
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr., 19 December 2022
Sec. Nutritional Epidemiology
Volume 9 - 2022 | https://doi.org/10.3389/fnut.2022.1088051
This article is part of the Research TopicEconomic and Health Impacts of Dietary InterventionsView all 7 articles
 Joice Silva Vieira Leal1
Joice Silva Vieira Leal1 Aline Siqueira Fogal1
Aline Siqueira Fogal1 Adriana Lúcia Meireles1,2Letícia de Oliveira Cardoso3Ísis Eloah Machado1,4Mariana Carvalho de Menezes1,2*
Adriana Lúcia Meireles1,2Letícia de Oliveira Cardoso3Ísis Eloah Machado1,4Mariana Carvalho de Menezes1,2*Introduction: The consumption of sugar-sweetened beverages (SSBs) is among the main risk factors for non-communicable diseases (NCDs). This study aimed to estimate the financial costs of hospitalizations and procedures of high and medium complexity for NCDs attributable to the consumption of SSBs in the Brazilian Unified Health System (SUS) in 2019.
Methods: This ecological study used data from the Global Burden of Disease (GBD) 2019 and the Department of Informatics of the Unified Health System (DATASUS). The attributable costs were estimated from the population-attributable fraction (PAF) and the costs in the treatment of chronic diseases [type 2 diabetes mellitus and ischemic heart disease (IHD)], stratified by sex, age group, level of complexity of treatment, and federative units.
Results: In 2019, in Brazil, US$ 14,116,240.55 were the costs of hospitalizations and procedures of high and medium complexity in the treatment of NCDs attributable to the consumption of SSBs. These values were higher in males (US$ 8,469,265.14) and the southeast and southern regions, mainly in the state of São Paulo. However, when evaluating these results at a rate per 10,000 inhabitants, it was observed that the states of Paraná, Tocantins, and Roraima had higher costs per 10,000 inhabitants. Regarding the age groups, higher costs were observed in the older age groups.
Conclusion: This study revealed the high financial impact of the NCDs treatment attributed to the consumption of SSBs in Brazil and the variability among Brazilian macro-regions. The results demonstrate the urgency and need for the expansion of policies to reduce the consumption of SSBs in Brazil with strategies that consider regional particularities.
The accelerated growth of non-communicable diseases (NCDs) has highlighted modifiable risk factors, including dietary risks (1). The World Health Organization points out that consumption of sugar-sweetened beverages (SSB) is among the main risk factors for chronic diseases and recommends limiting consumption of this group of beverages, including soft drinks and artificial juices (2). The prevalence of SSB consumption globally is demonstrated in recent studies, according to the national representative survey in Saudi Arabia 71.2% of adults consumed SSBs weekly, while 35.5% consumed SSBs daily (3). Another study conducted in the same country explored weekly and daily SSB consumption rates in a multiethnic population of middle-aged men, and showed that most individuals (93.8%) were weekly SSB consumers and about one-third (32.6%) were daily SSB consumers (4). In a national survey of Australian adults, 55.9 and 19.3% of men consumed SSBs weekly and daily, respectively (5). A Norwegian study reported that the rate of SSBs intake among adults was 34% (6). Another study indicated that 63.9% of American adults drank SSBs daily. In addition, the daily consumption rates of regular soda, fruit juices, and energy/sports drinks were 21, 6.6, and 5.7%, respectively (7). The daily consumption rate of SSBs among British adults was 20.4% (8). In Brazil, According to the last National Health Survey, 9.2% of the adult population regularly consume soft drinks (at least 5 days a week), being a more frequent habit among men and the younger population (9). Recent estimates of the Surveillance System of Risk and Protection Factors for Chronic Diseases by Telephone Survey reveal that the frequency of consumption of soft drinks on five or more days of the week was 14%, being higher among men (17.2%) than women (11.3%), considering the sample in Brazilian capitals (10).
The association between the consumption of SSBs and the development of diabetes and cardiovascular risk may be related to the high energy density of these beverages and their role in increasing the body weight, with obesity or overweight being an intermediate factor in this relationship. The biological mechanisms between these risk factors and the outcomes are mainly related to the high sugar content of these beverages, reduced satiety, and lack of compensatory mechanisms in calorie intake at subsequent meals (11). In addition, this development may stem from metabolic effects related to the high glycemic load (GL) of these beverages, which consequently induces a rapid elevation in blood glucose and insulin levels (11, 12). Diets with high GL may promote insulin resistance (12), increase inflammatory biomarkers (13), and are associated with an increased risk of type 2 diabetes mellitus (DM-2) (14, 15) and coronary heart disease (16). Although the association between the consumption of SSBs and NCDs has been well reported in the scientific literature (17), few studies have estimated the impact of this risk factor on the costs of health services, which pay for the treatment of these diseases. A recent study (18) estimated that in Brazil, approximately US$ 890 million were used in hospitalizations, outpatient procedures, and medications in the treatment of hypertension, diabetes, and obesity in the Unified Health System [Sistema Único de Saúde (SUS)] (18). A large part of these costs could be avoided by reducing the risk factors related to these diseases. An analysis of the impact of voluntary reduction of sodium in industrialized food would lead to savings of US$ 220 million in 20 years by reducing the total expenditure on the treatment of cardiovascular diseases (19). Further study of the impact of risk factors on the costs of different levels of healthcare is needed to direct priorities for investment in prevention policies (18). This study aimed to estimate the direct financial costs of hospitalizations and procedures of high and medium complexity for NCDs attributable to the consumption of SSBs in 2019 at the national level and in Brazilian federative units. Thus, it will be possible to obtain the cost values that could be saved in the country if the consumption of SSBs is reduced.
