
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr. , 02 June 2022
Sec. Nutritional Epidemiology
Volume 9 - 2022 | https://doi.org/10.3389/fnut.2022.891376
This article is part of the Research Topic Dietary Intake, Eating Behavior and Health Outcomes View all 36 articles
 Matteo Di Maso1†
Matteo Di Maso1† Francesca Bravi1†
Francesca Bravi1† Monica Ferraroni1,2*
Monica Ferraroni1,2* Carlo Agostoni3,4
Carlo Agostoni3,4 Simone R. B. M. Eussen5
Simone R. B. M. Eussen5 Tamás Decsi6
Tamás Decsi6 Pasqua A. Quitadamo7
Pasqua A. Quitadamo7 Paola Tonetto8
Paola Tonetto8 Chiara Peila8
Chiara Peila8 Claudio Profeti9Guglielmo Salvatori10Iwona Kazmierska11
Claudio Profeti9Guglielmo Salvatori10Iwona Kazmierska11 Adriano Decarli1Elisabetta Vacca5
Adriano Decarli1Elisabetta Vacca5 Enrico Bertino12
Enrico Bertino12 Bernd Stahl5,13
Bernd Stahl5,13 Guido E. Moro14 on behalf of MEDIDIET Working Group Members
Guido E. Moro14 on behalf of MEDIDIET Working Group MembersBackground and Aims: The content of fatty acids (FA) in human milk may be influenced by maternal nutrition. We evaluated the role of a Mediterranean diet in influencing the content of FA in human milk among 282 breastfeeding mothers participating in the MEDIDIET study.
Materials and Methods: Mediterranean Diet Score (MDS), a composite index, was used to evaluate adherence to the Mediterranean diet. It includes 9 components (i.e., vegetables, fruit, cereals, legumes, monounsaturated to saturated FA ratio – MUFA/SFA, fish, dairy products, meat, and alcohol) and therefore potentially ranges from 0 (no adherence) to 9 (complete adherence) points. None of the mothers obtained the highest score due to the low alcohol consumption in the study population. Mothers were categorized in approximate tertiles of adherence: 0–3 (34.4%), 4 (26.2%), and 5–8 points (39.4%). The mean content of FA across categories of MDS was compared using ANOVA and test for trend.
Results: A high adherence of breastfeeding mothers to the Mediterranean diet was associated with lower content of SFA in human milk (42.58 ± 4.36 for MDS = 0–3, 42.58 ± 4.89 for MDS = 4, and 40.92 ± 5.22% of fats for MDS = 5–8 points; p ANOVA and p for trend = 0.02). Conversely, a high adherence was associated with higher content of MUFA in human milk (43.27 ± 4.27 for MDS = 0–3, 43.27 ± 4.47 for MDS = 4, and 45.24 ± 5.22% of fats for MDS = 5–8 points; p ANOVA and p for trend < 0.01), ω-3 FA (1.07 ± 0.25 for MDS = 0–3, 1.22 ± 0.49 for MDS = 4, and 1.31 ± 0.51% of fats for MDS = 5–8 points; p ANOVA and p for trend < 0.01), and the major types of ω-3 FA (i.e., α-linolenic acid – ALA, eicosapentaenoic acid – EPA, docosahexaenoic acid – DHA, docosapentaenoic acid – DPA). These associations were mainly driven by the adherence to the vegetables, MUFA/SFA, fish, and dairy products components of the Mediterranean diet.
Conclusion: A high adherence to the Mediterranean diet was associated with human milk showing a lower content of SFA and higher content of MUFA and ω-3 FA, including DHA. The Mediterranean diet may contribute in human milk production with higher content of specific FA which is directly involved in infant’s neural and visual development, as reported by previous studies.
Human milk is a mixture of nutritive and bioactive compounds (e.g., nutrients, hormones, antibodies, immune and stem cells, digestive enzymes, and macrophages) that contribute to the growth and development of the infant (1). Maternal dietary habits may influence the composition of human milk, especially the fatty acids (FA) content (2). In particular, it has been shown that maternal dietary habits modify the content of polyunsaturated FA (PUFA) in human milk and, to a lesser extent, the content of saturated FA (SFA) and monounsaturated FA (MUFA) (3).
Many studies investigated the relationship between maternal nutrition and the composition of human milk according to the intake of single foods or nutrients (4), while a few studies evaluated the role of a posteriori dietary patterns (5–8). In particular, only one study from China (7) and one of our previous analyses (5) investigated the adherence of breastfeeding mothers to a posteriori dietary patterns concerning the content of FA in human milk. Two additional studies evaluated the relationship between the adherence of breastfeeding mothers to a posteriori dietary patterns and the composition of their human milk focusing on macronutrients, without taking into account FA (6, 8).
The traditional Mediterranean diet is a plant-oriented dietary pattern characterized by a high intake of minimally processed foods, fresh fruits, bread and other cereals (generally minimally refined), potatoes, legumes, and nuts; a moderate intake of dairy products (mostly cheese and yogurt); a moderate to low intake of fish and poultry; a low intake of red meat; a high intake of olive oil (especially virgin and extra-virgin olive oils) used as the main source of fat; and a moderate intake of wine, consumed with meals (9). Adherence to the Mediterranean diet has been associated with a range of health benefits, including a reduced risk of cardiovascular diseases, diabetes, metabolic syndrome, overweight and obesity, several cancer types, as well as a lower disease-specific and overall mortality (10–13). However, no study has investigated so far the association between maternal adherence to the Mediterranean diet, measured by one of the proposed scores, and the content of FA in human milk.
The Italian MEDIDIET study aims to evaluate the relationship between the habitual diet of breastfeeding mothers and the nutritional composition, as well as oxidative/anti-oxidative properties of their milk (14). The role of the Mediterranean diet in influencing human milk composition is at the core of the MEDIDIET study. Thus, we present here the FA human milk profile of breastfeeding mothers participating in the MEDIDIET study according to their adherence to the traditional Mediterranean diet.
Between 2012 and 2014, the MEDIDIET study was carried out in five Italian maternity wards (i.e., Turin, Florence, Rome, San Giovanni Rotondo – SGR, and Palermo) enrolling 300 healthy breastfeeding mothers. Information on study design, inclusion criteria, maternal diet assessment, human milk collection, and analysis of human milk samples has been provided in detail elsewhere (14). Briefly, mothers were 25–41 years old and gave birth to healthy term infants. In particular, inclusion criteria for mothers were
• not chronically diseased (i.e., free of diabetes, autoimmune diseases, cardiovascular disease, renal disease, and hypertension);
• seronegative for hepatitis B, hepatitis C, and human immunodeficiency viruses;
• non-smokers during pregnancy and lactation;
• non-abusers of drugs or alcohol;
• non-severely obese (i.e., BMI < 35 kg/m2);
• not on a restricted diet.
Inclusion criteria for infants were:
• born at ≥37 gestational weeks;
• weight range of 2,500–4,500 g;
• body length range of 46–56 cm;
• exclusively breastfed from birth to the day of human milk collection (i.e., 6 ± 1 week postpartum).
All mothers signed an informed consent form to participate in the study. The Ethics Committee of participating hospitals approved the study (protocol number: 31060 MD) as per the ethical standards of the Declaration of Helsinki.
On the day of human milk collection (i.e., 6 ± 1 weeks postpartum), mothers provided a sample of their foremilk (30–50 ml) expressed in the morning after breakfast and before lunch, using a breast pump. The time elapsed since the end of the previous breastfeeding session ranged from 1 to 3 h. The freshly expressed human milk was stirred and divided in sterile 10 ml tubes, overlaid with nitrogen gas to avoid oxidation, and then stored at −70°. Human milk analyses included macronutrient composition (i.e., protein, lactose, fat, and energy density), oxidative parameters, and complete FA profile as reported in Moro et al. (14). Briefly, FAs with a chain length between 4 and 24 carbon atoms of total lipids of human milk samples were analyzed as methyl esters by capillary gas chromatography with flame ionization detection (“GC-FID”) according to the method proposed by Beermann et al. (15). In addition, the lipid content was analyzed using the method outlined by Lucas et al. (16) and Jones et al. (17). In particular, the FA analyzed included SFA, MUFA, trans-FA (TFA), branched-chain FA (BFA), and PUFA. Peak identification of SFA, MUFA, TFA, and both ω-3 and ω-6 FA methyl esters were verified and calibrated by comparison with authentic standards (NuChek Prep; Elysian, MN, United States: GLC-463, GLC-473, GLC-642, GLC-643, GLC-674, and Sigma-Aldrich Ltd., St. Louis, MO, United States: Supelco PUFA3). The standard mix of BFA methyl esters was originally analyzed by Danone Nutricia Research, Utrecht, the Netherlands. Lastly, FA concentrations were recorded as% of fats.
