
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr., 26 October 2022
Sec. Nutrition and Metabolism
Volume 9 - 2022 | https://doi.org/10.3389/fnut.2022.991277
This article is part of the Research TopicAssociation of Dietary Saturated Fatty Acids, Serum Saturated Fatty Acids and Their Trajectories with Cardiovascular DiseaseView all 5 articles
 Inés Domínguez-López1,2,3†
Inés Domínguez-López1,2,3† Camila Arancibia-Riveros1,2†
Camila Arancibia-Riveros1,2† Anna Tresserra-Rimbau1,2,3Sara Castro-Barquero3,4Rosa Casas3,4
Anna Tresserra-Rimbau1,2,3Sara Castro-Barquero3,4Rosa Casas3,4 Zenaida Vázquez-Ruiz3,5
Zenaida Vázquez-Ruiz3,5 Emilio Ros3,6
Emilio Ros3,6 Montserrat Fitó3,7
Montserrat Fitó3,7 Ramon Estruch3,4
Ramon Estruch3,4 M. Carmen López-Sabater1,2,3
M. Carmen López-Sabater1,2,3 Rosa M. Lamuela-Raventós1,2,3*
Rosa M. Lamuela-Raventós1,2,3*Desaturase enzyme activities (DEA) are associated with several metabolic diseases. The aim of the present study was to assess the relationship between estimated plasma DEA and the metabolic syndrome (MetS), as well as their relationship with individual components of the MetS. We conducted a longitudinal study of 148 participants recruited at random from the PREDIMED trial (Hospital Clinic site). At baseline and after 1 year of follow-up, DEA were estimated from product/precursor ratios of individual plasma fatty acids. Logistic regressions were used to assess the relationship of estimated DEA MetS, adjusted for potential cofounders. Estimated Δ5 desaturase (D5D) activity was associated with lower risk of MetS, whereas stearoyl-CoA (SCD)-16 and SCD-18 were negatively associated with MetS status. SCD-16, SCD-18, and Δ6 desaturase (D6D) were positively associated with triglycerides, SCD-18 was inversely associated with HDL-cholesterol. Estimated D6D activity was found to be associated with increases in diastolic blood pressure. In contrast, D5D was negatively associated with triglycerides, diastolic blood pressure and waist circumference. The present longitudinal study suggests that estimated SCD-16, SCD-18, and D6D have a negative impact in MetS and its components, whereas D5D may have beneficial effects for metabolic health.
The prevalence of metabolic syndrome (MetS) has increased in the last three decades and the global prevalence has been estimated to be about 1 quarter of the world population (1). The prevalence in Spain reached 30% in 2012 (2), and this number is estimated to increase in approximately 94,000 cases every year (3). MetS is defined as a set of criteria that, when grouped together, represent a risk for developing cardiovascular disease (CVD) and type 2 diabetes (T2D), such as elevated blood triglycerides (TG) or glucose (4). The development of MetS can be promoted by unmodifiable risk factors, including genetics or aging, but also by modifiable lifestyle habits, such as physical activity or diet (5). The incidence of MetS is particularly higher in men aged over 45 years with an educational level below university studies. Healthier lifestyle therapies in the management of MetS focus on reducing weight, sedentarism, and improving the diet. It has been reported that the incidence of MetS can be reduced with a higher adherence to the Healthy Lifestyle Score, which includes never smoking, moderate to high physical activity, higher adherence to Mediterranean diet, or moderate alcohol consumption, among others (6). Other studies recommend to reach a greater adherence to Mediterranean diet to reduce its development (3).
The traditional Mediterranean diet has been recognized as protective against the development of MetS and other chronic diseases, such as T2D, CVD, and hypertension (7, 8). This healthy dietary pattern is characterized by a high intake of fruits, vegetables, legumes, nuts, and whole grains, and olive oil (9). The Mediterranean diet provides a high content of healthy fats that mostly come from olive oil and favors a better lipid profile.
The plasma fatty acid (FA) profile is considered a more reliable biomarker of dietary fat intake than food frequency questionnaires (FFQ) (10), but it may also be affected by non-dietary factors, such as endogenous metabolism. FAs can be synthesized, elongated, or desaturated in reactions catalyzed by the enzymes stearoyl-CoA desaturase (SCD-1), Δ6 desaturase (D6D), and Δ5 desaturase (D5D) (11), as shown in Figure 1. Altered desaturase enzyme activities (DEA), calculated with the ratios of the FAs that intervene in the reaction, are associated with cardiometabolic risk factors, such as T2D, obesity and MetS (12, 13). However, studies assessing the effect of estimated DEA on MetS and its individual components remain scarce. We hypothesized that altered ratios of estimated DEA would be associated with MetS and the individual components that constitute it. Thus, the aim of this substudy was to assess the relationship of estimated DEA with MetS and its components after 1 year of follow-up in a Mediterranean population.
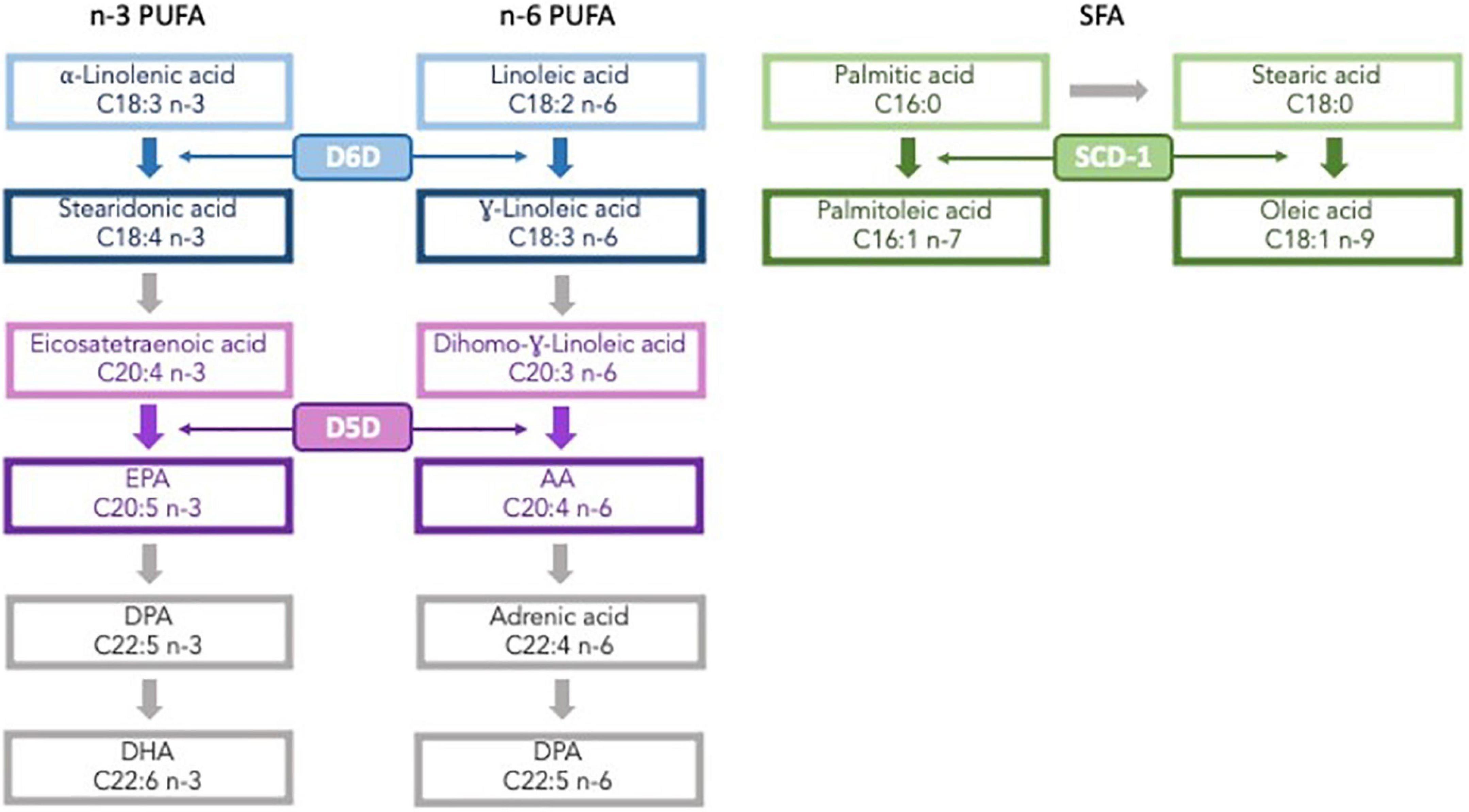
Figure 1. Fatty acid synthetic pathway. PUFA, polyunsaturated fatty acids; D6D, D6 desaturase; D5D, D5 desaturase; EPA, eicosapentaenoic acid; DPA, docosapentaenoic acid; DHA, docosahexaenoic acid; AA, arachidonic acid; SFA, saturated fatty acids; SCD, stearoyl coenzyme A desaturase.