This descriptive ecological study used secondary public domain data obtained from the Global Burden of Disease (GBD) 2019 study conducted by the Institute for Health Metrics and Evaluation and the Department of Informatics of the Unified Health System (DATASUS). The study population included adult individuals of both sexes, in all the federative units of Brazil, aged over 25 years; the GBD makes available estimates of the burden of NCDs attributed to dietary factors from the age of 25 years because it considers that the health effects resulting from these risk factors appear after this age (20).
In this study, we evaluated the consumption of SSBs as a risk factor, defined as any intake (in grams per day) of beverages with ≥50 kcal per 226.8 g, including carbonated beverages, soft drinks, energy drinks, and fruit juices, excluding 100% fruit and vegetable juices, this exposure is defined by the GBD based on published systematic reviews (21).
The GBD selects the 24-h recall as the gold standard method of measuring food intake to assess the mean intake at the population level to ensure the comparability of data. SSBs intake was measured in a continuous and non-categorical manner (21). To estimate the mean daily intake of each risk factor, the GBD uses the Gaussian method standardized for country, year, age, and sex (22).
Two outcomes attributed to the consumption of SSBs were described and considered in the present study: DM-2 (23) described according to the International Statistical Classification of Diseases and Health Problems, version 10 (ICD-10) using the following codes: E11–E11.1 and E11.3–E11.9; and ischemic heart diseases (IHDs), with the following ICD-10 codes: I20–I21.6, I21.9–I25.9, and Z82.4–Z82.49 (20, 24). The IHDs represent the following diseases: acute myocardial infarction, chronic stable angina, chronic IHD, and heart failure due to IHD, all of which were identified using standard case definitions. Myocardial infarction was defined according to the Fourth Universal Definition of Myocardial Infarction and adjusted to include out-of-hospital sudden cardiac death. Stable angina was defined using the Rose Angina Questionnaire (25).
The 2019 GBD, from reviews in the scientific literature, considers two metabolic risk factors as mediators for the outcome of DM-2: elevated fasting plasma glucose and body mass index (BMI), which are described as factors involved in the causal pathway of DM-2 development related to SSBs consumption (21).
To estimate the fraction of the attributable burden or population-attributable fraction (PAF) of each outcome (DM-2 and IHD) to the consumption of SSBs, three components were used: (a) the level of risk factor exposure, that is, the average daily consumption of SSBs by the population, (b) the counterfactual level of risk factor exposure or theoretical minimum risk exposure level (TMREL), and (c) the relative risk of the outcome due to exposure (consumption of SSBs) relative to the TMREL (23).
To determine the mean TMREL value, the GBD conducted a systematic review of the scientific literature to identify national or subnational representative surveys that provide data on the dietary intake of SSBs in countries (22). The TMREL value for some harmful dietary factors with uniform risk function growth was set to 0 g, as is the case with the consumption of SSBs (21). The relative risks in relation to the TMREL were obtained from surveys in published systematic reviews. PAF represents the proportion of NCDs that would be reduced or eliminated in Brazil in 2019 if exposure to a particular risk factor (such as consumption of SSBs) in the past was reduced to an ideal exposure scenario (0 g/day) (21, 26). The PAF value is age-, sex-, location-, and year-specific, allowing for stratified analyses (27).
The PAF values for each outcome attributed to the consumption of SSBs (DM-2 and DIC) were extracted from the GBD. Since obesity is a mediating factor in the causal pathway of SSBs consumption and DM-2 (21), GBD does not estimate the PAF of obesity. However, since obesity is described as a diagnosis in the SUS databases, to obtain the PAF of obesity attributed to the consumption of SSBs, we chose, by convention, to use the same PAF as for DM-2.
We estimated the direct costs allocated to the treatment of NCDs attributed to the consumption of SSBs, which refer to direct care to the individual and include hospital admissions, outpatient procedures, examinations, tests and controls, inputs, medications, emergency services, employee compensation, nursing services, and other services directly linked to patient care (27, 28).
To estimate the financial costs, the hospital information system (SIH) and outpatient information system (SIA), available via DATASUS, were used as data sources. These databases were used because they provide the cost per procedure related to the main disease available from the ICD-10 code (“DATASUS”, [S.d.]). Thus, the variable “ICD-10 codes” was used to link the information from SIH and SIA to the PAF made available by the GBD.
The database was extracted from the SIA data files [individualized outpatient production bulletin–BPA I and authorization of high complexity procedures (APAC) and SIH (authorization of hospital admissions, AIH)] on the DATASUS website for the years 2019, 2020, and 2021. Subsequently, only procedures and hospitalizations performed in 2019 were included. For the extraction and processing of these data, the microdatasus package was used in the statistical program R (29).
After the data extraction and processing step in the R program, the ICD-10 package of the STATA software, version 15, was used to group the outcomes that generated the procedures, from the ICD-10 codes, into the GBD 2019 causes attributable to the consumption of SSBs (DM-2 and DIC).
Finally, the Microsoft Excel 2019 program was used to combine the information on PAF values for the year 2019, obtained from the GBD study, with information on total costs by outpatient procedures and hospitalizations, by age group, sex, and federative units.
