
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Nutr. , 20 October 2022
Sec. Clinical Nutrition
Volume 9 - 2022 | https://doi.org/10.3389/fnut.2022.1040089
This article is part of the Research Topic Environmental Factors Implicated in Obesity View all 11 articles
 Diana Fonseca-Pérez1
Diana Fonseca-Pérez1 Cecilia Arteaga-Pazmiño2Claudia P. Maza-Moscoso3Sara Flores-Madrid4
Cecilia Arteaga-Pazmiño2Claudia P. Maza-Moscoso3Sara Flores-Madrid4 Ludwig Álvarez-Córdova1,4*
Ludwig Álvarez-Córdova1,4*Sarcopenic obesity is characterized by the loss of muscle strength, mass and muscle functionality and increased adipose tissue (obesity) according to different criteria and cut-off points. The prevalence of sarcopenic obesity among older adults is growing worldwide, and many factors are involved in its development. Diet and food security have been described as the main contributors to the development of obesity and sarcopenia. Food insecurity consists of limited or uncertain access to adequate and nutritious foods. This narrative review aims to summarize the existing data on food insecurity as a risk factor for sarcopenic obesity in the elderly.
It is widely recognized that aging and obesity are common public health issues worldwide. According to the World Population Prospect of the United Nations, in 2017, adults older than 65 involved almost 13% of the global population. This percentage is increasing at a more rapid rate compared to the portion of any other age group, and it is due to recent changes in the increase in life expectancy (1). Along with aging comes a loss of skeletal muscle mass and function, commonly accompanied by body fat (BF) gain.
Obesity is considered a worldwide pandemic (2), and is usually diagnosed by body mass index (BMI) above 30 kg/m2. Currently, some factors have been identified as contributors to obesity, such as genetic predisposition and unhealthy lifestyle, especially sedentary habits and excess of caloric intake (3).
Not only obesity is linked to metabolic syndrome, type 2 diabetes (T2D), and some cardiovascular events, as well as the development of drastic personal, social, economic, and healthcare tasks. Obese individuals are at higher risk of chronic and acute diseases, including end-stage organ failures, cancer, and infections, which can lead to complications and hospitalizations. Indeed, the rising rates of obesity have contributed to the coexistence of this disease with other comorbidities like sarcopenia (4).
The European Working Group on Sarcopenia in Older People (EWGSOP) in 2018 redefined the operational definition of sarcopenia as the presence of low muscle mass and strength, and severe sarcopenia if low physical performance is confirmed (5). Sarcopenia is considered as a syndrome with a multifactorial etiology whose prevalence increases with age (6). Several conditions in older adults have been described that may contribute to the development of sarcopenia, like lack of physical activity and dietary habits, which are similar to obesity-related risk factors (7). The term “sarcopenic obesity” (SO) was introduced to define a clinical and functional condition described by the conjunction of obesity and sarcopenia (6, 7).
Despite well-known risk factors for sarcopenia and obesity, growing evidence has shown that bad eating habits are one of these factors and can cause food insecurity. For example, in the United States, food insecurity increased significantly from 5.5 to 12.4% in the last ten years among older adults, and they have been related to obesity and sarcopenia (8–10). However, there is no scientific evidence exploring food insecurity as a risk factor for SO in aged people. For this reason, it is essential to describe how food insecurity may contribute to SO in older adults.
This narrative review aims to summarize the existing data on food insecurity as a risk factor for SO in the elderly. To accomplish this and contribute to the field, we will describe the presence of obesity and sarcopenia in older adults and the conjunction of both pathologies, food insecurity, and dietary intake as risk factors for SO.
A comprehensive search was carried out through PubMed and Web of Science for papers published until August 2022. We reviewed studies focusing on SO and its determinants, the relationship better obesity and food insecurity, and sarcopenia and food insecurity.
The aging process causes many changes in body composition (BC) of the elderly population, regardless of metabolic and physiological functions, resulting in a decrease in lean mass, also called fat-free mass (FFM) (11). Related to fat mass (FM), there is an increase in adiposity and a redistribution of fat from subcutaneous regions to intra-abdominal, intrahepatic, and intramuscular areas, characteristics associated with diseases such as diabetes and cardiovascular disease (12).
Older adults have more body fat percentages (BFP) than their younger counterparts, and there are gender differences in anthropometric measures and BFP. For example, women showed higher values of BMI, subcutaneous fat, and BFP; older men are prone to show more weight and lean mass (13).
Due to these BC changes, aging is linked with obesity and probably with sarcopenia or both of them. These conditions could aggravate disability and frailty, increasing morbidity and mortality rates (14).
Sarcopenia and Obesity have to be measured by using validated methods for measuring body composition, like whole-body Dual-energy X-ray Absorptiometry (DXA), bioelectrical impedance analysis (BIA), Computed Tomography (CT), and Magnetic Resonance Imaging (MRI) to diagnose obesity, sarcopenia, or both of them (5) DXA evaluates bone mineral density and is considered a method to assess whole-body and regional soft-tissue composition, which provides good data about the total amount of FM and FFM by body segments (13). BIA is an adequate and low cost method to measure total water and FFM. CT has accurate and reproducible data for FM, FFM, and visceral fat. MRI identifies changes in muscle structure (5). Using these methods, measurements of FM and FFM can properly make an accurate diagnosis against traditional anthropometric measurements.
The World Obesity Federation in 2017 stated that obesity is a chronic disease. There is a link between FM and the vulnerability of the host, making it significant as a health problem (15). There has been an increase of obesity at all ages on the past decade. In older adults, the prevalence of obesity on both sexes has been found at 37.5 and 39.4%, respectively (16). The association between excess of body fat in older adults and the whole or specific disease mortality is still under debate (17). Obesity is defined, regardless of age, as a BMI greater than or equal to 30 kg/m2. There is no consensus regarding the best measure of obesity in the older population. BMI is an easy tool that correlates with the percentage of body fat in young and middle-aged adults. However, physiological changes in BC render BMI less accurate with aging.
The changes in age-related BC, specially fat distribution, could assist in perceiving the link between adiposity, morbidity, and mortality in older adults. Recent data suggest that the distribution of FM, visceral fat, and reduction of FFM would be more relevant than BMI seeking health problems associated with obesity in older adults (17).
