 Sandra Wagner1,2*
Sandra Wagner1,2* Thomas Merkling1
Thomas Merkling1 Marie Metzger3
Marie Metzger3 Laetitia Koppe4,5
Laetitia Koppe4,5 Maurice Laville5Marie-Christine Boutron-Ruault6Luc Frimat7,8Christian Combe9,10Ziad A. Massy2,3,11Bénédicte Stengel2,3Denis Fouque4,5
Maurice Laville5Marie-Christine Boutron-Ruault6Luc Frimat7,8Christian Combe9,10Ziad A. Massy2,3,11Bénédicte Stengel2,3Denis Fouque4,5
- 1Université de Lorraine, INSERM CIC 1433, Nancy CHRU, Inserm U1116, Nancy, France
- 2FCRIN INI-CRCT, Nancy, France
- 3Centre de Recherche en Epidémiologie et Santé des Populations (CESP), Univ Paris-Saclay, UVSQ, INSERM, Equipe Epidémiologie Clinique, Villejuif, France
- 4Département de Néphrologie, Hopital Lyon Sud – HCL, Pierre-Bénite, France
- 5Université de Lyon, CarMeN Laboratory, INSA-Lyon, INSERM U1060, INRA, Université Claude Bernard Lyon 1, Villeurbanne, France
- 6Centre de Recherche en Epidémiologie et Santé des Populations (CESP), Université Paris-Saclay, UVSQ, INSERM, Gustave Roussy, Equipe Exposome-Hérédité, Villejuif, France
- 7EA4360 APEMAC, Université de Lorraine, Université Paris Descartes, Nancy, France
- 8Département de Néphrologie, CHU de Nancy, Vandoeuvre-lès-Nancy, France
- 9Service de Néphrologie-Transplantation-Dialyse-Aphérèse, Centre Hospitalier Universitaire de Bordeaux, Bordeaux, France
- 10INSERM, U1026, Université Bordeaux Segalen, Bordeaux, France
- 11Service de Néphrologie, Hôpital Ambroise Paré, APHP, Paris, France
Background and Aims: Little is known about the effects of probiotics on inflammation in the context of chronic kidney disease (CKD). We investigated the association between probiotic intake and inflammation in patients with moderate-to-advanced CKD.
Methods: We performed a cross-sectional study of 888 patients with stage 3–5 CKD and data on serum C-reactive protein (CRP) levels and a concomitant food frequency questionnaire. We estimated the odds ratios (ORs) [95% confidence interval (CI)] for various CRP thresholds (>3, >4, >5, >6, and >7 mg/L) associated with three intake categories (no yoghurt, ordinary yoghurt, and probiotics from yoghurts or dietary supplements) and two frequency categories (daily or less than daily).
Results: The 888 study participants (median age: 70; men: 65%) had a median estimated glomerular filtration rate of 28.6 mL/min/1.73 m2 and a median [interquartile range] CRP level of 3.0 [1.6, 7.0] mg/L. Fifty-seven percent consumed ordinary yoghurt and 30% consumed probiotic yoghurt. The median intake frequency for yoghurt and probiotics was 7 per week. Relative to participants not consuming yoghurt, the ORs [95% CI] for CRP > 6 or >7 mg/L were significantly lower for participants consuming ordinary yoghurt (0.58 [0.37, 0.93] and 0.57 [0.35, 0.91], respectively) and for participants consuming probiotics (0.54 [0.33, 0.9] and 0.48 [0.28, 0.81], respectively), independently of age, sex, body mass index, CKD stage, cardiovascular disease, and fibre, protein and total energy intakes. The ORs were not significantly lower for CRP thresholds >3, >4, and >5 mg/L and were not significantly greater in daily consumers than in occasional consumers.
Conclusion: We observed independent associations between the consumption of yoghurt or probiotics and lower levels of inflammation in patients with CKD. There was no evidence of a dose-effect relationship.
Clinical Trial Registration: [https://www.clinicaltrials.gov/ct2/show/NCT03381950], identifier [NCT03381950].
Introduction
Inflammation is a prominent feature of chronic kidney disease (CKD), which affects 10–15% of the population worldwide (1–4). Furthermore, inflammation is an established risk factor for early mortality and acts as a catalyst for the development of other complications, such as cardiovascular disease (CVD) (5). Although inflammation has many causes, gut dysbiosis (i.e., alteration of the intestinal microbiota) is now emerging as a key topic of interest (2, 6, 7).
Probiotic consumption appears to be a promising means of limiting dysbiosis and its harmful effects on health (8–10). Probiotics have been defined by the United Nations’ Food and Agriculture Organization (FAO) and the World Health Organization (WHO) as “live microorganisms that, when administrated in adequate amounts, confer a health benefit on the host” (11). Probiotics can modulate the composition of the intestinal microbiota, create a more favourable environment, and in principle reduce inflammation. Only a few clinical trials have focused on the effects of probiotics (e.g., dietary supplements) on inflammation in CKD, and the results have been inconsistent (12–17). In some studies of patients on dialysis, probiotic intake was associated with lower levels of pro-inflammatory cytokines, such as Tumour Necrosis Factor-α (TNF-α), Interleukins (IL-6, and IL-5), or C-reactive protein (CRP) and higher levels of anti-inflammatory cytokines (e.g., IL-10) (12–15). In contrast, other studies did not find any effects of probiotics on inflammatory markers (16, 17).
Although probiotic microorganisms can be specifically included in the diet as supplements, they are naturally present in food items such as yoghurts. The commercial use of the denomination “yoghurt” is strictly regulated: according to the FAO/WHO Codex Alimentarius, the milk must have been fermented by only two authorised bacterial strains (Lactobacillus delbrueckii subsp. bulgaricus and Streptococcus salivarius subsp. thermophilus), and the finished product must contain at least 10 million living bacterial organisms per g. The National Health and Nutrition Examination Survey (NHANES) investigated the association between probiotics/yoghurt intake and CKD; frequent intake was found to be associated with a lower likelihood of proteinuria (18). The NHANES did not, however, investigate levels of inflammation markers.
The primary objective of the present study was to investigate the associations of the intake of probiotic-containing yoghurt/dietary supplements or ordinary yoghurt with inflammation (as assessed by the serum CRP concentration) in patients with CKD stages 3–5. We also investigated the association between the frequency of intake and inflammation. We hypothesised that both probiotic intake and ordinary yoghurt intake would be associated with lower levels of inflammation.
Population and Methods
The CKD-Renal Epidemiology and Information Network (CKD-REIN) study is a prospective cohort study carried out in 40 private- or public-sector nephrology clinics throughout France. Between July 2013 and March 2016, the study included 3033 adult outpatients with moderate or advanced CKD [defined as an estimated glomerular filtration rate (eGFR) <60 ml/min/1.73 m2] being monitored by a nephrologist and with no history of kidney transplantation or long-term dialysis. The patients were then followed up once a year for 5 years. The CKD-REIN study design and methods have been described in detail elsewhere (19, 20). The study protocol was approved by a national independent ethics committee (INSERM, Paris, France: reference: IRB00003888) and the French National Consultative Committee on Information Processing in Medical Research (Comité Consultatif sur le Traitement de l’Information en matière de Recherche dans le domaine de la Santé, Paris, France; reference: CCTIRS N° 12.360/CPP). All patients gave their written informed consent to participation.
Data Collection
Data were collected extensively at baseline and then annually. Clinical data (including the CKD history, comorbidities, and medication use) were collected by trained clinical research associates from medical records and prescriptions. Data on sociodemographics, smoking habits, and dietician visits during the previous year were recorded either in patient interviews or via self-questionnaires. Blood pressure, height, and weight were measured. Patients were considered to have hypertension if this disorder was reported in their medical records or if they were taking antihypertensive medications. Patients were considered to have diabetes if (i) the disorder was self-reported, (ii) they used glucose-lowering medication, or (iii) they had a glycated haemoglobin level ≥6.5%, a fasting glucose level ≥7.0 mmol/L, or a randomly measured glucose level ≥11 mmol/L.
