 Carlos Alberto Rodrigues de Sousa1,2
Carlos Alberto Rodrigues de Sousa1,2 Luciana Fidalgo Nogueira3
Luciana Fidalgo Nogueira3 José Cipolla-Neto3
José Cipolla-Neto3 Claudia Roberta de Castro Moreno2,4
Claudia Roberta de Castro Moreno2,4 Elaine Cristina Marqueze1,3*
Elaine Cristina Marqueze1,3*- 1Carlos Chagas Filho Biophysics Institute, Federal University of Rio de Janeiro, Rio de Janeiro, Brazil
- 2Department of Epidemiology, Postgraduate Program in Public Health, Catholic University of Santos, São Paulo, Brazil
- 3Department of Physiology and Biophysics, Institute of Biomedical Sciences, University of São Paulo, São Paulo, Brazil
- 4Department of Health, Life Cycles and Society, Faculty of Public Health, University of São Paulo, São Paulo, Brazil
Introduction: Interactions between circadian clocks and key mediators of chronic low-grade inflammation associated with fat consumption may be important in maintaining metabolic homeostasis and may pose a risk for the development of obesity-associated comorbidities, especially type 2 diabetes (T2DM).
Objective: The aims of the present study were to evaluate the effects of melatonin administration on diabetes risk markers according to dietary lipid profile (pro-inflammatory versus anti-inflammatory) in excessive weight night workers, and to determine the effect of administration on fat consumption profile.
Methods: A randomized, controlled, double-blind, crossover clinical trial involving 27 nursing professionals working permanent night shifts under a 12×36-hour system. The melatonin group (12 weeks) used synthetic melatonin (3 mg) only on days off and between shifts, while the placebo group (12 weeks) was instructed to take a placebo, also on days off and between shifts. For inflammatory characteristics, participants were divided into pro-inflammatory (saturated fats, trans fats and cholesterol) and anti-inflammatory (monounsaturated, polyunsaturated fats and EPA + DHA) groups according to fatty acid determinations. At baseline and at the end of each phase, blood glucose, insulin, glycosylated hemoglobin plasma concentrations were collected, and HOMA-IR was calculated.
Conclusion: Melatonin administration for 12 weeks had no effect on T2DM risk markers according to dietary lipid profile (pro-inflammatory or anti-inflammatory potential) in excessive weight night workers. Among the limitations of the study include the fact that the low dose may have influenced the results expected in the hypothesis, and individual adaptations to night work were not evaluated. The insights discussed are important for future research investigating the influence of melatonin and fats considered anti- or pro-inflammatory on glucose and insulin homeostasis related to night work.
1 Introduction
Engaging in night shift work can impact biological rhythms and is often associated with alterations in sleep patterns, poor quality of life and reduced recovery (1). Circadian misalignment at eating times, as well as activity during the night among night workers, has been associated with an increased risk of developing diabetes mellitus (DM), hypertension, obesity and cardiovascular disease (1–4).
Diet composition, especially a high-fat and high saturated fat (SFA) diet, modulates the rhythmicity of the peripheral circadian clock in vitro and in vivo (5, 6). There is evidence of an increased preference for high-fat foods for breakfast (6), where this is because the timing of this meal is a potential zeitgeber, promoting interactions between the body’s central clock and nutrient sensory pathways (e.g., AMPK). In this context, highly palatable foods, such as fats, can directly signal the orexigenic centers and regions associated with hedonic stimulation, stimulating food-seeking behavior (7–10).
Some studies have identified a higher fat intake among night workers. Heath et al. (11) found that fat intake by night workers exceeded the recommended level (with fat representing 20%–35% of total energy intake and comprising 15.5% saturated fat). In another study, of airline employees at high risk of developing type 2 diabetes mellitus (T2DM) and/or diabetics, the authors found that women over 47.6 years of age who worked day and night shifts on board (flight), had higher energy intake from fat (at 33.9%, comprising 12.8% saturated fat) compared to women in the same age group who worked exclusively during the day (12).
The dysmetabolism seen in night workers can lead to changes in eating patterns or vice versa, such as an increase in daily energy consumption (13), greater hunger and longer duration of food intake (14). Excess adiposity, now recognized as a low-grade inflammatory state, can also reduce insulin responsiveness in insulin-sensitive tissues and promote the risk of T2DM through action on circulating cells (15). In addition, insufficient and poor sleep quality, often associated with night work, is also associated with a higher likelihood of obesity and DM, further increasing the risk of this group of workers (1, 16, 17). In situations of low-grade inflammation, such as obesity, the chronicity of in-flammation can lead to comorbidities, such as cardiovascular disease, insulin resistance, anemia, hyperlipidemia, metabolic syndrome, T2DM and cancer (18–20). Among the promising therapeutic strategies, it was recently demonstrated that melatonin, as the main product of the pineal gland, is considered a broad-spectrum antioxidant, can be applied in pathological conditions such as T2DM, mainly for its regulatory effects on the expression of the glucose transporter gene type 4 (GLUT4), glucose homeostasis and insulin sensitivity (21–23).
Another risk factor for night workers is a decrease in melatonin levels caused by exposure to artificial light during the work shift, a phenomenon associated with the risk of developing T2DM (24–28). The role of melatonin is mainly related to biological rhythms and the coordination of behavioral and physiological adaptations to the light–dark cycle, i.e., the hormone acts as an important regulator of allostasis (29). Cipolla-Neto et al. (30) suggested that supplementation or replacement could improve metabolic changes associated with reductions in serum melatonin levels, as occurs among night workers. Regarding glucose metabolism, a meta-analysis of 12 clinical trials showed that melatonin administration reduced fasting blood glucose, but had no influence on levels of glycated hemoglobin, insulin or insulin resistance (IR) (31). Subsequently, another meta-analysis with 16 studies showed positive results for the administration of melatonin on glucose metabolism, with a dose ranging between 3 and 10 mg for up to 24 weeks of duration (32).
Melatonin administration, given its action on mechanisms of glycemic homeostasis, inflammation, and energy metabolism (33–35), can represent a therapeutic and/or preventive alternative for metabolic alterations associated with night work. Recent research has demonstrated that the administration of 3 mg of melatonin in overweight individuals reduced circadian misalignment, especially among the most misaligned (earlier chronotype) and reduced body weight and body mass index (BMI), without changing caloric intake or participants’ physical activity levels (36, 37). Animal models supplemented with melatonin and subjected to circadian misalignment associated with a high-fat diet showed significant improvement in fasting glucose, oral glucose tolerance and inflammatory profile (38, 39). However, no studies investigating the effect of melatonin administration on DM markers based on dietary lipid profile have been conducted in humans, specifically among night workers.
Thus, the aim of the present study was to evaluate the effects of melatonin administration on DM risk markers (glucose, insulin, glycosylated hemoglobin and HOMA-IR), according to dietary lipid profile (pro-inflammatory versus anti-inflammatory) in excessive weight night workers. Therefore, the study hypothesis holds that melatonin administration improves diabetes risk markers in excessive weight night workers who have a diet of predominantly anti-inflammatory fats, and also decreases fat consumption.
2 Manuscript formatting
2.1 Study type
The present study is a randomized, controlled, double-blind, crossover clinical trial, evaluating the effect of melatonin on dietary lipid consumption and its influence on diabetes markers in night workers. The present project is part of a larger study, detailed in-formation on the original study is available from Marqueze et al. (36).
2.2 Population and sample
The participants of the present study were nursing professionals (nurses and nursing technicians) who worked permanent night shifts under a 12×36-hour system (12 h on, 36 h off) at a large private hospital in São Paulo, Brazil. The sample power was calculated a posteriori based on the test of difference of repeated measures (within-between interaction), an effect size of 0.25, alpha error of 5%, two groups (consumption and intervention), and three measures (baseline, melatonin, and placebo). Thus, the study population of 27 participants had a sample power of 80% (G*Power).
2.3 Inclusion and exclusion criteria
Subjects that met the following criteria were included in the study: women; aged 20–50 years; body mass index (BMI) ≥25 kg kg/m2 and < 40 kg/m2; working night shift for ≥6 months; who declared having no intention of following any restricted diets and starting new physical activities while participating in the study. Individuals that met the following criteria were excluded from the study: women who were pregnant, nursing, had infants aged <1 year; were experiencing the climacteric or menopause period; held a second night job; were in regular use of medications or dietary supplements that influence sleep, alertness or the circadian timing system (barbiturates, antidepressants, benzodiazepines, melatonin, ritalin, modafinil, sleep aids); had a past history of neurological or psychiatric illnesses, or drug and alcohol abuse; circadian or sleep disorders; presented metabolic problems (except participants with T2DM and treated dyslipidemias or using statins and anti-triglycerides); cardiovascular diseases (except treated systemic arterial hypertension); clinically-diagnosed inflammation and/or chronic infections; eating disorders (bulimia, anorexia); had anemia or had donated >400 mL of blood in the three months preceding the study; had undergone major surgery in the last six months prior to participating in the research.
2.4 Data collection and data processing
Initially, the human resources sector of the institution was contacted and provided a list of all nursing professionals. A total of 238 female professionals engaged in permanent night shifts under the 12×36-hour system were identified. Shortly after this process, the nursing professionals were contacted, informed about the study, and invited to undergo screening according to the study inclusion and exclusion criteria.
