 Hannah G. Juncker1,2Eliza J. M. Ruhé1
Hannah G. Juncker1,2Eliza J. M. Ruhé1 Aniko Korosi2
Aniko Korosi2 Johannes B. van Goudoever1*
Johannes B. van Goudoever1* Marit J. van Gils3
Marit J. van Gils3 Britt J. van Keulen1
Britt J. van Keulen1- 1Department of Pediatrics, Emma Children's Hospital, Amsterdam Reproduction & Development Research Institute, Amsterdam UMC, Vrije Universiteit, University of Amsterdam, Amsterdam, Netherlands
- 2Swammerdam Institute for Life Sciences - Center for Neuroscience, University of Amsterdam, Amsterdam, Netherlands
- 3Department of Medical Microbiology and Infection Prevention, Amsterdam Infection and Immunity Institute, Amsterdam UMC, University of Amsterdam, Amsterdam, Netherlands
Importance: SARS-CoV-2-specific antibodies in human milk might protect the breastfed infant against COVID-19. One of the factors that may influence human milk antibodies is psychological stress, which is suggested to be increased in lactating women during the COVID-19 pandemic.
Objective: To determine whether psychological stress is increased in lactating women during the COVID-19 pandemic, and if maternal stress is associated with the level of SARS-CoV-2-specific antibodies in human milk.
Design: Population-based prospective cohort study.
Setting: Data collection took place in the Netherlands between October 2020 and February 2021.
Participants: Lactating women living in the Netherlands were eligible to participate in this study. In total, 2310 women were included.
Exposures: Stress exposure during the COVID-19 pandemic was determined using the Perceived Stress Scale (PSS) questionnaire and maternal lifetime stress was determined by the Life Stressor Checklist – revised (LSC-r) questionnaire.
Main Outcome(s) and Measure(s): Stress experience during the COVID-19 pandemic was compared with a pre-pandemic cohort. SARS-CoV-2-specific antibodies in human milk were measured using an Enzyme-Linked Immunosorbent Assay (ELISA) with the Spike protein of SARS-CoV-2. The association between maternal stress and human milk antibodies was determined using a multiple regression model.
Results: The PSS score of lactating mothers was not increased during the pandemic compared to the PSS score in the prepandemic cohort. Six hundred ninety-one participants had SARS-CoV-2-specific antibodies and were included in the regression models to assess the association between maternal stress and human milk antibodies. No association was found between PSS scores and human milk antibodies. In contrast, the LSC-r score was negatively associated with SARS-CoV-2-specific IgA in human milk (β = 0.98, 95% CI: 0.96–0.997, p = 0.03).
Conclusions and Relevance: Our results suggest that lactating women in the Netherlands did not experience higher stress levels during the COVID-19 pandemic. Breastfed infants of mothers with high chronic stress levels receive lower amounts of antibodies through human milk, which possibly makes them more vulnerable to respiratory infections. This emphasizes the importance of psychological wellbeing during lactation.
Introduction
COVID-19 usually has a mild course in children; however, young infants are more susceptible to severe disease development, which could be due to an immature immune system (1). Human milk provides additional immunological protection for these infants as it contains multiple immunological components. Human milk antibodies are suggested to play an important role in the protection against respiratory infections (2–5). Antibodies against the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) have been found in human milk after maternal infection and vaccination (6–12). It is very likely that these antibodies play a critical role in protecting the infant against COVID-19. Indeed, breastfeeding in SARS-CoV-2 positive mothers, protects their infants from developing symptoms of COVID-19 (13). Moreover, although SARS-CoV-2 RNA has been detected in human milk, replication competent SARS-CoV-2 has not been isolated and transmission of the virus to the infant through human milk has not been reported (14–18).
Human milk antibody titers are influenced by many different factors, including maternal psychological stress (19–21). However, there is still controversy on the effect of maternal stress on the secretion of immunoglobulin A (IgA), the most abundant antibody in human milk (19, 22–25). Most studies point toward the view that perceived stress reduces IgA in human milk (19). It is important to elucidate this relationship, as it is plausible to assume that maternal stress might be increased during the COVID-19 pandemic. Indeed, several studies have highlighted concerns about the mental health of postpartum women in the COVID-19 pandemic, showing an increase in depressive symptoms, anxiety and maternal distress (26–29). The mental state and overall functioning of the mothers may have suffered from the lockdown measures due to limited access to support systems, changes in hospital policies including unaccompanied pregnancy checkups, mother-infant separation policies, and the stress that comes from their overall concerns about exposure to COVID-19 (29).
The aim of this study is to investigate maternal psychological stress during the COVID-19 pandemic and its potential impact on SARS-CoV-2-specific antibodies in human milk. We hypothesize that maternal psychological stress is higher during the pandemic and that perceived stress levels are negatively associated with IgA against SARS-CoV-2 in human milk.
Methodology
Study Design and Population
The COVID MILK – POWER MILK study is a prospective cohort study, which included lactating women between October 12th and February 23th in the Netherlands who did not yet receive a SARS-CoV-2 vaccine. Participants were recruited via (social) media and could sign themselves up by sending an e-mail. Ethical approval was obtained from the Medical Ethics Committee of the Amsterdam UMC, location VUmc. Written informed consent was obtained from all participants.
