 Barbara Virginia Caixeta Crepaldi1
Barbara Virginia Caixeta Crepaldi1 Letícia Martins Okada1
Letícia Martins Okada1 Rafael Moreira Claro2
Rafael Moreira Claro2 Maria Laura da Costa Louzada3
Maria Laura da Costa Louzada3 Leandro F. M. Rezende4Renata Bertazzi Levy5
Leandro F. M. Rezende4Renata Bertazzi Levy5 Catarina Machado Azeredo1*
Catarina Machado Azeredo1*- 1Programa de Pós-Graduação em Ciências da Saúde, Faculdade de Medicina, Universidade Federal de Uberlândia, Uberlândia, MG, Brazil
- 2Departamento de Nutrição, Escola de Enfermagem, Universidade Federal de Minas Gerais, Belo Horizonte, MG, Brazil
- 3Departamento de Nutrição da Faculdade de Saúde Pública, Universidade de São Paulo, São Paulo, SP, Brazil
- 4Departamento de Medicina Preventiva, Escola Paulista de Medicina, Universidade Federal de São Paulo, São Paulo, SP, Brazil
- 5Departamento de Medicina Preventiva, Faculdade de Medicina, Universidade de São Paulo, São Paulo, SP, Brazil
Background: It remains uncertain how the intersection between educational, gender, and race/skin color inequalities influences food consumption in Brazil. In this study, we examined the educational inequality in the consumption of in natura/minimally processed and ultra-processed foods by Brazilians with an intersectional perspective between sex and race/color.
Methods: We used cross-sectional data from the Telephone Surveillance System (VIGITEL 2019), comprising 52,443 participants ≥ 18 years. Daily food consumption was considered high when consumption of ≥5 foods for each food group was reported the day before the survey. Educational inequality in food consumption was assessed by the slope index of inequality (SII) and the relative index of inequality (RII) according to sex and race/color (White; Black/Brown). Positive SII and RII values > 1.0 indicate higher food consumption among more educated participants.
Results: The consumptions of in natura/minimally processed and ultra-processed foods were more prevalent in those with the highest level of education (≥12 years) and intermediate education (9–11 years), respectively. However, highly educated White women had higher consumption of in natura/minimally processed foods than Black women with the same education level, and White men in low and intermediate school levels had higher consumption of these foods than Black men with the same education levels. We found higher absolute educational inequality for in natura/minimally processed foods among White women (SII 21.8, 95% CI 15.3, 28.4) and Black/Brown men (SII 19.3, 95% CI 12.5, 26.1). Black/Brown men (SII 7.3, 95% CI 0.5, 14.0) and Black/Brown women (SII 5.6, 95% CI 1.0, 10.2) had higher absolute educational inequality than White men (SII −3.3, 95% CI −10.9, 4.3; P = 0.04) in the consumption of ultra-processed foods.
Conclusion: Educational inequalities influenced the consumption of in natura/minimally processed more than ultra-processed foods, and, for the latter, inequalities were greater among Black/Brown men and women than among White men.
Introduction
The participation of ultra-processed foods in diet has grown in the last few decades in different countries, especially in low- and middle-income countries (1, 2). In Brazil, for example, in natura or minimally processed foods have being intensely replaced by ultra-processed foods (3, 4). Ultra-processed foods are formulations of many ingredients, mainly of industrial use exclusively, which contain little or no intact food in their composition. These products are often added with a series of additives that provide attractive sensory attributes, such as texture, smell, and/or taste (5). The increasing consumption of ultra-processed foods is problematic because results in a general deterioration in the dietary nutritional profile and increases the risk of developing non-communicable diseases (NCDs) (6, 7).
The socioeconomic level, assessed mainly by income and educational attainment, is one of the major determinants of populational dietary patterns. In low- and middle-income countries, higher educational attainment, and income have been associated both with healthier dietary patterns (with higher consumption of fruits and vegetables and whole grains), but also with a higher intake of ultra-processed foods, such as sweets and candies, concomitantly, and paradoxically (8–11). In Brazil, despite the paradoxical pattern, the consumption of some ultra-processed foods, such as instant noodles and reconstituted meat products, is already more frequent among socially disadvantaged individuals (12).
Concomitantly, other sociodemographic characteristics, such as sex and/or skin color, also exert a great influence on populational dietary patterns (9). Brown men and women have lower regular consumption of fruits and vegetables compared to their White counterparts, and Black/Brown men have a higher regular consumption of beans when compared to White men (13). However, these comparisons between sex-skin color groups have not properly considered differences in socioeconomic level (13, 14). Socioeconomic inequalities observed in Brazil may interact and overlap with the race/color and sex dimensions (15). There is limited understanding of how the intersectional nature of sex and skin color/race determines the magnitude of socioeconomic inequalities in food consumption of individuals. The perspectives of intersectionality consider that the dimensions of inequality, such as race/color and sex, are interact and interdependent, and that these are experienced simultaneously (16, 17). Social inequalities in food consumption should be considered for NCDs prevention and control in low- and middle-income countries (10). Monitoring of food consumption and the interaction of equity stratifiers (education, sex, and race/color) can contribute to the development of equitable health policies.
In this study, we aimed to identify and quantify the magnitude of educational inequalities in the consumption of in natura/minimally processed and ultra-processed foods among Brazilians in 2019, according to the intersection between sex and race/skin color.
Methods
Study population, sampling, and data source
We used data from participants of the Brazilian Surveillance of Risk and Protective Factors for Chronic Diseases through Telephone Interviews (VIGITEL 2019), adults 18 years or older, residing in households with a landline in the 26 Brazilian state capitals and the Federal District. VIGITEL is a cross-sectional monitoring system for the frequency and distribution of the main determinants of NCDs, managed by the Brazilian Ministry of Health (18).
The sampling process consisted of drawing telephone lines by city, stratified by zip code, followed by drawing an individual residing in a selected household. The sample was weighted in order to minimize possible sampling biases, considering the non-universal coverage of the fixed telephone system and the difference in the probability of each individual being selected for the study. A final weight was assigned to each respondent, considering the inverse of the number of telephone lines in the respondent’s household, the number of adults living in the household, and a third factor aiming to match the sociodemographic composition of the sample (sex, education, and age) in each city in 2019 to that of the entire population [based on official projection (Brazilian Institute of Geography and Statistics – IBGE] (Rake Method) (18). The final weight assigned to each interviewed participant (Rake Method), allows the correspondence of the population of individuals aged 18 years or more in each city, with and without fixed telephone line, in 2019 (18).
