
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr. , 15 March 2022
Sec. Clinical Nutrition
Volume 9 - 2022 | https://doi.org/10.3389/fnut.2022.824193
 Bingwei Ma1,2†
Bingwei Ma1,2† Peng Yang1,3†
Peng Yang1,3† Jingyang Gao1,3†Lei Du1Chunjun Sheng1,3Taofeek Usman4
Jingyang Gao1,3†Lei Du1Chunjun Sheng1,3Taofeek Usman4 Xingchun Wang1,3*
Xingchun Wang1,3* Shen Qu1,3*
Shen Qu1,3*Vitamin A deficiency (VAD) occurs in obesity and may be associated with thyroid dysfunction. We aimed to investigate the association of VA with thyroid function in obesity and after laparoscopic sleeve gastrectomy (LSG). Nine hundred and seventy-six obese subjects were enrolled for this study and were divided into VAD, marginal vitamin A deficiency (MVAD), and vitamin A normal (NVA) groups. VAD was defined as VA ≤ 200 ng/ml, MVAD was defined as VA > 200 but <300 ng/ml, and NVA was defined as VA ≥ 300 ng/ml. Thyroid function was compared among groups and the relationship of VA and thyroid function was analyzed. Two hundred and forty-four of the 976 obese subjects underwent LSG, and the change in thyroid function and VA at 3, 6, and 12 months after surgery was measured. Results showed that 37% of all the subjects had subclinical hypothyroidism (SH), and the SH group had lower VA levels than the non-SH group (P = 0.008). Forty-nine percent of all the subjects had MVAD, 9% had VAD, while the MVAD or VAD group had lower FT4 than the NVA group (P = 0.005 and P = 0.001). The VAD group also had higher TSH than NVA group (P = 0.037). VA was significantly negatively associated with TSH (r = −0.151, P = 0.006) and positively associated with FT4 (r = 0.228, P < 0.001). TSH was significantly decreased at 3, 6, and 12 months (3M: from 4.43 ± 2.70 to 2.63 ± 1.46 mU/l, P < 0.001; 6M: from 4.43 ± 2.70 to 3.84 ± 2.34 mU/l, P = 0.041; 12M: from 4.43 ± 2.70 to 2.85 ± 1.68 mU/l, P = 0.024). After LSG surgery, VA levels were slightly increased, when compared to pre-surgery levels, at 3, 6, and 12 months (3M: from 262.57 ± 68.19 to 410.33 ± 76.55 ng/ml, P = 0.065; 6M: from 262.57 ± 68.19 to 281.36 ± 93.23 ng/ml, P = 0.343; 12M: from 262.57 ± 68.19 to 300.37 ± 86.03 ng/ml, P = 0.083). SH group also had lower TSH and higher VA than the non-SH group at 3 months post-surgery [TSH: −1.4(−2.3, −0.3) vs. −0.2(−0.8, −0.2) mU/l, P < 0.001; VA: 163.99 ± 32.58 vs. 121.69 ± 27.59 ng/ml, P = 0.044]. In conclusion VA, which is related to thyroid hormone production, protects against thyroid dysfunction in obese subjects. The improvement of thyroid function in subjects with SH after LSG may be related to the increased VA levels observed post-surgery.
Clinical Trial Registration: ClinicalTrial.gov ID: NCT04548232.
With changes in human lifestyle and environment, the prevalence of obesity is increasing as caloric intake in excess of caloric expenditure leads to a positive energy balance, obesogenic environment, and expression of genetic factors associated with poor nutrition (1). Obese individuals are predisposed to glucose and lipid disorders as well as vitamin deficiency (2). Most vitamins are deficient in obese individuals, especially the fat-soluble vitamins which include vitamin A (VA) (2). VA, also defined as all-trans-retinol and plasma VA levels, were significantly lower in patients with metabolic syndrome (MS) than those without MS (3, 4). VA has some influence on energy metabolism as it has been reported that rats fed a VA deficient diet exhibit increased adiposity and weight gain (5, 6).
Obesity has been significantly related to thyroid hormone dysfunction (7, 8). The metabolism of thyroid hormone requires iodine but is also influenced by micronutrients such as VA (9). VA regulates thyroid gland metabolism, the synthesis of thyroid hormone, the peripheral function of thyroid hormone as well as the secretion of thyroid stimulating hormone (TSH) by the pituitary (10, 11). Vitamin A deficiency (VAD) affects the synthesis of thyroglobulin, pairing of iodotyrosine residues to form T4 and T3 and reduces thyroid iodine uptake (10, 11), while VA supplementation reduced thyroid stimulation by thyrotropin and decreased the rate of goiter (12). However, no study focuses on the association of VA and thyroid dysfunction in obese individuals.
Laparoscopic sleeve gastrectomy (LSG) is one of the most effective methods to treat obesity as it not only led to decreased bodyweight but also improved metabolism (13–15). The effects of LSG on VA levels are inconsistent. One study indicated that VA levels were decreased after SG and gastric bypass (RYGB) (16). Another study pointed out that VAD was observed in 9.4% of SG and 15.9% of RYGB within 1-year post-operation and 5.2% of SG, and 7.7% of RYGB after 1 year (17). Another study showed no influence of bariatric surgery on serum VA levels (18). As to thyroid function, the consensus view is that LSG may improve thyroid function (19, 20).
