 Ruiyao CaoJiaoyan ChenYuanyuan WangXingwang PengMei Han
Ruiyao CaoJiaoyan ChenYuanyuan WangXingwang PengMei Han Keke LiuJuan ZhangRongying YaoHui Han
Keke LiuJuan ZhangRongying YaoHui Han Lianguo Fu*
Lianguo Fu*- Department of Child and Adolescent Health, School of Public Health, Bengbu Medical College, Bengbu, China
Background: Negative gender cognitive attitudes (disliking one’s own gender or wanting to be the opposite gender) and unhealthy eating behaviors have become common in Chinese children and adolescents. The aim of this study was to analyze the associations between negative gender attitudes and eating behaviors among Chinese children and adolescents.
Methods: Primary and secondary school students aged 8–15 years were selected as participants using a stratified cluster random sampling method. The self-designed questionnaire was used to investigate the participants’ negative gender cognitive attitudes. Eating frequency questionnaire was used to investigate participants’ eating behaviors. Under the leading reading of standardized training investigators, the questionnaire for children aged 8–15 years was completed by themselves in the form of centralized filling.
Results: A total of 6.5% [43/657, boys: 6.1% (21/347), girls: 7.1% (22/310)] of children disliked their own gender, 8.8% [58/657, boys: 5.5% (19/347), girls: 12.6% (39/310)] of children wanted to be of the opposite gender, and the proportion of girls with negative gender attitudes was higher than that of boys (P < 0.05). Boys who disliked their own gender or wanted to be the opposite gender had higher frequencies of unhealthy eating behaviors and lower frequencies of healthy eating behaviors than boys who liked their own gender or did not want to be the opposite gender (P < 0.05). Girls who disliked their own gender or wanted to be the opposite gender had higher frequencies of protein eating behaviors than girls who liked their own gender or did not want to be the opposite gender (P < 0.05). There was a significant interaction between disliking one’s own gender and wanting to be the opposite gender in midnight snack eating among boys (P < 0.05) and in carbonated drink and high protein eating behaviors among girls (P < 0.05).
Conclusion: Boys with negative gender cognitive attitudes express more unhealthy eating behaviors and fewer healthy eating behaviors; girls with negative gender cognitive attitudes exhibit more protein eating behaviors.
Introduction
The gender role is the construction of gender attitudes, behaviors, cognitions and emotions in a specific cultural background (1). Most children’s gender experience of being male or female is in line with the gender assigned at birth, but inconsistencies can lead to gender dysphoria (2). Children who have a strong desire to be another gender are defined as children with gender dysphoria (3, 4). A study among Dutch children showed that 1.4% of boys wished to be of the opposite gender, and 2.0% of girls wished to be of the opposite gender (5). Recent studies suggested that the prevalence of a self-reported transgender identity in children and adolescents ranges from 0.5 to 1.3% and is more prominent among girls than boys (6). Compared with children without gender dysphoria, children with gender dysphoria have a higher risk of eating disorders (7, 8). Some studies in Canadian adolescents showed that 5% of adolescents with gender dysphoria had eating disorders (9). Transgender adolescents participate in negative eating behaviors to change their appearance or modify their bodies to adapt to their gender identity (10). The increase in disordered eating behaviors will lead to higher dissatisfaction with their bodies (11) and contribute to adolescents becoming sexual minorities. Gender role orientation plays an important role in adolescent eating disorders (12). Some children and adolescents may not be defined as gender dysphoric, but they may dislike their gender or want to be the opposite gender. There have been few reports on whether these negative gender attitudes are related to eating behaviors.
Adolescence is a window of opportunity to develop healthy dietary patterns and nutritional status, which may have lasting effects on future health (13). The unhealthy dietary characteristics of adolescents include a low intake of fruits and vegetables and a high intake of energy-intensive and nutrient-poor foods, such as carbonated drinks and western fast food (14). Micronutrient deficiencies are prevalent among adolescents, with profound effects on their quality of life, risk of premature death, and the health of their offspring (15). Dietary quality plays a key role in preventing these forms of adolescent malnutrition. High intake of fruits and vegetables has been associated with increased blood vitamin concentrations in European adolescents (16), while low intake is a major contributor to the global burden of disease, particularly non-communicable diseases (17). Carbonated drinks usually contain a small amount of nutrients and sugar. Drinking sugary drinks is closely related to obesity and type 2 diabetes in adolescents (18). Adolescents’ fast food consumption is associated with metabolic markers of obesity, diabetes and cardiovascular disease (19).
Healthy eating behaviors are important to develop health among children, and negative gender attitudes may play an important role in eating behaviors. The purpose of this study was to analyze the associations between negative gender attitudes and eating behaviors, which is a new perspective to promote healthy eating behaviors among children and adolescents.
Materials and methods
Participants
A total of 692 students (369 boys and 318 girls) aged 8–15 years were selected from two 9-year compulsory education schools using the stratified cluster sampling method. There were 657 effective samples (347 boys, 310 girls), and the effective rate was 99.0%. The project was approved by the Medical Research Ethics Committee of Bengbu Medical College [(2015) No. 003], and participants’ guardians signed informed consent forms. This study was conducted in accordance with the Declaration of Helsinki.
Measurement
Medical staff who receive standardized training were recruited as surveyors. The participants were asked to have an empty stomach, wear light clothes, and be barefoot. Height was measured using a mechanical height meter to the nearest 0.1 cm. Weight was measured using an electronic body weight meter to the nearest 0.1 kg. Waist circumference (WC) was measured to the nearest 0.1 cm using a nylon tape scale. WC is the circumference of the waist along a horizontal line at 1 cm above the navel. BMI = Weight (kg)/Height (m)2; Waist-to-height ratio (WHtR) = WC (cm)/Height (cm). The students were divided into overall overweight/obese and non-overweight/obese groups according to the sex-age BMI standard (20). According to the standard of WHtR ≥ 0.46, children and adolescents were divided into abdominal obesity and non-abdominal obesity groups (21). Under the leading reading of standardized training investigators, the questionnaires of eating behaviors and negative gender attitude for children aged 8–15 years were completed by themselves in the form of centralized filling.
Eating behaviors survey
An eating frequency questionnaire was used to investigate the frequencies of dining out, midnight snacks, fried food, high-calorie snacks, preserved vegetables, western fast food, carbonated drink, fish meat, shrimps, eggs, milk, fresh vegetables, fruits, and breakfast. The frequency of each eating behavior was assigned as 1 time/day = 7, 4–6 times/week = 5, 1–3 times/week = 2, 1 time/2 weeks = 0.5, 1 time/month = 0.25, and never = 0 (22). The higher the score, the higher the frequency of eating behaviors. The Cronbach coefficient of the questionnaire was 0.630. Exploratory factor analysis (EFA) was used to extract 3 common factors from 14 eating behaviors by orthogonal rotation with maximum variance, including unhealthy eating behavior, healthy eating behavior and protein eating behavior. The unhealthy eating behavior factor included dining out and consuming midnight snacks, fried food, high-calorie snacks, preserved vegetables, western fast food, and carbonated drink; the healthy eating behavior factor included eggs, milk, fresh vegetables, fruits and breakfast; and the protein eating behavior factor included fish, meat and shrimp. The KMO test value of factor analysis was 0.770, and Bartlett’s sphericity test showed a statistically significant difference (χ2 = 1465.198, P < 0.001) (see Table 1 for details).
