 Marina Alonso-Cabezas1
Marina Alonso-Cabezas1 Marina Pollán2,3
Marina Pollán2,3 Isabel Alonso-Ledesma2Nerea Fernández de Larrea-Baz2,3Pilar Lucas2
Isabel Alonso-Ledesma2Nerea Fernández de Larrea-Baz2,3Pilar Lucas2 Ángeles Sierra2,3Adela Castelló2,3,4Marina Nieves Pino5
Ángeles Sierra2,3Adela Castelló2,3,4Marina Nieves Pino5 Beatriz Pérez-Gómez2,3Mercedes Martínez-Cortés5
Beatriz Pérez-Gómez2,3Mercedes Martínez-Cortés5 Virginia Lope2,3*
Virginia Lope2,3* Emma Ruiz-Moreno2,3
Emma Ruiz-Moreno2,3- 1Department of Nutrition and Food Sciences, Faculty of Farmacy, Complutense University of Madrid, Madrid, Spain
- 2Department of Epidemiology of Chronic Diseases, National Center for Epidemiology, Instituto de Salud Carlos III, Madrid, Spain
- 3Consortium for Biomedical Research in Epidemiology & Public Health (CIBERESP), Instituto de Salud Carlos III, Madrid, Spain
- 4Department of Surgery, Medical and Social Sciences, Faculty of Medicine, University of Alcalá, Alcalá de Henares, Madrid, Spain
- 5Servicio de Prevención y Promoción de la Salud, Madrid Salud, Ayuntamiento de Madrid, Madrid, Spain
Background: A healthy diet when approaching menopause could prevent some of the symptoms associated with the climacteric. Few studies examine adherence to current healthy dietary recommendations in middle-aged premenopausal women. Our objective was to analyze the diet quality and the adherence to the Spanish Society of Community Nutrition (SENC) dietary recommendations in middle-aged Spanish premenopausal women, and to identify the associated sociodemographic and lifestyle factors.
Methods: This is a cross-sectional study based on 1251 premenopausal women, aged 39–50, who attended to Madrid City Council Medical Diagnostic Center. Women completed an epidemiological and a food frequency questionnaire. Degree of adherence to the SENC recommendations was estimated with a score that evaluated null (0 points) and full (1 point) adherence of each specific recommendation. Associations were explored using an ordinal logistic multivariable regression model.
Results: Regarding food groups, the worst adherence was found for sweets, red/processed meat, olive oil and eggs. Most of the participants exceeded the recommended caloric intake from proteins and fats, and practically all of them showed vitamin D intake deficiency. The overall score ranged from 2 to 12 (out of 15), with a median of 6.0 (interquartile range: 5.0–7.0). Former smokers (OR: 1.38; 95%CI: 1.08–1.78), as well as those with higher educational level (ORSSecondary:1.68; 95%CI: 0.97–2.93, ORUniversity:1.82; 95%IC: 1.05–3.14), with two or more children (OR: 1.31; 95%IC: 1.00-1.72), with higher caloric intake (OR>2188.2kcal/day: 8.22; 95%CI: 6.19–10.92) and with greater physical activity (OR≥21METS−h/week: 1.29; 95%CI: 0.95-1.76) showed greater adherence.
Conclusions: Almost two-thirds of middle-aged premenopausal participants showed low or moderate compliance with SENC recommendations. Education, smoking, parity, and physical activity were associated with the degree of adherence to these recommendations.
Introduction
When studying different climacteric stages, it is often remarked the impact that perimenopause and menopause has on women's quality of life, but the premenopausal period is frequently forgotten on this matter. Premenopause is a natural period in a woman's adult life defined as the phase prior to perimenopause or the menopausal transition (1). There are studies showing that the clinical manifestations of the menopause can appear early, even before menstrual irregularities (2).
The fact that many middle-aged premenopausal women begin to show a clinical decline during the period close to menopausal transition, leads us to emphasize the need to assess the health status of these women before the onset of menopause. Although therapeutic intervention may be necessary, certain lifestyles, such as diet and physical activity, can help reduce many typical symptoms. The Mediterranean diet can be a useful tool in the management of menopause related obesity (3), and can improve cardiovascular risk factors, bone mineral density, mood, symptoms of depression, and prevent cognitive decline (4).
Diet quality is affected by a large number of factors, not only sex and age but also education, occupation, income level, and conventional indexes of socioeconomic status (5, 6). Studying the sociodemographic characteristics of women associated with dietary patterns is, therefore, very helpful to understand the inequalities of health and as it is currently of great interest in the nutritional epidemiology field (7). The study of the nutritional status of middle-aged women approaching menopause, as well as the associated factors or lifestyles, can help prevent or mitigate climacteric symptoms and improve the quality of life of these women.
Although several studies have been published that associate dietary intake with various menopausal symptoms (advising a high consumption of fruits, vegetables, whole grains, low-fat foods and products with high content in vitamin D) as a recent review suggests (8), these recommendations are very general and do not inform on the frequency and weight of daily servings. In 2019, the Spanish Society of Community Nutrition (SENC) updated its Food-Based Dietary Guidelines (9). These guidelines are based on the current dietary model of the Spanish population and include the Healthy Eating Pyramid, recommended serving sizes, practical recommendations for designing menus, purchasing, storing, and cooking food (10). Although there are previous studies that have evaluated the degree of compliance with the SENC dietary recommendations in the Catalan (11) and Balearic (12) population, in Spanish men and women from the EPIC (13), ANIBES (14), and SUN (15) studies, as well as in adolescents (16) and in women before and during pregnancy (17), none of them have focused on evaluating the factors associated with adherence to these recommendations in women approaching menopause.
The objective of this study is to evaluate the diet quality and the adherence to the SENC dietary recommendations in middle-aged Spanish premenopausal women, and to explore the sociodemographic and lifestyle factors that influence such adherence.
