 Eskezyiaw Agedew
Eskezyiaw Agedew Zeweter Abebe
Zeweter Abebe Abebe Ayelign
Abebe Ayelign
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr. , 02 November 2023
Sec. Nutritional Epidemiology
Volume 10 - 2023 | https://doi.org/10.3389/fnut.2023.1274406
This article is part of the Research Topic Nutrition and Sustainable Development Goal 2: Zero Hunger View all 24 articles
Introduction: Dietary pattern analysis allows us to characterize the dietary intakes of individuals rather than nutrient intake data and strongly predicts disease risks. The relationship between food intake and adolescents’ nutritional health is not well understood yet. Therefore, this study aimed to generate evidence for context-specific dietary intervention for adolescents.
Objective: This study aimed to determine dietary patterns and their relationship with nutritional outcomes and identify the contributing factors among adolescents in the Agrarian Community of Northwest Ethiopia.
Methods: A cross-sectional survey was conducted among 622 randomly selected adolescents. Dietary data were collected over a 1-week recall period using the Food Frequency Questionnaire (FFQ). After testing the basic assumptions, an exploratory factor analysis was conducted to determine the dietary patterns. Anthropometric data on weight and height were collected to determine the nutritional status using WHO Anthroplus 2010 software. A chi-square test was conducted to evaluate the effect of different dietary patterns on nutritional outcomes. A multivariable binary logistic regression model was used to identify factors affecting the dietary patterns of adolescents.
Result: Three types of dietary patterns, namely, traditional, mixed, and animal-source foods with traditional alcoholic beverage consumption were identified. These dietary patterns explain 58.64% of the variance in adolescent diet in the study setting. The burden of stunting was 15.12% vs. 11.21, 19.40% vs. 6.94, and 8.36% vs.17.97% among adolescents with lower traditional, mixed, and higher animal sources with alcoholic dietary pattern consumption habits, respectively (value of p <0.05). Adolescents who resided in low-land agroecology (AOR = 2.44; 95% CL: 1.24, 4.81) and had access to animal-source foods (AOR = 1.64; 95% CI: 1.04, 2.60) were associated with lower consumption of traditional dietary patterns. Similarly, adolescents who resided in low-land (AOR = 1.80; 95% CI: 1.18, 2.74) had formal education (AOR = 2.38; 95% CI: 1.35, 4.19) and had poor nutrition knowledge (AOR = 2.83; 95% CL: 1.55, 5.19) were associated with lower consumption of mixed dietary patterns. Moreover, adolescents residing in the high-land (AOR = 2.50; 95% CI: 1.37, 4.56) and being female (AOR =1.87; 95% CI: 1.27, 2.74) were significant factors associated with lower consumption of animal-sourced foods with traditional alcoholic beverage consumption patterns.
Conclusion: Multidimensional modifiable factors were explored that could be targeted for public health interventions for the identified dietary patterns. Integrated and multifaceted dietary intervention approaches are needed to promote healthy diets and discourage the consumption of unhealthy diets to reduce undernutrition in the study area and similar settings.
Adolescence is a transitional period characterized by the rapid growth and development that are the foundation for later life, health, and wellbeing. At this time, adolescents require essential nutrients such as protein, calcium, and iron for optimal growth and development (1, 2). This rapid growth rate combined with a lower nutrient intake leads to a risk of nutritional vulnerability and deficiencies in this age group (3).
The dietary pattern of an individual is sustainable nutrition behaviors to enhance the overall health of adolescents (1, 2). It helps to measure the number, proportion, variety, or combination of different foods and beverages in a more comprehensive way. This approach considers the interactions between foods and nutrients to promote health or reduce disease risk (4, 5).
Dietary pattern analysis of the target population helps to predict the risk of disease better than the analysis of isolated nutrients because the joint effect of the various nutrients involved would be better identified (5). It helps to understand the relationship between dietary habits and disease outcomes, which is important for public health actions to develop and provide diet-based intervention programs (6).
Unhealthy dietary patterns developed during adolescence can lead to diet-related chronic non-communicable diseases in later life (7, 8). Adolescents consume diets that are not in line with the recommended healthy diet; only 17% of adolescents have a diversified diet at the global level (9). This poor nutritional habit of adolescents leads to stunting, which exposes them to concurrent and future adverse health outcomes (3).
Adolescents from developed countries such as the United States, Europe, and Australia had low consumption habits of healthy diets such as fruits, vegetables, dairy products, and whole grains but higher consumption of unhealthy diets such as soft drinks and fast foods (10, 11). This problem also exists in adolescents living in low- and middle-income countries, where their eating habits are characterized by unhealthy habits (1, 2, 6, 12).
Adolescents had poor dietary habits in Ethiopia (13). According to a study conducted in Northwest Ethiopia, 32.30% of the adolescents had adequate dietary diversity, 97.70% of adolescent girls consumed starchy staples, 42.6% had no fruit intake, and only 1.70% of them consumed animal-source food (9, 14).
The burden of stunting and thinness among adolescents in Ethiopia ranges 12.50–33.10% and 12.60–58.30%, respectively (15–18). This figure indicates that undernutrition among adolescents is a significant health problem (19, 20). Adolescents’ dietary habits were influenced by various socioeconomic factors, such as lack of exposure to nutrition education and influence from family, peers, and the media. Access to and availability of diversified food items were the most commonly reported factors (2, 21).
Adolescents provide a second opportunity for nutritional interventions to mitigate all forms of nutritional deficiency (22). Hence, there is a need for updated evidence on dietary consumption patterns for designing and implementing appropriate nutrition interventions targeting adolescents. Previous studies have mainly focused on determining nutritional status and dietary diversity score assessments of adolescents, which did not consider the complexity of diets (23–26).
There is a lack of evidence to investigate dietary patterns and their relationship with nutrition outcomes among adolescents. Therefore, this study was conducted to generate evidence for public health interventions for adolescents’ nutritional interventions.
A cross-sectional survey was conducted among adolescents who resided in six randomly selected areas of Dembecha Woreda, Northwest Ethiopia. Data were collected from 10 December 2021 to 20 January 2021. The study area consists of three agroecology zones (low-, mid-, and high-lands), which are conducive to diversified agricultural production.
Adolescents aged 10–19 years were the target population for the current study. These populations are overlooked for nutritional intervention in developing countries, including Ethiopia, as well as in the current setting. Adolescents with spinal curvature, who could not stand properly or walked with a wheelchair, did not participate in the study.
A single population proportion formula was used to determine the total number of adolescents in this study, based on the following assumptions: a 5% error margin, a 95% confidence interval, and a proportion of 44.6% for the consumption habit (P) of dark green leafy vegetables in southwest Ethiopia (25) with a design effect of 1.5. After adding a 10% non-response rate, the final sample size was 627.
The study area was purposefully selected due to its unique three agroecology zones (low-, mid-, and high-lands), which represent the northwest region of the country. Then, from each agroecology zone, two research settings, or Kebeles (the lowest administrative unit in the case of Ethiopia), were randomly selected as study areas for data collection.
Subsequently, from a randomly selected study setting, eligible households with at least one adolescent were registered, and a sampling frame was prepared. The number of adolescents assigned is proportional to the size (population) of a particular site. Finally, 357 adolescents from high-land, 77 from mid-land, and 188 from low-land agroecology zones were interviewed.