Overall, the mechanism of VA on thyroid hormones remains unclear and few studies have investigated the association of VA and thyroid hormones in obesity. Therefore, we carried out a study to clarify the relationship between VA and thyroid hormones and the changes in VA and thyroid function after LSG.
This study enrolled 976 subjects with obesity. The definition of obesity is body mass index (BMI) ≥ 30 kg/m2 (21). They were divided into subclinical hypothyroidism (SH) group (TSH over 2.5 mU/l) and normal thyroid group depending on the TSH levels (8, 22, 23). VAD was defined as VA ≤ 200 ng/ml (24, 25), marginal vitamin A deficiency (MVAD) was defined as VA > 200 ng/ml but <300 ng/ml, and vitamin A normal (NVA) was defined as VA ≥ 300 ng/ml. Among them, 244 obese subjects underwent LSG. The inclusion criteria were as follows: (1) aged over 16 and <65 years old, (2) BMI ≥ 37.5 kg/m2, or BMI ≥ 37.5 kg/m2 complicated with type 2 diabetes (T2DM). The exclusion criteria including (1) secondary obesity including hypothalamus obesity, Cushing syndrome, etc., (2) Pregnant or lactating women, (3) contraindications of laparoscopic surgery, such as intra-abdominal infection and adhesion, gastrointestinal diseases, (4) serious heart, liver, and kidney failure which is intolerance to surgery. Assessments were taken at baseline and follow up measurements were taken at 3, 6, 12 months after surgery. The flowchart is as shown in Figure 1. All subjects enrolled did not receive VA supplement or any other intervention after surgery. All subjects enrolled were evaluated by an endocrinologist for thyroid function and vitamin A levels and assessed for compliance with enrollment criteria. The experimental scheme was approved by the Ethics Committee of local hospital and all subjects enrolled in this study signed the informed consent form.
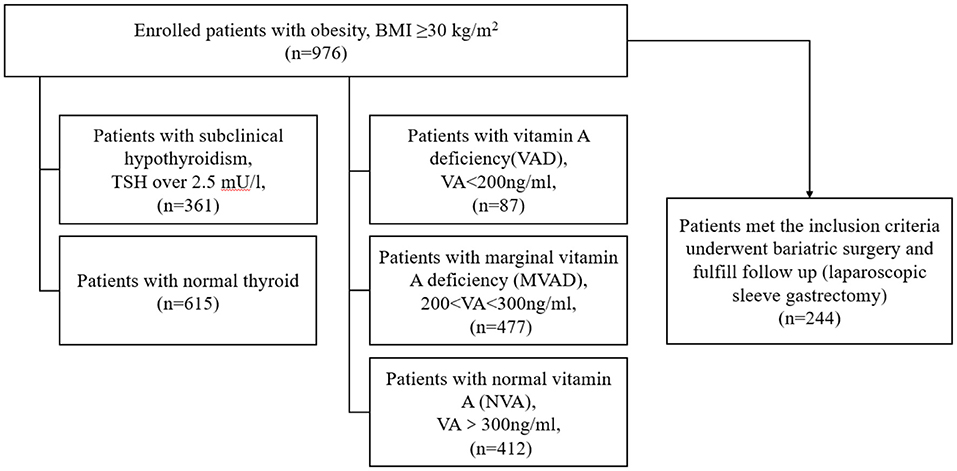
Figure 1. Flowchart of grouping and enrollment in this study.
Variables including age and gender were recorded. Anthropometric measurements including height and body weight were measured by professional staff and BMI was calculated by the following formula: body mass index (BMI) = body weight (kg)/height (m)2. Subjects were asked to fast for over 8 h before venous blood was collected among them. All the anthropometric and laboratory measurements were measured at baseline and follow up at 3, 6, 12 months after surgery. Laboratory measurements of glucose metabolism included fasting plasma glucose (FPG) and fasting insulin (FINS). FPG was measured by Roche Cobas c 701 fully automatic biochemical analyzer and FINS was measured by Roche Cobas e 601 analyzer. Homeostasis model assessment of insulin resistance (HOMA-IR) which was calculated to assess the insulin resistance by the following formula: FINS (uIU/ml) × FBG (mmol/l)/22.5 (26, 27). Lipid metabolic markers including total cholesterol (TCH), triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and free fatty acid (FFA) were also measured with Roche Cobas c 701 fully automatic biochemical analyzer. Thyroid hormones including free triiodothyronine (FT3), free thyroxine (FT4), total thyroxine (TT3), total triiodothyronine (TT4), and TSH were tested to assess the thyroid function by ADVIA Centaur XP Immunoassay System. Serum vitamin A levels were determined using isotope dilution ultra-high-performance liquid chromatography-tandem mass spectrometry (ID-UPLC-MSMS).
Data of this study were statistically analyzed by SPSS software (Version 20.0). Normal distribution of data was also evaluated. If the continuous data were normally distributed, they were expressed as mean ± standard deviation (X ± SD). Otherwise, continuous data non-normally distributed was expressed as medians (interquartile ranges, IQR). Categorical variables were presented as numbers or percent. The normally distributed data were compared using an independent sample t-test, and non-normally distributed data were compared with the Mann & Whitney U-test. Pearson's or Spearman's test depended on the data normally distributed to investigate the correlations between thyroid hormone and other markers. A paired two-tailed t-test was adopted when comparing the data before and after surgery. A P < 0.05 was considered statistically significant.
