
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr. , 07 July 2022
Sec. Nutritional Epidemiology
Volume 9 - 2022 | https://doi.org/10.3389/fnut.2022.928840
This article is part of the Research Topic Nutrition and Oral Health: Public Health Relevance View all 18 articles
 Qingrong Deng1,2†
Qingrong Deng1,2† Yuying Wu1,2†
Yuying Wu1,2† Xiaoying Hu1,2†Huiqing Wu1,2Mengzhu Guo1,2Yimin Lin1,2Menglin Yu1,2Wenwen Huang1,2
Xiaoying Hu1,2†Huiqing Wu1,2Mengzhu Guo1,2Yimin Lin1,2Menglin Yu1,2Wenwen Huang1,2 Yuxuan Wu1,2
Yuxuan Wu1,2 Lisong Lin3
Lisong Lin3 Yu Qiu3
Yu Qiu3 Jing Wang4
Jing Wang4 Baochang He1,2,3
Baochang He1,2,3 Fa Chen1,2*
Fa Chen1,2*Oolong tea is one of the world's most popular non-alcoholic beverages, particularly in coastal Southeast China. Hitherto, epidemiological studies on the association between oolong tea consumption and the risk of patients with oral squamous cell carcinoma (OSCC) are very limited. This study aimed to evaluate the potential effect of oolong tea consumption on OSCC risk in Southeast China. From January 2010 to October 2020, face-to-face interviews were conducted for 744 newly diagnosed OSCC patients and 1,029 healthy controls to collect information on demographics, oolong tea consumption behaviors, and other lifestyle factors. Propensity score matching (PSM), inverse probability of treatment weight (IPTW), and stabilized inverse probability of treatment weight (SIPTW) were utilized to minimize confounding effects. Multivariate, conditional, and weighted logistic regression was used to evaluate the associations of oolong tea consumption behaviors with OSCC risk. Participants who drank oolong tea showed a lower risk of OSCC when compared to their non-drink counterparts [PSM population, OR (95%CI): 0.69 (0.49–0.97); SIPTW population, OR (95%CI): 0.74 (0.58–0.94)]. Moreover, the reduced risk was found to be significantly associated with certain tea-drinking habits (consumed amount over 500 mL per day, a duration of <20 years, age at initiation older than 30 years, and warm and moderately concentrated tea). Similar results were yielded in the sensitivity analyses (Multivariate adjustment and the IPTW analysis). Furthermore, subgroup analysis revealed that the negative association of oolong tea drinking with OSCC risk was more evident among those with poor oral hygiene. This study provides supportive evidence that oolong tea consumption may have a potentially beneficial effect in preventing OSCC, especially for those with poor oral hygiene.
Oral cancer is the most typical tumor in the head and neck, with oral squamous cell carcinoma (OSCC) accounting for nearly 90% of its pathological classifications (1). The incidence of oral cancer has shown a gradual upward trend in recent years, which makes it a growing concern for the global public, particularly in developing nations (2, 3). It was estimated that the worldwide number of new oral cancer will reach 421,907 by 2025 (4).
Tea has been recognized as one of the world's most renowned beverages, with common varieties including green tea, black tea, and oolong tea (5). Among which, oolong tea is a traditional type of tea origin in southeast China, very popular throughout Asia (6). Accumulating evidence has indicated that oolong tea is rich in polyphenols, flavonoids, and other chemical compounds, which has been posing an increasing interest worldwide (7). Previous studies revealed that oolong tea consumption was associated with a lower risk of numerous chronic diseases, such as hypertension (8), dyslipidemia (9), ischemic stroke (10), and cardiovascular diseases (11). There are also some reports on the effect of oolong tea consumption on several cancers including esophageal cancer (12), ovarian cancer (13), and nasopharyngeal cancer (14). However, to date, research on the potential association between oolong tea consumption and OSCC risk is very limited. Although our previous study suggests a negative association between drinking tea and oral cancer risk (15, 16), continued research into the role of oolong tea consumption is worthy of further exploration. Therefore, the purpose of this study was to investigate the relationship between oolong tea drinking behaviors and oral cancer risk using propensity score analyses (including propensity score matching, PSM; inverse probability of treatment weight, IPTW; and stabilized inverse probability of treatment weight, SIPTW) to minimize the potential confounding effects.