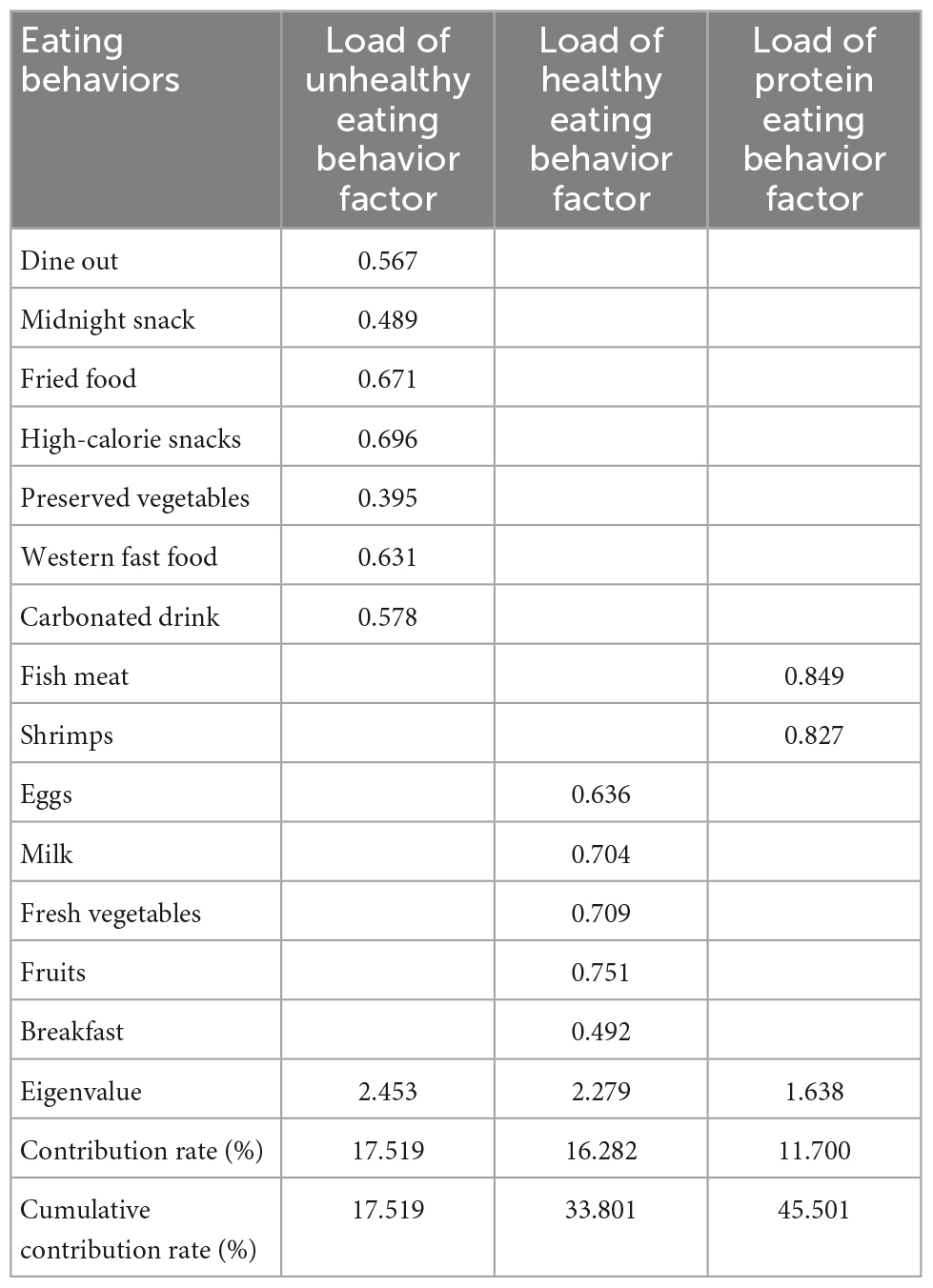
Table 1. Exploratory factor analysis of eating behavior frequency.
Negative gender attitude survey
The self-designed questionnaire was developed to investigate children and adolescents’ negative gender attitudes. Question 1 (Disliking your own gender): Do you like your own gender? Answer: Like, Not completely like, Dislike. Disliking your own gender was divided into two ranks: “Yes” (“Not completely like” or “dislike”) and “No” (“Like”). Question 2 (Wanting to be the opposite gender): Do you want to be a member of the opposite gender? Answer: Not wanting, Not completely wanting, Wanting (23). Wanting to be the opposite gender was divided into two ranks: “Yes” (“Wanting” or “Not completely wanting”) and “No” (“Not wanting”). The Cronbach’s coefficient of the questionnaire was 0.728.
Statistical analyses
All analyses were conducted using IBM SPSS 23.0 software. The quantitative data are described as the mean ± SD, and count data are described as the rate or proportion (%). Two independent sample t-tests were used to compare the differences in quantitative variables between the two groups. The chi-square test was used to compare the differences in qualitative variables between the two groups. After adjusting for age and body type, multiple linear regression was used to analyze the relationships between negative gender attitudes and eating behaviors. P < 0.05 was considered statistically significant.
Results
Differences in age, eating behaviors, gender attitudes, and body shape between boys and girls
A total of 657 adolescents aged 8–15 years were included in this study, including 347 boys and 310 girls. The proportion of children disliking their own gender was 6.5% [43/657, boys: 6.1% (21/347), girls: 7.1% (22/310)], and the proportion of children who wanted to be of the opposite gender was 8.8% [58/657, boys: 5.5% (19/347), girls: 12.6% (39/310)] (see Figure 1 for details). The proportion of girls with the above negative gender attitudes was significantly higher than those of boys (P < 0.05). The proportion of children with abdominal obesity and overall overweight or obesity was 29.8% [196/657, boys: 33.1% (115/347), girls: 26.1% (81/310)] and 31.5% [207/657, boys: 34.3% (119/347), girls: 28.4% (88/310)], respectively, and was higher in boys than in girls (P < 0.05). There was no significant difference in age between boys and girls (P > 0.05). The frequencies of consuming breakfast, midnight snacks, preserved vegetables, western fast food, carbonated drinks, fish, meat, and shrimp were higher in boys than in girls, as well as unhealthy eating behaviors and high protein eating behaviors (P < 0.05). There were no significant differences between boys and girls in the frequencies of dining out, eating fried food, high-calorie snacks, fresh vegetables and fruits (P > 0.05) (see Table 2 for details).
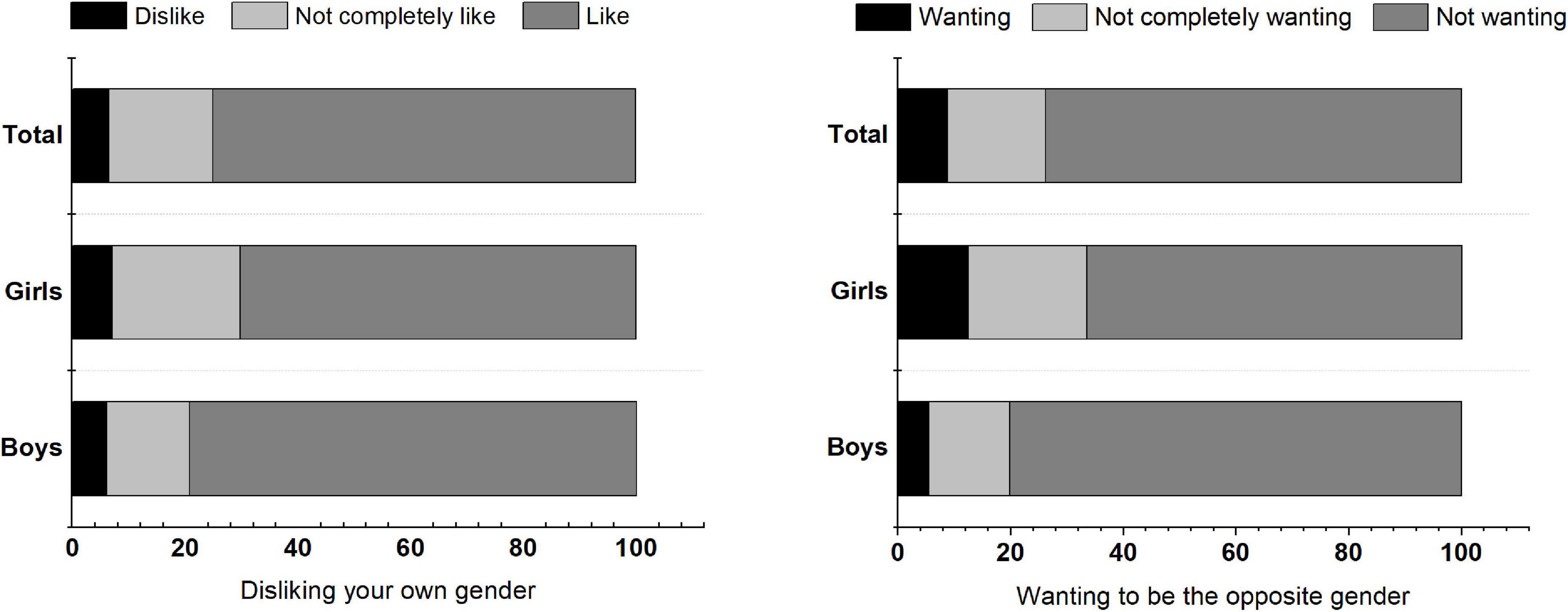
Figure 1. Proportion of disliking your own gender and wanting to be the opposite gender among children and adolescents.