Thirty-seven percent of all participants in this study had SH and this group had lower VA than the non-SH participants (275.90 ± 77.71 vs. 303.37 ± 97.37 ng/ml, P = 0.008) as presented in Figure 2. Forty-nine percent of the participants had MVAD while 9% had VAD. The MVAD or VAD group of participants had lower FT4 than NVA group (P = 0.005 and P = 0.001). Meanwhile, VAD group had significantly higher TSH levels than NVA group [2.20 (1.85, 3.90) vs. 1.90 (1.20, 2.90) mU/l, P = 0.037; Figure 3]. Additionally, FPG, FINS, and HOMA-IR were significantly higher while HDL-C was significantly lower in the VAD group than the NVA group (P < 0.05; Table 1).
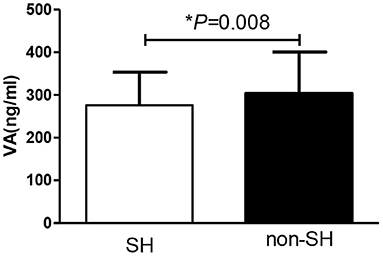
Figure 2. Comparison of VA levels between obese patients with or without SH.
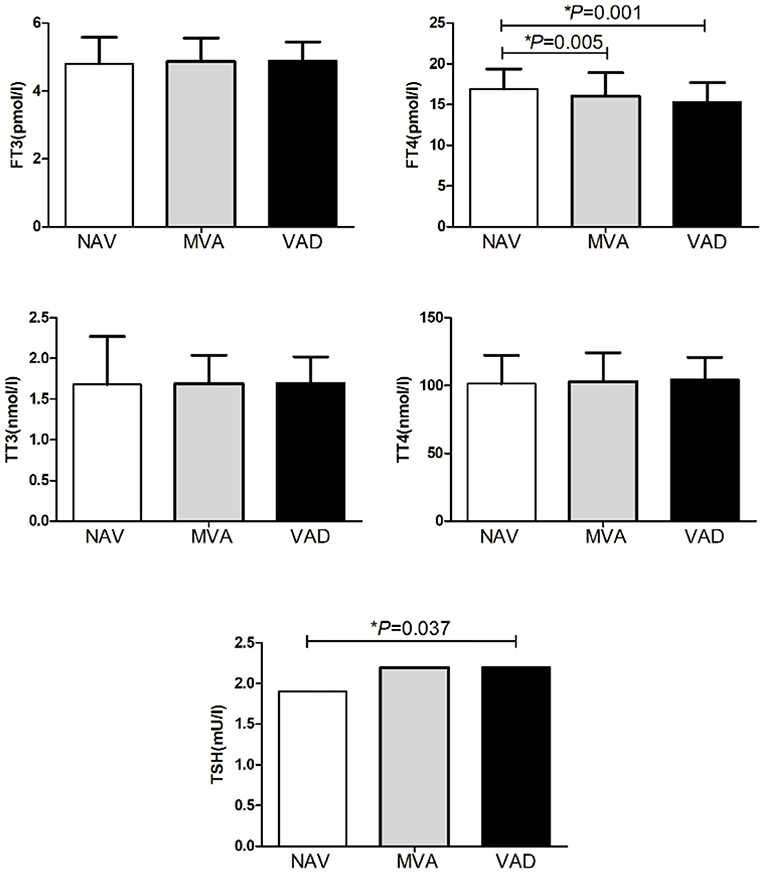
Figure 3. Comparison of thyroid hormone among obese patients with different degree of VA.
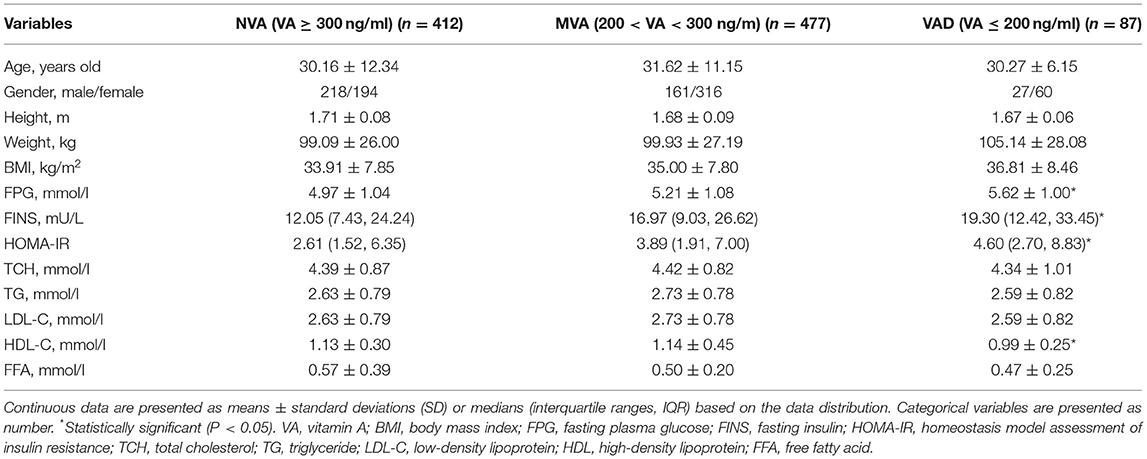
Table 1. Comparison of metabolism among patients with different degree of VA.