Each year, patients were prescribed a set of standard blood and urine tests to be performed at their usual clinical laboratory. Inflammation status was assessed with standard or ultrasensitive assays for serum CRP, depending on the assays used in that laboratory. The eGFR was estimated with the CKD Epidemiology Collaboration equation (21). Albuminuria or proteinuria were measured and classified according to the Kidney Disease: Improving Global Outcomes (KDIGO) 2012 categories: A1, normal (<3 mg/mmol); A2, moderately elevated (3–30); A3, severely elevated (>30) (20).
Dietary Assessment
The patients self-administered a validated, short food frequency questionnaire (FFQ) once in 2017 (22). Each participant had to report his/her usual dietary intake over the previous year, the questionnaire included two parts. Part 1 of the FFQ focussed on intake frequencies and portion sizes during the previous year for 40 food items. Intake frequencies were quantified as “never or less than once a month,” “x times a month,” “x times a week,” or “x times a day.” Food portion sizes were estimated using standard serving sizes and food images. Part 2 of the FFQ focussed on the intake of nutrient-containing food items of specific interest in CKD, such as protein, sodium, and potassium. Based on these data, we calculated daily intakes in g per day for each food item by multiplying the intake frequency by the portion size. An ad hoc composition table was developed using data from the INCA2 survey (a representative survey of the general population in France), in order to estimate the percentage of each food included in a food item group (23). Nutritional data were then obtained using the food composition database developed by the French Data Centre on Food Quality (Ciqual, last updated in 2013) (24).
The FFQ also collected data on prebiotic and probiotic dietary supplements, ordinary yoghurts, and “probiotic yoghurts” (any yoghurt or yoghurt-like item containing strains like Bifidobacteria). The latter’s intake frequencies were qualified as daily or less than daily.
Statistics
A total of 2,820 patients had completed the FFQ in 2017. We conducted a cross-sectional analysis of 888 (31%) patients who had CRP data for the year covered by the FFQ [i.e., blood samples taken in the 12 months preceding the FFQ completion date (Figure 1)]. The mean ± standard deviation time interval between inclusion in the CKD-REIN participants and completion of the FFQ was 1.96 ± 0.6 years. We first compared baseline characteristics for participants included in the present study and those not included. We then assessed participants as a function of their intake category (no yoghurt; ordinary yoghurt; probiotic yoghurt/dietary supplements), using an analysis of variance, a Kruskal–Wallis test or a chi-squared test, as appropriate. Next, we used logistic regression to estimate crude and adjusted odds ratio (ORs) and their 95% confidence intervals (CIs) for the association between inflammation and yoghurt or probiotic intake. Inflammation was studied as a binary variable, and the ORs were estimated for several commonly used CRP thresholds for inflammation (>3, >4, >5, >6, or >7 mg/L) (25–28). We checked for potential interactions between the CRP assay method (a standard assay for 59% of the participants, an ultrasensitive assay for 25%, and missing data for 16%) and yoghurt and probiotic intakes. Given that all the interactions were non-significant (i.e., p > 0.20 for all), we always adjusted the ORs for the assay method but did not include interaction terms in the models. We also adjusted for covariates significantly associated with inflammation in the crude analyses: age, educational level, atheromatous CVD, body mass index (BMI), CKD stage, and intakes of starch, eggs, and sweet snacks. We also forced variables known to affect inflammation (such as sex, and the protein, fibre, and total energy intakes) into the models. Since kidney replacement therapy (KRT) is likely to modify the relationship between yoghurt and probiotic intakes and inflammation, we removed the 70 patients having received KRT before the CRP assay date and FFQ completion from our sensitivity analyses (leaving 818 patients). Lastly, we investigated the association between inflammation and the frequency of yoghurt intake in five intake categories: no yoghurt consumption, occasional consumption of ordinary yoghurt, occasional consumption of probiotics, daily consumption of ordinary yoghurt and daily consumption of probiotics.
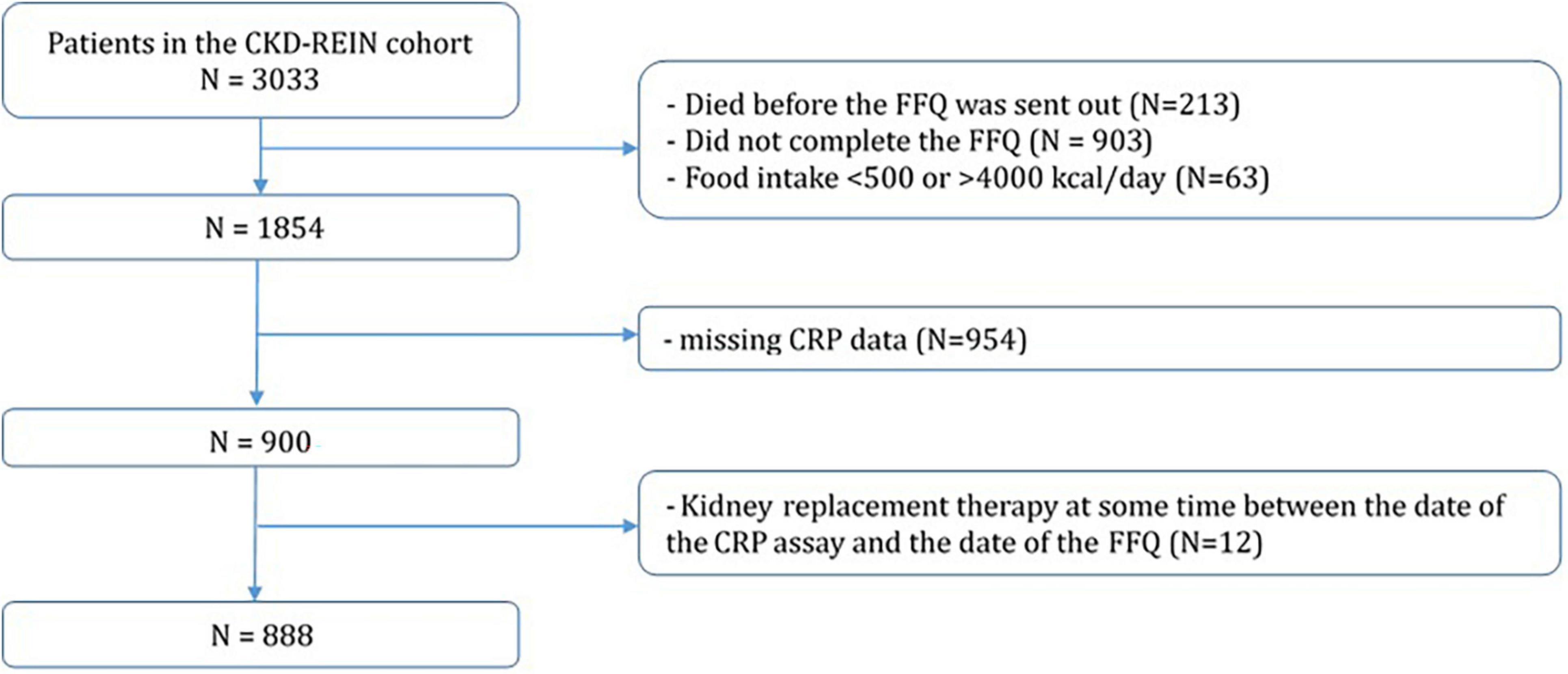
Figure 1. Study flowchart.
Due to the lack of data for some variables (missing data >5% for physical activity, albuminuria, and dietician visits), we applied multiple imputations (25 imputed datasets, fully conditional specification using all covariates, and a maximum of 30 iterations). Logistic regressions were fitted on each imputed dataset, and ORs, CIs and likelihood-ratio test p-values were combined according to Rubin’s rules (29); using the mice R package (30). All statistical analyses were performed using the R software (version 3.6.1) (31).
