 Wenqian Li
Wenqian Li Chang Liu1†
Chang Liu1†- 1Department of Reproductive Medicine, First Affiliated Hospital, School of Medicine, Shihezi University, Shihezi, China
- 2Department of Obstetrics and Gynecology, Reproductive Medical Center, Peking University Third Hospital, Beijing, China
Polycystic ovary syndrome (PCOS) is a common reproductive endocrine disease that is characterized by oligo-ovulation or anovulation, hyperandrogenism, and polycystic ovaries observed using ultrasound with high clinical heterogeneity. At present, the etiology of PCOS is not clear but is thought to be related to genetic, metabolic, endocrine and environmental factors. Hyperandrogenism interacts with insulin resistance and overweight/obesity, forming a vicious cycle of mutual promotion and participating in the occurrence and progression of PCOS. Oxidative stress (OS) refers to the imbalance between the oxidation system and antioxidation system in the human body, which is associated with the occurrence and development of various diseases. Recent studies have shown that OS may be closely related to ovulation disorders in PCOS, and antioxidants can improve the oxidative stress state of PCOS. However, previous studies did not examine the effect of the interaction between OS and hyperandrogenism, insulin resistance or overweight/obesity on ovulation disorders in PCOS. This article reviews the interaction between OS and hyperandrogenism, insulin resistance and overweight/obesity; the effects of OS, hyperandrogenism, insulin resistance and overweight/obesity on ovulation disorders in PCOS; and the application of antioxidants in PCOS.
Introduction
Polycystic ovary syndrome (PCOS) is a clinical syndrome characterized by anovulation or oligo-ovulation, hyperandrogenism and polycystic ovaries, affecting the female reproductive system, endocrine metabolism and psychological status. The overall prevalence rate is 6%-10%(1), and PCOS is an important cause of ovulation disorder infertility. The clinical manifestations of PCOS have high heterogeneity. Most patients also have endocrine and metabolic disorders, such as insulin resistance, obesity, dyslipidemia and compensatory hyperinsulinemia. Because its pathogenesis has not been fully elucidated, PCOS has gradually become a research hotspot in recent years. Previous studies have confirmed that genetic factors, environmental factors and epigenetics are related to the occurrence of PCOS. Hyperandrogenemia and insulin resistance, as the pathophysiological basis of PCOS, play an important role in its occurrence and development. At the same time, overweight/obesity can make PCOS symptoms worse by amplifying various features. Oxidative stress (OS) refers to the imbalance between oxidation and antioxidation in the human body. The accumulation of excessive oxidative active substances leads to tissue cell dysfunction. It has been confirmed that OS is involved in the regulation of the occurrence and development of various diseases, especially PCOS. How does OS regulate hyperandrogenism, insulin resistance and overweight/obesity, leading to ovulation disorders in PCOS patients? This paper reviews this issue.
Polycystic ovary syndrome
Polycystic ovary syndrome (PCOS) is one of the most common reproductive endocrine diseases. The incidence of PCOS is approximately 6-10% in the population (1). PCOS has high clinical heterogeneity: it can have no obvious clinical symptoms, or the symptoms can include irregular menstruation, infertility, androgen excess, obesity and so on (2). At the same time, PCOS is often accompanied by embryonic high androgen exposure, endocrine and metabolic disorders, chronic inflammation, immune abnormalities, oxidative stress and other risk factors. The risk of cardiovascular and cerebrovascular diseases, type II diabetes, endometrial hyperplasia, endometrial cancer, metabolic syndrome and neurodegenerative diseases is increased in the long term, which seriously affects the physical and mental health of women (3–6). At present, the Rotterdam diagnostic criteria established in 2003 are internationally accepted. PCOS diagnosis requires two of the following three items: anovulation or oligo-ovulation, hyperandrogenism, and polycystic ovaries. Other causes that may lead to hyperandrogenism, such as congenital adrenal hyperplasia and Cushing syndrome, can be diagnosed as PCOS (7). To date, there is no unified and clear conclusion on the mechanism of PCOS in the medical field, but scholars generally believe that PCOS is the result of the interaction between environmental factors and genetic factors (8).
Oxidative stress
Oxidative stress (OS) refers to the imbalance between the oxidation system and antioxidation system in the human body. The accumulation of active oxidation substances in the body causes protein and DNA damage and lipid peroxidation, which further lead to cell dysfunction (9). Reactive oxygen species (ROS) and reactive nitrogen species (RNS) are two basic types of oxidative active molecules in the body. Typical representative types of ROS include superoxide anion (O2–), hydroxyl radical (OH) and hydrogen peroxide (H2O2). The main source of ROS in vivo is oxidative phosphorylation of mitochondria, and the secondary sources are cytochrome P450 enzyme, peroxisome, xanthine oxidase and activated inflammatory cells (10). RNS includes nitric oxide (NO) and nitrogen dioxide (NO2)(11). Ionizing radiation, metal ions, and pollutants in the atmosphere are important sources of exogenous oxidizing active molecules (12). The body’s aging and inflammatory response can also promote the production of oxidative active molecules. ROS and RNS have dual effects on cells. Low and medium concentrations of oxidative active molecules can participate in a variety of physiological functions (such as the body’s anti-infection process), or they can be used as a second messenger for cells that are responsible for intracellular signal transduction, gene expression regulation, and cell proliferation, differentiation and apoptosis control (13). Antioxidants in the body include antioxidant enzymes and non-enzymatic antioxidants. Antioxidant enzymes include superoxide dismutase (SOD), catalase, and glutathione (GSH) peroxidase, and non-enzymatic antioxidants include vitamin C, vitamin E, GSH, taurine, hypotaurine, zinc, selenium, carotenoids, and metal binding proteins. All of them have the ability to scavenge oxidative active molecules and maintain the oxidant/antioxidant balance (14). Excessive oxidative active molecules can affect the function of biological molecules by modifying protein molecules, causing lipid peroxidation and DNA damage. At the same time, when the body’s antioxidant defense function is not enough to remove a large number of oxidized active molecules, the imbalance between oxidant and antioxidant levels will eventually lead to OS, resulting in cell damage and causing a variety of biological processes (15).