A pretested, structured interviewer-administered questionnaire was used for data collection. The tool was adapted from peer-reviewed articles and customized to the local context. Data on the dietary patterns of adolescents were collected using a validated food frequency questionnaire (FFQ) and contextualized to the setting over 1 week. To develop the FFQ assessment tool, a list of local food items that were consumed at different times during meals and snacks was collected by conducting a pilot study on 30 adolescents for 2 non-consecutive weekdays and 1 weekend day (27). The FFQ was organized in a semi-quantitative manner and administered using 24-h dietary recall methods.
Anthropometric data on adolescents’ weight and height were measured using a standard weight and height scale with precisions of ±0.1 kg and ± 0.1 cm, respectively, based on WHO protocol (28). During measurement, adolescents wore lightweight clothing without shoes to minimize error. Trained human nutrition graduates collected data through interviews and anthropometric measurements.
Data quality was ensured in all phases of the research activities. The tool was translated from English into an Amharic version (the local language). Training was provided to data collectors on the sampling procedures and interview techniques. The questionnaire was pretested using 5% of the total sample size at one site, which was not included in the actual study. In addition, before conducting actual dietary data collection from each sample, the FFQ was tested for internal reliability in 30 adolescents. The test results showed Cronbach’s alpha coefficient (α) of 0.79.
This result indicates that the FFQ is reliable for measuring the dietary patterns of adolescents. During the measurement of anthropometric weight and height data, calibration of the instrument was performed after each measurement. In addition, local food-colored pictures were used to minimize recall bias. The research lead investigator closely followed the day-to-day data collection process to ensure the completeness and consistency of the administered questionnaire.
Statistical analysis was carried out using SPSS version 25 and WHO Anthro Plus software. A descriptive analysis was conducted to characterize the data using frequencies, percentages, means, and standard deviations. Before conducting further analysis, extreme values and the normality distribution of continuous variables were checked.
Dietary patterns were determined using exploratory factor analysis (EFA). Kaiser–Meyer–Olkin (KMO; value of p > 0.05) and Bartlett’s test of sphericity (value of p<0.05) were used to check the adequacy of the sample-to-factors ratio. The existence of a correlation between food items was determined for each step of factor analysis (29). Then, EFA was run under orthogonal rotation with the varimax method to select interpretable and independent dietary patterns. Factors with a communality above 0.5 and an eigenvalue above 1 explained by principal components were used to decide the final dietary patterns (30).
Nutritional outcomes of adolescents were determined based on height for age (HA), and body mass index (BMI) for age z-scores was computed using WHO AnthroPlus software (31, 32). A chi-square test was conducted to evaluate the effect of the identified dietary patterns on the burden of stunting and thinness of adolescents. Significant differences were determined with a value of p of < 0.05.
To identify factors for the identified dietary patterns, the first binary logistic regression analysis was carried out to measure the existence of an association between dietary patterns and factors. Then, factors that showed an association between binary logistic regression analysis and those with a p-value of <0.3 were fitted to the multivariable logistic regression model to identify significant factors. Significant factors were reported with a p-value of less than 0.05.
Based on factor loadings, dietary patterns were determined using EFA. Based on the score, possible different dietary patterns were developed (33, 34). Then, each dietary pattern was classified into quartiles (Q) based on their contribution to each pattern, assuming an increasing order from Q1 to Q4 (35). Finally, Q1 and Q2 were combined to represent low consumption habit (0), while Q3 and Q4 represent high consumption of dietary habit (1) (35).
Adolescents’ nutritional status is determined based on height for age and body mass index for age using WHO AnthroPlus software (32). Then, HA z-scores < −2 SD were categorized as “stunted” and < −3 SD were categorized as “severely stunted,” and BMI for age z-scores < −2 SD was categorized as “thin” and > +1 SD was categorized as “overweight/obese” using the WHO cutoff points (31).
Ethical clearance was secured from the Institutional Review Board (IRB) of Addis Ababa University from the College of Natural and Computational Sciences. The study aims, possible risks, benefits, and privacy were described verbally to the study participants. Participation in the study was voluntary, and we gave them full autonomy to participate. To maintain confidentiality, the names and other identifiers of the study participants were not recorded in the data collection tool. Data on the anonymity and confidentiality of the study participants were assured. Informed verbal consent was obtained from parents of adolescents aged <18 years. Direct verbal informed consent was obtained from adolescents aged >18 years.
From the calculated sample size of 627 participants, 622 were involved in the study, with a response rate of 99.20%. The mean age of adolescents was 15.2 ± 2.02 years. More than half (60.10%) of the participants were girls. In total, 82.30% of adolescents’ mothers had no formal education, 11.90% attended elementary education, and the remaining 5.80% attended secondary education and above. Regarding the wealth index, 40.50% had lower thirds, 34.40% had medium thirds, and the remaining 25.10% had higher thirds (Table 1).
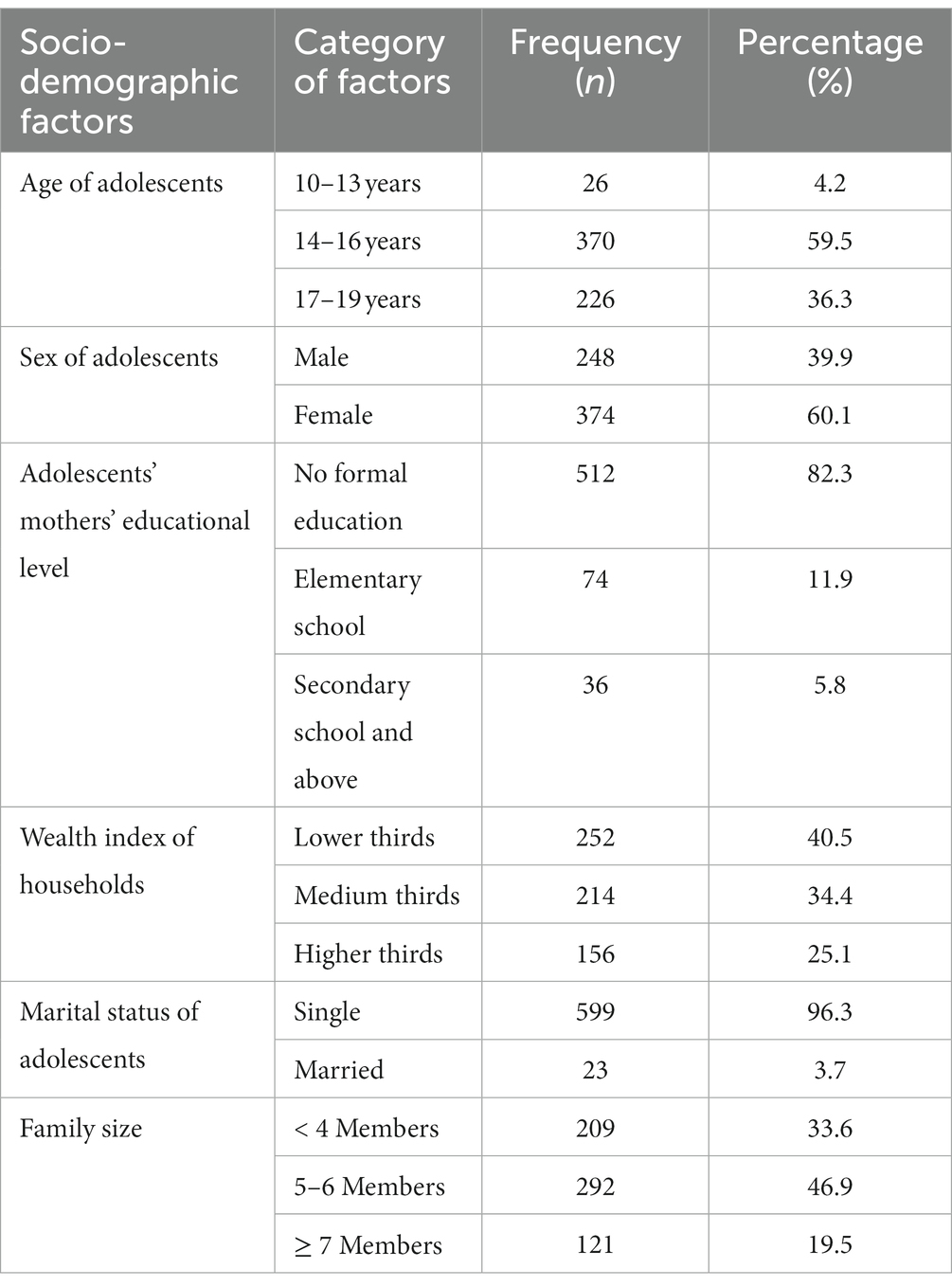
Table 1. Background characteristics of adolescents in Dembecha Woreda, Northwest Ethiopia, 2021.