In 2007, the Spanish Society of Parenteral and Enteral Nutrition published the following BMI cohort points to identify overweight and obesity in older adults: 27.0–29.9 kg/m2 (overweight); 30.0-34.9 kg/m2 (obesity class I); 35.0–39.9 kg/m2 (obesity class II); 40.0–49.9 kg/m2 (obesity class II); and 50 kg/m2 (obesity class IV) (18).
Sarcopenia is a progressive and generalized skeletal muscle disturbance (5). The prevalence range may differ depending on the clinical scenario, and the main difference can be the method proposed for the description. Peterman-Rocha et al. found that the prevalence of sarcopenia varies significantly in the systematic (10–27%) vs. a narrative review (0.2–86.5%), regardless of the differences in the methodology and cut-off points (19). These differences can be due to the scientific criteria of the selection of the studies. The classification systems most usually used are EWGSPOP and the Asian Working Group on Sarcopenia (AWSP) (19). In 2019, Rodriguez-Rejón et al. found that despite the methodology used to diagnose sarcopenia, the results did not change in frequency (20).
Primary sarcopenia occurs with aging, and secondary sarcopenia develops due to physical inactivity, malnutrition, and diseases, such as neurodegenerative disease, endocrine disease, or malignancies (5).
This condition is associated with increased adverse outcomes, including falls, functional decline, frailty, and mortality. At first, sarcopenia was an age-related process in older people (21); nowadays, evidence shows it can be present across the lifespan and is influenced by lifestyle risk factors (22), genetics, and also secondary to disease (23).
In order to assess sarcopenia, revised guidelines suggest measuring muscle functionality and validating strength, which is better at predicting unfavorable outcomes (24). Actually, EWGSOP2 valued low muscle strength as a leading parameter of sarcopenia and an adequate measure of muscle function. However, sarcopenia is probably when low muscle strength is present. The diagnosis is made when the low muscle quantity is registered, and severe sarcopenia when quality is confirmed (5).
Sarcopenic obesity (SO) was first described by Baumgartner in 2000 as a clinical and functional condition characterized by the presence of obesity and the diagnosis of sarcopenia (7, 25, 26). Both conditions, loss of MM and muscle capability and gaining body fat, may increase the risk for non-communicable diseases like diabetes and cardiovascular disease and increase the chances of adverse health outcomes such as disability or impairment, cardiometabolic diseases, other comorbidities, and mortality more than sarcopenia or obesity individually (5, 26).
Sarcopenia and obesity share pathological factors, including aging, changes in BC, inflammation, and hormones (27). The aging process carries a low metabolic rate and metabolic adaptations, including adaptive thermogenesis and changes in oxidative capacity; this process favors the development and onset of SO (28). Changes in BC related to age are the main risk factor for SO. Studies have shown that FM increases with age, especially between 60 and 75 years old (27–29). Muscle mass and strength decline progressively around 30, accelerating after 60 years. In addition, there are changes in fat accumulation with aging; visceral fat and intramuscular fat tend to increase, while subcutaneous fat in other body regions declines. Fat infiltration is associated with lower muscle strength and leg performance capacity (29).
Another associated risk is low physical activity, a well-known risk factor of obesity, low muscle strength, muscle atrophy, and reduced metabolic rate (30).
Inflammation also contributes to SO (31). The adipose tissue produces pro-inflammatory cytokines such as interleukin-6, tumor necrosis factor-alpha, and adipokines such as leptin and adiponectin, which regulate the inflammatory response (32, 33). Obese subjects have a pro-inflammatory state which may be one of the key factors in decreasing muscle strength, creating a vicious cycle (33).
Obese individuals have muscle catabolism because insulin has no anabolic function due to insulin resistance (34). Insulin resistance correlates independently with poor muscle strength, and older patients with diabetes show accelerated loss of leg muscle strength and quality (34). Indeed, low levels of sex-specific hormones are an important factor related to SO (34). After menopause, a decline in estrogen levels can result in increased body weight and FM as well as shifts in the accumulation of fat from subcutaneous to visceral deposits. In older men, total lower levels of testosterone are associated with sarcopenia and may contribute to muscle impairment in obese individuals (35, 36).
On the other hand, obesity can independently lead to loss of muscle mass and function due to the negative impact of adipose tissue, which causes metabolic alterations that include oxidative stress, inflammation, and insulin resistance. All of them negatively affect muscle mass (37).
In addition, diet is a risk factor that affects sarcopenia and obesity by different mechanisms. Generally, sarcopenia is associated with an insufficient nutritional intake, whereas obesity is an outcome of excessive energy intake, leading to an imbalance between energy intake and energy expenditure (38).
Due to the clinical and epidemiologic importance of assessing SO, screening tools and diagnostic criteria for this condition have been published recently (5). However, despite the classification, the method used for screening and diagnosing sarcopenia is critical for appropriate and prompt interventions in older adults.
Screening of SO is based on elevated BMI or waist circumference and indicators of sarcopenia such as clinical symptoms and risk factors or the use of SARC-F. The clinical symptoms and risk factors include age >65 years, chronic diseases, recent acute disease or nutritional alterations, repeated falls, weakness, exhaustion, fatigue, and movement limitations (Table 1) (6).