Oxidative stress in polycystic ovary syndrome
Oxidative stress is associated with the occurrence and development of various diseases, such as cardiovascular and cerebrovascular diseases, neurodegenerative diseases, multiple cancers and type II diabetes, which seriously threaten human health (16–20). Previous studies have shown that OS is closely related to the occurrence and development of PCOS. Papalou et al. (21) analyzed the role of OS in PCOS and suggested that the accumulation of oxidative active molecules in PCOS patients cannot be offset by antioxidant defense function. OS is an important part of PCOS pathophysiology and regulates the occurrence and development of PCOS with other pathogenic factors. When studying the relationship between circulating apoptosis markers and oxidative stress in PCOS patients, Uyanikoglu et al. (22) found that in the blood of PCOS patients, the total oxidation state, total antioxidation state and oxidative stress index were all higher than those of healthy women in the control group, and the total oxidation state was higher than the total antioxidation state, indicating that there was an imbalance between oxidants and antioxidants in PCOS patients. Similarly, the meta-analysis results of Murri et al. (23) suggested that the levels of OS markers in the blood of PCOS patients, such as homocysteine, asymmetric dimethylarginine, malondialdehyde (MDA) and SOD, were significantly higher than those in the control group, while the levels of antioxidant markers, such as GSH and paraoxonase-1, were significantly lower than those in the control group.
Oxidative stress, Hyperandrogenemia, insulin resistance and ovulation disorder in polycystic ovary syndrome
Hyperandrogenism
Hyperandrogenism (HA) is one of the main clinical features of PCOS. The proportion of patients with elevated serum androgen is 60-75% (24). Elevated serum testosterone level may be related to the occurrence of PCOS (25). Gonadotropin-releasing hormone (GnRH) pulse secretion in females occurs during adrenarche. By regulating the gonadal axis, the secretion of adrenocorticotropic hormone (ACTH) and luteinizing hormone (LH) is increased (26), thereby stimulating the secretion of excessive androgens from the adrenal gland and ovary. Because of the high reactivity of 17-ketosteroid to adrenocorticotropic hormone, the synthesis of androgen in the adrenal gland is active, which can significantly increase the level of serum androgen (27). Therefore, adrenal androgen secretion appears earlier than ovarian steroid secretion, which may be the initial source of female androgen (28). The increase in LH pulse secretion frequency can promote the production of excessive androgen in theca-interstitial cells. Although progesterone can slow down the pulse frequency of GnRH by inhibiting the discharge of GnRH neurons, excessive androgen can still accelerate the pulse frequency of LH by reducing the effect of progesterone (29), causing the secretion of androgen in ovarian tissue. In addition, PCOS patients usually have insulin resistance, and their insulin levels are elevated (30). Insulin can directly or synergistically act with LH to stimulate the proliferation of theca-interstitial cells and inhibit the production and secretion of serum sex hormone binding globulin (SHBG), thereby improving the level and bioavailability of serum androgen (31, 32). At the same time, a high insulin level can inhibit the production of insulin-like growth factor-I (IGF-I) receptor, indirectly increase the level and biological activity of IGF-I, and facilitate cooperation with LH to indirectly stimulate androgen production (33).
Insulin resistance
Insulin resistance (IR) refers to the physiological concentration of insulin required to promote the ability of peripheral tissue cells to use glucose, and 50-80% of PCOS patients have varying degrees of IR (34). The combination of insulin and its receptor causes tyrosine phosphorylation of insulin receptor substrate (IRS), activates signal transduction pathways, triggers a series of cascade reactions, and realizes its physiological function (35). Of these effects, tyrosine phosphorylation of the IRS plays an important role in the process of insulin signal transduction. Defects in insulin signal transduction are the main cause of IR in PCOS patients. In addition, PCOS tissue (especially adipose tissue) cells are infiltrated by macrophages so that the body has a low degree of inflammation (36). Macrophages in adipose tissue can produce a large number of proinflammatory factors, such as tumor necrosis factor-α (TNF-α) and interleukin (IL)-1. They play a role in the paracrine and endocrine mechanisms, activate inflammatory pathways in insulin target cells, activate serine kinases in adipocytes, and cause serine phosphorylation of IRS-1, which hinders the signal transduction of insulin (37–39). The activation of some serine kinases can induce the production of suppressor of cytokine signaling 3 (SOCS3), thereby inhibiting the expression of IRS-1 and tyrosine phosphorylation, interfering with insulin activity, reducing the sensitivity of tissue cells to insulin, and ultimately leading to IR (40, 41).