The PREDIMED (PREvención con DIeta MEDiterránea) study was a 5-year large, parallel-group, multicenter, randomized, controlled, clinical trial conducted in Spain from October 2003 to December 2010 with the aim of assessing the effect of a Mediterranean diet on the primary prevention of CVD.1 In summary, 7,447 participants aged 55–80 years at high cardiovascular risk were included. Eligible participants were men and women with T2D, dyslipidemia, hypertension, overweight/obesity or family history of premature CVD. Exclusion criteria included sever chronic illnesses, alcohol or drug abuse, and BMI > 40 kg/m2. A detailed description of methods and participants has been published elsewhere (14).
For the current analysis, we used a randomly selected subsample of participants from the PREDIMED-Hospital Clinic recruitment center. To estimate DEA, a total of 148 participants with available data on plasma FA profiles at baseline and after 1 year of follow-up were included.
The protocol was approved by the Research Ethics Committees at the Hospital Clinic recruiting center and all participants signed a written informed consent form.
A validated semi-quantitative 137-item FFQ was collected by trained dietitians to assess dietary intake at baseline and after 1 year (15). Nutrient intakes were calculated from Spanish food composition tables (16). One female participant who reported implausible energy intakes (>3,500 and <500 Kcal/day for females, and >4,000 and <800 Kcal/day for males) was excluded from the analysis (17). Mediterranean diet adherence was assessed with a 14-item questionnaire with a value of 0 or 1 for each dietary component (18).
Trained personnel carried out anthropometric measurements at baseline and 1-year follow-up. Physical activity was assessed with a validated Spanish version of the Minnesota physical activity questionnaire (19). The anthropometric measurements used in this study were body mass index (BMI), calculated as weight in kg/height2 in m2, and waist circumference (WC). Diastolic and systolic blood pressure (DBP and SBP, respectively) was measured in triplicate with a validated semi-automatic sphygmomanometer after a minimum of 5 mins rest in a seated position.
Blood samples were collected after an overnight fast, coded, and stored at –80C° until analysis. Biochemical analyses [glucose, triglycerides, total cholesterol, and high-density lipoprotein cholesterol (HDL-c)] were performed by standard enzymatic procedures. The FA profile in plasma was determined in total lipids by fast gas chromatography with a flame ionization detector (GC-FID) with a previous derivatization to the corresponding FA methyl esters (FAMEs) (20). Fast analyses were performed on a Shimadzu GC-2010 Gas Chromatograph (Shimadzu, Kyoto, Japan) equipped with an FID and Shimadzu AOC-20i Autoinjector. Separation of FAMEs was carried out on a capillary column (10 m × 0.10 mm i.d.), coated with an SGE-BPX70 cross-linked stationary phase (70% cyanopropyl polysilphenylene-siloxane, 0.20 μm film thickness) from SGE (SGE Europe Ltd., United Kingdom). Methyl ester peaks were identified by comparison of their relative retention times with the standards Supelco 37 component FAMEs mix and PUFA No. 2 (Animal source), purchased form Merck (Darmstadt, Germany). Results were expressed as relative percentages of total FAs.
Plasma FA levels at baseline and changes after 1-year of follow-up are detailed in Supplementary Table 1 according to MetS status.
DEA were estimated as the product/precursor ratios of FAs in plasma according to the following: SCD-16 = C16:1 n – 7/C16:0, SCD–18 = C18:1 n – 9/C18:0, D6D = C18:3 n – 6/C18:2 n – 6, and D5D = C20:4 n – 6/C20:3 n – 6 (11).
For the present work we applied the definition of MetS proposed by six major organizations and societies (IDF, NHLBI, AHA, WHF, IAC, and IASO) (21). Accordingly, participants who presented 3 of 5 of the following risk factors were included in the MetS group: elevated TG (>150 mg/dL or drug treatment for elevated TG), reduced HDL-c (< 40 mg/dL in men and <50 mg/dL in women), elevated blood pressure (SBP > 130 and/or DBP > 85 mmHg, or antihypertensive drug treatment), elevated fasting glucose (>100 mg/dL or drug treatment of elevated glucose), and elevated WC (>102 cm for men and >88 for women).
Baseline characteristics of the participants with and without MetS are presented as means ± SD for continuous variables and percentages for categorical variables. T-tests were used to assess differences in continuous variables and Chi-Square tests were used for categorical values. T-tests were also used to assess differences in plasma FA profile between participants with and without MetS, as well as within-group differences between baseline and 1-year of follow-up.
Baseline values and 1-year changes of estimated DEA were normalized and scaled in multiples of 1-SD with Blom inverse normal transformation (22). Changes in estimated DEA and MetS components were calculated as a 1-year value minus the baseline value.
The associations between the prevalence of MetS and estimated DEA were assessed with a logistic regression analysis to calculate the odds ratios (OR) and 95% confidence interval (CI) adjusting for potential confounders (sex, age, physical activity, BMI, smoking status, educational level, and total energy intake) and stratifying for sex. Multinomial logistic regression was employed to assess the relative risk ratio (RRR) of 1-year changes in MetS status and in estimated DEA, also stratifying for sex, and incorporating the intervention group into the adjustment models.