Results
Characteristics of the Study Population (Overall, and According to the Yoghurt and Probiotic Intake)
We included 888 participants (median age: 70; men: 65%; prevalence of diabetes: 40%), 164 (20%) of whom had consulted a dietician at least once (Table 1). The included and non-included CKD-REIN participants did not differ significantly with regard to clinical and demographic characteristics (Supplementary Table 1). The median [interquartile range (IQR)] eGFR was 29 [20–39] mL/min/1.73 m2. Thirty percent reported the consumption of probiotics (median [IQR] weekly intake: 7 [3–7] items), and 57% reported the consumption of ordinary yoghurts (median [IQR] weekly intake: 7 [3–8] items). When considering the patients who reported consuming probiotics, 84% consumed probiotic yoghurts only, 9% consumed probiotic dietary supplements only, and 7% consumed both. None of the participants reported the use of prebiotics alone as a dietary supplement.
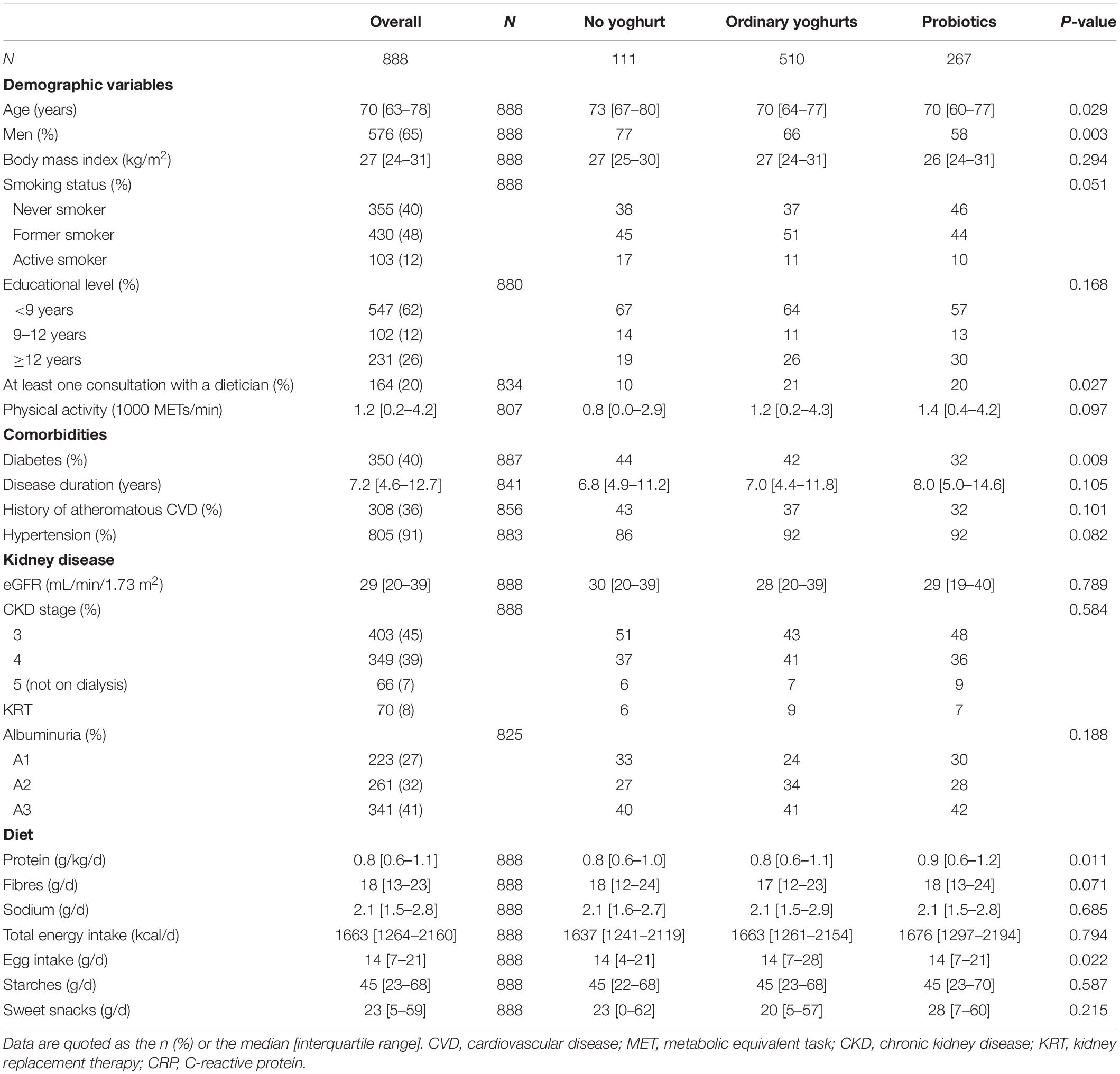
Table 1. Characteristics of the study participants, overall and according to the intakes of ordinary yoghurt and probiotics.
Relative to non-consumers, patients reporting ordinary yoghurt intake or probiotic intake were younger, more likely to be female and less likely to be active smokers (Table 1). They also had a higher level of physical activity and a higher protein intake and were more likely to have reported at least one consultation with a dietician visit. However, the consumers and non-consumers did not differ with regard to the eGFR level, the CKD stage or any of the clinical characteristics (with the exception of diabetes, which was less prevalent among participants reporting probiotic intake).
The median (IQR) serum CRP level in the overall population was 3.0 [1.6–7.0] mg/L. The CRP level increased significantly with the CKD stage (p < 0.001): 2.9 [1.5–6.0] for stage 3, 3.3 [1.5–6.7] for stage 4, 4.4 [2.0–13.0] for stage 5 not on dialysis, and 4.6 [2.5–9.0] mg/L for patients having received KRT (Figure 2).
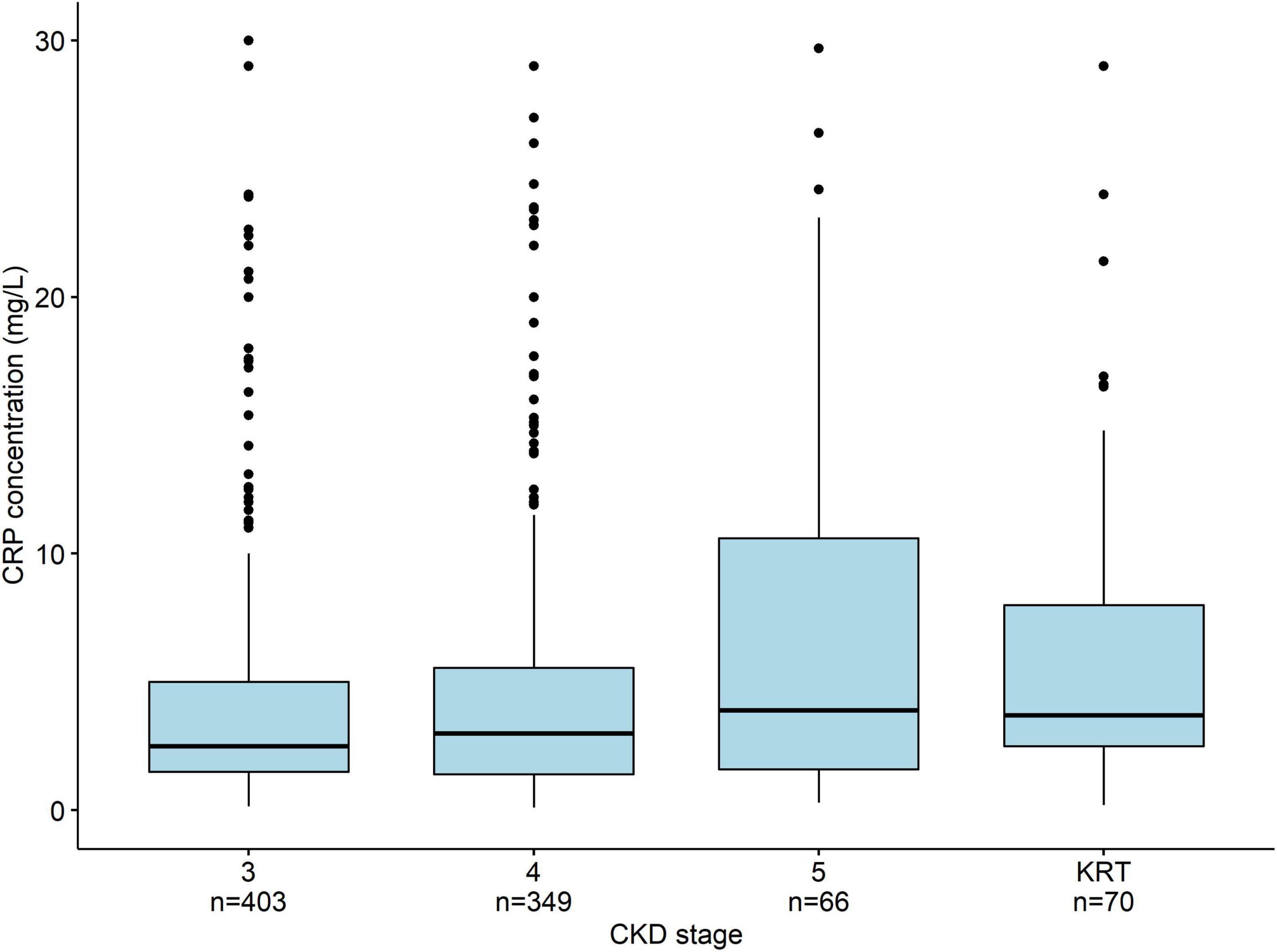
Figure 2. The median (IQR) serum CRP concentration as a function of the CKD stage. The CRP levels rise significantly (p < 0.001) with the CKD stage. To facilitate visual comparisons, outliers (including some >300 mg/L) are not displayed. The whiskers correspond to 1.5 times the IQR.