Interaction between oxidative stress, Hyperandrogenemia, and insulin resistance: A vicious cycle
A large number of studies have confirmed that PCOS patients are in a long-term state of oxidative stress imbalance, and OS has become a key factor in the pathogenesis of PCOS (23, 42). As an important pathophysiological basis of PCOS, HA and IR can be induced or aggravated under OS imbalance. In PCOS, a glucose diet can induce an increase in OS levels and activate nuclear transcription factor-kB, causing the body to be in a state of chronic low-grade inflammation and promoting the expression of various inflammatory factors, such as TNF-α and IL-6 (43, 44). On the one hand, TNF-α in the ovary can stimulate the proliferation of theca-interstitial cells (45), and the expression of cytochrome P450-17α-hydroxylase (CYP17) is upregulated in the inflammatory state, increasing the production of androgen (46). On the other hand, the expression of hepatocyte nuclear factor-4α (HNF-4α) in the OS state is downregulated, which increases the biological activity of androgen by inhibiting the expression and secretion of SHBG and eventually leads to HA (47). HA in PCOS can improve the sensitivity of mononuclear cells (MNCs) to glucose and increase the production of ROS and inflammatory factors by promoting the preactivation of MNCs (48). At the same time, TNF-α, as a mediating factor of IR, activates the inflammatory pathway in insulin target cells to cause serine phosphorylation of IRS-1, resulting in defects in the insulin signaling pathway; interferes with insulin activity; hinders the uptake of glucose by muscle and adipose tissue; and causes IR. The sensitivity of tissue to insulin decreased in the IR state, and compensatory hyperinsulinemia occurred. High-level insulin stimulates the proliferation of theca-interstitial cells, increases the production and secretion of testosterone, reduces the serum SHBG level, improves the bioavailability of serum androgen, and further aggravates HA. IR can also promote liver glycogen synthesis and adipose tissue mobilization so that serum free fatty acid (FFA) levels increase (49). High free fatty acids and a high glucose state promote the production of ROS, and OS imbalance is further aggravated. OS interacts with HA and IR, forming a vicious cycle of mutual promotion and participating in the occurrence and progression of PCOS.
Overweight/obesity
Overweight/obesity is one of the common clinical manifestations of PCOS, and 40-70% of PCOS patients having obesity (50). Relevant evidence indicates that metabolic abnormalities tend to appear to the overweight/obese PCOS patients (especially abdominal obesity) compared to the PCOS patients with normal BMI (51). Overweight and obese PCOS patients have a considerable amount of macrophage infiltration in their adipose tissues, which has a significantly positive correlation with the severity of obesity (52). Adipose macrophages are highly pro-inflammatory in property; they raise levels of oxidatively active substances and promote the development of OS and low-grade inflammatory states (53). Pro-inflammatory factors generated by macrophages work on adipocytes; therefore, more macrophages accumulate, thus a positive feedback mechanism is formed, followed by an aggravated OS and low-level inflammation. In addition, these pro-inflammatory factors can activate the pathway of inflammation inside insulin target cells thus block the signal transduction of insulin. Furthermore, abnormal lipid metabolism is also a clinical manifestation in overweight/obese population, the FFA level increase causes IR by activating serine kinase among insulin target cells and interfering with insulin signal transduction (39). The adipocytes secreted by overweight/obese PCOS patients, such as adiponectin, resistin, leptin, and other adipokines are strongly correlated to IR (54), leading to HA in an indirect way, and HA can cause abdominal fat accumulation (55). As a consequence, a vicious circle forms causing more serious obesity. Therefore, overweight/obesity caused by inappropriate diet and insufficient exercise can result in PCOS, and the vicious cycle of IR, HA and OS may promote the development of PCOS. Relevant evidence reveals that an appropriate diet, with antioxidants addition and bariatric surgery can be beneficial for those overweight/obese patients with OS imbalance (56–58).
