
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Nutr. , 27 October 2023
Sec. Nutrition and Microbes
Volume 10 - 2023 | https://doi.org/10.3389/fnut.2023.1274122
 Aruba Sohail1†
Aruba Sohail1† Huzaifa Ahmad Cheema2*†
Huzaifa Ahmad Cheema2*† Maidah Sohail Mithani1Abia Shahid2
Maidah Sohail Mithani1Abia Shahid2 Ahmad Nawaz2Alaa Hamza Hermis3Sampath Chinnam4
Ahmad Nawaz2Alaa Hamza Hermis3Sampath Chinnam4 Abdulqadir J. Nashwan5*
Abdulqadir J. Nashwan5* Ivan Cherrez-Ojeda6,7
Ivan Cherrez-Ojeda6,7 Rehmat Ullah Awan8‡
Rehmat Ullah Awan8‡ Sharjeel Ahmad9‡
Sharjeel Ahmad9‡Background: Although numerous modalities are currently in use for the treatment and prophylaxis of COVID-19, probiotics are a cost-effective alternative that could be used in diverse clinical settings. Hence, we conducted a meta-analysis to investigate the role of probiotics in preventing and treating COVID-19 infection.
Methods: We searched several databases from inception to 30 May 2023 for all randomized controlled trials (RCTs) and comparative observational studies that evaluated probiotics (irrespective of the regimen) for the treatment or prevention of COVID-19. We conducted our meta-analysis using RevMan 5.4 with risk ratio (RR) and mean difference (MD) as the effect measures.
Results: A total of 18 studies (11 RCTs and 7 observational studies) were included in our review. Probiotics reduced the risk of mortality (RR 0.40; 95% CI: 0.25–0.65, I2 = 0%). Probiotics also decreased the length of hospital stay, rate of no recovery, and time to recovery. However, probiotics had no effect on the rates of ICU admission. When used prophylactically, probiotics did not decrease the incidence of COVID-19 cases (RR 0.65; 95% CI: 0.37–1.12; I2 = 66%). The results for all outcomes were consistent across the subgroups of RCTs and observational studies (P for interaction >0.05).
Conclusion: The results of this meta-analysis support the use of probiotics as an adjunct treatment for reducing the risk of mortality or improving other clinical outcomes in patients with COVID-19. However, probiotics are not useful as a prophylactic measure against COVID-19. Large-scale RCTs are still warranted for determining the most efficacious and safe probiotic strains.
Systematic Review Registration: PROSPERO (CRD42023390275: https://www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=390275).
New variants of COVID-19 continue to be reported worldwide significantly impacting morbidity and mortality. Thus, research to investigate novel treatment modalities still holds significance in the clinical setting. Numerous therapies have been investigated for treating COVID-19 (1, 2); however, questionable efficacy or safety, high costs, and the need for parenteral administration are among the issues that limit the widespread use of many of these agents (3–6). Probiotics can be a cost-effective alternative that could be used in diverse clinical settings.
Probiotics are defined as “live microorganisms that when administered in adequate amounts, confer a health benefit on the host (7).” Clinical trials have shown the efficacy of single or multiple strains of probiotics in the management of respiratory tract infections (8, 9). Recently, the use of probiotics for COVID-19 has also been proposed (10); however, the efficacy of probiotics in the treatment of COVID-19 remains inconclusive. Previous meta-analyses either did not include several key studies or only assessed the effect of probiotics on a limited number of clinical outcomes which limits the applicability of their findings (11–13). In this meta-analysis, we have thus included all the studies available in the literature to investigate the role of probiotics in preventing and treating COVID-19 infection.
Our meta-analysis was registered with PROSPERO (CRD42023390275) and conducted by following the recommendations of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (14).
We searched MEDLINE (via PubMed), Embase, the Cochrane Library, and ClinicalTrials.gov from inception to 30 May 2023, without using any filters or restrictions. The search strategy consisted of the following terms: (“COVID-19′′ or “coronavirus disease 2019′′ or “novel coronavirus” or “SARS-CoV-2′′) AND (“probiotics” or “S. thermophilus” or “L.acidophilus” or “synbiotics” or “Lactobacillus rhamnosus GG” or “SIM01” or “Bifidobacterium”). Reference lists of relevant articles were also manually screened to retrieve additional relevant studies. A partial search of Google Scholar was conducted to find any relevant grey literature.
All the literature obtained from our searches was imported into Mendeley Desktop 1.19.8 and duplicates were removed. The remaining articles were subjected to a rigorous screening process by two independent reviewers. The inclusion criteria were: (1) study design: randomized controlled trials (RCTs) and comparative observational studies; (2) population: patients with COVID-19 irrespective of age or disease severity; (3) intervention: probiotics (irrespective of the regimen) used to treat or prevent COVID-19; and (4) comparator: placebo or standard care.
We extracted all information relating to the study characteristics such as author names, location, study population, details of intervention and comparator groups, and our outcomes of interest. The primary outcome was the risk of all-cause mortality, while the secondary outcomes included the rates of ICU admission, length of hospital stay, time to recovery, and the rate of no recovery. For studies that assessed the use of probiotics as a prophylactic measure against COVID-19, our outcome was the incidence of COVID-19 cases.