In the main analyses, we used data from the total sample (52,443 adults). The participants who did not know or did not want to inform their educational level (n 743; 1.4% of the initial sample) had their data imputed by VIGITEL, from the most frequently observed value considering sex and age (19). Information regarding self-declaration of race/skin color was audited for participants answering “others,” in order to standardize the classification of synonyms, especially frequent in the case of Brown individuals (people who declared themselves, for example, morenos). At the end of the audit, the Black and Brown categories were grouped.
In the subgroup analysis by sex and race/skin color, participants who declared themselves Yellow (n 427; 0.8% of the initial sample) and Indigenous (n 617; 1.2% of the initial sample) were excluded due to the low frequency, which limits the power to detect significant differences within the group. In these analyses, participants who did not know or did not want to declare their race/skin color (n 1.163; 2.2% of the initial sample) were also excluded, totaling 50,236 included participants.
Study variables
Consumption of in natura/minimally processed and ultra-processed foods
Consumption of in natura/minimally processed (fruits, vegetables, roots and tubers, grains, legumes, meat, eggs, milk, nuts, and seeds) were evaluated in relation to the day before the interview, representing markers of healthy eating (18). In addition, consumption of ultra-processed foods (soft drinks, artificial juices, powdered drink mixes, powdered chocolate milk mix, flavored yogurt, salty snacks, sweet cookies and cake, sweet desserts, reconstituted meat products, bread, sauces, margarine, and ready-to-heat products) were evaluated in relation to the day before the interview, representing markers of unhealthy eating (18). The two food groups relied on the NOVA classification, which categorizes foods according to the extent and purpose of their processing (5). More details about the foods included in the in natura/minimally processed and ultra-processed food groups are provided in Supplementary material 1.
Food consumption was assessed through the following question: “Now I am going to list some foods and I would like you to tell me if you ate any of them yesterday (from when you woke up to when you went to sleep).” In order to assess the consumption of in natura/minimally processed and ultra-processed foods, respectively, the instruction was followed by questions in the following format: “I will start with in natura or staple foods [specific foods mentioned in the interview, described in Supplementary material 1] (yes or no),” and “Now I will list industrialized foods or products [specific foods mentioned in the interview, described in Supplementary material 1] (yes or no)” (18). The food questionnaire used by VIGITEL 2019 was based on instruments with satisfactory validity in Brazil, as documented by Sattamini (20).
A daily consumption equal to or higher than 5 different foods for each food group (in natura/minimally processed foods and ultra-processed foods) was considered as “high consumption,” in compliance with the assessment parameter adopted by VIGITEL (18). In the Brazilian context, a consumption equal to or greater than 5 groups of ultra-processed foods reflects a participation of about 44.0% of ultra-processed foods in the total caloric value of the diet (21).
Equity stratifiers
Food consumption was described according to years of schooling (0–3; 4–8; 9–11; ≥12 years) and the intersection between sex and race/skin color (White men; Black/Brown men; White women; Black/Brown women).
The categories of school level we used, are based on Brazilian cutoffs for illiterate/less than primary school (0–3 years of study), primary (elementary) school (4–8 years), secondary (middle) school (9–11 years) and higher education (≥12 years of study). In Brazil there is a marked difference between job types and income level based on these categories of education, thus we used these categories to capture not only the role of education, per se, but also indirectly the role of income. In addition to the use of complex measures of inequality that consider all levels of education, we aimed to verify the frequency of consumption of in natura/minimally processed foods and ultra-processed foods according to years of education. Considering that the different levels of education may present differences in food consumption, the use of ordered stratifiers with more than two categories is more informative.
Statistical analysis
The sociodemographic characteristics and food consumption were expressed in means or relative frequencies for the total sample and subgroups with intersection between sex and race/color. For the presentation of inequalities in food consumption according to schooling in the total sample and subgroups, graphs of equiplot type were generated (Pelotas, Brazil).1
We calculated simple measures of inequality (22), such as absolute difference [most educated group (≥12 years of study) – least educated group (0–3 years of study)] and ratio (most educated group/least educated group) of the prevalence of consumption in natura/minimally processed and ultra-processed foods in the total sample and subgroups with intersection between sex and race/color.
Complex measures of inequality
The magnitude of inequality in food consumption was estimated based on the level of education (educational inequality) through absolute (slope index of inequality – SII) and relative differences (relative index of inequality – RII) (22).
The SII represents the difference in the prevalence of food consumption between the more educated and less educated groups (difference in prevalence), whereas the RII represents the ratio of the prevalence between these groups. SII and RII consider all levels of schooling in the population instead of just comparing the two most extreme groups of schooling (23). SII and RII were estimated based on education for the total sample of participants and the subgroups with the intersection between sex and race/skin color.
Slope index of inequality and RII were estimated through logistic regression, a more appropriate analysis in the presence of prevalence indicators (24). The obtained SII values were multiplied by 100, ranging from −100 to +100, to facilitate visualization and understanding of results. Negative SII values indicate that food consumption is more prevalent in less educated groups, while positive values indicate a higher prevalence in more educated groups. SII values equal to ± 100 express total inequality, whereas zero represents a situation of total equality (absence of inequality) (22).
In general, the RII measures assume positive values (23), in which values farther from than 1.0 reflect higher levels of inequality (25). Results higher than 1.0 indicate a concentration of food consumption among more educated individuals and values lower than 1.0, including negative values, indicate a gradient in favor of the less educated ones (23, 25). If there is no inequality, the RII assumes a value of 1.0 (25).
SII and RII values were estimated with 95% confidence intervals. We performed the t-test to analyze whether educational inequality in food consumption assessed by SII and RII differed between subgroups (considering all possible comparisons). Associations with a value of P < 0.05 were considered statistically significant.
Population attributable risk
In order to quantify inequality, we also calculated the population attributable risk, an absolute inequality measure that shows the possible improvement (in percentage points) in food consumption if all schooling categories had the same prevalence of food consumption as the most favored group (here considered ≥ 12 years of study) (22). The population attributable fraction, a relative inequality measure, represents the possible proportional improvement if there was no inequality between the categories of schooling. Higher results indicate more pronounced inequalities (22, 26).
Regarding population attributable risk, the prevalence of food consumption identified in the most favored group was subtracted from that in the total population (here considered for the total sample and the sample of each subgroup with intersection between sex and race/color). The population attributable fraction was obtained by dividing the absolute population attributable risk by the prevalence of food consumption in the total population (22).
Statistical analyses and graphs were performed using the Stata/SE software version 16 (StataCorp LLC, College Station, United States), considering the VIGITEL sample design for descriptive analyses (Stata’s survey module) and the weights of the sample in the estimation of SII and RII values.