Effect of oxidative stress, Hyperandrogenemia, and insulin resistance on ovulation disorder in polycystic ovary syndrome
As the basis of follicular growth and development, the follicular fluid microenvironment is particularly important in determining follicular quality. There are various sources of reactive oxygen species in the follicular fluid microenvironment. Related evidence shows that OS markers are expressed in human ovaries in normal cycles (59, 60). In normal follicular fluid, oxidation occurs in a relatively balanced state; that is, there are not only ROS at the physiological level in follicular fluid but also a variety of antioxidant enzymes and non-enzymatic oxidants (61). As the main energy supply organ in follicular fluid, mitochondrial activity is closely related to follicular quality. In the OS-activated state, the follicular fluid of PCOS patients produces excessive ROS, resulting in an imbalance of oxidation/antioxidation in the microenvironment and damaging the function of mitochondria in the follicular fluid (62). Dysfunctional mitochondria arrest and degrade oocytes during meiosis, directly damage oocytes, and cause follicular apoptosis, resulting in ovulation disorders (63). In addition to the changes in the follicular fluid microenvironment, abnormal follicular growth and development are the primary causes of PCOS ovulation disorder. Ovulation disorder in PCOS is characterized by antral follicle growth arrest, and its mechanism is not yet clear. At present, it is believed that the causes can be divided into two aspects: early developmental abnormalities of endogenous follicles independent of gonadotropins and endocrine disorders, such as excessive proliferation of antral follicles caused by HA and IR and follicular development arrest (64). Abnormal early follicular development leads to the inability to choose the dominant follicles, which is a major cause of PCOS ovulation disorder. HA can stimulate the initiation of early follicular development by increasing the expression of IGF-1 receptor, resulting in excessive proliferation of antral follicles and an increase in the proportion of small follicles growing in the ovary (65–67). Hyperinsulinemia and/or high levels of LH synergistically improve the sensitivity of granulosa cells to LH, leading to premature differentiation of granulosa cells and an imbalance in LH/FSH levels, so that FSH deficiency destroys the choice of dominant follicles, leading to the accumulation of small antral follicles (68, 69); at the same time, the premature response of small antral follicles to high LH promotes the early terminal differentiation of follicles (70). In the ovary, the proliferation and differentiation of granulosa cells play an important role in the development of follicles. In granulosa cells before ovulation, FSH regulates glucose conversion into glycogen storage through the IRS-2/PI3K/Akt2 pathway, which plays an important role in the occurrence, development and ovulation of follicles (71). In PCOS, high LH can cause FSH signaling pathway defects and interfere with glucose uptake and glycogen synthesis in granulosa cells, resulting in follicular growth arrest and ovulation disorders (72). In addition, a new study found that HA can increase OS imbalance and low-level inflammation in the ovary and upregulate the expression of inflammatory factors by activating NLRP3 inflammatory bodies, thereby inducing pyroptosis of ovarian granulosa cells, damaging follicular function and leading to ovulation disorders (73).
OS, HA and IR play an important role in the development of PCOS, and the vicious cycle between them leads to and aggravates ovulation disorder in PCOS (Figure 1). The above evidence explains the related mechanism of OS, HA and IR in ovulation disorders in the physiological mechanism of PCOS but does not clarify whether OS can cause PCOS ovulation disorders in other ways, such as inducing immune dysfunction or regulating gene expression. Therefore, we need more evidence to explore the mechanism of OS on PCOS ovulation disorder from different perspectives.
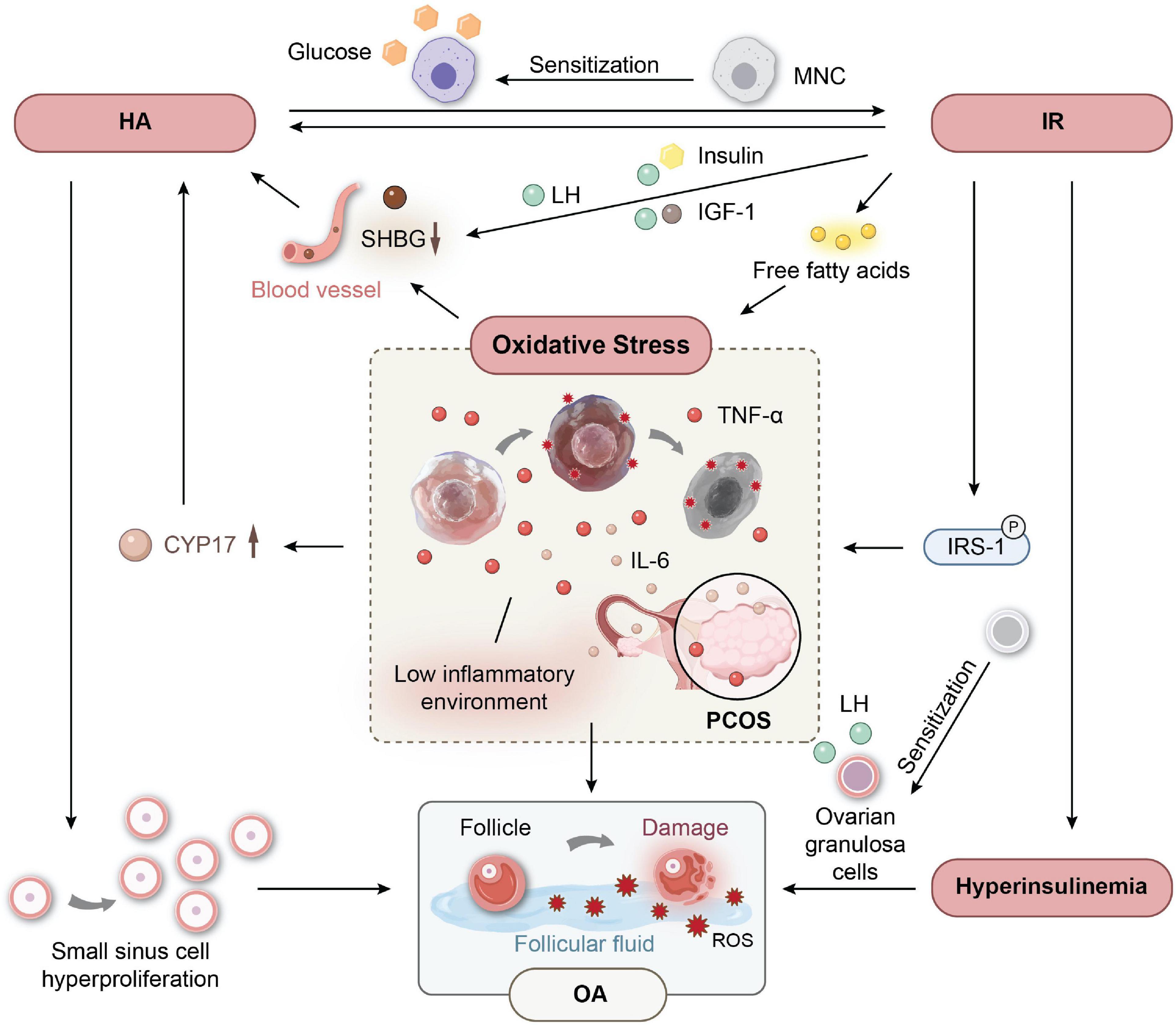
Figure 1. The vicious circle between oxidative stress (OS) and Hyperandrogenemia (HA), insulin resistance (IR) leads to ovulation disorder in (polycystic ovary syndrome) PCOS.
