
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr. , 13 May 2022
Sec. Food Chemistry
Volume 9 - 2022 | https://doi.org/10.3389/fnut.2022.855004
This article is part of the Research Topic Baby foods: Quality, Safety, Technology, and Regulation View all 6 articles
 Luisma Sanchez-Siles1,2*Sergio Román3Juan F. Haro-Vicente1,2Maria Jose Bernal1,2Michelle Klerks1,2Gaspar Ros4Ángel Gil5,6,7,8
Luisma Sanchez-Siles1,2*Sergio Román3Juan F. Haro-Vicente1,2Maria Jose Bernal1,2Michelle Klerks1,2Gaspar Ros4Ángel Gil5,6,7,8There is an urgent need to reduce sugar intake in early childhood. Commercial infant cereals are among the first solid foods introduced to infants at the beginning of the complementary feeding period in most countries. The aim of this study was to examine infants’ overall acceptability of low-sugar complementary cereals. To do so, a between-subjects experimental study with 165 parents and their infants aged 6–24 months was conducted where one group tested a high-sugar refined cereal (21 g/100 g), and the other a low-sugar cereal (<1 g/100 g) with 50% of whole grain, which represented a 95.2% decrease in sugar content. We found no significant differences between the two groups in terms of infants’ overall acceptability (infant’s reaction, estimated intake and relative intake). Importantly, infants’ reactions to high- and low-sugar cereals were not influenced by the time that infants had been consuming sweet cereals (15–25% sugar) before the experiment took place. In addition, parent’s overall liking and sensory evaluation (sweetness, color, taste, texture, and aroma) was positive and very similar in both groups. Overall, our findings show that it is feasible to reduce sugar content in infant cereals without sacrificing its sensory acceptability by infants and their parents. This represents a good opportunity for the infant food industry to adhere to current healthy and sustainable demands of lowering the sugar intake leading to important benefits in infants’ health, without compromising competitiveness in the market.
Excessive sugar consumption has been long associated with many diseases such as obesity, diabetes, high blood pressure, dental caries and cholesterol (1, 2). Accordingly, regulatory bodies, public health authorities, and professional organizations have been calling for a reduction in the sugar content of processed foods (3–5). Such reduction has straight-forward health benefits, but represents major challenges for the food processing industry (6–9). In particular, there might be technical difficulties as sugar’s role in foods is not restricted to providing sweetness only; it has other functions such as providing texture, color, and stability (8). For instance, the enzymatic hydrolysis of infant cereals (which produces free sugars) was traditionally carried out to stabilize their viscosity after preparation and for the physiological aim to increase the starch digestibility (10). Hence, the development of technical solutions to reformulate foods requires know-how and resources which may increase the product’s costs. Factors such as consumer education and legislation also play important roles in the success of reformulation strategies of sugar-reduced foods (9). Still, consumer acceptance becomes a fundamental challenge for food manufacturers. That is to say, consumers might dislike the taste of sugar-reduced foods, and thus may not purchase the reformulated/healthier version. For instance, findings from Markey et al. p. 138, who examined consumers’ acceptability and purchase intention of several sugar-reformulated foods and drinks, evidenced that: “significant improvements in the sensory qualities of some sugar-reduced products are required before their acceptance [by consumers]” (11), while Hutchings et al. p. 2,287 review concluded that: “substantial reduction of sugar in processed foods without compromising sensory properties may be an impossible dream” (12).
Only recently, scholars have paid attention to analyzing consumers’ sensory and hedonic responses to sugar-reduced foods (a summary of relevant studies is provided in Table 1). These studies provide very interesting insights, but their findings are not always consistent. In particular, while lowering sugar content did not affect sensory acceptance or liking in some studies (13–17), others reported mixed findings (18–25). For example, Oliveira et al. found that sensory perception was negatively affected for sugar content reductions higher than 10% and overall liking significantly decreased when reductions were higher than 20%, but not in lower reductions (23). Oliveira et al. p. 8 evidenced that sugar reductions up to 25% were accepted by consumers if 0.2% of flavor were added to the yogurts and still the modified yogurts were perceived as less sweet, and some subjects detected “unpleasant tastes” (26). In fact, other studies have even shown that sensory perceptions were negatively affected, and overall liking significantly reduced (11, 27–29).
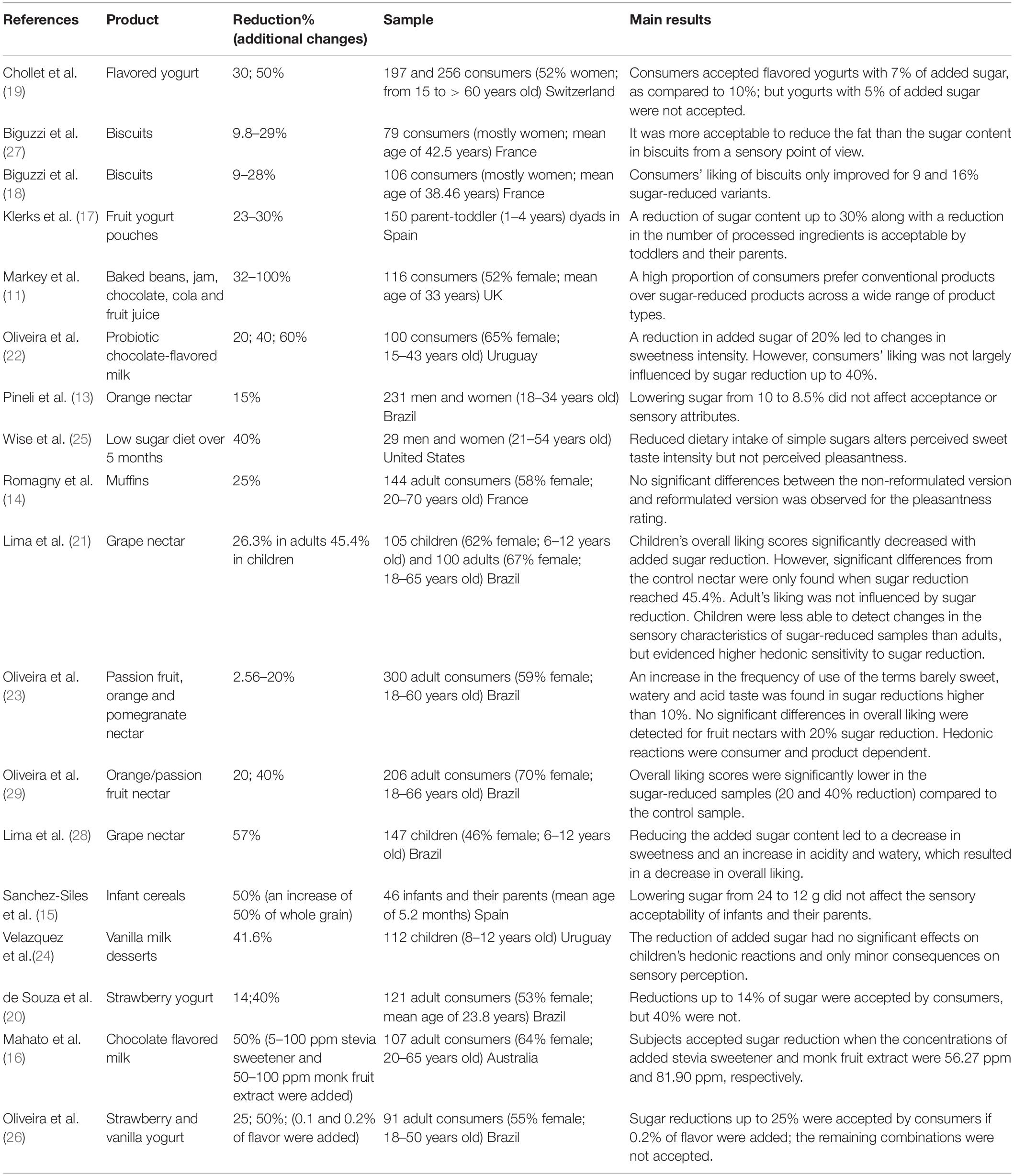
Table 1. Summary of studies evaluating consumers’ sensory and hedonic reactions to sugar-reduced foods.
Most likely, these varied reactions from consumers stem from the differences in terms of the (sugar-reduced) products tested (biscuits, fruit nectars and juices, chocolate, cola soft drinks, muffins, chocolate-flavored milk, milk desserts, baked beans and infant cereals), percentage of reduction in sugar (ranging from 2.56 to 100%) and consumers’ age and gender (adults, children, and infants) as evidenced in prior research (23, 29). Two key implications can be derived from this increasingly relevant stream of research: sugar reduction strategies are far from easy to be implemented and more research is needed in this regard, particularly in under-researched population segments such as children and infants (30).
All previous studies on consumers’ acceptability of sugar-reduced foods have been carried out mostly with adults and to a minor extent with children as shown in Table 1. One notable exception is Sanchez-Siles et al. who evaluated the sensory acceptability of infant cereals with a sugar reduction of 50% (from 24 g/100 g to 12 g/100 g) (15). Their preliminary findings on 46 infants from one Spanish city suggest that sugar reductions are feasible. Similar to that study, our interest in the present work is on infants (and their parents). Notably, food preferences are formed in infancy and shape later food preferences (31, 32). Exposure to sweet products early in life can promote a preference for sweet foods (33) as well as poor eating habits in childhood (34) which could lead to the development of many diseases as argued earlier. There is a need, therefore, to limit sugar intake, particularly in early childhood in order to promote lasting healthy eating habits (35, 36). Also, exposure to less sweet foods in infancy could reduce food neophobia/avoidance of bitter taste later in life (37, 38).