VA levels were significantly negatively associated with TSH (r = −0.151, P = 0.006) while positively associated with FT4 (r = 0.228, P < 0.001). Additionally, VA levels were significantly negatively associated with FPG (r = −0.188, P < 0.001) and positively associated with FFA (r = 0.124, P = 0.022). Adjusted for FFA and FPG, VA levels were still positively associated with FT4 (r = 0.150, P = 0.008; Table 2). Further regression analysis showed that FT4 was also significantly associated with VA levels (β = 18.238, P = 0.007) as in Table 3.
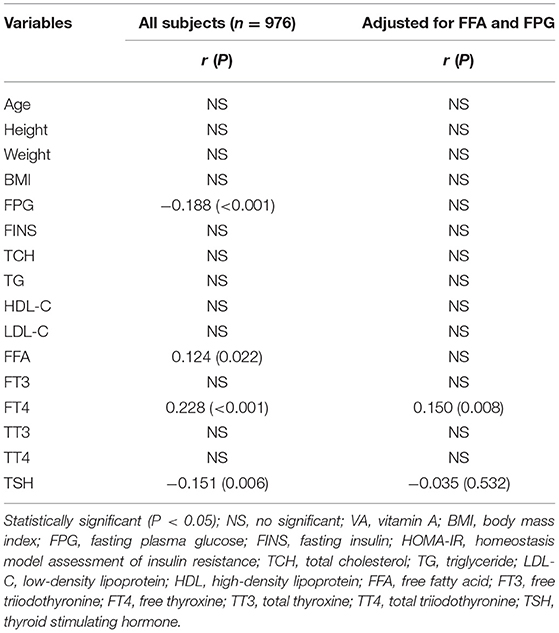
Table 2. Association of VA and thyroid function.
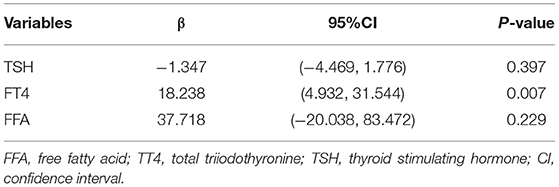
Table 3. Regression analysis of VA and thyroid function.
LSG led to significantly decreased body weight and improved glucose-lipid metabolism at 3, 6, and 12 months after surgery (P < 0.05; Table 4). Additionally, thyroid function was improved as TSH, FT3, and TT3 was significantly decreased at 3, 6, and 12 months after surgery (all P < 0.05). FT4 at 3 months, and TT4 at 6 and 12 months were significantly decreased after surgery as shown in Figure 4. Additionally, change in TSH at 6 months was positively associated with the change in BMI (r = 0.284, P = 0.026).
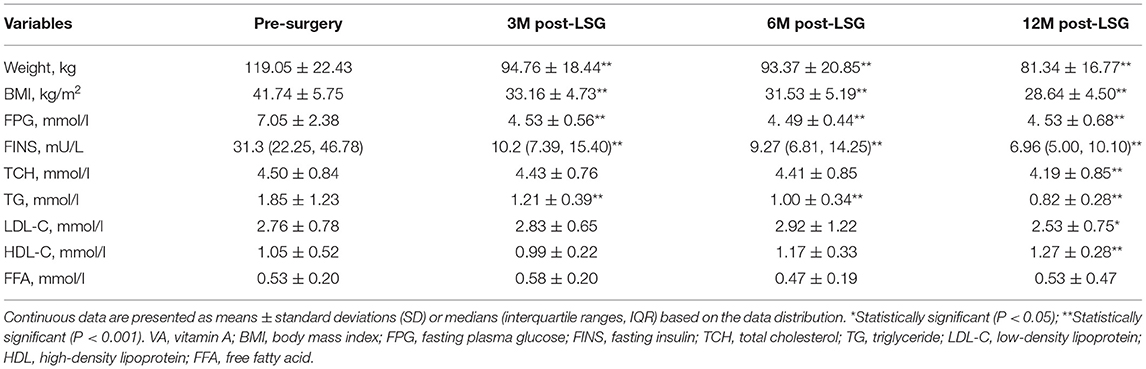
Table 4. Change in metabolic marker follow up 3, 6 month and 12 months post-operation.