Pre-screening took place from February to April 2018 and was carried out individually at participants´ workplace during their shift. Those professionals who met the inclusion and exclusion criteria (n = 46) were invited to participate in the survey and specific dates were scheduled for baseline data collection.
The clinical trial was conducted from April 2018 to August 2019. It is important to mention that seasonality was not a limiting factor in the present study, given that the length of days and nights are almost equivalent in Brazil, resulting in a photoperiod close to 12 h per day (40). After the collection of initial data (baseline), participants were randomized into two groups, with 23 women allocated to the first group (Melatonin Group – GM) and 23 to the second group (Placebo Group – PG) for a 12-week period. In the second phase of this crossover study (lasting three months), volunteers allocated to the intervention group in the first phase switched over to the control group for the second phase and vice versa (control group subjects switched over to intervention group). In the second phase, 19 volunteers (41.3%) discontinued the study during the protocol because they had started a second night job, became pregnant, changed shifts, or quit their job. Although we did not perform intention-to-treat analysis, which may be a limitation of the study, our final sample met the number necessary for good sampling power (80%).
Sociodemographic characteristics, along with work and health-related aspects, were collected through self-administered questionnaires. Although questionnaires were completed by participants, a researcher was always available to clarify any doubts. All assessments took place at the participants´ workplace during their working hours, between 12:00 am and 05:00 am, according to the shift schedule provided by the institution. Assessments took place at baseline, in the last 10 days of the first phase, and in the last 10 days of the second phase, including the evaluation of biochemical parameters.
2.5 Protocol
Each participant followed the protocol for 25 weeks (12 weeks for intervention, 12 weeks for placebo, plus 1 week for baseline). The GM group used synthetic melatonin only on days off and between shifts, i.e., on days when they slept during the night. On night workdays, melatonin was not taken by the participants. All participants were instructed to take a fast-release 3 mg melatonin tablet (Aché Pharmaceutics®, Brazil), one hour before the desired time to go to sleep. Subjects filled out a diary with information on the time they took melatonin, as well as bedtime and waking times. It is important to mention that the melatonin administration has not been associated with adverse events to date; however, the volunteers were instructed to report any symptoms to the researchers so that the necessary referrals could be made, but no symptoms or discomfort were reported by the participants.
The PG group was instructed to take a placebo pill identical in appearance to the melatonin pill, receiving the same instructions for use as the intervention group. The placebo pill resembled melatonin but contained no active ingredient, exerting no effect on the body (gluten-free and lactose-free). The study was double-blind, where neither the participants nor the lead researcher was aware of whether the study subjects were part of the intervention group or the control group. Over the three months of each phase, participants took melatonin for an average of 45 days (SD 10.3 days) and placebo for 44.3 days (SD 8.2 days). The length of the study was 18 months, as not all participants started the protocol at the same time. The illustrated diagram of the study is presented in Figure 1. Marqueze et al. (36) present detailed information about the study protocol.
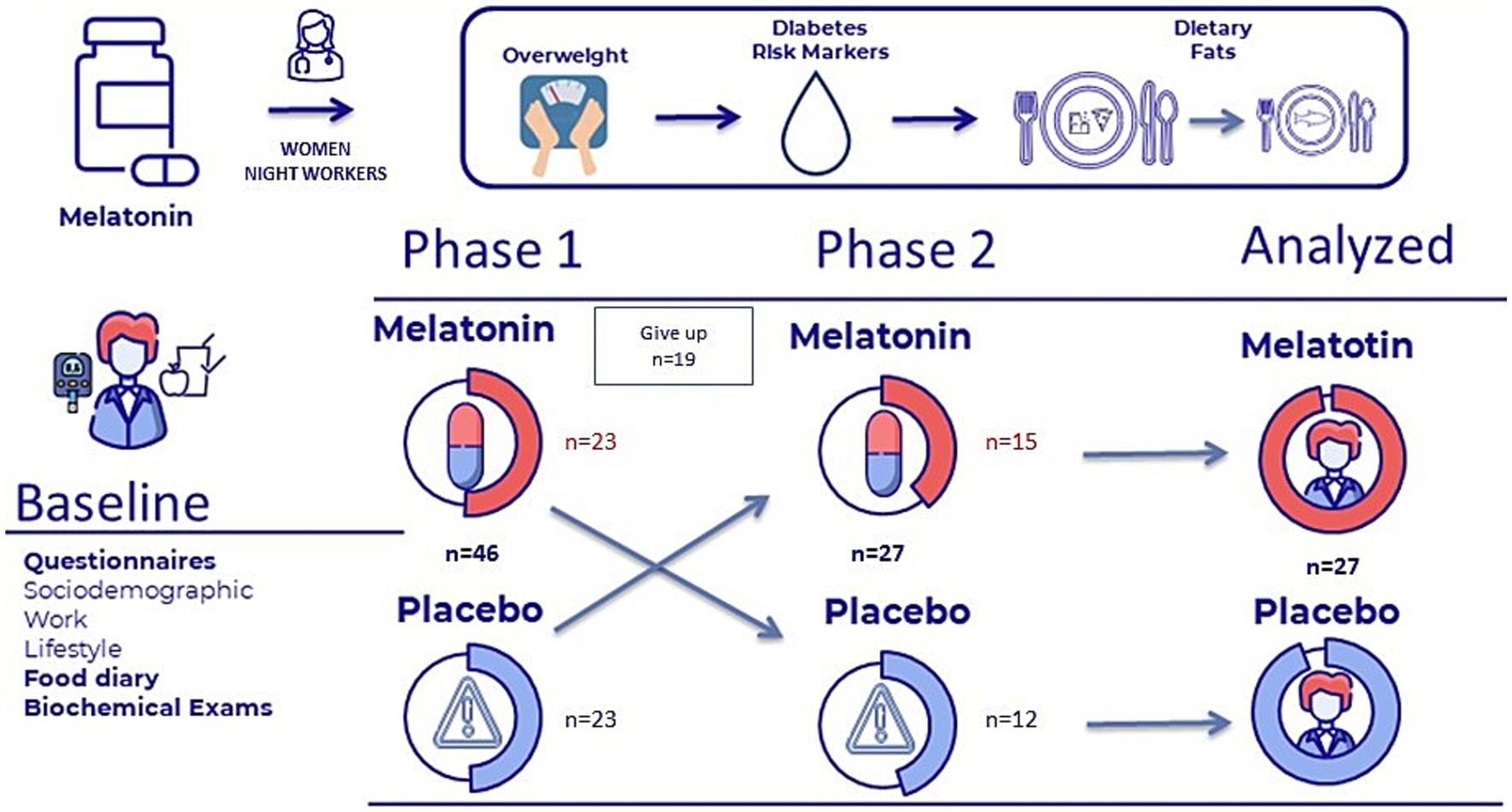
Figure 1. Illustrated diagram of the study.
2.6 Dietary assessment
Monthly, study participants kept food diaries on a typical working day and a typical day off (for a total period of 7 months, with the first evaluation completed before commencement of the protocol). The time window for recording this data was from 7:00 pm to 7:00 pm the following day, for both working days and days off. Food diaries are a good method for assessing dietary patterns (41), and one-day records have previously been used in other studies (42, 43). The evaluations were conducted by a duly trained nutritionist, under the supervision of the research coordinator. It is important to mention that the assessment of the dietary pattern (one working day and one day off) was first performed at baseline and again for every month of the protocol thereafter (at three-time points), totaling seven months and 14 days of food records. Importantly, participants had the option of a nutritionist-planned dinner provided by the hospital. In addition, all units had a pantry where they could store food brought in from outside the hospital and have meals.
The diaries were analyzed using the Nutrition Data System for Research (NDSR – United States Department of Agriculture – USDA), 2007 version. Due to cultural differences between Brazilian and North American food consumption (with the US serving as the reference for the NDSR), the composition of typical Brazilian foods and preparations was added based on the Brazilian Food Composition Table (44) and on specific processed food labels. Only two participants reported using dietary supplements, which were included in the assessment of food consumption, and there were no significant monthly differences in food intake.
The dietary lipid profile was determined based on saturated, monounsaturated and polyunsaturated fats, trans fats, cholesterol, eicosapentaenoic acid (EPA) + docosahexaenoic acid (DHA) and total fat (grams). The evaluation of the dietary lipid profile regarding DM markers was based on total fat (≥ 35% E) (45). The dietary fatty acid profile, according to inflammatory status, was attributed by tallying the average intake (grams) of dietary lipid recorded for working days and days off over the study period, i.e., at baseline and the end of the first and second phases (3 timepoints) and grouping these according to the following classification (46, 47).
1. Pro-inflammatories = saturated fats, trans fats and cholesterol;
2. Anti-inflammatories = monounsaturated and polyunsaturated fats, eico-spentaenoic acid (EPA) + docosahexaenoic acid (DHA).
