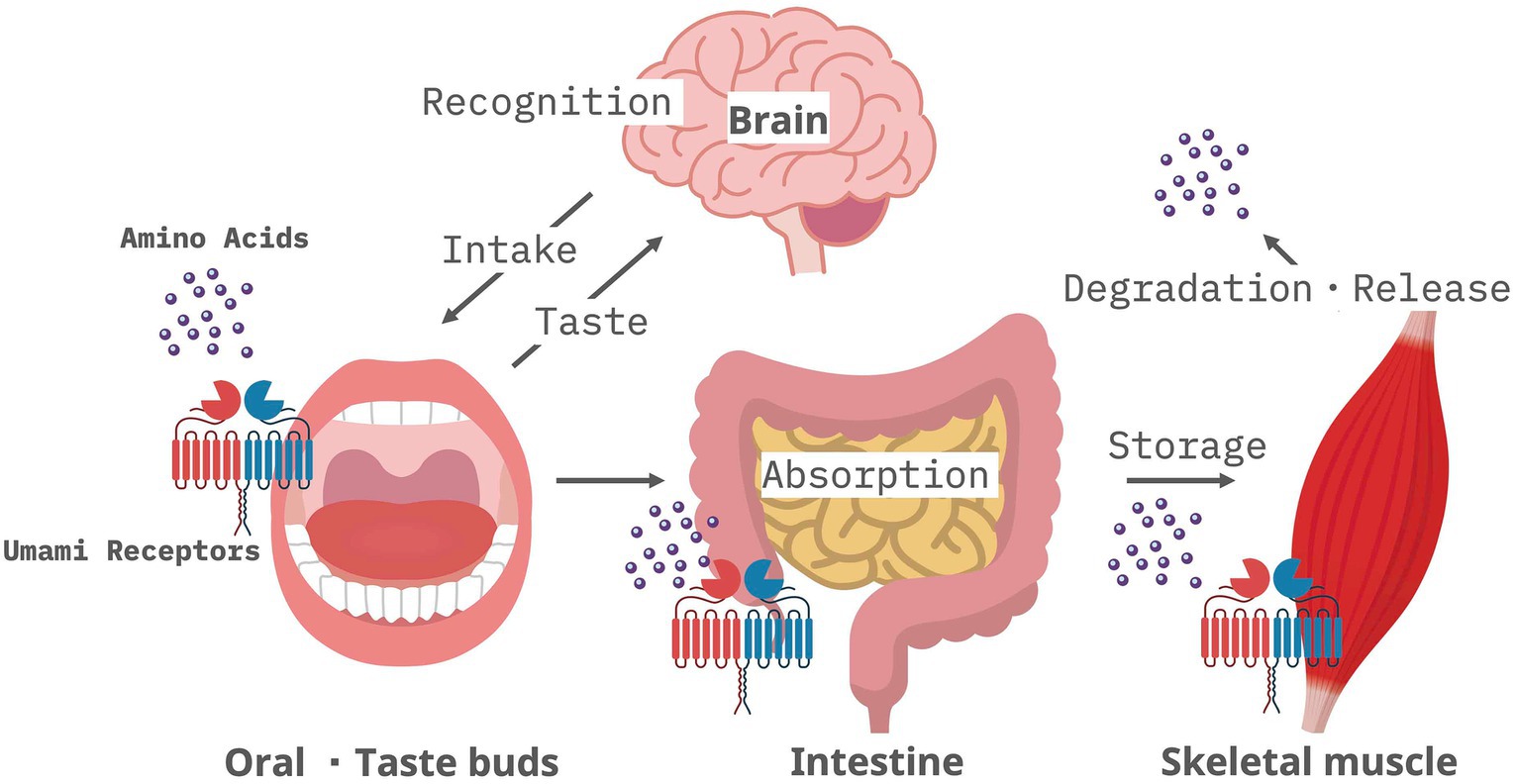
Figure 2. Amino acid network via umami receptors expressed by oral mucosa, intestine, and skeletal muscle.