The food lists were grouped into common food groups based on their similarity in nutrient contributions. Eight food groups were identified from the collected dietary consumption data. These food groups consist of traditional, legumes, tubers, whole grains, foods with high carbohydrate content, fruits and vegetables, animal sources, and traditional alcoholic beverages. Based on the EFA factor loading analysis, in the first component, traditional and legume diets had higher scores of 0.962 and 0.964, respectively. In the second component, fruit and vegetable diets, high carbohydrate (tea and white bread), and whole grain diets were identified with scores of 0.710, 0.653, and 0.519, respectively. In the third component, animal-source foods (eggs, meat, milk, and milk products) and traditional alcoholic beverages were identified with factor loadings of 0.746 and 0.625, respectively (Table 2).
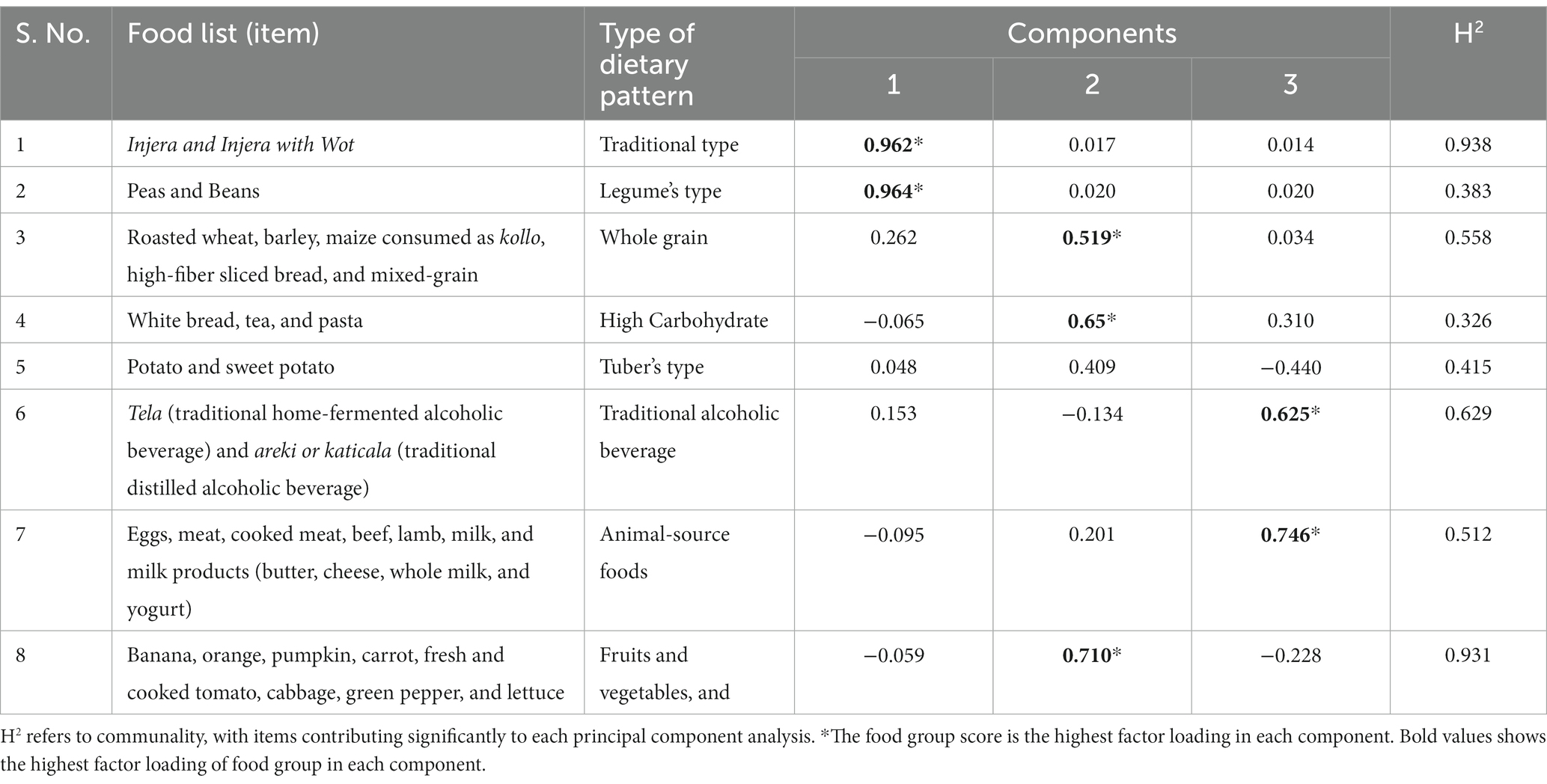
Table 2. Exploratory factor analysis results of food frequency and factor loading consumed by adolescents in Dembecha Woreda, Northwest Ethiopia, 2021.
Based on EFA analysis, three major types of dietary patterns were identified, which explained 58.64% of the variance in adolescent diets. The label assigned to each component was based on the items with high factor-loading scores and the interpretability of the factors. These include (1) the traditional type, explained by 26.71%; (2) mixed type, explained by 16.63%; and (3) animal-source foods with traditional alcoholic beverages, explained by 15.30% (Figure 1). From the identified dietary patterns, traditional, mixed, and animal-source dietary patterns were identified as healthy types; high-carbohydrate and traditional alcoholic beverage drinking patterns were identified as unhealthy types.