Study Procedures and Sample Collection
To determine SARS-CoV-2 antibodies, a human milk and blood sample were collected during a study visit. In the morning of the appointment, participants were instructed to empty one breast completely before the first feeding moment, either manually or with an electric breast pump, mix the milk and subsequently store 20 ml in the refrigerator until collection by the researcher. During the study visit, 5 ml of blood was collected. At the study site, serum and milk samples were stored at −80°C up until analysis. After the study visit, participants received a questionnaire, which included two validated test tools to examine the level of stress experienced by the participants.
Perceived Stress Scale (PSS)
To investigate stress during the COVID-19 pandemic and its influence on maternal antibodies, the PSS questionnaire was used. The PSS is a validated 14-item questionnaire developed by Cohen et al. (30, 31). The questionnaire aims to determine how stressful one experiences certain situations (30, 31). For each question the respondent is asked to indicate how many times they felt a certain way since the outbreak of COVID-19. Each question is scored on a 5-point Likert Scale ranging from 0–4 (0 = never; 1 = almost never; 2 = sometimes; 3 = fairly often; 4 = very often).
Life Stressor Checklist – Revised (LSC-r)
To investigate the influence of maternal lifetime stressors on human milk antibody levels, the LSC-r questionnaire was used. The LSC-r evaluates the maternal lifetime history of stress. The validated checklist is a 30-item scale to identify the exposure to traumatic events or other stressful life events (32). For this research, we used the questions that form a comparative baseline for lifetime traumatic stress. We combined two scoring methods of the questionnaire for this study. This approach combines a score for high magnitude stressors (criteria A stressors) and a score for low magnitude stressors (other life stressors) (32) resulting in an overall life stressor score ranging from 0–13, with the highest score representing the highest level of lifetime history of stress (32).
Determination of SARS-CoV-2 Antibody Titers in Human Milk and Serum
Before analysis, the collected human milk and serum samples were stored at the Amsterdam UMC, location VUmc, at −80°C. To assess the SARS-CoV-2-specific IgA antibodies in human milk and IgG antibodies in serum, an enzyme-linked immunosorbent assay (ELISA) with the SARS-CoV-2 spike protein was used as described previously (33). In brief, whole human milk and serum samples were diluted 1:10 or 1:100, respectively, in 1% casein PBS (Thermo Scientific) and IgA or IgG were detected using horseradish peroxidase (HRP)-labeled goat anti-human IgA (Biolegend) or HRP-labeled goat anti-human IgG (Jackson, Immunoresearch), respectively, which were validated using monoclonal antibodies. A relative operating characteristic (ROC) curve analysis was performed to determine the cut-off value for both milk and serum samples using pre-pandemic negative samples and polymerase chain reaction proven positive samples. The human milk samples were considered positive at an optical density (OD) 450 nm cut-off value of 0.502, and the serum samples at an OD450 nm value of 0.452. With these cut-off values, the sensitivity was 67.9% (95% confidence interval (CI): 61.0–74.1%) for IgA antibodies in human milk with a specificity of 99.0% (95% CI: 94.7–100.0%) and for serum IgG antibodies the sensitivity was 95.9 (95% CI: 92.9–97.6%) with a specificity of 99.1 (95% CI: 94.9–100%). For cross-comparison, negative and positive controls were included in each run.
Statistical Analysis
The obtained data is registered in the Clinical Data Management System “Castor Electronic Data Capture (EDC).” In order to perform the statistical analysis, the data was transferred into IBM Statistical Package for Social Sciences Statistics (SPSS) for Windows version 26. Characteristics were described in descriptive statistics including frequencies, mean values with standard deviations (SD) or median with interquartile ranges (IQR). Participants with missing data for stress measures or antibody levels were excluded from further analyses.
We compared PSS scores in our cohort with a recent study conducted in the United States before the outbreak of COVID-19 (34). This pre-pandemic cohort consisted of 151 lactating mothers between 18 and 40 years old who filled out the PSS questionnaire at weeks 1 and 2 postpartum, as well as at 1-, 2-, 3-, and 6-months postpartum. This pre-pandemic cohort was comparable with our cohort in baseline characteristics including age, BMI and history of depression. Unpaired t-tests were performed to compare PSS scores between this pre-pandemic cohort and our cohort for each month postpartum.
To investigate the influence of maternal stress on human milk antibodies, lactating mothers who tested positive for SARS-CoV-2-specific antibodies in serum or human milk were included. IgA values were log-transformed before analyses. Due to a non-linear relation between PSS and IgA levels, participants were divided in three groups: low stress (PSS 0-14.99), moderate stress (15.00–21.99) and high stress (22.00–56.00) based on the 33.3–66.6 percentiles. Pearson Chi square tests, one-way ANOVA and Kruskal Wallis tests were used to assess differences in characteristics between PSS subgroups based on the distribution.