Humans with decreased sensitivity to umami taste were reported to show significant weight loss and deterioration in general health compared to those with other taste disorders (sweet, salty, sour, and bitter) (68). In this report, it was interpreted that the patients had difficulty perceiving umami, which may have made the food less palatable and reduced their food intake. Moreover, a reduction in the expression level and sensitivity of umami receptors at the genomic level diminishes taste perception and impairs the function of umami receptors in the small intestinal mucosa, skeletal muscle, and other organs that comprise the amino acid sensing network. In other words, the observed weight loss and decline in overall health may be manifestations of underlying nutritional deficiencies caused by impaired digestion and absorption and reduced skeletal muscle mass resulting from abnormal skeletal muscle metabolism. Multiple single nucleotide polymorphisms are observed in the gene encoding the umami receptor, with each mutation having a different sensitivity to the umami receptor in vitro (69). Therefore, based on their genetic background, humans have reduced sensitivity to umami receptors in the body.
Medical advancements have significantly extended our lifespans, allowing us to delay death’s inevitable arrival. However, this progress has created a disparity between healthy life expectancy, the number of years an individual can expect to live independently in society, and overall life expectancy, which simply marks the end of life. In addition, the collapse of current healthcare systems and the economic disparity in the selection of life are becoming realities due to the extremely expensive drugs created by the latest life science and technology. If we can advocate an inexpensive extension of healthy life expectancy based on food, we can solve these problems and make a major shift toward a sustainable super-aging society.
This review article highlights the association between swallowing disorders and sarcopenia of the associated muscles. Diseases that cause skeletal muscle atrophy, such as sarcopenia, significantly reduce healthy life expectancy. Currently, no commercialized interventions, except for exercise, exist to maintain or restore skeletal muscle mass and function. Considering the high prevalence and pathogenesis of sarcopenia, the prevention and treatment of sarcopenia should be based on a healthy diet combined with adequate exercise rather than expensive medicine such as molecularly targeted drugs. Sufficient amino acid intake, a crucial component of skeletal muscle, is essential for preventing sarcopenia. Future research endeavors to identify amino acid combinations that efficiently activate the umami receptors of each cell in the amino acid network may contribute to overcoming sarcopenia and thereby extending healthy life expectancy in this super-aging society.
Author contributions
MO: Writing – original draft, Writing – review & editing. MM: Writing – review & editing. TO: Writing – review & editing. HS: Writing – review & editing. TK: Writing – review & editing. SK: Conceptualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by grants from the Ministry of Education, Culture, Sports, Science, and Technology of Japan (KAKEN 22K19634 to SK), from Society for Research on Umami Taste (SK), the YMFG Regional Enterprise Support Foundation (SK).
Acknowledgments
We are grateful to the member of Division of Molecular Signaling and Biochemistry (Kyushu Dental University) for comments and assistance.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Yoshimatsu, Y, Melgaard, D, Westergren, A, Skrubbeltrang, C, and Smithard, DG. The diagnosis of aspiration pneumonia in older persons: a systematic review. Eur Geriatr Med. (2022) 13:1071–80. doi: 10.1007/s41999-022-00689-3