The adequacy of the dietary pattern was estimated using the Dietary Reference Intakes (DRI) and in cases where these were not available, the Recommended Dietary Allowances (RDA), both established by the US National Academy of Sciences (45). Dietary profile was established based on: 1. Total caloric intake (kcal/day); 2. Carbohydrates (45-65%E); 3. Fats (20-35%E); 4. Proteins (10-35%E); and 5. Dietary fiber (14 g/1000 kcal) (45). For fat profile, the recommendations of the updated Brazilian Directive on Dyslipidemia and Prevention of Atherosclerosis – 2017 were used (48).
2.7 Risk markers for diabetes
For determination of plasma concentrations of blood glucose, insulin, glycosylated hemoglobin and HOMA-IR (Homeostasis Model Assessment of Insulin Resistance), blood collection was performed after a 12-h fast, before morning medication, with no consumption of alcoholic beverages the day before collection, and after a night’s sleep of at least six hours after the volunteers’ days off. Glycemic profile values were evaluated according to the criteria of the American Diabetes Association (49). The variables include the following criteria: blood glucose (≥100 mg/dL), insulin (≥23 ng/dL), glycosylated hemoglobin (≥5.7%) and HOMA-IR. The blood glucose and insulin values provided the basis for calculating the HOMA-IR index, using the formula: HOMA-IR = fasting glucose in mmol/l x fasting insulin in μU/mL/22.5 (50). According to the BRAMS study, a value of >2.71 was adopt-ed to identify IR in adults (51).
2.8 Study variables
The dependent variables of the study were the diabetes risk markers (glycemia, insulin, glycosylated hemoglobin and the HOMA-IR index) and the profile of dietary lipids (saturated, monounsaturated, polyunsaturated, trans, cholesterol, EPA + DHA) consumed by the participants during the intervention. The independent variable was the inflammatory profile of dietary lipids (pro-inflammatory or anti-inflammatory). The adjustment variables included age, BMI and total time working nights. The descriptive variables were age, education, job role at hospital, weekly working hours (hours/week), net income, smoking status, weekly physical activity time (where ≥150 min of moderate or intense leisure-time activity per week was defined as physically active) (52, 53), dietary profile (described in dietary assessment) and anthropometric data (weight and height) measured according to Lohman et al. (54). Body Mass Index (BMI) in kg/m2 was calculated from the measurements of weight (kg) and height (m). For the classification of BMI for adults, the criterion recommended by the WHO was adopted, where a value >24.99 kg/m2 indicates overweight (55).
2.9 Statistical analysis
The Shapiro–Wilk test was applied to test the normality of the quantitative variables. Parametric variables were expressed as mean and standard deviation (SD) or standard error (SE), while non-parametric variables were expressed as median and interquartile range-IQR (P25%–P75%). The Wilcoxon test was used to observe differences in fat consumption on days off and on working days.
The effects of melatonin administration on dietary lipid profile and DM markers according to the inflammatory profile of dietary lipids was assessed using a generalized linear model (GLM) with the LSD (Least Significant Difference) post hoc test for the test comparing 3 means (related samples) with two factors (intervention and dietary lipid pro-file). In all tests, a p-value <0.05 was considered significant. All data was analyzed using Statistica 12.0 and STATA 14.0 (Stata corp, Texas, United States) packages.
2.10 Ethical aspects
The project was approved by the Research Ethics Committee of the School of Public Health of the University of São Paulo (FSP-USP) (protocol no 2,450,682, December 20, 2017) and by the Ethics Board of the participating Hospital (protocol No. 2,489,636, February 7, 2018). The study was registered with the Brazilian Registry of Clinical Trials (RBR-6pncm9) and on the International Clinical Trials Registry Platform of the World Health Organization (UTN no U1111-1238-7395). Participants were guaranteed confidentiality and anonymity, and the study was only carried out after participants had a clear understanding of the objectives of the study and signed the Free and Informed Consent Form, which complied with Resolution 466/2012.
3 Results
At the end of data collection period, 27 volunteers had completed the intervention. Participants had a mean age of 37.1 years (SD 5.9 years, IQR 32.1–42.6 years) and mean BMI of 29.9 kg/m2 (SD 3.3 kg/m2), fifteen were overweight and twelve were obese. Mean time working at the hospital was 8.4 years (SD 4.4 years) and the median time working nights at the institution was 5.3 years (IQR 2–4 years). Most participants had attained postgraduate education, and more than half had an income >5,000 Brazilian reais (BRL) per month. For marital status, most participants reported having a partner (Table 1).
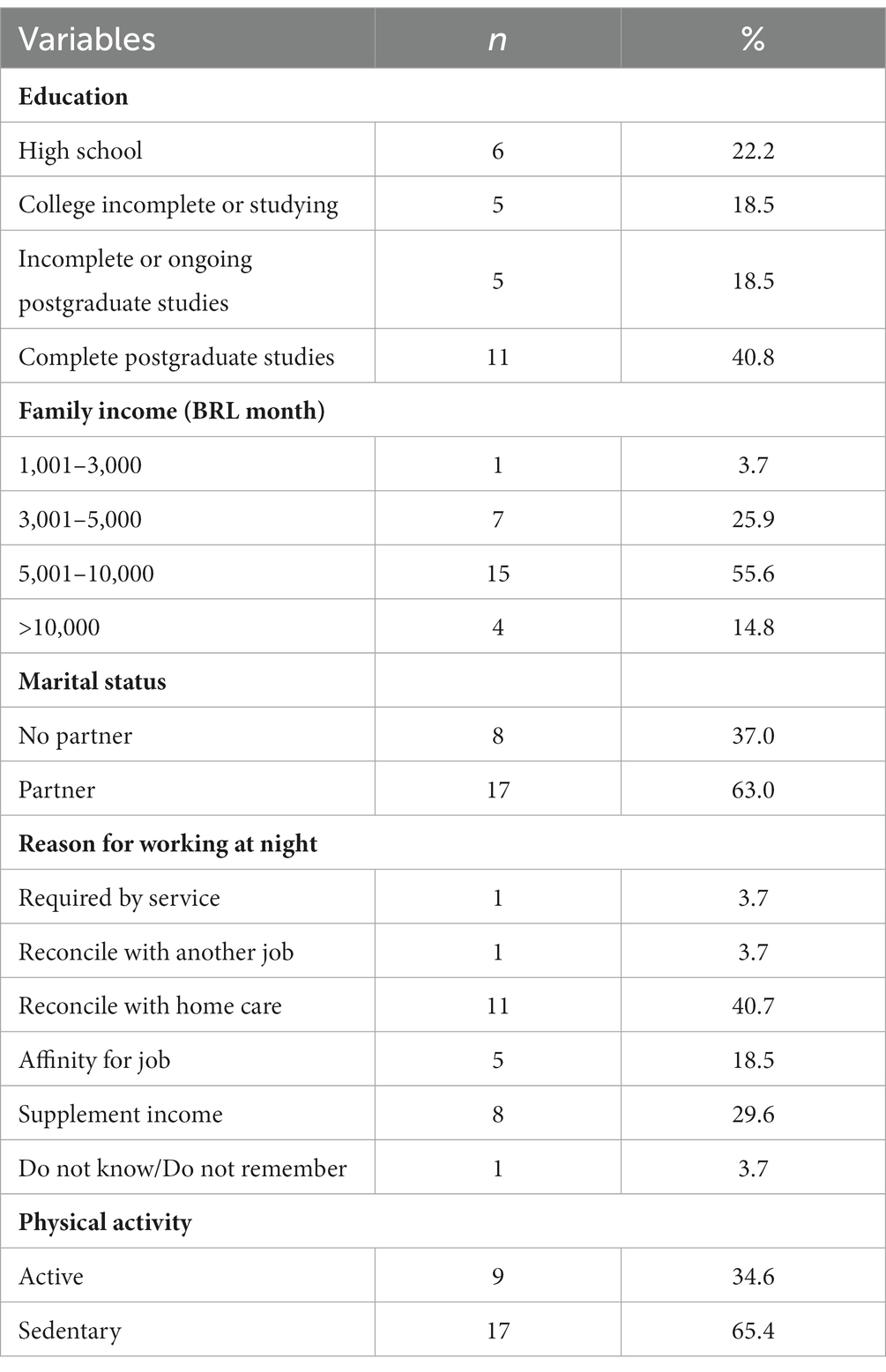
Table 1. Sociodemographic data of participants (n = 27).
Regarding the reasons for working nights, most volunteers chose this shift to reconcile work with home care. A sedentary lifestyle (< 150 min/week of moderate physical activity) was predominant among the study participants.
Participants had an average energy consumption of more than 1,500 kcal/day, and the distribution of macronutrients (carbohydrates, proteins, and lipids) was within recommended values. Regarding dietary fiber, the volunteers had low consumption at baseline. Mean dietary cholesterol intake was within recommended levels (Table 2).