A validated and reproducible food frequency questionnaire (FFQ) (18–20) was administered by trained interviewers to investigate the habitual diet of mothers (from partum to the day of human milk collection). The FFQ included 7 sections to collect information on the weekly intake of 78 food items, recipes, and beverages as follows: (1) milk, hot beverages, and sweeteners; (2) typical Italian first courses (e.g., pasta, risotto, gnocchi, lasagne); bread, and cereals; (3) second courses (including meat, fish, and cheese); (4) side dishes (e.g., vegetables); (5) fruits; (6) sweets, desserts, and soft drinks; and (7) alcoholic beverages. The serving size was defined in “natural” units (e.g., 1 cup of milk, 1 coffee spoon of sugar, 1 egg, 1 apple) or as smaller, on average, or larger than a standard Italian serving (e.g., 80 g of pasta, 100 g of mixed salad, 175 g of potatoes, and 150 g of beef). Occasional intakes (i.e., less than once a week, but greater than once per month) were coded as 0.5 servings per week. Dietary data collected using the FFQ were used to estimate maternal intake of energy and nutrients using an Italian food composition database (21). In this computation, we weighted the fat composition of each food or recipe according to information on the type of fat used for cooking or as dressing.
To evaluate the adherence of the maternal diet to the Mediterranean one, we used an a priori score (i.e., Mediterranean Diet Score – MDS) developed by Trichopoulou et al. (22, 23). According to the proposed methodology, the MDS includes 9 dietary components: (1) vegetables; (2) fruit; (3) cereals (including bread and potatoes); (4) legumes; (5) MUFA to SFA ratio (MUFA/SFA) as a proxy of olive oil consumption (23); (6) fish; (7) dairy products (including milk); (8) meat (including poultry, red and processed meat); (9) and alcohol. Each of the 9 components is assigned a score of 0 or 1 using fixed or median intakes as cutoffs according to the component considered. In particular, for components more frequently consumed in the Mediterranean diet (i.e., vegetables, fruit, cereals, legumes, fish, and MUFA/SFA), a score of 1 is given if the individual intake is greater or equal to the median, and 0 if the individual intake is lower than the median; for components less frequently consumed (i.e., dairy products and meat), a score of 1 is given if the individual intake is lower than the median, and 0 if the individual intake is greater or equal to the median. For alcohol component, a score of 1 is given for an individual consumption ranging from 5 to less than 25 g of ethanol/day, and 0 if the individual consumption is outside this range. The MDS is obtained by adding up the 9 component scores, and therefore, it potentially ranges from 0 (no adherence) to 9 (complete adherence) points.
The FA content was not available for 18 human milk samples due to insufficient milk volume, thus leaving 282 samples for the present analysis. We categorized the MDS in approximate tertiles: 0–3 points (n = 97; 34.4%) for a low adherence, 4 points (n = 74; 26.4%) for a medium adherence, and 5–8 points (n = 111; 39.4%) for a high adherence to the Mediterranean diet. None of the mothers obtained the theoretical highest score (i.e., MDS = 9) mainly due to the common Italian behavior of excluding or substantially reducing alcohol from the diet during the lactation period (24). We compared the mean content of FA in human milk according to categories of MDS using ANOVA adjusting for the ratio between the maternal energy intake and maternal pre-pregnancy weight (kcal/day/kg). In addition, we used the test for trend to evaluate the linear relationship of the mean contents of FA in human milk across categories of MDS. All analyses were conducted using R version 4.0.5.
Table 1 reports the demographic characteristics, pre-pregnancy BMI, and energy intake of the 282 breastfeeding mothers. Mothers had a mean age of 33 ± 4 years, a mean pre-pregnancy BMI of 22.3 ± 3.2 kg/m2, and a mean energy intake of 1947 ± 443 kcal/day.
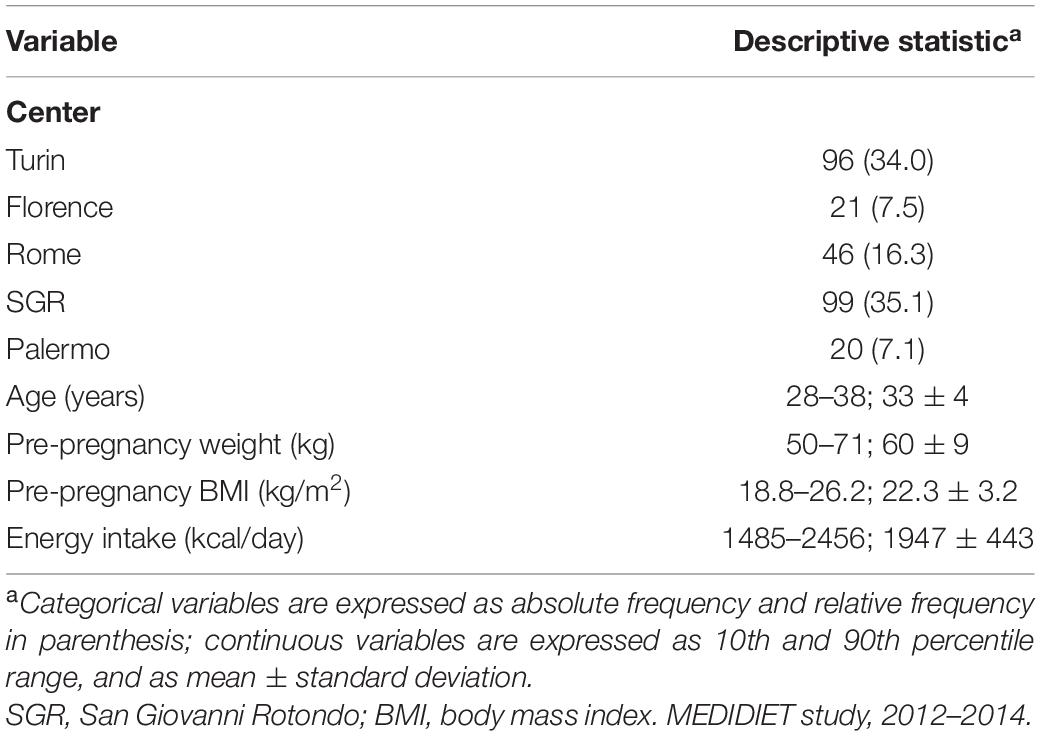
Table 1. Distribution of 282 Italian breastfeeding mothers according to center, age, pre-pregnancy weight and BMI, and energy intake.
The distributions of MDS components (10th, 25th, 50th, 75th, and 90th percentile and mean ± standard deviation) are reported in Table 2. Overall, the median intakes (servings/week) of components more frequently consumed in the Mediterranean diet were 11.0 for vegetables, 15.0 for fruit, 22.0 for cereals, 1.0 for legumes, and 2.0 for fish; the median intake of the MUFA/SFA component was 1.24. The median intakes (servings/week) of components less frequently consumed in the Mediterranean diet were 11.0 for dairy products, and 8.0 for meat; the median intake for the alcohol component was 0.0 g ethanol/day.