2. Marik, PE. Aspiration pneumonitis and aspiration pneumonia. N Engl J Med. (2001) 344:665–71. doi: 10.1056/NEJM200103013440908
3. Teramoto, S, Fukuchi, Y, Sasaki, H, Sato, K, Sekizawa, K, Matsuse, T, et al. High incidence of aspiration pneumonia in community-and hospital-acquired pneumonia in hospitalized patients: a multicenter, prospective study in Japan. J Am Geriatr Soc. (2008) 56:577–9. doi: 10.1111/j.1532-5415.2008.01597.x
4. Teramoto, S, Matsuse, T, and Fukuchi, Y. Clinical significance of nocturnal oximeter monitoring for detection of sleep apnea syndrome in the elderly. Sleep Med. (2002) 3:67–71. doi: 10.1016/s1389-9457(01)00129-0
5. Leopold, NA, and Kagel, MC. Dysphagia--ingestion or deglutition?: a proposed paradigm. Dysphagia. (1997) 12:202–6. doi: 10.1007/PL00009537
6. Marik, PE, and Kaplan, D. Aspiration pneumonia and dysphagia in the elderly. Chest. (2003) 124:328–36. doi: 10.1378/chest.124.1.328
7. Sue, EE. Dysphagia and aspiration pneumonia in older adults. J Am Acad Nurse Pract. (2010) 22:17–22. doi: 10.1111/j.1745-7599.2009.00470.x
8. Gupte, T, Knack, A, and Cramer, JD. Mortality from aspiration pneumonia: incidence, trends, and risk factors. Dysphagia. (2022) 37:1493–500. doi: 10.1007/s00455-022-10412-w
9. Yoneyama, T, Yoshida, M, Matsui, T, and Sasaki, H. Oral care and pneumonia. Oral Care Working Group Lancet. (1999) 354:515. doi: 10.1016/s0140-6736(05)75550-1
10. Uchida, M, Yamaguchi, K, Tamai, T, Kobayashi, K, and Tohara, H. Effects of simulated kyphosis posture on swallowing and respiratory functions. J Phys Ther Sci. (2023) 35:593–7. doi: 10.1589/jpts.35.593
11. Grelot, L, Barillot, JC, and Bianchi, AL. Pharyngeal Motoneurones: respiratory-related activity and responses to laryngeal afferents in the Decerebrate cat. Exp Brain Res. (1989) 78:336–44. doi: 10.1007/BF00228905
12. Komatsu, R, Okazaki, T, Ebihara, S, Kobayashi, M, Tsukita, Y, Nihei, M, et al. Aspiration pneumonia induces muscle atrophy in the respiratory, skeletal, and swallowing systems. J Cachexia Sarcopenia Muscle. (2018) 9:643–53. doi: 10.1002/jcsm.12297
13. Wakabayashi, H. Presbyphagia and Sarcopenic dysphagia: association between aging, sarcopenia, and deglutition disorders. J Frailty Aging. (2014) 3:97–103. doi: 10.14283/jfa.2014.8
14. Shaker, R, Kern, M, Bardan, E, Taylor, A, Stewart, ET, Hoffmann, RG, et al. Augmentation of Deglutitive upper esophageal sphincter opening in the elderly by exercise. Am J Phys. (1997) 272:G1518–22. doi: 10.1152/ajpgi.1997.272.6.G1518
15. Yoshida, M, Groher, ME, Crary, MA, Mann, GC, and Akagawa, Y. Comparison of surface Electromyographic (Semg) activity of submental muscles between the head lift and tongue press exercises as a therapeutic exercise for pharyngeal dysphagia. Gerodontology. (2007) 24:111–6. doi: 10.1111/j.1741-2358.2007.00164.x
16. Wada, S, Tohara, H, Iida, T, Inoue, M, Sato, M, and Ueda, K. Jaw-opening exercise for insufficient opening of upper esophageal sphincter. Arch Phys Med Rehabil. (2012) 93:1995–9. doi: 10.1016/j.apmr.2012.04.025
17. Ortega, O, Rofes, L, Martin, A, Arreola, V, Lopez, I, and Clave, P. A comparative study between two sensory stimulation strategies after two weeks treatment on older patients with oropharyngeal dysphagia. Dysphagia. (2016) 31:706–16. doi: 10.1007/s00455-016-9736-4
18. Kokabu, S, Lowery, JW, Toyono, T, Sato, T, and Yoda, T. On the emerging role of the taste receptor type 1 (T1r) family of nutrient-sensors in the musculoskeletal system. Molecules. (2017) 22:469. doi: 10.3390/molecules22030469
19. Wolfe, RR. The underappreciated role of muscle in health and disease. Am J Clin Nutr. (2006) 84:475–82. doi: 10.1093/ajcn/84.3.475
20. Chakkalakal, JV, Jones, KM, Basson, MA, and Brack, AS. The aged niche disrupts muscle stem cell quiescence. Nature. (2012) 490:355–60. doi: 10.1038/nature11438