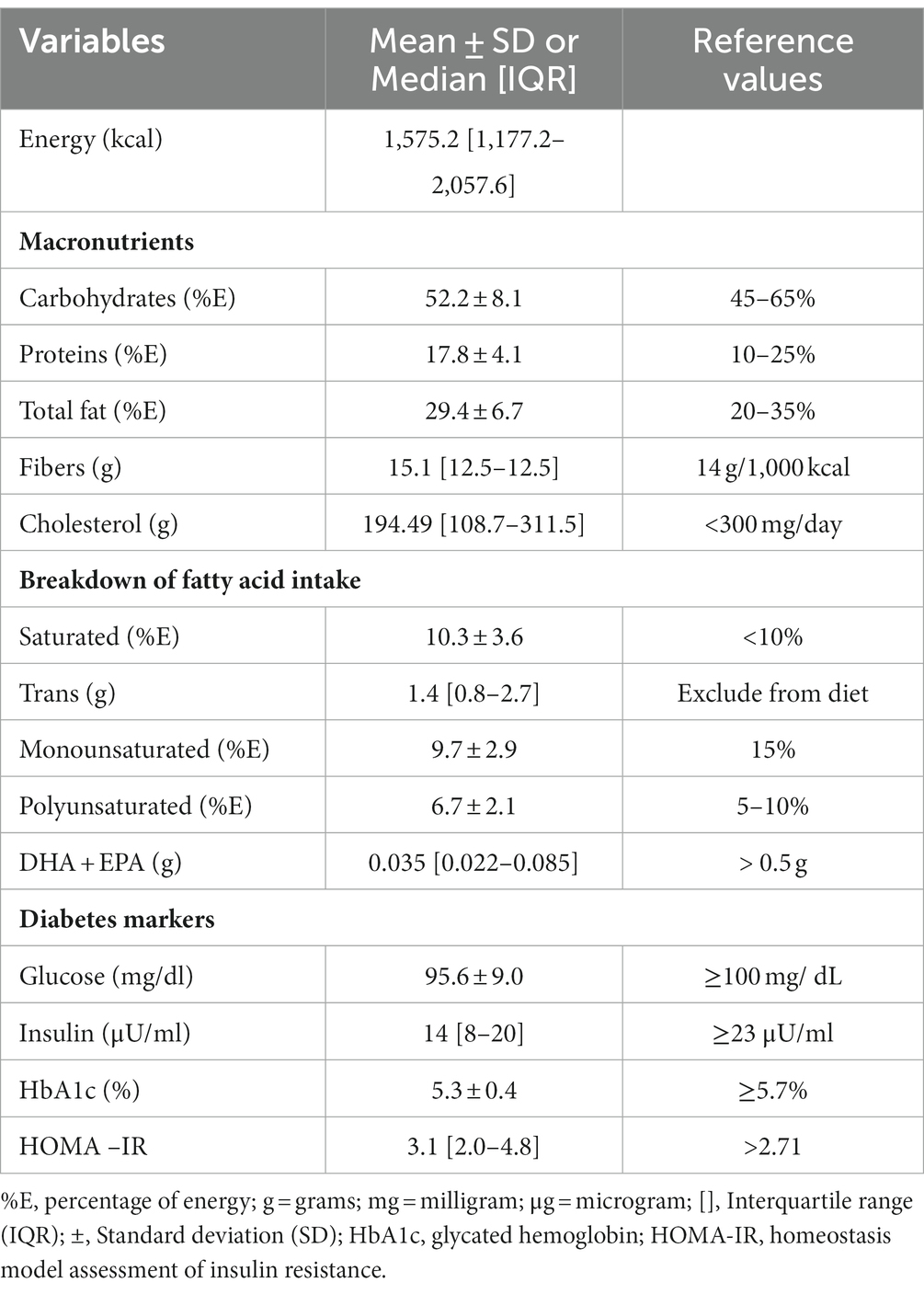
Table 2. Dietary pattern (average days off plus days at work) and diabetes markers at baseline of participants (n = 27).
Mean values for glycemia, insulin, and HbA1c were all within recommended reference ranges, but the mean HOMA-IR index was high (Table 2), and the presence of IR at baseline was detected in 17 (62.9%) volunteers. While none of the participants had values consistent with DM at baseline, 9 (33.3%) participants had glycemia indicative of pre-diabetes (≥100 mg/ dL).
Regarding total consumption of fats during the study, consumption levels of 81.5% of participants were within recommended ranges (20-35%E), with a median consumption of 56.4 g/day of fat (IQR 45.0–66.9 g/day). Notably, only four individuals had a high consumption of total fat (≥35%E) during the study period, but consumption of both saturated and trans fatty acids was high, whereas the intake of long-chain monounsaturated and polyunsaturated fatty acids was low (DHA + EPA) (Table 3).
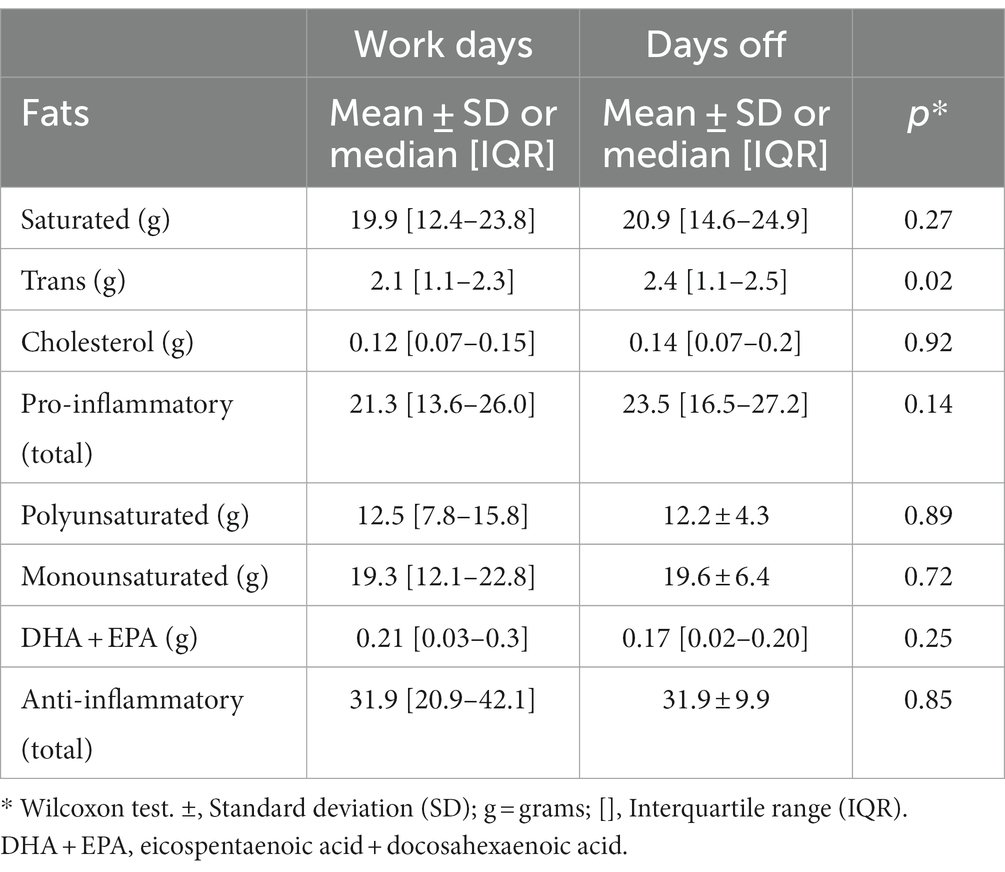
Table 3. Fat profile (mean of baseline, melatonin and placebo) on days off and work days of participants during study (n = 27).
The profile of fats consumed at each of the three timepoints is shown in Table 4. Results show that melatonin administration had no effect on the individual intake profile of each fat (saturated, trans, polyunsaturated, monounsaturated, EPA + DHA and cholesterol). For this evaluation, we chose not to separate consumption on days off and work because, as previously tested, we observed statistical differences only for saturated fat. Likewise, no effect on consumption was evident when grouped according to inflammatory characteristics or total fat (g).
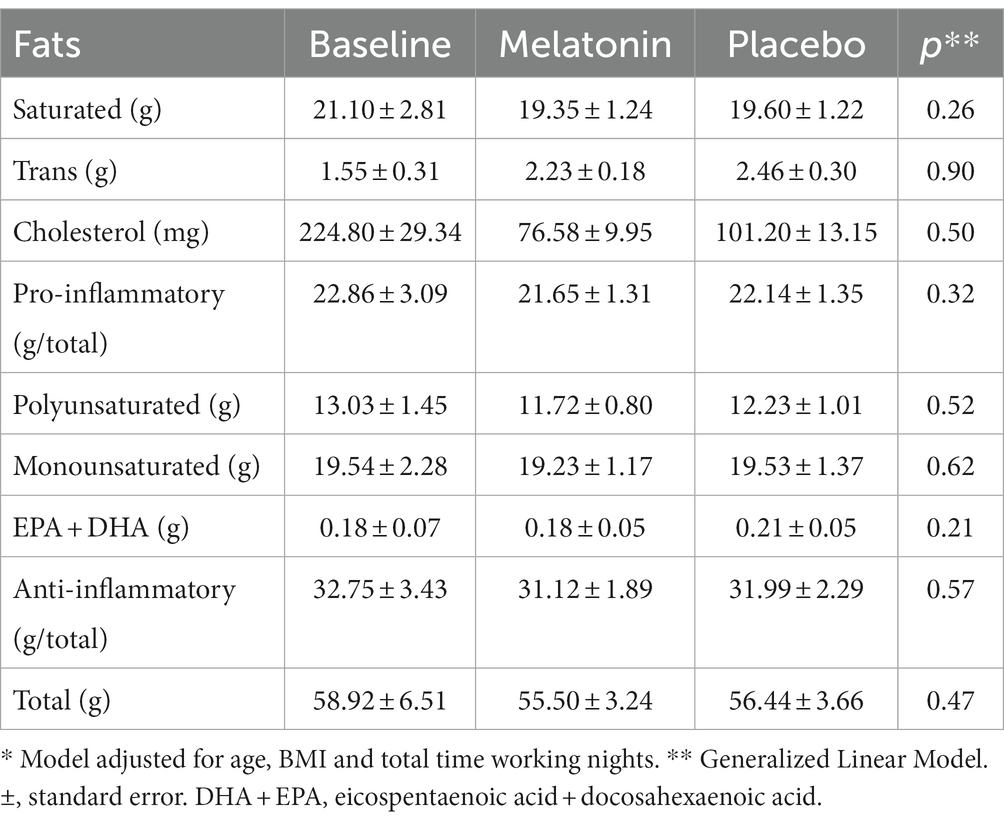
Table 4. Effect of melatonin administration on dietary lipid consumption profile of participants (n = 27)*.