Multivariable adjusted linear regression models were used to assess differences between estimated DEA per 1-SD increase and MetS components (TG, HDL-c, DBP, SBP, glucose, and WC). The adjustment model for potential confounders included: sex, age, physical activity, smoking status, educational level, total energy intake, and BMI (except for WC). In addition, related medication was added in the adjustment model for each MetS component: TG and HDL-c were further adjusted for cholesterol-lowering drugs; DBP and DSP were further adjusted for antihypertensive medication; glucose was further adjusted for insulin and other hypoglycemic drugs; SCD-16 and SCD-18 were further adjusted for PUFA intake. The longitudinal analysis considering 1-year changes in estimated DEA and MetS components was carried out using the same models, further adjusted for the intervention groups.
For all analyses, two-sided significance was determined at a p < 0.05. Analyses were performed with Stata 16.0 (Stata-Corp LP, TX, USA).
Table 1 shows the baseline characteristics of the 148 participants according to MetS status. Approximately two thirds of the participants had MetS, whereas 47 volunteers were considered to not suffer from this syndrome. Among the participants with MetS, the majority were women (62.4%), whereas among those without MetS, the majority were men (57.4%). As expected, more participants with MetS suffered from T2D (83.2%), had higher BMI (29.5 ± 3.8 kg/m2) and performed less physical activity (249 ± 237.3 METS-min/day). Surprisingly, a higher percentage of participants without MetS had dyslipidaemia (82.98%).
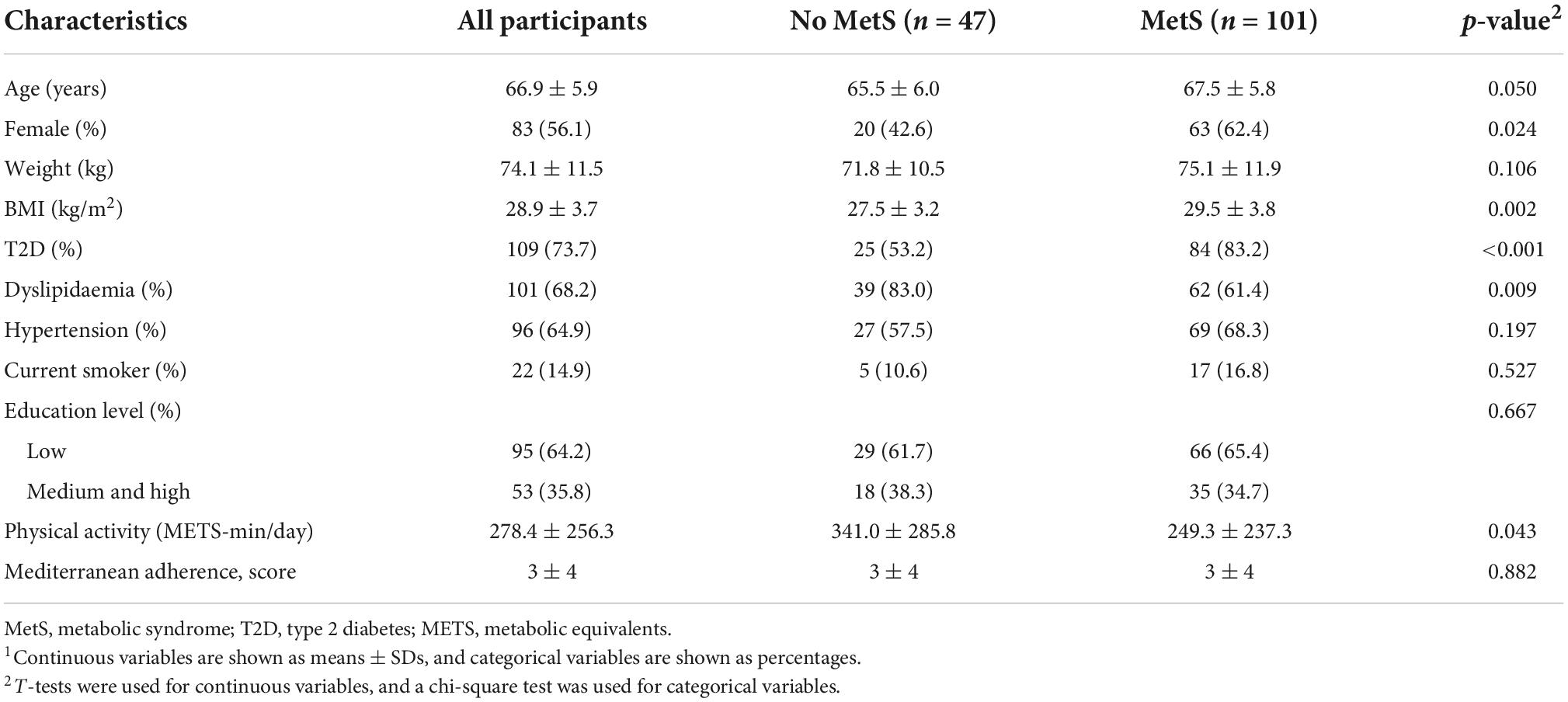
Table 1. Baseline characteristics of participants according to MetS1.
Dietary intake of all participants and stratified for MetS are in Table 2. The mean energy intake was 2,515.6 ± 541.1 kcal/day and the most consumed type of fat were monounsaturated fatty acids (MUFA). The two groups of participants with and without MetS were well-balanced and there were no differences in any nutrient except for polyunsaturaded fatty acids (PUFA) intake, as those with MetS reported significantly lower consumption (17.1 ± 6.6 g/day).
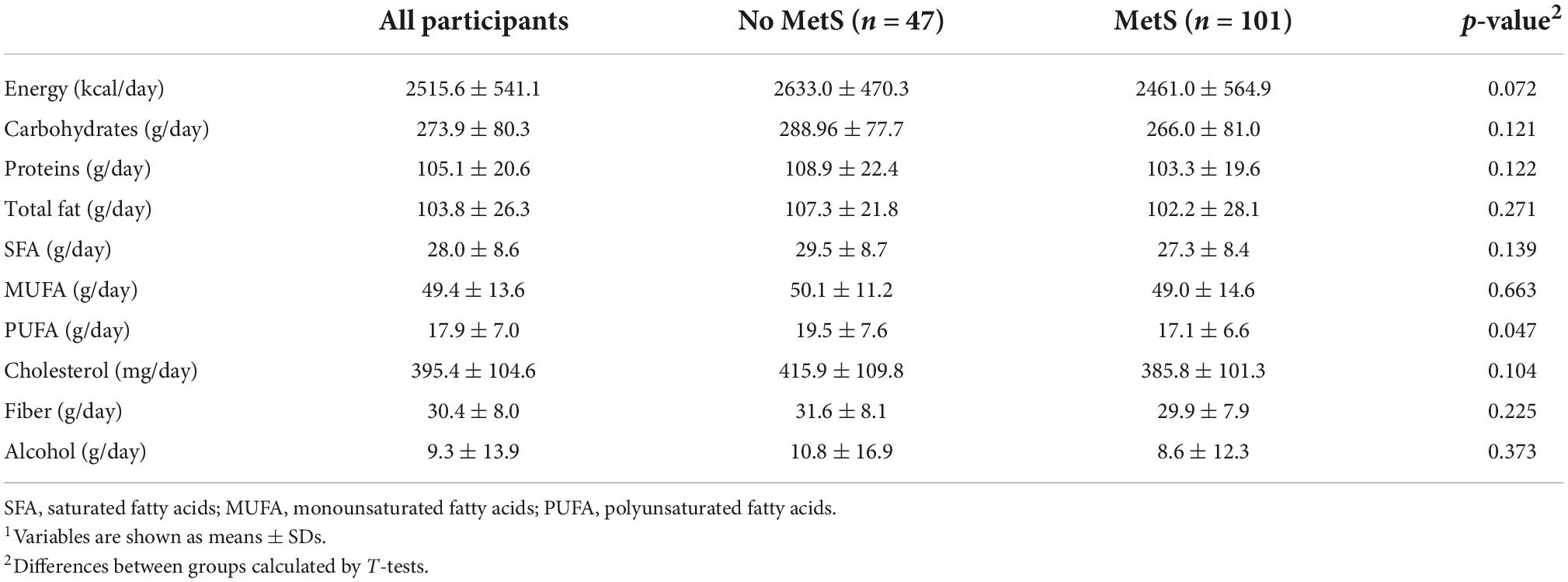
Table 2. Dietary intake for all participants and according to MetS at baseline1.