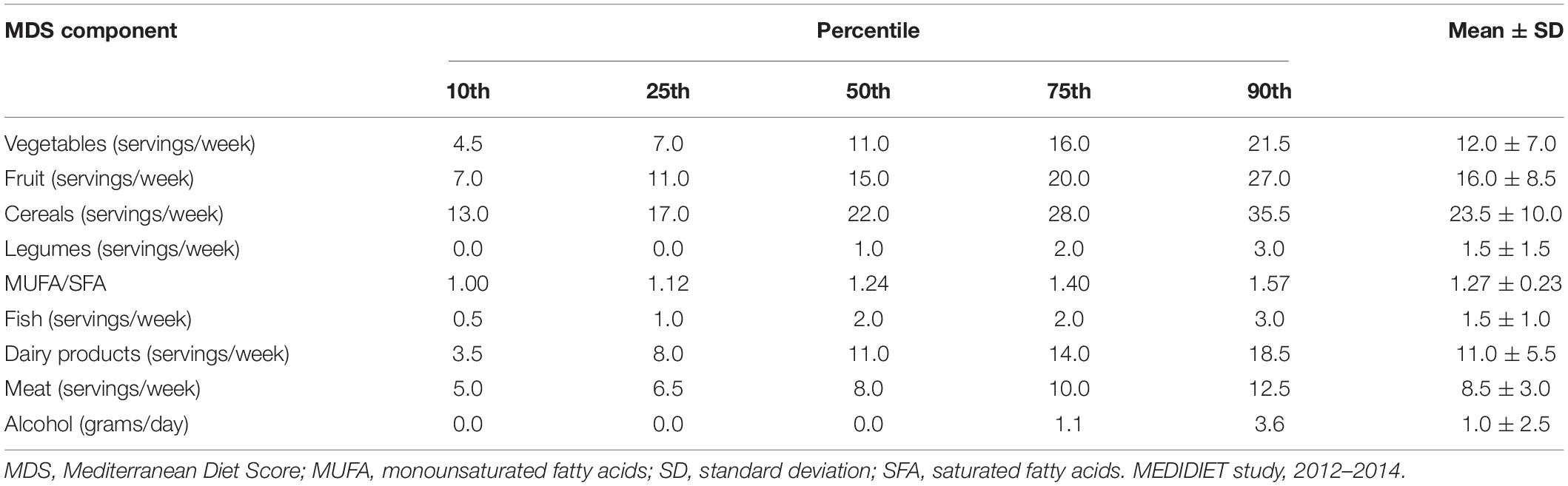
Table 2. Distribution of components of the Mediterranean Diet Score.
High adherence to the Mediterranean diet was associated with a significantly lower content of SFA in human milk (p ANOVA = 0.02 and p for trend = 0.02; Table 3). In particular, the mean contents of SFA were 42.58 ± 4.36% of fats for mothers with low adherence to the Mediterranean diet (MDS = 0–3 points), 42.58 ± 4.89% of fats for mothers with medium adherence (MDS = 4 points), and 40.92 ± 5.22% of fats for mothers with high adherence (MDS = 5–8 points). Considering the major types of SFA, a high adherence of breastfeeding mothers to the Mediterranean diet was associated with a significantly lower content of palmitic acid (PA) and stearic acid (SA).
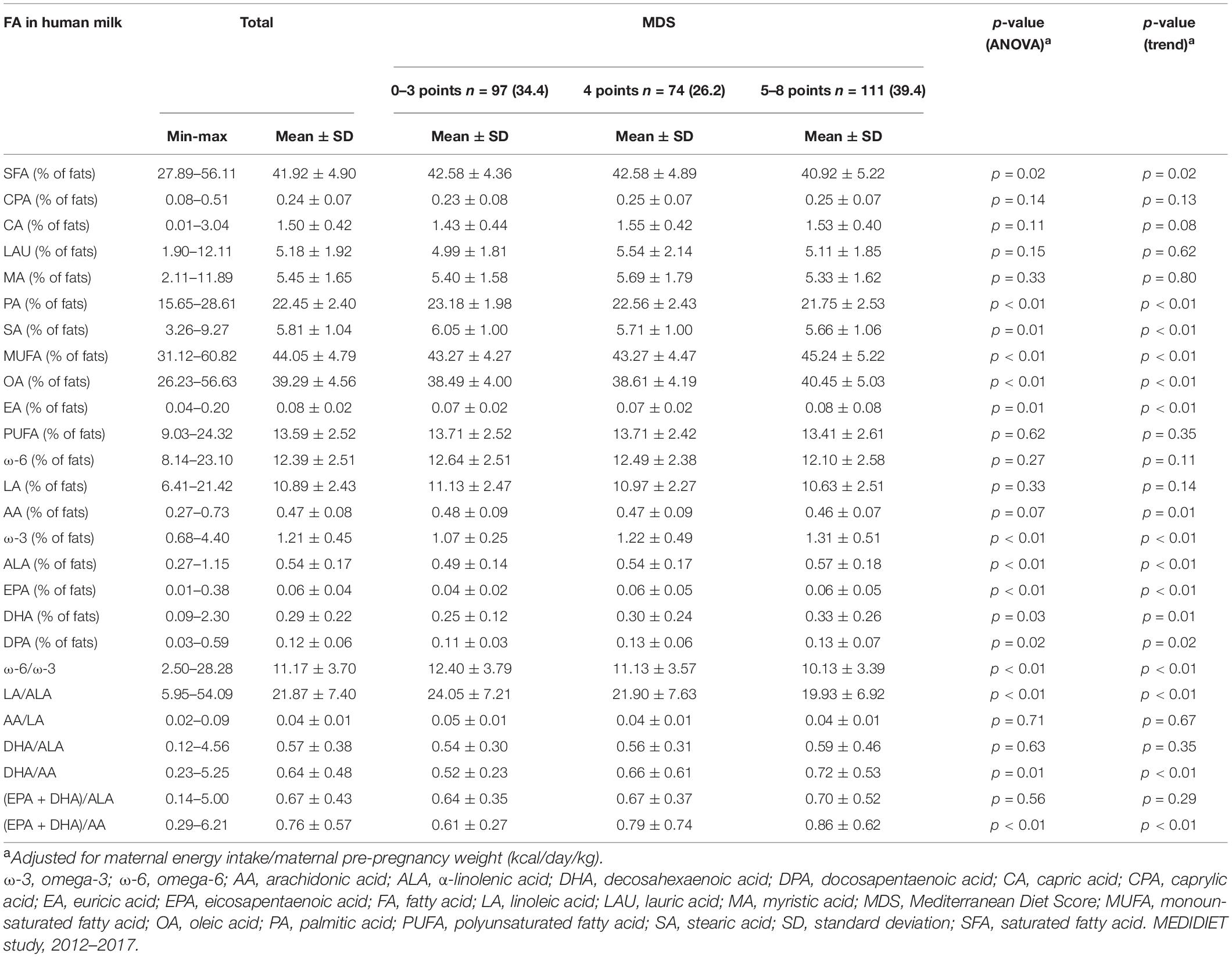
Table 3. Mean and standard deviation contents of selected fatty acids (expressed as% of fats) in human milk according to the adherence of breastfeeding mothers to the Mediterranean Diet Score (expressed approximately in tertiles).
Conversely, high adherence to the Mediterranean diet was associated with a significantly higher content of MUFA in human milk (43.27 ± 4.27% of fats for MDS = 0–3 points; 43.27 ± 4.47% of fats for MDS = 4 points; 45.24 ± 5.22% of fats for MDS = 5–8 points; p ANOVA and p for trend < 0.01). Both the oleic acid (OA) and the erucic acid (EA), the major types of MUFA, significantly increased according to the adherence to the Mediterranean diet.
The content of PUFA in human milk was not associated with the adherence to the Mediterranean diet (p ANOVA = 0.62 and p for trend = 0.35). However, considering the major types of PUFA, a significantly lower content of arachidonic acid (AA) in human milk was observed among mothers with high adherence to the Mediterranean diet (0.48 ± 0.09% of fats for MDS = 0–3 points; 0.47 ± 0.09% of fats for MDS = 4 points; 0.46 ± 0.07% of fats for MDS = 5–8 points; p for trend = 0.01). Conversely, a significantly higher content of ω-3 FA in human milk was observed among mothers highly adherent to the Mediterranean diet (1.07 ± 0.25% of fats for MDS = 0–3 points, 1.22 ± 0.49% of fats for MDS = 4 points, and 1.31 ± 0.51% of fats for MDS = 5–8 points; p ANOVA and p for trend < 0.01). Likewise, significantly higher content of the major types of ω-3 FA in human milk (i.e., α-linolenic acid – ALA, eicosapentaenoic acid – EPA, docosahexaenoic acid – DHA, docosapentaenoic acid – DPA) was observed among mothers with high adherence to the Mediterranean diet. In addition, high adherence to the Mediterranean diet was associated with a significantly lower ratio between ω-6 and ω-3 FA (p ANOVA and p for trend < 0.01) and the ratio between LA and ALA (p ANOVA and p for trend < 0.01) in human milk. Conversely, high adherence to the Mediterranean diet was associated with a higher DHA/AA (p ANOVA = 0.01; p for trend < 0.01) and (EPA + DHA)/AA (p ANOVA and p for trend < 0.01) in human milk. No clear association was observed for the others FA considered.