Melatonin administration alone exerted no influence on the biochemical markers evaluated. Similarly, no effects of melatonin administration on level of total fat consumption, were found (Table 5). The assessment of fats dichotomized into pro-inflammatory and anti-inflammatory groups also showed no isolated effect on glycemic parameters or interaction with exogenous melatonin (Table 6).
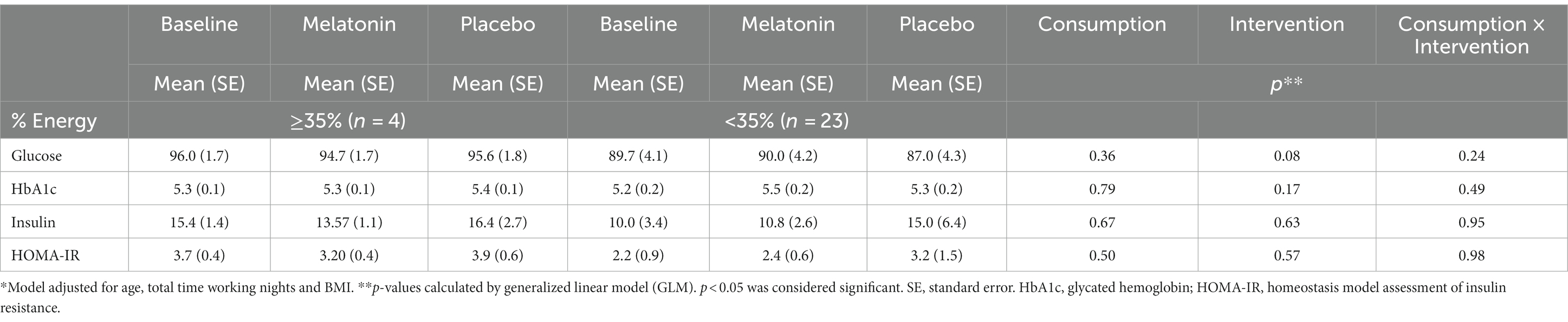
Table 5. Effect of melatonin on diabetes markers, according to consumption pattern, during intervention (mean baseline, melatonin and placebo) for total fats (%E) in excessive weight night workers (n = 27)*.
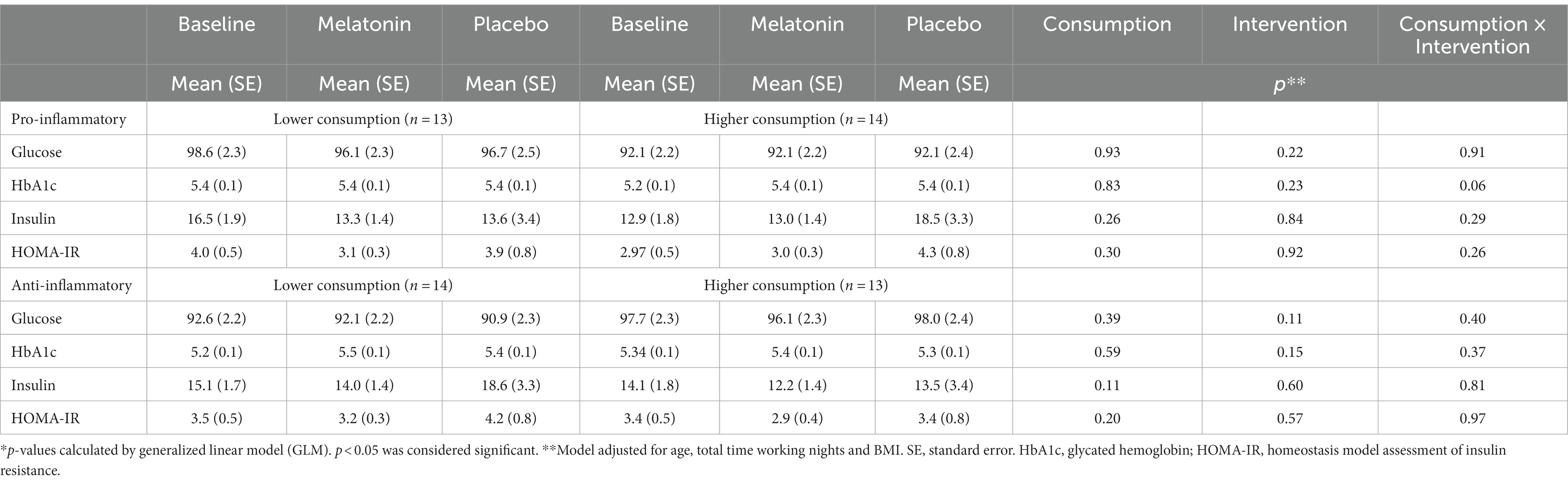
Table 6. Effect of melatonin on diabetes markers, according to consumption pattern, during intervention (mean baseline, melatonin and placebo) for pro-inflammatory (g) and anti-inflammatory (g) fats in excessive weight night workers (n = 27)*.
4 Discussion
In the present study, melatonin administration promoted no improvement in risk markers for diabetes, according to the inflammatory profile of dietary lipids in excessive weight night workers and exerted no effect on dietary lipid profile. Some studies involving animal and human models have shown positive results after melatonin administration in terms of blood glucose and insulin resistance under various conditions (56–58). However, there is a dearth of clinical trials involving night workers. In animal models with female guinea pigs that received 10 mg/kg of melatonin and 45% dietary lipid and were exposed 24 h a day to artificial light, administration significantly improved oral glucose tolerance (39). In another study, of mice without circadian misalignment that received 60% fat and were treated with melatonin, showed reduced fasting blood glucose (38). However, results of the present study failed to replicate these findings, where chronic circadian misalignment may have attenuated the effect of the intervention on common markers of glycemic homeostasis.
In another study, employing the same dose of melatonin administered in the present study (3 mg), Modabbernia et al. (58) supplemented 36 schizophrenic women (mean age 33 years) for eight weeks and observed no subsequent improvement in DM parameters (fasting glucose, insulin and HOMA-IR). By contrast, a meta-analysis by Delpino, Figueiredo and Nunes (32), nine out of the 15 studies showed a beneficial effect of melatonin on DM markers. Of the studies included in the analysis, two evaluated women only, with results showing improvement in insulin resistance and fasting glucose.
In the present study, it is important to consider the chronic circadian misalignment presented by the volunteers, who exhibited insulin resistance, even though their glucose and glycated hemoglobin levels were within the reference range. These factors might have prevented improvement in glucose intolerance and insulin resistance after melatonin administration (59, 60). To explain this effect, at the molecular level in Rizza et al. (61), night workers have a high REV-ERBα/BMAL1 mRNA ratio (possible chronic circadian misalignment due to exposure to prolonged artificial light) associated with a significant correlation between HbA1c and the expression of IL-1β RNA in leukocytes, even with values of glycemic parameters within reference standards, very common in low chronic inflammation associated with the risk of T2DM (61).
Regarding total fat consumption in the present study, despite not reaching statistical significance, there was a tendency towards a reduction or maintenance of fasting glucose, insulin, glycosylated hemoglobin and HOMA-IR, after melatonin administration in the presence of adequate consumption of total fat in the diet. This same pattern, however, was not observed in participants with inadequate consumption. This suggests a possible improvement in subclinical glucose tolerance, suppressed by the inflammatory status caused by the chronic misalignment inherent to chronic night work (62, 63).
Given the importance of the composition of dietary lipids in the pathophysiology of chronic diseases, especially T2DM, in the present study, fats consumed were dichotomized according to the characteristics of inflammatory responses (pro-inflammatory or anti-inflammatory), a well elucidated theory in the literature (64–66). Given the knowledge that night workers tend to have a more pro-inflammatory diet, the influence of the inflammatory profile of the fats present in the diet on melatonin response in the present study was explored (67, 68). However, no significant difference was found after dichotomizing dietary lipids regarding the pro-inflammatory factor. Explaining this effect, SFAs make up most of the pro-inflammatory component, and SFA ingestion is known to cause more marked lipemia than MUFAs or PUFAs, which can lead to a higher pro-inflammatory state exacerbated by low-grade inflammation and circadian misalignment (69–72).