For the quality assessment, the revised Cochrane Risk of Bias Tool (RoB 2.0) (15) was used for RCTs, while the Newcastle Ottawa Scale (NOS) was used for observational studies (16).
We conducted our meta-analysis using RevMan 5.4 with risk ratio (RR) and mean difference (MD) as the effect measures for categorical and continuous variables, respectively. We utilized a random-effects model as we anticipated our included studies to be substantially heterogeneous (17). We evaluated heterogeneity using the Chi2 test and the I2 statistic. We conducted a subgroup analysis for all of our outcomes on the basis of the type of study (RCT vs. observational study). In addition, we conducted a sensitivity analysis on our primary outcome by excluding Shah et al. (18) which combined probiotics with a systemic enzyme complex. We could not assess publication bias as no outcome included 10 studies or more.
We included 18 studies (11 RCTs and 7 observational studies) in our review (18–35). The details of the screening process are presented in Figure 1.
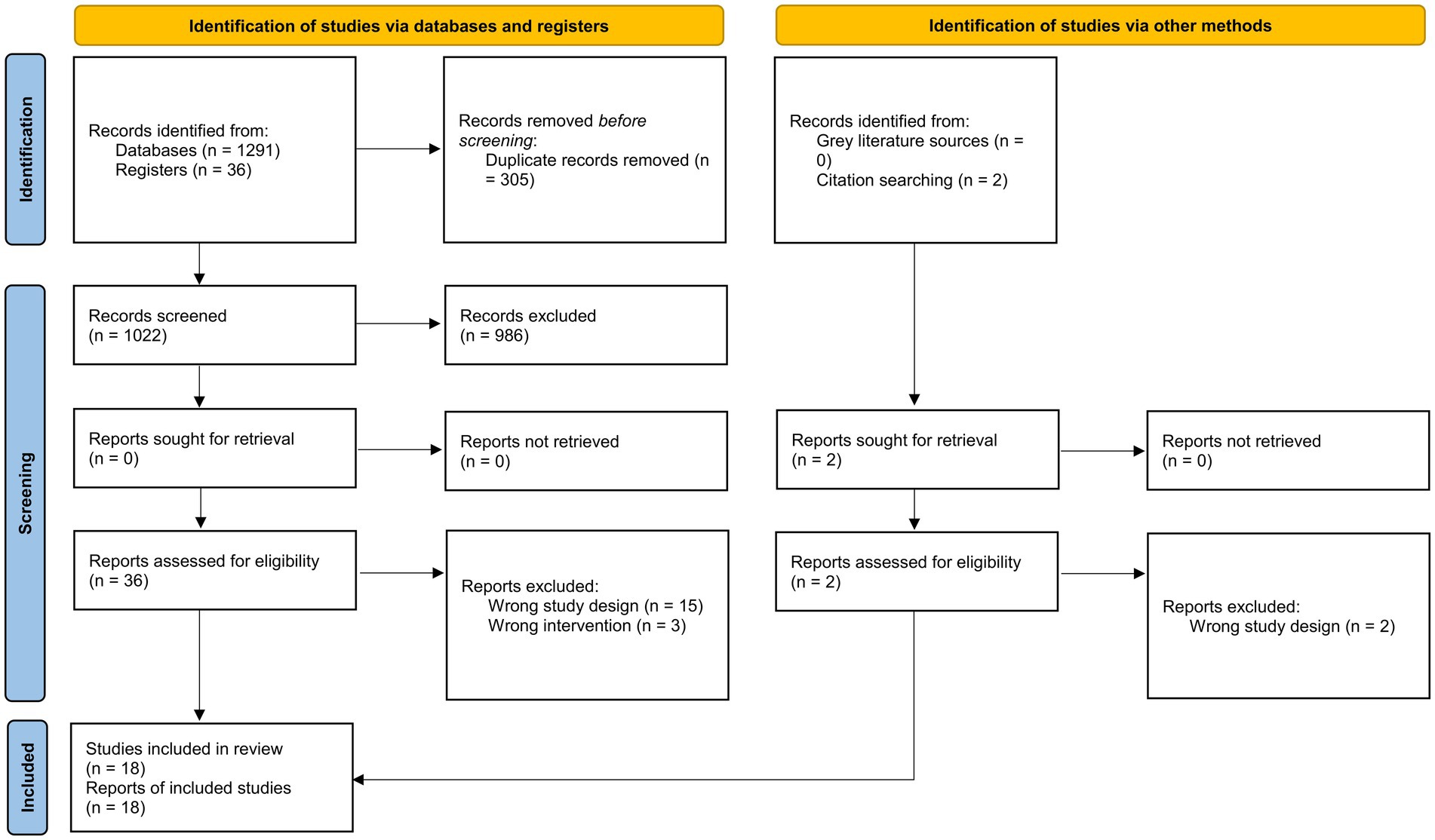
Figure 1. PRISMA 2020 flowchart.
Most of the studies had small sample sizes while the retrospective cohort study by Louca et al. was the largest with 445,850 subjects (33). The studies employed a variety of probiotic regimens and most used standard of care as the comparator. The detailed characteristics of each study are presented in Supplementary Table S1.