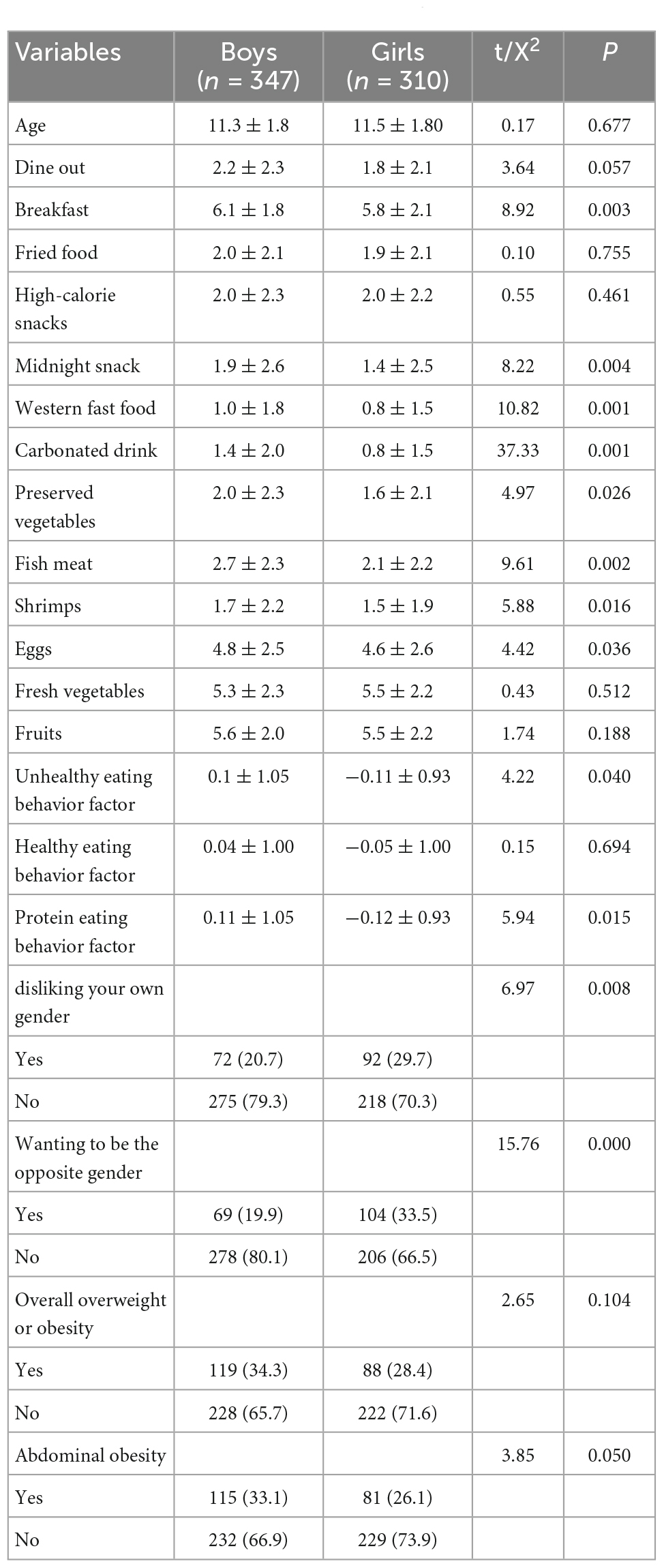
Table 2. Comparisons of differences in age, eating behaviors, gender attitude, and body shape between boys and girls.
Comparisons of eating behaviors and negative gender attitudes between children and adolescents with different body shapes
The frequency of drinking carbonated drinks among girls with overall overweight or obesity was higher than that of girls with non-overall overweight or obesity, but the frequencies of eating midnight snacks and eggs among girls with non-overall overweight or obesity were higher than those of girls with overall overweight or obesity. The frequencies of dining out, eating western fast food and high protein eating behaviors among abdominally obese boys were higher than those in non-abdominally obese boys (P < 0.05). The frequency of drinking carbonated drinks among girls with abdominal obesity was higher than that in girls with non-abdominal obesity (P < 0.05), but the frequencies of eating fish, meat and eggs among girls with non-abdominal obesity were higher than those in girls with abdominal obesity (P < 0.05) (see Table 3 for details).