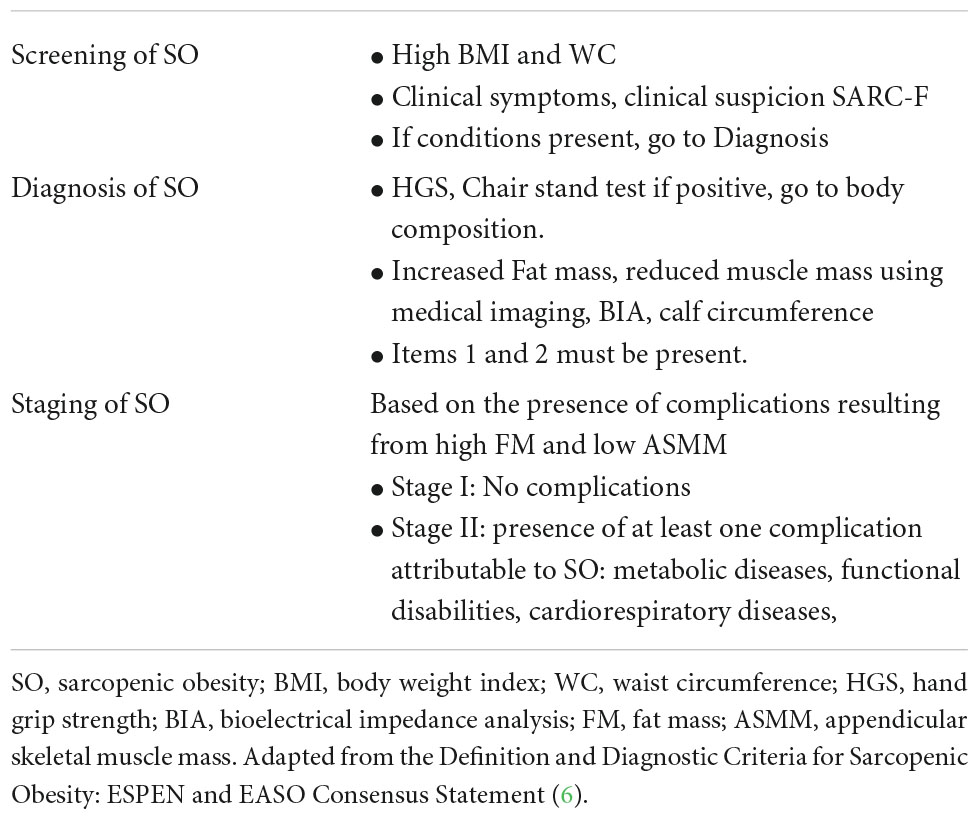
Table 1. Screening, diagnosis, and staging of sarcopenic obesity.
To diagnose sarcopenia and obesity, MM and FM body can be assessed by diverse techniques, such as anthropometry, BIA, and medical imaging. Anthropometry includes BMI diagnosis, skin-fold thickness, and body circumferences. Despite some studies of cut-off points for older adults, the limitation is the lack of precision in evaluating the MM and the high probability of error (39, 40).
BIA measures MM and FM established on electrical conduction through tissues; limitations include hydration levels, exercise, and food or liquid intake. Medical imaging has an advantage for diagnosing and grading sarcopenia and obesity. It is an accurate and reliable method and can be applied for longitudinal changes in clinical trials and as a treatment assessment tool (41).
SO, as other clinical conditions, require standardization and cut-off points for diverse populations or ethnicity, especially due to dissimilarity regardless of body type, adiposity, and lifestyles of the worldwide population, mainly for the Asian and Latin American populations.
Diagnosis of SO should include altered skeletal muscle functional parameters and altered BC (42). For skeletal muscle functional parameters, hand grip strength and knee strength can be used (43). For BC, DEXA or BIA are recommended, and if possible, TC (44).
The staging of SO should be based on the presence or absence of complications. The screening, diagnosis, and staging summary are presented in Table 1, adapted from the Definition and Diagnostic Criteria for Sarcopenic Obesity: ESPEN and EASO Consensus Statement (6).
Food insecurity is a severe global public health concern. Around 2,300 million people worldwide were affected by moderate or severe food insecurity in 2021 due mainly to conflicts, meteorological phenomena, and socio-economic perturbations (45). There should be an update of food and agricultural policies to make healthy diets more affordable. Food insecurity is defined as limited or uncertain access to adequate and nutritious foods due to many factors, especially financial resources (46).
Food insecurity and hunger are concepts that could seem like synonyms. Nevertheless, food insecurity is a household-level economic and social condition limiting access to food, and hunger is an individual-level physiological condition resulting from food insecurity (47). In addition, The United States Department of Agriculture (USDA) classifies food insecurity as reduced quality, variety, or desirability of the diet with little or no indication of reduced food intake and very low food security as multiple indications of disrupted eating patterns and reduced food intake (48).
It has been reported that food insecurity increases have affected people of all ages, particularly those in vulnerable situations (48). Older adults are exposed to many conditions that increase their vulnerability. Food insecurity has been well described as a critical factor that leads to health issues in the aged population, mainly affecting those primarily alone, who have fixed incomes and chronic health concerns (49, 50). Consequently, the prevalence of chronic diseases, poor management of chronic diseases, and decreased health-related quality of life in older adults are associated with food insecurity (49, 51).
One of the main ways that food insecurity can be a determinant of health and diseases is its impact on diet quality.
Diet quality (DQ) can be determined by many indicators such as specific nutrient quantitative and qualitative content or by designed tools that assess an individual’s overall diet quality (52, 53).
Poor DQ is a direct and preventable cause of death globally. Food insecurity has been associated with lower DQ (54), particularly with more than 50 adverse associations with differences according to sex and ethnicity (55, 56).
The decline in diet quality has been observed in cohorts that aged from middle to older adulthood, especially in response to drastic changes derived from social or health issues (57, 58). The proportion of US older adults with poor diet quality significantly increased from 50.9 to 60.9% between 2001 to 2018, with a significant decreasing trend in diet scores among both sexes and all age groups (59).
DQ can also impact nutritional status. Carrier et al. found that diet quality was associated with malnutrition in older adults living in long-term care. In this cohort, several individual nutrients were associated with low calf circumferences (<31 cm). In the same study, older adults with better dietary quality and habits were more likely to have better nutritional status. In addition, a US longitudinal study showed that malnutrition was significantly associated with poorer diet quality and lower energy and protein intake (60).
It is important to mention that sarcopenia could increase the risk of inadequate diets. For example, in long-term care homes in Spain, the risk of a poorer diet was higher in females and residents with sarcopenia (61). In community-dwelling older adults, diet quality has been associated with the number of comorbidities and baseline risk of malnutrition (62). In contrast, prospective associations of poor DQ with long-term incidence of protein-energy malnutrition have not been found (63).
Those differences could result from the method to assess DQ, the definition of malnutrition or risk of malnutrition, and institutional or community-dwelling older adults’ location.
On the contrary, a recent systematic review and meta-analysis describe a significant association between healthy dietary patterns and maintenance of gait speed with age, an indicator of sarcopenia risk (64).