After grouping the data, the financial costs per NCDs attributable to the consumption of SSBs were obtained by multiplying the total values of hospitalizations and high and medium complexity procedures by the corresponding PAF for each location (Brazil and federative units), sex, and age group. In addition, for comparison purposes among the federative units, the total values per federative unit were divided by the resident population according to data provided by the DATASUS and multiplied by 10,000 inhabitants.
These costs were obtained in reais (Brazilian currency) and converted into US$–dollars, considering the 2019 exchange rate according to the Organization for Economic Cooperation and Development (OECD) (US$ 3.944). The cost values in the treatment of NCDs attributed to the regular consumption of SSBs were presented by age group, sex, outcome, federative unit, Brazilian macro-region, and level of complexity (outpatient or inpatient).
In Brazil, the costs in 2019 were US$ 14,116,240.55 (equivalent to R$ 55,674,452.74), with high and medium complexity procedures in the treatment of NCDs attributed to the consumption of SSBs. These values were higher in males (US$ 8,469,265.14) than in females (US$ 5,646,975.42). The costs of NCDs treatment attributed to the consumption of SSBs were US$ 162,277.61 for DM-2, US$ 1,572,456.50 for obesity, and US$ 12,381,506.46 for IHD (Table 1).
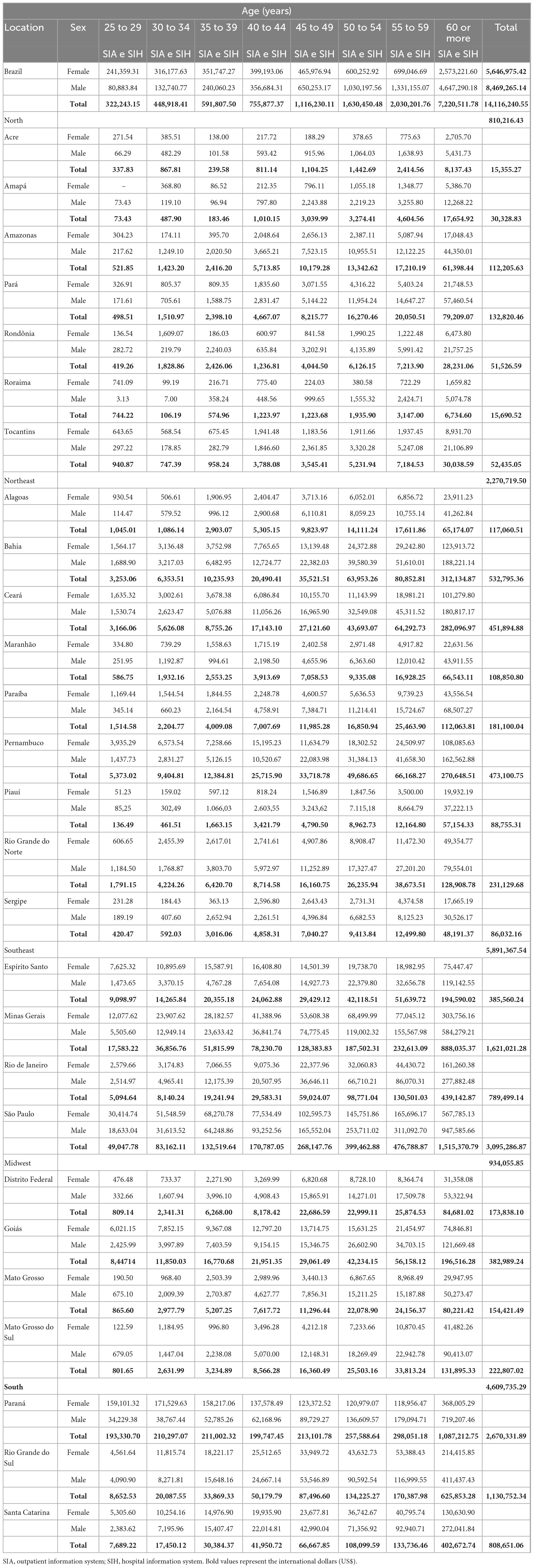
Table 1. Financial costs in the treatment of NCDs attributed in the consumption of SSBs, international dollars (US$), in the year 2019, by sex, age group, regions and Brazilian federative units, and outpatient information system (SIA) and hospital information system (SIH), according to Global Burden of Disease (GBD) 2019.
Regarding age groups, higher costs were observed in the older age groups, and an increase in SUS costs with high and medium complexity procedures in the treatment of NCDs attributable to the consumption of SSBs, corresponding to a total cost with individuals over 60 years old of US$ 7,220,511.78.
When evaluated according to the state, the states of São Paulo (US$ 3,095,286.87) and Paraná (US$ 2,670,331.89) had the highest total costs, and the states of Acre (US$ 15,355.27) and Roraima (US$ 15,690.52) had the lowest financial costs in the treatment of NCDs attributed to the consumption of SSBs (Table 1). For the Brazilian macro-regions, the southeast and southern regions presented the highest cost values, as shown in Figure 1.