Materials and Methods
Study Population and Data Collection
DDM-Madrid is a cross-sectional study that recruited, between June 2013 and May 2015, a total of 1466 premenopausal women (39–50 years) that attended the Madrid City Council Medical Diagnostic Center (Madrid Salud), where they attended for their occupational gynecological examination. Women were invited to participate by phone before their medical appointment, and 88% agreed to collaborate. The study was conducted in accordance with the Declaration of Helsinki guidelines and was approved by the Ethics and Animal Welfare Committee of the Institute of Health Carlos III. All participants signed an informed consent form.
Trained interviewers administered a face-to-face structured computerized epidemiological questionnaire to participants, which included sociodemographic information, work history, tobacco smoking and alcohol consumption. Recreational physical activity during the previous year was measured using a translation of a validated questionnaire that considers duration, frequency, and intensity of 26 activities (18). Total metabolic equivalents (MET-h/week) were calculated according to the 2011 Compendium of Physical Activities (19). In addition, weight and height of the participants were measured using a certified bioimpedance scale (Tanita SC-330). After measuring each variable twice, with a third measure if the first two were discrepant, the mean values were used in the analyses.
Participants also answered a 117-item semi-quantitative food frequency questionnaire (FFQ) that has been validated in the Spanish adult population (20). It gathered information on eating habits for the previous 12 months, specifying standard portions or servings through 9 frequency categories (from “never or less than once a month” to “6 or more times a day”). The data was collected through an Access form and exported to Excel. The mean daily intake of some selected edible nutrients was calculated using the food composition tables of the U.S. Department of Agriculture (21), and other published tables for Spanish foods (22). The nutritional results as well as the data collected in all questionnaires were exported to STATA/MP 15.1 software.
Caloric and lipid profile was obtained according to the ranges recommended by Moreiras et al. (23), and the percentage of women at risk of insufficient intake were described following the European Food Safety Authority (EFSA) recommendations (24).
Subsequently, a score was created to assess the degree of compliance with the dietary recommendations for healthy eating proposed by the SENC (9, 10). Supplementary Table 1 shows the FFQ foods included in the score. When the participant complied with the recommendation of a food group, we assigned a score of 1, and when she did not comply, we assigned a score of 0. The final score was obtained as the sum of the individual scores. Therefore, our score ranged from 0 (when none of the recommendations were met) to 15 (when all were met).
After excluding 190 women who did not complete the FFQ, 13 participants for implausible dietary data, 5 participants who followed a vegetarian diet, and 7 without information on covariates, the final sample size included 1251 participants (Supplementary Figure 1).
Statistical Methods
Descriptive analyses of women's characteristics, food groups, and energy and micronutrient intake were carried out using medians and interquartile ranges (IQR) for continuous variables, and absolute figures and percentages for categorical variables.
Participants were categorized into three groups, according to the tertiles of the SENC global adherence score: low adherence (<6), moderate adherence (6), and high adherence (7–12). Baseline women's characteristics by level of adherence to the SENC recommendations were described with total figures and percentages, and significant differences between the three levels of adherence (low, moderate and high) and these characteristics were tested with Pearson's chi-square tests.
The association between the three categories of adherence and lifestyle and sociodemographic variables was assessed using an ordinal multivariable logistic regression model. Proportional odds assumption was tested using the Brant test. This model was adjusted for educational level plus those variables that were associated with adherence to the SENC recommendations in the previous analysis (p <0.20). Analyses were performed using STATA/MP 15.1 software.
Results
Diet quality according to the nutrient intake of the women is summarized in Tables 1, 2. Regarding caloric profile (distribution of macronutrients and alcohol as a percentage of total energy), most of the women exceeded the recommendations for caloric intake from proteins and fats, while caloric intake from carbohydrates was lower than recommended (i.e., were under 50%) for 92% of the participants. The consumption of saturated fat was higher than recommended, while the consumption of monounsaturated fats was lower in a large percentage of our participants (90.2% and 79.9%, respectively) (Table 1).
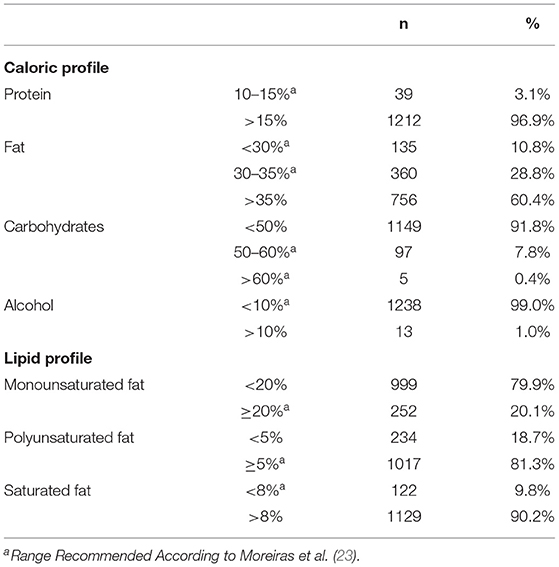
Table 1. Caloric profile and lipid profilea.
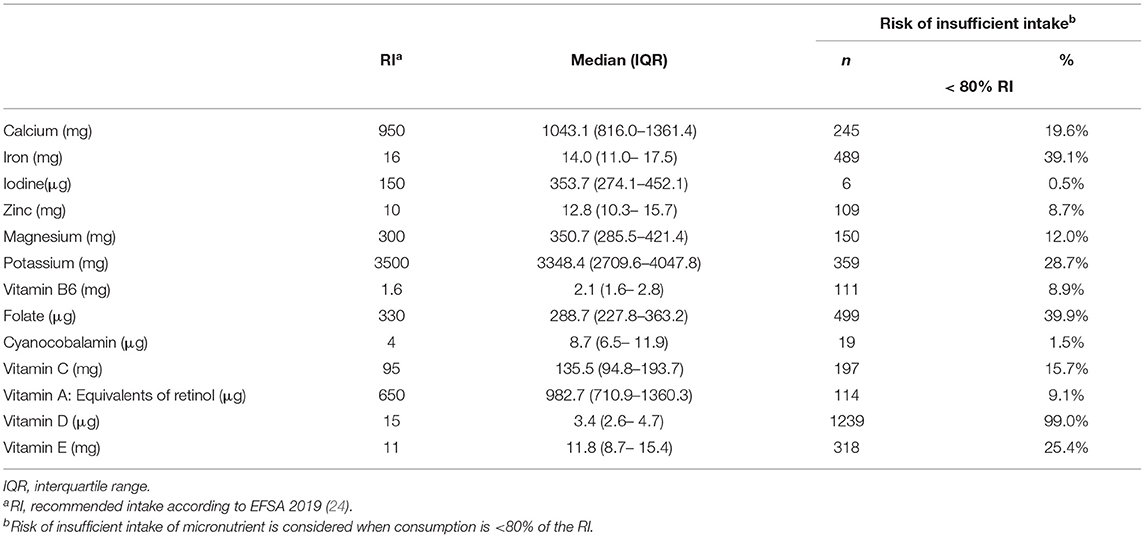
Table 2. Micronutrient daily intake and percentage of women at risk of insufficient intake.