Obesity and food insecurity are both public health concerns influenced by social disparities that impact the quality of life in older adults (64). Social and economic transitions in low and middle-income countries are contributing to an increase in the aging population and, together with the added burden of poverty and inequities, increase food insecurity, obesity, and associated comorbidities (65). Food insecurity is paradoxically associated with obesity in high-income countries. The first hypothesis of whether food insecurity causes obesity was published 27 years ago (66).
Explaining the link between food insecurity and body weight is a complex issue to the fact that it is not well understood what mechanisms cause it. One of the most studied hypotheses describes that food insecurity can cause obesity due to the high calorie and palatable food consumed by low food secure populations such as older adults could be (67). Also, the food insecure population could have limited knowledge about nutrition and resources to follow a healthy lifestyle, so they might have fewer opportunities to keep healthy eating and exercise to prevent and treat obesity (68). Furthermore, older adults’ nutrition knowledge can influence positively or negatively their health status and quality of life (69).
The resource scarcity hypothesis suggests that perceived food insecurity in a permissive environment with access to high-calorie foods may cause positive energy balance in individuals of low social status or socially vulnerable populations (70).
Physical limitations can also be a potential risk factor for food insecurity and the food insecurity-obesity paradox in older adults (71). However, some hypotheses suggest a bidirectional association between food insecurity and physical limitations (72).
In particular, the association between food insecurity and obesity has shown mixed findings by age and gender. This association appears not to be present in older men even though food insecurity and obesity coexist among low-income, older women due to differences in household income, educational attainment, and social networks (73–77).
Not long ago, it was found that individuals who experienced food insecurity had lower muscle mass strength and physical performance (78, 79). On the contrary, functional limitations are significantly associated with increasing food insecurity in older adults, and these associations could be influenced by ethnicity (80). Currently, food insecurity is strongly associated with sarcopenia (81–84). Prevalence of sarcopenia in older adults with food insecurity has been described in 24,4% in low- and middle-income countries; indeed, severe food insecurity was associated with 2.05 times higher odds for sarcopenia (84). Figure 1 illustrates the previously described interaction between food insecurity and SO in older adults.
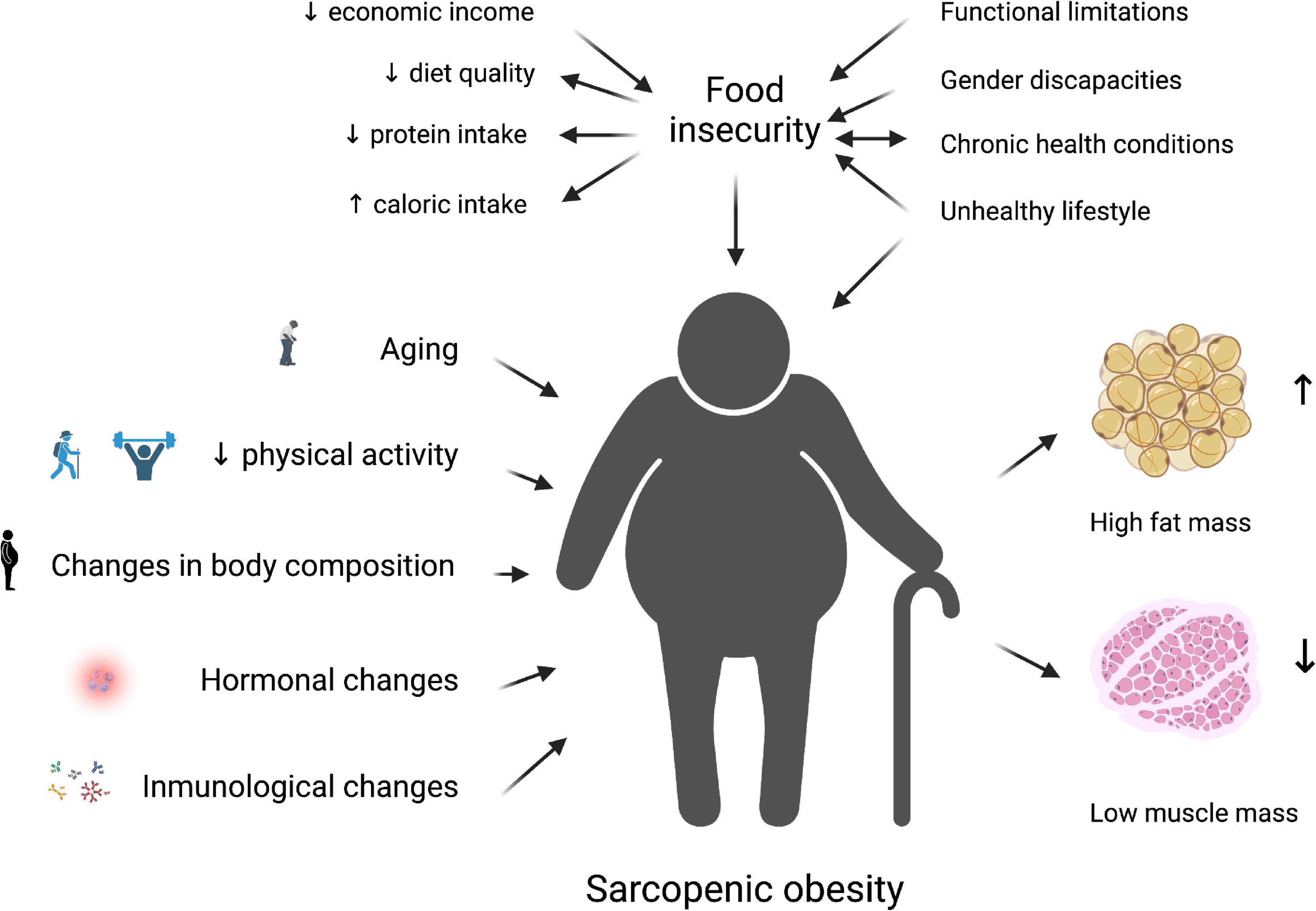
Figure 1. The interrelation between food insecurity and sarcopenic obesity in older adults is related to low economic income, impacting a low-quality diet with a small protein intake with a high energy offer. This scenario is worsened by unhealthy lifestyles and the presence of comorbidities, and body composition alteration due to hormonal and immunological changes, resulting in low muscle mass and high-fat mass. This image was created using Biorender.com.