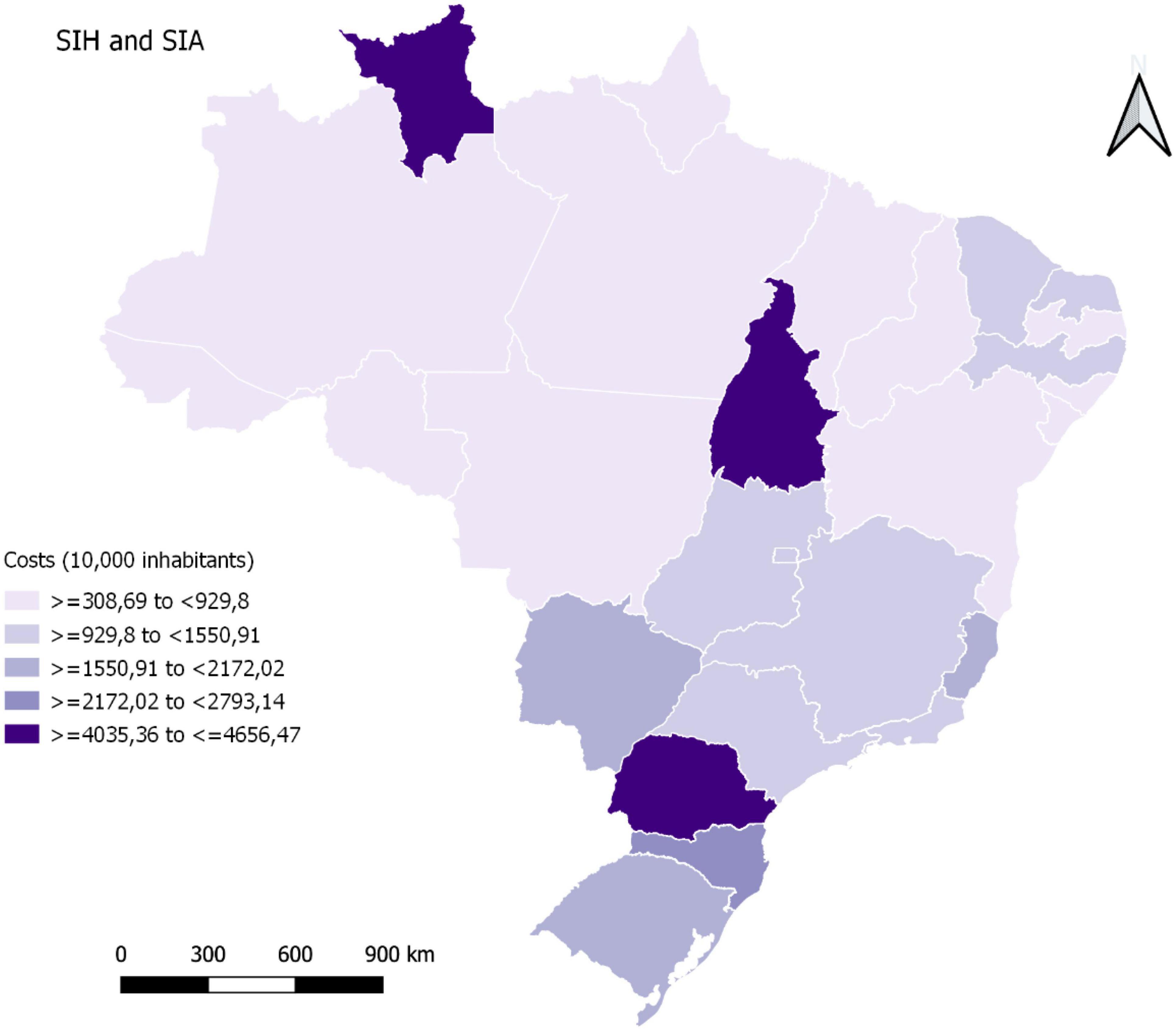
Figure 1. Financial costs in the treatment of non-transmissible chronic diseases (NCDs) attributed to the consumption of sugar-sweetened beverages (SSBs), in international dollars (US$) and in the federative units per 10,000 inhabitants, Brazil, 2019.
When evaluating these costs per 10,000 inhabitants, it was observed that the states of Paraná, Tocantins, and Roraima obtained the highest costs in the treatment of NCDs attributed to the consumption of SSBs in high and medium complexity procedures in the SUS in 2019 (Figure 1).
Table 2 shows the financial costs of the SUS in procedures (inpatient and outpatient) according to the SIH and SIA by sex, age group, and outcome. The results reveal that the cost values in 2019 with inpatient procedures were higher than those with outpatient procedures, regardless of the outcome, age group, and sex.