Results
In our study population, 54.0% correspond to women and 55.2% of the participants self-declared as Black/Brown race/color. The mean age among total sample was about 43 years old (SD 16.7) and the most frequent education category was between 9 and 11 years of study (38.4%). The sociodemographic distribution of participants according to the intersecting subgroups between sex and race/color and the percent of consumption of each food group is presented in Table 1. We identified a higher prevalence of participants with education between 9 and 11 years of study among Black/Brown men and women while the most frequent education category among White men and women was 12 or more years of study. In general, the percent of high consumption of in natura/minimally processed foods (≥5 different foods on the previous day) was low (29.8%), especially among Black/Brown men (25.2%), White men (29, 6%), and Black/Brown women (29.7%). The high consumption of ultra-processed foods (≥5 different foods on the previous day) was observed in almost a fifth of the total sample (18.2%), with a higher frequency among Black/Brown men (23.8%) and White men (20.0%) (Table 1).

Table 1. Sociodemographic characteristics, prevalence of consumption of in natura/minimally processed foods and ultra-processed foods in Brazil.a
The consumption of in natura/minimally processed foods by the total sample and subgroups was lower among less-educated participants than the more educated ones. Although White men had a lower educational discrepancy, we observed an important educational gradient among White women (Figure 1A). At the highest level of education (≥12 years of study), White and Black/Brown men had a similar consumption frequency (approximately 34.0%). However, the prevalence of consumption was higher in less educated White men compared to Black/Brown men with intermediate education. Among more educated women, White women had a higher consumption frequency than Black/Brown women, especially when considering the highest level of education (41.6% vs. 35.4%). However, at the highest level of education, Black/Brown women had a consumption frequency similar to that of men (Black/Brown and White) (Figure 1A). In general, among the in natura/minimally processed foods included in this study, vegetables and nuts and seeds were the food categories that most clearly showed a pattern of consumption inequality favoring more educated individuals (see Supplementary material 2).
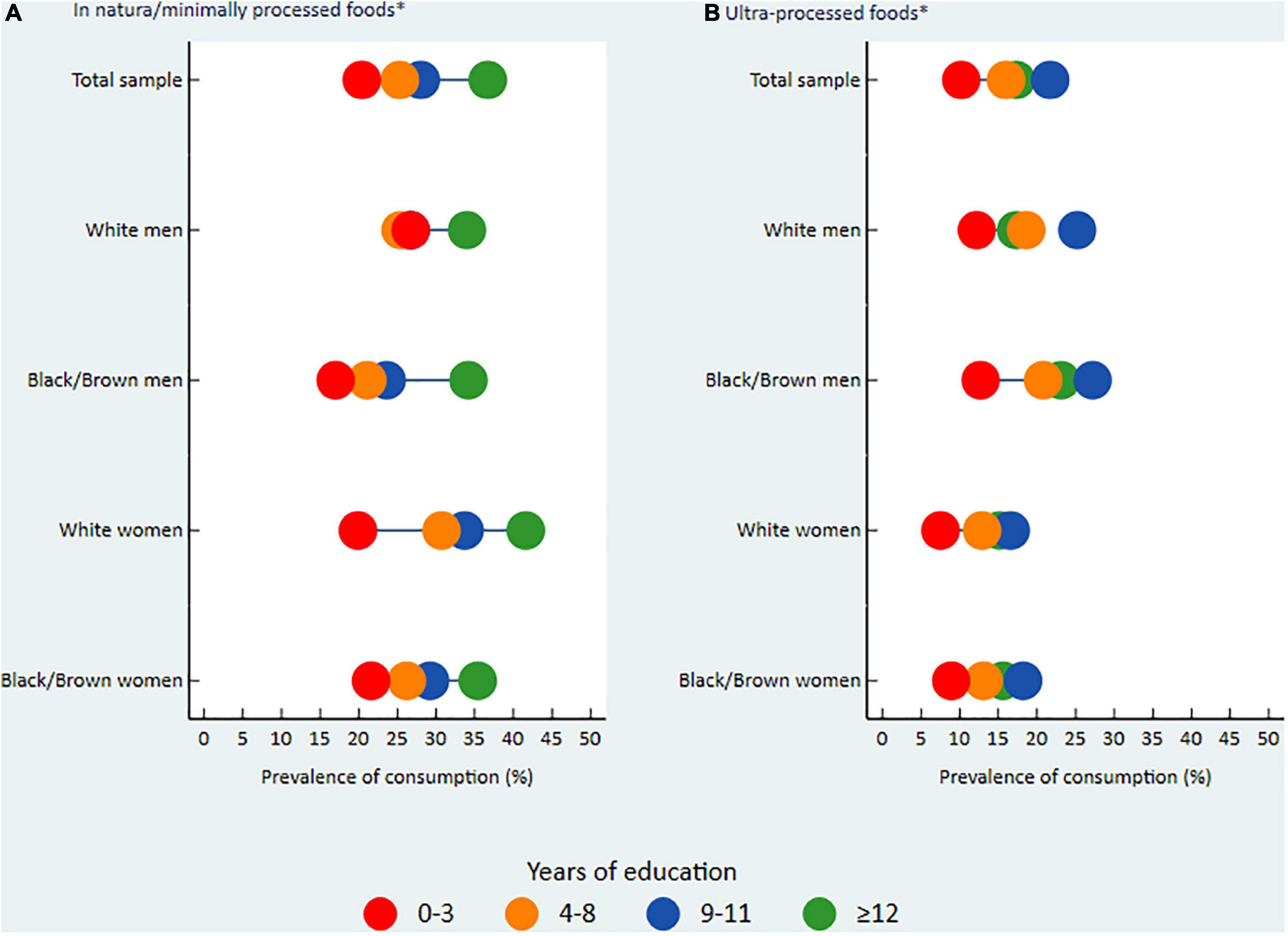
Figure 1. Prevalence of consumption of in natura/minimally processed foods (A) and ultra-processed foods (B) in Brazil.a VIGITEL, Surveillance of Risk and Protective Factors for Chronic Diseases through Telephone Interviews. aPrevalence of consumption of each food group [in natura/minimally processed foods (A) and ultra-processed foods (B)], by years of education and intersection of sex and skin color/race, VIGITEL 2019 (equiplot). *Consumption equal to or higher than 5 different foods from each food group, the day before the interview.