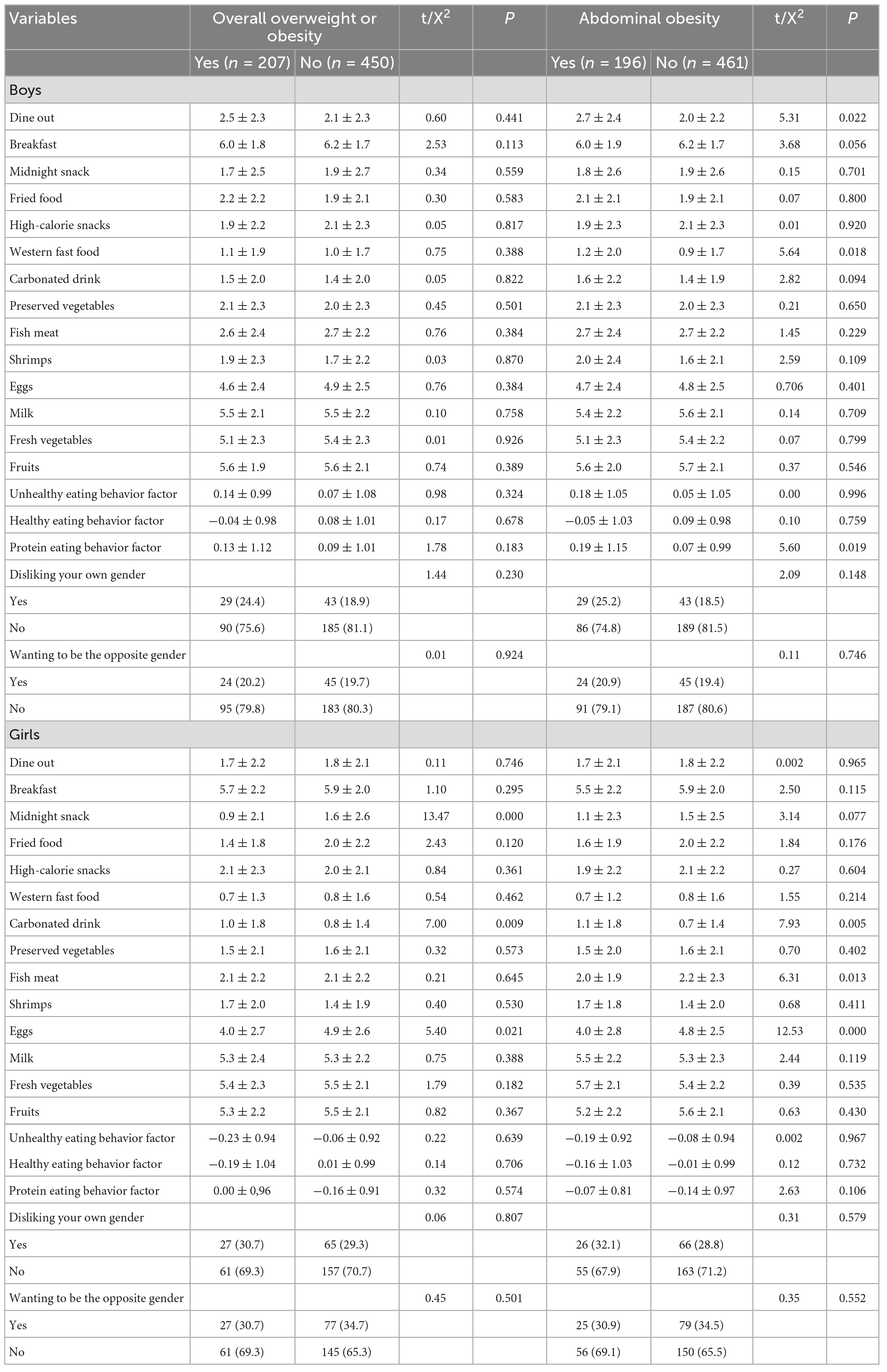
Table 3. Comparisons of differences in eating behaviors, negative gender attitude between children and adolescents with different body shapes.
Comparisons of eating behaviors of children and adolescents who dislike their own gender and who like their own gender
The results showed that boys who disliked their own gender had higher frequencies of dining out and eating midnight snacks, high-calorie snacks, western fast food, preserved vegetables, unhealthy eating behaviors and protein eating behaviors than boys who liked their own gender. Girls who liked their own gender (P < 0.05) consumed fruits and fresh vegetables less frequently and expressed fewer healthy eating behaviors than both boys who liked their own gender and girls who liked their own gender (except for fruits) (P < 0.05). Girls who disliked their own gender dined out and consumed western fast food, carbonated drinks, fish, meat, and shrimp more frequently and exhibited more protein eating behaviors than girls who liked their own gender (P < 0.05). However, there were no significant differences in dining out or consuming western fast food, carbonated drinks, fish, meat, shrimp and protein eating behaviors between girls who disliked their own gender and boys who liked their own gender (see Table 4 for details).
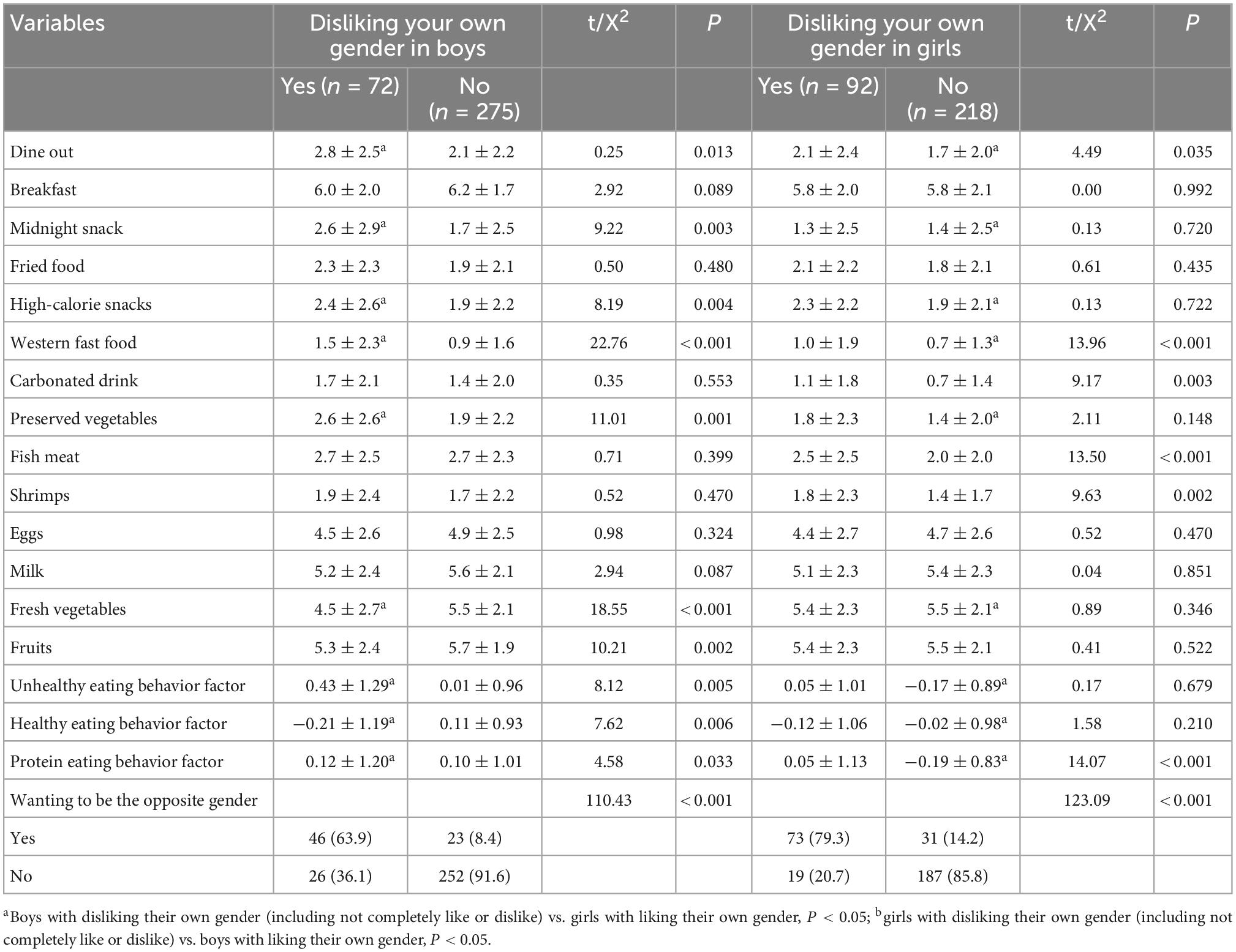
Table 4. Comparisons of differences in eating behaviors between children and adolescents with disliking their own gender and liking their own gender.
Comparisons of eating behaviors of children and adolescents who want to be the opposite gender and those who do not
The results showed that boys who wanted to be the opposite gender ate western fast food, high-calorie snacks, and preserved vegetables more frequently and exhibited more unhealthy eating behaviors than boys who did not want to be the opposite gender. Girls who did not want to be the opposite gender (P < 0.05) ate eggs, fresh vegetables, and fruits less frequently and exhibited fewer healthy eating behaviors than boys who did not want to be the opposite gender (P < 0.05) and ate fresh vegetables and fruits less frequently than girls who did not want to be the opposite gender (P < 0.05). There were no significant differences in the frequencies of eating eggs and healthy eating behaviors between boys who wanted to be of the opposite gender and girls who did not want to be of the opposite gender (P > 0.05). Girls who wanted to be the opposite gender ate shrimp, fish, and meat more frequently and expressed more high protein eating behaviors than girls who did not want to be the opposite gender (P < 0.05) and ate eggs less frequently than girls who did not want to be the opposite gender and boys who did not want to be the opposite gender (P < 0.05). There were no significant differences in the frequencies of shrimp, fish, and meat consumption or high protein eating behaviors between girls who wanted to be of the opposite gender and boys who did not want to be of the opposite gender (P > 0.05) (see Table 5 for details).