The double burden of malnutrition has been proposed as a term that can describe a scenery where critical nutrients are poor independently of excess energy intake. In this sense, the excess FM can lead to sarcopenia and, consequently, SO (85).
Against these conditions, improve food insecurity (86), healthy eating patterns such as the Mediterranean, and physical activity (87), have been described as strategies to achieve healthy aging and reduce the risk of obesity and sarcopenia.
Sarcopenia and obesity share pathological factors, including aging and changes in BC. Changes in BC are the leading risk factor for SO. That is why SO needs to be screened and diagnosed adequately. The relationship between food insecurity and SO is mediated mainly by diet and disabilities associated with aging. Food insecurity can determine diet quality which is an important modifiable risk factor in the development of sarcopenia and obesity.
All authors have conceptualized this narrative review, analyzed current literature, wrote the original draft, reviewed the final version, and agreed to the published version of this manuscript.
Special acknowledgments to Miriam Mercedes Moscoso de Maza for her contribution in reviewing the translation of this document.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. United Nations. World Population Prospects: The 2017 Revision, Key Findings and Advance Tables. New York, NY: United Nations (2017).
2. Boutari C, Mantzoros CS. A 2022 update on the epidemiology of obesity and a call to action: as its twin COVID-19 pandemic appears to be receding, the obesity and dysmetabolism pandemic continues to rage on. Metabolism. (2022) 133:155217. doi: 10.1016/j.metabol.2022.155217
3. NCD Risk Factor Collaboration [NCD-RisC]. Trends in adult body-mass index in 200 countries from 1975 to 2014: a pooled analysis of 1698 population-based measurement studies with 192 million participants. Lancet. (2016) 387:1377–96. doi: 10.1016/S0140-6736(16)30054-X
4. Bischoff SC, Boirie Y, Cederholm T, Chourdakis M, Cuerda C, Delzenne NM, et al. Towards a multidisciplinary approach to understand and manage obesity and related diseases. Clin Nutr. (2017) 36:917–38. doi: 10.1016/j.clnu.2016.11.007
5. Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. (2019) 48:601. doi: 10.1093/ageing/afz046
6. Donini LM, Busetto L, Bischoff SC, Cederholm T, Ballesteros-Pomar MD, Batsis JA, et al. Definition and diagnostic criteria for sarcopenic obesity: ESPEN and EASO consensus statement. Obes Facts. (2022) 15:321–35. doi: 10.1159/000521241
7. Barazzoni R, Bischoff S, Boirie Y, Busetto L, Cederholm T, Dicker D, et al. Sarcopenic obesity: time to meet the challenge. Obes Facts. (2018) 11:294–305. doi: 10.1159/000490361
8. Leung CW, Wolfson JA. Food insecurity among older adults: 10-year national trends and associations with diet quality. J Am Geriatr Soc. (2021) 69:964–71. doi: 10.1111/jgs.16971
9. Pereira MHQ, Pereira MLAS, Campos GC, Molina MCB. Food insecurity and nutritional status among older adults: a systematic review. Nutr Rev. (2022) 80:631–44. doi: 10.1093/nutrit/nuab044
10. Batsis J, Petersen C, Gooding T. Association of food insecurity and sarcopenia: the National Health and Nutrition Examination Surveys. Innov Aging. (2020) 4:773. doi: 10.1093/geroni/igaa057.2793
11. Dao T, Green AE, Kim YA, Bae SJ, Ha KT, Gariani K, et al. Sarcopenia and muscle aging: a brief overview. Endocrinol Metab. (2020) 35:716–32. doi: 10.3803/EnM.2020.405
12. Chait A, den Hartigh LJ. Adipose tissue distribution, inflammation and its metabolic consequences, including diabetes and cardiovascular disease. Front Cardiovasc Med. (2020) 7:22. doi: 10.3389/fcvm.2020.00022
13. Silveira EA, Barbosa LS, Noll M, Pinheiro HA, de Oliveira C. Body fat percentage prediction in older adults: agreement between anthropometric equations and DXA. Clin Nutr. (2021) 40:2091–9. doi: 10.1016/j.clnu.2020.09.032
14. Kalinkovich A, Livshits G. Sarcopenic obesity or obese sarcopenia: a cross talk between age-associated adipose tissue and skeletal muscle inflammation as a main mechanism of the pathogenesis. Ageing Res Rev. (2017) 35:200–21. doi: 10.1016/j.arr.2016.09.008
15. The Lancet Diabetes Endocrinology. Should we officially recognise obesity as a disease? Lancet Diabetes Endocrinol. (2017) 5:483. doi: 10.1016/S2213-8587(17)30191-2
16. Flegal KM, Kruszon-Moran D, Carroll MD, Fryar CD, Ogden CL. Trends in obesity among adults in the United States, 2005 to 2014. JAMA. (2016) 315:2284–91. doi: 10.1001/jama.2016.6458
17. Bosello O, Vanzo A. Obesity paradox and aging. Eat Weight Disord. (2021) 26:27–35. doi: 10.1007/s40519-019-00815-4
18. Spanish Society of Parenteral and Enteral Nutrition, Spanish Society of Geriatrics and Gerontology. Nutritional Assessment in the Elderly [Internet]. Madrid (ESP): Galénitas-Nigra Trea. (2008). Available online at: https://www.segg.es/media/descargas/Acreditacion%20de%20Calidad%20SEGG/Residencias/valoracion_nutricional_anciano.pdf (accessed September, 2022).