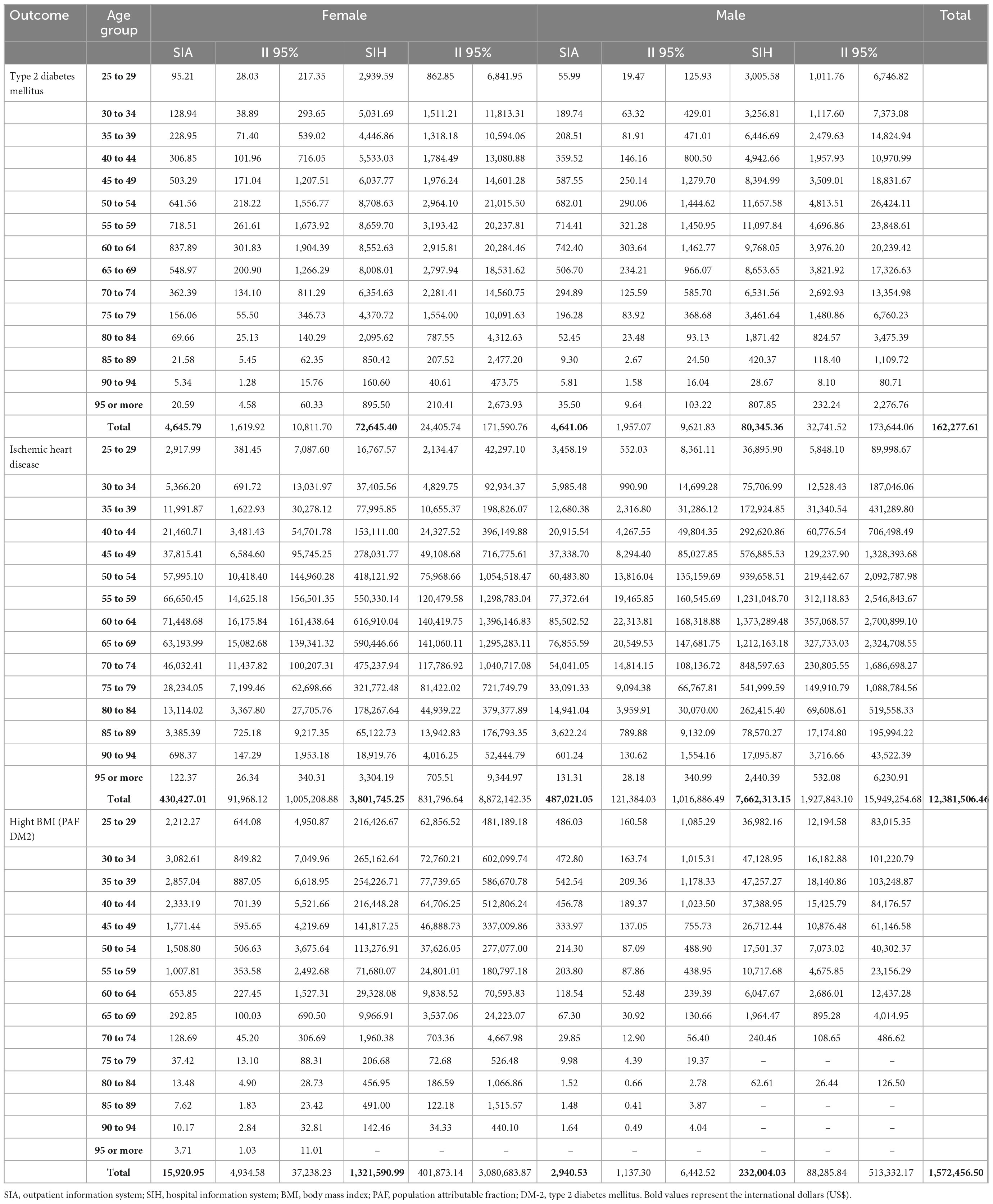
Table 2. Financial costs of hospitalizations and high and medium complexity procedures for NCDs attributed to the consumption of SSBs, in international dollars (US$), by age group, sex, and outcomes, Brazil, 2019, SIA and SIH, according to GBD 2019.
In 2019, $ 14,116,240.55 was used in the medium and high complexity procedures in the treatment of NCDs attributed to the consumption of SSBs, in the SUS. These values were higher in males and showed geographic variability.
According to data from the Health Economics Bulletin in 2019 from the Brazilian Ministry of Health (2021), the Brazilian government invested approximately 4% of the Gross Domestic Product in public health actions and services, totaling R$ 289.6 billion (30). According to information made available by the Pan American Health Organization, from 2010 to 2015, there was a global increase in average costs of public health services from 3.8 to 4.2% (1, 2). NCDs are a global health problem that directly impacts the costs of countries’ health systems, and their main risk factors are behavioral and modifiable, such as the consumption of SSBs. Analyzing the healthcare costs of other risk factors for NCDs, Ding et al. (31) report that the global estimate of costs related to physical inactivity was $ 53.8 billion in 2013. Therefore, several strategies have been adopted globally to reduce the health impact of NCDs and their risk factors (31).
Regarding the risk factor studied, in recent years, several countries have adopted policies with the intention of reducing the consumption of SSBs in the population, including taxing them at higher rates. In some places, these measures have proven effective, as is the case in Mexico (32). A cross-sectional study conducted in different countries demonstrated the relevance of tax policies by establishing a relationship between the affordability of SSBs and the prevalence of overweight and obesity (33). Age-standardized prevalence rates of overweight and obesity have increased due to the increased affordability of SSBs, reinforcing current recommendations that fiscal policies and other actions are important to encourage a reduction in the consumption of SSBs and control population weight gain (34).
However, in Brazil, this is still an agenda under discussion among researchers, civil society, and public powers (35, 36). Despite the great debate around policies to reduce the consumption of SSBs, there are currently observed actions contrary to these policies, such as the wide range of tax benefits granted to the SSB production industry, culminating in the reduction of the final price of their products, making them more accessible to the population (35).
The values of costs for NCDs treatment attributable to the consumption of SSBs were higher in males compared with females, this may be related to the higher consumption of SSBs by males, as revealed by the latest population surveys conducted in Brazil, such as the VIGITEL of 2021, which showed that the consumption of soft drinks in the Brazilian population is higher in men (17.2%) than that in women (11.3%) (10). In addition, the National Health Survey (PNS) 2019 pointed out that 9.2% of Brazilian adults regularly consumed soft drinks, being a more frequent habit among men (11.6%) than that of among women (7.2%) (9).
The values of costs for NCDs treatment attributable to the consumption of SSBs were also higher in the southeast region, especially in the state of São Paulo, followed by the states of the southern region; however, when evaluating these results in a rate per 10,000 inhabitants, it was observed that the states of Paraná, Tocantins, and Roraima, which belong to the northern region, had higher values of costs. These findings may be related to inequalities in access to healthcare in Brazil and regional diversity (37). Studies have shown that access to and use of health services in Brazil reflects inequalities among distinct social groups (38). The data found in the last PNS corroborate these studies, revealing that the Brazilian regions with the highest proportions seeking healthcare were the southeast (20.9%) and southern (19.8%) regions with better living conditions and higher human development indexes, while the northern region had the lowest proportion (13.7%) (9).