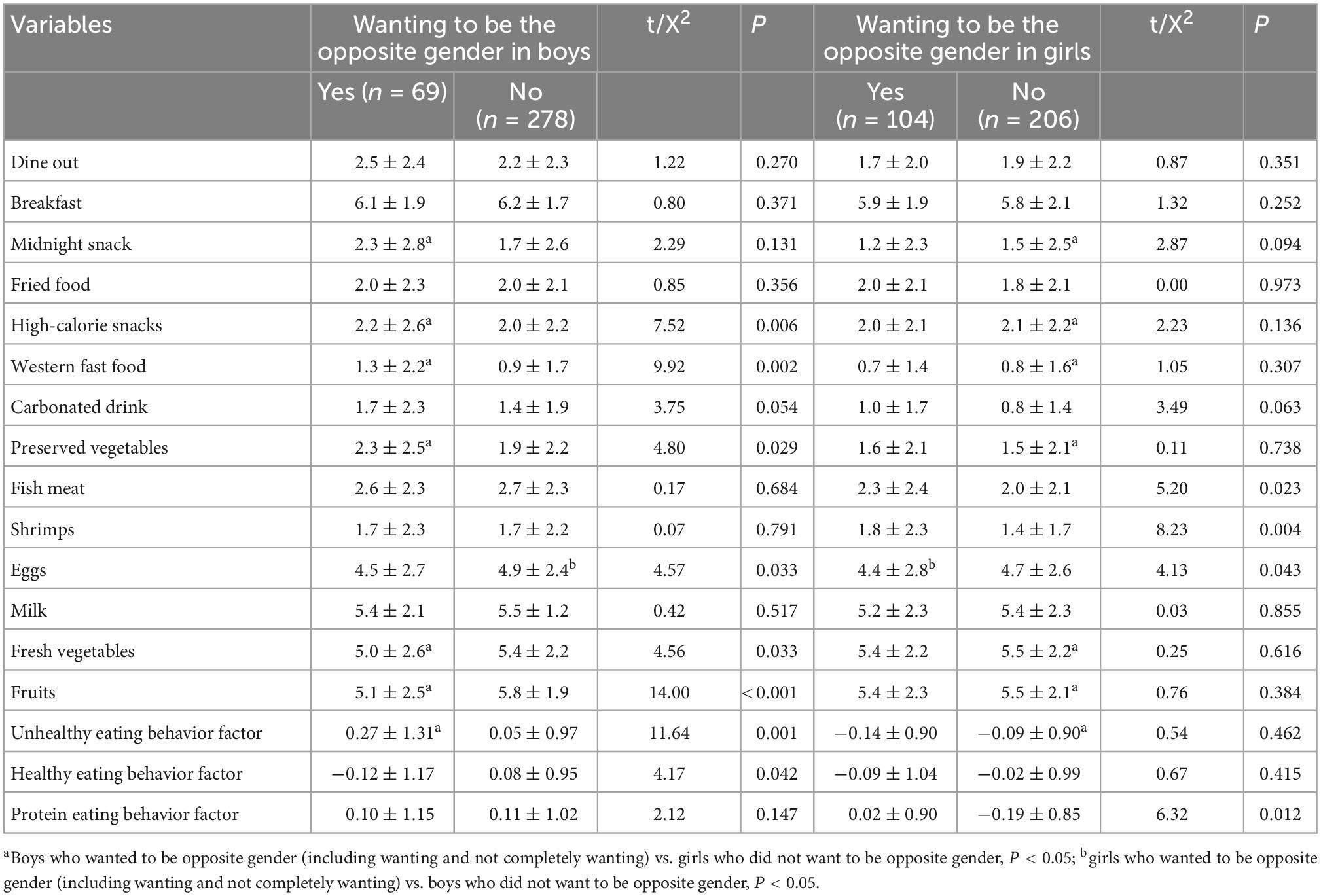
Table 5. Comparisons of differences in eating behaviors between children and adolescents with wanting to be opposite gender and no wanting to be opposite gender.
Interactions between disliking your own gender and wanting to be the opposite gender in eating behaviors
After adjusting for age, overall obesity and abdominal obesity, each eating behavior was treated as a dependent variable. Disliking one’s own gender (yes = 1, no = 0), wanting to be the opposite gender (yes = 1, no = 0), and the interaction item between disliking one’s own gender and wanting to be the opposite gender were used as independent variables. Multiple linear regressions were performed using a stepwise method. The results showed that disliking one’s own gender positively correlated with unhealthy eating behavior and negatively correlated with eating fresh vegetables in boys (P < 0.05). There was a significant interaction between disliking one’s own gender and wanting to be of the opposite gender predicting midnight snack consumption (P < 0.05). Disliking one’s own gender positively correlated with eating western fast food and unhealthy eating behavior in girls (P < 0.05). Wanting to be the opposite gender negatively correlated with eating western fast food and unhealthy eating behavior in girls (P < 0.05). There were positive interactions between disliking one’s own gender and wanting to be the opposite gender that predicted consumption of carbonated drinks, fish, meat, and shrimp and high protein eating among girls (P < 0.05) (see Table 6 and Figure 2 for details).
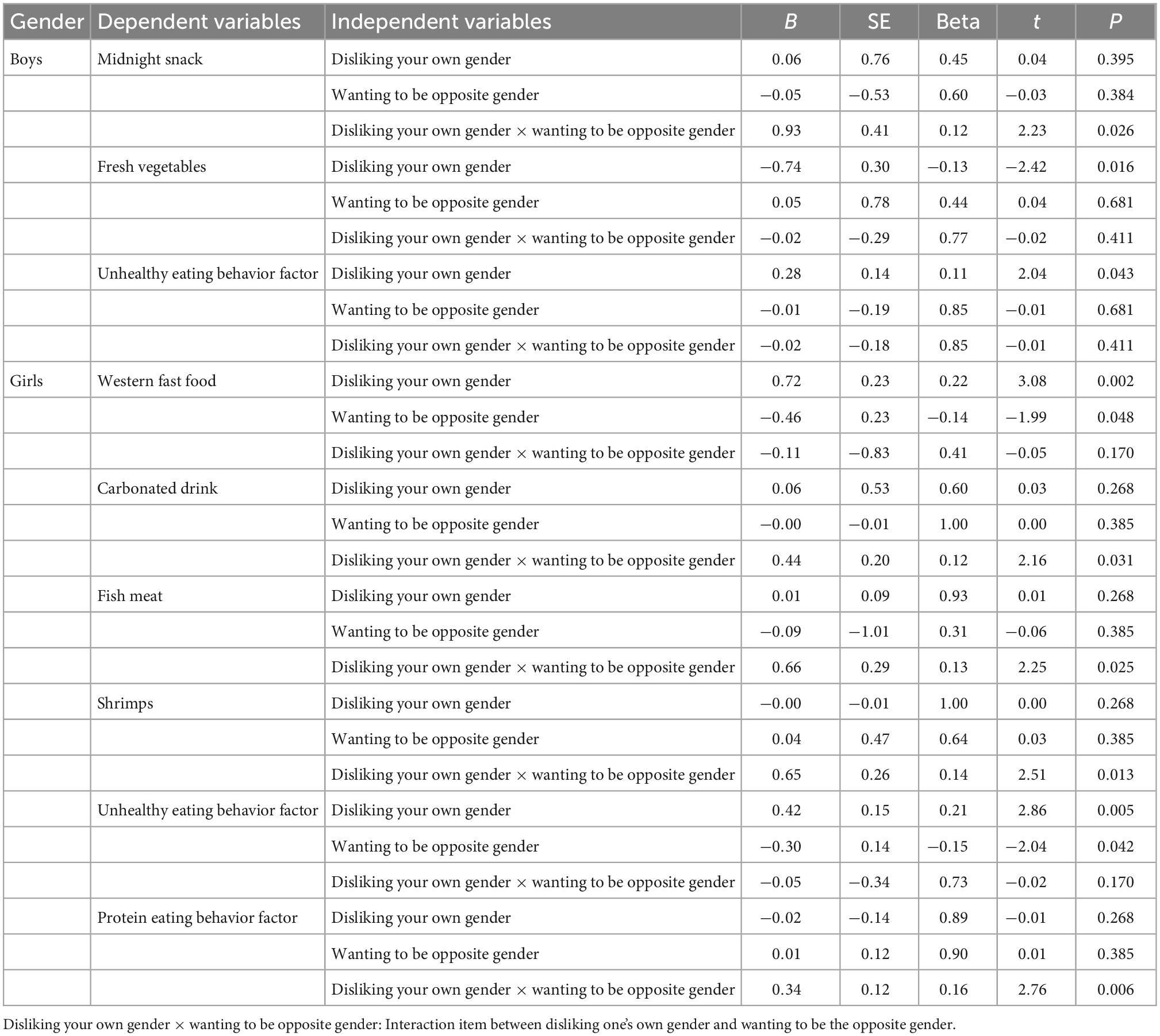
Table 6. The results of multiple linear regression on associations between eating behaviors and negative gender attitude after adjusting for age, overall obesity and abdominal obesity.