19. Petermann-Rocha F, Balntzi V, Gray SR, Lara J, Ho FK, Pell JP, et al. Global prevalence of sarcopenia and severe sarcopenia: a systematic review and meta-analysis. J Cachexia Sarcopenia Muscle. (2022) 13:86–99. doi: 10.1002/jcsm.12783
20. Rodríguez-Rejón AI, Ruiz-López MD, Artacho Martín-Lagos R. Diagnóstico y prevalencia de sarcopenia en residencias de mayores: EWGSOP2 frente al EWGSOP1 [Diagnosis and prevalence of sarcopenia in long-term care homes: EWGSOP2 versus EWGSOP1]. Nutr Hosp. (2019) 36:1074–80. doi: 10.20960/nh.02573
21. Larsson L, Degens H, Li M, Salviati L, Lee YI, Thompson W, et al. Sarcopenia: aging-related loss of muscle mass and function. Physiol Rev. (2019) 99:427–511. doi: 10.1152/physrev.00061.2017
22. Marcos-Pardo PJ, González-Gálvez N, López-Vivancos A, Espeso-García A, Martínez-Aranda LM, Gea-García GM, et al. Sarcopenia, diet, physical activity and obesity in European middle-aged and older adults: the lifeage study. Nutrients. (2020) 13:8. doi: 10.3390/nu13010008
23. Dent E, Woo J, Scott D, Hoogendijk EO. Toward the recognition and management of sarcopenia in routine clinical care. Nat Aging. (2021) 1:982–90. doi: 10.1038/s43587-021-00136-1
24. Schaap LA, van Schoor NM, Lips P, Visser M. Associations of sarcopenia definitions, and their components, with the incidence of recurrent falling and fractures: the longitudinal aging study Amsterdam. J Gerontol A Biol Sci Med Sci. (2018) 73:1199–204. doi: 10.1093/gerona/glx245
25. Santanasto AJ, Goodpaster BH, Kritchevsky SB, Miljkovic I, Satterfield S, Schwartz AV, et al. Body composition remodeling and mortality: the health aging and body composition study. J Gerontol A Biol Sci Med Sci. (2017) 72:513–9. doi: 10.1093/gerona/glw163
26. Kim JH, Lim S, Choi SH, Kim KM, Yoon JW, Kim KW, et al. Sarcopenia: an independent predictor of mortality in community-dwelling older Korean men. J Gerontol A Biol Sci Med Sci. (2014) 69:1244–52. doi: 10.1093/gerona/glu050
27. Roh E, Choi KM. Health consequences of sarcopenic obesity: a narrative review. Front Endocrinol. (2020) 11:332. doi: 10.3389/fendo.2020.00332
28. Genovesi LA, Millar A, Tolson E, Singleton M, Hassall E, Kojic M, et al. Systems pharmacogenomics identifies novel targets and clinically actionable therapeutics for medulloblastoma. Genome Med. (2021) 13:103. doi: 10.1186/s13073-021-00920-z
29. Stenholm S, Harris TB, Rantanen T, Visser M, Kritchevsky SB, Ferrucci L. Sarcopenic obesity: definition, cause and consequences. Curr Opin Clin Nutr Metab Care. (2008) 11:693–700. doi: 10.1097/MCO.0b013e328312c37d
30. Frimel TN, Sinacore DR, Villareal DT. Exercise attenuates the weight-loss-induced reduction in muscle mass in frail obese older adults. Med Sci Sports Exerc. (2008) 40:1213–9. doi: 10.1249/MSS.0b013e31816a85ce
31. Lynch GM, Murphy CH, Castro EM, Roche HM. Inflammation and metabolism: the role of adiposity in sarcopenic obesity. Proc Nutr Soc. (2020) 16:1–13. doi: 10.1017/S0029665120007119
32. Mendham AE, Goedecke JH, Micklesfield LK, Brooks NE, Faber M, Christensen DL, et al. Understanding factors associated with sarcopenic obesity in older African women from a low-income setting: a cross-sectional analysis. BMC Geriatr. (2021) 21:247. doi: 10.1186/s12877-021-02132-x
33. Kawai T, Autieri MV, Scalia R. Adipose tissue inflammation and metabolic dysfunction in obesity. Am J Physiol Cell Physiol. (2021) 320:C375–91. doi: 10.1152/ajpcell.00379.2020
34. Hong SH, Choi KM. Sarcopenic obesity, insulin resistance, and their implications in cardiovascular and metabolic consequences. Int J Mol Sci. (2020) 21:494. doi: 10.3390/ijms21020494
35. Geraci A, Calvani R, Ferri E, Marzetti E, Arosio B, Cesari M. Sarcopenia and menopause: the role of estradiol. Front Endocrinol. (2021) 12:682012. doi: 10.3389/fendo.2021.682012
36. Morley JE. Hormones and sarcopenia. Curr Pharm Des. (2017) 23:4484–92. doi: 10.2174/1381612823666161123150032
37. Morgan PT, Smeuninx B, Breen L. Exploring the impact of obesity on skeletal muscle function in older age. Front Nutr. (2020) 7:569904. doi: 10.3389/fnut.2020.569904
38. Trouwborst I, Verreijen A, Memelink R, Massanet P, Boirie Y, Weijs P, et al. Exercise and nutrition strategies to counteract sarcopenic obesity. Nutrients. (2018) 10:605. doi: 10.3390/nu10050605
39. Canda Moreno AS. Puntos de corte de diferentes parámetros antropométricos para el diagnóstico de sarcopenia [Anthropometric parameters’ cut-off points for diagnosis of sarcopenia]. Nutr Hosp. (2015) 32:765–70. doi: 10.3305/nh.2015.32.2.9193
40. Choi KM. Sarcopenia and sarcopenic obesity. Korean J Intern Med. (2016) 31:1054–60. doi: 10.3904/kjim.2016.193
41. Lee K, Shin Y, Huh J, Sung YS, Lee IS, Yoon KH, et al. Recent issues on body composition imaging for sarcopenia evaluation. Korean J Radiol. (2019) 20:205–17. doi: 10.3348/kjr.2018.0479
42. Tagliafico AS, Bignotti B, Torri L, Rossi F. Sarcopenia: how to measure, when and why. Radiol Med. (2022) 12:228–37. doi: 10.1007/s11547-022-01450-3
43. Chun SW, Kim W, Choi KH. Comparison between grip strength and grip strength divided by body weight in their relationship with metabolic syndrome and quality of life in the elderly. PLoS One. (2019) 14:e0222040. doi: 10.1371/journal.pone
44. Batsis JA, Barre LK, Mackenzie TA, Pratt SI, Lopez-Jimenez F, Bartels SJ. Variation in the prevalence of sarcopenia and sarcopenic obesity in older adults associated with different research definitions: dual-energy X-ray absorptiometry data from the National Health and Nutrition Examination Survey 1999-2004. J Am Geriatr Soc. (2013) 61:974–80. doi: 10.1111/jgs.12260
45. Food and Agriculture Organization of the United Nations. The State of Food Security and Nutrition in the World 2022 the State of Food Security and Nutrition in the World 2022: Repurposing Food and Agricultural Policies to Make Healthy Diets More Affordable. Rome: Food & Agriculture Organization of the United Nations (2022).