Two trials were at a high risk of bias, only one was at a low risk of bias, and the rest had some concerns of bias (Figure 2). The most frequent bias was in the randomization process. Of the observational studies, only two were deemed to be of high quality (Table 1).
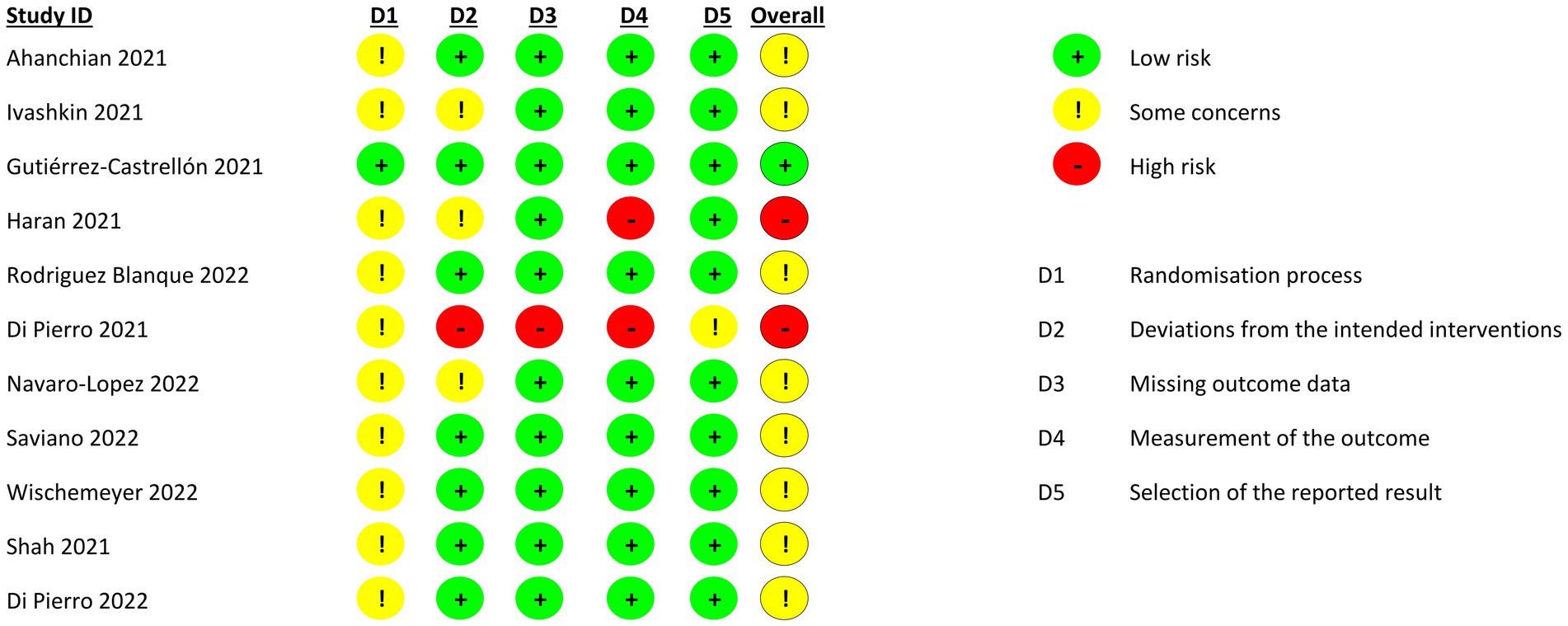
Figure 2. Quality assessment of included trials.
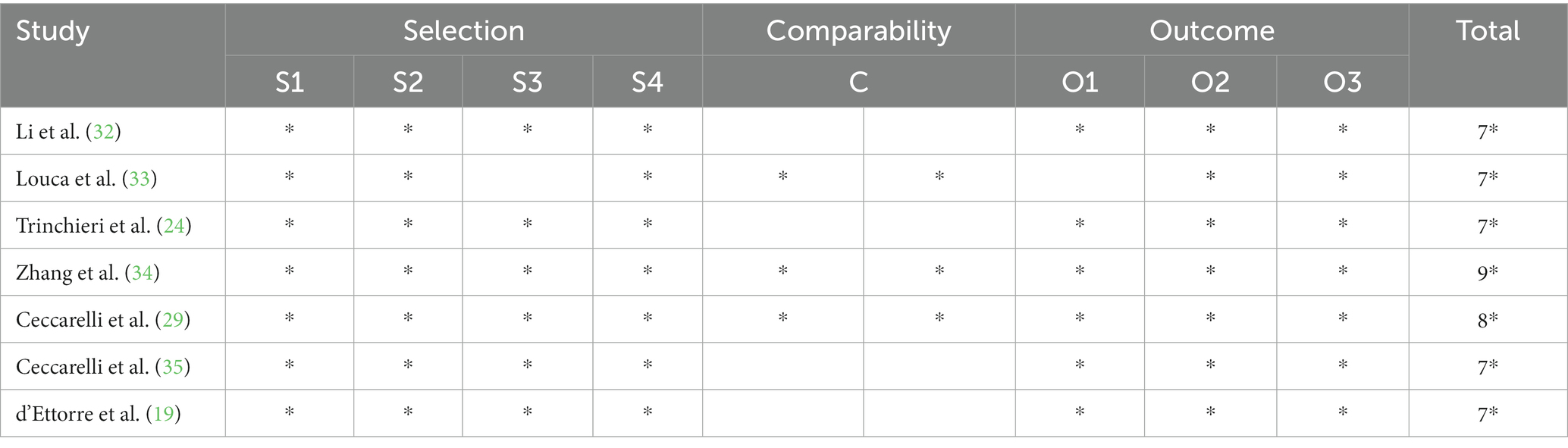
Table 1. Quality assessment of observational studies.