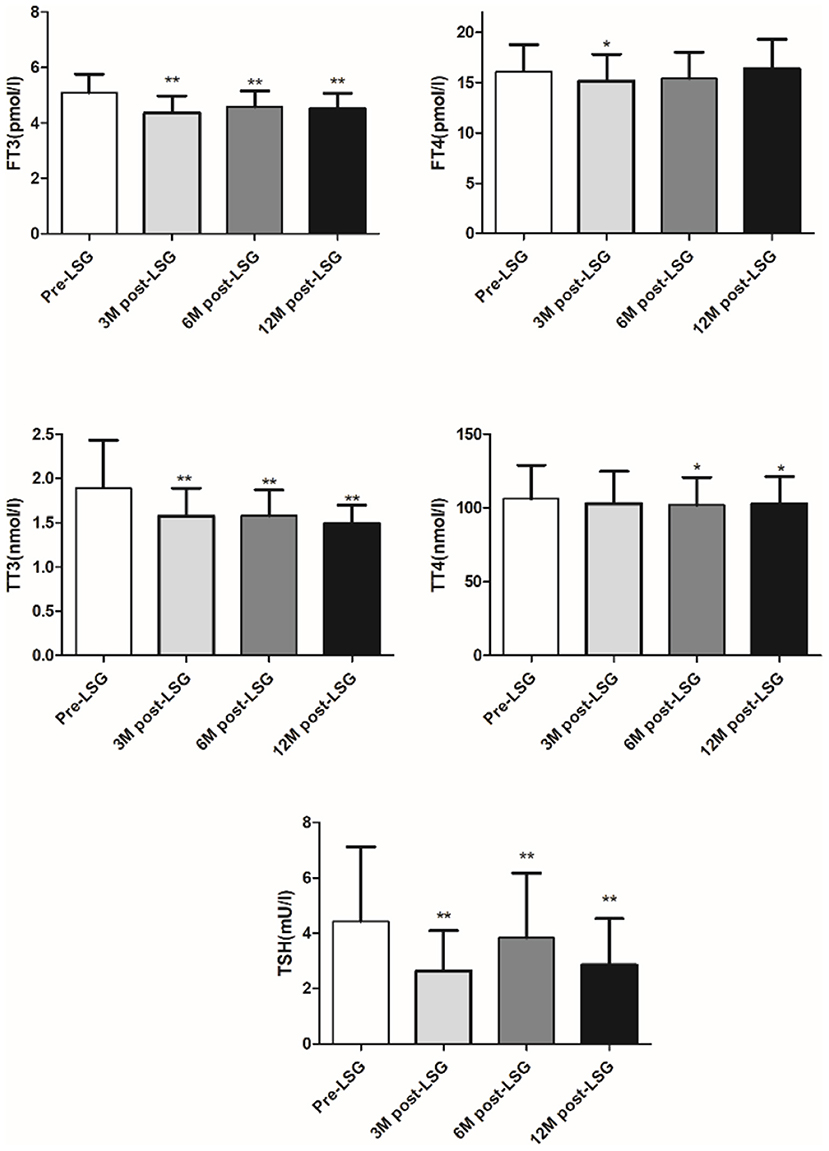
Figure 4. Change in thyroid hormone after LSG. *P < 0.05, **P < 0.001.
VA levels were slightly increased after LSG at 3, 6, and 12 months (3M: from 262.57 ± 68.19 to 410.33 ± 76.55 ng/ml, P = 0.065; 6M: from 262.57 ± 68.19 to 281.36 ± 93.23 ng/ml, P = 0.343; 12M: from 262.57 ± 68.19 to 300.37 ± 86.03 ng/ml, P = 0.083) but these changes were not statistically significant as presented in Figure 5. The SH group had a lower TSH and higher VA than the non-SH group at 3 months [TSH: −1.4 (−2.3, −0.3) vs. −0.2(−0.8, −0.2) mU/l, P < 0.001; VA: 163.99 ± 121.69 vs. 32.58 ± 27.59 ng/ml, P = 0.044] as presented in Figure 6.
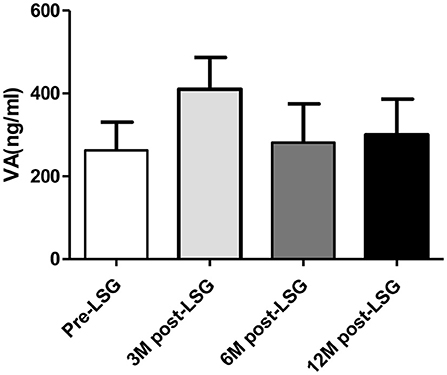
Figure 5. Change in VA levels after LSG.
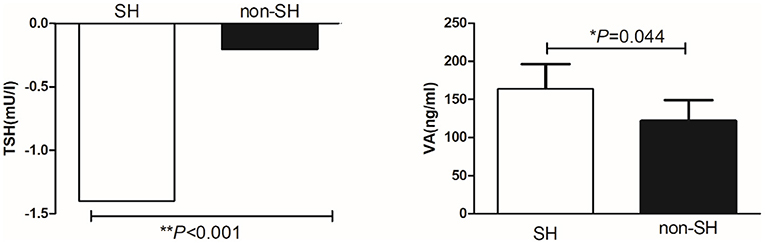
Figure 6. Comparison of change in TSH and VA between obese patients with or without SH.
Obesity affects 27.5% of adults and 47.1% of children worldwide (28). Comorbidities associated with obesity include metabolic disorders as well as thyroid dysfunction and vitamin deficiency (2, 29). VAD affects over 30% of the global population, as well as the obese (10). VAD among school-age children in Chongqing, China was found to be significantly associated with obesity (30). VAD may also aggravate the pathological state of obesity (2). In our study, 37% of the enrolled subjects with obesity had SH. MVAD occurred in 49% of the included subjects with obesity and VAD occurred in 9% of the included subjects with obesity. However, few studies investigated the association of VA and thyroid function in an obese population. Therefore, we inferred that VA and thyroid disorders, which are common in obese subjects, may crosstalk with each other and that formed the basis of this study.