To examine the association between PSS and LSC-r scores and maternal antibodies, multiple regression analyses were performed. The PSS regression model was adjusted for factors that differed between the PSS groups. In literature, age of the mother, BMI of the mother, parity, lactation stage and sex of the child have shown to influence antibody levels in human milk (21, 23, 35, 36). Those variables were added to the LSC-r regression model when they influenced the model with >10%. To correct for the logarithmic transformation, the following formulas were used to accurately interpret the regression coefficients: β = eβ and 95.0% confidence interval= e(β±1.96 x standard error). For the statistical analysis, the hypothesis was tested two-tailed and a p-value of <0.05 was considered statistically relevant. GraphPad Prism for Windows (version 8.2.1.) was used to illustrate the data distributions.
Results
Stress Levels of Lactating Mothers During the COVID-19 Pandemic
Baseline Characteristics
In total, 2310 mothers participated in the study, of whom 2,163 (94%) filled out the characteristics questionnaire (Table 1). The participants were on average 33.2 (SD ± 3.9) years of age and were breastfeeding their child for 38.0 (25.0–59.0) weeks.
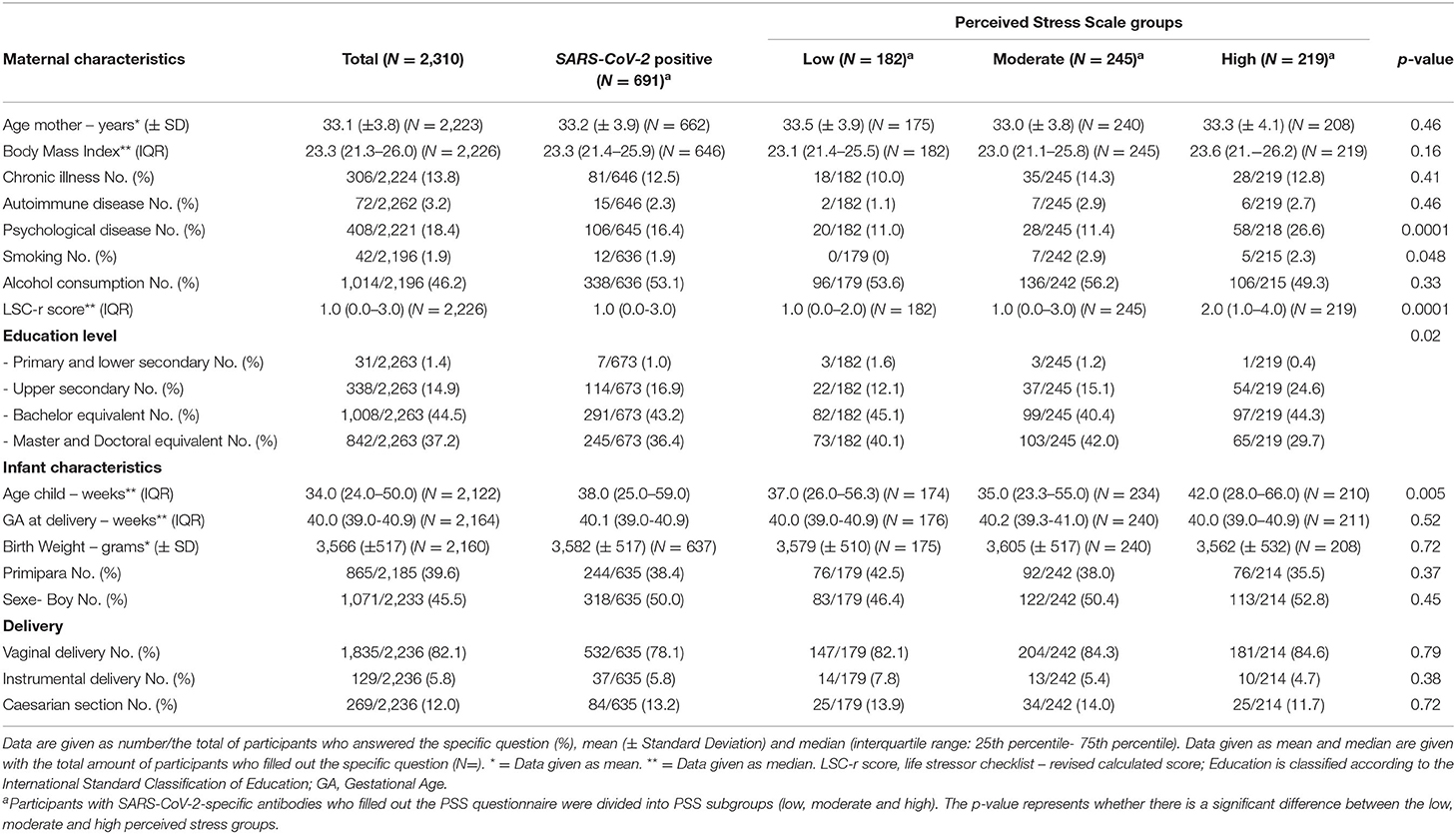
Table 1. Participants characteristics based on perceived stress scores (PSS) in participants with an ELISA confirmed SARS-CoV- 2 infection in serum or human milk.