This study showed that the total values for outpatient procedures were lower than those for inpatient services in 2019. This is due to the higher amount paid in inpatient procedures, thus totaling a larger sum than that for outpatient services (39). It is noteworthy that the care model proposed by the SUS is a highly effective and efficient way to act on the main causes of health problems and risks to wellbeing, as well as deal with emerging challenges that threaten health and wellbeing in the future. Primary health care is a cost-effective investment, as there is evidence that quality primary care reduces total healthcare costs and improves efficiency, for example, by reducing hospital admissions. Thus, strengthening this model of care is important for addressing NCDs and their risk factors, as well as for being cost-effective. Furthermore, strengthening systems in the community with the decentralization of health services contribute to building resilience, which is fundamental to resisting shocks in health systems (1, 2).
The results of this study should be interpreted in light of its limitations. The diversity and plurality of the Brazilian regions can be interfering factors, for example, with the different quality of the databases, due to the difficulty of access to a quality service, because of availability and geographical distance, both in the northern and northeast regions, the estimates collected from these regions are limiting (38). Furthermore, caution is recommended when interpreting the results of the federative unit and sex because of the amplitude of the uncertainty intervals, which sometimes overlap.
In addition, data on the consumption of SSBs come from various sources, and the 2019 GBD does not yet include more recent sources that estimate SSBs consumption, such as the Household Budget Survey (POF) 2017–2018 and National Health Survey 2019. Finally, it is noteworthy that the cost estimates reflect only the data in the SUS and do not include cost figures in private and supplementary healthcare institutions. If these costs are also accounted for, the amount allocated to the treatment of NCDs attributed to the consumption of SSBs would be higher.
The results of this study reveal the impact of the SUS on health and financial costs, which could be lowered if the consumption of SSBs was reduced in the Brazilian population. Notably, the literature presents evidence of successful public health measures implemented in some countries and localities, such as taxation of SSBs, marketing restrictions, mandatory nutrition labeling, and awareness campaigns (2, 40). Specifically, in Brazil, important advancements have been made as a result of efforts by researchers and experts on the subject, such as the new legislation on front nutrition labeling on packaged foods, which provides clearer information to consumers about the main critical ingredients present in ultra-processed foods, such as sugar, fat, and salt (41). However, it is still necessary to break the inertia and political interest that generate actions contrary to health, being urgent and necessary to implement articulated policies to reduce the consumption of SSBs. Therefore, the commitments made by Brazil in the United Nations Decade of Action for Nutrition (2016–2025) and in the Plan of Strategic Actions for the Confrontation of Chronic Diseases and NCDs in Brazil 2021–2030 (42) involve reducing the regular consumption of SSB by at least 30% in the adult population (1).
This study showed that, in Brazil, in 2019, the consumption of SSBs reflected a significant financial impact on the SUS from medium and high complexity procedures in the treatment of NCDs. These results reveal that if the consumption of SSBs was reduced in Brazil, a relevant financial amount could have been saved in the treatment of these comorbidities; these values could have been reverted to health protection and promotion policies. Despite Brazil’s commitment to reducing the consumption of SSBs, little progress has been made in the policy field in recent years to achieve this goal. There is an urgent need for the implementation and strengthening of articulated actions, especially those based on evidence that considers the Brazilian regional disparities to contribute to the reduction of the high burden that NCDs impose on the population.
The original contributions presented in this study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by the Comitê de Ética em Pesquisa Envolvendo Humanos–Universidade Federal Ouro Preto. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
JL conception and study design, analysis and interpretation of data, writing the manuscript, and critical review and final approval. AF and LC analysis and interpretation of data and critical review and final approval. AM conception and study design, analysis and interpretation of data, and critical review and final approval. ÍM conception and study design, project administration, analysis and interpretation of data, critical review, and management of financial resources and final approval. MM conception and study design, analysis and interpretation of data, critical review, supervision, and final approval. All authors contributed to the article and approved the submitted version.
This study used data from the Institute for Health Metrics and Evolution, funded by the Bill and Melinda Gates Foundation Acknowledgments. Conselho Nacional de Desenvolvimento Científico e Tecnologico, process number: 442636/2019-9. JL was a research fellow at the Universidade Federal de Ouro Preto.
We would like to acknowledge the Institute of Health Metrics and Evaluation (IHME) and the Department of Informatics of the Unified Health System (DATASUS) for providing data to the study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Pan American Health Organization [PAHO]. Ultraprocessed Foods and Beverages in Latin America: Trends, Effect on Obesity, and Implications for Public Policy. Washington, DC: Pan American Health Organization (2018). 78 p.
2. World Health Organization [WHO]. Fiscal Policies for Diet and Prevention of Noncommunicable Diseases, Technical Mee- ting Report, 5–6 May 2015. Geneva: WHO (2016).