Table 4 reports the content of SFA in human milk according to the adherence of breastfeeding mothers to each component of MDS. For components more frequently consumed in the Mediterranean diet, one point (i.e., adherence) corresponded to an individual intake greater or equal to the median intake of vegetables, fruit, cereals, legumes, MUFA/SFA, and fish, respectively; for components less frequently consumed in the Mediterranean diet, one point corresponded to an individual intake less than the median intake of dairy products and meat, respectively; for alcohol component, one point corresponded to an individual alcohol intake ranging from 5 to less than 25 g of ethanol/day. Mothers who adhered to the vegetable component showed human milk with a significantly lower content of SFA (41.16 ± 5.29% of fats) than the human milk of non-adherent mothers (42.64 ± 4.41% of fats; p = 0.01). Likewise, mothers who were adherent to MUFA/SFA (41.07 ± 5.15 vs. 42.74 ± 4.52% of fats; p < 0.01) and dairy products (41.24 ± 4.71 vs. 42.58 ± 5.01; p = 0.02) components showed lower content of SFA in human milk. A similar pattern was observed for PA and SA.
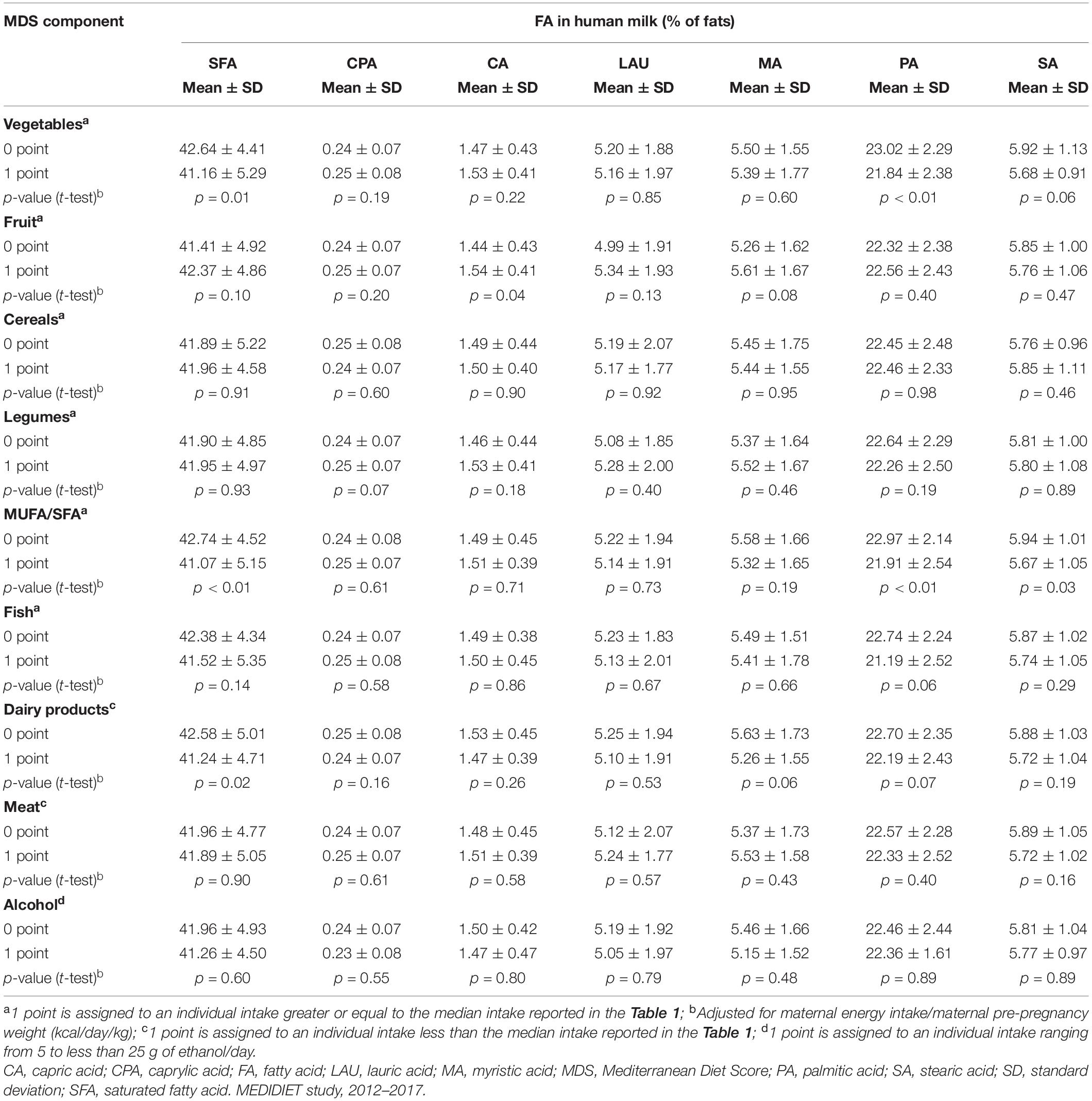
Table 4. Mean and standard deviation contents of major saturated fatty acids in human milk (expressed as% of fats) according to the adherence of breastfeeding mothers to single components of the Mediterranean Diet Score.
Table 5 reports the content of MUFA in human milk according to the adherence of breastfeeding mothers to each component of MDS. A significantly higher content of MUFA was observed for mothers who adhered to the vegetables (44.73 ± 5.34 vs. 43.41 ± 4.14% of fats; p = 0.02), MUFA/SFA (44.90 ± 5.03 vs. 43.23 ± 4.42% of fats; p < 0.01), and dairy products (44.87 ± 4.47 vs. 43.26 ± 4.97% of fats; p < 0.01) components. The adherence of such components resulted in human milk with higher contents of OA and EA.