46. Schroeder K, Smaldone A. Food insecurity: a concept analysis. Nurs Forum. (2015) 50:274–84. doi: 10.1111/nuf.12118
47. U.S. Department of Agriculture. Definition of Food Security. (2022). Available online at: https://www.ers.usda.gov/topics/food-nutrition-assistance/food-security-in-the-us/definitions-of-food-security/ (accessed July 15, 2022).
48. Choi SK, Fram MS, Frongillo EA. Very low food security in US households is predicted by complex patterns of health, economics, and service participation. J Nutr. (2017) 147:1992–2000. doi: 10.3945/jn.117.253179
49. Fernandes SG, Rodrigues AM, Nunes C, Santos O, Gregório MJ, de Sousa RD, et al. Food insecurity in older adults: results from the epidemiology of chronic diseases cohort study 3. Front Med. (2018) 5:203. doi: 10.3389/fmed.2018.00203
50. Tucher EL, Keeney T, Cohen AJ, Thomas KS. Conceptualizing food insecurity among older adults: development of a summary indicator in the national health and aging trends study. J Gerontol B Psychol Sci Soc Sci. (2021) 76:2063–72. doi: 10.1093/geronb/gbaa147
51. Pequeno NPF, Cabral NLDA, Oliveira ÂGRC, Crispim SP, Rocha C, Marchioni DM, et al. Chronic diseases and emotional disorders are associated with low perception of quality of life in food insecurity/security. Front Public Health. (2022) 10:893601. doi: 10.3389/fpubh.2022.893601
52. Morze J, Danielewicz A, Hoffmann G, Schwingshackl L. Diet quality as assessed by the healthy eating index, alternate healthy eating index, dietary approaches to stop hypertension score, and health outcomes: a second update of a systematic review and meta-analysis of cohort studies. J Acad Nutr Diet. (2020) 120:1998–2031.e15. doi: 10.1016/j.jand.2020.08.076
53. Miller V, Webb P, Micha R, Mozaffarian D, Global Dietary Database. Defining diet quality: a synthesis of dietary quality metrics and their validity for the double burden of malnutrition. Lancet Planet Health. (2020) 4:e352–70. doi: 10.1016/S2542-5196(20)30162-5
54. Jimenez Rincon S, Dou N, Murray-Kolb LE, Hudy K, Mitchell DC, Li R, et al. Daily food insecurity is associated with diet quality, but not energy intake, in winter and during COVID-19, among low-income adults. Nutr J. (2022) 21:19. doi: 10.1186/s12937-022-00768-y
55. Hanson KL, Connor LM. Food insecurity and dietary quality in US adults and children: a systematic review. Am J Clin Nutr. (2014) 100:684–92. doi: 10.3945/ajcn.114.084525
56. Leung CW, Tester JM. The association between food insecurity and diet quality varies by race/ethnicity: an analysis of National Health and Nutrition Examination Survey 2011-2014 results. J Acad Nutr Diet. (2019) 119:1676–86. doi: 10.1016/j.jand.2018.10.011
57. Fanelli Kuczmarski M, Stave Shupe E, Pohlig RT, Rawal R, Zonderman AB, Evans MK. A longitudinal assessment of diet quality and risks associated with malnutrition in socioeconomic and racially diverse adults. Nutrients. (2019) 11:2046. doi: 10.3390/nu11092046
58. Durán-Agüero S, Ortiz A, Pérez-Armijo P, Vinueza-Veloz MF, Ríos-Castillo I, Camacho-Lopez S, et al. Quality of the diet during the COVID-19 pandemic in 11 Latin-American countries. J Health Popul Nutr. (2022) 41:33. doi: 10.1186/s41043-022-00316-8
59. Long T, Zhang K, Chen Y, Wu C. Trends in diet quality among older US adults from 2001 to 2018. JAMA Netw Open. (2022) 5:e221880. doi: 10.1001/jamanetworkopen.2022.1880
60. Carrier N, Villalon L, Lengyel C, Slaughter SE, Duizer L, Morrison-Koechl J, et al. Diet quality is associated with malnutrition and low calf circumference in Canadian long-term care residents. BMC Nutr. (2019) 5:57. doi: 10.1186/s40795-019-0314-7
61. Rodríguez-Rejón AI, Ruiz-López MD, Artacho R. Dietary intake and associated factors in long-term care homes in Southeast Spain. Nutrients. (2019) 11:266. doi: 10.3390/nu11020266
62. Bloom I, Pilgrim A, Jameson KA, Dennison EM, Sayer AA, Roberts HC, et al. The relationship of nutritional risk with diet quality and health outcomes in community-dwelling older adults. Aging Clin Exp Res. (2021) 33:2767–76. doi: 10.1007/s40520-021-01824-z
63. Hengeveld LM, Wijnhoven HAH, Olthof MR, Brouwer IA, Harris TB, Kritchevsky SB, et al. Prospective associations of poor diet quality with long-term incidence of protein-energy malnutrition in community-dwelling older adults: the health, aging, and body composition (Health ABC) study. Am J Clin Nutr. (2018) 107:155–64. doi: 10.1093/ajcn/nqx020
64. Van Elswyk ME, Teo L, Lau CS, Shanahan CJ. Dietary patterns and the risk of sarcopenia: a systematic review and meta-analysis. Curr Dev Nutr. (2022) 6:nzac001. doi: 10.1093/cdn/nzac001
65. Pan L, Sherry B, Njai R, Blanck HM. Food insecurity is associated with obesity among US adults in 12 states. J Acad Nutr Diet. (2012) 112:1403–9. doi: 10.1016/j.jand.2012.06.011
66. Mendham AE, Lundin-Olsson L, Goedecke JH, Micklesfield LK, Christensen DL, Gallagher IJ, et al. Sarcopenic obesity in Africa: a call for diagnostic methods and appropriate interventions. Front Nutr. (2021) 8:661170. doi: 10.3389/fnut.2021.661170