Differently, for the consumption of ultra-processed foods, a higher prevalence was identified among participants with intermediate education (9–11 years of study) in the total sample and subgroups. We observed a higher educational discrepancy between White and Black/Brown men. White men with intermediate education, and especially those with the highest level of education (≥12 years of study), had a lower frequency of consumption of ultra-processed foods compared to their respective Black/Brown counterparts (17.3% vs. 23.1% in the highest level of education). A slight educational discrepancy was observed between White and Black/Brown women (Figure 1B). The ultra-processed foods that were more frequently consumed by Brazilians were margarine and bread, with higher prevalence among participants with intermediate education and those with a higher level of education, respectively (see Supplementary material 3).
Among the most educated groups, the most frequent consumption of in natura/minimally processed foods and ultra-processed foods was also identified through positive SII results and RII results above 1.0 (Table 2). Educational inequality was higher for the consumption of in natura/minimally processed foods (SII 19.3, 95% CI 16.1, 22.5; RII 1.9, 95% CI 1.7, 2.1) than for ultra-processed foods (SII 3.6, 95% CI 0.7, 6.6; RII 1.2, 95% CI 1.0, 1.4), mainly identified by absolute measures. In general, the values found for the simple measures of inequality, difference, and ratio also confirmed that the consumption of these two food groups was more prevalent among more educated participants (Table 2).

Table 2. Consumption of in natura/minimally processed and ultra-processed foods, as well measures of inequality in Brazil.a
The consumption of in natura/minimally processed foods remained concentrated among the most educated individuals in all intersectional subgroups of sex and race/skin color. The magnitude of absolute and relative inequalities was higher in Black/Brown men (SII 19.3, 95% CI 12.5, 26.1; RII 2.2, 95% CI 1.5, 2.8) and White women (SII 21.8, 95% CI 15.3, 28.4; RII 1.9, 95% CI 1.5, 2.2). The population attributable risk results indicate that, if educational inequality were eliminated, the consumption of in natura/minimally processed foods would increase by 9.0 percentage points and 35.7% for Black/Brown men and 5.7 percentage points and 19.2% among Black/Brown women (Table 2).
In the analysis of the magnitude of educational inequality in the consumption of ultra-processed foods, we identified a significant absolute inequality for Black/Brown men (SII 7.3, 95% CI 0.5, 14.0) and Black/Brown women (SII 5.6, 95% CI 1.0, 10.2), but not for White men and women. However, we observed among White men a possibly higher consumption of ultra-processed foods in the least educated individuals (SII −3.3, 95% CI −10.9, 4.3; RII 0.9, 95% CI 0.5, 1.2). In the comparison between subgroups, Black/Brown men and women showed a higher absolute inequality in relation to White men (P = 0.04, for both). If educational inequality ceased to exist among White men, there would be a reduction of 2.7 percentage points and 13.5% in the consumption of ultra-processed foods (Table 2).
Discussion
The present study showed that the consumption of in natura/minimally processed foods was more prevalent in participants with a higher level of education, while that of ultra-processed foods was more frequent among those with intermediate education in the total sample and all analyzed subgroups with the intersection between sex and race/skin color. In middle-income countries, such as Brazil, the level of education influences the employability and income of the population (27, 28). Higher educational level impacts on a higher socioeconomic level (29), and influences healthy food choices even in the lower income population (30). In addition, considering that the price of healthy foods, such as fruits and vegetables, tends to be higher than the price of ultra-processed foods in Brazil (31), such factors may justify the more frequent consumption of in natura/minimally processed foods among the most educated in the present study. On the other hand, the more frequent consumption of ultra-processed foods among people with intermediate education (9–11 years of study) is possibly due to the considerable participation of this group in the informal labor market, characterized by intense working (32) that can make it difficult to buy and prepare food/drinks at home (33).
The consumption of in natura/minimally processed foods was the food group that showed the highest absolute educational inequality, especially between White women and Black/Brown men, while White men showed lower absolute and relative inequality. Additionally, in the consumption of ultra-processed food, Black/Brown men and women had a significantly higher absolute inequality than White men. Elimination of educational inequality would result in increased consumption of in natura/minimally processed foods of 36.0% for Black/Brown men and 19.0% for Black/Brown women. In addition, the elimination of educational inequality among White men would reduce the consumption of ultra-processed food by 13.5% in this group.
We identified that Black/Brown men with low to intermediate levels of education consumed less in natura/minimally processed foods than White men with lower levels of education. Considering that a higher level of education implies better wages in Brazil (27) and that having higher incomes increases the opportunity for adherence to the consumption of healthy foods (34), it would be expected that the intermediate education level of Black/Brown men would favor higher access to and consumption of these foods in relation to less educated White men. However, in a country marked by a historical and expressive racial inequality in social indicators, Black/Brown men only had the same prevalence of healthy food consumption as White men in the highest level of education. This result may be explained by the fact that, although the unemployment rate is higher among Black/Brown people than among White people, regardless of education, this difference is relatively smaller among those with a higher level of education, although the wage disadvantages remain expressive (27).
We identified that Black/Brown women with the highest level of education achieved the prevalence of consumption of in natura/minimally processed foods of their respective counterparts of White men and Black/Brown men, despite Black/Brown women having the worst work income in Brazil (for example, 44.4% of White men’s earnings) (35). Unequally, considering that education determined more the differences in the consumption of healthy foods among White women than among the other subgroups, we observed, in the highest level of education, an expressive lower frequency of consumption of healthy foods among Black/Brown women in relation to White women. Brazilian women have better educational indicators compared to men, and White women have higher work incomes than Black/Brown women (35). The greater education of women associated with higher income among White women may have contributed to the higher consumption of healthy foods in this group (11, 28, 36). Healthy eating patterns among Brazilian women, especially those with higher education and income, have been identified in other epidemiological studies (8, 9, 37).
We also identified an important privilege of White skin among more educated men, favoring a lower frequency of consumption of ultra-processed foods in relation to their Black/Brown male counterparts. While higher levels of education seem to facilitate the consumption of ultra-processed products among Black/Brown men and women, educational inequality among White men showed that the consumption of ultra-processed food already seems to reach the less socioeconomically advantaged population in a more concentrated manner. The White men’s wage advantages in relation to all subgroups (35) may have contributed to this finding.
The consumption of ultra-processed foods reaching White men with less education in a more concentrated manner and a slighter educational discrepancy in the subgroups for this food group reinforce the occurrence of the food transition process in Brazil (9), which has already occurred in developed countries (38, 39). The progression of the dietary pattern transition is characterized by higher consumption of cheaper, more caloric, and less nutritious foods at lower educational and income levels (1, 38, 39). In developing countries, such as Brazil, unhealthy food options are increasingly more accessible (40). On the other hand, healthy foods such as fruits and vegetables observed continuous increases in its price (40).