The OR of having MetS according to estimated DEA per 1-SD increase at baseline are shown in Table 3. The logistic regression model showed that in all participants higher rates of D5D activity were associated with lower incidence of MetS [OR = 0.53 (95% CI: 0.36; 0.79), p-value = 0.002]. Higher SCD-18 activity tended to lower the incidence of MetS, although it did not achieve statistical significance [OR = 1.54 (95% CI: 0.96; 2.58), p-value = 0.096].
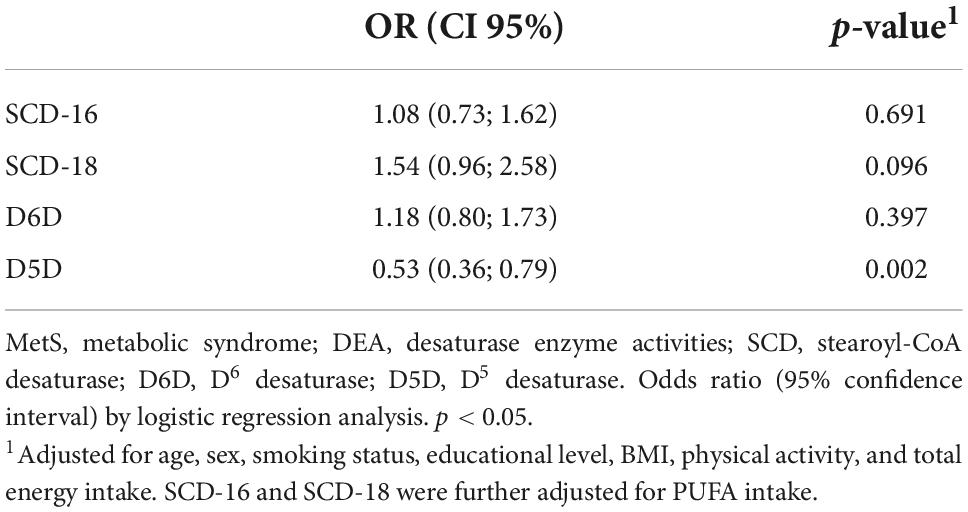
Table 3. Odds ratio associated with having MetS with DEA according to sex at baseline per 1-SD increase (n = 148).
The associations between estimated DEA per 1-SD and MetS components after full adjustment are shown in Table 4. Higher estimated SCD-18 and D6D activity were positively associated with higher concentrations of TG [β = 40.50 (95% CI: 23.00; 58.02) per 1-SD increase, p-value = 0.001, and β = 15.45 (95% CI: 1.57; 29.33) per 1-SD increase, p-value = 0.029, respectively]. Higher rates of estimated SCD-18 activity were also associated with lower HDL-c [β = –4.02 (95% CI: –6.20; –1.85) per 1-SD increase, p-value = < 0.001]. Lastly, DBP and WC were inversely associated with estimated D5D activity [β = –1.79 (95% CI: –3.10; 0.48) per 1-SD increase, p-value = 0.008, and β = –0.94 (95% CI: –1.82; 0.06) per 1-SD increase, p-value = 0.037].
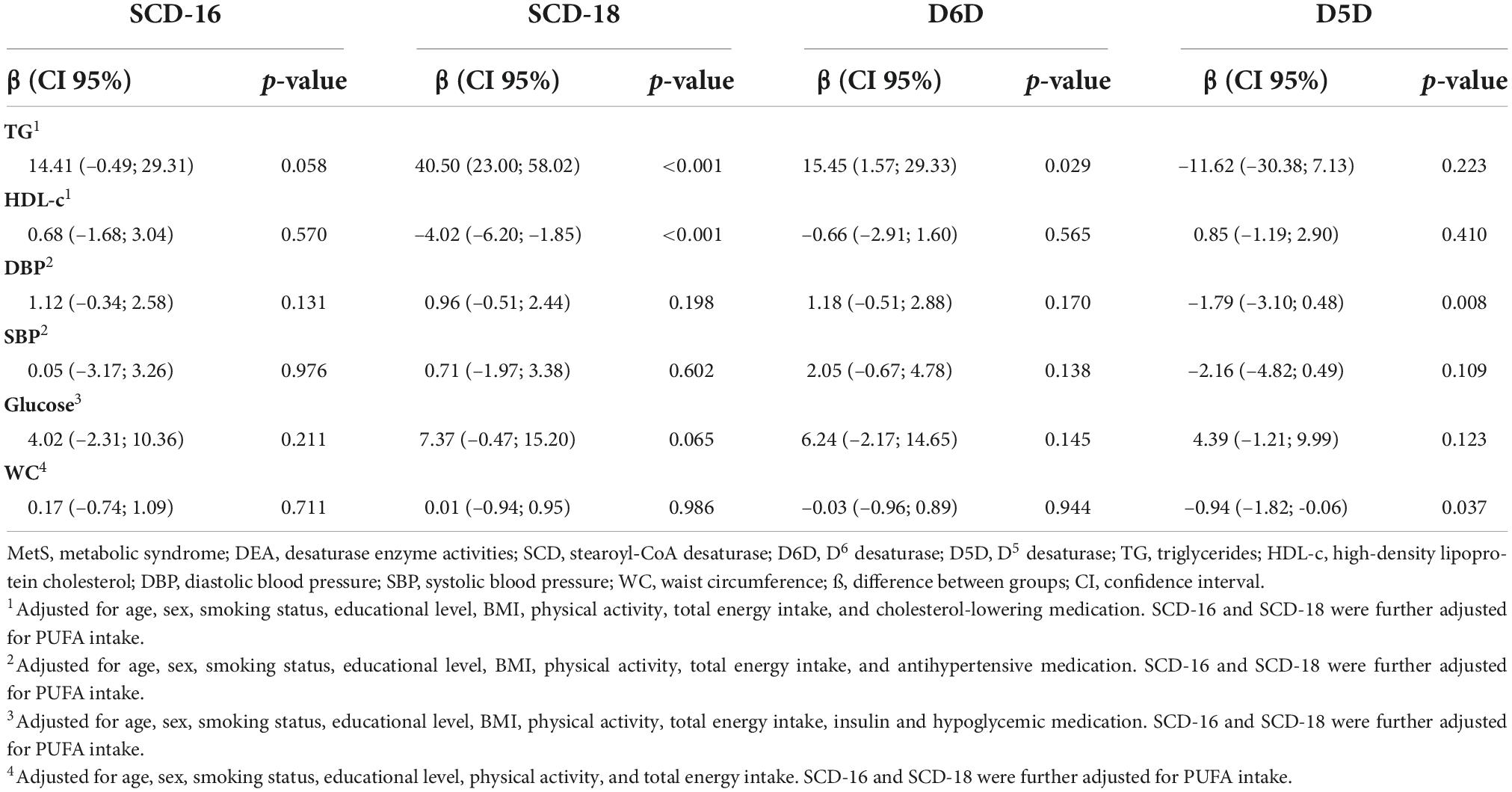
Table 4. Multivariable-adjusted regression for estimated DEA per 1-SD increase and MetS components at baseline.