Table 2 shows the median micronutrient intake and the percentage of women at risk of insufficient intake. The most generalized deficient intake was observed for vitamin D (99.0%), followed by far by folate (39.9%), iron (39.1%), and potassium (28.7%).
Table 3 shows the score for the degree of adherence to the SENC recommendations by food groups, their distribution, and the median daily and weekly intake by food groups. Most women did not comply with the daily recommended amounts of olive oil (94.1%), fruits (88.1%), vegetables (79.2%), cereals, potatoes, pulses and others (73.3%) and dairy products (54.1%). On the other hand, the recommendation for water intake was highly met (71.6%). Regarding weekly recommendations, the worst adherences were found for sweets (97.2%), red meat, processed meat and other fats (95.4%), eggs (92.9%), nuts (75.6%) and white meat (65.8.0%), while a high adherence was observed for snacks (97.9%), alcohol (92.2%), legumes (81.4%) and fish (73.4%).
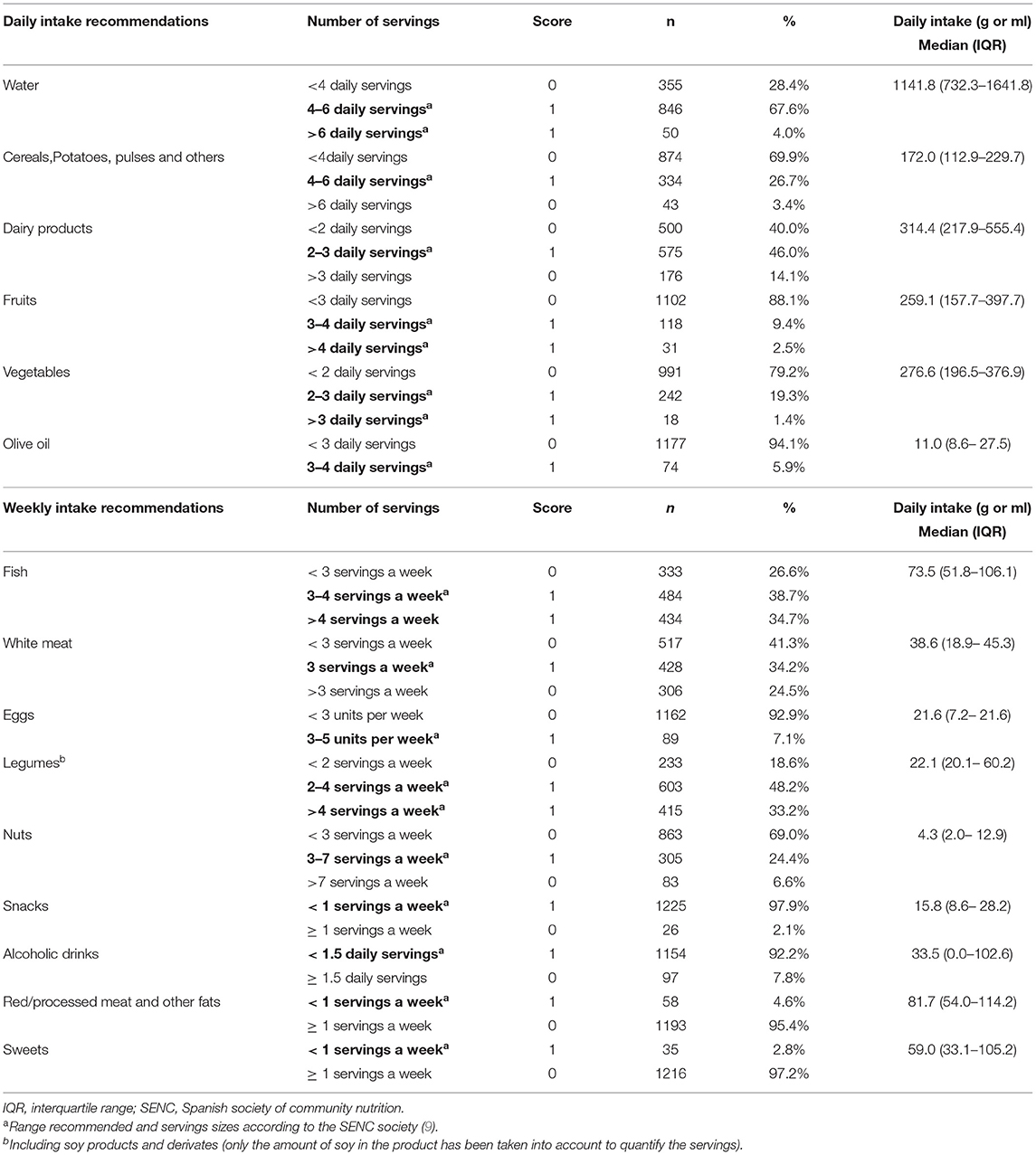
Table 3. Score and adherence to the SENC food–based dietary recommendations.
Table 4 shows the distribution of sociodemographic and life-style characteristics by tertiles of adherence to the SENC recommendations. The overall score ranged from 2 to 12, with a median of 6.0 (IQR: 5.0-7.0). The percentage of women with low, moderate, and high adherence was 40.5%, 27.8% and 31.7%, respectively. In general, low adherence was more frequent among nulliparous, smokers, and those who consumed fewer calories.