21. Sousa-Victor, P, Gutarra, S, García-Prat, L, Rodriguez-Ubreva, J, Ortet, L, Ruiz-Bonilla, V, et al. Geriatric muscle stem cells switch reversible quiescence into senescence. Nature. (2014) 506:316–21. doi: 10.1038/nature13013
22. Sousa-Victor, P, García-Prat, L, Serrano, AL, Perdiguero, E, and Muñoz-Cánoves, P. Muscle stem cell aging: regulation and rejuvenation. Trends Endocrinol Metab. (2015) 26:287–96. doi: 10.1016/j.tem.2015.03.006
23. Price, FD, von Maltzahn, J, Bentzinger, CF, Dumont, NA, Yin, H, Chang, NC, et al. Inhibition of JAK-STAT signaling stimulates adult satellite cell function. Nat Med. (2014) 20:1174–81. doi: 10.1038/nm.3655
24. Tierney, MT, Aydogdu, T, Sala, D, Malecova, B, Gatto, S, Puri, PL, et al. STAT3 signaling controls satellite cell expansion and skeletal muscle repair. Nat Med. (2014) 20:1182–6. doi: 10.1038/nm.3656
25. Bernet, JD, Doles, JD, Hall, JK, Kelly Tanaka, K, Carter, TA, and Olwin, BB. p38 MAPK signaling underlies a cell-autonomous loss of stem cell self-renewal in skeletal muscle of aged mice. Nat Med. (2014) 20:265–71. doi: 10.1038/nm.3465
26. Cuervo, AM, Bergamini, E, Brunk, UT, Dröge, W, Ffrench, M, and Terman, A. Autophagy and aging: the importance of maintaining “clean” cells. Autophagy. (2005) 1:131–40. doi: 10.4161/auto.1.3.2017
27. He, C, and Klionsky, DJ. Regulation mechanisms and signaling pathways of autophagy. Annu Rev Genet. (2009) 43:67–93. doi: 10.1146/annurev-genet-102808-114910
28. Carnio, S, LoVerso, F, Baraibar, MA, Longa, E, Khan, MM, Maffei, M, et al. Autophagy impairment in muscle induces neuromuscular junction degeneration and precocious aging. Cell Rep. (2014) 8:1509–21. doi: 10.1016/j.celrep.2014.07.061
29. Rubinsztein, DC, Mariño, G, and Kroemer, G. Autophagy and aging. Cell. (2011) 146:682–95. doi: 10.1016/j.cell.2011.07.030
30. Sandri, M. Signaling in muscle atrophy and hypertrophy. Physiology (Bethesda). (2008) 23:160–70. doi: 10.1152/physiol.00041.2007
31. Glass, DJ. Signalling pathways that mediate skeletal muscle hypertrophy and atrophy. Nat Cell Biol. (2003) 5:87–90. doi: 10.1038/ncb0203-87
32. Sandri, M, Sandri, C, Gilbert, A, Skurk, C, Calabria, E, Picard, A, et al. Foxo transcription factors induce the atrophy-related ubiquitin ligase atrogin-1 and cause skeletal muscle atrophy. Cell. (2004) 117:399–412. doi: 10.1016/s0092-8674(04)00400-3
33. Mizushima, N, Levine, B, Cuervo, AM, and Klionsky, DJ. Autophagy fights disease through cellular self-digestion. Nature. (2008) 451:1069–75. doi: 10.1038/nature06639
34. Wauson, EM, Zaganjor, E, Lee, AY, Guerra, ML, Ghosh, AB, Bookout, AL, et al. The G protein-coupled taste receptor T1r1/T1r3 regulates Mtorc1 and autophagy. Mol Cell. (2012) 47:851–62. doi: 10.1016/j.molcel.2012.08.001
35. Kokabu, S, Lowery, JW, Toyono, T, Seta, Y, Hitomi, S, Sato, T, et al. Muscle regulatory factors regulate T1r3 taste receptor expression. Biochem Biophys Res Commun. (2015) 468:568–73. doi: 10.1016/j.bbrc.2015.10.142
36. Hirata, Y, Toyono, T, Kokabu, S, Obikane, Y, Kataoka, S, Nakatomi, M, et al. Kruppel-like factor 5 (Klf5) regulates expression of mouse T1r1 amino acid receptor gene (Tas1r1) in C2c12 myoblast cells. Biomed Res. (2019) 40:67–78. doi: 10.2220/biomedres.40.67
37. Shimizu, N, Yoshikawa, N, Ito, N, Maruyama, T, Suzuki, Y, Takeda, S, et al. Crosstalk between glucocorticoid receptor and nutritional sensor mTOR in skeletal muscle. Cell Metab. (2011) 13:170–82. doi: 10.1016/j.cmet.2011.01.001
38. Wakabayashi, H, and Sakuma, K. Rehabilitation nutrition for sarcopenia with disability: a combination of both rehabilitation and nutrition care management. J Cachexia Sarcopenia Muscle. (2014) 5:269–77. doi: 10.1007/s13539-014-0162-x