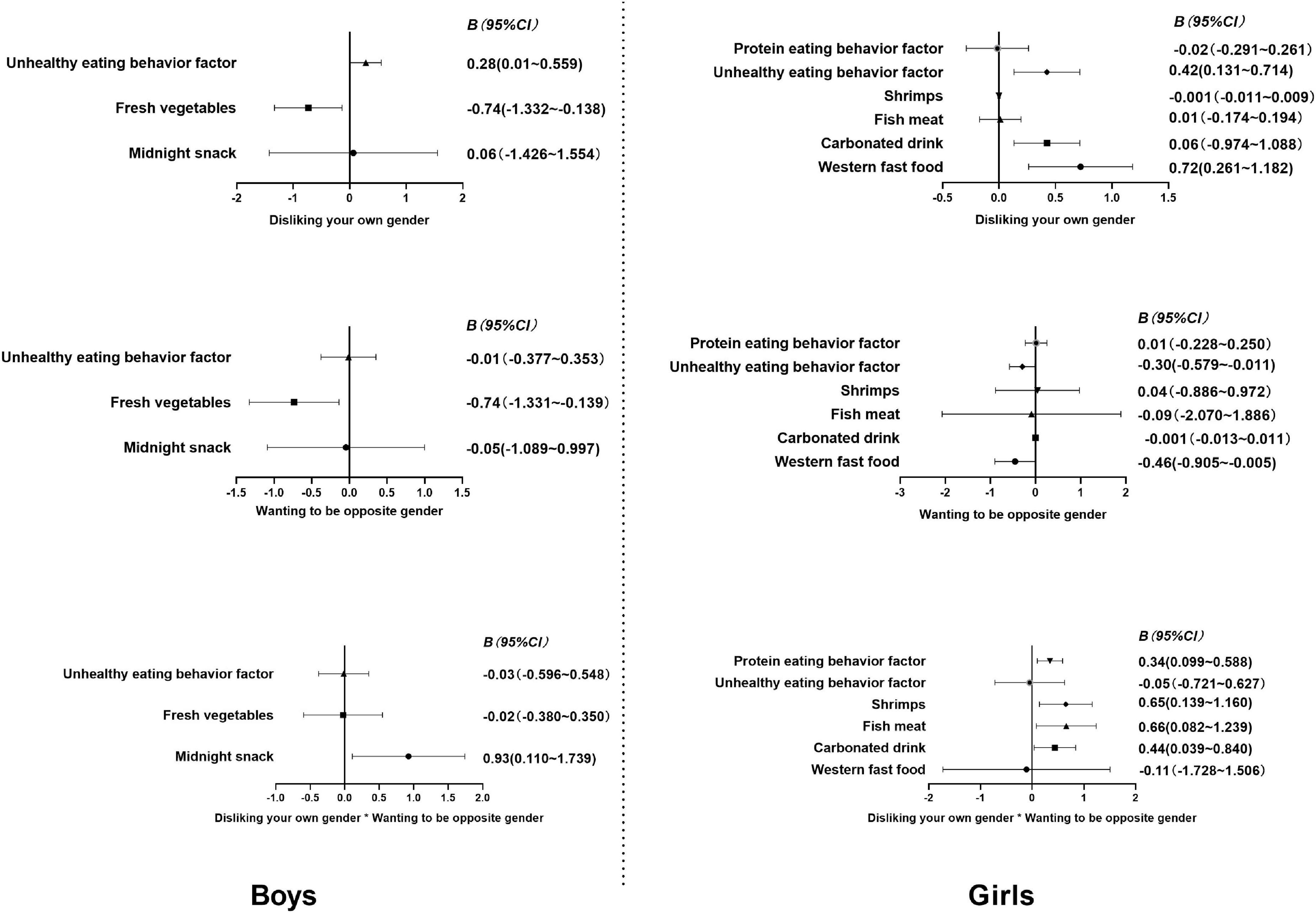
Figure 2. 95% CI of association coefficients between eating behaviors and negative gender attitude.
Discussion
It is common for children and adolescents to have negative gender attitudes (disliking their own gender or wanting to be the opposite gender) and unhealthy eating behaviors, and adolescence is an important stage in the formation of gender role orientation and healthy eating behaviors. This study reported the characteristics of negative gender attitudes and eating behavior among Chinese children and adolescents and revealed the relationships between negative gender attitudes and eating behaviors for the first time, to our knowledge. The study found that boys who did not like their gender or wanted to be the opposite gender had more unhealthy eating behaviors, while they had fewer healthy eating behaviors; Girls who did not like their gender or wanted to be the opposite gender had more protein eating behaviors.
The results of this study showed that 6.5% of children disliked their own gender, 8.8% of children wanted to be of the opposite gender, and the proportion of girls with negative gender attitudes was higher than that of boys. Steensma et al. (24) estimated that the incidence of persistent gender dysphoria from childhood to adolescence ranges from 2 to 27%. Cohen-Kettenis et al. (25) confirmed that girls had a higher tolerance for transgender behaviors. Zhang et al. (26) reported that girls were more dissatisfied with their gender than boys. Social culture may play an important role in negative gender attitudes. Zucker et al. (27) found that boys’ feminine behaviors were less accepted than girls’ masculine behaviors. This study showed that the proportion of children with abdominal obesity and overall obesity was 29.8 and 31.5%, respectively, and was higher in boys than in girls, which may be related to the fact that boys ate breakfast, midnight snacks, preserved vegetables, western fast food, carbonated drinks, fish, meat, and shrimp more frequently and expressed more unhealthy dietary behaviors and more protein dietary behaviors than girls. A study found that boys were twice as likely to be overweight as girls, and that boys’ less healthy eating habits were associated with higher daily intake of protein-rich foods (28). Previous studies have proven that girls are more likely than boys to skip midnight snacks, eat more fruits and drink fewer carbonated drinks (29).