Synthesis and metabolism of thyroid hormones involve iodine, enzymes, and proteins and are also influenced by micronutrients and vitamins (9). VA takes part in the uptake of iodine while its deficiency impairs the synthesis of thyroglobulin and reduces the uptake of thyroidal iodine (31, 32). Animals studies also found that thyroid of VA deficient rats took up less radioiodide than thyroid of control rats (32). Thyroid hormone synthesis was decreased in the VA-deficient rats (11), and the thyroid weight of VA deficient rats was increased and the level serum thyroxine levels of VA deficient rats was decreased to one-half that of the control rats (11). Our study found that obese subjects with SH had lower VA than obese subjects with normal thyroid function. Obese subjects with MVAD or VAD had lower FT4 than obese subjects with NVA. Additionally, obese subjects with VAD had higher TSH levels than obese subjects with NVA. VA levels were significantly negatively associated with TSH while positively associated with FT4. Logistic regression analysis of risk factors for SH found that VA was a protective factor for SH. We inferred that VA and thyroid function interacted with each other in subjects with obesity and adequate VA may reduce the risk for hypothyroidism in obese subjects.
Bariatric surgery is one of the most effective methods to reduce body weight as well as improve metabolism (13–15). However, findings regarding change in VA after bariatric surgery has been inconclusive. Decreased VA micronutrient was observed after bariatric surgery including SG and RYGB (16). One study pointed out that VAD was uncommon preoperatively (2.7% SG vs. 1.7% RYGB) but increased after surgery (9.4% SG vs. 15.9% RYGB within 1 year post-operation, and 5.2% SG vs. 7.7% RYGB after 1 year) (17). However, another study found that there was no influence of bariatric surgery on serum VA levels (18). Our study found that VA levels were not decreased at 3, 6, and 12 months after LSG but were slightly increased. We inferred it may due to the ethnic differences and the choice of different types of operations. As we know, LSG led to a smaller risk for nutritional deficiencies while gastric bypass procedures are related to increased nutritional deficiencies because this kind of procedure is more complex which changes the gastrointestinal anatomy (33). On another hand, elevated C-reactive protein (CRP) concentration was associated with lower VA concentrations in morbidly obese subjects (34). LSG has effects on reducing body weight, improving metabolism and chronic low-grade inflammation with decreasing CRP (35). Therefore, the effect of improved metabolism and reduced CRP caused by LSG on VA may have counteracted the effects of surgery itself. LSG may therefore have no adverse effect on VA levels in Chinese subjects with obesity according to our findings.
A systematic review and meta-analysis proved that TSH, FT3, and TT3 were decreased, with non-significant changes in TT4, FT4, and rT3 levels after bariatric surgery (19). Serve obesity may be characterized by a mild reversible central resistance to thyroid hormones. Thyroid hormone resistance caused by obesity may occur through a mechanism similar to that of insulin resistance which could explain the increase in TSH similar to that observed in hyperinsulinemia (20). In our study, thyroid function was improved significantly at 3, 6, and 12 months after surgery. Also, FT3, TT3, and TT4 were decreased significantly after surgery. These results may also indicate that LSG has effects on improving thyroid hormone resistance in subjects with obesity although the underlying mechanism needs further experimental investigation.
Additionally, an animal study showed that VAD caused the reduction of the β-cell mass in the fetal pancreas and may contribute to glucose intolerance in adult rats (36). VA levels were compared in 191 subjects with MS and 98 subjects without MS, the results found that VA was significantly lower in subjects with MS than in healthy subjects (4). Also, the OR (95% confidence intervals) for MS is 0.942 (0.901–0.985) with a two-fold increase in total VA intake in women indicating decreases of 5.8% risk for MS (16). Our study showed that FPG, FINS, and HOMA-IR were significantly higher in VAD obese subjects than NVA obese subjects and VA levels were significantly negatively associated with FPG. VA may also have effects on lipid metabolism. HDL-C levels were found lower in subjects with VAD when compared to subjects with normal VA levels (4). VAD among school-age children in Chongqing, China has been reported to be significantly associated with hypertriglyceridemia (30). Our study also showed that HDL-C was significantly lower in VAD than in NVA subjects with obesity. Overall, VAD may also play a role in glucose-lipid metabolism but the underlying mechanism needs further exploration.
Our study clarified the association of VA and thyroid hormone in obese individuals before and after LSG. However, there also some limitations of our study. Firstly, the sample size is relatively smaller, and we did not compare the effects of different bariatric surgery on thyroid function and VA. Secondly, the follow-up time is relatively short, and we did not add the group with VA supplement. We will further expand the sample size, extend the follow-up time and add VA intervention to better understand the association of VA and thyroid hormone in obesity. Additionally, animal experiments can be undertaken to explore the underlying mechanism.
VAD and SH are common in subjects with obesity. A crosstalk exists between VA and thyroid function as decreased VA in obese subjects was significantly related to thyroid dysfunction. Adequate VA levels may be a protective factor for thyroid function in obese subjects. Improved thyroid function was also observed after LSG and the improvement of thyroid function in obese subjects with subclinical hypothyroidism after LSG may be related to the increased VA levels observed in them.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Shanghai Tenth People's Hospital. The patients/participants provided their written informed consent to participate in this study.