The study was conducted on a hospital-based case-control design which was conducted from January 2010 to October 2020 in Fujian Province, China. A total of 744 patients with newly diagnosed cases of OSCC were recruited from the First Affiliated Hospital of Fujian Medical University, whereas 1,029 healthy controls were registered from the hospital's physical examination center during the same period. Potential research participants who satisfied all inclusion and exclusion criteria and provided written informed consent to participate were enrolled. Furthermore, the inclusion and exclusion criteria were previously described in detail (15). Briefly, all the participants were (1) aged 18–90 years old; and (2) capable of answering questions effectively. Cases were defined as histologically confirmed primary OSCC with no history of chemotherapy or radiation. Controls were classified as healthy people with no history of ophthalmic, cutaneous, respiratory, gastrointestinal, or oncological disorders. This study was approved by the Institutional Review Board of Fujian Medical University (Fuzhou, China) and carried out in conformity with the ethical criteria outlined in the Helsinki Declaration in 1964.
After obtaining written informed consent from research respondents, data were collected by trained professional investigators using an interview-based structured questionnaire. The information obtained included (1) demographics: age, gender, occupation, education level, residence, body height, and weight, etc.; (2) self-reported lifestyle habits: alcohol consumption (yes or no), tobacco smoking (yes or no), and oolong tea drinking-related habits; (3) common dietary intake frequency (Red meat, vegetable intake and fruits intake); and (4) oral hygiene indicators: tooth brushing/day, the numbers of missing teeth, duration of wearing dentures (years), regular dental visits (no/yes), and whether they had oral ulcers (no/ yes). The age was divided into non-elderly (<60 years) and elderly groups (≥60 years) according to the definition of elderly of the United Nations (1). And the dietary intake frequency (red meat, vegetable intake, and fruit intake) was grouped into two groups according to the median of the control group in the overall population. Red meat intake: <3 and ≥3 times/week. Vegetable intake: <2 and ≥2 times/day. Fruit intake: <3 and ≥3 times/week. We constructed a comprehensive index for assessing oral health conditions that are based on the five indicators above. The details have been published in a previous article (17) and were summarized in Supplementary Table 1.
Those who smoked more than 100 cigarettes throughout their lifetime were defined as smokers (18). And those that drank alcohol had at least one drink every week for at least 6 months (15). Oolong tea drinkers were defined as those who consume at least one cup of tea every week for at least 6 months. In this study, there were only 119 oolong tea drinkers who did not smoke or drink alcohol (90 in the control group and 29 in the OSCC group). The detailed data and interaction between tea consumption and smoking or alcohol drinking were presented in Supplementary Table 2.
The following are details on oolong tea drinking habits: (1) Oolong tea drinking history (yes or no); (2) Years of tea-drinking (years); (3) Average daily tea consumption (ml/day); (4) age reported started tea-drinking (in years); (5) Tea temperature (non-drinker/warm/hot); and (6) Tea concentration (light/moderate/strong). It relied on the subjects' assessment of the temperature of the tea. To minimize miss classification, we set a judgment criterion based on the average time from mixing the tea leaves with boiling water to the time of tea drinking. The temperature of tea drinking was classified as very hot (<1 min), hot (1–5 min), warm (5–10 min), and cold tea (more than 10 min) (19). The number of individuals who drink cool tea or very hot was too small to include in this analysis; and the concentration of tea was evaluated based on the volume filled by the brewed tea leaves in the cup (light, <25% of the cup; moderate, 25–50% of the cup; and strong, >50% of the cup) (15). Additionally, other oolong tea drinking habits (such as amount, duration, and age at initiation) were set as categorical variables according to the median of the control group who had a history of drinking oolong tea in overall population. The details are listed as followed: average daily intake amount was grouped into three groups (never drinking, <500 ml/d, ≥500 ml/d); duration of tea consumption was grouped into three groups (never drinking, <20 years, ≥20 years); age at onset of regular drinking was also classified into three groups (never drinking, <30 years, ≥30 years).
In the overall data, Chi-square or Fisher's exact tests were used to compare baseline features between OSCC patients and healthy controls. Propensity score analyses, including propensity score matching (PSM), inverse probability of treatment weight (IPTW), and stabilized inverse probability of treatment weight (SIPTW), were used to minimize selection bias and balance baseline differences and other confounding factors. The matching ratio in PSM was 1:1, and the caliper was 0.02, with 487 patients correctly matched with 487 healthy controls. Based on the PSM, IPTW is then calculated with the estimated propensity score. SPTW was also used to minimize sample size inflation and ensure accurate variance estimates (20, 21). Group differences were measured using standardized mean differences (SMD), with an SMD value of 0.1 considered balanced after the matching. To determine the associations between oolong tea-drinking habits and OSCC risk, we utilized multivariate logistic regression (in unmatched data), conditional logistic regression (in PSM data), and weighted logistic regression (in IPTW and SIPTW data). A two-tailed P-value of 0.05 was deemed statistically significant. R software version 4.0.3 was used for all analyses. For propensity scoring and matching analysis, the “MatchIt” package was used, and the “forestploter” package was used to visualize the stratified analysis results.