We found that boys who disliked their own gender or who wanted to be the opposite gender expressed more unhealthy eating behaviors and fewer healthy eating behaviors; girls who disliked their own gender had more frequent unhealthy eating behaviors. Becker et al. (30) reported that people with gender dysphoria suffered from eating disorders due to dissatisfaction with their gender-related body parts, inner distress and inability to accept them. Studies have shown that male sexual minorities may have lower diet quality and worse eating habits than non-minorities (31). Transgender individuals conceal or demonstrate their specific gender characteristics by unhealthy eating behaviors (32). Ålgars et al. (33) found that transgender persons try to conceal the characteristics of their assigned sex or demonstrate the characteristics of their required gender identity through changes in dietary behavior. The common gender stereotypes of parents often teach boys to change their feminine characteristics or behaviors, and poor teaching may increase boys’ psychological burden and unhealthy eating behaviors (34). Sociocultural pressure may increase the risk of disordered weight control behaviors (such as unhealthy eating behaviors) for gender-non-conforming girls (35). Adolescents with non-conforming gender expression in school and online environments are more likely to experience peer bullying and peer violence (36, 37) and may have an increased risk for disordered weight control behaviors (38). The greater the social pressure of children who want to be of the opposite gender, the more serious unhealthy eating behaviors may be (11).
In addition, we found that boys who disliked their own gender had more protein eating behaviors. Studies have shown that boys are more likely to have strong muscles, while girls are more likely to have slim bodies (39). Muscle strength is an important determinant of physical performance in children and adolescents (40). Boys who do not like their gender might feel that way because they are not strong enough and thus hope to become strong through higher protein eating behavior (41). Men’s pursuit of muscle is also an internal social and cultural pressure, which suggests that men should have a muscular body (42). However, we found that there were not more protein eating behaviors among boys who wanted to be the opposite gender, and there were no differences in healthy eating behaviors between boys who wanted to be the opposite gender and girls who did not, which shows that boys who want to be the opposite gender may not make themselves stronger, but their goal may be to make themselves more like girls through healthy eating behaviors. Studies have shown that boys who want to be the opposite gender still want to have large hips and breasts despite their healthy weight (43). Homosexual men pay more attention to thin bodies (11). We found that girls who disliked their own gender or who wanted to be the opposite gender had higher protein eating behavior, and there was no difference from boys who liked their gender or did not want to be the opposite gender. Girls who did not like their gender might not be slim enough, but they wanted to make themselves into boys through higher protein eating behaviors, which is in line with the femininity hypothesis (44). In addition, the results of multiple linear regression showed that girls who wanted to be of the opposite gender had fewer unhealthy eating behaviors than girls who did not want to be of the opposite gender, which shows that girls with this desire are more motivated to develop toward the opposite sex through eating behaviors. We found that there was a positive interaction between disliking one’s own gender and wanting to be the opposite gender in boys’ midnight snack eating and in girls’ consumption of carbonated drinks, fish, meat, and shrimp and their protein dietary factors, which indicates that if a child does not like their own gender and has the desire to become the opposite gender at the same time, the above eating behaviors will be more frequent.
This study has several limitations. First, based on a cross-sectional study, we found relationships between negative gender attitudes and eating behaviors; however, whether the correlations are causal remains to be verified by cohort studies. Second, the children and adolescents surveyed were from two primary and secondary schools in China, which has limitations in extending other adolescents. Finally, all the collected data were the participants’ self-reports, and their responses may be affected by factors such as denial, idealization and social expectations.
Conclusion
The proportion of girls with a negative gender attitude (disliking their own gender or wanting to be the opposite gender) was higher than that of boys. Boys who disliked their own gender or wanted to be the opposite gender may have higher frequencies of unhealthy eating behaviors and lower frequencies of healthy eating behaviors. Girls who disliked their own gender or wanted to be the opposite gender may have higher frequencies of protein eating behaviors. While encouraging children to develop healthy eating behaviors, we should pay attention to children’s positive attitudes toward their own gender cognition.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by the Medical Research Ethics Committee of Bengbu medical college [(2015) No. 003]. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
Author contributions
RC and JC: conceptualization. KL, YW, XP, and JZ: methodology. RC: formal analysis and data curation. LF, RY, and HH: investigation. RC and LF: writing — original draft preparation and writing — review and editing. MH, RY, and HH: visualization. LF: project administration. All authors contributed to the article and approved the submitted version.
Funding
This project was supported by the National Natural Science Foundation of China (Grant No. 81502823) and the 512 Talent Cultivation Plan of Bengbu Medical College (Grant No. by51201204).
Acknowledgments
We thank the participants who participated in the survey and the teachers who assisted in the survey.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Lampis J, Cataudella S, Busonera A, De Simone S, Tommasi M. The moderating effect of gender role on the relationships between gender and attitudes about body and eating in a sample of Italian adolescents. Eat Weight Disord. (2019) 24:3–11. doi: 10.1007/s40519-017-0372-2
5. Verhulst F, Tiemeier H. Epidemiology of child psychopathology: major milestones. Eur Child Adolesc Psychiatry. (2015) 24:607–17. doi: 10.1007/s00787-015-0681-9
6. Zucker K. Epidemiology of gender dysphoria and transgender identity. Sex Health. (2017) 14:404–11. doi: 10.1071/SH17067
7. Lowry R, Johns M, Gordon A, Austin S, Robin L, Kann L. Nonconforming gender expression and associated mental distress and substance use among high school students. JAMA Pediatr. (2018) 172:1020–8. doi: 10.1001/jamapediatrics.2018.2140
8. Kreukels B, Kohler B, Nordenstrom A, Roehle R, Thyen U, Bouvattier C, et al. Gender dysphoria and gender change in disorders of sex Development/Intersex conditions: results from the dsd-LIFE study. J Sex Med. (2018) 15:777–85. doi: 10.1016/j.jsxm.2018.02.021
9. Khatchadourian K, Amed S, Metzger D. Clinical management of youth with gender dysphoria in Vancouver. J Pediatr. (2014) 164:906–11. doi: 10.1016/j.jpeds.2013.10.068
10. Gordon A, Austin S, Schultz J, Guss C, Calzo J, Wang M. Gender expression, peer victimization, and disordered weight-control behaviors among U.S. High school students. J Adolesc Health. (2021) 68:1148–54. doi: 10.1016/j.jadohealth.2020.08.032
11. Blashill A. Gender roles, eating pathology, and body dissatisfaction in men: a meta-analysis. Body Image. (2011) 8:1–11. doi: 10.1016/j.bodyim.2010.09.002
12. Milano W, Ambrosio P, Carizzone F, De Biasio V, Foggia G, Capasso A. Gender dysphoria, eating disorders and body image: an overview. Endocr Metab Immune Disord Drug Targets. (2020) 20:518–24. doi: 10.2174/1871530319666191015193120
13. Georgiadis A, Penny M. Child undernutrition: opportunities beyond the first 1000 days. Lancet Public Health. (2017) 2:e399. doi: 10.1016/S2468-2667(17)30154-8
14. Keats E, Rappaport A, Shah S, Oh C, Jain R, Bhutta Z. The dietary intake and practices of adolescent girls in low- and Middle-Income countries: a systematic review. Nutrients. (2018) 10:1978. doi: 10.3390/nu10121978
15. Bundy D, de Silva N, Horton S, Patton G, Schultz L, Jamison D. Investment in child and adolescent health and development: key messages from disease control priorities, 3rd edition. Lancet. (2018) 391:687–99. doi: 10.1016/S0140-6736(17)32417-0
16. Mielgo-Ayuso J, Valtuena J, Cuenca-Garcia M, Gottrand F, Breidenassel C, Ferrari M, et al. Regular breakfast consumption is associated with higher blood vitamin status in adolescents: the HELENA (healthy lifestyle in Europe by nutrition in adolescence) study. Public Health Nutr. (2017) 20:1393–404. doi: 10.1017/S1368980016003645
17. Lim S, Vos T, Flaxman A, Danaei G, Shibuya K, Adair-Rohani H, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010: a systematic analysis for the global burden of disease study 2010. Lancet. (2012) 380:2224–60. doi: 10.1016/S0140-6736(12)61766-8
18. Hu F. Resolved: there is sufficient scientific evidence that decreasing sugar-sweetened beverage consumption will reduce the prevalence of obesity and obesity-related diseases. Obes Rev. (2013) 14:606–19. doi: 10.1111/obr.12040
19. Sahoo K, Sahoo B, Choudhury A, Sofi N, Kumar R, Bhadoria A. Childhood obesity: causes and consequences. J Fam Med Prim Care. (2015) 4:187–92. doi: 10.4103/2249-4863.154628
20. Kromeyer-Hauschild K, Zellner K. Trends in overweight and obesity and changes in the distribution of body mass index in schoolchildren of Jena, East Germany. Eur J Clin Nutr. (2007) 61:404–11. doi: 10.1038/sj.ejcn.1602533
21. Oliveira R, Guedes D. Performance of anthropometric indicators as predictors of metabolic syndrome in Brazilian adolescents. BMC Pediatr. (2018) 18:33. doi: 10.1186/s12887-018-1030-1
22. Northstone K, Smith A, Cribb V, Emmett P. Dietary patterns in UK adolescents obtained from a dual-source FFQ and their associations with socio-economic position, nutrient intake and modes of eating. Public Health Nutr. (2014) 17:1476–85. doi: 10.1017/S1368980013001547
23. Galambos N, Almeida D, Petersen A. Masculinity, femininity, and sex role attitudes in early adolescence: exploring gender intensification. Child Dev. (1990) 61:1905–14.