Association Between Inflammation and Yoghurt/Probiotic Intake
The median CRP level and the proportion of people with a CRP level above 5 mg/L were significantly lower for participants consuming ordinary yoghurts and those consuming probiotics than for participants not consuming either (Table 2). Of note, CRP was significantly higher in patients with higher intakes of starches, eggs, sweet snacks, but was not associated with protein or fibre intakes (data not shown). After adjusting for confounders, the ORs for the associations between inflammation and ordinary yoghurt and probiotic intake were significantly lower for the CRP thresholds >6 mg/L and >7 mg/L (respectively, 0.58 [0.37, 0.93] and 0.57 [0.35, 0.91] for patients consuming ordinary yoghurts) and respectively, 0.54 [0.33, 0.9] and 0.48 [0.28, 0.81], for patients consuming probiotics (Figure 3A). This was not the case for the thresholds >3, >4, and >5 mg/L. Although the removal of the 70 patients with KRT from the analysis slightly attenuated these associations, the ORs for ordinary yoghurts and probiotics were still statistically significant for the CRP thresholds >6 mg/L and >7 mg/L (Figure 3B).
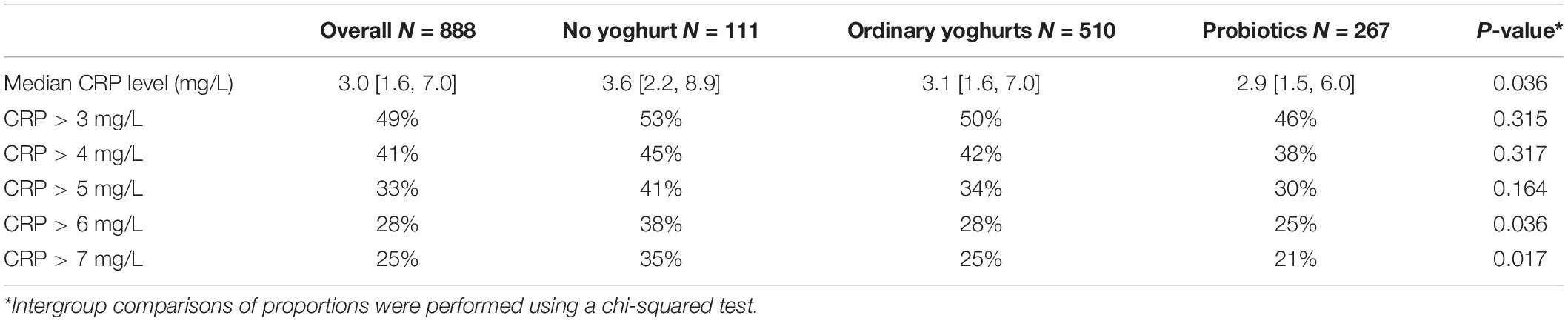
Table 2. Serum CRP concentrations and proportions of the values above the indicated thresholds, overall and according to the intakes of ordinary yoghurt and probiotics.
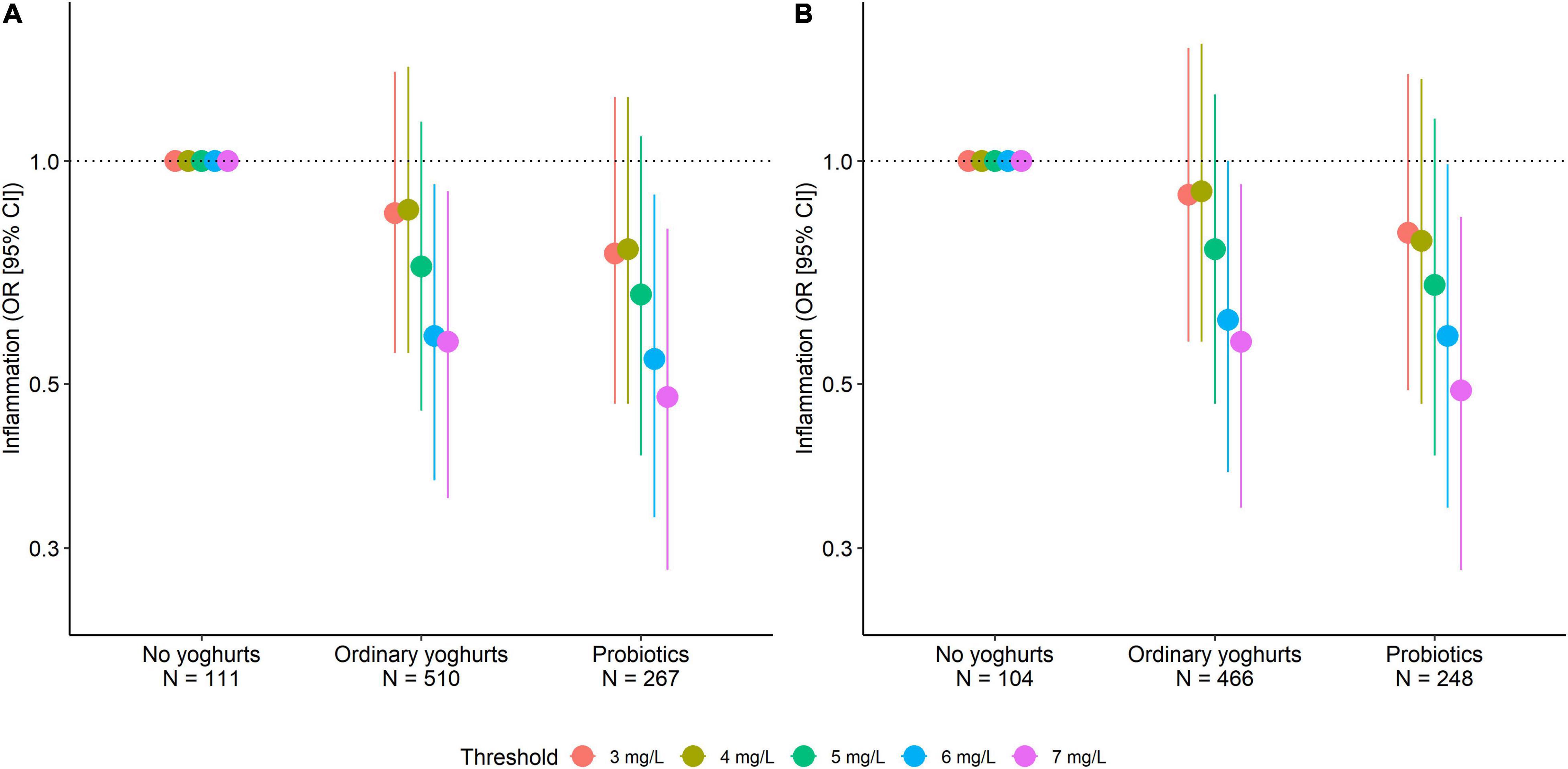
Figure 3. Adjusted odds ratios (95% CI) for various CRP thresholds as a function of intakes of ordinary yoghurt and probiotics (A) in all patients (N = 888) and (B) in patients not on KRT (N = 818). The adjustment variables included the CRP assay method, age, sex, educational level, BMI, history of atheromatous CVD, CKD stage, and intakes of starch, eggs, sweet snacks, protein, fibre, and energy.