This observational case-control research comprised 744 OSCC patients and 1,029 healthy controls. A baseline summary of pre-and post-matching participant demographics (age, gender, occupation, education level, BMI, and residence), lifestyle habits (smoking and alcohol consumption), and consumption frequency of red meat, vegetables, and fruits are presented in Table 1 (population after PSM and SIPTW) and Supplementary Table 3 (overall population and population after IPTW). Before matching analysis, imbalances were noted between the case and control subjects in the collected 11 variables except for gender (P < 0.05). After propensity matching adjustment (PSM, IPTW, and SIPTW analysis), all the distributions of observed covariates were comparable (SMD < 0.1, Table 1 and Supplementary Table 3 and Figure 1).
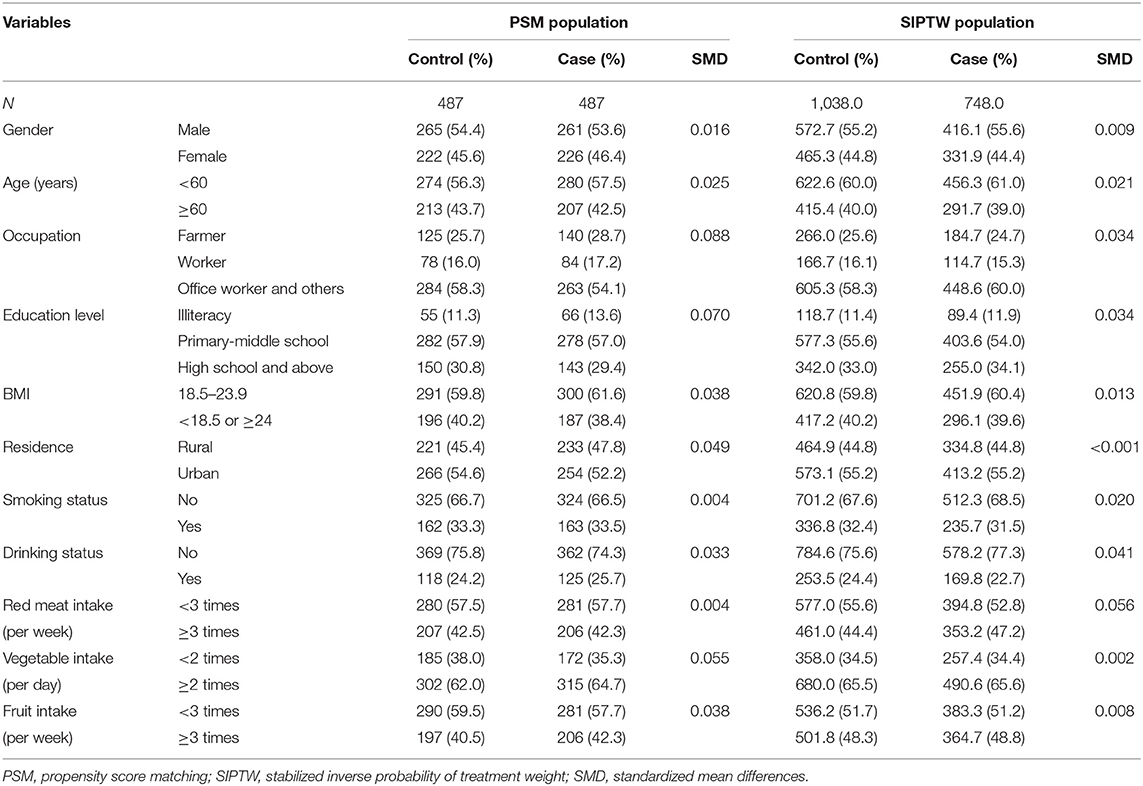
Table 1. Baseline characteristics of case and control groups after propensity score analyses.