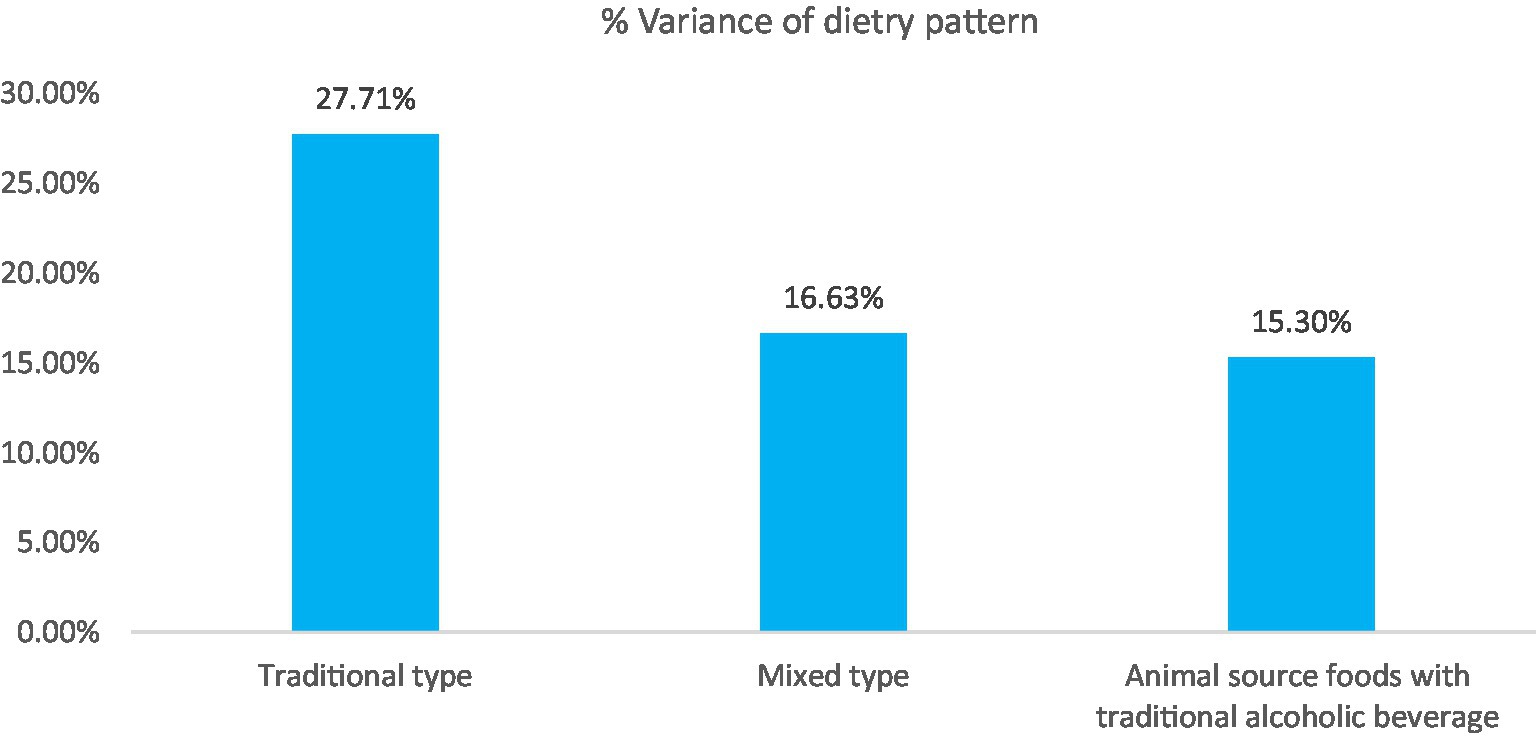
Figure 1. Percentage variance explained the three emerging dietary patterns of adolescents in Dembecha Woreda, Northwest Ethiopia, 2021.
The prevalence of stunting was 26.30% (95% CL: 22.70, 30.20%), thinness was 9.60% (95% CL: 7.30, 12.40%), and overweight was 1.80%. Of the adolescents, 22.80% were moderately stunted, and the remaining 3.60% were severely stunted. This community-level undernutrition indicated that one in four and one in 10 adolescents were stunted and thin in their nutritional status, which became significant public health problems.
The burden of stunting was 15.12% versus 11.21 and 19.40% versus 6.94% for the lower and higher traditional and mixed dietary patterns, respectively. In contrast, 7.30% versus 19.00% of stunting was observed in higher and lower animal sources with alcoholic dietary patterns and consuming habits of adolescents, respectively (p < 0.05). However, there were no significant differences in thinness between the lower and higher consumption habits of the identified dietary patterns (p-value >0.05; Table 3).
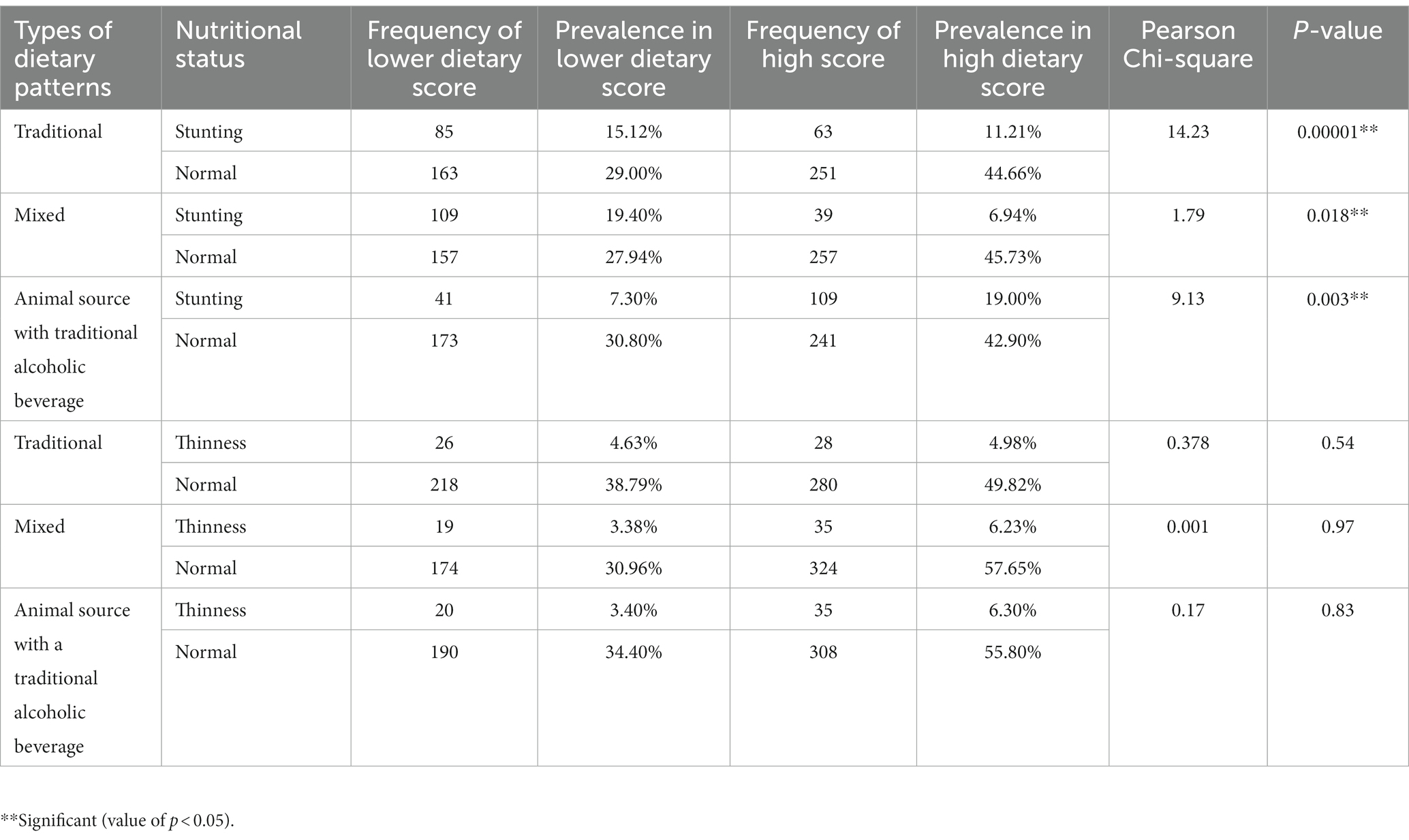
Table 3. Dietary patterns and its effect on nutritional outcomes of adolescents in Dembecha Woreda, Northwest Ethiopia, 2021.