The results of our meta-analysis showed that probiotics reduced the risk of mortality (RR 0.40; 95% CI: 0.25–0.65, I2 = 0%; Figure 3).
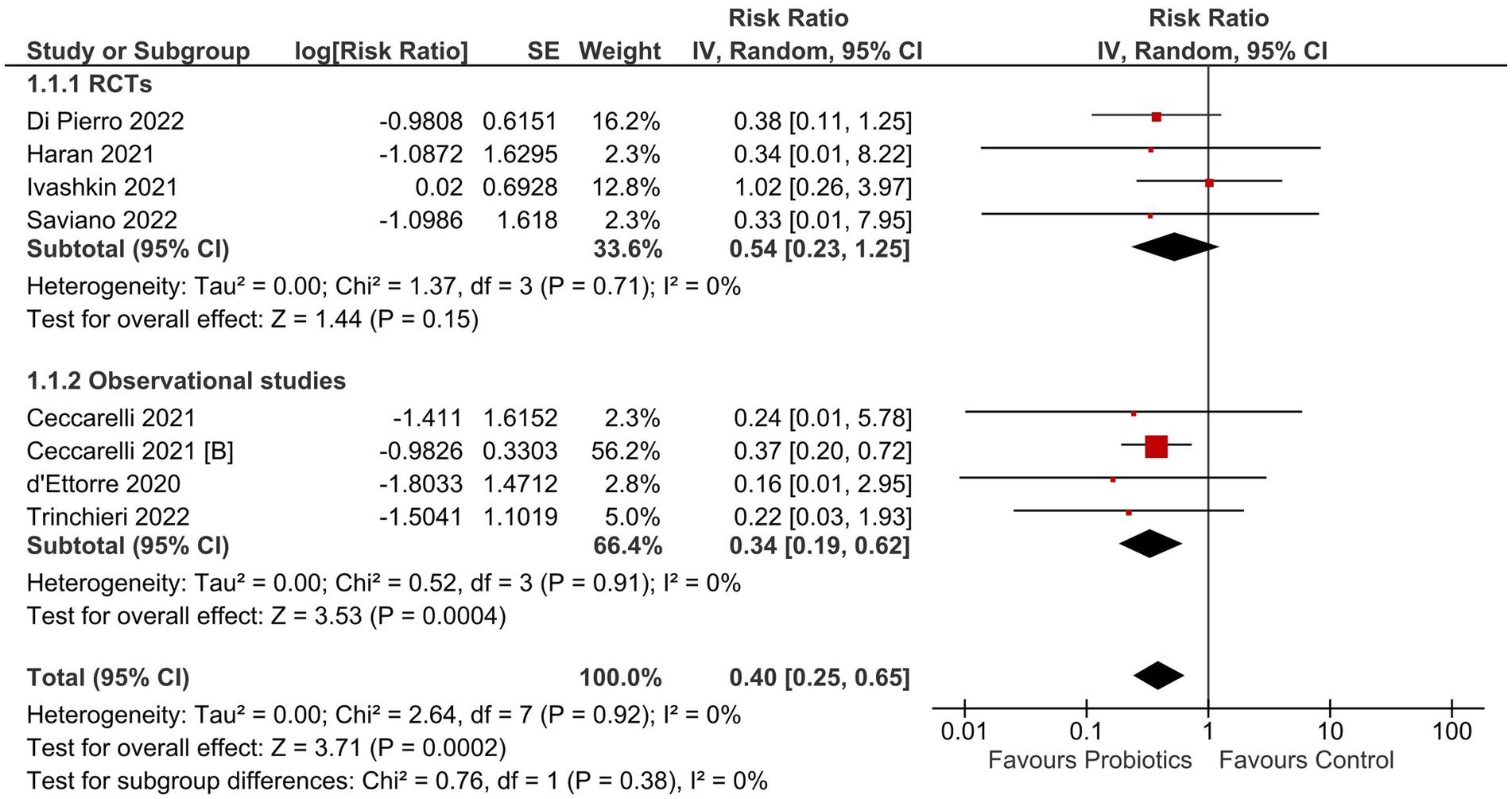
Figure 3. Effect of probiotics on all-cause mortality in COVID-19 patients.
Probiotics had no effect on the rates of ICU admission (RR 0.79; 95% CI: 0.52–1.20; I2 = 0%; Supplementary Figure S1). The length of hospital stay was significantly reduced with probiotics (MD -2.52 days; 95% CI: −4.66 to −0.38 days; I2 = 67%; Supplementary Figure S2). Probiotics reduced the rate of no recovery (RR 0.66; 95% CI: 0.55–0.78; I2 = 0%; Supplementary Figure S3) and decreased the time to recovery (MD -2.18 days; 95% CI: −3.87 to −0.48 days; I2 = 82%; Supplementary Figure S4). When taken prophylactically, probiotics did not decrease the incidence of COVID-19 cases (RR 0.65; 95% CI: 0.37–1.12; I2 = 66%; Supplementary Figure S5). The results for all outcomes were consistent across the subgroups of RCTs and observational studies (P for interaction >0.05).