In the complementary feeding period, infants are exposed to a wider variety of foods which increases the diversity of flavor, taste, and texture exposure they receive (39, 40). Interestingly, exposure to sodium in complementary foods was shown to be associated with a higher acceptance of salty taste in preschoolers (41). Commercial complementary cereals play a major role in infant nutrition as they are among the first solid foods introduced at the beginning of the complementary feeding period in most countries (3, 42). Also, cereals are an excellent source of energy and provide starch, fiber, and proteins as well as vitamins, minerals, and other bioactive compounds (43). This is particularly the case for whole grain, which consists of the endosperm, germ, and bran in the same relative proportions as in the intact kernel (44), rather than refined cereals (10, 45). In fact, the consumption of whole grain in infants and children has been emphasized by several public health institutions and professional organizations, e.g., (46–49). Unfortunately, many infant cereals contain high levels of sugar and low percentages of whole grain as evidenced in previous studies and reports (50–53).
In the light of these considerations and facts, the aim of this study is to examine infants’ overall acceptability and parents’ overall liking and sensory evaluations of a drastic reduction of sugar and addition of whole grain in complementary infant cereals. More specifically, we will compare high-a sugar refined cereal (21 g/100 g) with low-sugar cereal (<1 g/100 g) which has 50% of whole grain. Hopefully, our insights can provide policymakers as well as the food industry with valuable guidelines for the effective implementation of policies and actions to reduce sugar and increase whole grain intake in early childhood.
Parents with healthy infants from five Spanish cities (Madrid, Barcelona, Seville, Murcia, and Valencia) were recruited through an independent market research firm and from kindergartens. Eligible subjects consisted of parents who had at least one child aged 6–24 months; had primary responsibility for their child’s feeding and their infants were having complementary cereals before the experiment took place. Eligible infants needed to have a gestational age of 37–42 weeks and a birth weight higher than 2,500 grams. Exclusion criteria for participation included: (1) infants who had food allergies or intolerances, swallowing or digestion problems, or other medical issues that could influence the ability to eat and (2) infants who were consuming low sugar cereals [those which contain no more than 5 g of sugar per 100 g according to EU Regulation 1924/2006 (54)] and consequently were already used to this less sweet flavor of cereals. The final sample consisted of 165 parent-infant dyads.
This study was conducted according to the Declaration of Helsinki guidelines. Ethical approval was obtained from the Research Ethical Committee of the University of Murcia (code: CEI 2116/2018). All participants signed an informed parental consent form for each infant before the inclusion. Parents received a 30€ voucher or a gift for their participation.
Two different commercial infant cereals were studied: a high-sugar (21 g/100 g) infant cereal, in which sugar was produced by starch hydrolysis (high-sugar cereal), and a non-hydrolyzed low-sugar (<1 g/100 g) infant cereal (low-sugar cereal). Ingredient information and nutritional composition of the two infant cereals are described in Table 2. Both infant cereals were manufactured in the same production line, with the same processing conditions, and 2 months before testing to minimize quality differences between the samples and recreate normal consumer consumption. The only formulation differences between the two samples were: (1) the level of sugar produced during hydrolysis, and (2) the content of whole grain (0% whole grain in the high-sugar cereal and 50% whole grain in the low-sugar cereal). Nutritional properties of the reformulated low-sugar cereal were slightly better as a consequence of the addition of whole grain (Table 2). All samples used in this study were packaged into identical foil bags. Each bag was marked with a three-digit randomization code. Both samples were labeled equally and were designed and produced by Hero España S.A.
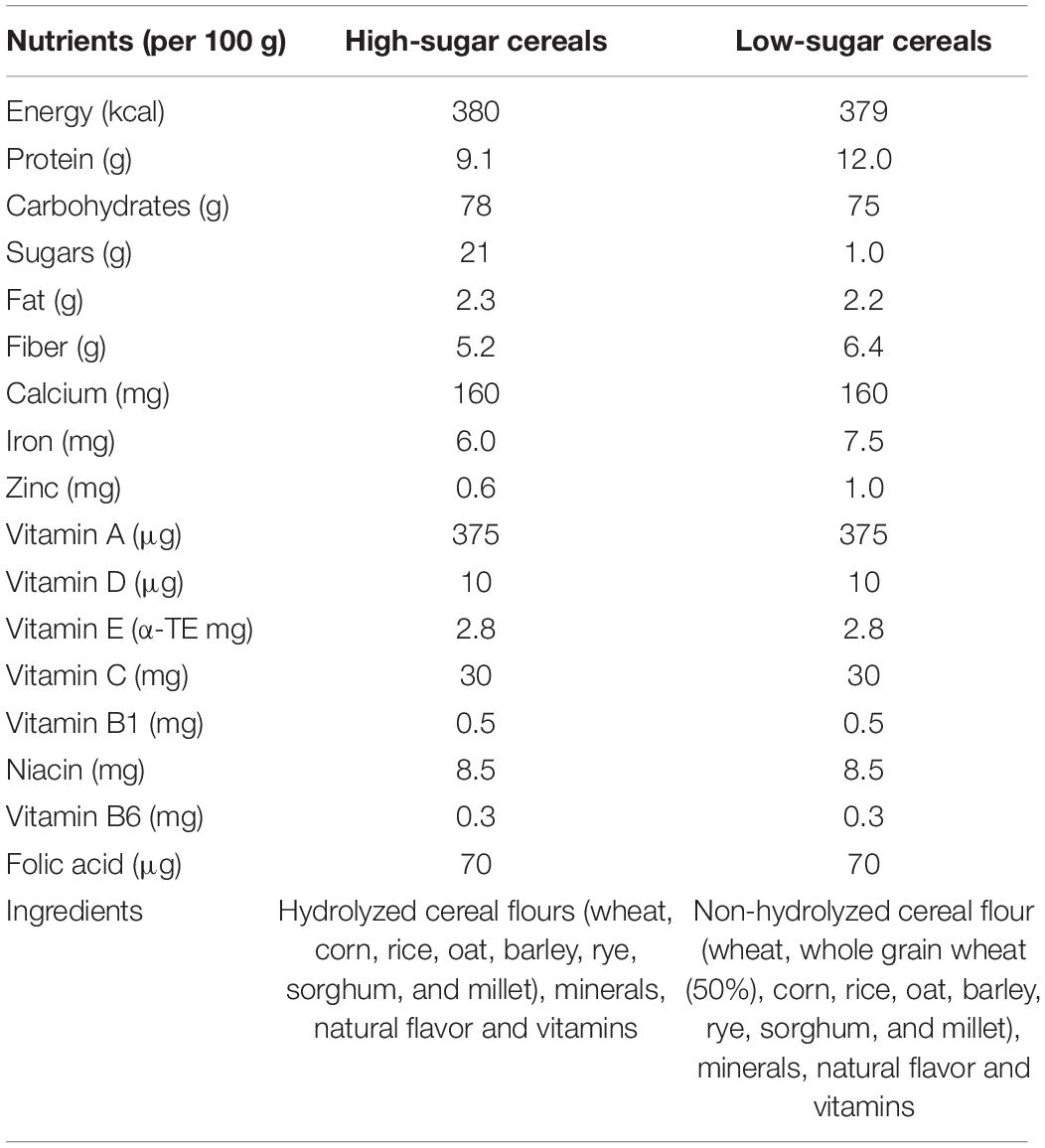
Table 2. Nutritional composition of infant cereals per 100 g.
The study uses a between-subjects experimental design and was carried out from October 2018 to January 2019. Parents were responsible for conducting the experiment and reporting on their children’s reactions and food intake. In-home studies present two advantages: they can be performed with few constraints on the participants, and children are in their usual environment with their usual feeder (55). Extant research has evidenced that parents are well aware of their infant’s responses toward foods and therefore are likely to be more sensitive to subtle differences in their reactions (15, 56–60). Parents were randomly allocated to one of the two groups: high-sugar refined (n = 82) and low-sugar whole grain cereals (n = 83).
The experiment was carried out during two consecutive days to have a more valid assessment of the reactions (as compared to a 1-day study). To be qualified for the study, infants had to be having commercial cereals at least 2 weeks before the experiment started. Prior to testing, to ensure accurate recording, parents were visited on day 1 by a research assistant who explained to them how to conduct the experiment, gave them clear and detailed written instructions, the questionnaire, and the infant cereals samples. Following standard procedures parents were given the following instructions: (1) to not feed their toddler with beverages or solid foods for 1 h before the testing so as not to influence their hunger status (58, 61), (2) to prepare cereals by mixing them with the infant formula milk that they had been using before the experiment took place, namely either follow-on formula (6–12 months) or growing-up milk (more than 12 months), which have very similar nutritional composition and properties. No further instructions were given in this regard as the aim was that infants were fed the very same way as they had been fed before the study took place so as not to bias the results (57), (3) to feed their infants in the habitual place, at a normal pace until the infant refused the spoon or bottle three consecutive times, (4) to fill out the evaluation of their infant’s reaction before conducting their own rating to avoid any possible bias and (5) to test and evaluate the cereals themselves only after infants have had theirs, in order ensure no interference with their infant’s reactions due to non-habitual parent behavior (product testing) during the feeding period. Parents’ reactions were included in our study because they play a major role in infant feeding practices and food brand/product selection (62, 63). Parents were also told to carry out the test the same time of days 1 and 2. No significant differences were found between the two groups (F = 4.21, p = 0.12) in terms of the moment of the day when the test took place (54.8% morning, 3.7% afternoon and 41.5% night in the high-sugar group vs. 43.4% morning, 10.8% afternoon and 45.8% night in the low-sugar group). On day 4, research assistants picked up questionnaires at the parents’ house. An overview of the study protocol is shown in Figure 1A.