The application of antioxidants in polycystic ovary syndrome
Based on a large number of studies confirming that PCOS patients do exhibit varying degrees of OS, antioxidant therapy may become an important direction for the treatment of PCOS (74) (Table 1). At present, there have been clinical studies on the use of antioxidants in patients with PCOS. Relevant evidence shows that antioxidants can effectively reduce the levels of OS and inflammatory markers in PCOS, improve the antioxidant capacity of the body and improve the OS imbalance. Jamilian et al. (75) found in clinical trials evaluating the effects of vitamin D and omega-3 fatty acids on PCOS patients that the combined use of vitamin D and omega-3 in the treatment of PCOS could significantly reduce the levels of serum total testosterone and serum high-sensitivity C-reactive protein (hs-CRP) and MDA, significantly reduce the expression of the IL-1 gene and significantly increase the level of serum total antioxidant capacity (TAC). In addition, Jamilian et al. (76) evaluated the effect of combined vitamin E and omega-3 supplementation on PCOS patients and found that the combined application of vitamin E and omega-3 could significantly reduce the expression of the IL-8 and TNF-α genes and upregulate the expression of peroxisome proliferator-activated receptor-γ (PPAR-γ). In the above two experiments, the OS status of PCOS patients was significantly improved. In another experiment, Afshar et al. (77) found that the combined application of magnesium and zinc can improve serum TAC and significantly downregulate the expression levels of the proinflammatory cytokines IL-1 and TNF-α so that the OS level of PCOS patients was significantly improved. Rahmani et al. (78) found that in their study, the expression levels of the proinflammatory cytokines IL-1, IL-8, and TNF-α in PCOS patients treated with CoQ10 were significantly downregulated in their experimental group. Mousavi et al. (79) found in a study of the effects of magnesium and/or melatonin on the metabolism of PCOS women that melatonin significantly reduced the level of TNF-α, and the combination of magnesium and melatonin significantly increased the level of TAC. In addition, studies have confirmed that antioxidants can not only reduce OS levels but also improve the clinical symptoms of PCOS patients. Shokrpour et al. (80) found in a study on the treatment of PCOS with magnesium and vitamin D that the combined application of magnesium and vitamin D could effectively reduce the level of hs-CRP and the incidence of hairy diseases, significantly increase the levels of TAC and NO, and reduce the OS level of the body. In another experiment, Gharaei et al. (81) found that astaxanthin treatment significantly increased TAC and increased the expression of nuclear factor E2-related factor 2 (Nrf2) and heme oxygenase-1 (HO-1) in PCOS. At the same time, MII oocytes and high-quality embryos were significantly increased, but there were no significant differences in MDA, SOD and OS markers in follicular fluid. Antioxidants can also significantly improve the IR status of PCOS patients. Tauqir et al. (82) found in a study of acetyl levocarnitine (ALC), metformin, and pioglitazone in the treatment of PCOS that the combination of ALC in the treatment of PCOS could more effectively reduce the fasting insulin level and significantly improve the levels of serum total testosterone, FSH and LH. Similarly, Kazemi et al. (83) found in a study of ellagic acid in the treatment of PCOS that ellagic acid could reduce the concentrations of serum insulin, MDA and serum total testosterone; downregulate the expression level of TNF-α; and significantly improve the OS and IR status of PCOS patients. In another study, Khorshidi et al. (84) found that quercetin in the treatment of PCOS could significantly reduce the gene expression of serum resistin and peripheral blood mononuclear cells and significantly reduce the levels of serum total testosterone and LH. However, compared with the control group, there was no significant difference in each index of IR in the experimental group. Although the therapeutic effect of antioxidants is not the same, the above test shows that antioxidants are beneficial to the treatment of PCOS and can effectively improve the oxidative stress state of PCOS patients.