Sensitivity analysis by excluding Shah et al. (18) which combined probiotics with a systemic enzyme complex produced no significant changes in the results of the length of hospital stay (MD -3.47 days; 95% CI: −5.22 to −1.72 days; I2 = 0%) and recovery time (MD -2.49 days; 95% CI: −4.51 to −0.48 days; I2 = 83%).
To the best of our knowledge, this is the most comprehensive meta-analysis to date which evaluates the therapeutic efficacy of probiotics in treating and preventing COVID-19. A previous meta-analysis by Neris Almeida Viana et al. assessed only the symptomatic recovery of COVID-19 patients and did not include several large and important studies (11). Other meta-analyses also have an outdated search and did not include several recent studies (12, 13). Moreover, none of these meta-analyses evaluated the role of probiotics as a prophylactic therapy. In this study, we assessed several important clinical outcomes such as mortality and ICU admission, which increases the reliability of our conclusions regarding the efficacy of probiotics. The primary findings of our study indicate that probiotics are effective in reducing the risk of mortality in COVID-19 patients by 60%. Probiotics also decreased the duration of hospitalization and recovery time. However, no benefit was found when given as prophylaxis for COVID-19.
The effectiveness of probiotics in therapy can be explained through intricate pathways and potential anatomical connections, primarily involving the gut-lung axis (GLA) (36, 37). The mesenteric lymphatic system serves as the conduit between the intestines and the lungs, facilitating the passage of intact bacteria, their components, or metabolites across the intestinal barrier into the systemic circulation. This process can subsequently impact the immune response within the lungs (38, 39). Dysbiosis in the gut microbiota has been documented in individuals with COVID-19, and this dysbiosis may arise either as a result of the COVID-19 infection itself or due to the antiviral medications administered during treatment (40). Consequently, the use of probiotics in COVID-19 patients could potentially offer advantages in preserving the equilibrium of the gut microbiota (10). In addition to their effects within the gastrointestinal tract, probiotics have demonstrated the potential to confer health benefits through various mechanisms. These mechanisms encompass immunomodulation, the maintenance of epithelial barrier function, and the modulation of signal transduction pathways (41). Therefore, probiotics may improve the clinical outcomes in COVID-19 patients along with other COVID-19 symptoms like diarrhea.
Numerous treatment modalities such as antivirals, immunomodulatory agents, monoclonal antibodies, repurposed drugs, and herbal therapies have been investigated for COVID-19 since the beginning of the pandemic (42–46). However, many factors such as low availability, high costs, and questionable efficacy hinder their widespread use (2, 3, 47, 48). Thus, probiotics prove to be an efficacious, inexpensive, and readily available treatment alternative for COVID-19. However, the findings of our study do not support the use of probiotics for prophylaxis as the association with the incidence of COVID-19 cases was reported to be insignificant. Future research should evaluate the efficacy of probiotics against newer COVID-19 variants as well as comparative efficacy in relation to other treatment modalities.
Several limitations should be considered when interpreting the findings of our study. First, this is a pooled analysis of individual studies, and a patient-level analysis was not conducted as we did not have access to the individual patient data. Second, the inclusion of observational studies might have introduced confounding bias; however, this was mitigated by pooling RCTs separately from observational studies. Third, the considerable heterogeneity in the population and intervention across the included studies in terms of disease severity, and composition and dose of probiotics precluded any attempts to conduct subgroup analyses on these potential effect modifiers. Therefore, our results may not be generalizable to some probiotic strains or a spectrum of disease severity. Lastly, only a few included studies were of high quality as most demonstrated poor internal validity.