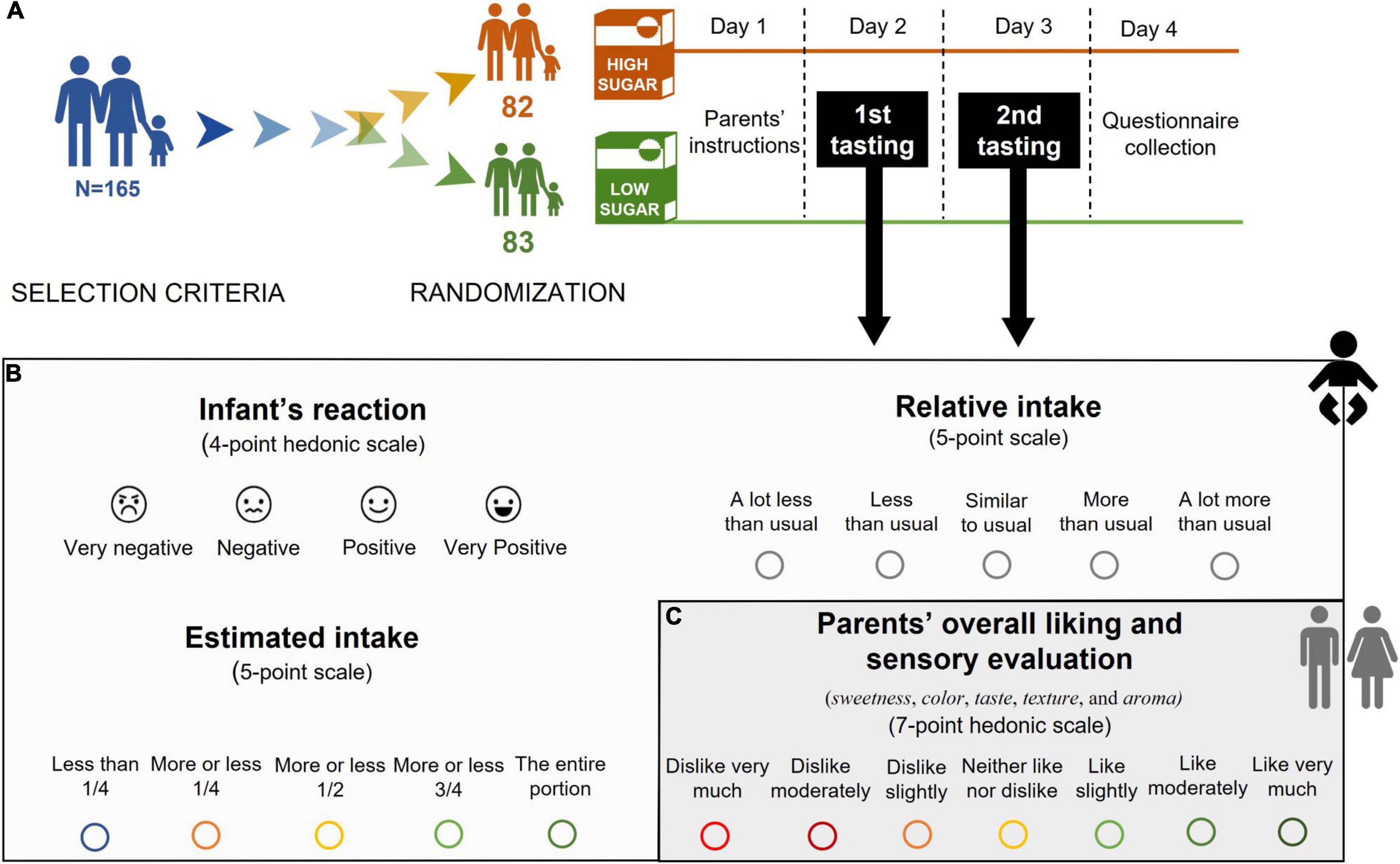
Figure 1. (A) Experimental design (B) Measurement of infant’s overall acceptability, and (C) parents’ overall liking and sensory evaluation.
Overall acceptability of cereals by infants was assessed through three different, yet related measures: the infant’s reaction toward the cereals (as perceived by parents), the estimated intake, and the relative intake of cereals compared to usual intake (see Figure 1B).
The infant’s reaction was measured by means of a 4-point hedonic scale (15, 32, 57, 58). The scale ranges from: “1 = very negative” if the infant spitted out the food, frowned, pushed the spoon away or stopped eating; “2 = negative” if the infant ate a couple of spoonfuls, grimaced and stopped eating; “3 = positive” if the infant ate some of the food without a specific reaction; “4 = very positive” if the infant accepted the first spoonful immediately and displayed signs of content, such as a relaxed face or a smile. All scores on the scale were accompanied with a corresponding smiley-face to guide the parents (Figure 1B).
The ingested amount (estimated intake) and the relative intake compared to usual infant cereal intake were measured via a 5-point scale with scores ranging from: “1 = less than 1/4” to “5 = the entire portion” and “1 = a lot less than usual” to 5 = a lot more than usual” (55) (Figure 1B).
As depicted in Figure 1C, overall liking was measured using a one-item 7-point hedonic scale ranging from “1 = dislike very much” to “7 = like very much” (15, 57). Parents were also asked to evaluate key sensory attributes: sweetness, color, taste, texture, and aroma on the same 7-point hedonic scale (64).
Parents were asked for general feeding practices (e.g., age of first introduction of food, first food introduced) and cereal feeding practices (e.g., mode of consuming infant cereals, frequency of cereals intake, weight (g) of cereals prepared in one serving, brand of cereals used before the study). The wording of questions, sequence and response options were based on our previous work (65).
Differences between the feeding groups (high-sugar and low-sugar cereals) were tested with Student’s t-tests and Pearson chi-square tests. All results with a significance level of p < 0.05 were considered statistically significant. SPSS Version 26.0 (IBM, SPSS Inc., Armonk, NY, United States) software was used for statistical analyses.
The characteristics of the 165 parent-infant dyads are presented in Table 3. There were no significant differences between the two groups in terms of demographic characteristics.
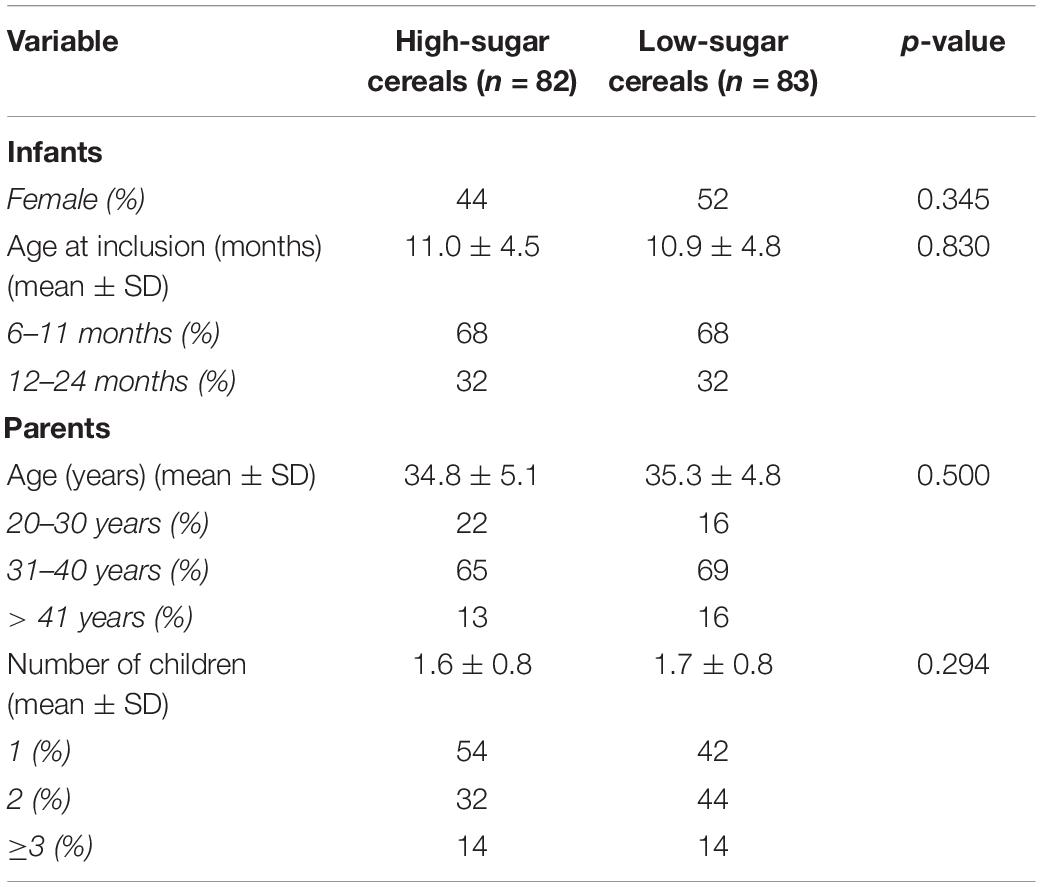
Table 3. Demographic characteristics of infants and parents per group.
No significant differences were found between the two groups in terms of general and cereal feeding practices, which further warrants the comparison between groups. As shown in Figure 2A, solids were mostly introduced between 4 and 6 months. Cereals (67%) were the first solid food introduced followed by fruits (26%) (Figure 2B). The mean age of introduction of cereals was 5.1 (± 1.2) months. The most frequent mode of preparation of cereals was the bottle (Figure 2C). Most of the infants (95%) consumed cereals daily (Figure 2D), mostly in the morning and/or at night (Figure 2E).