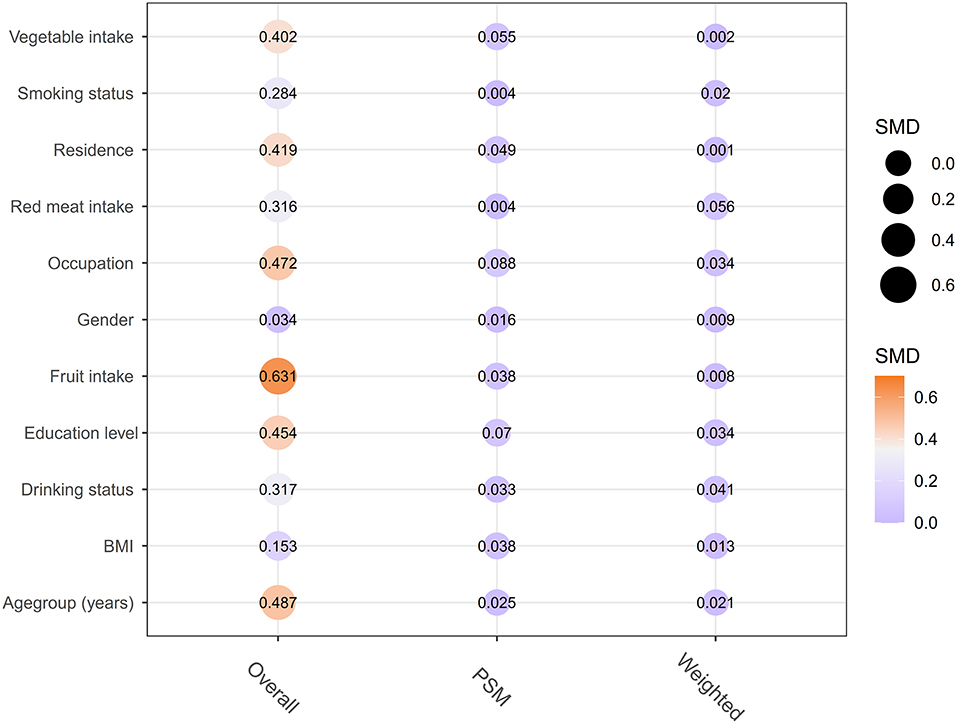
Figure 1. Comparison of the distribution of matching factors between cases and controls before and after matching, Group differences were assessed using standardized mean differences (SMD), with an SMD value of 0.1 considered balanced.
Table 2 presents the relationships between oolong tea-drinking habits and the risk of OSCC in PSM and SIPTW populations. Reduced risk of OSCC was observed among participants who had the consumption of oolong tea as compared to non-drinkers [PSM population, OR (95%CI): 0.69 (0.49–0.97); SIPTW population, OR (95%CI): 0.74 (0.58–0.94)]. Moreover, oolong tea drinkers who consumed over 500 mL per day had a statistically significant decrease in OSCC risk with the OR (95%CI) being 0.59 (0.38–0.92) in PSM analysis and 0.71 (0.57–0.96) in SIPTW analysis. Additionally, those who had a duration of oolong tea consumption of <20 years and those who started drinking tea at an age older than 30 years were less likely to develop OSCC than non-tea drinkers. Of note, both temperature and concentration of oolong tea were correlated with the risk of OSCC. In PSM data, there is a lower risk of OSCC for oolong tea drinkers who prefer warm and moderately concentrated tea over non-tea drinkers [Tea temperature: warm vs. never drinking, OR (95% CI): 0.56 (0.33–0.93); Tea concentration: moderate vs. never drinking, OR (95% CI): 0.56 (0.33–0.93)]. Similar relationship patterns were also identified in SIPTW data [Tea temperature: warm vs. never drinking, OR (95% CI): 0.70 (0.50–0.99); Tea concentration: moderate vs. never drinking, OR (95% CI): 0.64 (0.46–0.90)]. Subsequently, we performed sensitivity analyses on the overall population and the IPTW population to assess the stability of the results, and comparable results were obtained (Supplementary Table 4).
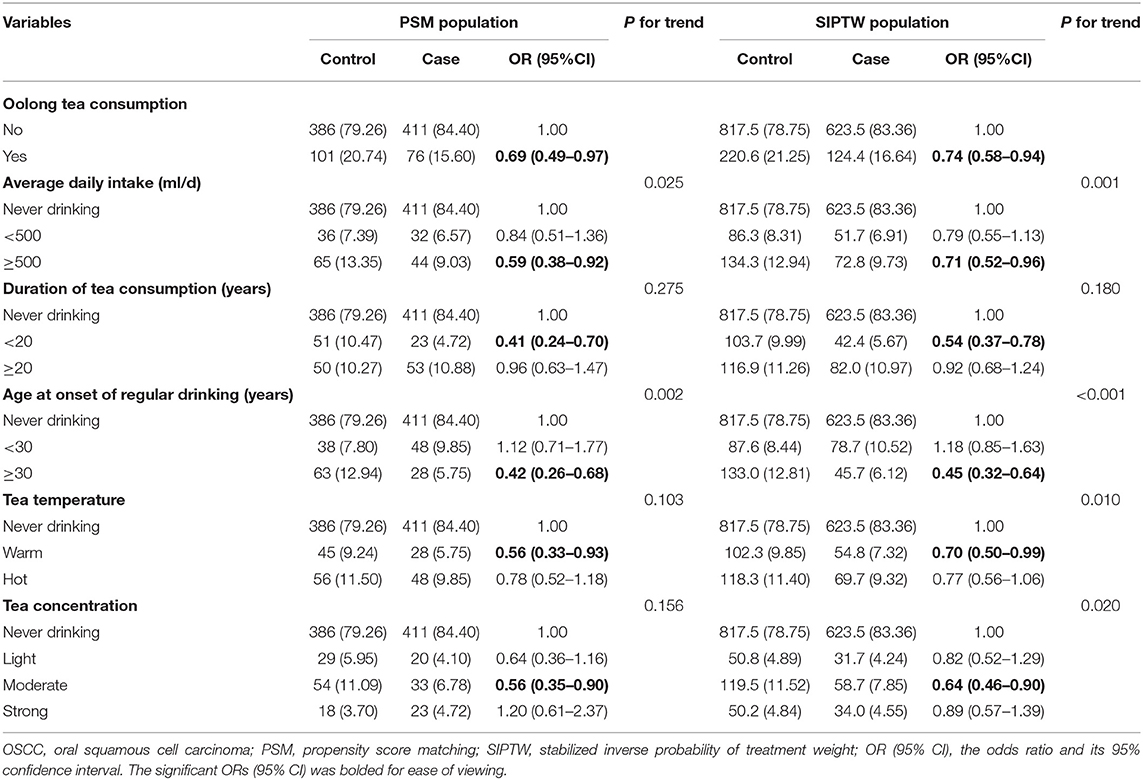
Table 2. The relationship between oolong tea-drinking habits and OSCC risk after propensity score analyses.
Based on the oral hygiene scores, the subjects were divided into subgroups for further analysis. A greater reduction in OSCC risk with oolong tea drinking was observed among those with poor oral hygiene compared to non-drinkers with good oral hygiene. Of note, as the sample size increases (PSM population to IPTW population), the observed inverse association with OSCC seems to be more pronounced (Figure 2).

Figure 2. Associations of oolong tea consumption and the risk of OSCC, stratified by different oral hygiene scores. Adjusted OR (95% CI) was calculated by adjusting for age, gender, occupation, education level, BMI, residence, smoking, and alcohol consumption, consumption frequency of red meat, vegetables, and fruits.
This hospital-based case-control study sought to shed light on the relationship between oolong tea consumption and OSCC risk using three powerful propensity score analyses. Overall, our results support a beneficial effect of oolong tea consumption on the reduced risk of OSCC. Furthermore, OSCC risk was found to be significantly associated with certain tea-drinking habits (amount, duration, age at initiation, temperature, and concentration). Of note, the possible preventive benefits of oolong tea consumption against OSCC were more prominent in individuals with poor oral hygiene.