24. Steensma T, McGuire J, Kreukels B, Beekman A, Cohen-Kettenis P. Factors associated with desistence and persistence of childhood gender dysphoria: a quantitative follow-up study. J Am Acad Child Adolesc Psychiatry. (2013) 52:582–90. doi: 10.1016/j.jaac.2013.03.016
25. Cohen-Kettenis P, Owen A, Kaijser V, Bradley S, Zucker K. Demographic characteristics, social competence, and behavior problems in children with gender identity disorder: a cross-national, cross-clinic comparative analysis. J Abnorm Child Psychol. (2003) 31:41–53. doi: 10.1023/a:1021769215342
26. Zhang Y, Li T, Yao R, Han H, Wu L, Wu X, et al. Comparison of Body-Image dissatisfaction among chinese children and adolescents at different pubertal development stages. Psychol Res Behav Manag. (2020) 13:555–62. doi: 10.2147/PRBM.S242645
27. Zucker K. Sex/gender research and meta-analysis. Arch Sex Behav. (2020) 49:365–6. doi: 10.1007/s10508-020-01651-9
28. Djordjevic-Nikic M, Dopsaj M. Characteristics of eating habits and physical activity in relation to body mass index among adolescents. J Am Coll Nutr. (2013) 32:224–33. doi: 10.1080/07315724.2013.791149
29. Morgan A, Svedberg P, Nyholm M, Nygren J. Advancing knowledge on social capital for young people’s mental health. Health Promot Int. (2021) 36:535–47. doi: 10.1093/heapro/daaa055
30. Becker I, Nieder T, Cerwenka S, Briken P, Kreukels B, Cohen-Kettenis P, et al. Body image in young gender dysphoric adults: a European multi-center study. Arch Sex Behav. (2016) 45:559–74. doi: 10.1007/s10508-015-0527-z
31. VanKim N, Corliss H, Jun H, Calzo J, AlAwadhi M, Austin S. Gender expression and sexual orientation differences in diet quality and eating habits from adolescence to young adulthood. J Acad Nutr Diet. (2019) 119:2028–40. doi: 10.1016/j.jand.2019.05.014
32. Vocks S, Stahn C, Loenser K, Legenbauer T. Eating and body image disturbances in male-to-female and female-to-male transsexuals. Arch Sex Behav. (2009) 38:364–77. doi: 10.1007/s10508-008-9424-z
33. Algars M, Alanko K, Santtila P, Sandnabba N. Disordered eating and gender identity disorder: a qualitative study. Eat Disord. (2012) 20:300–11. doi: 10.1080/10640266.2012.668482
34. Hania M, Roberts A, Sharif M. Gender incongruence/dysphoria in children and adolescents: overview and implications for dentistry. Br Dent J. (2021) 230:369–73. doi: 10.1038/s41415-021-2734-4
35. Copeland W, Bulik C, Zucker N, Wolke D, Lereya S, Costello E. Does childhood bullying predict eating disorder symptoms? a prospective, longitudinal analysis. Int J Eat Disord. (2015) 48:1141–9. doi: 10.1002/eat.22459
36. Gordon A, Conron K, Calzo J, White M, Reisner S, Austin S. Gender expression, violence, and bullying victimization: findings from probability samples of high school students in 4 US school districts. J Sch Health. (2018) 88:306–14. doi: 10.1111/josh.12606
37. Roberts A, Rosario M, Slopen N, Calzo J, Austin S. Childhood gender nonconformity, bullying victimization, and depressive symptoms across adolescence and early adulthood: an 11-year longitudinal study. J Am Acad Child Adolesc Psychiatry. (2013) 52:143–52. doi: 10.1016/j.jaac.2012.11.006
38. Meyer I. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: conceptual issues and research evidence. Psychol Bull. (2003) 129:674–97. doi: 10.1037/0033-2909.129.5.674
39. Nagata J, Domingue B, Darmstadt G, Weber A, Meausoone V, Cislaghi B, et al. Gender norms and weight control behaviors in U.S. Adolescents: a prospective cohort study (1994-2002). J Adolesc Health. (2020) 66:S34–41. doi: 10.1016/j.jadohealth.2019.08.020
40. Grosset J, Mora I, Lambertz D, Perot C. Voluntary activation of the triceps surae in prepubertal children. J Electromyogr Kinesiol. (2008) 18:455–65. doi: 10.1016/j.jelekin.2006.11.002
41. McCreary D, Sasse D. An exploration of the drive for muscularity in adolescent boys and girls. J Am Coll Health. (2000) 48:297–304. doi: 10.1080/07448480009596271
42. Tiggemann M, Martins Y, Churchett L. Beyond muscles: unexplored parts of men’s body image. J Health Psychol. (2008) 13:1163–72. doi: 10.1177/1359105308095971
43. McGuire J, Doty J, Catalpa J, Ola C. Body image in transgender young people: findings from a qualitative, community based study. Body Image. (2016) 18:96–107. doi: 10.1016/j.bodyim.2016.06.004
Keywords: disliking your own gender, wanting to be opposite gender, eating behaviors, children and adolescents, negative gender attitudes
Citation: Cao R, Chen J, Wang Y, Peng X, Han M, Liu K, Zhang J, Yao R, Han H and Fu L (2023) Associations between negative gender attitudes and eating behaviors in Chinese children and adolescents. Front. Nutr. 9:1053055. doi: 10.3389/fnut.2022.1053055
Received: 25 September 2022; Accepted: 06 December 2022;
Published: 04 January 2023.
Edited by:
Reema Fayez Tayyem, Qatar University, QatarReviewed by:
Sabika Allehdan, The University of Jordan, JordanHaleama Al Sabbah, Zayed University, United Arab Emirates
Copyright © 2023 Cao, Chen, Wang, Peng, Han, Liu, Zhang, Yao, Han and Fu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lianguo Fu, ✉ bGlhbmd1b2Z1QDE2My5jb20=