In conclusion, treatment with probiotics contributes to improved clinical outcomes including a decreased mortality rate and faster recovery. However, further large-scale trials are warranted for determining the most efficacious probiotic strains and regimens and evaluating the safety of these regimens.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
ArS: Conceptualization, Data curation, Formal analysis, Validation, Writing – original draft, Writing – review & editing. HC: Conceptualization, Data curation, Formal analysis, Writing – original draft, Writing – review & editing. MM: Formal analysis, Writing – original draft, Writing – review & editing. AbS: Data curation, Writing – original draft, Writing – review & editing. AhN: Formal analysis, Writing – original draft, Writing – review & editing. AH: Formal analysis, Writing – original draft, Writing – review & editing. SC: Writing – original draft, Writing – review & editing. AbN: Writing – original draft, Writing – review & editing. IC-O: Conceptualization, Writing – original draft, Writing – review & editing. RA: Conceptualization, Writing – original draft, Writing – review & editing. SA: Conceptualization, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
AN was employed by Hamad Medical Corporation.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2023.1274122/full#supplementary-material
1. Lamontagne, F, Agarwal, A, Rochwerg, B, Siemieniuk, RA, Agoritsas, T, Askie, L, et al. A living WHO guideline on drugs for covid-19. BMJ. (2020) 370:m3379. doi: 10.1136/bmj.m3379
2. Rayner, CR, Dron, L, Park, JJH, Decloedt, EH, Cotton, MF, Niranjan, V, et al. Accelerating clinical evaluation of repurposed combination therapies for COVID-19. Am J Trop Med Hyg. (2020) 103:1364–6. doi: 10.4269/ajtmh.20-0995
3. Dal-Ré, R, Becker, SL, Bottieau, E, and Holm, S. Availability of oral antivirals against SARS-CoV-2 infection and the requirement for an ethical prescribing approach. Lancet Infect Dis. (2022) 22:e231–8. doi: 10.1016/s1473-3099(22)00119-0
4. Fatima, M, Azeem, S, Saeed, J, Shahid, A, and Cheema, HA. Efficacy and safety of molnupiravir for COVID-19 patients. Eur J Intern Med. (2022) 102:118–21. doi: 10.1016/j.ejim.2022.05.024
5. Cheema, HA, Jafar, U, Sohail, A, Shahid, A, Sahra, S, Ehsan, M, et al. Nirmatrelvir–ritonavir for the treatment of COVID-19 patients: a systematic review and meta-analysis. J Med Virol. (2023) 95:e28471. doi: 10.1002/jmv.28471
6. Cheema, HA, Ali, A, Ali, M, Shahid, A, Ghafoor, MS, Ur Rehman, ME, et al. Efficacy and safety of Favipiravir for the treatment of COVID-19 outpatients: a systematic review and meta-analysis of randomized controlled trials. Am J Ther. (2023). doi: 10.1097/MJT.0000000000001649
7. Martín, R, and Langella, P. Emerging health concepts in the probiotics field: streamlining the definitions. Front Microbiol. (2019) 10:1047. doi: 10.3389/fmicb.2019.01047
8. Zhao, Y, Dong, BR, and Hao, Q. Probiotics for preventing acute upper respiratory tract infections. Cochrane Database Syst Rev. (2022) 8:CD006895. doi: 10.1002/14651858.CD006895.pub4
9. Cheema, HA, Shahid, A, Ayyan, M, Mustafa, B, Zahid, A, Fatima, M, et al. Probiotics for the prevention of ventilator-associated pneumonia: an updated systematic review and Meta-analysis of randomised controlled trials. Nutrients. (2022) 14:1600. doi: 10.3390/nu14081600
10. Xavier-Santos, D, Padilha, M, Fabiano, GA, Vinderola, G, Gomes Cruz, A, Sivieri, K, et al. Evidences and perspectives of the use of probiotics, prebiotics, synbiotics, and postbiotics as adjuvants for prevention and treatment of COVID-19: a bibliometric analysis and systematic review. Trends Food Sci Technol. (2022) 120:174–92. doi: 10.1016/j.tifs.2021.12.033
11. Neris Almeida Viana, S, do Reis Santos Pereira, T, de Carvalho Alves, J, Tianeze de Castro, C, Santana C Da Silva, L, Henrique Sousa Pinheiro, L, et al. Benefits of probiotic use on COVID-19: a systematic review and meta-analysis. Crit Rev Food Sci Nutr. (2022):1–13. doi: 10.1080/10408398.2022.2128713
12. Wu, J-Y, Huang, P-Y, Liu, T-H, Kuo, C-Y, Tsai, Y-W, Tang, H-J, et al. Clinical efficacy of probiotics in the treatment of patients with COVID-19: a systematic review and meta-analysis of randomized controlled trials. Expert Rev Anti-Infect Ther. (2023) 21:667–74. doi: 10.1080/14787210.2023.2189100
13. Zhu, J, Pitre, T, Ching, C, Zeraatkar, D, and Gruchy, S. Safety and efficacy of probiotic supplements as adjunctive therapies in patients with COVID-19: a systematic review and meta-analysis. PLoS One. (2023) 18:e0278356. doi: 10.1371/journal.pone.0278356
14. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
15. Sterne, JAC, Savović, J, Page, MJ, Elbers, RG, Blencowe, NS, Boutron, I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. (2019) 366:l4898. doi: 10.1136/bmj.l4898
16. Wells, G, Shea, B, O’Connell, D, and Peterson, J. The Newcastle-Ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa: Ottawa Hosp Res Inst (2000) Available at: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.