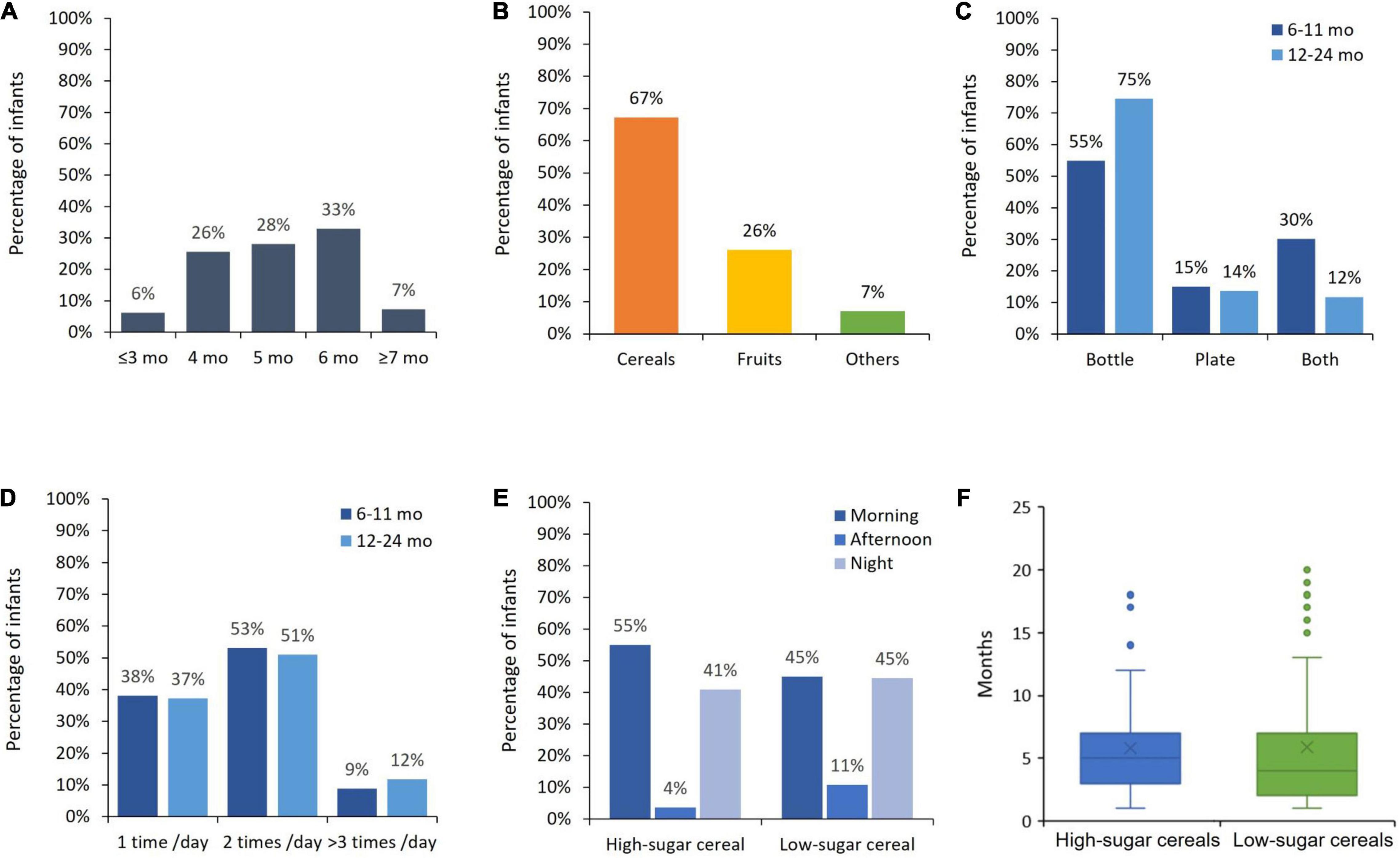
Figure 2. General and cereal feeding practices. (A) Timing (age) of introduction solids. (B) Types of first introduced solids. (C) Mode of infant cereal consumption. (D) Frequency of infant cereal consumption per day. (E) Moment of infant cereal consumption. (F) Duration in months of infant cereal consumption at inclusion.
On average, the infants had been fed cereals 5.8 (± 4.2) months and 5.9 (± 4.9) months (high-sugar and low-sugar groups, respectively) before starting the experiment (Figure 2F). Importantly, these mean values were not significantly different (F = 1.54, p = 0.21) which further warrants comparing both groups. Infants had been given cereals with a similar sugar level which ranged from 15 to 25% in both groups. This implies that infants were used to having sweet cereals at inclusion.
As shown in Table 4, there were no significant differences between the two groups in any of the three variables used to measure infants’ overall acceptability (infant’s reaction, estimated intake and relative intake) on either day of the experiment (days 1 and 2).
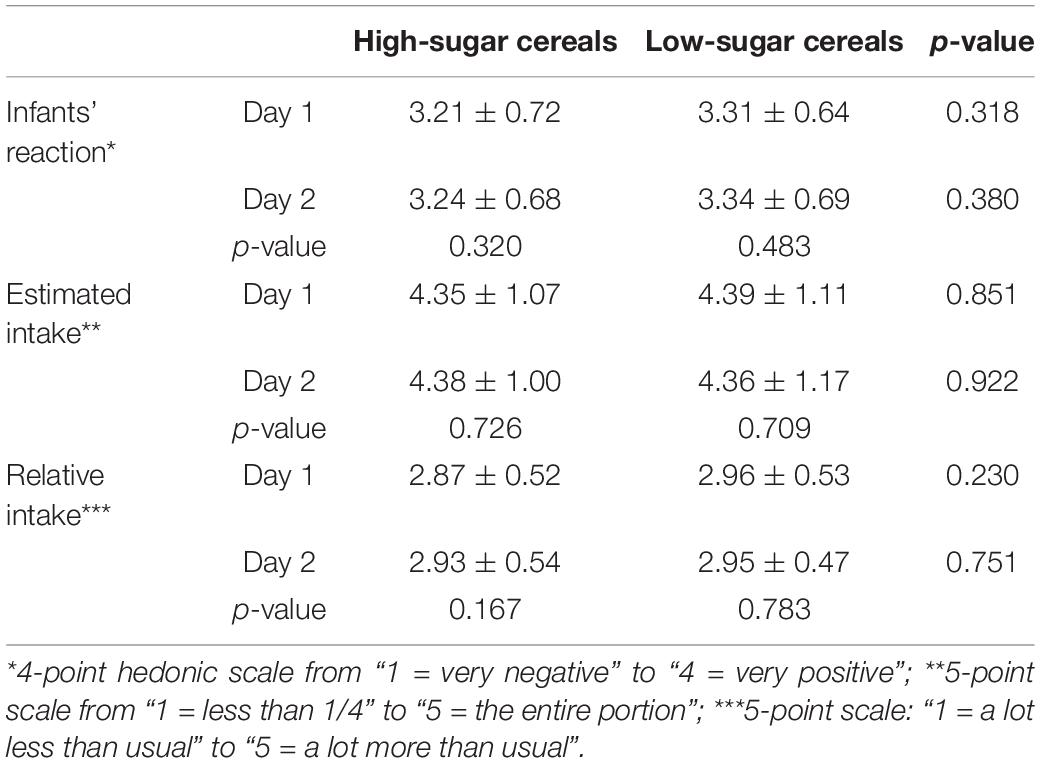
Table 4. Infants’ overall acceptability (differences by group on mean values).
In addition, as illustrated in Figure 3A, the frequency of positive and very positive reactions reported by parents was high in both groups (88 and 96% in the high-sugar and low-sugar group, respectively). Similarly, estimated intake was high (more than 60%) in both groups (Figure 3B) and relative intake was mostly similar to usual (before the start of the experiment) in both groups (83 and 87%, respectively as shown in Figure 3C). Overall, these results highlight the very good acceptability of low-sugar cereals by infants in our study.