Association Between Inflammation and the Frequency of Yoghurt/Probiotic Intake
Around half of the consumers of ordinary yoghurts and probiotics consumed these products daily (Supplementary Figure 1). With CRP thresholds >6 mg/L and >7 mg/L, the crude and adjusted ORs for the association with inflammation were significantly lower in all the consumer groups (relative to non-consumers) other than daily probiotic consumers (Supplementary Figure 2A). No dose-effect relationship was apparent. The exclusion of patients with KRT did not greatly affect these results (Supplementary Figure 2B).
Discussion
Our cross-sectional analysis of patients with moderate-to-advanced CKD participating in the CKD-REIN cohort study showed that a substantial proportion consumed probiotics in yoghurts or dietary supplements. Our results also showed that both ordinary yoghurt intake and probiotic intake were associated with lower risk of inflammation when the CRP threshold was >6 mg/L or >7 mg/L. This association was independent of other known major determinants of inflammation but did not appear to be dose-dependent.
Some clinical trials have shown that probiotic supplementation is associated with a reduction in the level of inflammation in CKD patients. After 6 or 12 months of supplementation with probiotics or symbiotics, patients on dialysis showed a significant decrease in pro-inflammatory cytokines and CRP levels and an increase in anti-inflammatory cytokine levels (12, 15). In contrast, other clinical trials found a non-significant trend toward a lower CRP level (13, 14) or did not find any significant changes in inflammatory biomarker levels (16, 17, 32). These discrepancies might have been due to interstudy differences in the bacterial strains (sometimes combined with a prebiotic), intake doses, and intake duration (between 4 weeks and 6 months). Furthermore, the results of meta-analyses are inconclusive. Thongprayoon et al. (33) and Zheng et al. (34) found that probiotic or symbiotic intake was associated with a significant decrease in the CRP level, whereas Pisano et al. (35) and Tao et al. (36) did not find any significant differences. However, the clinical trials performed to date focused on small number of patients on dialysis, who are known to have higher levels of inflammation than healthy adults. The French calcium and phosphate observatory noted a median (IQR) CRP level of 5 (3–13) mg/L for haemodialysis patients (37), which is similar to the value observed for patients having received KRT in our study [4.6 (2.5–9) mg/L]. Low-grade inflammation is observed in early-stage CKD. We found that CRP level increased progressively with CKD stage; this is in line with the findings of epidemiological studies (38, 39), the Chronic Renal Insufficiency Cohort (1), and the Cardiovascular Health Study (40).
The only randomised study in this field investigated the relationship between probiotic use and CRP level over a 3-month period in CKD stage 3–4 patients. However, the sample size was low (n = 13) and the study lacked the power to demonstrate a significant effect (41). All the studies of probiotics were clinical trials that assessed the effect of dietary supplements but did not consider yoghurt intake. However, yoghurt is a probiotic by definition, since it contains the two regulated bacterial strains (Lactobacillus delbrueckii subsp. bulgaricus and Streptococcus salivarius subsp. thermophilus). The present study is the first to have investigated the “real-life” relationship between yoghurt/probiotic intake and inflammation in a CKD population. Interestingly, we found that yoghurt and probiotic intakes were both associated with lower inflammation when the latter was defined as a CRP threshold >6 mg/L. The removal of patients with KRT only slightly attenuated these associations. Our results are consistent with the body of evidence showing that (i) probiotics are associated with a reduction of inflammation in CKD patients (12, 15), (ii) the consumption of probiotic yoghurt or acidified milk reduces post-prandial inflammation after a high fat meal test in healthy subject (42), and (iii) the consumption of yoghurt is associated with lower levels of inflammation biomarkers in healthy adults (43, 44). In our study, however, the beneficial effect of yoghurt and probiotic consumption was only apparent for a high level of inflammation (CRP > 6 mg/L).
It is widely acknowledged that chronic, low-grade inflammation accelerates the progression of CKD, atherosclerosis and cardiovascular complications and increases the mortality rate (28, 45–47). Although CRP is widely assessed as a marker of systemic inflammation, the defining threshold varies from one study to another as a function of the health risks considered: it is typically 5 mg/L for mortality and 3 mg/L for CVD (28). In the present study, the association between yoghurt and probiotic consumption on one hand and the CRP level on the other was not statistically significant when low CRP thresholds (3, 4, and 5 mg/L) were considered – suggesting that the relationship was diluted for low-grade inflammation. Findings regarding the effect of yoghurt consumption on cardiovascular risk remain controversial. Meta-analyses of both observational studies and randomised clinical trials report inconsistent results, showing protective effects (48) or no effect (49) of yoghurt on cardiovascular risk or mortality. Recently, a meta-analysis showed that probiotic intake was associated with a decrease in blood pressure (50). Furthermore, frequent yoghurt and probiotic intake was linked to a lower level of albuminuria but not with CKD progression in the NHANES (18), and a meta-analysis did not observe a relationship between probiotic intake and eGFR preservation (36) – suggesting that a probiotic-based strategy has limited effects only.
Dysbiosis is one of the causes of chronic inflammation in CKD (51). This condition can be observed in early-stage CKD and can create a progressively pro-inflammatory environment in the host (2, 52). Dysbiosis in CKD patients results in the predominance of bacterial families that possess urease-, indole- and p-cresol-forming enzymes (53). The resulting uraemic toxins accumulate in the body fluids and contribute to inflammation (54). Dysbiosis also indirectly damages the epithelial tight junctions and increases gut barrier permeability; this allows bacterial products like lipopolysaccharides to leak into the circulation and contributes to inflammation. Shi et al. reported that the bacterial DNA concentration is positively correlated with plasma levels of CRP and IL-6 (52). It has been suggested that probiotics can modulate the composition of the microbiota (10), notably by competing with pathogens for nutrients and receptor binding sites (8, 55) and by decreasing levels of uraemic toxins (56). Probiotics also help to protect the intestinal barrier, reduce the activation of the pro-inflammatory nuclear factor-kappa B, and thus slow the leakage of lipopolysaccharides (8, 57). However, other dietary factors such as proteins and fibres may modulate gut microbiota and, potentially, the inflammation status (58, 59). In our study, these nutrients were not significantly associated with CRP level, in contrast with eggs, starches, and sweet snacks, and the observed association between yoghurt and probiotic intakes and inflammation status was independent of all these dietary factors. Moreover, González et al. (60) demonstrated that yoghurt had the best ability to modulate the faecal microbiota among all fermented dairy products.
Yoghurt and probiotics may limit low-grade inflammation. However, given that (i) dysbiosis is not the only source of inflammation in CKD patients (61), and (ii) yoghurt and probiotics mainly act on the gastrointestinal tract, the overall effect of consumption on inflammation in CKD patients may be limited. This limited effect was also suggested by our results for the frequency of consumption. We found that occasional yoghurt intake and daily yoghurt intake were equally associated with lower inflammation. This apparent lack of dose-dependence suggests that a certain quantity of bacteria (Lactobacillus delbrueckii subsp. bulgaricus and Streptococcus salivarius subsp. thermophilus) is enough to obtain a positive effect on the gastrointestinal tract and the microbiota. In contrast, occasional probiotic consumption (but not daily probiotic consumption) was associated with a significantly lower level of inflammation whatever the CRP threshold. However, this discrepancy might be due to a lack of statistical power because the ORs for CRP levels >6 mg/L and daily probiotic consumption were very similar to those for occasional or daily consumption of ordinary yoghurt.