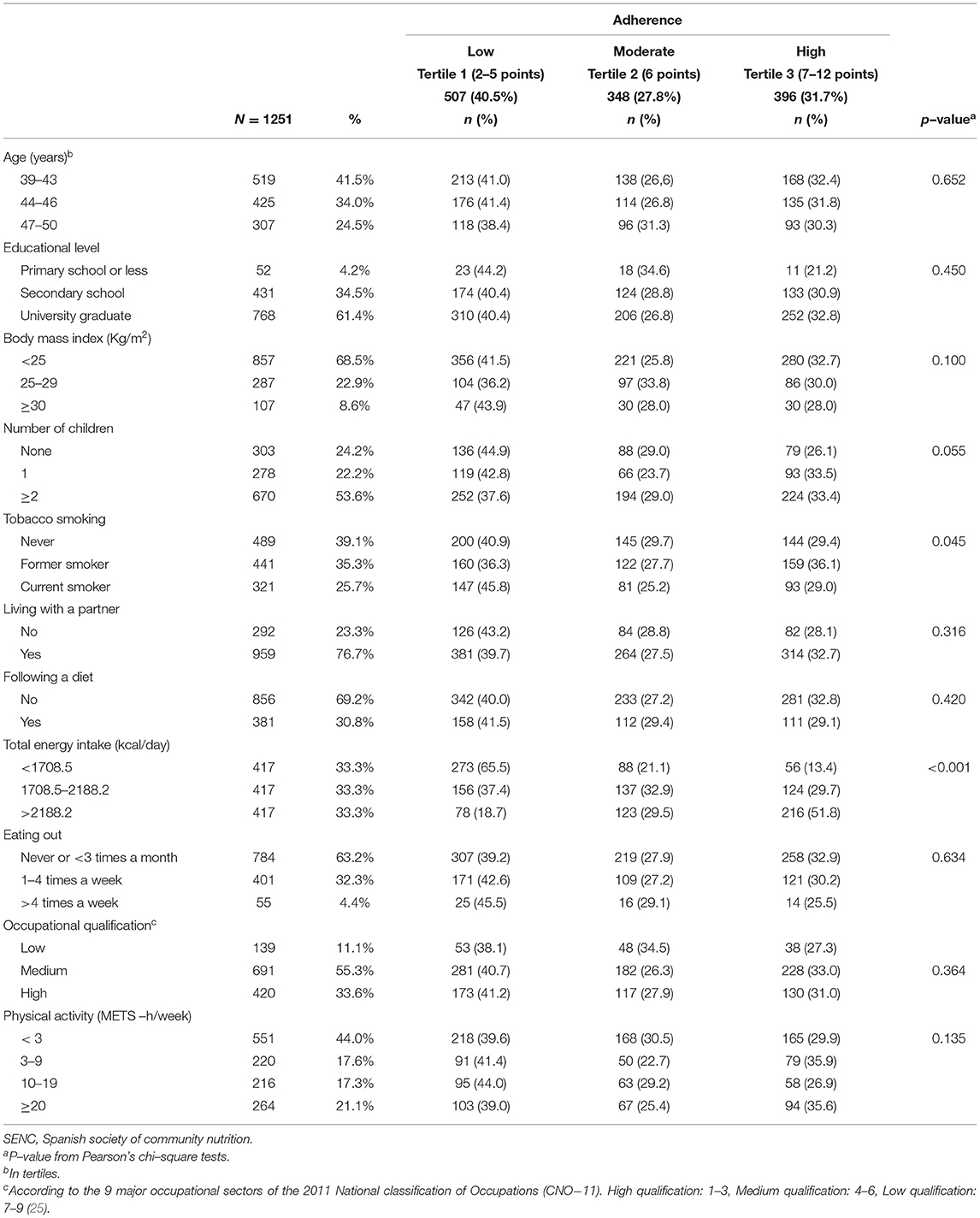
Table 4. Characteristics of the women, overall and by tertiles of the SENC adherence score.
The adjusted association between adherence to the SENC score and several sociodemographic and lifestyle factors is shown in Table 5. Former smokers (OR: 1.38; 95%CI: 1.08–1.78), as well as those with higher educational level (ORsecondary:1.68; 95%CI: 0.97–2.93, ORuniversity:1.82; 95%CI: 1.05–3.14), with two or more children (OR: 1.31; 95%CI: 1.00-1.72), with higher caloric intake (OR<2188.2kcal/day: 8.22; 95%CI: 6.19–10.92) and with greater physical activity (OR≥21METS−h/week: 1.29; 95%CI: 0.95–1.76) showed greater adherence to the SENC score, while those with higher body mass index (BMI) (OR≥30: 0.77; 95%CI: 0.52–1.15) presented a lower degree of adherence.
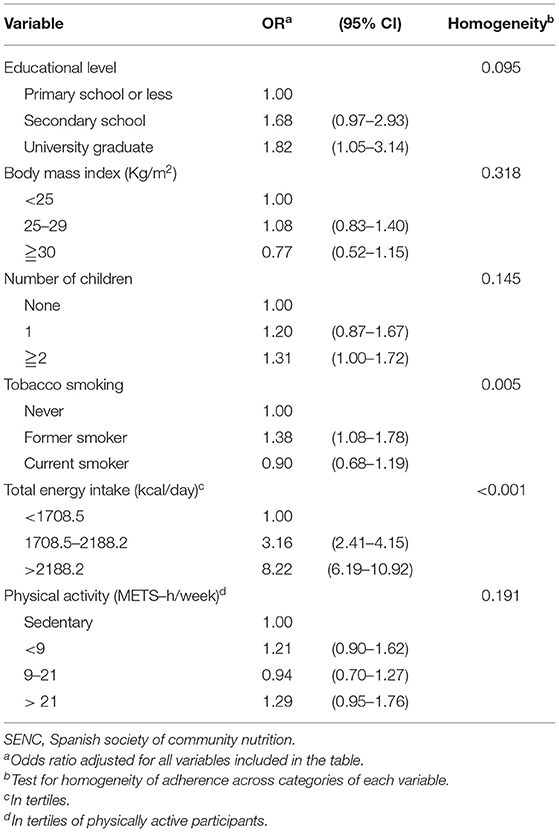
Table 5. Association between adherence to SENC recommendations and potential influential factors.