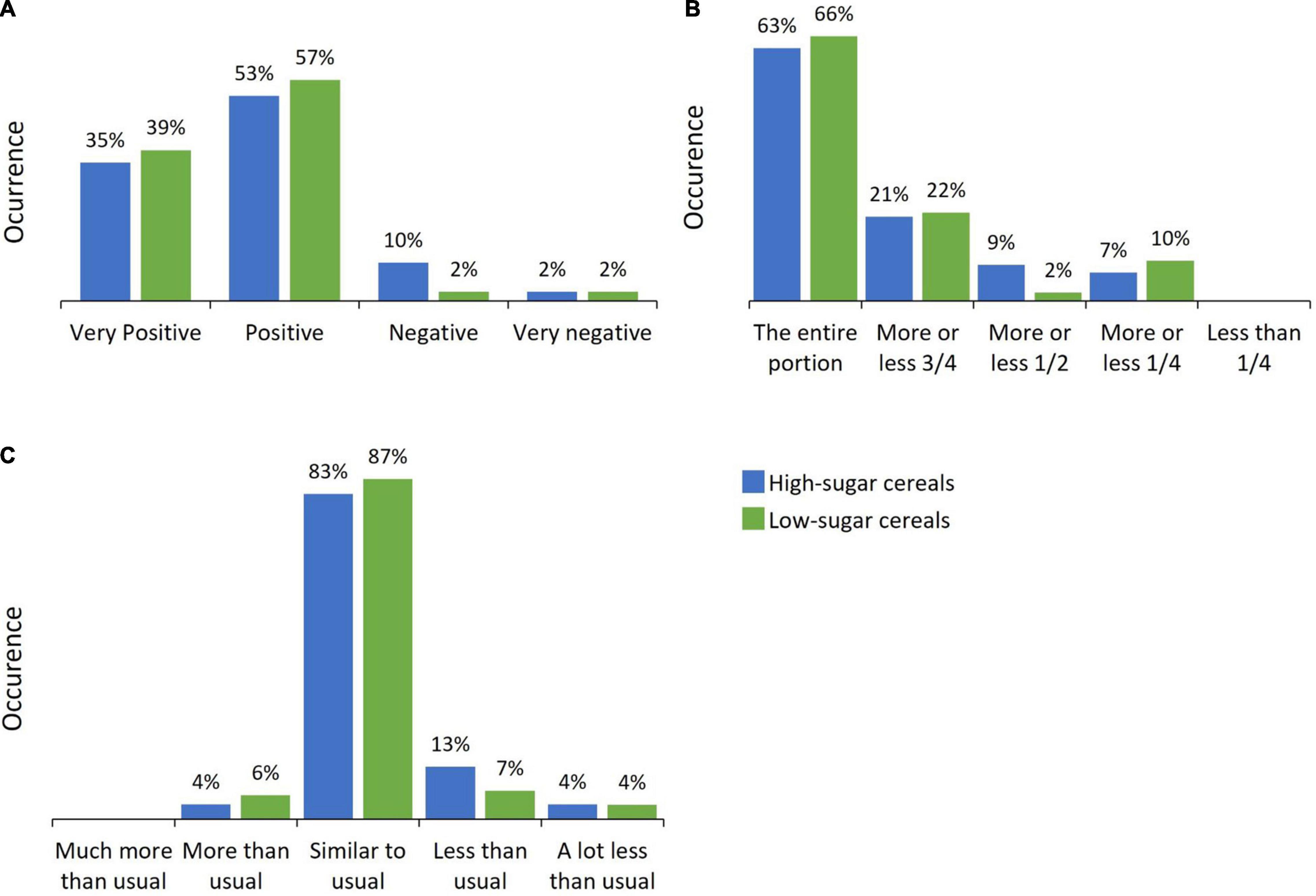
Figure 3. Infants’ overall acceptability (differences by group in percentages). (A) Infant’s reaction. (B) Estimated intake. (C) Relative intake.
To further substantiate our results, we examined the extent to which the number of months that infants had been exposed to sweet cereals (15–25% sugar) before the beginning of the study could have an influence on infants’ reactions to high- and low-sugar cereals in our experiment. We did not find any significant differences in infants’ reactions depending on the duration they had been consuming cereals before the experiment took place (Figure 4).
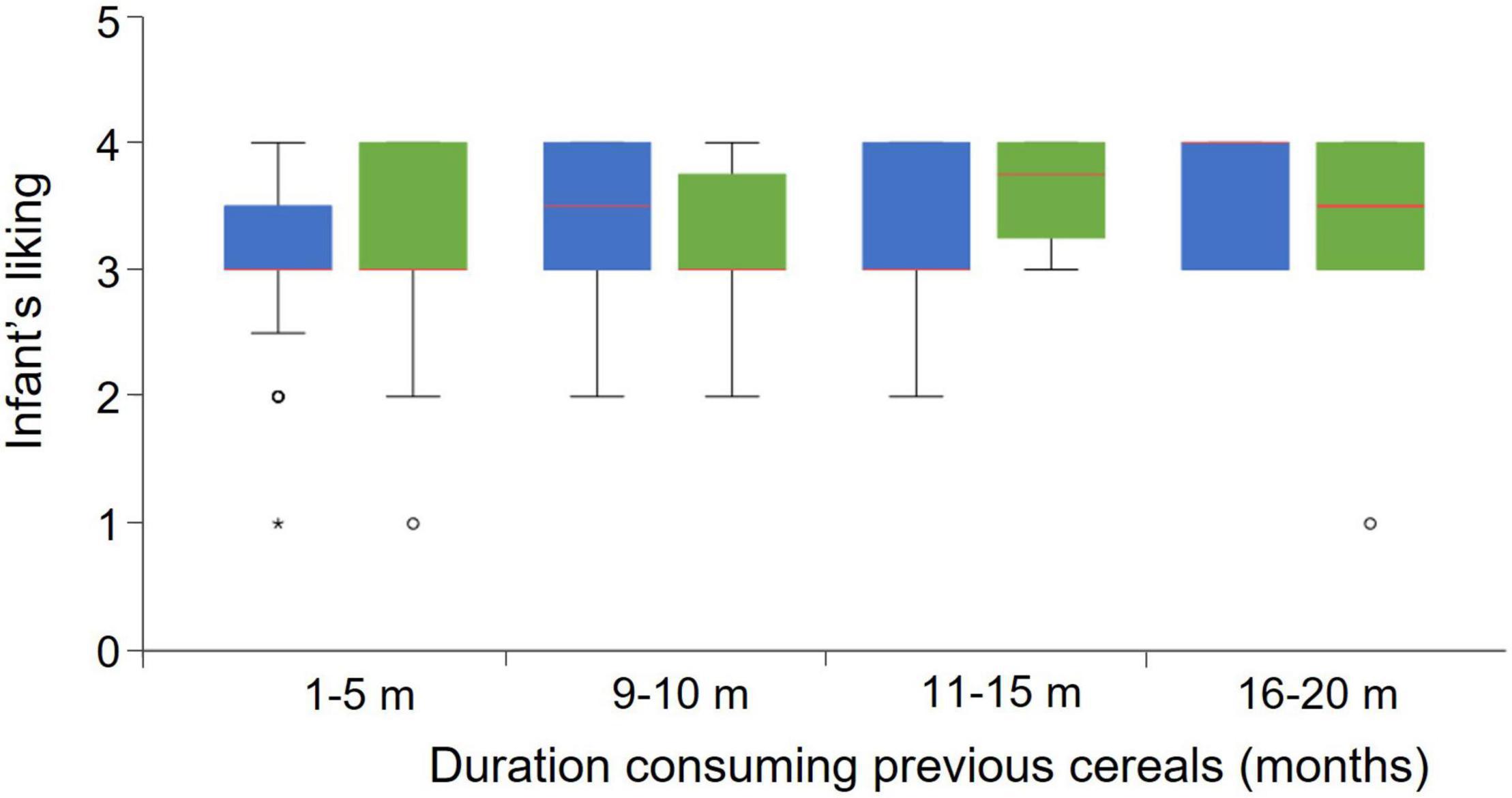
Figure 4. Influence of duration consuming previous cereals on infant’s reaction. Dots are mild outliers (Q1-1.5*IQR). The asterisk is an extreme outlier (Q1-3*IQR).
Consistent to findings reported above on infants’ overall acceptability, parents’ overall liking and sensory evaluation were positive and similar in both groups in all attributes considered. More specifically, as reported in Table 5, differences between the two groups were not significant.
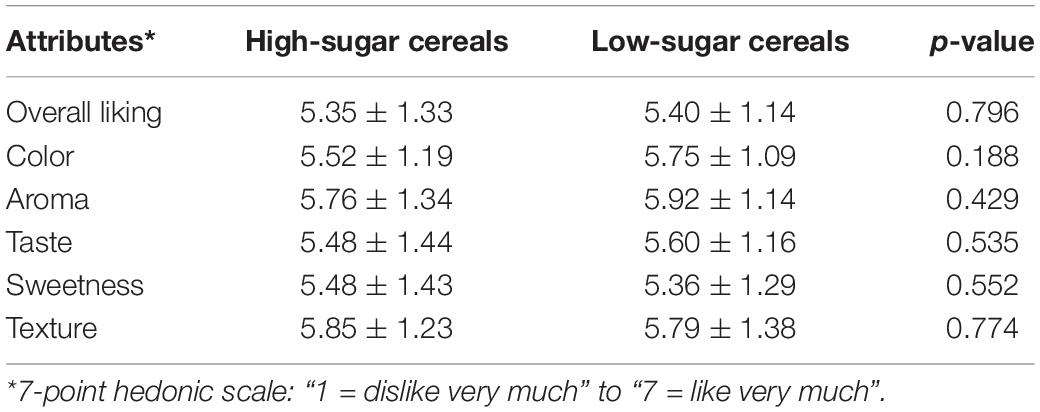
Table 5. Parents’ rating of overall liking and evaluation of sensory attributes (differences by group on mean values).
As shown in Table 6, the mean quantity of cereals intake per day was significantly larger in the high-sugar group (27.42 g) as compared to the low-sugar group (19.22 g). This larger intake of cereals, along with a much higher content of sugar, implies that sugar intake per day is more than 30 times larger in the high-sugar group (5.77 g), in comparison to the low-sugar group (0.19 g). Furthermore, the consumption of free sugars would be 3.40% of total daily energy intake in the high-sugar group, and only 0.12% in the low-sugar one. If we extrapolate these figures to annual consumption, the estimated yearly intake of sugar would be around 2 kg in the high-sugar group as compared to 69 g in the low-sugar group.