Postpartum PSS and LSC-r Scores
The PSS questionnaire was completed by 2,162 participants (94%). These women had a mean PSS score of 19.56 (SD ± 7.97). The PSS scores increased over the first postpartum year [r = 0.09, 95% CI: 0.12–0.40, p < 0.001, N = 1,619 (two-tailed)] (Figure 1). We compared the PSS scores of the women in our cohort to PSS scores in a pre-COVID-19 cohort of lactating women. The mean PSS score in this pre-pandemic cohort of 151 lactating women up to 6 months postpartum was 18.69 (SD ± 0.47) (34). The women up to 6 months postpartum in our cohort had a mean PSS score of 18.41 (SD ± 7.64) (N = 494), which did not differ from the pre-pandemic cohort at any time postpartum (mean difference: −0.27, 95% CI: −0.95–0.40, p = 0.43) (Figure 2). The LSC-r questionnaire was completed by 2162 participants (94%) and they scored a median of 1.00 (IQR: 0.0–3.0).
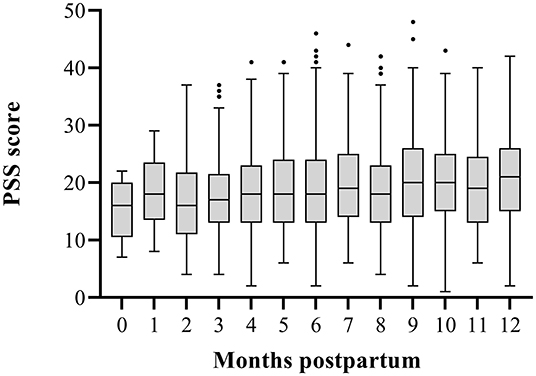
Figure 1. Perceived Stress Scale (PSS) scores up to 12 months postpartum. This figure shows the increase in PSS scores over the first postpartum year. The box represents the interquartile range with median PSS scores. Whiskers present the data range (Q1/Q3 +/−1.5IQR). ·= outlier.
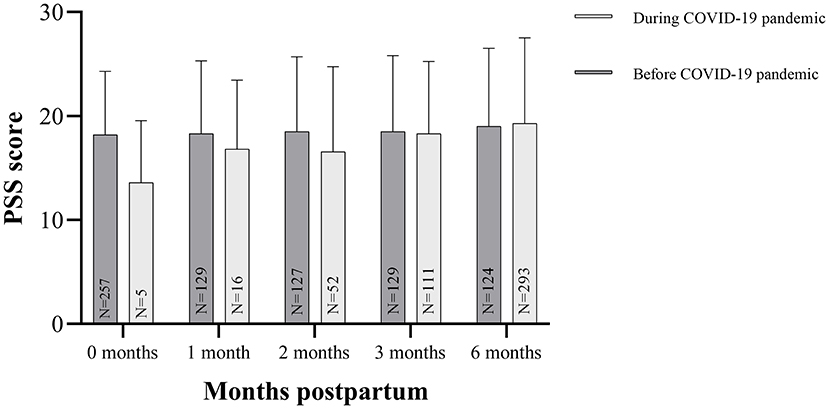
Figure 2. Perceived Stress Scale (PSS) scores during and before the COVID-19 pandemic. In this figure, the PSS scores are displayed as mean (SD) of the specific postpartum group up to six months postpartum. Mean PSS scores of a U.S. cohort before the COVID-19 pandemic are obtained in Paul et al. (34). There were no differences between our study cohort and the pre-pandemic cohort.
Maternal Stress and SARS-CoV-2-Specific Antibodies in Human Milk
Baseline Characteristics
Of the total study population, 691 participants tested positive for SARS-CoV-2-specific IgA in human milk or IgG in serum. These participants were categorized into subgroups based on their PSS scores: low (N = 182), moderate (N = 245) and high (N = 219) PSS groups. The per subgroup characteristics are depicted in Table 1. Women with high PSS scores had more mental illnesses (p < 0.0001), were breastfeeding for a longer time period (p = 0.005), smoked more often (p = 0.048), and scored higher on the LSC-r questionnaire (p < 0.0001).
PSS Scores and Maternal SARS-CoV-2-Specific Antibodies
To compare maternal SARS-CoV-2-specific antibodies between the PSS groups, a multiple regression was performed. No differences were observed in SARS-CoV-2-specific antibody levels in human milk between the PSS groups in both the unadjusted and adjusted model (Table 2, Figure 3).
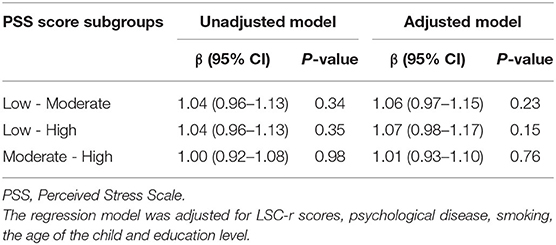
Table 2. The association between PSS scores and SARS-CoV-2-specific antibodies in human milk.
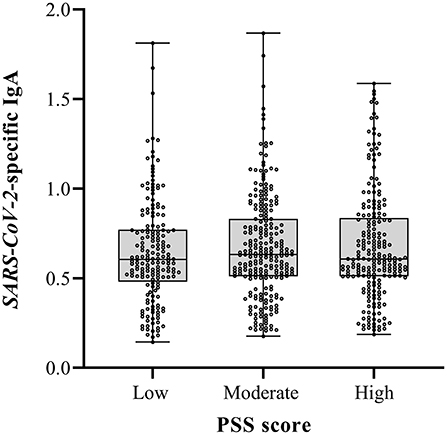
Figure 3. Perceived Stress Scale (PSS) scores and SARS-CoV-2 specific Immunoglobuline A (IgA) in human milk. The boxes represent the interquartile range with median SARS-CoV-2 specific IgA in human milk for the different PSS groups. Whiskers present the data range (Q1/Q3 +/−1.5IQR). The dots indicate the individual measurements. No differences in SARS-CoV-2 specific human milk IgA were found between groups.