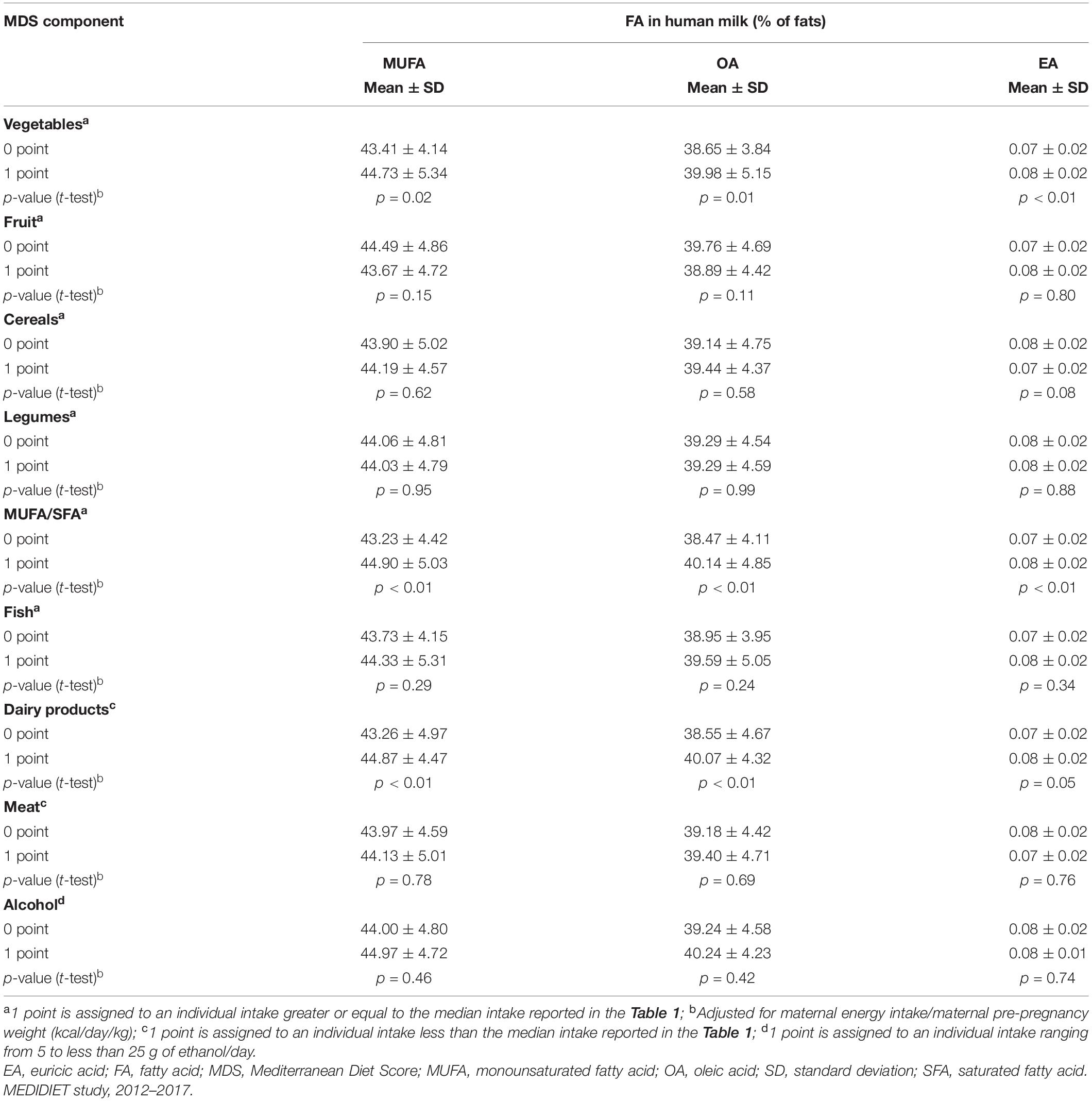
Table 5. Mean and standard deviation contents of major monounsaturated fatty acids in human milk (expressed as% of fats) according to the adherence of breastfeeding mothers to single components of the Mediterranean Diet Score.
Table 6 reports the content of PUFA in human milk according to the adherence of breastfeeding mothers to each component of MDS. A significantly higher content of ω-3 FA was observed for mothers who adhered to the vegetables (1.30 ± 0.48 vs. 1.12 ± 0.39% of fats p < 0.01), MUFA/SFA (1.30 ± 0.56 vs 1.12 ± 0.27; p < 0.01), and fish (1.29 ± 0.50 vs. 1.12 ± 0.36; p < 0.01). Similarly, the adherence of breastfeeding mothers to vegetables, MUFA/SFA, and fish components was significantly associated with human milk with higher contents of ALA, EPA, DHA, and DPA.
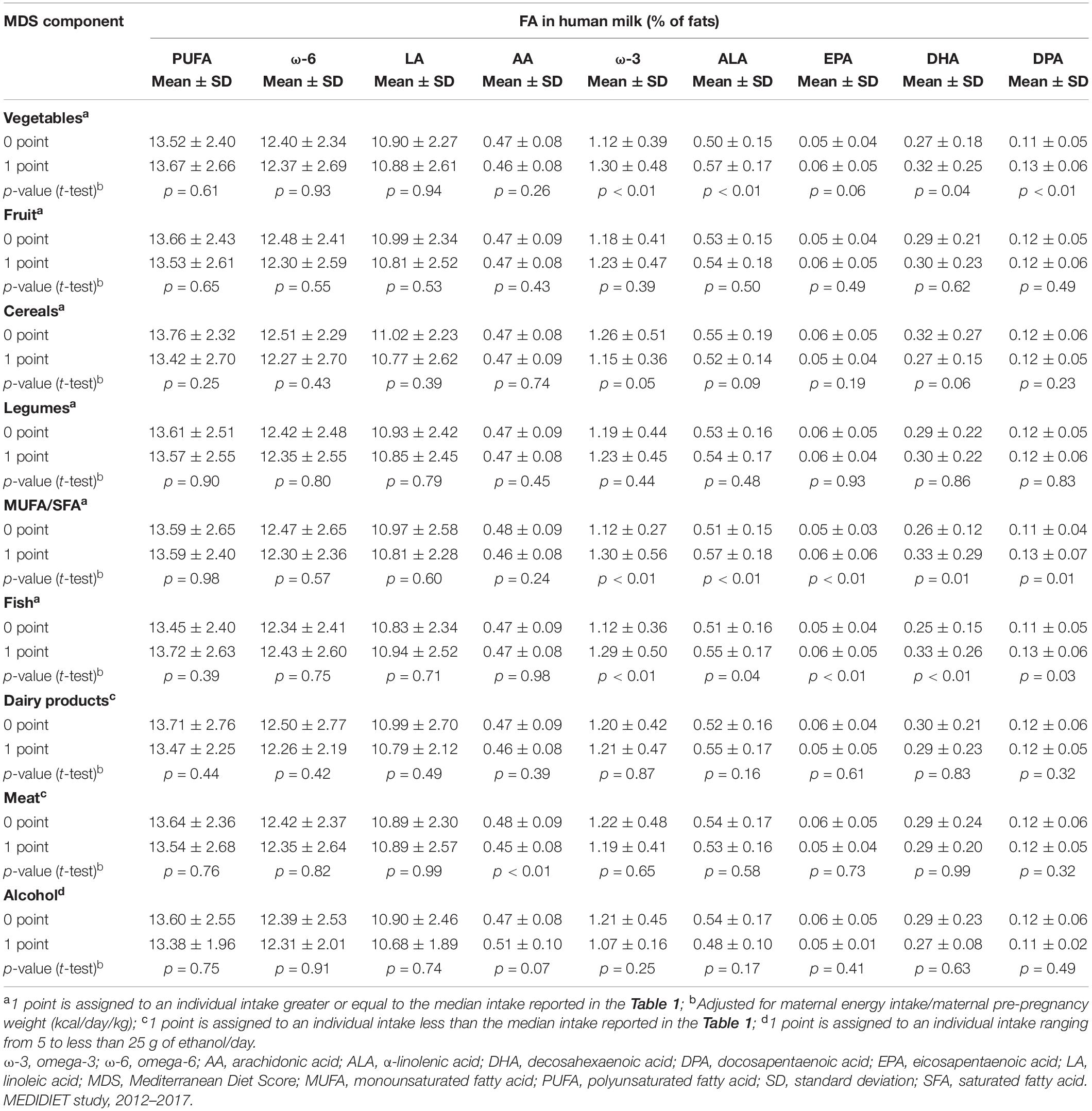
Table 6. Mean and standard deviation contents of major polyunsaturated fatty acids in human milk (expressed as% of fats) according to the adherence of breastfeeding mothers to single components of the Mediterranean Diet Score.
We assessed the association between the adherence of breastfeeding mothers to the Mediterranean diet and the FA content of their human milk using data from the Italian MEDIDIET study. High adherence to the Mediterranean diet was associated with lower content of SFA (including PA and SA), ω-6/ω-3, and LA/ALA, and higher content of MUFA (including OA and EA), ω-3 FA (including ALA, EPA, DHA, and DPA), and DHA/AA and (EPA + DHA)/AA) in human milk. These associations were mainly driven by the adherence to the vegetables, MUFA/SFA, fish, and dairy products components of the Mediterranean diet.