The relationship between 1-year changes in MetS status and estimated DEA per 1-SD increase is presented in Table 5. The multinomial regression model showed that increases in estimated D5D activity were associated with MetS improvement [OR = 2.04 (95% CI: 1.18; 3.56), p-value = 0.011], whereas increases in estimated SCD-18 activity were associated with a lower probability of improving MetS status [OR = 0.46 (95% CI: 0.29; 0.71), p-value = 0.001]. In addition, higher estimated SCD-16 activity was associated with an increased risk of worsening MetS status [OR = 2.15 (95% CI: 1.18; 3.94), p-value = 0.013].
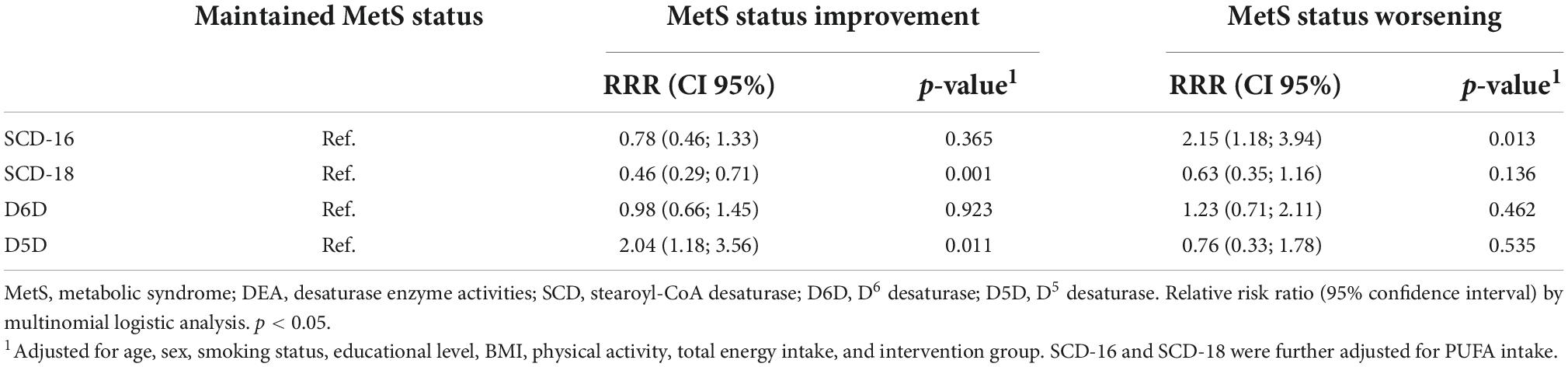
Table 5. Multinomial logistic regression for changes in MetS status and estimated DEA ratios after 1 year of follow-up per 1-SD increase.
Table 6 shows the associations between 1-year changes in DEA per 1-SD increase and MetS components. Changes in estimated SCD-16 and SCD-18 activity were positively associated with higher TG [β = 18.08 (95% CI: 7.02; 29.13) per 1-SD increase, p-value = 0.002, and β = 34.88 (95% CI: 19.97; 49.79) per 1-SD increase, p-value = 0.001, respectively]. Increases in the rate of estimated SCD-18 were associated with decreases in HDL-c concentrations [β = –1.53 (95% CI: –2.62; –0.44) per 1-SD increase, p-value = 0.006], whereas increases in levels of estimated D6D activity were associated with higher DBP [β = 1.70 (95% CI: 0.44; 2.97) per 1-SD increase, p-value = 0.009]. Finally, we observed a decrease in TG and DBP when estimated D5D activity increased [β = –13.09 (95% CI: –24.99; –1.19) per 1-SD increase, p-value = 0.031, and β = –1.52 (95% CI: –2.78; –0.26) per 1-SD increase, p-value = 0.018, respectively].
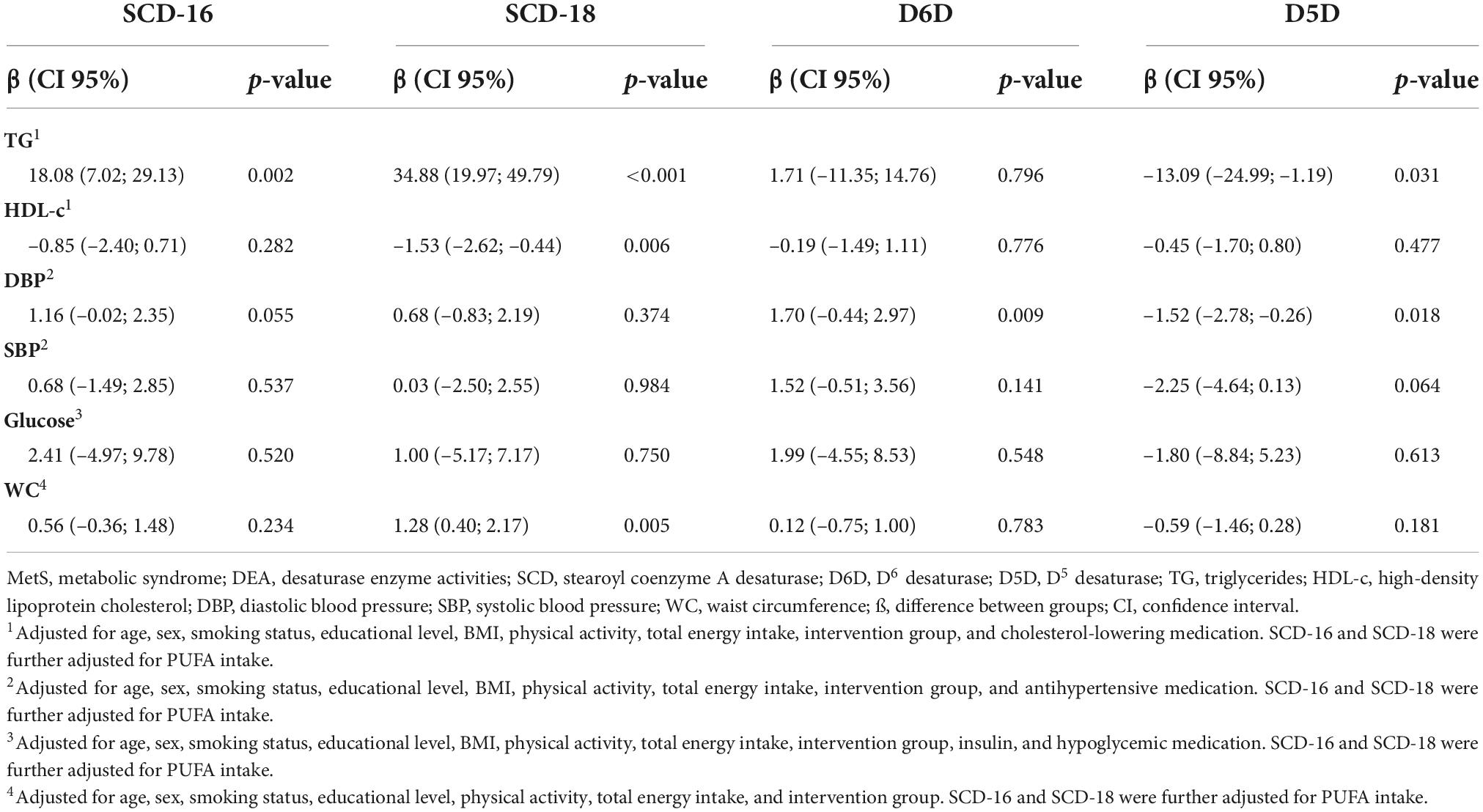
Table 6. Multivariable-adjusted regression for 1-year changes in estimated DEA per 1-SD increase and MetS components.