In the present study, we found the consumption of oolong tea reduced the risk of OSCC by 25–30%, which corresponded to the results of our previous studies (15, 16). In addition, the risk can be further reduced by a higher dose of tea exposure (more than 500 ml/day). Zhou et al. (22). recently published a meta-analysis and systematic review also showing that increasing one cup of tea per day reduces the incidence of oral cancer by 6.2%. More than 100 chemical components have been isolated and identified from oolong tea, among which polyphenols are the most significant ones (23, 24). The polyphenols contain multiple functional components, such as (-)-epigallocatechin gallate (EGCG) and theaflavin (TF) (25, 26), which were reported to have anti-inflammatory and antioxidant effects, and other biological properties (5, 27). Also, multiple in vitro and in vivo studies have indicated that several oolong tea polyphenol extracts could induce apoptosis or proliferation of cancer cells, including oral cancer cells, leading to tumor growth inhibition (28–31).
In the present study, individuals who had consumed oolong tea for <20 years and those who began drinking tea at an age ≥30 years were less likely to develop OSCC, indicating the long-term benefits of oolong tea, when compared to non-oolong-tea drinkers. It is hypothesized that the possible explanation is that the incidence of OSCC grows with increasing age, and young individuals accounted for more in the group with <20 years of tea drinking, while the elderly accounted for more in the group with ≥20 years of tea drinking. Certainly, this hypothesis will require further investigation in future studies.
In the present study, we also found a significantly lower risk of oral cancer among warm tea drinkers compared to non-tea drinkers, while this protective effect tended to diminish among hot tea drinkers (not reaching statistical significance). Recently, the International Agency for Research on Cancer (IARC) classified drinking very hot beverages above 65°C as “probably carcinogenic to humans” (32). According to the most recent study by Ernst et al. (33), hot beverages would increase the cell division rate in the oral mucosa at temperatures above 60°C, leading to cytotoxic effects and increased risk of cancer. Drinking moderately concentrated tea would be most beneficial to reducing OSCC risk in our study (Table 2 and Supplementary Table 4). However, the literature is controversial concerning the optimal tea-drinking concentration. Dose-response analyses of one meta-analysis suggested that with the concentration of tea consumption increased, the risk of oral cancer decreased (22). However, there have been other studies showing that fluoride found in oolong tea helps to prevent dental caries and promote healthy bone growth, but excess fluoride could lead to detrimental health problems in humans, especially fluorosis of the teeth and skeletal fluorosis (7).