The present study main strengths include its large population of CKD stage 3–5 patients (including a subgroup on KRT), the nationally representative network of investigating centres, and extensive data collection. Our detailed, validated FFQ enabled us to analyse ordinary and probiotic yoghurt consumption separately and to estimate the intakes of other nutrients (such as protein and fibre) that might modulate the composition of the microbiota. Our collection of clinical, nutritional and laboratory data enabled us to adjust our analyses for a large number of potential confounders, including relevant nutrients.
The study also had some limitations. Firstly, the study observational design prevented an assessment of the causal nature of the observed associations. Secondly, we only studied one inflammation biomarker. Nevertheless, CRP is acknowledged to be a reliable marker of inflammatory status (28, 62). Thirdly, the CRP data were generated in various local clinical laboratories, using standard or ultrasensitive assays. However, the type of assay used did not modify the studied associations. Fourthly, only 31% of the CKD-REIN participants alive in 2017 were eligible for our analysis; the remainder were excluded because they did not complete the FFQ, had inadequate food intake estimates, or did not have CRP assay data for the time period covered by the FFQ. Nonetheless, the participants included in or excluded from our analysis did not differ significantly with regard to their demographic and clinical characteristics. Lastly, recall bias cannot be ruled out when using FFQ, but ours has been validated against 24-hr recall over 1 year, and found to be reproducible and valid, thus limiting this bias (22).
Conclusion
Our findings indicate that consumption of yoghurts and probiotics (regardless of the frequency of intake) is associated with a lower risk of inflammation in patients with CKD, independently of other known determinants of inflammation. Further research, including microbiota analysis, is needed to better understand the modulation of inflammation by yoghurts and probiotics and their potential impact on the progression and complications of CKD.
Data Availability Statement
The data analysed in this study is subject to the following licenses/restrictions: Data available on request due to privacy/ethical restrictions. Requests to access these datasets should be directed to BS, YmVuZWRpY3RlLnN0ZW5nZWxAaW5zZXJtLkZy.
Ethics Statement
The study protocol was reviewed and approved by a National Independent Ethics Committee (INSERM, Paris, France: reference: IRB00003888) and the French National Consultative Committee on Information Processing in Medical Research (Comité Consultatif sur le Traitement de l’Information en matière de Recherche dans le domaine de la Santé, Paris, France; reference: CCTIRS N° 12.360/CPP). The patients provided their written informed consent to participate in this study.
Author Contributions
SW, DF, ZM, and BS designed the present study. TM performed the statistical analyses. SW and BS drafted the manuscript. All authors were involved in the interpretation of the results and critical review of the manuscript and approved the manuscript as submitted.
Funding
The CKD-REIN study was funded by the Agence Nationale de la Recherche through the 2010 Cohortes-Investissements d’Avenir programme and by the 2010 National Programme Hospitalier de Recherche Clinique. CKD-REIN was also supported through a public–private partnership with Amgen, Fresenius Medical Care, and GlaxoSmithKline since 2012; Otsuka Pharmaceutical since 2015; Baxter and Merck Sharp & Dohme-Chibret from 2012 to 2017; Sanofi-Genzyme from 2012 to 2015; Lilly France from 2013 to 2018; and Vifor Fresenius Medical Care Renal Pharma Ltd., and AstraZeneca since 2018. Inserm Transfert set up and has managed this partnership since 2011.
Conflict of Interest
SW received a grant from ISN-H4KH Initiative, outside the submitted work. LK received a grant from Fresenius Kabi outside the submitted work, together with consulting fees from AstraZeneca, Dr. Shäre, and Fresenius Kabi. DF received a grant from Fresenius Medical Care outside the submitted work, consulting fees from Fresenius Kabi and Sanofi, and honoraria from Lilly Fresenius Kabi, Sanofi, Vifor, and Astellas. ZM received honoraria from AstraZeneca and Boehringer Ingelheim. M-CB-R received honoraria from MAYOLY SPINDLER and GILEAD.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We thank the CKD-REIN study coordination staff for their efforts in setting up the cohort: Elodie Speyer, Reine Ketchemin, and all the clinical research associates and David Fraser (Biotech Communication SARL, Ploudalmézeau, France) for copy-editing assistance. We also thank the participating clinical sites, the investigators cited below, and all the patients. The members of the CKD-REIN study group are as follows. Steering committee and coordination: Natalia Alencar de Pinho, Carole Ayav, Serge Briancon, Dorothee Cannet, CC, DF, LF, Yves-Edouard Herpe, Christian Jacquelinet, ML, ZM, Christophe Pascal, Bruce M. Robinson, Roberto Pecoits-Filho, BS, Celine Lange, Karine Legrand, Sophie Liabeuf, MM, and Elodie Speyer. CKD-REIN investigators/collaborators: Thierry Hannedouche, Bruno Moulin, Sébastien Mailliez, Gaetan Lebrun, Eric Magnant, Gabriel Choukroun, Benjamin Deroure, Adeline Lacraz, Guy Lambrey, Jean Philippe Bourdenx, Marie Essig, Thierry Lobbedez, Raymond Azar, Hacene Sekhri, Mustafa Smati, Mohamed Jamali, Alexandre Klein, Michel Delahousse, CC, Severine Martin, Isabelle Landru, Eric Thervet, ZM, Philippe Lang, Xavier Belenfant, Pablo Urena, Carlos Vela, LF, Dominique Chauveau, Viktor Panescu, Christian Noel, François Glowacki, Maxime Hoffmann, Maryvonne Hourmant, Dominique Besnier, Angelo Testa, Francois Kuentz, Philippe Zaoui, Charles Chazot, Laurent Juillard, Stephane Burtey, Adrien Keller, Nassim Kamar, DF, and ML.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2022.772596/full#supplementary-material
Abbreviations
BMI, body mass index; CI, confidence interval; CKD-REIN, CKD-Renal Epidemiology and Information Network; CVD, cardiovascular disease; eGFR, estimated glomerular filtration rate; FFQ, food frequency questionnaire; FAO, Food and Agriculture Organization; IL, interleukin; IQR, interquartile range; KDIGO, Kidney Disease: Improving Global Outcomes; KRT, Kidney replacement therapy; OR, odds ratio; NHANES, National Health and Nutrition Examination Survey; WHO, World Health Organization.
References
1. Gupta J, Mitra N, Kanetsky PA, Devaney J, Wing MR, Reilly M, et al. Association between albuminuria, kidney function, and inflammatory biomarker profile in CKD in CRIC. Clin J Am Soc Nephrol. (2012) 7:1938-46. doi: 10.2215/CJN.03500412
2. Vaziri ND, Wong J, Pahl M, Piceno YM, Yuan J, DeSantis TZ, et al. Chronic kidney disease alters intestinal microbial flora. Kidney Int. (2013) 83:308-15. doi: 10.1038/ki.2012.345
3. Levin A, Tonelli M, Bonventre J, Coresh J, Donner J-A, Fogo AB, et al. Global kidney health 2017 and beyond: a roadmap for closing gaps in care, research, and policy. Lancet. (2017) 390:1888-917. doi: 10.1016/S0140-6736(17)30788-2