In the present longitudinal substudy of the PREDIMED trial, we observed that higher estimated activities of SCD-16, SCD18, and D6D had an adverse effect on MetS status and its components after 1 year of follow-up. In contrast, estimated D5D activity showed a protective effect against MetS and its components, particularly TG and DBP. To our knowledge, this is the first study to assess the effect of estimated DEA with MetS and its components after 1 year of follow-up in a Mediterranean population.
The activity of these desaturases is known to be related to metabolic health. Differences in the plasma FA profile and estimated DEA have been previously described between metabolically healthy and unhealthy individuals (23, 24). On this basis, Svendsen et al. proposed that these enzymatic activities could serve as novel biomarkers of metabolic health (13, 25). This is in accordance with the results of the present study, as we found that estimated DEA were associated with MetS at baseline and after 1 year of follow-up.
The analysis of plasma estimated DEA related to FA metabolism showed a beneficial effect of estimated D5D activity on the prevalence of MetS. These results are consistent with previous studies that report a positive influence of D5D on cardiovascular health. For example, higher D5D activity has been favorably associated with stroke risk factors, T2D, and abdominal obesity (26–28). D5D is the rate-limiting enzyme that catalyzes the transformation of eicosatetraenoic and dihomo-gamma-linoleic acid into eicosapentaenoic acid (EPA) and arachidonic acid (AA), respectively. Therefore, lower D5D activity leads to the accumulation of precursors and other intermediate FAs that increase cardiometabolic risk, such as gamma-linoleic or dihomo-gamma-linoleic acid (29). Despite all these findings, Mayneris-Perxachs et al. did not observe any association between D5D and the odds of having MetS in a cross-sectional sub-analysis with baseline data of the PREDIMED study (30). However, they did find that D6D and SCD-18 were adversely associated with MetS, which is consistent with our results. The activity of D6D, the key enzyme in the conversion of linoleic and alpha-linoleic acid, and SCD-1, which catalyzes the synthesis of MUFA from saturated fatty acids (SFA), is inhibited by PUFA intake (31). In this regard, evidence obtained in clinical trials has shown that diets with high intakes of PUFA down-regulate SCD-1 activity (32), particularly PUFA resulting from fish consumption (33). However, in relation with our findings, including PUFA intake as a confounder variable in the analyses of SCD-16 and SCD-18 minimally altered the results, suggesting that their associations with MetS and its components were not dependent on PUFA intake. Overall, our findings confirm the results of previous studies in which elevated D5D and reduced D6D and SCD-1 activities positively impacted cardiometabolic risk factors (24, 34).
SCD-16, SCD-18, and D6D are generally known to exert negative effects on metabolic health and other CVD risk factors. SCD-16 and SCD-18 have also been positively associated with BMI, blood pressure, and total cholesterol (35, 36), which is in accordance with our results. Other studies have found that D6D is related to higher TG, blood pressure, BMI and total cholesterol (37, 38). Moreover, D6D has showed a positive association with inflammatory biomarkers, such as ICAM-1 or C-reactive protein (37, 39), which suggests that this enzyme has a negative effect on metabolic health due to the activation of inflammatory pathways.
In contrast, estimated D5D activity has been favorably associated with MetS components, as it has been to related to higher HDL-c, lower blood pressure, and lower BMI (36, 40). Several mechanisms may explain the associations found between estimated DEA and MetS components. PUFA synthesized by D5D and D6D can modulate the expression of transcription factors that participate in lipogenesis and FA oxidation, such as PPAR. In addition, these FA also produce eicosanoids, which are inflammatory mediators that play major roles in lipogenesis or insulin resistance (41). Taken together, these results suggest that D5D products are involved in antiinflammatory responses and upregulation of transcription factors that lead to a better lipid profile and decreased CVD risk, whereas D6D and SCD products may have the opposite effect.
The main strength of the present study is its longitudinal nature, as this is considered the most rigorous method to establish a cause-effect relationship. Other strengths include the analysis of biological samples. Among the limitations of the study is that all the participants were >55 years and at high risk of CVD, thus the results may not be representative of other populations. Additionally, the sample size was relatively small compared to similar studies.
The present study shows that in a Mediterranean population of over 55 years and at high cardiovascular risk, estimated SCD-16, SCD-18, and D6D activities were adversely associated with MetS, whereas D5D was associated with a protective effect. Among the components that constitute the MetS, TG, HDL-c, DBP, and WC were adversely affected by estimated activities of SCD-16, SCD-18, and D6D. In contrast, D5D was associated with beneficial changes in TG and DBP. Therefore, our results contribute to the hypothesis that FA metabolism influences metabolic health and desaturases dysregulations may be indicative of metabolic alterations. Further research is needed to confirm the current findings in the general population.
The data analyzed in this study is subject to the following licenses/restrictions: The datasets presented in this article are not readily available because there are restrictions on the availability of data for the PREDIMED trial, due to the signed consent agreements around data sharing. Requestors wishing to access the PREDIMED-dataset generated and/or analyzed during the current study can make a request to the PREDIMED trial Steering Committee chair. Requests to access these datasets should be directed to RL-R, bGFtdWVsYUB1Yi5lZHU=.
The studies involving human participants were reviewed and approved by the Research Ethics Committees at the Hospital Clinic recruiting center and all participants signed a written informed consent form. The patients/participants provided their written informed consent to participate in this study.
ID-L: conceptualization, investigation, formal analysis, and writing – original draft. CA-R: methodology and writing – original draft. AT-R, RC, and ZV-R: writing – review and editing. SC-B: methodology and writing – review and editing. ER, MF, and RE: investigation and writing – review and editing. ML-S: formal analysis and writing – review and editing. RL-R: conceptualization, investigation, and writing – review and editing. All authors contributed to the article and approved the submitted version.