17. Borenstein, M, Hedges, LV, Higgins, JPT, and Rothstein, HR. A basic introduction to fixed-effect and random-effects models for meta-analysis. Res Synth Methods. (2010) 1:97–111. doi: 10.1002/jrsm.12
18. Shah, N, Parate, R, and Vispute, A. Potential of the combination of a systemic enzyme complex and probiotics administration to combat COVID-19: a randomized open label prospective analysis. Adv Clin Toxicol. (2021) 6:205. doi: 10.23880/act-16000205
19. d'Ettorre, G, Ceccarelli, G, Marazzato, M, Campagna, G, Pinacchio, C, Alessandri, F, et al. Challenges in the management of SARS-CoV2 infection: the role of oral bacteriotherapy as complementary therapeutic strategy to avoid the progression of COVID-19. Front Med. (2020) 7:389. doi: 10.3389/fmed.2020.00389
20. Gutiérrez-Castrellón, P, Gandara-Martí, T, Abreu AT, AY, Nieto-Rufino, CD, López-Orduña, E, Jiménez-Escobar, I, et al. Probiotic improves symptomatic and viral clearance in Covid19 outpatients: a randomized, quadruple-blinded, placebo-controlled trial. Gut Microbes. (2022) 14:2018899. doi: 10.1080/19490976.2021.2018899
21. Navarro-López, V, Hernández-Belmonte, A, Pérez Soto, MI, Ayo-González, M, Losa-Rodríguez, G, Ros-Sánchez, E, et al. Oral intake of Kluyveromyces marxianus B0399 plus Lactobacillus rhamnosus CECT 30579 to mitigate symptoms in COVID-19 patients: a randomized open label clinical trial. Med Microecol. (2022) 14:100061. doi: 10.1016/J.MEDMIC.2022.100061
22. Rodriguez-Blanque, R, Sánchez-García, JC, Cobos-Vargas, Á, Aguilar Quesada, A, Maldonado-Lobón, JA, Olivares, M, et al. Evaluation of the effect of Loigolactobacillus coryniformis K8 CECT 5711 consumption in health care workers exposed to COVID-19. Front Nutr. (2022) 9:1771. doi: 10.3389/FNUT.2022.962566/BIBTEX
23. Saviano, A, Potenza, A, Siciliano, V, Petruzziello, C, Tarli, C, Migneco, A, et al. COVID-19 pneumonia and gut inflammation: the role of a mix of three probiotic strains in reducing inflammatory markers and need for oxygen support. J Clin Med. (2022) 11:3758. doi: 10.3390/jcm11133758
24. Trinchieri, V, Marazzato, M, Ceccarelli, G, Lombardi, F, Piccirilli, A, Santinelli, L, et al. Exploiting Bacteria for improving hypoxemia of COVID-19 patients. Biomedicine. (2022) 10:1851. doi: 10.3390/biomedicines10081851
25. Wischmeyer, PE, Tang, H, Ren, Y, Bohannon, L, Ramirez, ZE, Andermann, TM, et al. Daily Lactobacillus probiotic versus placebo in COVID-19-exposed household contacts (PROTECT-EHC): a randomized clinical trial. medRxiv. (2022). doi: 10.1101/2022.01.04.21268275
26. Di Pierro, F, Iqtadar, S, Mumtaz, SU, Bertuccioli, A, Recchia, M, Zerbinati, N, et al. Clinical effects of Streptococcus salivarius K12 in hospitalized COVID-19 patients: results of a preliminary study. Microorganisms. (2022) 10:1926. doi: 10.3390/MICROORGANISMS10101926
27. Ivashkin, V, Fomin, V, Moiseev, S, Brovko, M, Maslennikov, R, Ulyanin, A, et al. Efficacy of a probiotic consisting of Lacticaseibacillus rhamnosus PDV 1705, Bifidobacterium bifidum PDV 0903, Bifidobacterium longum subsp. infantis PDV 1911, and Bifidobacterium longum subsp. longum PDV 2301 in the treatment of hospitalized patients with COVID-19: a randomized controlled trial. Probiotics Antimicrob Proteins. (2023) 15:460–8. doi: 10.1007/s12602-021-09858-5
28. Ahanchian, H, Ranjbar, A, Reihani, H, Yazdi, AP, Jafari, SA, Kiani, MA, et al. Synbiotic for prevention of SARS-Cov2 infection in high risk hospital staffs: a randomized controlled trial. Open J Nurs. (2021) 11:281–90. doi: 10.4236/OJN.2021.115025
29. Ceccarelli, G, Marazzato, M, Celani, L, Lombardi, F, Piccirilli, A, Mancone, M, et al. Oxygen sparing effect of bacteriotherapy in COVID-19. Nutrients. (2021) 13:2898. doi: 10.3390/nu13082898
30. Di Pierro, F, and Colombo, M. The administration of S. salivarius K12 to children may reduce the rate of SARS-CoV-2 infection. Minerva Med. (2021) 112:514–6. doi: 10.23736/S0026-4806.21.07487-5
31. Haran, JP, Zheng, Y, Knobil, K, Palma, NA, Lawrence, JF, and Wingertzahn, MA. Targeting the microbiome with KB109 in outpatients with mild to moderate COVID-19 reduced medically attended acute care visits and improved symptom duration in patients with comorbidities. medRxiv. (2021). doi: 10.1101/2021.03.26.21254422
32. Li, Q, Cheng, F, Xu, Q, Su, Y, Cai, X, Zeng, F, et al. The role of probiotics in coronavirus disease-19 infection in Wuhan: a retrospective study of 311 severe patients. Int Immunopharmacol. (2021) 95:107531. doi: 10.1016/J.INTIMP.2021.107531