Projections of the price of healthy and unhealthy foods from 2017 to 2030 in Brazil, using data from 1995 to 2017, showed that the price difference between these foods reduced over time and forecasted that ultra-processed foods will become cheaper than in natura/minimally processed foods as of 2026 (41). This would increase barriers to the consumption of healthy foods (42) and encourage the consumption of unhealthy foods, specially by people with lower incomes, as a way to control expenditures (34), widening dietary and health inequalities. The growing participation of ultra-processed foods in the diet of the Brazilian population has been observed in recent decades (3), including in the most vulnerable populations (12). Data from the Brazilian Household Budget Surveys 2017-2018, show that ultra-processed foods already contribute about one-fifth (19.7%) of the calories consumed by Brazilians, and that the consumption of some ultra-processed foods, such as instant noodles and reconstituted meat products, is more frequent in the lowest income quartiles of the population (12). In addition to the economic factor, food consumption can be influenced by other issues such as cultural, ethnic, and perceived racial discrimination (14, 42).
Robust epidemiological evidence on negative health effects associated with the consumption of ultra-processed foods has been described (6). High consumption of ultra-processed foods has been associated with higher calorie intake, body fat gain (43), overweight/obesity risk (6), type-2 diabetes (44), breast cancer (45), cardiovascular diseases, depression, and mortality for all the causes (6). Specifically for obesity, a study in the North American population showed that, for all levels of education, the age-adjusted prevalence of overweight/obesity was 44.0% higher in Black women than in White women and 2.0% higher in Black men than in White men (46). Thus, the consumption of ultra-processed foods may increase overweight, especially in the Black population, with emphasis on women, accentuating health inequalities.
It is expected that the consumption of ultra-processed foods will become more frequent in more vulnerable populations within a few years, such as Black/Brown and less educated individuals, if intersectoral and effective interventions are not articulated and adopted quickly. The guidelines for promoting the consumption of healthy foods and discouraging the consumption of unhealthy foods must be accompanied by plausible cultural and economic strategies for population adherence, especially the less educated and poorer (34, 42), because the ongoing COVID-19 pandemic enhances social, racial, and gender inequalities that already exist in Brazil (47). Public policies aimed at subsidizing in natura or minimally processed foods (48), may be effective in increasing purchase and consumption power of these foods by the vulnerable population (48, 49). In addition, a favorable a food environment with a high density of healthy eating establishments, such as street markets, is needed (50).
In addition to subsidizing healthy foods, the taxation of ultra-processed foods may discourage their consumption, especially by the most vulnerable population (48, 49). In Brazil, the price of ultra-processed foods was inversely associated with the prevalence of overweight and obesity, especially protecting individuals with higher socioeconomic vulnerability (51). In the same way, food marketing regulation can also contribute to improving the quality of the population’s diet (49). A new labeling system was recently approved in Brazil, encompassing frontal nutrition labeling and a magnifying glass design to identify high nutrient content, including added sugars (52). Despite this, the Brazilian model differs from those adopted by other Latin American countries and jurisdictions in the United States, with scientific evidence of beneficial effects (53). Complementary measures are needed to reduce the persuasive advertising of ultra-processed foods on television and the internet, identified in Latin American countries, including Brazil (54–56).
Our results show the importance of ensuring access to better educational opportunities, with emphasis on the Black/Brown population, as a way to improve the quality of food consumption. It is noteworthy that, despite the growing participation of the Black/Brown population in higher education in recent years, due to the increase in the number of places and the policies of democratization of access to public higher education, the percentage of Black/Brown individuals with complete higher education is still low compared to White population (32.0% vs. 66.0% in 2017) (57, 58). In addition to the benefit of education in the employability and income of the population (27), knowledge, including specific to health (28), such as information on types and characteristics of foods that contribute to making them more or less healthy, may also influence an adequate diet (42).
Our study has some limitations. VIGITEL collected data from individuals with access to a landline residing in Brazilian state capitals and the Federal District. Although weighting factors have been used to mitigate this limitation, the inclusion of the population without a landline in the System (having only a cell phone) has the potential to impact the estimates, such as a higher frequency of consumption of some ultra-processed foods (59). There is a possibility that respondents have a higher socioeconomic level than the population of capitals in general, because, in Brazil, access to fixed telephone lines has been reduced in recent years (60), and more socioeconomically privileged families are more likely to have a landline (61). Nevertheless, we identified the presence of expressive educational inequalities with the intersection between sex and race/color in food consumption. We did not include participants who declared themselves either Yellow or Indigenous in the intersection analysis due to limited sample size. This study innovates and advances in the perspective of intersectionality, showing the overlapping of inequalities in food consumption in Brazil. Another limitation is that the self-reported information made available by VIGITEL is subject to misclassification. However, there is an indication of good reproducibility and adequate validity of indicators of food and beverage consumption obtained through telephone surveys (62). Although VIGITEL used a method based on a list of foods (simplified food questionnaire) and not the open 24-h dietary recall, the simplified version was based on instruments with satisfactory validity, and the lack of quantification of consumption did not impact the understanding of the quality of the diet in the healthy and unhealthy dimensions proposed by the instrument (20, 21).
The strengths of the study are the analysis of the magnitude of social inequality in the consumption of two food groups (in natura/minimally processed and ultra-processed foods) of the NOVA classification, which has become a world reference for effective assessment of the quality of diets and their consequences in all forms of malnutrition (1, 4, 5). We used complex measures of inequality that took into account all levels of education of the representative sample of the population of the state capitals and the Federal District of an upper-middle-income country (UMIC) (63). Furthermore, our study fills a gap in the literature on the role of the intersectionality of sex and race/skin color in food consumption.
The present study has important implications for public health as it identifies the magnitude with which social inequality presents itself and the groups that are the most vulnerable to the consumption of foods classified according to the degree of processing. Our results can subsidize policies that equitably guarantee the possibility of adopting the golden rule: “always prefer in natura or minimally processed foods and freshly made dishes and meals to ultra-processed foods” presented in the renowned Dietary Guidelines for the Brazilian Population, which has a language accessible to less educated people (42). A variety in the consumption of in natura and minimally processed foods and the reduction in the consumption of ultra-processed foods goes beyond the fundamental importance of promoting healthy eating for the population (20). It implies the promotion of an environmentally sustainable and socially fairer food system (42, 64), mitigating the deepening of social inequalities caused by the food system that produces ultra-processed products (42).