LSC-r Scores and Maternal SARS-CoV-2-Specific Antibodies
To investigate the relationship between LSC-r scores and maternal SARS-CoV-2-specific antibodies, a multiple regression was performed. After adjustment for covariates, the LSC-r score was negatively associated with IgA in human milk (B = 0.98, 95% CI: 0.96–0.997, p = 0.03) (Table 3, Figure 4).
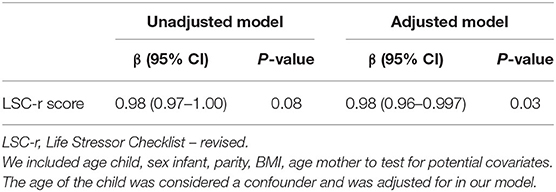
Table 3. The association between LSC-r scores and SARS-CoV-2-specific antibodies in human milk.
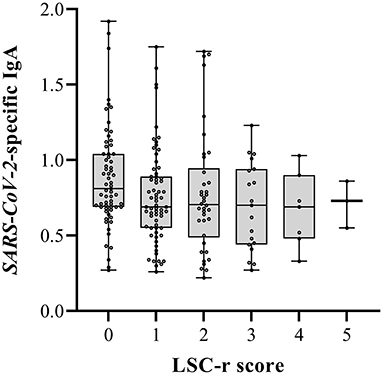
Figure 4. Life Stressor Checklist-revised (LSC-r) scores and SARS-CoV-2 specific Immunoglobuline A (IgA) in human milk. The boxes represent the interquartile range with median SARS-CoV-2 specific IgA in human milk for the different LSC-r scores. Whiskers present the data range (Q1/Q3 +/−1.5IQR). The dots indicate the individual measurements. Multiple lineair regression models were used to determine the association between SARS-CoV-2-specific IgA in human milk and the LSC-r scores (adjusted p-value 0.03).
Discussion
In contrast to our hypothesis, the results of this study suggest that lactating women did not experience higher levels of stress during the COVID-19 pandemic compared to lactating women before the pandemic. Interestingly, maternal lifetime stressors, but not current perceived stress, were negatively associated with human milk antibodies against SARS-CoV-2.
Several studies assessed stress levels in lactating women during the COVID-19 pandemic, of which the majority showed that stress and anxiety levels were increased, while some studies showed similar stress levels during and before the pandemic (26, 28, 37–43). The studies that found higher stress levels were carried out at the onset of the pandemic. It could be suggested that the lack of knowledge of the effects of COVID-19 in lactating women and infants at the very beginning of the pandemic caused stress. Considering that our study was conducted 7 months into the pandemic, this could entail that the women who participated in this study had potentially already adapted to the situation and that stress levels were normal again. Moreover, it could be suggested that lactating women did not experience increased stress levels during the pandemic due to other factors, such as a reduction in social and work obligations. For example, working from home results in reduced travel time and spending more time with family (44, 45).
Previous literature on the relationship between stress and human milk antibodies is controversial. Either positive, negative and no associations between maternal stress, anxiety or depression and human milk IgA have been reported (19, 22–25, 46). The before mentioned studies were hampered by their relatively small samples sizes (n = 50–119) and differed in type and timing of stress measurement, set up and human milk collection, hampering comparability between studies. Most of the before mentioned literature showed a negative association between maternal stress and human milk antibodies (19, 23, 25, 47). In our study, perceived stress among postpartum women showed no relation with SARS-CoV-2-specific antibodies in human milk. However, an inverse association between lifetime stressors and human milk antibodies was observed, also after correcting for possible confounders. This suggests that chronic stress levels may have more pronounced consequences for the maternal immune system compared to current stress levels. Indeed, former research states that chronic stress diminishes the immune response (22, 48–51).
Our study is strengthened by the large sample size, making it possible to identify and adjust for confounding factors. Human milk samples were collected in a standardized way, to minimize collection bias. Moreover, both acute as well as chronic stress was measured. Finally, the study questionnaire was completed by 94% of our study population, which minimizes missing data and improves the reliability and generalizability of our study results. A limitation of our study is that the stress levels were self-reported via questionnaires and that no biological stress measures were included. Moreover, our cohort consisted mostly of highly educated women. It might be that this is not entirely representative for perceived stress levels of all lactating women. In addition, to compare stress levels during the pandemic with pre-pandemic stress levels, our cohort was compared to a pre-pandemic cohort from the United States. Preferably, pre- and during pandemic stress levels should be measured in the same cohort. Finally, SARS-CoV-2-specific antibodies may depend on several other factors, including time after infection and severity of symptoms. However, as our sample size is relatively large, we expect that the influence of these factors on our results is minimal.