Discussion
This study tries to evaluate the quality of the diet in middle-aged Spanish premenopausal women, the degree of compliance with the SENC food-based dietary guidelines, and to explore the sociodemographic and lifestyle factors that are associated. Overall, 41% of participants showed low compliance with these recommendations, while 32% showed high compliance. More than 85% of the women did not consume the daily or weekly recommended amounts either due to a lack of olive oil, fruit and eggs, or due to an excess of sweets, red or processed meat. Practically all of participants had an insufficient intake of vitamin D. Most women exceeded the recommendations for caloric intake from proteins and fat (mainly saturated fat). Former smokers, those with a higher educational level, with two or more children or with higher caloric intake showed greater adherence to the SENC dietary recommendations.
The results on daily servings consumed are similar to those detected by Úbeda et al. in Spanish menopausal women (26). These authors -taking the 2004 SENC recommendations as reference (27) found an insufficient intake of fruits and nuts, as well as a high consumption of meat and its derivatives and sweets. However, and unlike our results, the alcohol consumption of their participants was higher than that recommended by the SENC (10). On the other hand, when comparing the mean consumption in grams with that of the nationally representative sample of the Spanish women population of the ANIBES study, the intake of dairy products, vegetables and fruits is lower in our participants compared to theirs; the consumption of water and eggs is higher, and that of olive oil and alcohol is very similar (28).
Considering the caloric profile, we have observed that the energy intake from fats and proteins is above current SENC recommendations, while the intake from carbohydrates (fruits, vegetables, cereals, potatoes, and legumes) is below. These results are in line with the evolution observed in the Spanish diet over the last fifty years, with a decrease in the contribution of carbohydrates to the diet and an increase of fats (29). Since fat accumulation and redistribution often occur during the climacteric stage, the contribution of high-fat foods at this stage of life should be carefully examined (30). A distinction must also be made between foods rich in polyunsaturated fats from those rich in saturated fats, since the first group is beneficial for the prevention of some degenerative diseases, and it has been described that they can improve the symptoms derived from menopause (31). Although the consumption of polyunsaturated fat was adequate in 81% of our participants, the consumption of saturated fat was excessive in 90% of them. The main sources of saturated fatty acids in the diet of the Spanish population are milk and dairy products, meat and its derivatives, and oils and fats (32). Several studies have associated the consumption of saturated fats with an increase in the intensity of symptoms related to menopause or with depressive symptoms in middle-aged women (8). Regarding monounsaturated fats (MUFA), their proportional contribution to the overall caloric intake was lower than that recommended by Moreiras et al. (23) in most of our women, contrary to what was observed in the previously mentioned study by Varela-Moreiras et al. (29). This last result may be due to the lower consumption of olive oil (main source of MUFAs in the Mediterranean diet) observed in our participants.
Micronutrient intake was, with some exceptions, mostly in accordance with EFSA recommendations. The main exception was vitamin D intake, which was lower than recommended in 99% of participants. This is consistent with the fact that vitamin D deficiency is very frequent in Spain, involving approximately 40% of the adult population (33). Vitamin D is necessary for intestinal calcium absorption and bone and muscle homeostasis, and can help reduce menopausal-related symptoms and improve sexual function and bone health in perimenopausal women (34). However, it should be noted that the most important source of vitamin D is sun exposure, and that only a modest quantity can be obtained from foods such as fatty fish, dairy products or eggs (35). We also found intakes of iron, folate and potassium below the recommended levels. These micronutrients must be carefully monitored over the years to detect possible negative trends early.
Compliance with the SENC recommendations was higher in women with higher educational level, in former smokers, in those with higher caloric intake, in those having two or more children and, to a lesser extent, in those with higher physical activity. The greater adherence in people with higher educational level is a fairly consistent finding in Europe, mainly in relation to fruits and vegetables consumption (36). It has been described that higher educational level can be related to increased competencies, skills and knowledge, which are important for engaging with health education messages and avoiding harmful behaviors (37). The higher cost of healthy diets has also been associated with lower adherence to these diets in population groups with lower educational level (38, 39).
The better adherence detected in women with children is consistent with that reported by other authors (40). Regarding grocery shopping, it has been observed that women with children tend to focus more on nutrition and the preferences of children, while women without children pay more attention to the taste and the preferences of other household members. Women without children have also been found to eat more often in fast food chains (41).
On the other hand, the greater adherence observed in former smokers may be explained by the fact that the acquisition of a healthy lifestyle (such as quitting smoking) can promote the acquisition of other healthy behaviors, such as improved diet or physical activity. In this sense, in a randomized controlled trial on different strategies to quit smoking, Berg et al. observed that reducing and quitting smoking was associated with higher intake of fruits and vegetables and more walking for exercise at 26 week follow-up (42).
Regarding total energy intake, its increase is usually associated with an increase in nutrient intake (43). However, a study that evaluated the diet quality in a representative Spanish population, showed that low energy density diets are associated with a healthier lifestyle and tend to be closer to the SENC dietary recommendations than high-energy density diets (44). Another study conducted in the elderly population, showed that meeting nutrient intake recommendations is difficult with low energy consumption, even in the case of diets based on the Mediterranean dietary pattern (45). A good diet should therefore achieve a greater richness in nutrients with a low energy intake (always within the recommendations).
Finally, the greater adherence detected in participants with greater physical activity has also been reported in previous studies, in which a positive association was observed with adherence to a “Spanish-Mediterranean” diet (46), Mediterranean diet (40) and other health conscious diets (44). In general, people with higher level of physical activity tend to be healthier than less active people, and tend to consume a more varied diet, while sedentary people consume more fast food products and fewer fruits and vegetables, which responds to less healthy eating profiles (47, 48). Regarding the SENC dietary recommendations in particular, lower adherence has been observed in Spanish adolescents with low physical activity (16), as well as greater adherence to the SENC food pyramid among the most physically active participants of the SUN cohort (15).