Adolescents who resided in low-land agroecology (AOR = 2.4; 95% CL: 1.24, 4.81) and mid-land agroecology (AOR = 0.48; 95%: 0.31, 0.74), the early age range of 10–13 years (AOR = 0.6; 95% CL: 0.46, 0.99), and had access to animal sources (AOR = 1.64; 95% CL: 1.04, 2.60) were significantly associated with a lower consumption habit of traditional dietary pattern (Table 4).
A mixed type of dietary pattern was the second component of a dietary pattern, which was explained by 16.63% of all dietary patterns. Among sociodemographic factors, adolescents who were male (AOR =2.28; 95% CL: 1.56, 3.34), resided in mid-land agroecology (AOR = 1.80; 95% CL: 1.18, 2.74), high-land agroecology (AOR = 2.14; 95% CL: 1.19, 3.87), whose mothers had no formal education (AOR = 2.38; 95% CL: 1.35, 4.19), lived with large family size (AOR = 1.69; 95% CL: 1.02, 2.80), and had poor nutritional knowledge (AOR = 2.83; 95% CL: 1.12, 4.05) had a significant association with lower consumption of a mixed type of dietary pattern (Table 4).
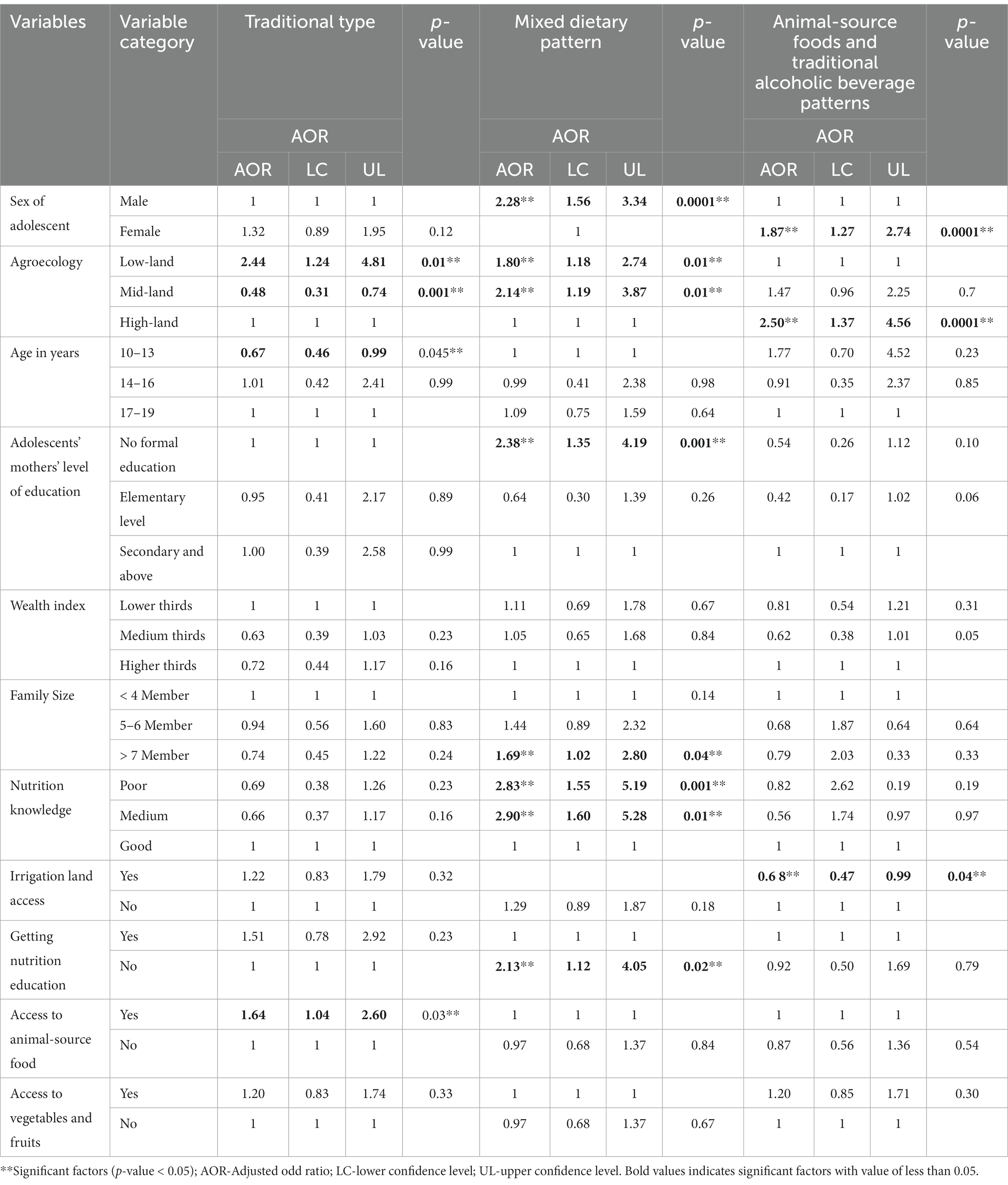
Table 4. Contributing factors for lower consumption of major dietary patterns among adolescents, Dembecha Woreda, Northwest Ethiopia, 2021.
A third type of dietary habit was explained by a 15.30% variance. This dietary pattern was characterized by the consumption habits of animal-source foods (milk, eggs, and meat) with traditional alcoholic drinking. Traditional alcohol consumption is an unhealthy dietary pattern. Overall, this type of dietary pattern lacks vitamins and minerals that are found in vegetables and fruits. Being female adolescents (AOR = 1.87; 95% CL: 1.27, 2.74), those who were residing in high-land agroecology (AOR = 2.50; 95% CL: 1.37, 4.56) and had access to irrigation land (AOR = 0.68; 95% CL: 0.47, 0.99) had a significant association with lower consumption of animal sources with traditional alcoholic beverage dietary patterns (Table 4).