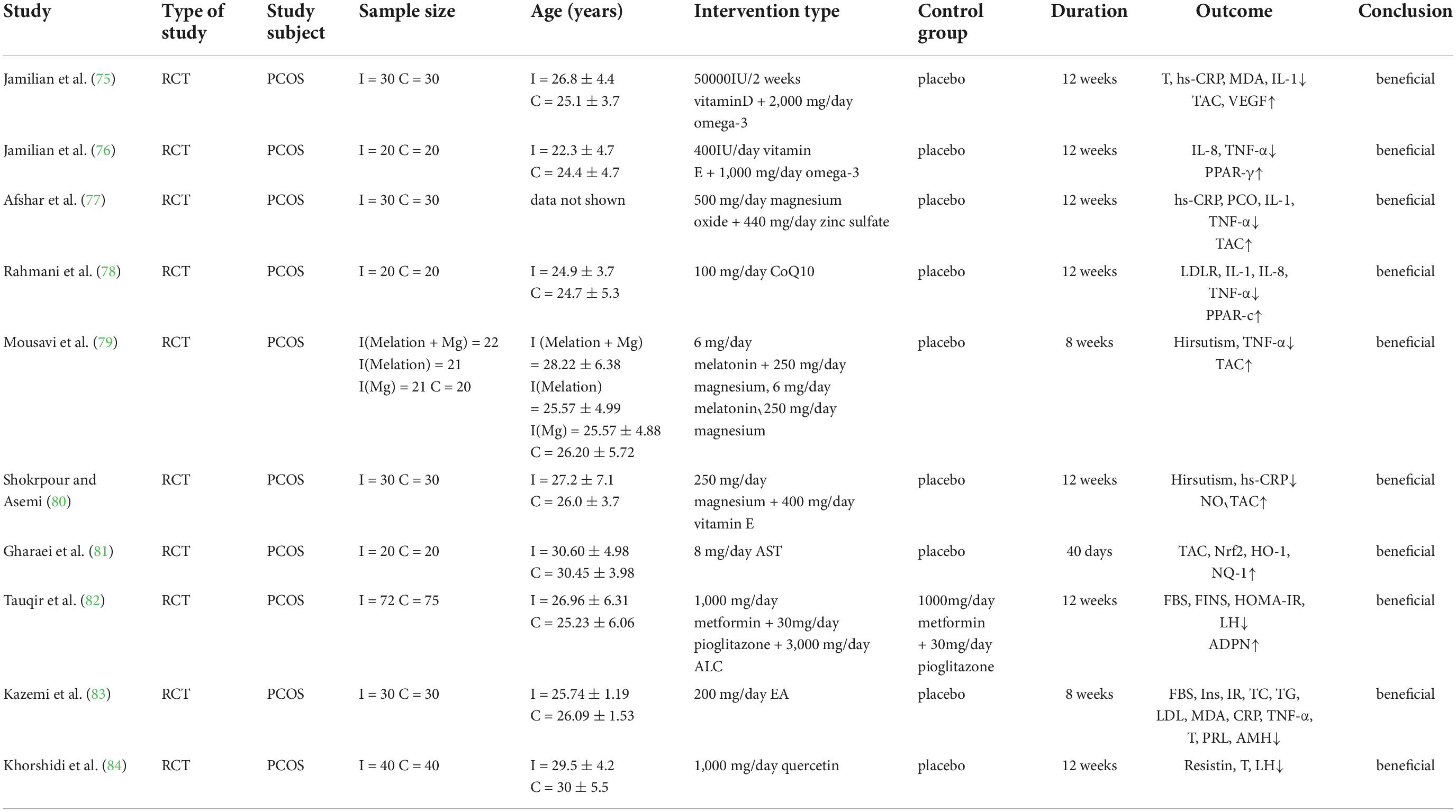
Table 1. Clinical study of antioxidant therapy for female polycystic ovary syndrome (PCOS).
Conclusion
In summary, OS, HA, IR, and ovulation disorders are closely related in PCOS patients. These factors interact to cause and aggravate ovulation disorders in PCOS through the amplifying effects of overweight/obesity. Dietary-induced OS promotes the production and secretion of a variety of inflammatory factors. At the same time, OS can promote the proliferation of theca-interstitial cells, upregulate CYP17, reduce serum SHBG levels, increase androgen secretion, improve the biological activity of serum free testosterone, and cause HA. HA can improve the sensitivity of MNCs to glucose, increase ROS and cause insulin signaling pathway defects, causing IR. IR leads to reduced tissue sensitivity to insulin and compensatory hyperinsulinemia and then stimulates the proliferation of theca-interstitial cells to increase the production and secretion of testosterone. At the same time, it reduces the serum SHBG level, improves the bioavailability of serum androgen, further aggravates HA, and forms a vicious cycle. Overweight/obesity exacerbates this vicious cycle by amplifying features such as HA, IR, and OS. OS imbalance affects the follicular fluid microenvironment, reduces the quality of follicles by damaging mitochondria, and even causes follicular apoptosis. HA and IR affect the growth and development of follicles, causing follicular growth stagnation, hindering the selection of dominant follicles and causing ovulation disorders. OS, HA, and IR interact to form a vicious cycle, leading to ovulation disorders in PCOS. However, the mechanism of OS in PCOS patients with ovulation disorders is not yet fully clear, and further studies are needed to confirm this hypothesis. The clinical application of antioxidant therapy may have a beneficial effect on the increase in OS levels in patients with PCOS, but there is still controversy about this treatment at this stage. More clinical trials are needed to confirm that it provides increasingly favorable evidence for the treatment of PCOS in the future.