At this point, we can only speculate what the stress-related changes in human milk antibodies mean for the protection of the breastfed infant. However, as infants drink this milk multiple times a day for a long period, it can be suggested that the protection will be affected. Large sample-sized, population-based studies are needed to address the actual effect of decreased human milk antibody levels on the protection of the breastfed infant from infections. Moreover, future studies should consider adding biological indicators of stress, for example human milk or hair cortisol concentrations, to assess stress levels in lactating women. Lastly, it would be valuable to measure total immunoglobulins and/or other immunological components in human milk to be able to investigate the effects of stress on the total immunological properties of human milk.
Conclusion
The results of this study demonstrated that lactating women in the Netherlands did not experience higher perceived stress levels seven months into the COVID-19 pandemic compared to stress levels of lactating women prior to the COVID-19 pandemic. Moreover, lifetime stress was associated with reduced SARS-CoV-2-specific antibodies in human milk, while current perceived stress was not. Our findings emphasize the importance of psychological well-being of lactating women and the need to identify and guide (expecting) mothers with high chronic stress levels.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by METc VUmc. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
HJ and BK had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Concept and design: HJ, ER, AK, JG, and BK. Acquisition, analysis, or interpretation of data: HJ, ER, MG, AK, JG, and BK. Drafting of the manuscript: HJ, ER, and BK. Critical manuscript revision for intellectual content: MG, AK, JG, and BK. Statistical analysis: HJ, ER, and BK. Obtained funding: MG, JG, and BK. Administrative, technical, or material support: HJ, ER, MG, JG, and BK. Supervision: JG and BK. All authors contributed to the article and approved the submitted version.
Funding
This study was funded by Stichting Steun Emma Kinderziekenhuis. The funder did not have any influence on the data collection or interpretation.
Conflict of Interest
JG was the founder and director of the Dutch National Human Milk Bank and a member of the National Health Council and has been a member of the National Breastfeeding Council from March 2010 to March 2020.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Gotzinger F, Santiago-Garcia B, Noguera-Julian A, Lanaspa M, Lancella L, Calo Carducci FI, et al. COVID-19 in children and adolescents in Europe: a multinational, multicentre cohort study. Lancet Child Adolesc Health. (2020) 4:653–61. doi: 10.1016/S2352-4642(20)30177-2
2. Hanson LA. Breastfeeding provides passive and likely long-lasting active immunity. Ann Allergy Asthma Immunol. (1998) 81:523–33. doi: 10.1016/S1081-1206(10)62704-4
3. Bachrach VR, Schwarz E, Bachrach LR. Breastfeeding and the risk of hospitalization for respiratory disease in infancy: a meta-analysis. Arch Pediatr Adolesc Med. (2003) 157:237–43. doi: 10.1001/archpedi.157.3.237
4. Payne S, Quigley MA. Breastfeeding and infant hospitalisation: analysis of the UK 2010 infant feeding survey. Matern Child Nutr. (2017) 13:12263. doi: 10.1111/mcn.12263
5. Hanson LA. Session 1: Feeding and infant development breast-feeding and immune function. Proc Nutr Soc. (2007) 66:384–96. doi: 10.1017/S0029665107005654
6. Perl SH, Uzan-Yulzari A, Klainer H, Asiskovich L, Youngster M, Rinott E, et al. SARS-CoV-2-specific antibodies in breast milk after COVID-19 vaccination of breastfeeding women. JAMA. (2021) 325:2013–4. doi: 10.1001/jama.2021.5782
7. Baird JK, Jensen SM, Urba WJ, Fox BA, Baird JR. SARS-CoV-2 antibodies detected in mother's milk post-vaccination. J Hum Lact. (2021) 37:492–8. doi: 10.1177/08903344211030168
8. Romero Ramírez DS, Lara Pérez MM, Carretero Pérez M, Suárez Hernández MI, Martín Pulido S, Pera Villacampa L, et al. SARS-CoV-2 antibodies in breast milk after vaccination. Pediatrics. (2021) 148:2286. doi: 10.1542/peds.2021-052286
9. Pace RM, Williams JE, Jarvinen KM, Belfort MB, Pace CD, Lackey KA, et al. COVID-19 and human milk: SARS-CoV-2, antibodies, and neutralizing capacity. medRxiv. (2020). doi: 10.1101/2020.09.16.20196071
10. Fox A, Marino J, Amanat F, Krammer F, Hahn-Holbrook J, Zolla-Pazner S, et al. Robust and specific secretory IgA against SARS-CoV-2 detected in human milk. iScience. (2020) 23:101735. doi: 10.1016/j.isci.2020.101735