Three main types of dietary patterns were identified, of which traditional, mixed, and animal-sourced foods were considered healthy types. However, high-carbohydrate and traditional alcoholic beverages were unhealthy. The identified dietary patterns were the most common and easily accessible in the local area through agricultural production in developing countries (12). This identified healthy and unhealthy dietary habits of adolescents were practiced among adolescents in developing countries such as Ghana (2) and India (36).
In the current study, adolescents had lower consumption habits of healthy dietary patterns of fruits and vegetables. This finding is similar to the study conducted among urban adolescents in Bangladesh, where their habitual dietary pattern indicated poor consumption of leafy vegetables (33). This feeding habit predisposes adolescents to essential micronutrient deficiencies (33, 37).
Overall, 26.30 and 9.60% of adolescents were stunted and thin in their nutritional outcomes. These findings indicate that undernutrition among adolescents is a public health concern in the study setting. The burden of stunting was 15.12% versus 11.21, 19.40% versus 6.94, and 8.36% versus 17.97% in adolescents with lower traditional, mixed, and higher animal sources with alcoholic dietary consumption habits, respectively. This is because the effect of lower consumption dietary pattern does not satisfy the daily requirement of nutrients for the physical growth and development of adolescents (21). Inadequate intake of macronutrients and micronutrients, poor quantity, and quality dietary habits lead to undernutrition (6, 37, 38).
Regarding animal sources with the traditional alcoholic dietary pattern, the prevalence of stunting was 7.30% in the lower consumption group and 19.00% in the higher consumption group. This diet is characterized by the feeding habits of food items such as meat, eggs, milk, and milk products, along with traditional alcoholic drinking. However, the effects of alcohol and its metabolism prevent the absorption and utilization of nutrients. Hence, it leads to a deficiency of micronutrients and macronutrients, leading to undernutrition (39).
There were no significant differences in thinness between adolescents with lower and higher scores in the three identified dietary patterns. Thinness among adolescents was not affected by long-term dietary habits but rather by immediate factors such as infections (40, 41), diversification in feeding practice (41), and household food insecurity (42, 43).
The second type of dietary pattern was identified as the mixed type. Of all adolescents, one-fourth (25.5%) consumed a whole-grain diet per week. This is considered a healthy type due to the nutritional contribution of vitamins and minerals, which are found in fruits and vegetables. In addition, a whole-grain-based diet can provide energy, starch, and dietary fiber (44–46). A similar pattern was identified in a study conducted among school-age children in Scandinavian countries (47) and Ghana (12).
Among sociodemographic factors, adolescents who live with large family sizes had two times lower consumption habits of mixed types of dietary patterns. This is due to the effect of large family influence on the economic insufficiency of households to meet their diversified dietary needs (48, 49). A similar study confirmed that the dietary patterns of adolescents were significantly determined by the socioeconomic status of a family (50). Adolescents who belonged to low socioeconomic status did not consume healthier diets as compared with those of middle and high socioeconomic status (49, 51).
Adolescents’ mothers who did not attend formal education were two times more likely to have lower consumption of mixed types of dietary patterns. As the educational status of adolescents’ mothers improved, they had a chance to get information on healthy dietary habits to translate nutritional knowledge into practice (52, 53).
Among modifiable factors, adolescents who had poor nutrition knowledge and lack of exposure to nutrition education were three and two times more likely to have a lower consumption habit of mixed types of dietary patterns. This might be due to the effect of poor nutritional knowledge on the mixed feeding habits of adolescents (49). Furthermore, as adolescents have sufficient basic nutritional knowledge, they can get enough information about the nutrient contents of diversified food items (49, 54, 55).
The third dietary pattern was mainly characterized by the consumption of milk, meat, and eggs, along with the drinking habit of traditional alcoholic beverages. From the animal-source foods, sea foods such as fish were not consumed in the study area due to a lack of access in the study setting (56, 57).
Female adolescents were nearly two times more likely to consume low-animal-source foods and alcohol as compared with their male counterparts. This is due to community social norms in intra-household food serving as staple food items are distributed fairly equally, and side dishes usually containing animal-source food (like meat, eggs and, milk) are provided for male adolescents (58).
In addition, evidence in developing countries indicates that at the household level, staple food items are distributed fairly to all family members, and side dishes usually containing more micronutrients (such as meat) are often preferably allocated to male heads of household and male children. This brings lower consumption habits for animal-source foods among adolescent girls (59, 60).
This is a comprehensive study that assesses the dietary patterns of adolescents and their effect on nutrition outcomes in the study setting. The study focused on adolescents, who were understudied and overlooked population group in nutrition interventions in developing countries. As a limitation, the inability to identify all food items that are used to prepare the local traditional diet, as adolescents were not involved in cooking at home, might lead to under-reported food items such as spices.
Generally, the dietary pattern of adolescents is dominated by a plant-based diet with limited consumption of micronutrient-rich sources of nutrition. From the identified dietary patterns, traditional, mixed, and animal-source dietary patterns were identified as healthy types; high carbohydrate and traditional alcoholic beverage drinking patterns were identified as unhealthy types. Significantly, the burden of stunting was relatively higher among adolescents who had lower consumption habits of traditional and mixed dietary patterns and higher consumption habits of animal sources with alcoholic diets. However, there were no significant differences in thinness between lower and higher consumption habits in the identified dietary pattern.
Multidimensional modifiable factors were identified for lower consumption of healthy dietary patterns, which could be targeted for public health interventions. Integrated and multifaceted dietary intervention approaches are needed to promote a healthy diet, discouraging the consumption of unhealthy diets to reduce the burden of stunting in the study area and similar settings. Enhancing the sea-food consumption habits of adolescents and the entire community by introducing small-scale fish farms as nutrition-sensitive intervention pilot projects in study settings and beyond.
The original contributions presented in the study are included in the article/supplementary materials, further inquiries can be directed to the corresponding author/s.
EA: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Supervision, Writing – original draft, Writing – review & editing. ZA: Conceptualization, Methodology, Supervision, Validation, Writing – review & editing. AA: Investigation, Methodology, Supervision, Validation, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The authors of this research study were sponsored with financial support from Addis Ababa University with Grant number FDSN/03/2021.
The authors would like to thank the study participants for their substantial contributions to participating in the study. In addition, the authors would like to thank data collectors and field facilitators for their support in collecting the data. The authors also extend their thanks to the Dembecha Woreda Health Office for their administrative support while implementing this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
AOR, Adjusted odd ratio; BMI, Body mass index; EEA, Exploratory factor analysis; HA, Height for age; FFQ, Food frequency questionnaire; IDA, iron deficiency anemia; IDD, iodine deficiency disorders; MNDs, Micronutrient deficiencies; VAD, vitamin-A deficiency; WHO, World Health Organization.