It is crucial to highlight that the preventative advantages of oolong tea drinking may vary on oral hygiene status, with individuals with poor oral hygiene experiencing stronger protective benefits. According to Yoo et al. (34), oolong tea extract has an antibacterial effect on oral streptococci such as Streptococcus mutans and Streptococcus sobrinus. In polyphenols, notably catechin, epigallocatechin-3-gallate selectively inhibits the development and adhesion of periodontopathogens (35). These findings imply that long-term consumption of oolong tea may be effective in mitigating the negative effects of poor oral hygiene on OSCC, which has significant public health implications.
There are certain merits to this study. Our findings represent the first comprehensive analysis of oolong tea consumption and related habits (including amount, duration, age at initiation, temperature, and concentration) and OSCC risk by utilizing traditional multivariate logistic regression (Supplementary Table 4) and advanced propensity score analyses (PSM, IPTW, and SIPTW analyses, Table 2 and Supplementary Table 4). However, several limitations of our investigation were unavoidable. Firstly, despite the adjustment of potential influencing factors to minimize this effect when performing the stratified analysis of oral hygiene scores, the balance between groups may still be disrupted, and future studies using other statistical methods (such as propensity score stratification) are needed. Secondly, it's difficult to accurately correlate each subject with the true situation since some subjects consumed more than one type of tea, while only the main tea consumed was recorded in the survey, and differences in composition between oolong teas of different origins may further obscure the true association between tea drinking and the risk of OSCC. Third, considering the relatively small sample size of oolong tea drinkers who neither smoked nor consumed alcohol in this study, we are unable to further analyze the associations of oolong tea consumption habits (amount, duration, age at initiation, and concentration) with OSCC risk among this population. the results must be validated in larger cohorts. Further research with larger sample size is warranted to confirm these results.
In conclusion, this study suggests an inverse association between oolong tea consumption and the risk of OSCC, especially for those with poor oral hygiene conditions. These findings may provide an additional understanding of the beneficial role of oolong tea consumption in decreasing the risk of OSCC, which has public health implications for oral cancer prevention.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
This study was approved by the Institutional Review Board of Fujian Medical University (Fuzhou, China) and carried out in conformity with the ethical criteria outlined in the Helsinki Declaration in 1964. The patients/participants provided their written informed consent to participate in this study.
FC, BH, and JW participated in the design of the study. BH, LL, and YQ were responsible for recruiting participants. MG, YL, MY, LL, WH, and YuxW were responsible for interviewing participants. QD, YuyW, and HW analyzed the data. QD, YuyW, and XH wrote the manuscript, which was revised by all authors. All authors contributed to the article and approved the submitted version.
This study was funded by the High-level Talents Research Start-up Project of Fujian Medical University (No. XRCZX2018001) and the Central Government-Led Local Science and Technology Development Special Project (No. 2020L3009).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors appreciated all the staff in the Department of Oral and Maxillofacial Surgery, the First Affiliated Hospital of Fujian Medical University, Fuzhou for their technical assistance.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2022.928840/full#supplementary-material
1. Almangush A, Mäkitie A, Triantafyllou A, de Bree R, Strojan P, Rinaldo A, et al. Staging and grading of oral squamous cell carcinoma: an update. Oral Oncol. (2020) 107:104799. doi: 10.1016/j.oraloncology.2020.104799
2. Ren Z, Hu C, He H, Li Y, Lyu J. Global and regional burdens of oral cancer from 1990 to 2017: results from the global burden of disease study. Cancer Commun. (2020) 40:81–92. doi: 10.1002/cac2.12009
3. Du M, Nair R, Jamieson L, Liu Z, Bi P. Incidence trends of lip, oral cavity, and pharyngeal cancers: global burden of disease 1990–2017. J Dent Res. (2020) 99:143–51. doi: 10.1177/0022034519894963
4. International Agency for Research on Cancer. Cancer Tomorrow. (2022). Available online at: https://gco.iarc.fr/tomorrow/home (accessed March 31, 2022).