Similarly, the amount of fats considered anti-inflammatory in the study proved unable to modify risk markers for DM following melatonin administration, even though blood glucose, insulin and HOMA-IR values were generally lower after administration. Consistent with the current study results, an isocaloric or ad libitum anti-inflammatory diet rich in mono and polyunsaturated fats (37% or 113 g of fat), with a saturated fat and cholesterol content below recommended levels, in individuals with DM and/or or pre-diabetes and obesity without circadian misalignment, was associated with a reduction in fasting blood glucose levels yet had no effect for insulin (73). On the other hand, in a controlled human model, exogenous melatonin alone influenced insulin sensitivity after a high-fat meal, with or without exposure to artificial light (62). This may explain the IR marker with higher values for placebo under all conditions in the present study.
The dietary profile found in the present study exhibits characteristics previously reported in the literature, demonstrating that night workers have more pro-inflammatory eating patterns compared to day workers, suggesting this may increase the risk of chronic diseases related to inflammation, such as DM (11, 74, 75).
Regarding the composition of fatty acids in the diet, consumption of saturated fat (%E) and trans fats by the study participants exceeded recommended levels, while low consumption of monounsaturated fatty acids and EPA + DHA was also observed, a profile commonly reported in studies assessing dietary intake among night workers (11, 12, 76, 77). Toward explaining this phenomenon, in the presence of circadian misalignment, the most palatable foods such as fats, act as potential zeitgebers, having a rapid direct effect on the orexigenic centers and regions associated with hedonic stimulation/reward, influencing food-seeking behaviour (7–9, 78).
In this context, fluctuations in fat consumption occurred among the night workers assessed, regardless of their job role. Since the volunteers in the present study performed half of the working days of the month at night, this variation in food consumption can be very common. Thus, Hemiö et al. (76) demonstrated that, among women at risk for DM, despite adequate fat consumption (≤35%), an increase of just one night shift was associated with an increase in total fat and saturated fat intake. Recently, plasma markers of lipid and liver function were found to have endogenous circadian rhythms that changed in response to a combined light and isocaloric meal schedule (27%E) (79). Although the authors did not assess glycemic regulation, this result may reinforce the importance of the present study, given that a specific macronutrient associated with glycemic dysregulation was investigated.
From this perspective, the composition of fatty acids and cholesterol in the diet is influenced by food choices, which in turn may be associated with circadian misalignment, leading to a greater preference for high-fat foods after night work. However, there is still no robust evidence on the relationship of melatonin administration with reduction in food consumption (6, 80).
The present study has several noteworthy strengths, including the assessment of the dietary profile every month throughout the intervention, the work in permanent shifts, i.e., the number of nights was the same among the participants, and also the fact that, to date, this is the only study that evaluates the influence of melatonin administration on DM risk markers in a double-blind randomized clinical trial under real-life conditions. The limitations of the study include the fact that the low dose may have influenced the expected results in the hypothesis, and individual adaptations to night work, circulating melatonin, and sleep assessments were not evaluated, factors that may have influenced the results. Although the study hypotheses were not confirmed, the insights discussed are important for future research investigating the influence of melatonin and fats considered anti- or pro-inflammatory on glucose and insulin homeostasis related to night work.
5 Conclusion
In summary, melatonin administration for 12 weeks had no effect on DM risk markers according to dietary lipids profile (pro-inflammatory or anti-inflammatory potential) in excessive weight night workers. Regarding fat consumption, melatonin administration promoted no change in consumption profile throughout the intervention for total fats, dichotomized into anti-inflammatory or pro-inflammatory types, or for isolated fats (saturated fat, trans fat, cholesterol, monounsaturated fat and EPA + DHA).
In the present study, the total consumption of anti-inflammatory fats was higher than pro-inflammatory fats, although a high consumption of saturated and trans-fat was evident and, in parallel, a low intake of monounsaturated and EPA + DHA. Therefore, given the originality of the topic addressed in the present study, future studies should be encouraged that involve a longer administration time, individualized doses, and possibly concomitant dietary prescription.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Research Ethics Committee of the School of Public Health of the University of São Paulo (FSP-USP) (protocol no 2,450,682, December 20, 2017) and by the Ethics Board of the participating Hospital (protocol no. 2,489,636, February 7, 2018). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
CS: Conceptualization, Formal analysis, Investigation, Methodology, Visualization, Writing – original draft, Writing – review & editing. LN: Conceptualization, Methodology, Supervision, Writing – original draft, Writing – review & editing. JC-N: Conceptualization, Project administration, Validation, Visualization, Writing – review & editing. CM: Conceptualization, Methodology, Validation, Visualization, Writing – review & editing. EM: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was supported by the Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP) (grant numbers 2014/50457–0, 2018/09704–4, 2019/03624–1, 2019/24327–5); Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) (grant numbers 150781/2017–2, 144800/2018–7, 118087/2019–3); and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) (grant numbers 88887.356981/2019–00, 88887.150178/2017–00).
Acknowledgments
The authors thank all study participants for their voluntary participation in this study. In addition, our sincere thanks to the hospital where the research took place, the funding agencies and the chronobiology and sleep group (GECS) associated with the Catholic University of Santos involved in the larger project of this research.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Ulhôa, MA , Marqueze, EC , Burgos, LGA , and Moreno, CRC . Shift work and endocrine disorders. Int J Endocrinol. (2015) 2015:1–11. doi: 10.1155/2015/826249
2. Rüger, M , and Scheer, F . Effects of circadian disruption on the cardiometabolic system. Rev Endocr Metab Disord. (2009) 10:245–60. doi: 10.1007/s11154-009-9122-8
3. Gan, Y , Yang, C , Tong, X , Sun, H , Cong, Y , Yin, X, et al. Shift work and diabetes mellitus: a meta-analysis of observational studies. Occup Environ Med. (2015) 72:72–8. doi: 10.1136/oemed-2014-102150
4. Silva-Costa, A , Rotenberg, L , Nobre, AA , Schmidt, MI , Chor, D , and Griep, RH . Gender-specific association between night-work exposure and type-2 diabetes: results from longitudinal study of adult health, ELSA-Brasil. Scand J Work Environ Health. (2015) 41:569–78. doi: 10.5271/sjweh.3520
5. Kim, SM , Neuendorff, N , and Earnest, DJ . Role of proinflammatory cytokines in feedback modulation of circadian clock gene rhythms by saturated fatty acids. Sci Rep. (2019) 9:1–9. doi: 10.1038/s41598-019-45322-9
6. Cain, SW , Filtness, AJ , Phillips, CL , and Anderson, C . Enhanced preference for high-fat foods following a simulated night shift. Scand J Work Environ Health. (2015) 41:288–93. doi: 10.5271/sjweh.3486
7. Webb, IC , Lehman, MN , and Coolen, LM . Diurnal and circadian regulation of reward-related neurophysiology and behavior. Physiol Behav. (2015) 143:58–69. doi: 10.1016/j.physbeh.2015.02.034
8. Blancas-Velazquez, A , Mendoza, J , Garcia, AN , and La Fleur, SE . Diet-induced obesity and circadian disruption of feeding behavior. Front Neurosci. (2017) 11:23. doi: 10.3389/fnins.2017.00023
9. Pickel, L , and Sung, H . Feeding rhythms and the circadian regulation of metabolism. Front Nutr. (2020) 7:7. doi: 10.3389/fnut.2020.00039
10. Panda, S . Circadian physiology of metabolism. Science. (2016) 354:1008–15. doi: 10.1126/science.aah4967
11. Heath, G , Coates, A , Sargent, C , and Dorrian, J . Sleep duration and chronic fatigue are differently associated with the dietary profile of shift workers. Nutrients. (2016) 8:771. doi: 10.3390/nu8120771
12. Hemiö, K , Puttonen, S , Viitasalo, K , Härmä, M , Peltonen, M , and Lindström, J . Food and nutrient intake among workers with different shift systems. Occup Environ Med. (2015) 72:513–20. doi: 10.1136/oemed-2014-102624