We conclude that the inequality in the consumption of in natura/minimally processed foods favors more educated individuals. The prevalence of consumption of ultra-processed foods is more concentrated among those with intermediate education. Educational inequalities influence more the consumption of healthy than unhealthy foods. Among the subgroups, Black/Brown men with intermediate education had lower consumption of in natura/minimally processed foods when compared to White men with lower education level, showing the impact of racism on diet. Absolute inequalities for the consumption of unhealthy foods presented a higher magnitude between Black/Brown men and women when compared to White men, which may drive inequalities in NCD. The increase in education could impact an expressive increase in the consumption of healthy foods in the Black/Brown population, and in the reduction in the consumption of unhealthy foods in White men, but without changes in Black/Brown women.
Data availability statement
The original contributions presented in this study are included in this article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by the National Research Ethics Commission (CONEP) of the National Health Council/Brazilian Ministry of Health: Certificate of Presentation and Ethical Appreciation (CAAE) number 65610017.1.0000.0008. The patients/participants provided their written informed consent to participate in this study.
Author contributions
BC and CA participated in the conception and design of the study, statistical analyses, data interpretation, and manuscript writing. RC and LO participated in the statistical analyses, data interpretation, manuscript writing, and review. LR, RL, RC, and ML participated in the interpretation of data, manuscript writing, and review. All authors carried out a critical review of the manuscript’s important intellectual content, approved the submitted final version, agreed to be responsible for all aspects of the work, and ensuring that issues related to the accuracy or integrity of any part of the work are investigated and resolved appropriately.
Funding
CA receives support from the Brazilian National Council for Scientific and Technological Development (CNPq, Brazil, N° 404905/2016-1 and N° 313491/2021-6) and LO receives support from CAPES Foundation.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2022.1055532/full#supplementary-material
Abbreviations
CAAE, Certificate of Presentation and Ethical Appreciation; CONEP, National Research Ethics Commission; IBGE, Brazilian Institute of Geography and Statistics; NCDs, non-communicable diseases; RII, relative inequality index; SII, slope of inequality index; UMIC, upper-middle-income country; VIGITEL, Surveillance of Risk and Protective Factors for Chronic Diseases through Telephone Interviews.
Footnotes
References
1. Monteiro CA, Cannon G, Moubarac J-C, Levy RB, Louzada MLC, Jaime PC. The UN Decade of Nutrition, the NOVA food classification and the trouble with ultra-processing. Public Health Nutr. (2017) 21:5–17. doi: 10.1017/S1368980017000234
2. Moodie R, Bennett E, Kwong EJL, Santos TM, Pratiwi L, Williams J, et al. Ultra-processed profits: the political economy of countering the global spread of ultra-processed foods - a synthesis review on the market and political practices of transnational food corporations and strategic public health responses. Int J Health Policy Manag. (2021) 10:968–82. doi: 10.34172/ijhpm.2021.45
3. Martins APB, Levy RB, Claro RM, Moubarac JC, Monteiro CA. Increased contribution of ultra-processed food products in the Brazilian diet (1987-2009). Rev Saude Publ. (2013) 47:656–65. doi: 10.1590/S0034-8910.2013047004968
4. Monteiro CA, Cannon G, Levy R, Moubarac J-C, Jaime P, Martins AP, et al. NOVA. The star shines bright. World Nutr. (2016) 7:28–38.
5. Monteiro CA, Cannon G, Levy RB, Moubarac J-C, Louzada ML, Rauber F, et al. Ultra-processed foods: what they are and how to identify them. Public Health Nutr. (2019) 22:936–41. doi: 10.1017/S1368980018003762
6. Pagliai G, Dinu M, Madarena MP, Bonaccio M, Iacoviello L, Sofi F. Consumption of ultra-processed foods and health status: a systematic review and meta-analysis. Br J Nutr. (2021) 125:308–18. doi: 10.1017/S0007114520002688
7. Louzada MLC, Martins APB, Canella DS, Baraldi LG, Levy RB, Claro RM, et al. Ultra-Processed Foods and the Nutritional Dietary Profile in Brazil. Rev Saúde Pública [Internet]. Faculdade de Saúde Pública da Universidade de São Paulo. (2015). Available online at: http://www.scielo.br/j/rsp/a/dm9XvfGy88W3WwQGBKrRnXh/?lang=en (accessed August 8, 2022).
8. Canuto R, Camey S, Gigante DP, Menezes AMB, Olinto MTA. Focused principal component analysis: a graphical method for exploring dietary patterns. Cad Saude Publ. (2010) 26:2149–56. doi: 10.1590/S0102-311X2010001100016
9. Canuto R, Fanton M, Lira PIC. Social inequities in food consumption in Brazil: a critical review of the national surveys. Cien Saude Colet. (2019) 24:3193–212. doi: 10.1590/1413-81232018249.26202017
10. Mayén A-L, Marques-Vidal P, Paccaud F, Bovet P, Stringhini S. Socioeconomic determinants of dietary patterns in low- and middle-income countries: a systematic review. Am J Clin Nutr. (2014) 100:1520–31. doi: 10.3945/ajcn.114.089029
11. Medina LPB, Barros MBA, Sousa NFS, Bastos TF, Lima MG. Szwarcwald CL. Social inequalities in the food consumption profile of the Brazilian population: national health survey, 2013. Rev Bras Epidemiol. (2019) 22:1–15. doi: 10.1590/1980-549720190015.supl.2
12. Instituto Brasileiro de Geografia e Estatística. Pesquisa de Orçamentos Familiares - POF 2017-2018 [Internet]. (2020). Available online at: https://www.ibge.gov.br/estatisticas/sociais/populacao/24786-pesquisa-de-orcamentos-familiares-2.html?edicao=28523&t=sobre (accessed October 16, 2020).
13. Malta DC, Moura L, Bernal RTI. Differentials in risk factors for chronic non-communicable diseases from the race/color standpoint. Cienc Saúde Coletiva. (2015) 20:713–25. doi: 10.1590/1413-81232015203.16182014
14. Rodrigues YE, Fanton M, Novossat RS, Canuto R. Perceived racial discrimination and eating habits: a systematic review and conceptual models. Nutr Rev. (2022) 80:1769–86. doi: 10.1093/nutrit/nuac001
15. Victora C. Socioeconomic inequalities in health: reflections on the academic production from Brazil. Int J Equity Health. (2016) 15:1–3. doi: 10.1186/s12939-016-0456-z
16. López N, Gadsden VL. Health Inequities, Social Determinants, and Intersectionality. Washington, DC: NAM Perspectives (2016). p. 1–15. doi: 10.31478/201612a
17. Davis A. As Mulheres Negras na Construção de Uma Nova Utopia. [Internet]. Portal Gelédes. (2011). Available online at: https://www.geledes.org.br/as-mulheres-negras-na-construcao-de-uma-nova-utopia-angela-davis/ (accessed May 16, 2021).