Our study has several strengths. Firstly, to our knowledge, this is the first study examining sociodemographic and lifestyle determinants associated with adherence to the SENC dietary recommendations in premenopausal women. We also count with a large sample size, a high participation rate and standard and validated tools to collect the data.
However, our study also has several limitations. First, it is a cross-sectional study, so it is not possible to establish causal relationships between the sociodemographic/lifestyle variables and compliance with the SENC recommendations. Second, these variables were self-reported, which implies a potential source of information bias. Third, these women were recruited from a single center in Madrid and, although they came from all over the province, this limits the ability to generalize the study results. With regard to dietary assessment, data were collected using FFQs, which did not prevent potential measurement errors and may suffer from inaccuracies. However, the use of FFQs still remains a widely used tool for dietary assessment in epidemiological studies (49). Finally, it is necessary to mention the limitations inherent to the calculation of the score of adherence to the SENC recommendations, such as the categorization of food intake into dichotomies of “compliance” and “non-compliance,” or the possible misclassification of some food groups (50, 51).
In conclusion, our results show that the degree of adherence to the SENC recommendations in middle-aged Spanish premenopausal women was, in general, low to moderate. Some recommendations should be promoted, mainly those related to a higher consumption of olive oil and eggs and a lower consumption of sweets, red meat, and processed meat. The consumption of vitamin D and fats, especially saturated fats, should be in accordance with the recommendations. In addition, adherence was better among more educated women, women with children, former smokers, and more physically active participants. It would be advisable to promote campaigns to disseminate the SENC recommendations, both to the general public and to this group of women in particular, as well as launching actions that promote healthier eating habits, with diets focused on preventing or mitigating climacteric symptoms and, ultimately, improve the quality of life of this group of women who are approaching menopause.
Data Availability Statement
Data described in the article are not publicly available due to restrictions imposed by the Institute of Health Carlos III Ethics Committee, but are available from the principal investigator on reasonable requests. To access the datasets requests should be directed to ER-M: ZS5ydWl6QGV4dGVybm9zLmlzY2lpaS5lcw==.
Ethics Statement
The study was reviewed and approved by the Ethics and Animal Welfare Committee of the Institute of Health Carlos III. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
MP, VL, and ER-M designed research. PL, AS, and BP-G conducted research. MP and MM-C provided essential materials. MA-C, IA-L, AC, VL, and ER-M analyzed data. MA-C, VL, ER-M, and NFL-B wrote the paper. MP, VL, and ER-M had primary responsibility for final content. All authors have read and approved the final manuscript.
Funding
This study was funded by the Spanish Ministry of Health (EC11–273) and by the Instituto de Salud Carlos III (PI15CIII/0029). The article presents independent research.
Author Disclaimer
The views expressed are those of the authors and not necessarily those of the Institute of Health Carlos III.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2022.904330/full#supplementary-material
Abbreviations
EFSA, European Food Safety Authority; FFQ, Food frequency questionnaire; MET, Total metabolic equivalents; MUFAs, Monounsaturated fatty acids; OR, Odds ratio; REDLINC, Collaborative Group for Research of the Climacteric in Latin America (Red Latinoamericana de Investigación en Climaterio).
References
1. Blümel JE, Lavín P, Vallejo MS, Sarrá S. Menopause or climacteric, just a semantic discussion or has it clinical implications? Climacteric. (2014) 17:235–41. doi: 10.3109/13697137.2013.838948
2. Blümel JE, Chedraui P, Baron G, Belzares E, Bencosme A, Calle A, et al. Menopausal symptoms appear before the menopause and persist 5 years beyond: a detailed analysis of a multinational study. Climacteric. (2012) 15:542–51. doi: 10.3109/13697137.2012.658462
3. Pugliese G, Barrea L, Laudisio D, Aprano S, Castellucci B, Framondi L, et al. Mediterranean diet as tool to manage obesity in menopause: a narrative review. Nutrition. (2020) 79–80:110991. doi: 10.1016/j.nut.2020.110991
4. Cano A, Marshall S, Zolfaroli I, Bitzer J, Ceausu I, Chedraui P, et al. The mediterranean diet and menopausal health: an EMAS position statement. Maturitas. (2020) 139:90–7. doi: 10.1016/j.maturitas.2020.07.001
5. Darmon N, Drewnowski A. Does social class predict diet quality? Am J Clin Nutr. (2008) 87:1107–17. doi: 10.1093/ajcn/87.5.1107
6. Novaković R, Cavelaars A, Geelen A, Nikolić M, Altaba II, Viñas BR, et al. Socio-Economic determinants of micronutrient intake and status in Europe: a systematic review. Public Health Nutr. (2014) 17:1031–45. doi: 10.1017/S1368980013001341
7. Murray C, Aravkin A, Zheng P, Abbafati C, Abbas K, Abbasi-Kangevari M, et al. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the global burden of disease study 2019. Lancet. (2020) 396:1223–49. doi: 10.1016/S0140-6736(20)30752-2
8. Noll PRES, Campos CAS, Leone C, Zangirolami-Raimundo J, Noll M, Baracat EC, et al. Dietary intake and menopausal symptoms in postmenopausal women: a systematic review. Climacteric. (2021) 24:128–38. doi: 10.1080/13697137.2020.1828854
9. Aranceta-Bartrina J, Partearroyo T, López-Sobaler AM, Ortega RM, Varela-Moreiras G, Serra-Majem L, et al. Updating the food-based dietary guidelines for the Spanish population: the Spanish Society of Community Nutrition (SENC) proposal. Nutrients. (2019) 11:2675. doi: 10.3390/nu11112675
10. Dapchich V, Salvador Castell G, Ribas Barva L, Perez Rodrigo C, Aranceta-Bartrina J, Serra-Majem L. Guía de la Alimentación Saludable para Atención Primaria y Colectivos Ciudadanos. Spanish(Healthy Eating Guide for Primary Care and Citizen Groups). SENC. Grupo Planeta (2018).