11. Juncker HG, Mulleners SJ, van Gils MJ, de Groot CJM, Pajkrt D, Korosi A, et al. The levels of SARS-CoV-2 specific antibodies in human milk following vaccination. J Hum Lact. (2021) 37:477–84. doi: 10.1177/08903344211027112
12. Juncker HG, Mulleners SJ, van Gils MJ, Bijl TPL, de Groot CJM, Pajkrt D, et al. Comparison of SARS-CoV-2-specific antibodies in human milk after mRNA-based COVID-19 vaccination and infection. Vaccines. (2021) 9:1475. doi: 10.3390/vaccines9121475
13. Dumitriu D, Emeruwa UN, Hanft E, Liao GV, Ludwig E, Walzer L, et al. Outcomes of neonates born to mothers with severe acute respiratory syndrome coronavirus 2 infection at a large medical center in New York City. JAMA Pediatr. (2020) 2:4298. doi: 10.1001/jamapediatrics.2020.4298
14. Chambers C, Krogstad P, Bertrand K, Contreras D, Tobin NH, Bode L, et al. Evaluation for SARS-CoV-2 in breast milk from 18 infected women. J Am Med Assoc. (2020) 324:1347–8. doi: 10.1001/jama.2020.15580
15. Pace RM, Williams JE, Jarvinen KM, Belfort MB, Pace CDW, Lackey KA, et al. Characterization of SARS-CoV-2 RNA, Antibodies, and Neutralizing Capacity in Milk Produced by Women with COVID-19. mBio. (2021) 12:20. doi: 10.1128/mBio.03192-20
16. Auriti C, De Rose DU, Tzialla C, Caforio L, Ciccia M, Manzoni P, et al. Vertical transmission of SARS-CoV-2 (COVID-19): are hypotheses more than evidences? Am J Perinatol. (2020) 37(S 02):S31–S8. doi: 10.1055/s-0040-1714346
17. Salvatori G, De Rose DU, Amadio P, Reposi MP, Piccioni L, Concato C, et al. Universal screening for SARS-CoV-2 of all human milk bank samples. J Human Lact: Off J Int Lact Consult Assoc. (2021) 37:40–2. doi: 10.1177/0890334420962074
18. Kilic T, Kilic S, Berber NK, Gunduz A, Ersoy Y. Investigation of SARS-CoV-2 RNA in milk produced by women with COVID-19 and follow-up of their infants: a preliminary study. Int J Clin Pract. (2021) 75:e14175. doi: 10.1111/ijcp.14175
19. Moirasgenti M, Doulougeri K, Panagopoulou E, Theodoridis T. Psychological stress reduces the immunological benefits of breast milk. Stress and Health. (2019) 35:681–5. doi: 10.1002/smi.2903
20. Emmett PM, Rogers IS. Properties of human milk and their relationship with maternal nutrition. Early Hum Dev. (1997) 49:S7–S28. doi: 10.1016/S0378-3782(97)00051-0
21. Bachour P, Yafawi R, Jaber F, Choueiri E, Abdel-Razzak Z. Effects of smoking, mother's age, body mass index, and parity number on lipid, protein, and secretory immunoglobulin A concentrations of human milk. Breastfeed Med. (2012) 7:179–88. doi: 10.1089/bfm.2011.0038
22. Groer MW, Humenick S, Hill PD. Characterizations and psychoneuroimmunologic implications of secretory immunoglobulin A and cortisol in preterm and term breast milk. J Perinat Neonatal Nurs. (1994) 7:42–51. doi: 10.1097/00005237-199403000-00005
23. Groer M, Davis M, Steele K. Associations between human milk SIgA and maternal immune, infectious, endocrine, and stress variables. J Hum Lact. (2004) 20:153-8. doi: 10.1177/0890334404264104
24. Groër M, Davis M, Casey K, Short B, Smith K, Groër S. Neuroendocrine and immune relationships in postpartum fatigue. MCN Am J Matern Child Nurs. (2005) 30:133–8. doi: 10.1097/00005721-200503000-00012
25. Kawano A, Emori Y. The relationship between maternal postpartum psychological state and breast milk secretory immunoglobulin A level. J Am Psychiatr Nurses Assoc. (2015) 21:23–30. doi: 10.1177/1078390314566882
26. Ceulemans M, Hompes T, Foulon V. Mental health status of pregnant and breastfeeding women during the COVID-19 pandemic: a call for action. Int J Gynecol & Obst. (2020) 151:146–7. doi: 10.1002/ijgo.13295
27. Zanardo V, Manghina V, Giliberti L, Vettore M, Severino L, Straface G. Psychological impact of COVID-19 quarantine measures in northeastern Italy on mothers in the immediate postpartum period. Int J Gynaecol Obstet. (2020) 150:184–8. doi: 10.1002/ijgo.13249
28. Stepowicz A, Wencka B, Bieńkiewicz J, Horzelski W, Grzesiak M. Stress and Anxiety Levels in Pregnant and Post-Partum Women during the COVID-19 Pandemic. International journal of environmental research and public health. (2020) 17:9450. doi: 10.3390/ijerph17249450
29. Molgora S, Accordini M. Motherhood in the Time of Coronavirus: The impact of the pandemic emergency on expectant and postpartum women's psychological well-being. Front Psychol. (2020) 11:567155. doi: 10.3389/fpsyg.2020.567155
30. Cohen S, Kamarck T, Mermelstein R, A. global measure of perceived stress. J Health Soc Behav. (1983) 24:385–96. doi: 10.2307/2136404