18. Brasil, Ministério da Saúde. Vigitel Brazil 2019: Surveillance of Risk and Protective Factors for Chronic Diseases by Telephone Survey: Estimates of Frequency and Sociodemographic Distribution of Risk and Protective Factors for Chronic Diseases in the Capitals of the 26 Brazilian STATES and the Federal District in 2019. [Internet]. Brasília: Ministério da Saúde (2020).
19. Bernal RTI, Iser BPM, Malta DC, Claro RM. Surveillance system for risk and protective factors for chronic diseases by telephone survey (Vigitel): changes in weighting methodology. Epidemiol Serv Saude. (2017) 26:701–12.
20. Sattamini I. Tools for Evaluating the Quality of Diets: Development, Adaptation and Validation in Brazil. São Paulo: Universidade de São Paulo (2019).
21. Costa CS, Faria FR, Gabe KT, Sattamini IF, Khandpur N, Leite FHM, et al. Nova Score for the Consumption of Ultra-Processed Foods: Description and Performance Evaluation in Brazil. Revista de Saúde Pública [Internet]. São Paulo: Faculdade de Saúde Pública da Universidade de São Paulo (2021).
22. World Health Organization. Handbook on Health Inequality Monitoring: With a Special Focus on Low- and Middle-Income Countries. Geneva: World Health Organization (2013).
23. Kim N-H, Kawachi I. Did the expansion of insurance coverage for oral health reduce self-reported oral health inequalities in Korea? Results of repeated cross-sectional analysis, 2007-2015. J Epidemiol. (2020) 30:537–41. doi: 10.2188/jea.JE20190119
24. Barros AJD, Victora CG. Measuring coverage in MNCH: determining and interpreting inequalities in coverage of maternal, newborn, and child health interventions. PLoS Med. (2013) 10:e1001390. doi: 10.1371/journal.pmed.1001390
25. Ferreira RC, Senna MIB, Rodrigues LG, Campos FL, Martins AEBL, Kawachi I. Education and income-based inequality in tooth loss among Brazilian adults: does the place you live make a difference? BMC Oral Health. (2020) 20:246. doi: 10.1186/s12903-020-01238-9
26. de Rezende LFM, Eluf J. Population attributable fraction: planning of diseases prevention actions in Brazil. Rev Saude Publ. (2016) 50:1–6. doi: 10.1590/S1518-8787.2016050006269
27. Instituto Brasileiro de Geografia e Estatística. Síntese de Indicadores Sociais: Uma Análise das Condições de vida da População Brasileira 2020. [Internet]. Rio de Janeiro: Instituto Brasileiro de Geografia e Estatística (2020).
29. Silva ICM, Restrepo-Mendez MC, Costa JC, Ewerling F, Hellwig F, Ferreira LZ, et al. Measurement of social inequalities in health: concepts and methodological approaches in the Brazilian context. Epidemiol Serv Saude. (2018) 27:1–11. doi: 10.5123/S1679-49742018000100017
30. Lins APM, Sichieri R, Coutinho WF, Ramos EG, Peixoto MVM, Fonseca VM. Healthy eating, schooling and being overweight among low-income women. Cien Saude Colet. (2013) 18:357–66. doi: 10.1590/S1413-81232013000200007
31. Claro RM, Maia EG, Costa BVL, Diniz DP. Food prices in Brazil: prefer cooking to ultra-processed foods. Cad Saúde Públ. (2016) 32:e00104715. doi: 10.1590/0102-311X00104715
32. Araújo AMC, Lombardi MR. Informal work, gender and race in Brazil in the early 21st century. Cad Pesqui. (2013) 43:452–77. doi: 10.1590/S0100-15742013000200005
33. Escoto KH, Laska MN, Larson N, Neumark-Sztainer D, Hannan PJ. Work hours and perceived time barriers to healthful eating among young adults. Am J Health Behav. (2012) 36:786–96. doi: 10.5993/AJHB.36.6.6
34. Drewnowski A. Obesity and the food environment: dietary energy density and diet costs. Am J Prev Med. (2004) 27:154–62. doi: 10.1016/j.amepre.2004.06.011
35. Instituto Brasileiro de Geografia e Estatística. Desigualdades Sociais por Cor ou Raça no Brasil [Internet]. (2019). Rio de Janeiro: Instituto Brasileiro de Geografia e Estatística. (accessed April, 2021).
36. Story M, Kaphingst KM, Robinson-O’Brien R, Glanz K. Creating healthy food and eating environments: policy and environmental approaches. Annu Rev Public Health. (2008) 29:253–72. doi: 10.1146/annurev.publhealth.29.020907.090926
37. Lenz A, Olinto MTA, Dias-da-Costa JS, Alves AL, Balbinotti M, Pattussi MP, et al. Socioeconomic, demographic and lifestyle factors associated with dietary patterns of women living in Southern Brazil. Cad Saude Publ. (2009) 25:1297–306. doi: 10.1590/S0102-311X2009000600012
38. Drewnowski A. The cost of US foods as related to their nutritive value. Am J Clin Nutr. (2010) 92:1181–8. doi: 10.3945/ajcn.2010.29300
39. Morris MA, Hulme C, Clarke GP, Edwards KL, Cade JE. What is the cost of a healthy diet? Using diet data from the UK Women’s cohort study. J Epidemiol Community Health. (2014) 68:1043–9. doi: 10.1136/jech-2014-204039
40. Overseas Development Institute. The Rising Cost of a Healthy Diet: Changing Relative Prices of Foods in High-Income and Emerging Economies. [Internet]. (2015). London: Overseas Development Institute.
41. Maia EG, Dos Passos CM, Levy RB, Bortoletto Martins AP, Mais LA, Claro RM. What to expect from the price of healthy and unhealthy foods over time? The case from Brazil. Public Health Nutr. (2020) 23:579–88. doi: 10.1017/S1368980019003586
42. Brasil, Ministério da Saúde. Dietary Guidelines for the Brazilian Population. [Internet]. (2014). Available online at: http://bvsms.saude.gov.br/bvs/publicacoes/guia_alimentar_populacao_brasileira_2ed.pdf (accessed May 26, 2021).