Author contributions
WL and CL wrote the manuscript. QY, YZ, and ML sorted out ideas. HS revised the manuscript. All authors read and approved the final manuscript.
Funding
This research was funded by the Shihezi University University-level Project Fund, grant number: ZZZC202062A.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
PCOS, Polycystic ovary syndrome; OS, Oxidative stress; ROS, Reactive oxygen species; RNS, Reactive nitrogen species; SOD, Superoxide dismutase; GSH, Glutathione; MDA, Malondialdehyde; HA, Hyperandrogenemia; GnRH, Gonadotropin-releasing hormone; ACTH, adrenocorticotropic hormone; LH, Luteinizing hormone; SHBG, Sex hormone binding globulin; IGF-I, Insulin-like growth factor-I; IR, Insulin resistance; IRS, Insulin receptor substrate; TNF- α, Tumor necrosis factor- α; IL-1, Interleukins 1; SOCS3, Suppressor of cytokine signaling 3; CYP17, Cytochrome P450-17 α -hydroxylase; HNF-4 α, Hepatocyte nuclear factor-4 α; MNCs, Mononuclear cells; FFA, Free fatty acid; hs-CRP, High-sensitivity C-reactive protein; TAC, Total antioxidant capacity; PPAR- γ, Peroxisome proliferator-activated receptor- γ; Nrf2, Nuclear factor E2-related factor 2; HO-1, Heme oxygenase-1; ALC, Acetyl levocarnitine; T, Testosterone; VEGF, Vascular endothelial growth factor; PCO, Polycystic ovary; LDLR, Low density lipoprotein receptor; FBS, Fasting blood sugar; FINS, Fasting insulin; HOMA-IR, Homeostatic model assessment for insulin resistance; ADPN, Adiponectin; Ins, insulin; TC, Total cholesterol; TG, Triglyceride; PRL, Prolactin; AMH, Anti-Müllerian hormone.
References
1. Wekker V, van Dammen L, Koning A, Heida KY, Painter RC, Limpens J, et al. Long-term cardiometabolic disease risk in women with PCOS: a systematic review and meta-analysis. Hum Reprod Update. (2020) 26:942–60. doi: 10.1093/humupd/dmaa029
2. Escobar-Morreale HF. Polycystic ovary syndrome: definition, aetiology, diagnosis and treatment. Nat Rev Endocrinol. (2018) 14:270–84. doi: 10.1038/nrendo.2018.24
3. Yin W, Falconer H, Yin L, Xu L, Ye W. Association between polycystic ovary syndrome and cancer risk. JAMA Oncol. (2019) 5:106–7. doi: 10.1001/jamaoncol.2018.5188
4. Gunning MN, Sir Petermann T, Crisosto N, van Rijn BB, de Wilde MA, Christ JP, et al. Cardiometabolic health in offspring of women with PCOS compared to healthy controls: a systematic review and individual participant data meta-analysis. Hum Reprod Update. (2020) 26:103–17. doi: 10.1093/humupd/dmz036
5. Glintborg D, Rubin KH, Nybo M, Abrahamsen B, Andersen M. Cardiovascular disease in a nationwide population of Danish women with polycystic ovary syndrome. Cardiovasc Diabetol. (2018) 17:37. doi: 10.1186/s12933-018-0680-5
6. Risal S, Pei Y, Lu H, Manti M, Fornes R, Pui HP, et al. Prenatal androgen exposure and transgenerational susceptibility to polycystic ovary syndrome. Nat Med. (2019) 25:1894–904. doi: 10.1038/s41591-019-0666-1
7. Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil Steril. (2004) 81:19–25. doi: 10.1016/j.fertnstert.2003.10.004
8. Stener-Victorin E, Deng Q. Epigenetic inheritance of polycystic ovary syndrome – Challenges and opportunities for treatment. Nat Rev Endocrinol. (2021) 17:521–33. doi: 10.1038/s41574-021-00517-x
9. Lu J, Wang Z, Cao J, Chen Y, Dong Y. A novel and compact review on the role of oxidative stress in female reproduction. Reprod Biol Endocrinol. (2018) 16:80. doi: 10.1186/s12958-018-0391-5
10. Allen RG, Tresini M. Oxidative stress and gene regulation. Free Radic Biol Med. (2000) 28:463–99. doi: 10.1016/S0891-5849(99)00242-7
11. Di Meo S, Reed TT, Venditti P, Victor VM. Role of ROS and RNS sources in physiological and pathological conditions. Oxid Med Cell Longev. (2016) 2016:1245049. doi: 10.1155/2016/1245049
12. Valko M, Rhodes CJ, Moncol J, Izakovic M, Mazur M. Free radicals, metals and antioxidants in oxidative stress-induced cancer. Chem Biol Interact. (2006) 160:1–40. doi: 10.1016/j.cbi.2005.12.009
13. Sies H, Jones DP. Reactive oxygen species (ROS) as pleiotropic physiological signalling agents. Nat Rev Mol Cell Biol. (2020) 21:363–83. doi: 10.1038/s41580-020-0230-3
14. Agarwal A, Aponte-Mellado A, Premkumar BJ, Shaman A, Gupta S. The effects of oxidative stress on female reproduction: a review. Reprod Biol Endocrinol. (2012) 10:49. doi: 10.1186/1477-7827-10-49