32. Wolfe J, Kimerling R, Brown P, Chrestman K, Levin K. The life stressor checklist-revised (LSC-R) [measurement instrument] (1997). Available online at: http://www.ptsd.va.gov/professional/assessment/te-measures/lsc-r.asp
33. Juncker HG, Romijn M, Loth VN, Ruhe EJM, Bakker S, Kleinendorst S, et al. Antibodies against SARS-CoV-2 in human milk: milk conversion rates in the Netherlands. J Hum Lact. (2021) 37:469–76. doi: 10.1177/08903344211018185
34. Paul S, Corwin EJ. Identifying clusters from multidimensional symptom trajectories in postpartum women. Res Nurs Health. (2019) 42:119–27. doi: 10.1002/nur.21935
35. Kawano A, Emori Y. Changes in maternal secretory immunoglobulin a levels in human milk during 12 weeks after parturition. Am J Hum Biol. (2013) 25:399–403. doi: 10.1002/ajhb.22387
36. Groer M, Ashmeade T, Duffy A, Morse S, Zaritt J. Changes in the immune components of preterm human milk and associations with maternal and infant characteristics. J Obstet Gynecol Neonatal Nurs. (2016) 45:639–48. doi: 10.1016/j.jogn.2016.04.009
37. Mappa I, Distefano FA, Rizzo G. Effects of coronavirus 19 pandemic on maternal anxiety during pregnancy: a prospectic observational study. J Perinat Med. (2020) 48:545–50. doi: 10.1515/jpm-2020-0182
38. Hiiragi K, Obata S, Misumi T, Miyagi E, Aoki S. Psychological stress associated with the COVID-19 pandemic in postpartum women in Yokohama, Japan. J Obstet Gynaecol Res. (2021). doi: 10.1111/jog.14776
39. Goyal D, Selix NW. Impact of COVID-19 on maternal mental health. MCN Am J Matern Child Nurs. (2021) 46:103–9. doi: 10.1097/NMC.0000000000000692
40. Almeida M, Shrestha AD, Stojanac D, Miller LJ. The impact of the COVID-19 pandemic on women's mental health. Arch Womens Ment Health. (2020) 23:741–8. doi: 10.1007/s00737-020-01092-2
41. Ceulemans M, Foulon V, Ngo E, Panchaud A, Winterfeld U, Pomar L, et al. Mental health status of pregnant and breastfeeding women during the COVID-19 pandemic-A multinational cross-sectional study. Acta Obstet Gynecol Scand. (2021) 100:1219–29. doi: 10.1111/aogs.14092
42. Chen Q, Li W, Xiong J, Zheng X. Prevalence and risk factors associated with postpartum depression during the COVID-19 pandemic: a literature review and meta-analysis. Int J Environ Res Public Health. (2022) 19:2219. doi: 10.3390/ijerph19042219
43. Wyszynski DF, Hernandez-Diaz S, Gordon-Dseagu V, Ramiro N, Koenen KC. Stress levels among an international sample of pregnant and postpartum women during the COVID-19 pandemic. J Matern Fetal Neonatal Med. (2021) 64:1–9. doi: 10.1080/14767058.2021.1936489
44. Ipsen C, van Veldhoven M, Kirchner K, Hansen JP. Six key advantages and disadvantages of working from home in Europe during COVID-19. Int J Environ Res Public Health. (2021) 18:1826. doi: 10.3390/ijerph18041826
45. Pierce M, Hope H, Ford T, Hatch S, Hotopf M, John A, et al. Mental health before and during the COVID-19 pandemic: a longitudinal probability sample survey of the UK population. The lancet Psychiatry. (2020) 7:883–92. doi: 10.1016/S2215-0366(20)30308-4
46. Ziomkiewicz A, Apanasewicz A, Danel DP, Babiszewska M, Piosek M, Orczyk-Pawiłowicz M. Maternal distress and social support are linked to human milk immune properties. Nutrients. (2021) 13:1857. doi: 10.3390/nu13061857
47. Nagai N, Noguchi M, Hiraishi M, Furuta N, Nakayama H, Oka K, et al. State anxiety of a puerpera and immunity component in the mother's milk. Japanese J Pediat. (2000) 53:815–20.
49. Cohen S, Miller GE, Rabin BS. Psychological stress and antibody response to immunization: a critical review of the human literature. Psychosom Med. (2001) 63:7–18. doi: 10.1097/00006842-200101000-00002
50. Shields GS, Slavich GM. Lifetime stress exposure and health: a review of contemporary assessment methods and biological mechanisms. Soc Personal Psychol Compass. (2017) 11:12335. doi: 10.1111/spc3.12335
Keywords: SARS-CoV-2, stress, COVID-19, lactation, passive immunity, breast milk
Citation: Juncker HG, Ruhé EJM, Korosi A, van Goudoever JB, van Gils MJ and van Keulen BJ (2022) Maternal Stress and Human Milk Antibodies During the COVID-19 Pandemic. Front. Nutr. 9:923501. doi: 10.3389/fnut.2022.923501
Received: 19 April 2022; Accepted: 01 June 2022;
Published: 30 June 2022.
Edited by:
Julio Villena, CONICET Centro de Referencia para Lactobacilos (CERELA), ArgentinaReviewed by:
Susana Salva, Centro de Referencia para Lactobacilos (CONICET), ArgentinaTalat Kilic, Inönü University, Turkey
Copyright © 2022 Juncker, Ruhé, Korosi, van Goudoever, van Gils and van Keulen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Johannes B. van Goudoever, aC52YW5nb3Vkb2V2ZXJAYW1zdGVyZGFtdW1jLm5s