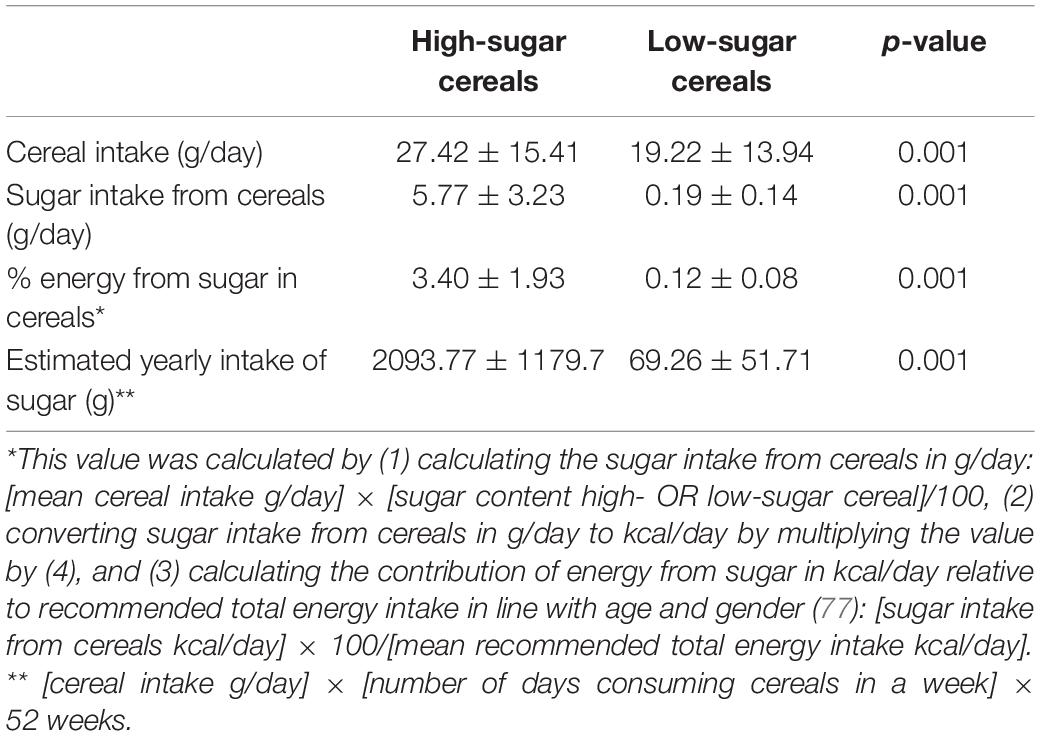
Table 6. Sugar intake from cereals (differences by group).
This study examined infants and their parents’ acceptability of a high-sugar refined cereal vs. low-sugar whole grain cereal. We found no significant differences between the two groups in terms of infants’ overall acceptability (infant’s reaction, estimated and relative cereals intake). Importantly, infants’ reactions to high- and low-sugar cereals were not influenced by the time that infants had been consuming sweet cereals (15–25% sugar) before the experiment took place. In addition, parent’s overall liking and sensory evaluation (sweetness, color, taste, texture, and aroma) were not significantly different between groups. Overall, our findings suggest that it is feasible to reduce sugar content in infant cereals (and add whole grain) without sacrificing its sensory acceptability by infants (and their parents).
The reduction of sugar levels can be extremely challenging for food manufacturers because of the expected changes in food sensory characteristics (7). Only recently, as described in the introduction, sensory and consumer scientists have paid attention to testing consumers’ reactions to sugar-reduced food products. Most of these studies have been conducted with adults and to a minor extent with children, who tried the reformulated (sugar-reduced) products only once. On the contrary, we focused on infants who tested the reformulated products more than once during 2 days, thus improving the reliability of the results. Our findings concur with those studies which evidenced that sugar reductions are feasible (13, 14, 16, 17). However, as infant cereals were prepared with infant formula, which contains about 7 g of lactose/100 ml, we could hypothesize that their sweet taste might improve the acceptability of this large sugar reduction (95.2%) (15, 57) in comparison with other studies where smaller reduction failed to do so (11, 20, 26, 28, 29). This implies that the product category to be reformulated represents a key factor which significantly affects the extent to which sugar levels can be reduced and still be accepted by consumers. For example, recent findings from Klerks et al. reveal that a reduction of sugar content up to 30% in yogurt pouches is sensory accepted by toddlers (1–4 years old) and their parents (17). Furthermore, our results build and significantly add to Sanchez-Siles et al.’s (15) study in many ways. First, we test a much larger sugar reduction (95.2 vs. 50%). Second, we evaluate a wider spectrum of sensory reactions both in infants and their parents. Third, we use a larger sample of infants (165 vs. 46) from several cities (5 vs. 1). Fourth, and most importantly, infants in our study were already used to having sweet cereals (15–25% sugar), whereas infants in Sanchez-Siles et al.’s (15) had never tried cereals before. Notably, our findings along with previous results from Sanchez-Siles et al. (15) and Haro-Vicente et al. (57) demonstrate that the addition of whole grain does not affect infant cereal’s acceptability (15, 57).
Overall, the insights offered in this study are particularly relevant as they indicate that infants (in these early stages of their life), even used to having sweet cereals, can accept cereals that are highly reduced in sugar. This provides further evidence to previous studies suggesting that even though infants are born with an innate preference for sweet taste, such preferences are likely to be modified during the complementary feeding period (34, 66). This is one of the reasons why several international health agencies and pediatric associations recommend stricter regulations regarding sugar intake in infants and children. For example, in 2015 the WHO recommended that the consumption of free or added sugars should not exceed 5% of total daily energy intake for children below 2 years, while the ESPGHAN Committee on Nutrition recommended that sugar should not be added to complementary foods (3). Similarly, the American Heart Association [AHA] (4, 46) and the new Dietary Guidelines for Americans (47) recommended to avoid the consumption of any added sugar in children younger than 2 years old, and a Policy brief from the WHO Regional Office for Europe (5) has recently called for a complete prohibition of added, free sugars and sweeteners (including syrups, honey, fruit juice, fruit juice concentrates, and non-sugar sweeteners) in all commercial complementary foods.
Surprisingly, most of these organizations and agencies focus the guidelines on “free sugars,” but none of them have considered the sugars produced during the hydrolyzation of cereals. The level and type of sugar produced depend on the degree of hydrolysis (time and temperature) and the type of enzyme used. The use of gluco-amylase improves the sweetness (due to the production of glucose), while the use of alpha-amylase produces dextrins and maltose (less sweet than glucose and sucrose). Depending on the degree of hydrolysis the sugar level in cereals can reach up to 30% of sugar (10). This is particularly disturbing because sugar produced while hydrolyzing cereals is not specifically mentioned or defined in any current legislation around the world. As a result, some manufacturers claim that they are producing cereals “with non-added sugar,” while they may have a very high content of produced sugar as a result of the hydrolysis process. Therefore, we strongly encourage policymakers to consider sugars produced in the hydrolysis as free sugars.
We found cereals to be the first solid foods introduced (in 67% of the participants in our study), in line with previous studies in Spain (65) and other countries such as United Kingdom, Ireland and Canada (67–69). Also, our results showed that the frequency of intake of infant cereals was high (95% of infants consumed cereals daily and around 50% were fed with cereals two times per day). Thus, cereals may represent the first time infants try solid foods with added and/or produced sugar. Importantly, daily consumption of cereals (and sugar) was significantly higher in the high-sugar group (hydrolyzed cereal) as compared to the low-sugar group (non-hydrolyzed cereal). The lower intake observed is directly related to the presence or not of hydrolysis. That is, when starch is hydrolyzed, the viscosity is reduced, and consequently more grams of cereals have to be added to obtain the same texture properties (mainly viscosity) of the cereals without hydrolysis. Therefore, a reduction of 95.2% of sugar as tested in our study would imply that infants would be reducing their sugar intake with more than 2 kilos yearly (see Table 6). This estimated reduction would be directly in line with the development and promotion of sustainable healthy diets (70–72), and would make it much easier to comply with the WHO recommendation of sugar consumption not exceeding 5% of total daily energy intake. Furthermore, the elimination of hydrolysis would represent a significant reduction in food processing, leading to less-processed, more natural products consistent with the latest food international consumers’ trends (73, 74).
While our study offers important implications, we recognize some limitations which can lead to interesting future research directions. First, unlike prior research (15), we conducted our experiment with infants and parents located in five different Spanish cities. Still, our findings need to be validated in other countries with special emphasis on contexts where infant cereals are characterized by a high sweetness intensity (e.g., Middle East countries). Second, following extant research (18, 28, 29), our study relied on a between-subject design where each group tested only one product (either non-reformulated or reformulated cereals). Importantly, both groups can be considered as equivalent (75), as there were no significant differences in terms of the relevant characteristics for the topic under research (e.g., number of months having cereals at inclusion, age, gender of the subjects). Future research could try to replicate our findings through a repeated measures design where the same group of subjects (infants and their parents) test both products. Third, infants (and their parents) tested the cereals several times over two consecutive days and results did not differ between days 1 and 2. Still, participants could try the cereals for a longer period in future studies. Finally, our analyses were focused on complementary infant cereals. Future research is needed to examine infants’ reactions to sugar reductions in other product categories such as snacks (some of them characterized by high levels of sugar) and where sugar function is not restricted to delivering a sweet taste, but also providing bulk and texture (76).
Findings from our study indicate that it could be possible to significantly reduce sugar content (or even eliminate it) and add whole grain in infant cereals without influencing infants’ overall acceptability. This is extremely relevant, as prior research has shown that exposure to low-sugar foods in infancy may promote the acceptance of and eventually a preference for those foods across the lifespan. The current study represents a promising case for the infant food industry to adhere to current healthy and sustainable demands leading to important benefits in infants’ health, without compromising competitiveness in the market.
The raw data supporting the conclusions of this article will be made available without undue reservation, upon request to the corresponding author.
The studies involving human participants were reviewed and approved by the Research Ethical Committee of the University of Murcia (code: CEI 2116/2018). Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
LS-S: contributes to the conceptualization, methodology, supervision, writing—original draft, writing—review and editing. SR: contributes to the conceptualization, writing—original draft, writing—review and editing. JH-V: contributes to the data curation, formal analysis, investigation, methodology, writing—review and editing. MB: contributes to the conceptualization, data curation, formal analysis, methodology, and writing—review and editing. MK: contributes to the writing—original draft and writing—review and editing. GR and ÁG: contributes to the conceptualization and writing—review and editing. All authors read and approved the final manuscript and agreed to be accountable for the content of the work.