3. Al-Hanawi MK, Ahmed MU, Alshareef N, Qattan AMN, Pulok MH. Determinants of sugar-sweetened beverage consumption among the saudi adults: findings from a nationally representative survey. Front Nutr. (2022) 9:744116. doi: 10.3389/fnut.2022.744116
4. AlFaris NA, Alshwaiyat NM, Alkhalidy H, AlTamimi JZ, Alagal RI, Alsaikan RA, et al. Sugar-sweetened beverages consumption in a multi-ethnic population of middle-aged men and association with sociodemographic variables and obesity. Front Nutr. (2022) 9:987048. doi: 10.3389/fnut.2022.987048
5. Miller C, Ettridge K, Wakefield M, Pettigrew S, Coveney J, Roder D, et al. Consumption of sugar-sweetened beverages, juice, artificially-sweetened soda and bottled water: an Australian population study. Nutrients. (2020) 12:817. doi: 10.3390/nu12030817
6. Paulsen MM, Myhre JB, Andersen LF. Beverage consumption patterns among norwegian adults. Nutrients. (2016) 8:561. doi: 10.3390/nu8090561
7. Park S, McGuire LC, Galuska DA. Regional differences in sugar-sweetened beverage intake among US adults. J Acad Nutr Diet. (2015) 115:1996–2002. doi: 10.1016/j.jand.2015.06.010
8. Barrett P, Imamura F, Brage S, Griffin SJ, Wareham NJ, Forouhi NG. Sociodemographic, lifestyle and behavioural factors associated with consumption of sweetened beverages among adults in Cambridgeshire, UK: the Fenland Study. Public Health Nutr. (2017) 20:2766–77. doi: 10.1017/S136898001700177X
9. National Health Interview Survey. Perception of Health Status, Lifestyles, Chronic Diseases and Oral Health. Brazil: Ibge (2019).
10. Secretaria de Vigilância em Saúde D de, Análise em Saúde e Vigilância de Doenças não Transmissíveis. Surveillance of Risk And Protection Factors For Chronic Diseases By Telephone Survey - Vigitel Brazil 2021. Brasília: Ministry of Health (2021).
11. Tey SL, Salleh NB, Henry J, Forde CG. Effects of aspartame-, monk fruit-, stevia- and sucrose-sweetened beverages on postprandial glucose, insulin and energy intake. Int J Obes. (2017) 41:450–7. doi: 10.1038/ijo.2016.225
12. Ludwig DS. The glycemic indexphysiological mechanisms relating to obesity, diabetes, and cardiovascular disease. JAMA. (2002) 287:2414–23. doi: 10.1001/jama.287.18.2414
13. Liu S, Manson JAE, Buring JE, Stampfer MJ, Willett WC, Ridker PM. Relation between a diet with a high glycemic load and plasma concentrations of highsensitivity C-reactive protein in middle-aged women1-3. Am J Clin Nutr. (2002) 75:492–8. doi: 10.1093/ajcn/75.3.492
14. Livesey G, Taylor R, Livesey HF, Buyken AE, Jenkins DJA, Augustin LSA, et al. Dietary glycemic index and load and the risk of type 2 diabetes: a systematic review and updated meta-analyses of prospective cohort studies. Nutrients. (2019) 11:1280. doi: 10.3390/nu11061280
15. Bhupathiraju SN, Tobias DK, Malik VS, Pan A, Hruby A, Manson JE, et al. Glycemic index, glycemic load, and risk of type 2 diabetes: results from 3 large US cohorts and an updated meta-analysis. Am J Clin Nutr. (2014) 100:218–32. doi: 10.3945/ajcn.113.079533
16. Livesey G, Livesey H. Coronary heart disease and dietary carbohydrate, glycemic index, and glycemic load: dose-response meta-analyses of prospective cohort studies. Mayo Clin Proc Innov Qual Outcomes. (2019) 3:52–69. doi: 10.1016/j.mayocpiqo.2018.12.007
17. de Koning L, Malik VS, Kellogg MD, Rimm EB, Willett WC, Hu FB. Sweetened beverage consumption, incident coronary heart disease, and biomarkers of risk in men. Circulation. (2012) 125:1735–41. doi: 10.1161/CIRCULATIONAHA.111.067017
18. Nilson EAF, da Santin Andrade R, de Brito DA, de Oliveira ML. Costs attributable to obesity, hypertension, and diabetes in the Unified Health System, Brazil, 2018. Pan Am J Public Health. (2020) 44:1. doi: 10.26633/RPSP.2020.32
19. Nilson EAF, Pearson-Stuttard J, Collins B, Guzman-Castillo M, Capewell S, O’Flaherty M, et al. Estimating the health and economic effects of the voluntary sodium reduction targets in Brazil: microsimulation analysis. BMC Med. (2021) 19:225. doi: 10.1186/s12916-021-02099-x
20. Abbafati C, Machado DB, Cislaghi B, Salman OM, Karanikolos M, McKee M, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. (2020) 396:1204–22. doi: 10.1016/S0140-6736(20)30925-9
21. Abbafati C, Machado DB, Cislaghi B, Salman OM, Karanikolos M, McKee M, et al. Global burden of 87 risk factors in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. (2020) 396:1223–49.
22. Afshin A, Sur PJ, Fay KA, Cornaby L, Ferrara G, Salama JS, et al. Health effects of dietary risks in 195 countries, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. (2019) 393:1958–72.
23. Stanaway JD, Afshin A, Gakidou E, Lim SS, Abate D, Abate KH, et al. Global, regional, and national comparative risk assessment of 84 behavioral, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Stuy. Lancet. (2018) 392:1923–94.