39. Wakabayashi, H. Triad of rehabilitation, nutrition, and Oral Management for Sarcopenic Dysphagia in older people. Geriatr Gerontol Int. (2023). doi: 10.1111/ggi.14651
40. Xiao, W, Feng, Y, Holst, JJ, Hartmann, B, Yang, H, and Teitelbaum, DH. Glutamate prevents intestinal atrophy via luminal nutrient sensing in a mouse model of Total parenteral nutrition. FASEB J. (2014) 28:2073–87. doi: 10.1096/fj.13-238311
41. Babaei, A, Kern, M, Antonik, S, Mepani, R, Ward, BD, Li, SJ, et al. Enhancing effects of flavored nutritive stimuli on cortical swallowing network activity. Am J Physiol Gastrointest Liver Physiol. (2010) 299:G422–9. doi: 10.1152/ajpgi.00161.2010
42. Palmer, PM, McCulloch, TM, Jaffe, D, and Neel, AT. Effects of a sour bolus on the intramuscular Electromyographic (Emg) activity of muscles in the submental region. Dysphagia. (2005) 20:210–7. doi: 10.1007/s00455-005-0017-x
43. Logemann, JA, Pauloski, BR, Colangelo, L, Lazarus, C, Fujiu, M, and Kahrilas, PJ. Effects of a sour bolus on oropharyngeal swallowing measures in patients with neurogenic dysphagia. J Speech Hear Res. (1995) 38:556–63. doi: 10.1044/jshr.3803.556
44. Pelletier, CA, and Dhanaraj, GE. The effect of taste and palatability on lingual swallowing pressure. Dysphagia. (2006) 21:121–8. doi: 10.1007/s00455-006-9020-0
45. Ding, R, Logemann, JA, Larson, CR, and Rademaker, AW. The effects of taste and consistency on swallow physiology in younger and older healthy individuals: a surface Electromyographic study. J Speech Lang Hear Res. (2003) 46:977–89. doi: 10.1044/1092-4388(2003/076)
46. Miyaoka, Y, Haishima, K, Takagi, M, Haishima, H, Asari, J, and Yamada, Y. Influences of thermal and gustatory characteristics on sensory and motor aspects of swallowing. Dysphagia. (2006) 21:38–48. doi: 10.1007/s00455-005-9003-6
47. Miura, Y, Morita, Y, Koizumi, H, and Shingai, T. Effects of taste solutions, carbonation, and cold stimulus on the power frequency content of swallowing submental surface electromyography. Chem Senses. (2009) 34:325–31. doi: 10.1093/chemse/bjp005
48. Moritaka, H, Kitade, M, Sawamura, S, Takihara, T, Awano, I, Ono, T, et al. Effect of carbon dioxide in carbonated drinks on Linguapalatal swallowing pressure. Chem Senses. (2014) 39:133–42. doi: 10.1093/chemse/bjt062
49. Bulow, M, Olsson, R, and Ekberg, O. Videoradiographic analysis of how carbonated thin liquids and thickened liquids affect the physiology of swallowing in subjects with aspiration on thin liquids. Acta Radiol. (2003) 44:366–72. doi: 10.1080/j.1600-0455.2003.00100.x
50. Hasselbalch, H, Jorgensen, F, Wamberg, T, and Hey, H. Alternatives to optimal Administration of Tablets. Acta Med Scand. (1985) 217:527–30. doi: 10.1111/j.0954-6820.1985.tb03257.x
51. Sdravou, K, Walshe, M, and Dagdilelis, L. Effects of carbonated liquids on oropharyngeal swallowing measures in people with neurogenic dysphagia. Dysphagia. (2012) 27:240–50. doi: 10.1007/s00455-011-9359-8
52. Larsson, V, Torisson, G, Bulow, M, and Londos, E. Effects of carbonated liquid on swallowing dysfunction in dementia with Lewy bodies and Parkinson’s disease dementia. Clin Interv Aging. (2017) 12:1215–22. doi: 10.2147/CIA.S140389
53. Morishita, M, Okubo, M, and Sekine, T. Effects of carbonated thickened drinks on pharyngeal swallowing with a flexible endoscopic evaluation of swallowing in older patients with oropharyngeal dysphagia. Healthcare (Basel). (2022) 10:1769. doi: 10.3390/healthcare10091769
54. Saiki, A, Yoshimi, K, Nakagawa, K, Nagasawa, Y, Yoshizawa, A, Yanagida, R, et al. Effects of thickened carbonated Cola in older patients with dysphagia. Sci Rep. (2022) 12:22151. doi: 10.1038/s41598-022-25926-4
55. Dessirier, JM, Simons, CT, Carstens, MI, O’Mahony, M, and Carstens, E. Psychophysical and neurobiological evidence that the Oral sensation elicited by carbonated water is of Chemogenic origin. Chem Senses. (2000) 25:277–84. doi: 10.1093/chemse/25.3.277