13. de Assis, MAA , Kupek, E , Nahas, MV , and Bellisle, F . Food intake and circadian rhythms in shift workers with a high workload. Appetite. (2003) 40:175–83. doi: 10.1016/S0195-6663(02)00133-2
14. Brondel, L , Romer, MA , Nougues, PM , Touyarou, P , and Davenne, D . Acute partial sleep deprivation increases food intake in healthy men. Am J Clin Nutr. (2010) 91:1550–9. doi: 10.3945/ajcn.2009.28523
15. Shoelson, SE , Lee, J , and Goldfine, AB . Inflammation and insulin resistance. J Clin Invest. (1793-1801) 116:1793–801. doi: 10.1172/JCI29069
16. Spiegel, K , Tasali, E , Penev, P , and Cauter, EV . Brief communication: sleep curtailment in healthy young men is associated with decreased leptin levels, elevated ghrelin levels, and increased hunger and appetite. Ann Intern Med. (2004) 141:846–50. doi: 10.7326/0003-4819-141-11-200412070-00008
17. Antunes, LDC , Levandovski, R , Dantas, G , Caumo, W , and Hidalgo, MP . Obesity and shift work: chronobiological aspects. Nutr Res Rev. (2010) 23:155–68. doi: 10.1017/S0954422410000016
18. Lee, Y , Kim, M , Choi, K , Kim, J , Bae, W , Kim, S, et al. Relationship between inflammation biomarkers, antioxidant vitamins, and bone mineral density in patients with metabolic syndrome. Nutr Res Pract. (2011) 5:150–6. doi: 10.4162/nrp.2011.5.2.150
19. Fritsche, KL . The science of fatty acids and inflammation. Adv Nutr. (2015) 6:293S–301S. doi: 10.3945/an.114.006940
20. Corrêa, TAF , Quintanilha, BJ , Norde, MM , Pinhel, MAS , Nonino, CB , and Rogero, MM . Nutritional genomics, inflammation and obesity. Arch Endocrinol Metab. (2020) 64:205–22. doi: 10.20945/2359-3997000000255
21. Pourhanifeh, MH , Hosseinzadeh, A , Dehdashtian, E , Hemati, K , and Mehrzadi, S . Melatonin: new insights on its therapeutic properties in diabetic complications. Diabetol Metab Syndr. (2020) 12:30. doi: 10.1186/s13098-020-00537-z
22. Genario, R , Cipolla-Neto, J , Bueno, AA , and Santos, HOS . Melatonin supplementation in the management of obesity and obesity-associated disorders: a review of physiological mechanisms and clinical applications. Pharmacol Res. (2021) 163:105254. doi: 10.1016/j.phrs.2020.105254
23. Zarezadeh, M , Barzegari, M , Aghapour, B , Adeli, S , Khademi, F , Musazadeh, V, et al. Melatonin effectiveness in amelioration of oxidative stress and strengthening of antioxidant defense system: findings from a systematic review and dose-response Meta-analysis of controlled clinical trials. Clin Nutr ESPEN. (2022) 48:109–20. doi: 10.1016/j.clnesp.2022.01.038
24. Moreno, CRC , Marqueze, EC , Sargent, C , Wright, KP Jr, Ferguson, SA , and Tucker, P . Working time society consensus statements: evidence-based effects of shift work on physical and mental health. Ind Health. (2019) 57:139–57. doi: 10.2486/indhealth.SW-1
25. Hunter, CM , and Figueiro, MG . Measuring light at night and melatonin levels in shift workers: a review of the literature. Biol Res Nurs. (2017) 19:365–74. doi: 10.1177/1099800417714069
26. Vetter, C , Dashti, HS , Lane, JM , Anderson, SG , Schernhammer, ES , Rutter, MK, et al. Night shift work, genetic risk, and type 2 diabetes in the UK biobank. Diabetes Care. (2018) 41:762–9. doi: 10.2337/dc17-1933
27. Amaral, FGD , Andrade-Silva, J , Kuwabara, WM , and Cipolla-Neto, J . New insights into the function of melatonin and its role in metabolic disturbances. Expert Rev Endocrinol Metab. (2019) 14:293–300. doi: 10.1080/17446651.2019.1631158
28. Wei, T , Li, C , Heng, Y , Gao, X , Zhang, G , Wang, H, et al. Association between night-shift work and level of melatonin: systematic review and meta-analysis. Sleep Med. (2020) 75:502–9. doi: 10.1016/j.sleep.2020.09.018
29. Cipolla-Neto, J , and Amaral, FGD . Melatonin as a hormone: new physiological and clinical insights. Endocr Rev. (2018) 39:990–1028. doi: 10.1210/er.2018-00084
30. Cippolla-Neto, J , Amaral, FG , Afeche, SC , Tan, DX , and Reiter, RJ . Melatonin, energy metabolism, and obesity. J Pineal Res. (2014) 56:371–81. doi: 10.1111/jpi.12137
31. Doosti-Irani, A , Ostadmohammadi, V , Mirhosseini, N , Mansournia, MA , Reiter, RJ , Kashanian, M, et al. The effects of melatonin supplementation on glycemic control: a systematic review and meta-analysis of randomized controlled trials. Horm Metab Res. (2018) 50:783–90. doi: 10.1055/a-0752-8462
32. Delpino, FM , Figueiredo, LM , and Nunes, BP . Effects of melatonin supplementation on diabetes: a systematic review and meta-analysis of randomized clinical trials. Clin Nutr. (2021) 40:4595–605. doi: 10.1016/j.clnu.2021.06.007
33. Koopman, ADM , Rauh, SP , Van’t Riet, E , Groeneveld, L , Van Der Heijden, AA , Elders, PJ, et al. The association between social jetlag, the metabolic syndrome, and type 2 diabetes mellitus in the general population: the new Hoorn study. J Biol Rhythm. (2017) 32:359–68. doi: 10.1177/0748730417713572
34. Javeed, N , and Matveyenko, AV . Circadian etiology of type 2 diabetes mellitus. Physiology. (2018) 33:138–50. doi: 10.1152/physiol.00003.2018
35. Hong, F , Pan, S , Xu, P , Xue, T , Wang, J , Guo, Y, et al. Melatonin orchestrates lipid homeostasis through the hepatointestinal circadian clock and microbiota during constant light exposure. Cell. (2020) 9:489. doi: 10.3390/cells9020489
36. Marqueze, EC , Nogueira, LFR , Vetter, C , Skene, DJ , Cipolla-Neto, J , and Moreno, CRC . Exogenous melatonin decreases circadian misalignment and body weight among early types. J Pineal Res. (2021) 71:e12750. doi: 10.1111/jpi.12750
37. Mohammadi, S , Rastmanesh, R , Jahangir, F , Amiri, Z , Djafarian, K , Mohsenpour, MA, et al. Melatonin supplementation and anthropometric indices: a randomized double-blind controlled clinical trial. Biomed Res Int. (2021) 2021:3502325–9. doi: 10.1155/2021/3502325
38. Sun, H , Wang, X , Chen, J , Song, K , Gusdon, AM , Li, L, et al. Melatonin improves non-alcoholic fatty liver disease via MAPK-JNK/P38 signaling in high-fat-diet-induced obese mice. Lipids Health Dis. (2016) 15:202–8. doi: 10.1186/s12944-016-0370-9
39. Liu, W , Zhang, Y , Chen, Q , Liu, S , Xu, W , Shang, W, et al. Melatonin alleviates glucose and lipid metabolism disorders in guinea pigs caused by different artificial light rhythms. J Diabetes Res. (2020) 2020:1–16. doi: 10.1155/2020/4927403
40. Moreno, C , Vasconcelos, S , Marqueze, E , Lowden, A , Middleton, B , Fischer, F, et al. Sleep patterns in Amazon rubber tappers with and without electric light at home. Sci Rep. (2015) 5:14074. doi: 10.1038/srep14074
41. Fisberg, RM , Marchioni, DML , and Colucci, ACA . Avaliação do consumo alimentar e da ingestão de nutrientes na prática clínica. Arq Bras Endocrinol Metabol. (2007) 53:617–24. doi: 10.1590/S0004-27302009000500014
42. Slimani, N , Kaaks, R , Ferrari, P , Casagrande, C , Clavel-Chapelon, F , Lotze, G, et al. European prospective investigation into Cancer and nutrition (EPIC) calibration study: rationale, design and population characteristics. Public Health Nutr. (2007) 5:1125–45. doi: 10.1079/PHN2002395
43. Mota, MC , Silva, CM , Balieiro, LCT , Fahmy, WM , Marqueze, EC , Moreno, CRC, et al. Social jetlag is associated with impaired metabolic control during a 1-year follow-up. Front Physiol. (2021) 12:1346. doi: 10.3389/fphys.2021.702769
44. TACO/NEPA-UNICAMP . Tabela brasileira de Composição de Alimentos, 4ªedição. rev. e ampl. Campinas, SP: NEPA-UNICAMP (2011).
45. Trumbo, P , Schlicker, S , Yates, AA , and Poos, M . Food and Nutrition Board of the Institute of Medicine, The National Academies. Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein and amino acids. J. Am. Diet. Assoc. (2002). 102, 1621–1631. doi: 10.1016/s0002-8223(02)90346-9
46. Calder, PC , Ahluwalia, N , Brouns, F , Buetler, T , Clement, K , Cunningham, K, et al. Dietary factors and low-grade inflammation in relation to overweight and obesity. Br J Nutr. (2011) 106:S5–S78. doi: 10.1017/S0007114511005460
47. Basu, A , Devaraj, S , and Jialal, I . Dietary factors that promote or retard inflammation. Arterioscler Thromb Vasc Biol. (2006) 26:995–1001. doi: 10.1161/01.ATV.0000214295.86079.dl
48. Faludi, AA , Izar, MCDO , Saraiva, JFK , Chacra, APM , Bianco, HT , Afiune, A, et al. Atualização da diretriz brasileira de dislipidemias e prevenção da aterosclerose–2017. Arq Bras Cardiol. (2017) 109:1–76. doi: 10.5935/abc.20170121
49. American Diabetes Association . 2. Classification and diagnosis of diabetes: standards of medical Care in Diabetes—2020. Diabetes Care. (2020) 43:s14–31. doi: 10.2337/dc20-S002
50. Matthews, DR , Hosker, JP , Rudenski, AS , Naylor, BA , Treacher, DF , and Turner, RC . Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. (1985) 28:412–9. doi: 10.1007/BF00280883
51. Geloneze, B , Vasques, AC , Stabe, CF , Pareja, JC , Rosado, LE , Queiroz, EC, et al. HOMA1-IR and HOMA2-IR indexes in identifying insulin resistance and metabolic syndrome: Brazilian metabolic syndrome study (BRAMS). Arq Bras Endocrinol Metabol. (2009) 53:281–7. doi: 10.1590/s0004-27302009000200020
52. World Health Organization—WHO . The World health report 2002: Reducing risks, promoting healthy life. World Health Organization, (2002). Available at:https://www.who.int/publications-detail-redirect/9241562072.