1. Abubakar, A, Issah, AN, Yussif, B, and Agbozo, F. Dietary habit, nutritional status and related factors among adolescents in tamale Metropolis. Ghana Afr J Food Sci. (2023) 17:10–23. doi: 10.5897/AJFS2021.2147
2. Abizari, A-R, and Ali, Z. Dietary patterns and associated factors of schooling Ghanaian adolescents. J Health Popul Nutr. (2019) 38:1–10. doi: 10.1186/s41043-019-0162-8
3. Deka, MK, Malhotra, AK, Yadav, R, and Gupta, S. Dietary pattern and nutritional deficiencies among urban adolescents. J Family Med Prim Care. (2015) 4:364–8. doi: 10.4103/2249-4863.161319
4. Seyoum Keflie, T, Samuel, A, Lambert, C, Nohr, D, and Biesalski, HK. Dietary patterns and risk of micronutrient deficiencies: their implication for nutritional intervention in Ethiopia. J Nutrit Health Food Sci. (2018) 6:1–16. doi: 10.15226/jnhfs.2018.001120
5. Corrêa, RS, Vencato, PH, Rockett, FC, and Bosa, VL. Dietary patterns: are there differences between children and adolescents? Cien Saude Colet. (2017) 22:553–62. doi: 10.1590/1413-81232017222.09422016
6. Borges, CA, Slater, B, Santaliestra-Pasías, A, Mouratidou, T, Huybrechts, I, Widhalm, K, et al. Dietary patterns in European and Brazilian adolescents: comparisons and associations with socioeconomic factors. Nutrients. (2018) 10:57. doi: 10.3390/nu10010057
7. Akseer, N, al-Gashm, S, Mehta, S, Mokdad, A, and Bhutta, ZA. Global and regional trends in the nutritional status of young people: a critical and neglected age group. Ann N Y Acad Sci. (2017) 1393:3–20. doi: 10.1111/nyas.13336
8. Hinnig, P, Monteiro, J, de Assis, M, Levy, R, Peres, M, Perazi, F, et al. Dietary patterns of children and adolescents from high, medium and low human development countries and associated socioeconomic factors: a systematic review. Nutrients. (2018) 10:436. doi: 10.3390/nu10040436
9. Birru, SM, Tariku, A, and Belew, AK. Improved dietary diversity of school adolescent girls in the context of urban Northwest Ethiopia: 2017. Ital J Pediatr. (2018) 44:1–6. doi: 10.1186/s13052-018-0490-0
10. Aljaraedah, TY, Takruri, HR, and Tayyem, RF. Dietary practices and nutrient intake among adolescents: a general review. Obesity Med. (2019) 16:100145. doi: 10.1016/j.obmed.2019.100145
11. Keats, EC, Rappaport, A, Shah, S, Oh, C, Jain, R, and Bhutta, Z. The dietary intake and practices of adolescent girls in low-and middle-income countries: a systematic review. Nutrients. (2018) 10:1978. doi: 10.3390/nu10121978
12. Ogum Alangea, D, Aryeetey, RN, Gray, HL, Laar, AK, and Adanu, RMK. Dietary patterns and associated risk factors among school age children in urban Ghana. BMC Nutr. (2018) 4:22–9. doi: 10.1186/s40795-018-0230-2
13. Worku, M, Hailemicael, G, and Wondmu, A. Dietary diversity score and associated factors among high school adolescent girls in Gurage zone, Southwest Ethiopia. World J Nutr Health. (2017) 5:41–5. doi: 10.12691/jnh-5-2-3
14. Gonete, KA, Tariku, A, Wami, SD, and Akalu, TY. Dietary diversity practice and associated factors among adolescent girls in Dembia district, Northwest Ethiopia, 2017. Public Health Rev. (2020) 41:1–13. doi: 10.1186/s40985-020-00137-2
15. Tariku, A, Belew, AK, Gonete, KA, Hunegnaw, MT, Muhammad, EA, Demissie, GD, et al. Stunting and its determinants among adolescent girls: findings from the nutrition surveillance project, Northwest Ethiopia. Ecol Food Nutr. (2019) 58:481–94. doi: 10.1080/03670244.2019.1636793
16. Gebregyorgis, T, Tadesse, T, and Atenafu, A. Prevalence of thinness and stunting and associated factors among adolescent school girls in Adwa town, North Ethiopia. Int J Food Sci. (2016) 2016:1–8. doi: 10.1155/2016/8323982
17. Tegegne, M, Sileshi, S, Assefa, T, and Kalu, A. Nutritional status and associated factors of adolescent school girls, Goba Town, Southeast Ethiopia. Nutrition. (2016) 4:5.
18. Amha, A, and Girum, T. Prevalence and associated factors of thinness among adolescent girls attending governmental schools in Aksum town, northern Ethiopia. Med J Dr DY Patil Univ. (2018) 11:158–64. doi: 10.4103/MJDRDYPU.MJDRDYPU_153_17
19. Berhe, K, Kidanemariam, A, Gebremariam, G, and Gebremariam, A. Prevalence and associated factors of adolescent undernutrition in Ethiopia: a systematic review and meta-analysis. BMC Nutr. (2019) 5:1–13. doi: 10.1186/s40795-019-0309-4
20. De, K. Effect of socio-economic status on nutritional status on adolescent girls of Paschim Medinipur, West Bengal, India. Vitam Miner. (2017) 5:2376–1318. doi: 10.4172/2376-1318.1000149
21. Adamu, A, Adjei, G, and Kubuga, C. Effects of dietary patterns on the nutritional status of upper primary school children in tamale metropolis. Pak J Nutr. (2012) 11:591–609.
22. Nithya, D, and Bhavani, R. Dietary diversity and its relationship with nutritional status among adolescents and adults in rural India. J Biosoc Sci. (2018) 50:397–413. doi: 10.1017/S0021932017000463
23. Endalifer, ML, Andargie, G, Mohammed, B, and Endalifer, BL. Factors associated with dietary diversity among adolescents in Woldia, Northeast Ethiopia. BMC Nutr. (2021) 7:1–8. doi: 10.1186/s40795-021-00430-6
24. Halala Handiso, Y, Belachew, T, Abuye, C, and Workicho, A. Low dietary diversity and its determinants among adolescent girls in southern Ethiopia. Cogent Food Agric. (2020) 6:1832824. doi: 10.1080/23311932.2020.1832824
25. Melaku, Y, Dirar, A, Feyissa, GT, and Tamiru, D. Optimal dietary practices and nutritional knowledge of school adolescent girls in Jimma town, south West Ethiopia. Int J Adolesc Youth. (2018) 23:299–307. doi: 10.1080/02673843.2017.1369889
26. Gonete, KA, Tariku, A, Wami, SD, and Derso, T. Prevalence and associated factors of anemia among adolescent girls attending high schools in Dembia District, Northwest Ethiopia, 2017. Arch Public Health. (2018) 76:1–9. doi: 10.1186/s13690-018-0324-y
27. FAO. Dietary assessment a resource guide to method selection and application in low resource settings. Rome, Italy: FAO (2017).
28. World Health Organization. WHO STEPS surveillance manual: The WHO STEPwise approach to chronic disease risk factor surveillance. Geneva: World Health Organization (2005).
29. Mengistu, G, Azage, M, and Gutema, H. Iron deficiency anemia among in-school adolescent girls in rural area of Bahir Dar city administration, North West Ethiopia. Anemia. (2019) 2019:1–8. doi: 10.1155/2019/1097547
30. Omage, K, and Omuemu, VO. Assessment of dietary pattern and nutritional status of undergraduate students in a private university in southern Nigeria. Food Sci Nutr. (2018) 6:1890–7. doi: 10.1002/fsn3.759
31. World Health Organization. Growth reference 5–19 years: BMI-for-age (5–19 years). (2007). https://www.who.int/growthref/who2007_bmi_for_age/en/. (Accessed April 16, 2023).