Previous studies investigated the relationship between maternal intakes of single foods or nutrients and the FA composition in human milk. A longitudinal Finnish study (25) reported a weak positive correlation (r = 0.21) between maternal intake of high-fat dairy products and the content of SFA in human milk, collected at 3 months of lactation. Likewise, we observed a lower content of SFA in human milk for mothers with high adherence to the Mediterranean diet, which is characterized by a moderate to low consumption of dairy products. Accordingly, two studies (26, 27) found positive correlations between maternal intake of SFA and the content of SFA in human milk (r = 0.60 and r = 0.215, respectively). The lower content of SFA in human milk observed among mothers with high adherence to the Mediterranean diet could not provide optimal food for the infant’s needs (2, 28–31). However, the mean content of SFA in human milk among mothers who highly adhered to the Mediterranean diet (40.92 ± 5.22% of fats) was in agreement with the typical human milk composition of FA, which contains approximately 35–45% of SFA, 45–50% of MUFA, and 15% of PUFA (32, 33).
The Italian cross-sectional study by Scopesi et al. (26) reported a positive correlation of 0.63 between maternal intake of MUFA and the content of MUFA in human milk (collected during the 1st month of lactation) which is in agreement with the higher content of MUFA in human milk observed in this study for mothers who were adherent to the Mediterranean diet. The higher content of MUFA in human milk for these mothers likely derives from the consumption of olive oil, the major fat source of the Mediterranean diet, which is rich in MUFA, especially in the form of OA (34).
A cross-sectional study conducted in Denmark (35) reported a higher content of ω-3 FA (including EPA, DHA, and DPA) in human milk (collected at 4 months postpartum) for mothers who had a high intake of fish, as compared to mothers who did not consume it. A longitudinal Greek study (36) reported positive correlations between maternal PUFA intake and the contents of ω-3 FA (r = 0.26) and DHA (r = 0.27) in human milk, collected in the 1st month of lactation. Likewise, the cross-sectional study of Kim et al. (27) reported a weak positive correlation (r = 0.211) between maternal intake of PUFA and the content of ω-3 FA in human milk (collected from 1 to 11 months postpartum) for South Korean mothers. The cross-sectional study by Olafsdottir et al. (37) reported a positive correlation of 0.43 between maternal PUFA intake and the content of ALA in human milk (collected from 2 to 4 months postpartum) for Icelandic mothers. We observed a higher content of ω-3 FA and the major types of ω-3 FA in human milk for mothers with high adherence to the Mediterranean diet. The moderate consumption of fish jointly with the high consumption of vegetables (various of them are relatively rich in ω-3 FA) results in an appreciable intake of ω-3 FA for populations belonging to the Mediterranean area (34).
Three Chinese studies assessed the association between a posteriori dietary patterns of breastfeeding mothers and the composition of human milk (6–8). Dietary patterns were derived through principal component analysis based on food group intakes of mothers. Among the dietary patterns identified in the cross-sectional study by Hu et al. (6), the “high-in-plant-foods” dietary pattern was negatively associated with total fats content in human milk, collected within 2 months postpartum. We observed a lower content of SFA, a higher content of MUFA, and a stationary content of PUFA in human milk for high adherence to the Mediterranean diet. In the cross-sectional study by Tian et al. (7), the dietary pattern characterized by “dairy and soybean products, and nuts” showed higher content of SFA in human milk; the dietary pattern characterized by “meats, mushrooms and algae, and marine products” and the dietary pattern characterized by “vegetables and fruit” showed higher content of PUFA and ω-6 FA in human milk (collected from 22 days to 6 months postpartum). In our study, neither the adherence to the Mediterranean diet nor the adherence to vegetables, fruit, and fish components was associated with the contents of PUFA and ω-6 FA in human milk. No dietary pattern identified in the cross-sectional study of Huang et al. was associated with the FA profile in human milk, collected in the postpartum period from 7 days to 6 months and beyond (8). In our previous analysis of the same data, we identified five a posteriori dietary patterns based on nutrient intakes of breastfeeding mothers (5). The nutritional profile of three out of five dietary patterns, named “Proteins and FA with legs,” “FA with fins,” and “FA with leaves,” was consistent with the Mediterranean diet and therefore they showed similar associations with the FA content in human milk. In particular, the “Proteins and FA with legs” dietary pattern, characterized by high maternal intake of animal proteins (including dairy products), was weakly positively correlated (r = 0.12) with the content of SFA and weakly negatively correlated (r = −0.20) with the content of MUFA in human milk. The “FA with fins” dietary pattern, characterized by high maternal intake of fish, was weakly positively correlated (r = 0.23) with the content of ω-3 FA (including ALA, EPA, DHA, and DPA) in human milk. The “FA with leaves,” dietary pattern characterized by a high intake of vegetables, was weakly positively correlated (r = 0.17) with the content of MUFA and weakly negatively correlated (r = −0.19) with the content of SFA in human milk.
The FA in human milk derives from the endogenous synthesis in the mammary gland and uptake from maternal plasma. In both cases, the content of FA in human milk may be influenced by maternal nutrition (2, 38, 39). Furthermore, the role of FA in the infant diet is gaining interest because FA is involved in several growth processes, especially in visual and neural functions (28, 40). In particular, DHA is selectively enriched in a few specific membrane lipids, which include the glycerophospholipids of the retina and brain gray matter (29). High concentrations of DHA are present in phosphatidylserine and the ethanolamine phosphoacylglycerols of gray matter and the outer segments of rod and cone photoreceptors in the retina (41). Considerable evidence showed that poor maternal DHA status increased the risk of inadequate transferring of DHA in human milk and consequently a delayed or reduced neural and visual system development of the infant (30, 42–44).
We observed some maternal dietary behaviors diverging from the typical Mediterranean diet such as an overall low intake of legumes, an overall quite high intake of dairy products and meat, and a low intake of vegetables for mothers from Southern Italy (Supplementary Table 1). This could be partially explained by the results of a recent internet survey describing the nutritional behavior of the Italian population and their compliance with the Mediterranean pyramid recommendations. The authors reported “a rather low adherence” of participants to some Mediterranean pyramid recommendations, especially by females and in the South (45). In addition, we observed that the human milk of mothers in the South had a lower content of ω-6 and ALA (Supplementary Table 2), likely due to these changing dietary habits. Nevertheless, we generally did not find other modified associations between the adherence to the Mediterranean diet and the content of FA in human milk across the strata of geographical area (Supplementary Table 2).
Some studies showed differences in the FA profile of human milk according to maternal pre-pregnancy weight and/or BMI (46, 47). However, no difference emerged in the distributions of maternal pre-pregnancy weight and BMI according to the adherence to the MDS, excluding possible confounding effects of these variables (Supplementary Table 3). Nevertheless, mothers highly adherent to the Mediterranean diet tended to be older than those with low or medium adherence, not excluding a possible residual confounding due to age (Supplementary Table 3). In addition, the cross-sectional design of this study did not allow to establish a causal relationship between the Mediterranean diet and the content of FA in human milk. Nevertheless, it is unlikely that differences in the contents of FA in human milk could have modified the maternal adherence to the Mediterranean diet. However, it could not be ruled out that the existence of external factors (e.g., socioeconomic status or healthy lifestyles) trigger the adherence to the Mediterranean diet and the composition of human milk in parallel and causatively influence the content of FA. Dietary information of breastfeeding mothers was self-reported and possibly biased from incomplete recall. However, it was collected by trained interviewers using structured FFQ which has been validated (18) and tested for the reproducibility (19, 20) in the Italian adult population, minimizing possible recall bias. Although we used a validated and reproducible FFQ, the maternal nutrient intakes could be underestimated. Nevertheless, we previously compared maternal nutrient intakes of mothers participating in the MEDIDIET study with those of mothers from other developed countries in a reviewing framework. The energy intake of mothers participating in the MEDIDIET study was lower than the average energy requirement (i.e., 2,300 kcal/day) recommended during the lactation period, but it was in agreement with those of the majority of studies included in the review (48).
Possible systematic and random errors in the assessment of the content of FA in human milk were reduced by a standard protocol for the collection and analysis of human milk samples. In addition, we collected all human milk samples in a short window of time (i.e., 6 ± 1 weeks postpartum) and in the morning for all mothers participating in the MEDIDIET study, avoiding the variability due to different lactation stages or different times of the day. However, we did not collect human milk samples repeatedly over time making it difficult to make conclusions on the impact of maternal diet on the composition of human milk in a comprehensive way.