SQ and XW made substantial contribution to the conception and design of the work. BM contributed to the data acquisition and draft manuscript. PY contributed to the analysis. JG contributed to the interpretation. LD helped in drafting the article. CS revised it critically for important intellectual content. TU revised the language. All authors gave the final approval of the version to be published and agreed for the accuracy or integrity of any part of the work.
This research was supported by the Climbing Talent Program of Shanghai Tenth People's Hospital (2021SYPDRC047).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Hill JO. Understanding and addressing the epidemic of obesity: an energy balance perspective. Endocr Rev. (2006) 27:750–61. doi: 10.1210/er.2006-0032
2. Thomas-Valdes S, Tostes M, Anunciacao PC, da Silva BP, Sant'Ana HMP. Association between vitamin deficiency and metabolic disorders related to obesity. Crit Rev Food Sci Nutr. (2017) 57:3332–43. doi: 10.1080/10408398.2015.1117413
3. Blaner WS. Vitamin A signaling and homeostasis in obesity, diabetes, and metabolic disorders. Pharmacol Ther. (2019) 197:153–78. doi: 10.1016/j.pharmthera.2019.01.006
4. Godala M, Materek-Kusmierkiewicz I, Moczulski D, Rutkowski M, Szatko F, Gaszynska E, et al. The risk of plasma vitamin A, C, E and D deficiency in patients with metabolic syndrome: a case-control study. Adv Clin Exp Med. (2017) 26:581–86. doi: 10.17219/acem/62453
5. Ribot J, Felipe F, Bonet ML, Palou A. Changes of adiposity in response to vitamin A status correlate with changes of PPAR gamma 2 expression. Obes Res. (2001) 9:500–9. doi: 10.1038/oby.2001.65
6. Bonet ML, Oliver J, Pico C, Felipe F, Ribot J, Cinti S, et al. Opposite effects of feeding a vitamin A-deficient diet and retinoic acid treatment on brown adipose tissue uncoupling protein 1 (UCP1), UCP2 and leptin expression. J Endocrinol. (2000) 166:511–7. doi: 10.1677/joe.0.1660511
7. Song RH, Wang B, Yao QM Li Q, Jia X, Zhang JA. The impact of obesity on thyroid autoimmunity and dysfunction: a systematic review and meta-analysis. Front Immunol. (2019) 10:2349. doi: 10.3389/fimmu.2019.02349
8. Wang X, Liu H, Chen J, Huang Y, Li L, Rampersad S, et al. Metabolic characteristics in obese patients complicated by mild thyroid hormone deficiency. Horm Metab Res. (2016) 48:331–7. doi: 10.1055/s-0042-105150
9. O'Kane SM, Mulhern MS, Pourshahidi LK, Strain JJ, Yeates AJ. Micronutrients, iodine status and concentrations of thyroid hormones: a systematic review. Nutr Rev. (2018) 76:418–31. doi: 10.1093/nutrit/nuy008
10. Zimmermann MB. Interactions of vitamin A and iodine deficiencies: effects on the pituitary-thyroid axis. Int J Vitam Nutr Res. (2007) 77:236–40. doi: 10.1024/0300-9831.77.3.236
11. Oba K, Kimura S. Effects of vitamin A deficiency on thyroid function and serum thyroxine levels in the rat. J Nutr Sci Vitaminol. (1980) 26:327–34. doi: 10.3177/jnsv.26.327
12. Zimmermann MB, Jooste PL, Mabapa NS, Schoeman S, Biebinger R, Mushaphi LF, et al. Vitamin A supplementation in iodine-deficient African children decreases thyrotropin stimulation of the thyroid and reduces the goiter rate. Am J Clin Nutr. (2007) 86:1040–44. doi: 10.1093/ajcn/86.4.1040
13. Wang X, Huang Y, Gao J, Sun H, Jayachandran M, Qu S. Changes of serum retinol-binding protein 4 associated with improved insulin resistance after laparoscopic sleeve gastrectomy in Chinese obese patients. Diabetol Metab Syndr. (2020) 12:7. doi: 10.1186/s13098-019-0511-1
14. Ma B, Sun H, Zhu B, Wang S, Du L, Wang X, et al. Hepatic steatosis is associated with elevated serum iron in patients with obesity and improves after laparoscopic sleeve gastrectomy. Obes Facts. (2021) 14:64–71. doi: 10.1159/000511736
15. Wang X, Sun H, Ma B, Gao J, Yin J, Qu S. Insulin-like growth factor 1 related to chronic low-grade inflammation in patients with obesity and early change of its levels after laparoscopic sleeve gastrectomy. Obes Surg. (2020) 30:3326–32. doi: 10.1007/s11695-020-04473-9
16. Park S, Ham JO, Lee BK. Effects of total vitamin A, vitamin C, and fruit intake on risk for metabolic syndrome in Korean women and men. Nutrition. (2015) 31:111–8. doi: 10.1016/j.nut.2014.05.011
17. Johnson LM, Ikramuddin S, Leslie DB, Slusarek B, Killeen AA. Analysis of vitamin levels and deficiencies in bariatric surgery patients: a single-institutional analysis. Surg Obes Relat Dis. (2019) 15:1146–52. doi: 10.1016/j.soard.2019.04.028