33. Louca, P, Murray, B, Klaser, K, Graham, MS, Mazidi, M, Leeming, ER, et al. Modest effects of dietary supplements during the COVID-19 pandemic: insights from 445 850 users of the COVID-19 symptom study app. BMJ Nutr Prev Health. (2021) 4:149–57. doi: 10.1136/bmjnph-2021-000250
34. Zhang, L, Han, H, Li, X, Chen, C, Xie, X, Su, G, et al. Probiotics use is associated with improved clinical outcomes among hospitalized patients with COVID-19. Ther Adv Gastroenterol. (2021) 14:175628482110356. doi: 10.1177/17562848211035670
35. Ceccarelli, G, Borrazzo, C, Pinacchio, C, Santinelli, L, Innocenti, GP, Cavallari, EN, et al. Oral bacteriotherapy in patients with COVID-19: a retrospective cohort study. Front Nutr. (2021) 7:341. doi: 10.3389/fnut.2020.613928
36. Li, N, Ma, W-T, Pang, M, Fan, Q-L, and Hua, J-L. The commensal microbiota and viral infection: a comprehensive review. Front Immunol. (2019) 10:10. doi: 10.3389/fimmu.2019.01551
37. Enaud, R, Prevel, R, Ciarlo, E, Beaufils, F, Wieërs, G, Guery, B, et al. The gut-lung axis in health and respiratory diseases: a place for inter-organ and inter-kingdom crosstalks. Front Cell Infect Microbiol. (2020) 10:9. doi: 10.3389/fcimb.2020.00009
38. Bingula, R, Filaire, M, Radosevic-Robin, N, Bey, M, Berthon, J-Y, Bernalier-Donadille, A, et al. Desired turbulence? Gut-lung axis, immunity, and lung cancer. J Oncol. (2017) 2017:5035371–15. doi: 10.1155/2017/5035371
39. McAleer, JP, and Kolls, JK. Contributions of the intestinal microbiome in lung immunity. Eur J Immunol. (2018) 48:39–49. doi: 10.1002/eji.201646721
40. Aguila, EJT, Lontok, MADC, and Aguila, EJT. Letter: role of probiotics in the COVID-19 pandemic. Aliment Pharmacol Ther. (2020) 52:931–2. doi: 10.1111/apt.15898
41. Wan, LYM, Chen, ZJ, Shah, NP, and El-Nezami, H. Modulation of intestinal epithelial defense responses by probiotic Bacteria. Crit Rev Food Sci Nutr. (2016) 56:2628–41. doi: 10.1080/10408398.2014.905450
42. Forrest, JI, Rayner, CR, Park, JJH, and Mills, EJ. Early treatment of COVID-19 disease: a missed opportunity. Infect Dis Ther. (2020) 9:715–20. doi: 10.1007/s40121-020-00349-8
43. Cheema, HA, Shafiee, A, Athar, MMT, Shahid, A, Awan, RU, Afifi, AM, et al. No evidence of clinical efficacy of famotidine for the treatment of COVID-19: a systematic review and meta-analysis. J Infect. (2023) 86:154–225. doi: 10.1016/j.jinf.2022.11.022
44. Cheema, HA, Jafar, U, Elrashedy, AA, Shahid, A, Awan, RU, Ehsan, M, et al. Efficacy and safety of fluvoxamine for the treatment of COVID-19 patients: a systematic review and meta-analysis. J Infect. (2022) 85:702–69. doi: 10.1016/j.jinf.2022.10.012
45. Wang, J, Levi, J, Ellis, L, and Hill, A. Minimum manufacturing costs, national prices, and estimated global availability of new repurposed therapies for coronavirus disease 2019. Open Forum Infect Dis. (2022) 9:ofab581. doi: 10.1093/ofid/ofab581
46. Cheema, HA, Sohail, A, Fatima, A, Shahid, A, Shahzil, M, Ur Rehman, ME, et al. Quercetin for the treatment of COVID-19 patients: a systematic review and meta-analysis. Rev Med Virol. (2023) 33:e2427. doi: 10.1002/rmv.2427
47. Fatima, U, Rizvi, SSA, Raina, N, Fatima, S, Rahman, S, Kamal, MA, et al. Therapeutic management of COVID-19 patients: clinical manifestation and limitations. Curr Pharm Des. (2021) 27:4223–31. doi: 10.2174/1381612826666201125112719
Keywords: probiotics, COVID-19, SARS-CoV-2, synbiotics, meta-analysis
Citation: Sohail A, Cheema HA, Mithani MS, Shahid A, Nawaz A, Hermis AH, Chinnam S, Nashwan AJ, Cherrez-Ojeda I, Awan RU and Ahmad S (2023) Probiotics for the prevention and treatment of COVID-19: a rapid systematic review and meta-analysis. Front. Nutr. 10:1274122. doi: 10.3389/fnut.2023.1274122
Edited by:
George Grant, University of Aberdeen, United KingdomReviewed by:
Giovanni Tarantino, University of Naples Federico II, ItalyCopyright © 2023 Sohail, Cheema, Mithani, Shahid, Nawaz, Hermis, Chinnam, Nashwan, Cherrez-Ojeda, Awan and Ahmad. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Abdulqadir J. Nashwan, YW5hc2h3YW5AaGFtYWQucWE=; Huzaifa Ahmad Cheema, aHV6YWlmYWFobWFkY2hlZW1hQGdtYWlsLmNvbQ==
†These authors have contributed equally to this work and share first authorship
‡These authors have contributed equally to this work and share senior authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.