Another limitation of this study is the lack of information on follow-up of the infant growth. Thus, we can establish the relationship between maternal nutrition and human milk composition and only infer the relationship between human milk properties and infant outcomes using results from external studies.
The multicentric design of the MEDIDIET study allowed us to include mothers from different Italian regions strengthening the findings of this study. The inclusion of healthy breastfeeding mothers with healthy infants allowed transferring of these results to the general population. In addition, another strength includes the detailed set of FA in human milk provided in this analysis. Lastly, to the best of our knowledge, this is the first study aimed to evaluate the relationship between the Mediterranean diet and the content of FA in human milk using a formal score of adherence.
High adherence to the Mediterranean diet was associated with human milk with lower content of SFA and higher contents of MUFA, ω-3 FA, and the major types of ω-3 FA, including DHA. The Mediterranean diet may contribute to human milk production with higher content of specific FA which is directly involved in the growth and development of neural and visual functions of the infant, as reported by previous studies. If the results of this study were confirmed by further analyses, possibly including infant outcomes, this would help in the development of dietary guidelines for breastfeeding mothers to promote good dietary practices – such as the Mediterranean diet – and their positive implications for infants.
The original contributions presented in this study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by the Ethics Committee of participating hospitals. The patients/participants provided their written informed consent to participate in this study.
Ansaldi Giulia (Neonatal Care Unit of the University, City of Health and Science Hospital, Turin, Italy);
Amadio Patrizia (Ospedale Pediatrico Bambino Gesù, Rome, Italy);
Chester Elena (Neonatal Care Unit of the University, City of Health and Science Hospital, Turin, Italy);
Di Nicola Paola (Neonatal Care Unit of the University, City of Health and Science Hospital, Turin, Italy);
Monzali Francesca (Azienda Ospedaliera Universitaria Meyer, Florence, Italy);
Palumbo Giuseppina (“Casa Sollievo della Sofferenza” Foundation, San Giovanni Rotondo, Italy);
Roselli Elena (Azienda Ospedaliera Universitaria Meyer, Florence, Italy);
Siemens Louise (Ospedale Buccheri La Ferla, FBF, Palermo, Italy);
Sottemano Stefano (Neonatal Care Unit of the University, City of Health and Science Hospital, Turin, Italy);
Villani Antonio (“Casa Sollievo della Sofferenza” Foundation, San Giovanni Rotondo, Italy).
GM, MF, and AD designed the research idea. FB and MD performed the statistical analyses and wrote the manuscript. MF, FB, MD, CA, SE, EB, GM, and BS interpreted the results. GM directed data acquisition of the MEDIDIET study. PT, PQ, GS, CP, and IK managed data acquisition of the MEDIDIET study. All authors have read and approved the final version of the manuscript.
This study was sponsored by the Danone Nutricia Research, Utrecht, Netherlands. FB was supported by a grant from the Department of Clinical Sciences and Community Health of the University of Milan (PSR2015-1719FBRAV) at the time when data were analyzed. MD was supported by an academic fellowship focusing on maternal nutrition.
The statistical analyses were performed by the Department of Clinical Sciences and Community Health, Branch of Medical Statistics, Biometry and Epidemiology “G.A. Maccacaro”, Università degli Studi di Milano, Milan, Italy (MD, FB, and MF) without the involvement of the Sponsor. SE, EV, and BS were employees of Danone Nutricia Research, Utrecht, Netherlands.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank Eva Szabó and Tamás Marosvölgyi for performing the FA analyses and Maria Parpinel for her help in the assessment of maternal nutrient intakes. In addition, We also thank Frank Wiens who was the former project leader of the MEDIDIET study for Danone Nutricia Research.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2022.891376/full#supplementary-material
2. Innis SM. Impact of maternal diet on human milk composition and neurological development of infants. Am J Clin Nutr. (2014) 99:734S–41S. doi: 10.3945/ajcn.113.072595
3. Pham Q, Patel P, Baban B, Yu J, Bhatia J. Factors affecting the composition of expressed fresh human milk. Breastfeed Med. (2020) 15:551–8. doi: 10.1089/bfm.2020.0195
4. Bravi F, Wiens F, Decarli A, Dal Pont A, Agostoni C, Ferraroni M. Impact of maternal nutrition oh breast-milk composition: a systematic review. Am J Clin Nutr. (2016) 104:646–62. doi: 10.3945/ajcn.115.120881
5. Bravi F, Di Maso M, Eussen S, Agostoni C, Salvatori G, Profeti C, et al. Dietary patterns of breastfeeding mothers and human milk composition: data from the Italian MEDIDIET study. Nutrients. (2021) 13:1722. doi: 10.3390/nu13051722
6. Hu R, Eussen S, Sijtsma FPC, Papi B, Stahl B, Jin Y, et al. Maternal dietary patterns are associated with human milk composition in Chinese lactating women. Nutrition. (2021) 9:111392. doi: 10.1016/j.nut.2021.111392
7. Tian HM, Wu YX, Lin YQ, Chen XY, Yu M, Lu T, et al. Dietary patterns affect maternal macronutrient intake levels and the fatty acid profile of breast milk in lactating Chinese mothers. Nutrition. (2019) 58:83–8. doi: 10.1016/j.nut.2018.06.009
8. Huang Z, Hu YM. Dietary patterns and their association with breast milk macronutrient composition among lactating women. Int Breastfeed J. (2020) 15:52. doi: 10.1186/s13006-020-00293-w
9. Guasch-Ferre M, Willett WC. The Mediterranean diet and health: a comprehensive overview. J Intern Med. (2021) 290:549–66. doi: 10.1111/joim.13333
10. Sanchez-Sanchez ML, Garcia-Vigara A, Hidalgo-Mora JJ, Garcia-Perez MA, Tarin J, Cano A. Mediterranean diet and health: a systematic review of epidemiological studies and intervention trials. Maturitas. (2020) 136:25–37. doi: 10.1016/j.maturitas.2020.03.008
11. Dinu M, Pagliai G, Casini A, Sofi F. Mediterranean diet and multiple health outcomes: an umbrella review of meta-analyses of observational studies and randomised trials. Eur J Clin Nutr. (2018) 72:30–43. doi: 10.1038/ejcn.2017.58
12. Morze J, Danielewicz A, Przybylowicz K, Zeng H, Hoffmann G, Schwingshackl L. An updated systematic review and meta-analysis on adherence to mediterranean diet and risk of cancer. Eur J Nutr. (2021) 60:1561–86. doi: 10.1007/s00394-020-02346-6
13. Serra-Majem L, Roman-Vinas B, Sanchez-Villegas A, Guasch-Ferre M, Corella D, La Vecchia C. Benefits of the Mediterranean diet: Epidemiological and molecular aspects. Mol Aspects Med. (2019) 67:1–55. doi: 10.1016/j.mam.2019.06.001
14. Moro GE, Bertino E, Bravi F, Tonetto P, Gatta A, Quitadamo PA, et al. Adherence to the traditional mediterranean diet and human milk composition: rationale, design, and subject characteristics of the MEDIDIET study. Front Pediatr. (2019) 7:66. doi: 10.3389/fped.2019.00066
15. Beermann C, Green A, Mobius M, Schmitt JJ, Boehm G. Lipid class separation by HPLC combined with GC FA analysis: comparison of seed lipid compositions from different Brassica napus L. varieties. J Am Oil Chem Soc. (2003) 80:747–53. doi: 10.1007/s11746-003-0767-0