4. KDIGO. Clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. (2012) 3:15–18.
5. Bazeley J, Bieber B, Li Y, Morgenstern H, de Sequera P, Combe C, et al. C-reactive protein and prediction of 1-year mortality in prevalent hemodialysis patients. Clin J Am Soc Nephrol. (2011) 6:2452-61. doi: 10.2215/CJN.00710111
6. Mafra D, Lobo JC, Barros AF, Koppe L, Vaziri ND, Fouque D. Role of altered intestinal microbiota in systemic inflammation and cardiovascular disease in chronic kidney disease. Future Microbiol. (2014) 9:399-410. doi: 10.2217/fmb.13.165
7. Li F, Wang M, Wang J, Li R, Zhang Y. Alterations to the gut microbiota and their correlation with inflammatory factors in chronic kidney disease. Front Cell Infect Microbiol. (2019) 9:206. doi: 10.3389/fcimb.2019.00206
9. Mafra D, Borges N, Alvarenga L, Esgalhado M, Cardozo L, Lindholm B, et al. Dietary components that may influence the disturbed gut microbiota in chronic kidney disease. Nutrients. (2019) 11:496. doi: 10.3390/nu11030496
10. McFarlane C, Ramos CI, Johnson DW, Campbell KL. Prebiotic, probiotic, and synbiotic supplementation in chronic kidney disease: a systematic review and meta-analysis. J Ren Nutr [Internet]. (2018). Available online at: https://linkinghub.elsevier.com/retrieve/pii/S1051227618301912 (accessed October 29, 2018),
11. Hill C, Guarner F, Reid G, Gibson GR, Merenstein DJ, Pot B, et al. Expert consensus document: the international scientific association for probiotics and prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat Rev Gastroenterol Hepatol. (2014) 11:506-14. doi: 10.1038/nrgastro.2014.66
12. Wang I-K, Wu Y-Y, Yang Y-F, Ting I-W, Lin C-C, Yen T-H, et al. The effect of probiotics on serum levels of cytokine and endotoxin in peritoneal dialysis patients: a randomised, double-blind, placebo-controlled trial. Benef Microbes. (2015) 6:423-30. doi: 10.3920/BM2014.0088
13. Natarajan R, Pechenyak B, Vyas U, Ranganathan P, Weinberg A, Liang P, et al. Randomized controlled trial of strain-specific probiotic formulation (Renadyl) in dialysis patients. BioMed Res Int [Internet]. (2014) 2014:568571. doi: 10.1155/2014/568571
14. Viramontes-Hörner D, Márquez-Sandoval F, Martín-del-Campo F, Vizmanos-Lamotte B, Sandoval-Rodríguez A, Armendáriz-Borunda J, et al. Effect of a symbiotic gel (Lactobacillus acidophilus + Bifidobacterium lactis + Inulin) on presence and severity of gastrointestinal symptoms in hemodialysis patients. J Ren Nutr. (2015) 25:284-91. doi: 10.1053/j.jrn.2014.09.008
15. Soleimani A, Zarrati Mojarrad M, Bahmani F, Taghizadeh M, Ramezani M, Tajabadi-Ebrahimi M, et al. Probiotic supplementation in diabetic hemodialysis patients has beneficial metabolic effects. Kidney Int. (2017) 91:435-42. doi: 10.1016/j.kint.2016.09.040
16. Borges NA, Carmo FL, Stockler-Pinto MB, de Brito JS, Dolenga CJ, Ferreira DC, et al. Probiotic supplementation in chronic kidney disease: a double-blind, randomized, placebo-controlled trial. J Ren Nutr. (2018) 28:28-36. doi: 10.1053/j.jrn.2017.06.010
17. Shariaty Z, Mahmoodi Shan GR, Farajollahi M, Amerian M, Behnam Pour N. The effects of probiotic supplement on hemoglobin in chronic renal failure patients under hemodialysis: a randomized clinical trial. J Res Med Sci. (2017) 22:74. doi: 10.4103/jrms.JRMS_614_16
18. Yacoub R, Kaji D, Patel SN, Simoes PK, Busayavalasa D, Nadkarni GN, et al. Association between probiotic and yogurt consumption and kidney disease: insights from NHANES. Nutr J [Internet]. (2016) 15:10. doi: 10.1186/s12937-016-0127-3
19. Stengel B, Combe C, Jacquelinet C, Briançon S, Fouque D, Laville M, et al. The French chronic kidney disease-renal epidemiology and information network (CKD-REIN) cohort study. Nephrol Dial Transplant. (2014) 29:1500-7.
20. Stengel B, Metzger M, Combe C, Jacquelinet C, Briançon S, Ayav C, et al. Risk profile, quality of life and care of patients with moderate and advanced CKD?: the French CKD-REIN cohort study. Nephrol Dial Transplant [Internet]. (2018). Available online at: https://academic.oup.com/ndt/advance-article/doi/10.1093/ndt/gfy058/4963503 (accesed September 20, 2018), doi: 10.1093/ndt/gfy058
21. Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF, Feldman HI, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. (2009) 150:604-12.
22. Affret A, Wagner S, El Fatouhi D, Dow C, Correia E, Niravong M, et al. Validity and reproducibility of a short food frequency questionnaire among patients with chronic kidney disease. BMC Nephrol. (2017) 18:297. doi: 10.1186/s12882-017-0695-2
23. Afssa. (Agence Française de Sécurité Sanitaire des Aliments). INCA2 - Etude Individuelle Nationale des Consommations Alimentaires 2. (2009). Available online at: https://www.anses.fr/fr/system/files/PASER-Ra-INCA2.pdf (accessed 22 July 2017)
24. Anses. (Agence Nationale de Sécurité Sanitaire- Alimentation, Environnement et Travail). (2016). Available online at: https://pro.anses.fr/TableCIQUAL/index.htm (accessed 22 July 2017).
25. Ioannou K, Stel VS, Dounousi E, Jager KJ, Papagianni A, Pappas K, et al. Inflammation, endothelial dysfunction and increased left ventricular mass in chronic kidney disease (CKD) patients: a longitudinal study. PLoS One. (2015) 10:e0138461. doi: 10.1371/journal.pone.0138461
26. Menon V, Wang X, Greene T, Beck GJ, Kusek JW, Marcovina SM, et al. Relationship between C-reactive protein, albumin, and cardiovascular disease in patients with chronic kidney disease. Am J Kidney Dis. (2003) 42:44-52.
27. Ikizler TA, Wingard RL, Harvell J, Shyr Y, Hakim RM. Association of morbidity with markers of nutrition and inflammation in chronic hemodialysis patients: a prospective study. Kidney Int. (1999) 55:1945-51. doi: 10.1046/j.1523-1755.1999.00410.x
28. Nacb Lmpg Committee Members, Myers GL, Christenson RHM, Cushman M, Ballantyne CM, Cooper GR, et al. National academy of clinical biochemistry laboratory medicine practice guidelines: emerging biomarkers for primary prevention of cardiovascular disease. Clin Chem. (2009) 55:378-84. doi: 10.1373/clinchem.2008.115899
29. Rubin D. Multiple Imputation for Nonresponse in Surveys. New York, NY: John Wiley & Sons (2004).
30. van Buuren S, Groothuis-Oudshoorn K. Mice: Multivariate imputation by chained equations in R. J Stat Softw. (2011) 45:1–67.
31. Core Team R. R: A Language and Environment for Statistical Computing [Internet]. Vienna: R Foundation for Statistical Computing (2019).
32. Rossi M, Johnson DW, Morrison M, Pascoe EM, Coombes JS, Forbes JM, et al. Synbiotics easing renal failure by improving gut microbiology (SYNERGY): a randomized trial. Clin J Am Soc Nephrol. (2016) 11:223-31.
33. Thongprayoon C, Kaewput W, Hatch ST, Bathini T, Sharma K, Wijarnpreecha K, et al. Effects of probiotics on inflammation and uremic toxins among patients on dialysis: a systematic review and meta-analysis. Dig Dis Sci. (2019) 64:469-79. doi: 10.1007/s10620-018-5243-9
34. Zheng HJ, Guo J, Wang Q, Wang L, Wang Y, Zhang F, et al. Probiotics, prebiotics, and synbiotics for the improvement of metabolic profiles in patients with chronic kidney disease: a systematic review and meta-analysis of randomized controlled trials. Crit Rev Food Sci Nutr. (2021) 61:577-98. doi: 10.1080/10408398.2020.1740645
35. Pisano A, D’Arrigo G, Coppolino G, Bolignano D. Biotic supplements for renal patients: a systematic review and meta-analysis. Nutrients (2018) 10:1224. doi: 10.3390/nu10091224
36. Tao S, Tao S, Cheng Y, Liu J, Ma L, Fu P. Effects of probiotic supplements on the progression of chronic kidney disease: a meta-analysis. Nephrol (Carlton Vic). (2019) 24:1122-30. doi: 10.1111/nep.13549
37. Pelletier S, Roth H, Bouchet J-L, Drueke TB, Hannedouche T, Jean G, et al. Évolution de la prise en charge des troubles minéraux et osseux des patients hémodialysés en France entre 2008 et 2012 : observatoire national du métabolisme minéral et osseux. Néphrologie Thérapeutique. (2016) 12:171-7.