18. Brandao LP, Vilar L, Cavalcanti BM, Brandao PH, Arantes TE, Campos JM. Serum levels of vitamin A, visual function and ocular surface after bariatric surgery. Arq Gastroenterol. (2017) 54:65–9. doi: 10.1590/s0004-2803.2017v54n1-13
19. Guan B, Chen Y, Yang J, Yang W, Wang C. Effect of bariatric surgery on thyroid function in obese patients: a systematic review and meta-analysis. Obes Surg. (2017) 27:3292–305. doi: 10.1007/s11695-017-2965-2
20. Gokosmanoglu F, Aksoy E, Onmez A, Ergenc H, Topkaya S. Thyroid homeostasis after bariatric surgery in obese cases. Obes Surg. (2020) 30:274–78. doi: 10.1007/s11695-019-04151-5
21. Engin A. The definition and prevalence of obesity and metabolic syndrome. Adv Exp Med Biol. (2017) 960:1–17. doi: 10.1007/978-3-319-48382-5_1
22. Spencer CA, Schwarzbein D, Guttler RB, LoPresti JS, Nicoloff JT. Thyrotropin (TSH)-releasing hormone stimulation test responses employing third and fourth generation TSH assays. J Clin Endocrinol Metab. (1993) 76:494–8. doi: 10.1210/jcem.76.2.8432796
23. Vanderpump MP, Tunbridge WM, French JM, Appleton D, Bates D, Clark F, et al. The incidence of thyroid disorders in the community: a twenty-year follow-up of the Whickham Survey. Clin Endocrinol. (1995) 43:55–68. doi: 10.1111/j.1365-2265.1995.tb01894.x
24. Zimmermann MB, Wegmuller R, Zeder C, Chaouki N, Torresani T. The effects of vitamin A deficiency and vitamin A supplementation on thyroid function in goitrous children. J Clin Endocrinol Metab. (2004) 89:5441–7. doi: 10.1210/jc.2004-0862
25. El-Zayat SR, Sibaii H, Mahfouz NN, Sallam SF, Fahmy RF, Abd El-Shaheed A. Effect of vitamin A deficiency on thymosin-beta4 and CD4 concentrations. J Genet Eng Biotechnol. (2018) 16:57–61. doi: 10.1016/j.jgeb.2017.10.007
26. Park SY, Gautier JF, Chon S. Assessment of insulin secretion and insulin resistance in human. Diabetes Metab J. (2021) 45:641–54. doi: 10.4093/dmj.2021.0220
27. Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. (1985) 28:412–9. doi: 10.1007/BF00280883
28. Apovian CM. Obesity: definition, comorbidities, causes, and burden. Am J Manag Care. (2016) 22(7 Suppl):s176–85.
29. Fontenelle LC, Feitosa MM, Severo JS, Freitas TE, Morais JB, Torres-Leal FL, et al. Thyroid function in human obesity: underlying mechanisms. Horm Metab Res. (2016) 48:787–94. doi: 10.1055/s-0042-121421
30. Wei X, Peng R, Cao J, Kang Y, Qu P, Liu Y, et al. Serum vitamin A status is associated with obesity and the metabolic syndrome among school-age children in Chongqing, China. Asia Pac J Clin Nutr. (2016) 25:563–70. doi: 10.6133/apjcn.092015.03
31. Wolf G. The regulation of the thyroid-stimulating hormone of the anterior pituitary gland by thyroid hormone and by 9-cis-retinoic acid. Nutr Rev. (2002) 60:374–7. doi: 10.1301/00296640260385919
32. Strum JM. Alterations within the rat thyroid gland during vitamin A deficiency. Am J Anat. (1979) 156:169–82. doi: 10.1002/aja.1001560202
33. Lange J, Konigsrainer A. Malnutrition as a complication of bariatric surgery - a clear and present danger? Visc Med. (2019) 35:305–11. doi: 10.1159/000503040
34. Aasheim ET, Hofso D, Hjelmesaeth J, Birkeland KI, Bohmer T. Vitamin status in morbidly obese patients: a cross-sectional study. Am J Clin Nutr. (2008) 87:362–9. doi: 10.1093/ajcn/87.2.362
35. Randell EW, Twells LK, Gregory DM, Lester KK, Daneshtalab N, Dillon C, et al. Pre-operative and post-operative changes in CRP and other biomarkers sensitive to inflammatory status in patients with severe obesity undergoing laparoscopic sleeve gastrectomy. Clin Biochem. (2018) 52:13–9. doi: 10.1016/j.clinbiochem.2017.10.010
Keywords: vitamin A, thyroid function, obesity, sleeve gastrectomy, subclinical hypothyroidism
Citation: Ma B, Yang P, Gao J, Du L, Sheng C, Usman T, Wang X and Qu S (2022) Relationship of Vitamin A and Thyroid Function in Individuals With Obesity and After Laparoscopic Sleeve Gastrectomy. Front. Nutr. 9:824193. doi: 10.3389/fnut.2022.824193
Received: 29 November 2021; Accepted: 14 February 2022;
Published: 15 March 2022.
Edited by:
Lidia Santarpia, University of Naples Federico II, ItalyReviewed by:
Andreas Alexandrou, National and Kapodistrian University of Athens, GreeceCopyright © 2022 Ma, Yang, Gao, Du, Sheng, Usman, Wang and Qu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shen Qu, cXVzaGVuY25AaG90bWFpbC5jb20=; Xingchun Wang, d2FuZ3gyOEB1cG1jLmVkdQ==
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.