5. Khan N, Mukhtar H. Tea polyphenols in promotion of human health. Nutrients. (2018) 11:39. doi: 10.3390/nu11010039
6. Zhang X, Du X. Effects of exogenous enzymatic treatment during processing on the sensory quality of summer Tieguanyin Oolong tea from the Chinese Anxi County. Food Technol Biotechnol. (2015) 53:180–9. doi: 10.17113/ftb.53.02.15.3642
7. Ng K, Cao Z, Chen H, Zhao Z, Zhu L, Yi T. Oolong tea: a critical review of processing methods, chemical composition, health effects, and risk. Crit Rev Food Sci Nutr. (2018) 58:2957–80. doi: 10.1080/10408398.2017.1347556
8. Yang Y, Lu F, Wu J, Wu C, Chang C. The protective effect of habitual tea consumption on hypertension. Arch Intern Med. (2004) 164:1534–40. doi: 10.1001/archinte.164.14.1534
9. Yi D, Tan X, Zhao Z, Cai Y, Li Y, Lin X, et al. Reduced risk of dyslipidaemia with oolong tea consumption: a population-based study in Southern China. Br J Nutr. (2014) 111:1421–9. doi: 10.1017/S0007114513003644
10. Liang W, Lee A, Binns C, Huang R, Hu D, Zhou Q. Tea consumption and ischemic stroke risk: a case-control study in Southern China. Stroke. (2009) 40:2480–5. doi: 10.1161/STROKEAHA.109.548586
11. Mineharu Y, Koizumi A, Wada Y, Iso H, Watanabe Y, Date C, et al. Coffee, green tea, black tea and oolong tea consumption and risk of mortality from cardiovascular disease in Japanese Men and Women. J Epidemiol Commun Health. (2011) 65:230–40. doi: 10.1136/jech.2009.097311
12. Chen Y-K, Lee C-H, Wu IC, Liu J-S, Wu D-C, Lee J-M, et al. Food intake and the occurrence of squamous cell carcinoma in different sections of the esophagus in Taiwanese Men. Nutrition. (2009) 25:753–61. doi: 10.1016/j.nut.2009.02.002
13. Lee AH, Su D, Pasalich M, Binns CW. Tea consumption reduces ovarian cancer risk. Cancer Epidemiol. (2013) 37:54–9. doi: 10.1016/j.canep.2012.10.003
14. Hsu W-L, Pan W-H, Chien Y-C, Yu KJ, Cheng Y-J, Chen J-Y, et al. Lowered risk of nasopharyngeal carcinoma and intake of plant vitamin, fresh fish, green tea and coffee: a case-control study in Taiwan. PLoS ONE. (2012) 7:e41779. doi: 10.1371/journal.pone.0041779
15. Chen F, He B, Yan L, Liu F, Huang J, Hu Z, et al. Tea consumption and its interactions with tobacco smoking and alcohol drinking on oral cancer in Southeast China. Eur J Clin Nutr. (2017) 71:481–5. doi: 10.1038/ejcn.2016.208
16. Chen F, Yan L, Lin L, Liu F, Qiu Y, Liu F, et al. Independent and joint effects of tea and milk consumption on oral cancer among non-smokers and non-drinkers: a case-control study in China. Oncotarget. (2017) 8:50091–7. doi: 10.18632/oncotarget.15096
17. Deng Q, Yan L, Lin J, Zhuang Z, Hong Y, Hu C, et al. Correction to: a composite oral hygiene score and the risk of oral cancer and its subtypes: a large-scale propensity score-based study. Clin Oral Investig. (2022) 26:2439. doi: 10.1007/s00784-021-04243-6
18. Hashibe M, Brennan P, Benhamou S, Castellsague X, Chen C, Curado M, et al. Alcohol drinking in never users of tobacco, cigarette smoking in never drinkers, and the risk of head and neck cancer: pooled analysis in the international head and neck cancer epidemiology consortium. J Natl Cancer Inst. (2007) 99:777–89. doi: 10.1093/jnci/djk179
19. Yang X, Ni Y, Yuan Z, Chen H, Plymoth A, Jin L, et al. Very hot tea drinking increases esophageal squamous cell carcinoma risk in a high-risk area of China: a population-based case-control study. Clin Epidemiol. (2018) 10:1307–20. doi: 10.2147/CLEP.S171615
20. Xu S, Ross C, Raebel M, Shetterly S, Blanchette C, Smith D. Use of stabilized inverse propensity scores as weights to directly estimate relative risk and its confidence intervals. Value Health. (2010) 13:273–7. doi: 10.1111/j.1524-4733.2009.00671.x
21. Schuster T, Lowe W, Platt R. Propensity score model overfitting led to inflated variance of estimated odds ratios. J Clin Epidemiol. (2016) 80:97–106. doi: 10.1016/j.jclinepi.2016.05.017