38. Xu G, Luo K, Liu H, Huang T, Fang X, Tu W. The progress of inflammation and oxidative stress in patients with chronic kidney disease. Ren Fail. (2015) 37:45-9. doi: 10.3109/0886022X.2014.964141
39. Yilmaz MB, Grossini E, Silva Cardoso JC, Édes I, Fedele F, Pollesello P, et al. Renal effects of levosimendan: a consensus report. Cardiovasc Drugs Ther. (2013) 27:581-90. doi: 10.1007/s10557-013-6485-6
40. Shlipak Michael G, Fried Linda F, Crump C, Bleyer Anthony J, Manolio Teri A, Tracy Russell P, et al. Elevations of inflammatory and procoagulant biomarkers in elderly persons with renal insufficiency. Circulation. (2003) 107:87-92. doi: 10.1161/01.cir.0000042700.48769.59
41. Ranganathan N, Friedman EA, Tam P, Rao V, Ranganathan P, Dheer R. Probiotic dietary supplementation in patients with stage 3 and 4 chronic kidney disease: a 6-month pilot scale trial in Canada. Curr Med Res Opin. (2009) 25:1919-30. doi: 10.1185/03007990903069249
42. Burton KJ, Rosikiewicz M, Pimentel G, Bütikofer U, von Ah U, Voirol M-J, et al. Probiotic yogurt and acidified milk similarly reduce postprandial inflammation and both alter the gut microbiota of healthy, young men. Br J Nutr. (2017) 117:1312-22. doi: 10.1017/S0007114517000885
43. Yuan M, Singer MR, Moore LL. Yogurt consumption is associated with lower levels of chronic inflammation in the framingham offspring study. Nutrients. (2021) 13:506. doi: 10.3390/nu13020506
44. Gadotti TN, Norde MM, Rogero MM, Fisberg M, Fisberg RM, Oki E, et al. Dairy consumption and inflammatory profile: a cross-sectional population-based study, São Paulo, Brazil. Nutr (Burbank Los Angel Cty Calif). (2018) 48:1-5. doi: 10.1016/j.nut.2017.10.003
46. Li W-J, Chen X-M, Nie X-Y, Zhang J, Cheng Y-J, Lin X-X, et al. Cardiac troponin and C-reactive protein for predicting all-cause and cardiovascular mortality in patients with chronic kidney disease: a meta-analysis. Clinics. (2015) 70:301-11. doi: 10.6061/clinics/2015(04)14
47. Silverstein DM. Inflammation in chronic kidney disease: role in the progression of renal and cardiovascular disease. Pediatr Nephrol. (2009) 24:1445-52. doi: 10.1007/s00467-008-1046-0
48. Dehghan M, Mente A, Rangarajan S, Sheridan P, Mohan V, Iqbal R, et al. Association of dairy intake with cardiovascular disease and mortality in 21 countries from five continents (PURE): a prospective cohort study. Lancet (Lond Engl). (2018) 392:2288-97. doi: 10.1016/S0140-6736(18)31812-9
49. Fontecha J, Calvo MV, Juarez M, Gil A, Martínez-Vizcaino V. Milk and dairy product consumption and cardiovascular diseases: an overview of systematic reviews and meta-analyses. Adv Nutr (Bethesda Md). (2019) 10(Suppl. 2):S164-89. doi: 10.1093/advances/nmy099
50. Dixon A, Robertson K, Yung A, Que M, Randall H, Wellalagodage D, et al. Efficacy of probiotics in patients of cardiovascular disease risk: a systematic review and meta-analysis. Curr Hypertens Rep [Internet]. (2020) 22:74. doi: 10.1007/s11906-020-01080-y
51. Lau WL, Kalantar-Zadeh K, Vaziri ND. The gut as a source of inflammation in chronic kidney disease. Nephron. (2015) 130:92-8. doi: 10.1159/000381990
52. Shi K, Wang F, Jiang H, Liu H, Wei M, Wang Z, et al. Gut bacterial translocation may aggravate microinflammation in hemodialysis patients. Dig Dis Sci. (2014) 59:2109-17. doi: 10.1007/s10620-014-3202-7
53. Wong J, Piceno YM, DeSantis TZ, Pahl M, Andersen GL, Vaziri ND. Expansion of urease- and uricase-containing, indole- and p-cresol-forming and contraction of short-chain fatty acid-producing intestinal microbiota in ESRD. Am J Nephrol. (2014) 39:230-7. doi: 10.1159/000360010
54. Ramezani A, Massy ZA, Meijers B, Evenepoel P, Vanholder R, Raj DS. Role of the gut microbiome in uremia: a potential therapeutic target. Am J Kidney Dis. (2016) 67:483-98. doi: 10.1053/j.ajkd.2015.09.027
55. Mousavi Khaneghah A, Abhari K, Es̨ I, Soares MB, Oliveira RBA, Hosseini H, et al. Interactions between probiotics and pathogenic microorganisms in hosts and foods: a review. Trends Food Sci Technol. (2020) 95:205-18.
56. Koppe L, Fouque D, Soulage CO. The role of gut microbiota and diet on uremic retention solutes production in the context of chronic kidney disease. Toxins [Internet]. (2018) 10:155. doi: 10.3390/toxins10040155
57. Artis D. Epithelial-cell recognition of commensal bacteria and maintenance of immune homeostasis in the gut. Nat Rev Immunol. (2008) 8:411-20. doi: 10.1038/nri2316
58. Cronin P, Joyce SA, O’Toole PW, O’Connor EM. Dietary fibre modulates the gut microbiota. Nutrients. (2021) 13:1655. doi: 10.3390/nu13051655
59. Madsen L, Myrmel LS, Fjære E, Liaset B, Kristiansen K. Links between dietary protein sources, the gut microbiota, and obesity. Front Physiol [Internet]. (2017) 8:1047. doi: 10.3389/fphys.2017.01047
60. González S, Fernández-Navarro T, Arboleya S, de los Reyes-Gavilán CG, Salazar N, Gueimonde M. Fermented dairy foods: impact on intestinal microbiota and health-linked biomarkers. Front Microbiol [Internet]. (2019) 10:1046. doi: 10.3389/fmicb.2019.01046
61. Akchurin OM, Kaskel F. Update on inflammation in chronic kidney disease. Blood Purif. (2015) 39:84-92.
62. Pearson Thomas A, Mensah George A, Alexander RW, Anderson JL, Cannon RO III, Criqui M, et al. Markers of inflammation and cardiovascular disease: application to clinical and public health practice: a statement for healthcare professionals from the centers for disease control and prevention and the American heart association. Circulation. (2003) 107:499-511. doi: 10.1161/01.cir.0000052939.59093.45
Keywords: inflammation, C-reactive protein, yoghurt, probiotic, chronic kidney disease, epidemiology
Citation: Wagner S, Merkling T, Metzger M, Koppe L, Laville M, Boutron-Ruault M-C, Frimat L, Combe C, Massy ZA, Stengel B and Fouque D (2022) Probiotic Intake and Inflammation in Patients With Chronic Kidney Disease: An Analysis of the CKD-REIN Cohort. Front. Nutr. 9:772596. doi: 10.3389/fnut.2022.772596
Received: 08 September 2021; Accepted: 07 March 2022;
Published: 30 March 2022.
Edited by:
Wei Ling Lau, University of California, Irvine, United StatesReviewed by:
Edite Teixeira-Lemos, Instituto Politécnico de Viseu, PortugalSilvia Lai, Sapienza University of Rome, Italy
Copyright © 2022 Wagner, Merkling, Metzger, Koppe, Laville, Boutron-Ruault, Frimat, Combe, Massy, Stengel and Fouque. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sandra Wagner, cy53YWduZXIyQGNocnUtbmFuY3kuZnI=