43. Hall KD, Ayuketah A, Brychta R, Cai H, Cassimatis T, Chen KY, et al. Ultra-processed diets cause excess calorie intake and weight gain: an inpatient randomized controlled trial of ad libitum food intake. Cell Metab. (2019) 30:67–77.e3. doi: 10.1016/j.cmet.2019.05.008
44. Levy RB, Rauber F, Chang K, Louzada MLC, Monteiro CA, Millett C, et al. Ultra-processed food consumption and type 2 diabetes incidence: a prospective cohort study. Clin Nutr. (2020). 40:3608–14. doi: 10.1016/j.clnu.2020.12.018
45. Fiolet T, Srour B, Sellem L, Kesse-Guyot E, Allès B, Méjean C, et al. Consumption of ultra-processed foods and cancer risk: results from NutriNet-Santé prospective cohort. BMJ Br Med J Publ Group. (2018) 360:1–11. doi: 10.1136/bmj.k322
46. Jackson CL, Szklo M, Yeh H-C, Wang N-Y, Dray-Spira R, Thorpe R, et al. Black-white disparities in overweight and obesity trends by educational attainment in the United States, 1997-2008. J Obes. (2013) 2013:1–9. doi: 10.1155/2013/140743
47. Alpino TMA, Santos CRB, Barros DC, Freitas CM. COVID-19 and food and nutritional (in)security: action by the Brazilian Federal Government during the pandemic, with budget cuts and institutional dismantlement. Cad Saúde Públ. (2020) 36:e00161320. doi: 10.1590/0102-311x00161320
48. World Health Organization. Fiscal Policies for Diet and Prevention of Noncommunicable Diseases [Internet]. Geneva: World Health Organization (2016).
49. FAO, IFAD, UNICEF, WFP, WHO. The State of Food Security and Nutrition in the World 2020 | FAO | Food and Agriculture Organization of the United Nations [Internet]. (2020). Available online at: http://www.fao.org/publications/sofi/2020/en/ (accesssed October 22, 2020).
50. Pessoa MC, Mendes LL, Gomes CS, Martins PA, Velasquez-Melendez G. Food environment and fruit and vegetable intake in a urban population: a multilevel analysis. BMC Public Health. (2015) 15:1012. doi: 10.1186/s12889-015-2277-1
51. Passos CMD, Maia EG, Levy RB, Martins APB, Claro RM. Association between the price of ultra-processed foods and obesity in Brazil. Nutr Metab Cardiovasc Dis. (2020) 30:589–98. doi: 10.1016/j.numecd.2019.12.011
52. Brasil, Agência Nacional de Vigilância Sanitária. Anvisa aprova norma sobre rotulagem nutricional [Internet]. Agência Nacional de Vigilância Sanitária - Anvisa. (2020). Available online at: https://www.gov.br/anvisa/pt-br/assuntos/noticias-anvisa/2020/aprovada-norma-sobre-rotulagem-nutricional (accessed November 2, 2020).
53. Grummon AH, Hall MG. Sugary drink warnings: a meta-analysis of experimental studies. PLoS Med. (2020) 17:e1003120. doi: 10.1371/journal.pmed.1003120
54. Antúnez L, Alcaire F, Brunet G, Bove I, Ares G. COVID-washing of ultra-processed products: the content of digital marketing on Facebook during the COVID-19 pandemic in Uruguay. Public Health Nutr. (2021) 24:1142–52. doi: 10.1017/S1368980021000306
55. Guimarães JS, Mais LA, Marrocos Leite FH, Horta PM, Oliveira Santana M, Martins APB, et al. Ultra-processed food and beverage advertising on Brazilian television by international network for food and obesity/non-communicable diseases research, monitoring and action support benchmark. Public Health Nutr. (2020) 23:2657–62. doi: 10.1017/S1368980020000518
56. Santana MO, Guimarães JS, Leite FHM, Mais LA, Horta PM, Bortoletto Martins AP, et al. Analysing persuasive marketing of ultra-processed foods on Brazilian television. Int J Public Health. (2020) 65:1067–77. doi: 10.1007/s00038-020-01456-6
57. Instituto Brasileiro de Geografia e Estatística. Pesquisa Nacional por Amostra de Domicílios Contínua - PNAD Contínua | IBGE [Internet]. (2018). Available online at: https://www.ibge.gov.br/estatisticas/sociais/populacao/17270-pnad-continua.html?edicao=20915&t=publicacoes (accessed March 20, 2021).
58. Instituto de Pesquisa Econômica Aplicada. TD 2569 - Ação Afirmativa e População Negra na Educação Superior: Acesso e Perfil Discente [Internet]. (2020). Available online at: https://www.ipea.gov.br/portal/index.php?option=com_content&view=article&id=35893 (accessed March 20, 2021).
59. Bernal RTI, Malta DC, Claro RM, Monteiro CA. Effect of the inclusion of mobile phone interviews to Vigitel. Rev Saude Publ. (2017) 51:1s–12s. doi: 10.1590/s1518-8787.2017051000171
60. Agência Nacional de Telecomunicações. Anatel - Telefonia Fixa [Internet]. (2020). Available online at: https://www.anatel.gov.br/paineis/acessos/telefonia-fixa (accessed December 3, 2020).
61. Bernal RTI, Malta DC, de Araujo TS, da Silva NN. Telephone survey: poststratification adjustments to compensate noncoverage bias in city of Rio Branco, Northern Brazil. Rev Saude Publ. (2013) 47:316–25. doi: 10.1590/S0034-8910.2013047003798
62. Monteiro CA, Moura EC, Jaime PC, Claro RM. Validity of food and beverage intake data obtained by telephone survey. Rev Saude Publ. (2008) 42:582–9. doi: 10.1590/S0034-89102008000400002
63. World Bank Country and Lending Groups. World Bank Data Help Desk [Internet]. (2020). Available online at: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed August 10, 2020).
Keywords: food consumption, NOVA, social inequalities, ultra-processed food, intersectionality
Citation: Crepaldi BVC, Okada LM, Claro RM, Louzada MLdC, Rezende LFM, Levy RB and Azeredo CM (2022) Educational inequality in consumption of in natura or minimally processed foods and ultra-processed foods: The intersection between sex and race/skin color in Brazil. Front. Nutr. 9:1055532. doi: 10.3389/fnut.2022.1055532
Received: 27 September 2022; Accepted: 17 November 2022;
Published: 08 December 2022.
Edited by:
Raquel Mendonça, Universidade Federal de Ouro Preto, BrazilReviewed by:
Júlia Carraro, Universidade Federal de Ouro Preto, BrazilEmyr Reisha Isaura, Airlangga University, Indonesia
Copyright © 2022 Crepaldi, Okada, Claro, Louzada, Rezende, Levy and Azeredo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Catarina Machado Azeredo, Y2F0YXJpbmEuYXplcmVkb0B1ZnUuYnI=