This research has been supported by the CICYT [PID2020-114022RB-I00], CIBEROBN from the Instituto de Salud Carlos III, ISCIII from the Ministerio de Ciencia, Innovación y Universidades (AEI/FEDER, UE), and Generalitat de Catalunya (GC) [2017SGR 196]. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
The PREDIMED trial was supported by the official funding agency for biomedical research of the Spanish government (Instituto de Salud Carlos III) through grants provided to research networks specifically developed for the trial: RTIC G03/140 (Coordinator: RE) and RTIC RD 06/0045 (Coordinator: Miguel Ángel Martínez-González). All investigators of the PREDIMED trial belong to Centro de Investigación Biomédica en Red (CIBER), an initiative of Instituto de Salud Carlos III. ID-L and SC-B thank the Spanish Ministry of Science Innovation and Universities for the Formación de Profesorado Universitario (FPU20/02478 and FPU17/00785) contract. AT-R is a Serra Húnter Fellow.
Author ER reports grants, personal fees, non-financial and other from the California Walnut Commission while the study was carried out; grants, personal fees, non-financial support and other from Alexion; and personal fees and other from Amarin, outside the submitted work. Author RL-R reports personal fees from Cerveceros de España, personal fees and other from Adventia, Wine in Moderation, Ecoveritas S.A., outside the submitted work. Author RE reports grants from the Fundación Dieta Mediterránea (Spain), and Cerveza y Salud (Spain), and personal fees for given lectures from Brewers of Europe (Belgium), the Fundación Cerveza y Salud (Spain), Pernaud-Ricard (Mexico), Instituto Cervantes (Alburquerque, United States), Instituto Cervantes (Milan, Italy), Instituto Cervantes (Tokyo, Japan), Lilly Laboratories (Spain), and the Wine and Culinary International Forum (Spain), as well as non-financial support for the organization of a National Congress on Nutrition and feeding trials with products from Grand Fountain and Uriach Laboratories (Spain).
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2022.991277/full#supplementary-material
AA, arachidonic acid; BMI, body mass index; CVD, cardiovascular disease; DBP, diastolic blood pressure; D5D, Δ 5 desaturase; D6D, Δ 6 desaturase; DEA, desaturase enzyme activities; EPA, eicosapentaenoic acid; FA, fatty acids; FAME, fatty acid methyl ester; FID, flame ionization detector; FFQ, food frequency questionnaire; GC, gas chromatography; HDL-c, high-density lipoprotein cholesterol; MetS, metabolic syndrome; MUFA, monounsaturated fatty acid; PUFA, polyunsaturated fatty acid; SFA, saturated fatty acids; SCD, stearoyl-CoA desaturase; SBP, systolic blood pressure; TG, triglycerides; T2D, type 2 diabetes.
2. Fernández-Bergés D, Cabrera De León A, Sanz H, Elosua R, Guembe MJ, Alzamora M, et al. Metabolic syndrome in Spain: Prevalence and coronary risk associated with harmonized definition and who proposal. DARIOS study. Rev Esp Cardiol. (2012) 65:241–8. doi: 10.1016/j.recesp.2011.10.015
3. Cuesta M, Fuentes M, Rubio M, Bordiu E, Barabash A, Garcia De La Torre N, et al. Incidence and regression of metabolic syndrome in a representative sample of the Spanish population: Results of the cohortZGlAYmV0LmVzstudy. BMJ Open Diabetes Res Care. (2020) 8:e001715. doi: 10.1136/bmjdrc-2020-001715
5. Sherling DH, Perumareddi P, Hennekens CH. Metabolic Syndrome: Clinical and policy implications of the new silent killer. J Cardiovasc Pharmacol Ther. (2017) 22:365–7.
6. Garralda-Del-Villar M, Carlos-Chillerón S, Diaz-Gutierrez J, Ruiz-Canela M, Gea A, Martínez-González MA, et al. Healthy lifestyle and incidence of metabolic syndrome in the SUN cohort. Nutrients. (2019) 11:65.
7. Estruch R, Ros E, Salas-Salvadó J, Covas M-I, Corella D, Arós F, et al. Primary prevention of cardiovascular disease with a mediterranean diet supplemented with extra-virgin olive oil or nuts. N Engl J Med. (2018) 378:e34.
8. Salas-Salvadó J, Bulló M, Estruch R, Ros E, Covas M-I, Ibarrola-Jurado N, et al. Prevention of diabetes with mediterranean diets a subgroup analysis of a randomized tria. Ann Intern Med. (2014) 161:157.
9. Bach-Faig A, Berry EM, Lairon D, Reguant J, Trichopoulou A, Dernini S, et al. Mediterranean diet pyramid today. Science and cultural updates. Public Health Nutr. (2011) 14:2274. doi: 10.1017/S1368980011002515
10. Hodson L, Skeaff CM, Fielding BA. Fatty acid composition of adipose tissue and blood in humans and its use as a biomarker of dietary intake. Prog Lipid Res. (2008) 47:348–80.
11. Nakamura MT, Nara TY. Structure, function, and dietary regulation of Δ6, Δ5, and Δ9 desaturases. Annu Rev Nutr. (2004) 24:345–76.
12. Yary T, Voutilainen S, Tuomainen TP, Ruusunen A, Nurmi T, Virtanen JK. Serum n-6 polyunsaturated fatty acids, Δ5- and D6-desaturase activities, and risk of incident type 2 diabetes in men: The Kuopio Ischaemic Heart Disease Risk Factor Study. Am J Clin Nutr. (2016) 103:1337–43. doi: 10.3945/ajcn.115.128629
13. Svendsen K, Olsen T, Nordstrand Rusvik TC, Ulven SM, Holven KB, Retterstøl K, et al. Fatty acid profile and estimated desaturase activities in whole blood are associated with metabolic health. Lipids Health Dis. (2020) 19:102.
14. Martínez-González MA, Buil-Cosiales P, Corella D, Bulló M, Fitó M, Vioque J, et al. Cohort profile: Design and methods of the PREDIMED-Plus randomized trial. Int J Epidemiol. (2019) 48:387.
15. Martin-Moreno JM, Boyle P, Gorgojo L, Maisonneuve P, Fernandez-rodriguez JC, Salvini S, et al. Development and validation of a food frequency questionnaire in Spain. Int J Epidemiol. (1993) 22:512–9.
16. Moreiras OCA, Cabrera L, Cuadrado C. Tablas de Composición de alimentos 7th ed Pirámide, editor. Madrid: Spanish Food Composition Tables (2003).
17. Willett WC, Howe G, Kushi L. Adjustment for total energy intake in epidemiologic studies. Am J Clin Nutr. (1997) 65(Suppl 4):1220S–8S.
18. Martínez-González MÁ, Corella D, Salas-salvadó J, Ros E, Covas MI, Fiol M, et al. Cohort profile: Design and methods of the PREDIMED study. Int J Epidemiol. (2012) 41:377–85.
19. Elosua R, Garcia M, Aguilar A, Molina L, Covas M-I, Marrugat J. Validation of the minnesota leisure time spanish women. Med Sci Sport Exerc. (2000) 32:1431–7.
20. Bondia-Pons I, Castellote AI, López-Sabater MC. Comparison of conventional and fast gas chromatography in human plasma fatty acid determination. J Chromatogr B Anal Technol Biomed Life Sci. (2004) 809:339.