24. Imamura F, O’Connor L, Ye Z, Mursu J, Hayashino Y, Bhupathiraju SN, et al. Consumption of sugar sweetened beverages, artificially sweetened beverages, and fruit juice and incidence of type 2 diabetes: systematic review, meta analysis, and estimation of population attributable fraction. BMJ. (2015) 351:1–12. doi: 10.1136/bmj.h3576
25. Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM, et al. Global burden of cardiovascular diseases and risk factors, 1990-2019: update from the GBD 2019 study. J Am Coll Cardiol. (2020) 76:2982–3021.
26. de Rezende LFM, Eluf-Neto J. Population attributable fraction: planning of diseases prevention actions in Brazil. Rev Saude Publica. (2016) 50:1–6. doi: 10.1590/S1518-8787.2016050006269
27. de Oliveira ML, Santos LMP, da Silva EN. Methodological bases for cost-ofillness studies in Brazil. Rev Nutr. (2014) 27:585–95. doi: 10.1590/1415-52732014000500007
28. de Siqueira ASE, De Siqueira-Filho AG, Land MGP. Analysis of the economic impact of cardiovascular diseases in the last five years in Brazil. Arq Bras Cardiol. (2017) 109:39–46. doi: 10.5935/abc.20170068
29. De Freitas Saldanha R, Bastos RR, Barcellos C. Microdatasus: a package for downloading and preprocessing microdata from Brazilian Health Informatics Department (DATASUS). Cad Saude Publica. (2019) 35:1–9. doi: 10.1590/0102-311X00032419
30. Ministry of Health. Bulletin Health Economics | Executive Secretariat | Ministry of Health. Brasilia: Virtual Health Library of the Ministry of Health (2021).
31. Ding D, Lawson KD, Kolbe-Alexander TL, Finkelstein EA, Katzmarzyk PT, van Mechelen W, et al. The economic burden of physical inactivity: a global analysis of major non-communicable diseases. Lancet. (2016) 388:1311–24. doi: 10.1016/S0140-6736(16)30383-X
32. Sánchez-Romero LM, Canto-Osorio F, González-Morales R, Colchero MA, Ng SW, Ramírez-Palacios P, et al. Association between tax on sugar sweetened beverages and soft drink consumption in adults in Mexico: open cohort longitudinal analysis of Health Workers Cohort Study. BMJ. (2020) 369:m1311. doi: 10.1136/bmj.m1311
33. Ferretti F, Mariani M. Sugar-sweetened beverage affordability and the prevalence of overweight and obesity in a cross section of countries. Global Health. (2019) 15:1–14. doi: 10.1186/s12992-019-0474-x
34. Mariath AB, Martins APB. Decade of action on nutrition and taxation of sugary drinks in Brazil: where are we? Cad Saude Publica. (2021) 37:e00157220. doi: 10.1590/0102-311X00157220
35. Pan American Health Organization, Act Health Promotion. Taxation of Sweetened Beverages in Brazil Taxation of Sweetened Beverages in Brazil. Washington, DC: Pan American Health Organization (2021). p. 1–53.
36. Malta DC, De Azeredo Passos VM, Machado ÍE, Marinho Souza MDF, Ribeiro ALP. The GBD Brazil network: better information for health policy decisionmaking in Brazil. Popul Health Metr. (2020) 18(Suppl 1):4–6.
37. StopaI SR, Deborah Carvalho MaltaII CNM, Célia Landmann Szwarcwald MG. Access and use of health services by the Brazilian population, National Health Survey 2013. Rev Saude Publica. (2017) 51:1s–11s. doi: 10.1590/s1518-8787.2017051000074
38. Malta DC, Duncan BB, Schmidt MI, Teixeira R, Ribeiro ALP, Felisbino-Mendes MS, et al. Trends in mortality due to non-communicable diseases in the Brazilian adult population: National and subnational estimates and projections for 2030. Popul Health Metr. (2020) 18(Suppl 1):1–14. doi: 10.1186/s12963-020-00216-1
39. DATASUS. Ministério Da Saúde Datasus. (2022). Available online at: https://datasus.saude.gov.br/informacoes-de-saude-tabnet/ (accessed November 08, 2022).
40. Pedraza LS, Popkin BM, Batis C, Adair L, Robinson WR, Guilkey DK, et al. The caloric and sugar content of beverages purchased at different store-types changed after the sugary drinks taxation in Mexico. Int J Behav Nutr Phys Act. (2019) 16:1–11. doi: 10.1186/s12966-019-0872-8
41. Ministry of Health/National Health Surveillance Agency. Resolution of the Collegiate Board of Directors - RDC 429 of October 08, 2020. Brazil: Brazilian Health Regulatory Agency (2020). p. 1–15.
Keywords: cost of illness, nutritional epidemiology, sugar-sweetened beverage, chronic non-communicable diseases, burden of disease
Citation: Leal JSV, Fogal AS, Meireles AL, Cardoso LdO, Machado ÍE and Menezes MCd (2022) Health economic impacts associated with the consumption of sugar-sweetened beverages in Brazil. Front. Nutr. 9:1088051. doi: 10.3389/fnut.2022.1088051
Received: 02 November 2022; Accepted: 30 November 2022;
Published: 19 December 2022.
Edited by:
Eduardo Augusto Fernandes Nilson, Center for Epidemiological Research in Nutrition and Health, Faculty of Public Health, University of São Paulo, BrazilReviewed by:
Naseem Alshwaiyat, Sultan Zainal Abidin University, MalaysiaCopyright © 2022 Leal, Fogal, Meireles, Cardoso, Machado and Menezes. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mariana Carvalho de Menezes, ✉ bWFyaWFuYS5tZW5lemVzQHVmb3AuZWR1LmJy
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.