11. Serra-Majem L, Ribas-Barba L, Salvador G, Serra J, Castell C, Cabezas C, et al. Compliance with dietary guidelines in the Catalan population: basis for a nutrition policy at the regional level (the PAAS strategy). Public Health Nutr. (2007) 10:1406–14. doi: 10.1017/S1368980007001012
12. Tur JA, Romaguera D, Pons A. Does the diet of the balearic population, a Mediterranean-type diet, ensure compliance with nutritional objectives for the Spanish population? Public Health Nutr. (2005) 8:275–83. doi: 10.1079/PHN2004693
13. Molina-Montes E, Uzhova I, Molina-Portillo E, Huerta J-M, Buckland G, Amiano P, et al. Adherence to the Spanish dietary guidelines and its association with obesity in the European Prospective Investigation into Cancer and Nutrition (EPIC)-Granada study. Public Health Nutr. (2014) 17:2425–35. doi: 10.1017/S1368980014000688
14. Rodríguez-Rodríguez E, Aparicio A, Aranceta-Bartrina J, Gil Á, González-Gross M, Serra-Majem L, et al. Low adherence to dietary guidelines in Spain, especially in the overweight/obese population: the ANIBES Study. J Am Coll Nutr. (2017) 36:240–47. doi: 10.1080/07315724.2016.1248246
15. Gómez-Donoso C, Martínez-González MÁ, Martínez JA, Sayón-Orea C, Fuente-Arrillaga C de. la, Bes-Rastrollo M. Adherence to dietary guidelines for the Spanish population and risk of overweight/obesity in the SUN cohort. PLoS ONE. (2019) 14:e0226565. doi: 10.1371/journal.pone.0226565
16. Roura E, Milà-Villarroel R, Lucía Pareja S, Adot Caballero A. Assessment of eating habits and physical activity among Spanish adolescents. the “Cooking and Active Leisure” TAS Program. PLoS ONE. (2016) 11:e0159962. doi: 10.1371/journal.pone.0159962
17. Olmedo-Requena R, Gómez-Fernández J, Mozas-Moreno J, Lewis-Mikhael A-M, Bueno-Cavanillas A, Jiménez-Moleón J-J. Factors associated with adherence to nutritional recommendations before and during pregnancy. Women Health. (2018) 58:1094–11. doi: 10.1080/03630242.2017.1388332
18. Chasan-Taber L, Erickson JB, Nasca PC, Chasan-Taber S, Freedson PS. Validity and reproducibility of a physical activity questionnaire in women. Med Sci Sports Exerc. (2002) 34:987–92. doi: 10.1097/00005768-200206000-00013
19. Ainsworth BE, Haskell WL, Herrmann SD, Meckes N, Bassett DR, Tudor-Locke C, et al. 2011 Compendium of physical activities: a second update of codes and MET values. Med Sci Sports Exerc. (2011) 43:1575–81. doi: 10.1249/MSS.0b013e31821ece12
20. Vioque J, Navarrete-Muñoz E-M, Gimenez-Monzó D, García-de-la-Hera M, Granado F, Young IS, et al. Reproducibility and validity of a food frequency questionnaire among pregnant women in a Mediterranean área. Nutr J. (2013) 12:26. doi: 10.1186/1475-2891-12-26
21. U.S Department of Agriculture. USDA National Nutrient Database for Standard Reference, Release 21. (2008). https://www.ars.usda.gov/research/publications/publication/?seqNo115=230658 (accessed July 12, 2021).
22. Farran A, Zamora R, Cervera P. Tablas de composición de alimentos del CESNID, (CESNID food composition tables). Barcelona: Mc-Graw-Hill / Interamericana y Edicions Universitat de Barcelona. (2013).
23. Moreiras O, Carbajal A, Cabrera L, Cuadrado C. Tablas de composición de alimentos Guía de prácticas, (Food Composition Tables. Practice Guide). 19th ed. Madrid: Piramide (2018). p. 496.
24. European Food Safety Authority (EFSA). Dietary Reference Values for nutrients Summary report. Parma: EFSA supporting publication (2017).
25. Spanish Statistical Office. (INE) National Classification of Occupations. CNO11 (2011). https://www.ine.es/dyngs/INEbase/es/operacion.htm?c=Estadistica_C&cid=1254736177033&menu=ultiDatos&idp=1254735976614 (accessed July 1, 2021).
26. Ubeda N, Basagoiti M, Alonso-Aperte E, Varela-Moreiras G. Hábitos alimentarios, estado nutricional y estilos de vida en una población de mujeres menopáusicas españolas (Dietary food habits, nutritional status and lifestyle in menopausal women in Spain). Nutr Hosp. (2007) 22:313–21. Available online at: https://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S0212-16112007000400005
27. Dapcich V, Salvador G, Ribas L, Pérez Rodrigo C, Aranceta J, Majem LS. Guía de la alimentación saludable. (Guide for healthy eating). Madrid: SENC (2004).