21. Alberti KGMM, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, et al. Harmonizing the metabolic syndrome: A joint interim statement of the international diabetes federation task force on epidemiology and prevention; National heart, lung, and blood institute; American heart association; World heart federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation. (2009) 120:1640–5. doi: 10.1161/CIRCULATIONAHA.109.192644
23. Pavithra N, Bannikoppa PS, Uthappa S, Kurpad AV, Mani I. Plasma fatty acid composition and estimated desaturase activities reflect dietary patterns in subjects with metabolic syndrome. Indian J Clin Biochem. (2018) 33:290–6. doi: 10.1007/s12291-017-0674-1
24. Warensjö E, Risérus U, Vessby B. Fatty acid composition of serum lipids predicts the development of the metabolic syndrome in men. Diabetologia. (2005) 48:1999–2005.
25. Zhao L, Ni Y, Ma X, Zhao A, Bao Y, Liu J, et al. A panel of free fatty acid ratios to predict the development of metabolic abnormalities in healthy obese individuals. Sci Rep. (2016) 6:28418. doi: 10.1038/srep28418
26. Saito E, Okada T, Abe Y, Odaka M, Kuromori Y, Iwata F, et al. Abdominal adiposity is associated with fatty acid desaturase activity in boys: Implications for C-reactive protein and insulin resistance. Prostaglandins Leukot Essent Fat Acids. (2013) 88:307–11. doi: 10.1016/j.plefa.2013.01.005
27. Kröger J, Zietemann V, Enzenbach C, Weikert C, Jansen EHJM, Döring F, et al. Erythrocyte membrane phospholipid fatty acids, desaturase activity, and dietary fatty acids in relation to risk of type 2 diabetes in the European Prospective Investigation into Cancer and Nutrition (EPIC)-Potsdam Study. Am J Clin Nutr. (2011) 93:127–42. doi: 10.3945/ajcn.110.005447
28. Daneshmand R, Kurl S, Tuomainen TP, Virtanen JK. Associations of estimated Δ-5-desaturase and Δ-6-desaturase activities with stroke risk factors and risk of stroke: The kuopio ischaemic heart disease risk factor study. Br J Nutr. (2017) 117:582–90. doi: 10.1017/S000711451700054X
29. Schulze MB, Minihane AM, Saleh RNM, Risérus U. Intake and metabolism of omega-3 and omega-6 polyunsaturated fatty acids: nutritional implications for cardiometabolic diseases. Lancet Diabetes Endocrinol. (2020) 8:915–30. doi: 10.1016/S2213-8587(20)30148-0
30. Mayneris-Perxachs J, Guerendiain M, Castellote AI, Estruch R, Covas MI, Fitó M, et al. Plasma fatty acid composition, estimated desaturase activities, and their relation with the metabolic syndrome in a population at high risk of cardiovascular disease. Clin Nutr. (2014) 33:90–7. doi: 10.1016/j.clnu.2013.03.001
31. Jones BH, Mäher MA, Banz WJ, Zemel MB, Whelan J, Smith PJ, et al. Adipose tissue stearoyl-CoA desaturase mRNA is increased by obesity and decreased by polyunsaturated fatty acids. Am J Physiol. (1996) 271(1 Pt 1):E44–9.
32. Velliquette RA, Gillies PJ, Kris-Etherton PM, Green JW, Zhao G, Vanden Heuvel JP. Regulation of human stearoyl-CoA desaturase by omega-3 and omega-6 fatty acids: Implications for the dietary management of elevated serum triglycerides. J Clin Lipidol. (2009) 3:281–8. doi: 10.1016/j.jacl.2009.06.002
33. Pérez-Heras AM, Mayneris-Perxachs J, Cofán M, Serra-Mir M, Castellote AI, López-Sabater C, et al. Long-chain n-3 PUFA supplied by the usual diet decrease plasma stearoyl-CoA desaturase index in non-hypertriglyceridemic older adults at high vascular risk. Clin Nutr. (2018) 37:157–62. doi: 10.1016/j.clnu.2016.11.009
34. Warensjö E, Öhrvall M, Vessby B. Fatty acid composition and estimated desaturase activities are associated with obesity and lifestyle variables in men and women. Nutr Metab Cardiovasc Dis. (2006) 16:128–36.
35. Murakami K, Sasaki S, Takahashi Y, Uenishi K, Watanabe T, Kohri T, et al. Lower estimates of δ-5 desaturase and elongase activity are related to adverse profiles for several metabolic risk factors in young Japanese women. Nutr Res. (2008) 28:816–24. doi: 10.1016/j.nutres.2008.08.009
36. Do HJ, Chung HK, Moon J, Shin M-J. Relationship between the estimates of desaturase activities and cardiometabolic phenotypes in Koreans. J Clin Biochem Nutr. (2011) 49:131–5. doi: 10.3164/jcbn.10-147
37. Jacobs S, Schiller K, Jansen EHJM, Boeing H, Schulze MB, Kröger J. Evaluation of various biomarkers as potential mediators of the association between Δ5 desaturase, Δ6 desaturase, and stearoyl-CoA desaturase activity and incident type 2 diabetes in the European prospective investigation into cancer and nutrition-potsdam. Am J Clin Nutr. (2015) 102:155–64. doi: 10.3945/ajcn.114.102707
38. Steffen LM, Vessby B, Jacobs DR Jr., Steinberger J, Hong C, Sinaiko AR. Serum phospholipid and cholesteryl ester fatty acids and estimated desaturase activities are related to overweight and cardiovascular risk factors in adolescents. Int J. (2010) 32:1297–304. doi: 10.1038/ijo.2008.89
39. Poudel-Tandukar K, Sato M, Ejima Y, Nanri A, Matsushita Y, Imaizumi K, et al. Relationship of serum fatty acid composition and desaturase activity to C-reactive protein in Japanese men and women. Atherosclerosis. (2012) 220:520–4. doi: 10.1016/j.atherosclerosis.2011.11.012
40. Kim SR, Jeon SY, Lee SM. The association of cardiovascular risk factors with saturated fatty acids and fatty acid desaturase indices in erythrocyte in middle-aged Korean adults. Lipids Health Dis. (2015) 14:133. doi: 10.1186/s12944-015-0135-x
Keywords: fatty acids, desaturases, gas chromatography, PREDIMED, metabolic syndrome, Mediterranean diet
Citation: Domínguez-López I, Arancibia-Riveros C, Tresserra-Rimbau A, Castro-Barquero S, Casas R, Vázquez-Ruiz Z, Ros E, Fitó M, Estruch R, López-Sabater MC and Lamuela-Raventós RM (2022) Relationship between estimated desaturase enzyme activity and metabolic syndrome in a longitudinal study. Front. Nutr. 9:991277. doi: 10.3389/fnut.2022.991277
Received: 11 July 2022; Accepted: 10 October 2022;
Published: 26 October 2022.
Edited by:
Xiaoyan Wu, Guilin Medical University, ChinaReviewed by:
Roser Granero, Universitat Autònoma de Barcelona, SpainCopyright © 2022 Domínguez-López, Arancibia-Riveros, Tresserra-Rimbau, Castro-Barquero, Casas, Vázquez-Ruiz, Ros, Fitó, Estruch, López-Sabater and Lamuela-Raventós. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rosa M. Lamuela-Raventós, bGFtdWVsYUB1Yi5lZHU=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.