This research was funded by Hero ÁG (Switzerland).
LS-S, JH-V, MB, and MK were members of the Research and Nutrition of Hero Group, a Swiss international food manufacturer; ÁG received honoraria-payments for specific speeches and seminar presentations from Hero, Nestlé; Lactalis and others baby food companies.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that this study received funding from Hero ÁG. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We would like to thank all parents and children who participated in this study.
1. Malik VS, Schulze MB, Hu FB. Intake of sugar-sweetened beverages and weight gain: a systematic review. Am J Clin Nutr. (2006) 84:274–88. doi: 10.1093/ajcn/84.1.274
2. Singh J, Rasane P, Kaur S, Kumar V, Dhawan K, Mahato DK, et al. Nutritional interventions and considerations for the development of low calorie or sugar free foods. Curr Diabetes Rev. (2020) 16:301–12. doi: 10.2174/1573399815666190807144422
3. Fewtrell M, Bronsky J, Campoy C, Domellöf M, Embleton N, Mis NF, et al. Complementary feeding: a position paper by the European society for paediatric gastroenterology, hepatology, and nutrition (ESPGHAN) committee on nutrition. J Pediatr Gastroenterol Nutr. (2017) 64:119–32. doi: 10.1097/MPG.0000000000001454
4. Vos MB, Kaar JL, Welsh JA, Van Horn LV, Feig DI, Anderson CA, et al. Added sugars and cardiovascular disease risk in children: a scientific statement from the American heart association. Circulation. (2017) 135:e1017–34. doi: 10.1161/CIR.0000000000000439
5. World Health Organization.Commercial Foods for Infants and Young Children in the WHO European Region: Policy Brief on Two New Reports by the WHO Regional Office for Europe. Geneva: World Health Organization (2019).
6. Deliza R, Lima MF, Ares G. Rethinking sugar reduction in processed foods. Curr Opin Food Sci. (2021) 40:58–66. doi: 10.1016/j.cofs.2021.01.010
7. Román S, Bodenstab S, Sanchez-Siles LM. Corporate tensions and drivers of sustainable innovation: a qualitative study in the food industry. Eur J Innov Manag. (2021). doi: 10.1108/EJIM-11-2020-0469
8. Buttriss JL. Food reformulation: the challenges to the food industry. Proc Nutr Soc. (2013) 72:61–9. doi: 10.1017/S0029665112002868
9. Lehmann U, Mak TN, Bolten CJ. Reformulation as a Strategy for Developing Healthier Food Products: Challenges and Recent Developments – An Industry Perspective. Lausanne: Nestle Research (2019). p. 89–110.
10. Klerks M, Bernal MJ, Roman S, Bodenstab S, Gil A, Sanchez-Siles LM. Infant Cereals: current status, challenges, and future opportunities for whole grains. Nutrients. (2019) 11:473. doi: 10.3390/nu11020473
11. Markey O, Lovegrove JA, Methven L. Sensory profiles and consumer acceptability of a range of sugar-reduced products on the UK market. Food Res Int. (2015) 72:133–9. doi: 10.1016/j.foodres.2015.03.012
12. Hutchings SC, Low JYQ, Keast RSJ. Sugar reduction without compromising sensory perception. An impossible dream? Crit Rev Food Sci Nutr. (2019) 59:2287–307. doi: 10.1080/10408398.2018.1450214
13. Pineli LLO, Aguiar LA, Fiusa A, Botelho RBA, Zandonadi RP, Melo L. Sensory impact of lowering sugar content in orange nectars to design healthier, low-sugar industrialized beverages. Appetite. (2016) 96:239–44. doi: 10.1016/j.appet.2015.09.028
14. Romagny S, Ginon E, Salles C. Impact of reducing fat, salt and sugar in commercial foods on consumer acceptability and willingness to pay in real tasting conditions: a home experiment. Food Qual Prefer. (2017) 56:164–72. doi: 10.1016/j.foodqual.2016.10.009
15. Sanchez-Siles LM, Bernal MJ, Gil D, Bodenstab S, Haro-Vicente JF, Klerks M, et al. Are sugar-reduced and whole grain infant cereals sensorially accepted at weaning? A randomized controlled cross-over trial. Nutrients. (2020) 12:1883. doi: 10.3390/nu12061883
16. Mahato DK, Keast R, Liem DG, Russell CG, Cicerale S, Gamlath S. Optimisation of natural sweeteners for sugar reduction in chocolate flavoured milk and their impact on sensory attributes. Int Dairy J. (2021) 115:104922. doi: 10.1016/j.idairyj.2020.104922
17. Klerks M, Román S, Haro-Vicente JF, Bernal MJ, Sanchez-Siles LM. Healthier and more natural reformulated baby food pouches: will toddlers and their parents sensory accept them? Food Qual Prefer. (2022) 99:104577. doi: 10.1016/j.foodqual.2022.104577
18. Biguzzi C, Lange C, Schlich P. Effect of sensory exposure on liking for fat– or sugar-reduced biscuits. Appetite. (2015) 95:317–23. doi: 10.1016/j.appet.2015.07.001
19. Chollet M, Gille D, Schmid A, Walther B, Piccinali P. Acceptance of sugar reduction in flavored yogurt. J Dairy Sci. (2013) 96:5501–11. doi: 10.3168/jds.2013-6610
20. de Souza LBA, Pinto VRA, Nascimento LGL, Stephani R, de Carvalho AF, Perrone ÍT. Low-sugar strawberry yogurt: Hedonic thresholds and expectations. J Sens Stud. (2021) 36:1–15. doi: 10.1111/joss.12643
21. Lima M, Ares G, Deliza R. Children and adults’ sensory and hedonic perception of added sugar reduction in grape nectar. J Sens Stud. (2018) 33:1–9. doi: 10.1111/joss.12317
22. Oliveira D, Antúnez L, Giménez A, Castura JC, Deliza R, Ares G. Sugar reduction in probiotic chocolate-flavored milk: Impact on dynamic sensory profile and liking. FRIN. (2015) 75:148–56. doi: 10.1016/j.foodres.2015.05.050
23. Oliveira D, Galhardo J, Ares G, Cunha LM, Deliza R. Sugar reduction in fruit nectars: impact on consumers’ sensory and hedonic perception. Food Res Int. (2018) 107:371–7. doi: 10.1016/j.foodres.2018.02.025
24. Velazquez AL, Vidal L, Varela P, Ares G. Cross-modal interactions as a strategy for sugar reduction in products targeted at children: case study with vanilla milk desserts. Food Res Int. (2020) 130:108920. doi: 10.1016/j.foodres.2019.108920
25. Wise PM, Nattress L, Flammer LJ, Beauchamp GK. Reduced dietary intake of simple sugars alters perceived sweet taste intensity but not perceived pleasantness. Am J Clin Nutr. (2016) 103:50–60. doi: 10.3945/ajcn.115.112300.1
26. Oliveira AAA, Andrade AC, Bastos SC, Condino JPF, Curzi Júnior A, Pinheiro ACM. Use of strawberry and vanilla natural flavors for sugar reduction: a dynamic sensory study with yogurt. Food Res Int. (2021) 139:109972. doi: 10.1016/j.foodres.2020.109972
27. Biguzzi C, Schlich P, Lange C. The impact of sugar and fat reduction on perception and liking of biscuits. Food Qual Prefer. (2014) 35:41–7. doi: 10.1016/j.foodqual.2014.02.001
28. Lima M, Ares G, Deliza R. Comparison of two sugar reduction strategies with children: case study with grape nectars. Food Qual Prefer. (2019) 71:163–7. doi: 10.1016/j.foodqual.2018.07.002
29. Oliveira D, Ares G, Deliza R. The effect of health/hedonic claims on consumer hedonic and sensory perception of sugar reduction: case study with orange/passionfruit nectars. Food Res Int. (2018) 108:111–8. doi: 10.1016/j.foodres.2018.03.003
30. Velázquez AL, Vidal L, Varela P, Ares G. Sugar reduction in products targeted at children: why are we not there yet? J Sens Stud. (2021) 36:e12666. doi: 10.1111/joss.12666
31. Nicklaus S. The role of food experiences during early childhood in food pleasure learning. Appetite. (2016) 104:3–9. doi: 10.1016/j.appet.2015.08.022
32. Schwartz C, Chabanet C, Lange C, Issanchou S, Nicklaus S. The role of taste in food acceptance at the beginning of complementary feeding. Physiol Behav. (2011) 104:646–52. doi: 10.1016/j.physbeh.2011.04.061
33. Mennella JA. Ontogeny of taste preferences: basic biology and implications for health. Am J Clin Nutr. (2014) 99:704–11. doi: 10.3945/ajcn.113.067694
34. Ventura AK, Worobey J. Early influences on the development of food preferences. Curr Biol. (2013) 23:R401–8. doi: 10.1016/j.cub.2013.02.037
35. Nicklaus S, Boggio V, Chabanet C, Issanchou S. A prospective study of food preferences in childhood. Food Qual Prefer. (2004) 15:805–18. doi: 10.1016/j.foodqual.2004.02.010
36. Nicklaus S, Remy E. Early Origins of overeating: tracking between early food habits and later eating patterns. Curr Obes Rep. (2013) 2:179–84. doi: 10.1007/s13679-013-0055-x
37. Nicklaus S. Relationships between early flavor exposure, and food acceptability and neophobia. In: Etiévant P, Guichard E, Salles C, Voilley A editors. Flavor: From Food to Behaviors, Wellbeing and Health. (Cambridge: Elsevier) (2016). p. 293–311. doi: 10.1016/b978-0-08-100295-7.00014-1
38. Schwartz C, Issanchou S, Nicklaus S. Developmental changes in the acceptance of the five basic tastes in the first year of life. Br J Nutr. (2009) 102:1375–85. doi: 10.1017/S0007114509990286
39. Nicklaus S. Children’s acceptance of new foods at weaning. Role of practices of weaning and of food sensory properties. Appetite. (2011) 57:812–5. doi: 10.1016/j.appet.2011.05.321
40. Nicklaus S, Demonteil L, Tournier C. Modifying the Texture of Foods for Infants and Young Children. Amsterdam: Elsevier Ltd (2015). doi: 10.1016/B978-1-78242-334-8.00008-0
41. Stein LJ, Cowart BJ, Beauchamp GK. The development of salty taste acceptance is related to dietary experience in human infants: a prospective study. Am J Clin Nutr. (2012) 95:123–9. doi: 10.3945/ajcn.111.014282
42. Fidler Mis N, Braegger C, Bronsky J, Campoy C, Domellöf M, Embleton ND, et al. Sugar in infants, children and adolescents: a position paper of the european society for paediatric gastroenterology, hepatology and nutrition committee on nutrition. J Pediatr Gastroenterol Nutr. (2017) 65:681–96. doi: 10.1097/MPG.0000000000001733
43. Fardet A. New hypotheses for the health-protective mechanisms of whole-grain cereals: what is beyond fibre? Nutr Res Rev. (2010) 23:65–134. doi: 10.1017/S0954422410000041
44. Cereals & Grains Association.Proposed Definition of Whole Grain as Food Ingredient. Saint Paul, MN: Cereals & Grains Association (2022).