56. Chandrashekar, J, Yarmolinsky, D, von Buchholtz, L, Oka, Y, Sly, W, Ryba, NJ, et al. The taste of carbonation. Science. (2009) 326:443–5. doi: 10.1126/science.1174601
57. Ebihara, T, Sekizawa, K, Nakazawa, H, and Sasaki, H. Capsaicin and swallowing reflex. Lancet. (1993) 341:432. doi: 10.1016/0140-6736(93)93023-t
58. Tsuji, K, Tsujimura, T, Sakai, S, Suzuki, T, Yoshihara, M, Nagoya, K, et al. Involvement of capsaicin-sensitive nerves in the initiation of swallowing evoked by carbonated water in anesthetized rats. Am J Physiol Gastrointest Liver Physiol. (2020) 319:G564–72. doi: 10.1152/ajpgi.00233.2020
59. Turkington, L, Ward, EC, Farrell, A, Porter, L, and Wall, LR. Impact of carbonation on neurogenic dysphagia and an exploration of the clinical predictors of a response to carbonation. Int J Lang Commun Disord. (2019) 54:499–513. doi: 10.1111/1460-6984.12458
60. Takeuchi, C, Takei, E, Ito, K, Kulvanich, S, Magara, J, Tsujimura, T, et al. Effects of carbonation and temperature on voluntary swallowing in healthy humans. Dysphagia. (2021) 36:384–92. doi: 10.1007/s00455-020-10147-6
61. Shimizu, A, Fujishima, I, Maeda, K, Murotani, K, Kayashita, J, Ohno, T, et al. Texture-modified diets are associated with poor appetite in older adults who are admitted to a post-acute rehabilitation hospital. J Am Med Dir Assoc. (2021) 22:1960–5. doi: 10.1016/j.jamda.2021.05.018
62. Janet, R, Fournel, A, Fouillen, M, Derrington, E, Corgnet, B, Bensafi, M, et al. Cognitive and hormonal regulation of appetite for food presented in the olfactory and visual modalities. NeuroImage. (2021) 230:117811. doi: 10.1016/j.neuroimage.2021.117811
63. Mineyama, R, Tezuka, F, Takagi, N, Kokabu, S, and Okubo, M. Nutritional management in a 101-year-old woman with physical inactivity and general weakness: a case report. Geriatrics (Basel). (2023) 8:8. doi: 10.3390/geriatrics8010008
64. Inayama, M, Goto, T, Kokabu, S, and Okubo, M. Weaning from tube feeding post stroke by eating, swallowing, and nutritional support in-home: a case report. Home Healthc Now. (2023) 41:221–5. doi: 10.1097/NHH.0000000000001173
65. Navarro, DA, Boaz, M, Krause, I, Elis, A, Chernov, K, Giabra, M, et al. Improved meal presentation increases food intake and decreases readmission rate in hospitalized patients. Clin Nutr. (2016) 35:1153–8. doi: 10.1016/j.clnu.2015.09.012
66. Yoshihara, A, Seida, Y, Kataoka, S, Hanada, N, and Miyazaki, H. The relationship between appetite and quality of life in community—dwelling older adults. (in Japanese). Dent. Health. (2004) 54:241–8. doi: 10.5834/jdh.54.3_241
67. Munoz, N, and Posthauer, ME. Nutrition strategies for pressure injury management: implementing the 2019 international clinical practice guideline. Nutr Clin Pract. (2022) 37:567–82. doi: 10.1002/ncp.10762
68. Sasano, T, Satoh-Kuriwada, S, Shoji, N, Iikubo, M, Kawai, M, Uneyama, H, et al. Important role of umami taste sensitivity in Oral and overall health. Curr Pharm Des. (2014) 20:2750–4. doi: 10.2174/13816128113199990577
Keywords: aspiration pneumonia, dysphagia, carbonated thickened drink, taste receptors, skeletal muscle, taste, preferences
Citation: Okubo M, Morishita M, Odani T, Sakaguchi H, Kikutani T and Kokabu S (2024) The importance of taste on swallowing function. Front. Nutr. 11:1356165. doi: 10.3389/fnut.2024.1356165
Edited by:
Ken Iwatsuki, Tokyo University of Agriculture, JapanReviewed by:
Yoshinari Uehara, Fukuoka University, JapanCopyright © 2024 Okubo, Morishita, Odani, Sakaguchi, Kikutani and Kokabu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shoichiro Kokabu, cjE0a29rYWJ1QGZhLmt5dS1kZW50LmFjLmpw
†ORCID: Shoichiro Kokabu, https://orcid.org/0000-0002-6663-4327