22. Zhou H, Wu W, Wang F, Qi H, Cheng Z. Tea consumption is associated with decreased risk of oral cancer: a comprehensive and dose-response meta-analysis based on 14 case-control studies (moose compliant). Medicine. (2018) 97:e13611. doi: 10.1097/MD.0000000000013611
23. Pan SY, Nie Q, Tai HC, Song XL, Tong YF, Zhang LJ, et al. Tea and tea drinking: China's outstanding contributions to the mankind. Chin Med. (2022) 17:27. doi: 10.1186/s13020-022-00571-1
24. Tong T, Liu YJ, Kang J, Zhang CM, Kang SG. Antioxidant activity and main chemical components of a novel fermented tea. Molecules. (2019) 24:2917. doi: 10.3390/molecules24162917
25. He X, Li J, Zhao W, Liu R, Zhang L, Kong X. Chemical fingerprint analysis for quality control and identification of Ziyang Green Tea by Hplc. Food Chem. (2015) 171:405–11. doi: 10.1016/j.foodchem.2014.09.026
26. Sun H, Chen Y, Cheng M, Zhang X, Zheng X, Zhang Z. The modulatory effect of polyphenols from Green Tea, Oolong Tea and Black Tea on human intestinal microbiota in vitro. J Food Sci Technol. (2018) 55:399–407. doi: 10.1007/s13197-017-2951-7
27. Hayat K, Iqbal H, Malik U, Bilal U, Mushtaq S. Tea and its consumption: benefits and risks. Crit Rev Food Sci Nutr. (2015) 55:939–54. doi: 10.1080/10408398.2012.678949
28. Yoshimura H, Yoshida H, Matsuda S, Ryoke T, Ohta K, Ohmori M, et al. The therapeutic potential of epigallocatechin-3-gallate against human oral squamous cell carcinoma through inhibition of cell proliferation and induction of apoptosis: in vitro and in vivo murine xenograft study. Mol Med Rep. (2019) 20:1139–48. doi: 10.3892/mmr.2019.10331
29. Pan MH, Liang YC, Lin-Shiau SY, Zhu NQ, Ho CT, Lin JK. Induction of apoptosis by the oolong tea polyphenol theasinensin a through cytochrome C release and activation of caspase-9 and caspase-3 in human u937 cells. J Agric Food Chem. (2000) 48:6337–46. doi: 10.1021/jf000777b
30. Brimson JM, Prasanth MI, Malar DS, Sharika R, Sivamaruthi BS, Kesika P, et al. Role of herbal teas in regulating cellular homeostasis and autophagy and their implications in regulating overall health. Nutrients. (2021) 13:2162. doi: 10.3390/nu13072162
31. Zhang X, Dai C, You Y, He L, Chen T. Tea regimen, a comprehensive assessment of antioxidant and antitumor activities of tea extract produced by tie guanyin hybridization. RSC Adv. (2018) 8:11305–15. doi: 10.1039/C8RA00151K
32. Loomis D, Guyton KZ, Grosse Y, Lauby-Secretan B, El Ghissassi F, Bouvard V, et al. Carcinogenicity of drinking coffee, mate, and very hot beverages. Lancet Oncol. (2016) 17:877–8. doi: 10.1016/S1470-2045(16)30239-X
33. Ernst B, Setayesh T, Nersesyan A, Kundi M, Fenech M, Bolognesi C, et al. Investigations concerning the impact of consumption of hot beverages on acute cytotoxic and genotoxic effects in oral mucosa cells. Sci Rep. (2021) 11:23014. doi: 10.1038/s41598-021-01995-9
34. Yoo S, Murata RM, Duarte S. Antimicrobial traits of tea- and cranberry-derived polyphenols against streptococcus mutans. Caries Res. (2011) 45:327–35. doi: 10.1159/000329181
Keywords: oolong tea consumption, OSCC, propensity score analyses, oral hygiene, risk assessment
Citation: Deng Q, Wu Y, Hu X, Wu H, Guo M, Lin Y, Yu M, Huang W, Wu Y, Lin L, Qiu Y, Wang J, He B and Chen F (2022) Oolong Tea Consumption and the Risk of Oral Squamous Cell Carcinoma: A Propensity Score-Based Analysis in Southeast China. Front. Nutr. 9:928840. doi: 10.3389/fnut.2022.928840
Received: 26 April 2022; Accepted: 17 June 2022;
Published: 07 July 2022.
Edited by:
Md Anwarul Azim Majumder, The University of the West Indies, Cave Hill, BarbadosReviewed by:
Cleverton Roberto De Andrade, São Paulo State University, BrazilCopyright © 2022 Deng, Wu, Hu, Wu, Guo, Lin, Yu, Huang, Wu, Lin, Qiu, Wang, He and Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fa Chen, Y2hlbmZhQGZqbXUuZWR1LmNu
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.