68. Angeles-Agdeppa I, Toledo MB, Zamora JAT. Moderate and severe level of food insecurity is associated with high calorie-dense food consumption of Filipino households. J Nutr Metab. (2021) 2021:5513409. doi: 10.1155/2021/5513409
69. van der Velde LA, Schuilenburg LA, Thrivikraman JK, Numans ME, Kiefte-de Jong JC. Needs and perceptions regarding healthy eating among people at risk of food insecurity: a qualitative analysis. Int J Equity Health. (2019) 18:184. doi: 10.1186/s12939-019-1077-0
70. Jeruszka-Bielak M, Kollajtis-Dolowy A, Santoro A, Ostan R, Berendsen AAM, Jennings A, et al. Are nutrition-related knowledge and attitudes reflected in lifestyle and health among elderly people? A study across five European countries. Front Physiol. (2018) 9:994. doi: 10.3389/fphys.2018.00994
71. Dhurandhar EJ. The food-insecurity obesity paradox: a resource scarcity hypothesis. Physiol Behav. (2016) 162:88–92. doi: 10.1016/j.physbeh.2016.04.025
72. Brewer DP, Catlett CS, Porter KN, Lee JS, Hausman DB, Reddy S, et al. Physical limitations contribute to food insecurity and the food insecurity-obesity paradox in older adults at senior centers in Georgia. J Nutr Elder. (2010) 29:150–69. doi: 10.1080/01639361003772343
73. Jackson JA, Branscum A, Tang A, Smit E. Food insecurity and physical functioning limitations among older U.S. adults. Prev Med Rep. (2019) 14:100829. doi: 10.1016/j.pmedr.2019.100829
74. Hernandez DC, Reesor L, Murillo R. Gender disparities in the food insecurity-overweight and food insecurity-obesity paradox among low-income older adults. J Acad Nutr Diet. (2017) 117:1087–96. doi: 10.1016/j.jand.2017.01.014
75. Thomas MK, Lammert LJ, Beverly EA. Food insecurity and its impact on body weight, type 2 diabetes, cardiovascular disease, and mental health. Curr Cardiovasc Risk Rep. (2021) 15:15. doi: 10.1007/s12170-021-00679-3
76. Domingos TB, Sichieri R, Salles-Costa R. Sex differences in the relationship between food insecurity and weight status in Brazil. Br J Nutr. (2022) 19:1–19. doi: 10.1017/S0007114522001192
77. Martin-Fernandez J, Caillavet F, Lhuissier A, Chauvin P. Food insecurity, a determinant of obesity? – An analysis from a population-based survey in the Paris metropolitan area, 2010. Obes Facts. (2014) 7:120–9. doi: 10.1159/000362343
78. Nzinga H. Broussard “What explains gender differences in food insecurity?”. Food Policy. (2019) 83:180–94. doi: 10.1016/j.foodpol.2019.01.003
79. Shafiee G, Heshmat R, Ostovar A, Nabipour I, Larijani B. Sarcopenia disease in Iran: an overview. J Diabetes Metab Disord. (2019) 18:665–74. doi: 10.1007/s40200-019-00452-9
80. Lee K. Relationships of food security with skeletal muscle mass and handgrip strength by sex. Nutrition. (2022) 102:111746. doi: 10.1016/j.nut.2022.111746
81. Petersen CL, Brooks JM, Titus AJ, Vasquez E, Batsis JA. Relationship between food insecurity and functional limitations in older adults from 2005-2014 NHANES. J Nutr Gerontol Geriatr. (2019) 38:231–46. doi: 10.1080/21551197.2019.1617219
82. Pérez-Zepeda M, Castrejón-Pérez R, Wynne-Bannister E, García-Peña C. Frailty and food insecurity in older adults. Public Health Nutr. (2016) 19:2844–9. doi: 10.1017/S1368980016000987
83. Smith L, Jacob L, Barnett Y, Butler LT, Shin JI, López-Sánchez GF, et al. Association between food insecurity and sarcopenia among adults aged =65 years in low- and middle-income countries. Nutrients. (2021) 13:1879. doi: 10.3390/nu13061879
84. Lynch DH, Petersen CL, Van Dongen MJ, Spangler HB, Berkowitz SA, Batsis JA. Association between food insecurity and probable sarcopenia: data from the 2011–2014 National Health and Nutrition Examination Survey. Clin Nutr. (2022) 41:1861–73. doi: 10.1016/j.clnu.2022.07.002
85. Barazzoni R, Gortan Cappellari G. Double burden of malnutrition in persons with obesity. Rev Endocr Metab Disord. (2020) 21:307–13. doi: 10.1007/s11154-020-09578-1
86. Gomes LA, Gregório MJ, Iakovleva TA, Sousa RD, Bessant J, Oliveira P, et al. A home-based eHealth intervention for an older adult population with food insecurity: feasibility and acceptability study. J Med Internet Res. (2021) 23:e26871. doi: 10.2196/26871
Keywords: food insecurity, low food security, sarcopenic obesity, sarcopenia, older adults
Citation: Fonseca-Pérez D, Arteaga-Pazmiño C, Maza-Moscoso CP, Flores-Madrid S and Álvarez-Córdova L (2022) Food insecurity as a risk factor of sarcopenic obesity in older adults. Front. Nutr. 9:1040089. doi: 10.3389/fnut.2022.1040089
Received: 08 September 2022; Accepted: 03 October 2022;
Published: 20 October 2022.
Edited by:
Diana Cardenas, El Bosque University, ColombiaReviewed by:
Joanne Karam, University of Balamand, LebanonCopyright © 2022 Fonseca-Pérez, Arteaga-Pazmiño, Maza-Moscoso, Flores-Madrid and Álvarez-Córdova. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ludwig Álvarez-Córdova, bHVkd2lnLmFsdmFyZXpAY3UudWNzZy5lZHUuZWM=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.