32. World Health Organization. Anthro plus for personal computers manual: Software for assessing growth of the World’s children and adolescents. Geneva, Switzerland: WHO (2010).
33. Kabir, Y, Shahjalal, HM, Saleh, F, and Obaid, W. Dietary pattern, nutritional status, anaemia and anaemia-related knowledge in urban adolescent college girls of Bangladesh. JPMA. The. J Pak Med Assoc. (2010) 60:633–8.
34. McNaughton, SA, Ball, K, Mishra, GD, and Crawford, DA. Dietary patterns of adolescents and risk of obesity and hypertension. J Nutr. (2008) 138:364–70. doi: 10.1093/jn/138.2.364
35. Zhen, S, Ma, Y, Zhao, Z, Yang, X, and Wen, D. Dietary pattern is associated with obesity in Chinese children and adolescents: data from China health and nutrition survey (CHNS). Nutr J. (2018) 17:1–9. doi: 10.1186/s12937-018-0372-8
36. Kotecha, P, Patel, SV, Baxi, RK, Mazumdar, VS, Shobha, M, Mehta, KG, et al. Dietary pattern of schoolgoing adolescents in urban Baroda, India. J Health Popul Nutr. (2013) 31:490–6. doi: 10.3329/jhpn.v31i4.20047
37. Ochola, S, and Masibo, PK. Dietary intake of schoolchildren and adolescents in developing countries. Ann Nutr Metab. (2014) 64:24–40. doi: 10.1159/000365125
38. Benazeera, UJ. Association between eating habits and body mass index (BMI) of adolescents. Int J Med Sci Public Health. (2014) 3:940–3. doi: 10.5455/ijmsph.2014.290420141
39. Lieber, CS. Relationships between nutrition, alcohol use, and liver disease. Alcohol Res Health. (2003) 27:220–31.
40. Shiferaw, H, and Gebremedhin, S. Undernutrition among HIV-positive adolescents on antiretroviral therapy in southern Ethiopia. Adolesc Health Med Ther. (2020) 11:101–11. doi: 10.2147/AHMT.S264311
41. Mersha, J, Tariku, A, and Gonete, KA. Undernutrition and associated factors among school adolescent girls attending schools in Mirab-Armachiho District, Northwest Ethiopia. Ecol Food Nutr. (2021) 60:473–90. doi: 10.1080/03670244.2021.1872022
42. Candler, T, Costa, S, Heys, M, Costello, A, and Viner, RM. Prevalence of thinness in adolescent girls in low-and middle-income countries and associations with wealth, food security, and inequality. J Adolesc Health. (2017) 60:447–454.e1. doi: 10.1016/j.jadohealth.2016.11.003
43. Wassie, MM, Gete, AA, Yesuf, ME, Alene, GD, Belay, A, and Moges, T. Predictors of nutritional status of Ethiopian adolescent girls: a community based cross sectional study. BMC Nutr. (2015) 1:1–7. doi: 10.1186/s40795-015-0015-9
44. Borneo, R, and León, AE. Whole grain cereals: functional components and health benefits. Food Funct. (2012) 3:110–9. doi: 10.1039/C1FO10165J
45. Šramková, Z, Gregová, E, and Šturdík, E. Chemical composition and nutritional quality of wheat grain. Acta Chim Slov. (2009) 2:115–38.
46. McKevith, B. Nutritional aspects of cereals. Nutr Bull. (2004) 29:111–42. doi: 10.1111/j.1467-3010.2004.00418.x
47. Frølich, W, Åman, P, and Tetens, I. Whole grain foods and health–a Scandinavian perspective. Food Nutr Res. (2013) 57:18503. doi: 10.3402/fnr.v57i0.18503
48. Heather, G, and Karen, C-N. Exploring nutrition literacy: attention to assessment and the skills clients need. Health. (2012) 2012:43019. doi: 10.4236/health.2012.43019
49. Koca, B, and Arkan, G. The relationship between adolescents’ nutrition literacy and food habits, and affecting factors. Public Health Nutr. (2021) 24:717–28. doi: 10.1017/S1368980020001494
50. Nilsen, SM, Krokstad, S, Holmen, TL, and Westin, S. Adolescents’ health-related dietary patterns by parental socio-economic position, the Nord-Trøndelag health study (HUNT). Eur J Pub Health. (2010) 20:299–305. doi: 10.1093/eurpub/ckp137
51. McClain, AD, Chappuis, C, Nguyen-Rodriguez, ST, Yaroch, AL, and Spruijt-Metz, D. Psychosocial correlates of eating behavior in children and adolescents: a review. Int J Behav Nutr Phys Act. (2009) 6:1–20. doi: 10.1186/1479-5868-6-54
52. Tefera, B, Pereznieto, P, and Emirie, G. Transforming the lives of girls and young women. Case study: Ethiopia. London: Overseas Development Institute (2013).
53. Videon, TM, and Manning, CK. Influences on adolescent eating patterns: the importance of family meals. J Adolesc Health. (2003) 32:365–73. doi: 10.1016/S1054-139X(02)00711-5
54. Özdenk, G, and Özcebe, L. Nutrition literacy, dietary behaviours and related factors among university personnel. Turk J Public Health. (2018) 16:178–89. doi: 10.1177/0017896919836
55. Papakonstantinou, E, Hargrove, JL, Huang, CL, Crawley, CC, and Canolty, NL. Assessment of perceptions of nutrition knowledge and disease using a group interactive system: the perception analyzer®. J Am Diet Assoc. (2002) 102:1663–8. doi: 10.1016/S0002-8223(02)90354-8
56. Kris-Etherton, PM, Harris, WS, and Appel, LJ. Fish consumption, fish oil, omega-3 fatty acids, and cardiovascular disease. Circulation. (2002) 106:2747–57. doi: 10.1161/01.CIR.0000038493.65177.94
57. Sirot, V, Dumas, C, Leblanc, JC, and Margaritis, I. Food and nutrient intakes of French frequent seafood consumers with regard to fish consumption recommendations: results from the CALIPSO study. Br J Nutr. (2011) 105:1369–80. doi: 10.1017/S0007114510005027
58. Gittelsohn, J, and Vastine, AE. Sociocultural and household factors impacting on the selection, allocation and consumption of animal source foods: current knowledge and application. J Nutr. (2003) 133:4036S–41S. doi: 10.1093/jn/133.11.4036S
59. Martínez Pérez, G, and Pascual García, A. Nutritional taboos among the Fullas in Upper River region, the Gambia. J Anthropol. (2013) 2013:1–9. doi: 10.1155/2013/873612
Keywords: dietary patterns, nutrition outcomes, adolescents, Ethiopia, context-specific
Citation: Agedew E, Abebe Z and Ayelign A (2023) Dietary patterns in relation with nutritional outcomes and associated factors among adolescents: implications for context-specific dietary intervention for the Agrarian Community, Northwest Ethiopia. Front. Nutr. 10:1274406. doi: 10.3389/fnut.2023.1274406
Edited by:
Charoula Konstantia Nikolaou, University of Greenwich, United KingdomReviewed by:
Archana Kumari, University of Delhi, IndiaCopyright © 2023 Agedew, Abebe and Ayelign. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Eskezyiaw Agedew, ZXNrMWFnaWRAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.