28. Partearroyo T, Samaniego-Vaesken M de L, Ruiz E, Aranceta-Bartrina J, Gil Á, González-Gross M, et al. Current food consumption amongst the Spanish ANIBES study population. Nutrients. (2019) 11:E2663. doi: 10.3390/nu11112663
29. Varela-Moreiras G, Ruiz E, Valero T, Ávila JM, del Pozo S. The Spanish diet: an update. Nutr Hosp. (2013) 28:13–20. doi: 10.3305/nh.2013.28.sup5.6914
30. da Costa Pimenta W, Santos Brant Rocha J, Prates Caldeira A, Araújo Veloso Popoff D, Maia Santos V, Murça de Souza JE, et al. Abdominal obesity and association with sociodemographic, behavioral and clinical data in climacteric women assisted in primary care. PLoS ONE. (2020) 15:e0237336. doi: 10.1371/journal.pone.0237336
31. Abshirini M, Siassi F, Koohdani F, Qorbani M, Khosravi S, Aslani Z, et al. Higher intake of dietary n-3 PUFA and lower MUFA are associated with fewer menopausal symptoms. Climacteric. (2019) 22:195–01. doi: 10.1080/13697137.2018.1547700
32. Ruiz E, Ávila JM, Valero T, Del Pozo S, Rodriguez P, Aranceta-Bartrina J, et al. Macronutrient distribution and dietary sources in the Spanish population: findings from the ANIBES study. Nutrients. (2016) 8:177. doi: 10.3390/nu8030177
33. Manios Y, Moschonis G, Lambrinou C-P, Tsoutsoulopoulou K, Binou P, Karachaliou A, et al. A systematic review of vitamin D status in southern European countries. Eur J Nutr. (2018) 57:2001–36. doi: 10.1007/s00394-017-1564-2
34. Lerchbaum E. Vitamin D and menopause–a narrative review. Maturitas. (2014) 79:3–7. doi: 10.1016/j.maturitas.2014.06.003
35. Lips P, van Schoor NM, de Jongh RT. Diet, sun, and lifestyle as determinants of vitamin D status. Ann N Y Acad Sci. (2014) 1317:92–8. doi: 10.1111/nyas.12443
36. De Irala-Estévez J, Groth M, Johansson L, Oltersdorf U, Prättälä R, Martínez-González MA, et al. systematic review of socio-economic differences in food habits in Europe: consumption of fruit and vegetables. Eur J Clin Nutr. (2000) 54:706–14. doi: 10.1038/sj.ejcn.1601080
37. Maguire ER, Monsivais P. Socio-economic dietary inequalities in UK adults: an updated picture of key food groups and nutrients from national surveillance data. Br J Nutr. (2015) 113:181–89. doi: 10.1017/S0007114514002621
38. Jones NRV, Tong TYN, Monsivais P. Meeting UK dietary recommendations is associated with higher estimated consumer food costs: an analysis using the national diet and nutrition survey and consumer expenditure data, 2008-2012. Public Health Nutr. (2018) 21:948–56. doi: 10.1017/S1368980017003275
39. Hoenink JC, Beulens JWJ, Harbers MC, Boer JMA, Dijkstra SC, Nicolaou M, et al. To what extent do dietary costs explain socio-economic differences in dietary behavior? Nutr J. (2020) 19:88. doi: 10.1186/s12937-020-00608-x
40. Maugeri A, Barchitta M, Fiore V, Rosta G, Favara G, La Mastra C, et al. Determinants of adherence to the mediterranean diet: findings from a cross-sectional study in women from Southern Italy. Int J Environ Res Public Health. (2019) 16:2963. doi: 10.3390/ijerph16162963
41. Raskind IG, Woodruff RC, Ballard D, Cherry ST, Daniel S, Haardörfer R, et al. Decision-making processes shaping the home food environments of young adult women with and without children. Appetite. (2017) 113:124–33. doi: 10.1016/j.appet.2017.02.027
42. Berg CJ, Thomas JL, An LC, Guo H, Collins T, Okuyemi KS, et al. Change in smoking, diet, and walking for exercise in blacks. Health Educ Behav. (2012) 39:191–97. doi: 10.1177/1090198111432252
43. Forman M. Nutritional Epidemiology. 2nd ed. (editor). Walter Willett. Oxford University Press, New York
44. Schröder H, Covas M, Elosua R, Mora J, Marrugat J. Diet quality and lifestyle associated with free selected low-energy density diets in a representative Spanish population. Eur J Clin Nutr. (2008) 62:1194–00. doi: 10.1038/sj.ejcn.1602843
45. Padro L, Benacer R, Foix S, Maestre E, Murillo S, Sanviçens E, et al. Assessment of dietary adequacy for an elderly population based on a mediterranean model. J Nutr Health Aging. (2002) 6:31–3.
46. Sánchez-Villegas A, Delgado-Rodríguez M, Irala-Estévez J de, Martínez-González MA. Gender, age, socio-demographic and lifestyle factors associated with major dietary patterns in the Spanish Project SUN (Seguimiento Universidad de Navarra). Eur J Clin Nur. (2003) 57:285–92. doi: 10.1038/sj.ejcn.1601528
47. Johnson L, Toumpakari Z, Papadaki A. Social gradients and physical activity trends in an obesogenic dietary pattern: cross-sectional analysis of the UK national diet and nutrition survey 2008–2014. Nutrients. (2018) 10:388. doi: 10.3390/nu10040388
48. Entrala-Bueno A, Iglesias C, de Jesús F. Diet and physical activity: a healthful binomial. Eur J Clin Nutr. (2003) 57 (Suppl. 1):S63–65. doi: 10.1038/sj.ejcn.1601818
49. Shim J-S, Oh K, Kim HC. Dietary assessment methods in epidemiologic studies. Epidemiol Health. (2014) 36:e2014009. doi: 10.4178/epih/e2014009
50. Kourlaba G, Panagiotakos DB. Dietary quality indices and human health: a review. Maturitas. (2009) 62:1–8. doi: 10.1016/j.maturitas.2008.11.021
Keywords: SENC recommendations, premenopause, dietary reference values, healthy diet, dietary guidelines, dietary habits, DDM-Madrid, cross-sectional study
Citation: Alonso-Cabezas M, Pollán M, Alonso-Ledesma I, Fernández de Larrea-Baz N, Lucas P, Sierra Á, Castelló A, Pino MN, Pérez-Gómez B, Martínez-Cortés M, Lope V and Ruiz-Moreno E (2022) Sociodemographic and Lifestyle Determinants of Adherence to Current Dietary Recommendations and Diet Quality in Middle-Aged Spanish Premenopausal Women. Front. Nutr. 9:904330. doi: 10.3389/fnut.2022.904330
Received: 25 March 2022; Accepted: 05 May 2022;
Published: 14 June 2022.
Edited by:
Santiago Navas-Carretero, University of Navarra, SpainReviewed by:
Valeria Del Balzo, Sapienza University of Rome, ItalyGreggory Davis, University of Louisiana at Lafayette, United States
Copyright © 2022 Alonso-Cabezas, Pollán, Alonso-Ledesma, Fernández de Larrea-Baz, Lucas, Sierra, Castelló, Pino, Pérez-Gómez, Martínez-Cortés, Lope and Ruiz-Moreno. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Virginia Lope, dmljYXJ2YWphbEBpc2NpaWkuZXM=