16. Lucas A, Gibbs JA, Lyster RL, Baum JD. Creamatocrit: simple clinical technique for estimating fat concentration and energy value of human milk. Br Med J. (1978) 1:1018–20. doi: 10.1136/bmj.1.6119.1018
17. Jones E, Dimmock PW, Spencer SA. A randomised controlled trial to compare methods of milk expression after preterm delivery. Arch Dis Child Fetal Neonatal Ed. (2001) 85:F91–5. doi: 10.1136/fn.85.2.f91
18. Decarli A, Franceschi S, Ferraroni M, Gnagnarella P, Parpinel MT, La Vecchia C, et al. Validation of a food-frequency questionnaire to assess dietary intakes in cancer studies in Italy. Results for specific nutrients. Ann Epidemiol. (1996) 6:110–8. doi: 10.1016/1047-2797(95)00129-8
19. Franceschi S, Negri E, Salvini S, Decarli A, Ferraroni M, Filiberti R, et al. Reproducibility of an Italian food frequency questionnaire for cancer studies: results for specific food items. Eur J Cancer. (1993) 29A:2298–305. doi: 10.1016/0959-8049(93)90225-5
20. Franceschi S, Barbone F, Negri E, Decarli A, Ferraroni M, Filiberti R, et al. Reproducibility of an Italian food frequency questionnaire for cancer studies. Results for specific nutrients. Ann Epidemiol. (1995) 5:69–75. doi: 10.1016/1047-2797(95)92893-d
21. Gnagnarella P, Parpinel M, Salvini S, Franceschi S, Palli D, Boyle P. The update of the Italian food composition database. J Food Compos Anal. (2004) 17:509–22. doi: 10.1016/j.jfca.2004.02.009
22. Trichopoulou A, Costacou T, Bamia C, Trichopoulos D. Adherence to a Mediterranean diet and survival in a Greek population. N Engl J Med. (2003) 348:2599–608. doi: 10.1056/nejmoa025039
23. Trichopoulou A, Kouris-Blazos A, Wahlqvist ML, Gnardellis C, Lagiou P, Polychronopoulos E, et al. Diet and overall survival in elderly people. BMJ. (1995) 311:1457–60. doi: 10.1136/bmj.311.7018.1457
24. Quarchioni E, Possenti V, Ferrante G, Masocco M, Minardi V, Salmaso S, et al. [Tobacco smoking and alcohol intake in pregnant and breastfeeding women: preliminary data of the survey PASSI 2014]. Epidemiol Prev. (2016) 40:76. doi: 10.19191/EP16.1.P076.019
25. Makela J, Linderborg K, Niinikoski H, Yang B, Lagstrom H. Breast milk fatty acid composition differs between overweight and normal weight women: the STEPS Study. Eur J Nutr. (2013) 52:727–35. doi: 10.1007/s00394-012-0378-5
26. Scopesi F, Ciangherotti S, Lantieri PB, Risso D, Bertini I, Campone F, et al. Maternal dietary PUFAs intake and human milk content relationships during the first month of lactation. Clin Nutr. (2001) 20:393–7. doi: 10.1054/clnu.2001.0464
27. Kim H, Kang S, Jung BM, Yi H, Jung JA, Chang N. Breast milk fatty acid composition and fatty acid intake of lactating mothers in South Korea. Br J Nutr. (2017) 117:556–61. doi: 10.1017/S0007114517000253
28. Innis SM. Dietary (n-3) fatty acids and brain development. J Nutr. (2007) 137:855–9. doi: 10.1093/jn/137.4.855
29. Innis SM. Human milk: maternal dietary lipids and infant development. Proc Nutr Soc. (2007) 66:397–404. doi: 10.1017/S0029665107005666
30. Innis SM. Fatty acids and early human development. Early Hum Dev. (2007) 83:761–6. doi: 10.1016/j.earlhumdev.2007.09.004
31. Schipper L, van Dijk G, van der Beek EM. Milk lipid composition and structure; The relevance for infant brain development. Ocl Oils Fat Crop Li. (2020) 27:5. doi: 10.1051/ocl/2020001
32. Delplanque B, Gibson R, Koletzko B, Lapillonne A, Strandvik B. Lipid quality in infant nutrition: current knowledge and future opportunities. J Pediatr Gastroenterol Nutr. (2015) 61:8–17. doi: 10.1097/MPG.0000000000000818
34. Galli C, Marangoni F. N-3 fatty acids in the Mediterranean diet. Prostag Leukotr Ess. (2006) 75:129–33. doi: 10.1016/j.plefa.2006.05.007
35. Lauritzen L, Jorgensen MH, Hansen HS, Michaelsen KF. Fluctuations in human milk long-chain PUFA levels in relation to dietary fish intake. Lipids. (2002) 37:237–44. doi: 10.1007/s11745-002-0886-2
36. Antonakou A, Skenderi KP, Chiou A, Anastasiou CA, Bakoula C, Matalas AL. Breast milk fat concentration and fatty acid pattern during the first six months in exclusively breastfeeding Greek women. Eur J Nutr. (2013) 52:963–73. doi: 10.1007/s00394-012-0403-8
37. Olafsdottir AS, Thorsdottir I, Wagner KH, Elmadfa I. Polyunsaturated fatty acids in the diet and breast milk of lactating icelandic women with traditional fish and cod liver oil consumption. Ann Nutr Metab. (2006) 50:270–6. doi: 10.1159/000091685
38. Brenna JT, Varamini B, Jensen RG, Diersen-Schade DA, Boettcher JA, Arterburn LM. Docosahexaenoic and arachidonic acid concentrations in human breast milk worldwide. Am J Clin Nutr. (2007) 85:1457–64. doi: 10.1093/ajcn/85.6.1457
39. Jensen RG, Lammi-Keefe CJ, Henderson RA, Bush VJ, Ferris AM. Effect of dietary intake of n-6 and n-3 fatty acids on the fatty acid composition of human milk in North America. J Pediatr. (1992) 120(4 Pt 2):S87–92. doi: 10.1016/s0022-3476(05)81241-7
40. Jeffrey BG, Weisinger HS, Neuringer M, Mitchell DC. The role of docosahexaenoic acid in retinal function. Lipids. (2001) 36:859–71. doi: 10.1007/s11745-001-0796-3
41. Innis SM. Perinatal biochemistry and physiology of long-chain polyunsaturated fatty acids. J Pediatr. (2003) 143(Suppl. 4):S1–8. doi: 10.1067/s0022-3476(03)00396-2
42. Innis SM. Trans fatty intakes during pregnancy, infancy and early childhood. Atheroscler Suppl. (2006) 7:17–20. doi: 10.1016/j.atherosclerosissup.2006.04.005
43. Innis SM. Polyunsaturated fatty acids in human milk: an essential role in infant development. Adv Exp Med Biol. (2004) 554:27–43. doi: 10.1007/978-1-4757-4242-8_5
45. Bracale R, Vaccaro CM, Coletta V, Cricelli C, Gamaleri FC, Parazzini F, et al. Nutrition behaviour and compliance with the Mediterranean diet pyramid recommendations: an Italian survey-based study. Eat Weight Disord. (2020) 25:1789–98. doi: 10.1007/s40519-019-00807-4
46. Sims CR, Lipsmeyer ME, Turner DE, Andres A. Human milk composition differs by maternal BMI in the first 9 months postpartum. Am J Clin Nutr. (2020) 112:548–57. doi: 10.1093/ajcn/nqaa098
47. Ellsworth L, Perng W, Harman E, Das A, Pennathur S, Gregg B. Impact of maternal overweight and obesity on milk composition and infant growth. Matern Child Nutr. (2020) 16:e12979. doi: 10.1111/mcn.12979
Keywords: maternal nutrition, Mediterranean diet, breastfeeding, lipids, fatty acids profile
Citation: Di Maso M, Bravi F, Ferraroni M, Agostoni C, Eussen SRBM, Decsi T, Quitadamo PA, Tonetto P, Peila C, Profeti C, Salvatori G, Kazmierska I, Decarli A, Vacca E, Bertino E, Stahl B and Moro GE (2022) Adherence to Mediterranean Diet of Breastfeeding Mothers and Fatty Acids Composition of Their Human Milk: Results From the Italian MEDIDIET Study. Front. Nutr. 9:891376. doi: 10.3389/fnut.2022.891376
Received: 07 March 2022; Accepted: 26 April 2022;
Published: 02 June 2022.
Edited by:
Rafaela Rosário, University of Minho, PortugalReviewed by:
Andrew J. Sinclair, Deakin University, AustraliaCopyright © 2022 Di Maso, Bravi, Ferraroni, Agostoni, Eussen, Decsi, Quitadamo, Tonetto, Peila, Profeti, Salvatori, Kazmierska, Decarli, Vacca, Bertino, Stahl and Moro. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Monica Ferraroni, bW9uaWNhLmZlcnJhcm9uaUB1bmltaS5pdA==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.