53. Pate, R , Pratt, M , Blair, S , Haskell, WMC , Bouchard, C , and King, AC . Physical activity and public health. A recommendation from the Centers for Disease Control and Prevention and the American College of Sports Medicine. JAMA. (2005) 273:402–7. doi: 10.1001/jama.273.5.402
54. Lohman, TG , Roche, AF , and Martorell, R . Anthropometric standardization reference manual, 1 st edition. Estados Unidos: Human Kinetics Books (1988).
55. World Health Organization—WHO . Physical status: The use and interpretation of anthropometry. Technical report series 854: Geneva, WHO: (1995). Disponível em: https://pubmed.ncbi.nlm.nih.gov/8594834/.
56. Peschke, E , Schucht, E , and Mühlbauer, E . Long-term enteral administration of melatonin reduces plasma insulin and increases expression of pineal insulin receptors in both Wistar and type 2-diabetic Goto-Kakizaki rats. J Pineal Res. (2010) 49:373–81. doi: 10.1111/j.1600-079X.2010.00804.x
57. Leite, EA , Gomes, PRL , Vilas-Boas, EA , Munhoz, AC , Motta-Teixeira, LC , Júnior, JSS, et al. A combination of melatonin and moderate-intensity aerobic exercise improves pancreatic beta-cell function and glycemic homeostasis in type 2 diabetic model of animals. Melatonin Res. (2021) 4:479–94. doi: 10.32794/mr112500106
58. Modabbernia, A , Heidari, P , Soleimani, R , Sobhani, A , Roshan, ZA , Taslimi, S, et al. Melatonin for prevention of metabolic side-effects of olanzapine in patients with first-episode schizophrenia: randomized double-blind placebo-controlled study. J Psychiatr Res. (2014) 53:133–40. doi: 10.1016/j.jpsychires.2014.02.013
59. Sharma, A , Laurenti, MC , Dalla Man, C , Varghese, RT , Cobelli, C , Rizza, RA, et al. Glucose metabolism during rotational shift-work in healthcare workers. Diabetologia. (2017) 60:1483–90. doi: 10.1007/s00125-017-4317-0
60. Sharma, S , Singh, H , Ahmad, N , Mishra, P , and Tiwari, A . The role of melatonin in diabetes: therapeutic implications. Arch Endocrinol Metab. (2015) 59:391–9. doi: 10.1590/2359-3997000000098
61. Rizza, S , Luzi, A , Mavilio, M , Ballanti, M , Massimi, A , Porzio, O, et al. Alterations in rev-ERBα/BMAL1 ratio and glycated hemoglobin in rotating shift workers: the EuRhythDia study. Acta Diabetol. (2021) 58:1111–7. doi: 10.1007/s00592-021-01676-z
62. Albreiki, MS , Middleton, B , and Hampton, SM . The effect of melatonin on glucose tolerance, insulin sensitivity and lipid profiles after a late evening meal in healthy young males. J Pineal Res. (2021) 71:e12770. doi: 10.1111/jpi.12770
63. Oladele, CA , Akintayo, CO , Badejogbin, OC , Oniyide, AA , Omoaghe, AO , Agunbiade, TB, et al. Melatonin ameliorates endocrine dysfunction and defective sperm integrity associated with high-fat diet-induced obesity in male Wistar rats. Andrologia. (2022) 54:e14242. doi: 10.1111/and.14242
64. Klein-Platat, C , Drai, J , Oujaa, M , Schlienger, JL , and Simon, C . Plasma fatty acid composition is associated with the metabolic syndrome and low-grade inflammation in overweight adolescents. Am J Clin Nutr. (2005) 82:1178–84. doi: 10.1093/ajcn/82.6.1178
65. Ravaut, G , Légiot, A , Bergeron, KF , and Mounier, C . Monounsaturated fatty acids in obesity-related inflammation. Int J Mol Sci. (2020) 22:330. doi: 10.3390/ijms22010330
66. Hariharan, R , Odjidja, EN , Scott, D , Shivappa, N , Hébert, JR , Hodge, A, et al. The dietary inflammatory index, obesity, type 2 diabetes, and cardiovascular risk factors and diseases. Obes Rev. (2022) 23:e13349. doi: 10.1111/obr.13349
67. Khazrai, YM , Defeudis, G , and Pozzilli, P . Effect of diet on type 2 diabetes mellitus: a review. Diabetes Metab Res Rev. (2014) 30:24–33. doi: 10.1002/dmrr.2515
68. Acosta-Montaño, P , and García-González, V . Effects of dietary fatty acids in pancreatic Beta cell metabolism, Implications in Homeostasis. Nutrients. (2018) 10:393. doi: 10.3390/nu10040393
69. Villegas, R , Salim, A , Flynn, A , and Perry, IJ . Prudent diet and the risk of insulin resistance. Nutr Metab Cardiovasc Dis. (2004) 14:334–43. doi: 10.1016/s0939-4753(04)80023-1
70. Botham, KM , and Wheeler-Jones, CP . Postprandial lipoproteins and the molecular regulation of vascular homeostasis. Prog Lipid Res. (2013) 52:446–64. doi: 10.1016/j.plipres.2013.06.001
71. Wright, KP Jr, Drake, AL , Frey, DJ , Fleshner, M , Desouza, CA , Gronfier, C, et al. Influence of sleep deprivation and circadian misalignment on cortisol, inflammatory markers, and cytokine balance. Brain Behav Immun. (2015) 47:24–34. doi: 10.1016/j.bbi.2015.01.004
72. Goldfine, AB , and Shoelson, SE . Therapeutic approaches targeting inflammation for diabetes and associated cardiovascular risk. J Clin Invest. (2017) 127:83–93. doi: 10.1172/JCI88884
73. Zwickey, H , Horgan, A , Hanes, D , Schiffke, H , Moore, A , Wahbeh, H, et al. Effect of the anti-inflammatory diet in people with diabetes and pre-diabetes: a randomized controlled feeding study. J Restor Med. (2019) 8:e20190107. doi: 10.14200/jrm.2019.0107
74. Wirth, MD , Burch, J , Shivappa, N , Steck, SE , Hurley, TG , Vena, JE, et al. Dietary inflammatory index scores differ by shift work status: NHANES 2005 to 2010. J Occup Environ Med. (2014) 56:145–8. doi: 10.1097/JOM.0000000000000088
75. Pan, A , Schernhammer, ES , Sun, Q , and Hu, FB . Rotating night shift work and risk of type 2 diabetes: two prospective cohort studies in women. PLoS Med. (2018) 8:e1001141. doi: 10.1371/journal.pmed.1001141
76. Hemiö, K , Lindström, J , Peltonen, M , Härmä, M , Viitasalo, K , and Puttonen, S . The association of work stress and night work with nutrient intake–a prospective cohort study. Scand J Work Environ Health. (2020) 46:533. doi: 10.5271/sjweh.3899
77. Peplonska, B , Kaluzny, P , and Trafalska, E . Rotating night shift work and nutrition of nurses and midwives. Chronobiol Int. (2019) 36:945–54. doi: 10.1080/07420528.2019.1602051
78. Frank, S , Gonzalez, K , Lee-Ang, L , Young, MC , Tamez, M , and Mattei, J . Diet and sleep physiology: public health and clinical implications. Front Neurol. (2017) 8:393. doi: 10.3389/fneur.2017.00393
79. Kent, BA , Rahman, SA , St Hilaire, MA , Grant, LK , Rüger, M , Czeisler, CA, et al. Circadian lipid and hepatic protein rhythms shift with a phase response curve different than melatonin. Nat Commun. (2022) 13:681–7. doi: 10.1038/s41467-022-28308-6
Keywords: fat, melatonin, circadian misalignment, night work, diabetes
Citation: de Sousa CAR, Nogueira LF, Cipolla-Neto J, Moreno CRdC and Marqueze EC (2024) 12-week melatonin administration had no effect on diabetes risk markers and fat intake in overweight women night workers. Front. Nutr. 11:1285398. doi: 10.3389/fnut.2024.1285398
Edited by:
Johnni Hansen, Danish Cancer Society Research Center (DCRC), DenmarkReviewed by:
Reza Rastmanesh, American Physical Society, United StatesBeata Peplonska, Nofer Institute of Occupational Medicine, Poland
Copyright © 2024 de Sousa, Nogueira, Cipolla-Neto, Moreno and Marqueze. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Elaine Cristina Marqueze, ZWNtYXJxdWV6ZUBnbWFpbC5jb20=