45. Liu RH. Whole grain phytochemicals and health. J Cereal Sci. (2007) 46:207–19. doi: 10.1016/j.jcs.2007.06.010
46. American Heart Association [AHA].Dietary Recommendations for Healthy Children. Dallas, TX: American Heart Association (AHA) (2018).
47. U.S. Department of Agriculture, U.S. Department of Health and Human Services.Dietary Guidelines for Americans 2020-2025. Washington DC: U.S. Department of Agriculture (2020).
48. National Health and Medical Research Council.A Modelling System to Inform the Revision of the Australian Guide to Healthy Eating. Canberra, CAN: National Health and Medical Research Council (2011).
49. Varea Calderón V, Dalmau Serra J, Lama More R, Leis Trabazo R. Papel de los cereales en la alimentación infantil. Acta Pediatr España. (2013) 71: 91–8.
50. European Commission.Feeding Infants and Young Children, A Compilation of National Food-Based Dietary Guidelines and Specific Products Available in the EU Market. Brussels: European Commission (2019).
51. Garcia AL, McLean K, Wright CM. Types of fruits and vegetables used in commercial baby foods and their contribution to sugar content. Matern Child Nutr. (2016) 12:838–47. doi: 10.1111/mcn.12208
52. Rito AI, Dinis A, Rascôa C, Maia A, De Carvalho I, Mariana M, et al. Improving breakfast patterns of portuguese children — an evaluation of ready-to-eat cereals according to the European nutrient profile model. Eur J Clin Nutr. (2019) 73:465–73. doi: 10.1038/s41430-018-0235-6
53. Theurich MA, Koletzko B, Grote V. Nutritional adequacy of commercial complementary cereals in Germany. Nutrients. (2020) 12:1590. doi: 10.3390/nu12061590
54. Regulation (EC) No 1924/2006. Regulation (EC) No 1924/2006 of the European parliament and of the council of 20 December 2006 on nutrition and health claims made on foods. Off J Eur Union. (2007) 2007:3–18. doi: 10.2147/JPR.S160660
55. Madrelle J, Lange C, Boutrolle I, Valade O, Weenen H, Monnery-patris S, et al. Development of a new in-home testing method to assess infant food liking. Appetite. (2017) 113:274–83. doi: 10.1016/j.appet.2017.03.002
56. Gerrish CJ, Mennella JA. Flavor variety enhances food acceptance in formula-fed infants. Am J Clin Nutr. (2001) 73:1080–5. doi: 10.1093/ajcn/73.6.1080
57. Haro-Vicente JF, Bernal-Cava MJ, Lopez-Fernandez A, Ros-Berruezo G, Bodenstab S, Sanchez-Siles LM. Sensory acceptability of infant cereals with whole grain in infants and young children. Nutrients. (2017) 9:65. doi: 10.3390/nu9010065
58. Lange C, Visalli M, Jacob S, Chabanet C, Schlich P, Nicklaus S. Maternal feeding practices during the first year and their impact on infants’ acceptance of complementary food. Food Qual Prefer. (2013) 29:89–98. doi: 10.1016/j.foodqual.2013.03.005
59. Maier A, Chabanet C, Schaal B, Issanchou S, Leathwood P. Effects of repeated exposure on acceptance of initially disliked vegetables in 7-month old infants. Food Qual Prefer. (2007) 18:1023–32. doi: 10.1016/j.foodqual.2007.04.005
60. Remy E, Issanchou S, Chabanet C, Nicklaus S. Repeated exposure of infants at complementary feeding to a vegetable puàee increases acceptance as effectively as flavor-flavor learning and more effectively than flavor-nutrient learning. J Nutr. (2013) 143:1194–200. doi: 10.3945/jn.113.175646
61. Forestell CA, Mennella JA. Early determinants of fruit and vegetable acceptance. Pediatrics. (2007) 120:1247–54. doi: 10.1542/peds.2007-0858
62. Komninou S, Halford JCG, Harrold JA. Differences in parental feeding styles and practices and toddler eating behaviour across complementary feeding methods: managing expectations through consideration of effect size. Appetite. (2019) 137:198–206. doi: 10.1016/j.appet.2019.03.001
63. Román S, Sánchez-Siles LM. Parents’ choice criteria for infant food brands: a scale development and validation. Food Qual Prefer. (2018) 64:1–10. doi: 10.1016/j.foodqual.2017.10.008
64. Kuang L, Burgess B, Cuite CL, Tepper BJ, Hallman WK. Sensory acceptability and willingness to buy foods presented as having benefits achieved through the use of nanotechnology. Food Qual Prefer. (2020) 83:103922. doi: 10.1016/j.foodqual.2020.103922
65. Klerks M, Roman S, Bernal MJ, Haro-Vicente JF, Sanchez-Siles LM. Complementary feeding practices and parental pressure to eat among spanish infants and toddlers: a cross-sectional study. Int J Environ Res Public Health. (2021) 18:1982. doi: 10.3390/ijerph18041982
66. De Cosmi V, Scaglioni S, Agostoni C. Early taste experiences and later food choices. Nutrients. (2017) 9:107. doi: 10.3390/nu9020107
67. Donovan SMO, Murray DM, Hourihane JOB, Kenny LC, Irvine AD, Kiely M. Adherence with early infant feeding and complementary feeding guidelines in the cork BASELINE birth cohort study. Public Health Nutr. (2015) 18:2864–73. doi: 10.1017/S136898001500018X
68. Friel JK, Isaak CA, Hanning R, Miller A. Complementary food consumption of Canadian infants. Open Nutr J. (2009) 3:11–6. doi: 10.2174/1874288200903010011
69. McAndrew F, Thompson J, Fellows L, Large A, Speed M, Renfrew MJ. Infant Feeding Survey 2010. London: NHS health and social care information centre (2012).
70. European Commission.Farm to Fork Strategy: For a fair, Healthy and Environmentally-Friendly Food System. Brussels: European Commission (2020).
71. Willett W, Rockström J, Loken B, Springmann M, Lang T, Vermeulen S, et al. Food in the anthropocene: the EAT–lancet commission on healthy diets from sustainable food systems. Lancet. (2019) 393:447–92. doi: 10.1016/S0140-6736(18)31788-4
72. World Health Organization.Sustainable Healthy Diets: Guiding Principles. Geneva: World Health Organization (2019).
73. Román S, Sánchez-Siles LM, Siegrist M. The importance of food naturalness for consumers: Results of a systematic review. Trends Food Sci Technol. (2017) 67:44–57. doi: 10.1016/j.tifs.2017.06.010
74. Sanchez-Siles LM, Michel F, Román S, Bernal MJ, Philipsen B, Haro JF, et al. The food naturalness index (FNI): An integrative tool to measure the degree of food naturalness. Trends Food Sci Technol. (2019) 91:681–90. doi: 10.1016/j.tifs.2019.07.015
75. Edmonds WA, Kennedy TD. Between-subjects approach. An Applied Guide to Research Designs: Quantitative, Qualitative, and Mixed Methods. (Los Angeles, CA: Sage Publications) (2019).
76. Goldfein KR, Slavin JL. Why sugar is added to food: food science 101. Compr Rev Food Sci Food Saf. (2015) 14:644–56. doi: 10.1111/1541-4337.12151
Keywords: sensory acceptability, sugar reduction, cereals, complementary feeding, whole grains, public health
Citation: Sanchez-Siles L, Román S, Haro-Vicente JF, Bernal MJ, Klerks M, Ros G and Gil Á (2022) Less Sugar and More Whole Grains in Infant Cereals: A Sensory Acceptability Experiment With Infants and Their Parents. Front. Nutr. 9:855004. doi: 10.3389/fnut.2022.855004
Received: 14 January 2022; Accepted: 07 April 2022;
Published: 13 May 2022.
Edited by:
Adriana Arisseto, State University of Campinas, BrazilReviewed by:
Francis Kweku Amagloh, University for Development Studies, GhanaCopyright © 2022 Sanchez-Siles, Román, Haro-Vicente, Bernal, Klerks, Ros and Gil. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luisma Sanchez-Siles, luisma.sanchez@hero.es
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.