15. Forman HJ, Zhang H. Targeting oxidative stress in disease: promise and limitations of antioxidant therapy. Nat Rev Drug Discov. (2021) 20:689–709. doi: 10.1038/s41573-021-00233-1
16. Szliszka E, Czuba ZP, Domino M, Mazur B, Zydowicz G, Krol W. Ethanolic extract of propolis (EEP) enhances the apoptosis- inducing potential of TRAIL in cancer cells. Molecules. (2009) 14:738–54. doi: 10.3390/molecules14020738
17. Ushio-Fukai M, Ash D, Nagarkoti S, Belin de Chantemèle EJ, Fulton DJR, Fukai T. Interplay between reactive oxygen/reactive nitrogen species and metabolism in vascular biology and disease. Antioxid Redox Signal. (2021) 34:1319–54. doi: 10.1089/ars.2020.8161
18. Singh A, Kukreti R, Saso L, Kukreti S. Oxidative stress: a key modulator in neurodegenerative diseases. Molecules. (2019) 24:1583. doi: 10.3390/molecules24081583
19. Forrester SJ, Kikuchi DS, Hernandes MS, Xu Q, Griendling KK. Reactive oxygen species in metabolic and inflammatory signaling. Circ Res. (2018) 122:877–902. doi: 10.1161/CIRCRESAHA.117.311401
20. Moloney JN, Cotter TG. ROS signalling in the biology of cancer. Semin Cell Dev Biol. (2018) 80:50–64. doi: 10.1016/j.semcdb.2017.05.023
21. Papalou O, Victor VM, Diamanti-Kandarakis E. Oxidative stress in polycystic ovary syndrome. Curr Pharm Des. (2016) 22:2709–22. doi: 10.2174/1381612822666160216151852
22. Uyanikoglu H, Sabuncu T, Dursun H, Sezen H, Aksoy N. Circulating levels of apoptotic markers and oxidative stress parameters in women with polycystic ovary syndrome: a case-controlled descriptive study. Biomarkers. (2017) 22:643–7. doi: 10.1080/1354750X.2016.1265004
23. Murri M, Luque-Ramírez M, Insenser M, Ojeda-Ojeda M, Escobar-Morreale HF. Circulating markers of oxidative stress and polycystic ovary syndrome (PCOS): a systematic review and meta-analysis. Hum Reprod Update. (2013) 19:268–88. doi: 10.1093/humupd/dms059
24. Huang A, Brennan K, Azziz R. Prevalence of hyperandrogenemia in the polycystic ovary syndrome diagnosed by the National Institutes of Health 1990 criteria. Fertil Steril. (2010) 93:1938–41. doi: 10.1016/j.fertnstert.2008.12.138
25. Rosenfield RL. Normal and premature adrenarche. Endocr Rev. (2021) 42:783–814. doi: 10.1210/endrev/bnab009
26. Pagán YL, Srouji SS, Jimenez Y, Emerson A, Gill S, Hall JE. Inverse relationship between luteinizing hormone and body mass index in polycystic ovarian syndrome: investigation of hypothalamic and pituitary contributions. J Clin Endocrinol Metab. (2006) 91:1309–16. doi: 10.1210/jc.2005-2099
27. Barnes RB, Rosenfield RL, Burstein S, Ehrmann DA. Pituitary-ovarian responses to nafarelin testing in the polycystic ovary syndrome. N Engl J Med. (1989) 320:559–65. doi: 10.1056/NEJM198903023200904
28. McCartney CR, Prendergast KA, Blank SK, Helm KD, Chhabra S, Marshall JC. Maturation of luteinizing hormone (gonadotropin-releasing hormone) secretion across puberty: evidence for altered regulation in obese peripubertal girls. J Clin Endocrinol Metab. (2009) 94:56–66. doi: 10.1210/jc.2008-1252
29. Pielecka J, Quaynor SD, Moenter SM. Androgens increase gonadotropin-releasing hormone neuron firing activity in females and interfere with progesterone negative feedback. Endocrinology. (2006) 147:1474–9. doi: 10.1210/en.2005-1029
30. Amato MC, Vesco R, Vigneri E, Ciresi A, Giordano C. Hyperinsulinism and polycystic ovary syndrome (PCOS): role of insulin clearance. J Endocrinol Invest. (2015) 38:1319–26. doi: 10.1007/s40618-015-0372-x
31. Cara JF, Rosenfield RL. Insulin-like growth factor I and insulin potentiate luteinizing hormone-induced androgen synthesis by rat ovarian thecal-interstitial cells. Endocrinology. (1988) 123:733–9. doi: 10.1210/endo-123-2-733
32. Deswal R, Yadav A, Dang AS. Sex hormone binding globulin – An important biomarker for predicting PCOS risk: a systematic review and meta-analysis. Syst Biol Reprod Med. (2018) 64:12–24. doi: 10.1080/19396368.2017.1410591
33. Bergh C, Carlsson B, Olsson JH, Selleskog U, Hillensjö T. Regulation of androgen production in cultured human thecal cells by insulin-like growth factor I and insulin**supported by grant no. 5987 from the Swedish Medical Research Council, Swedish Medical Society, The Medical Society of Göteborg, Kabi-Pharmacia Ltd., Nordisk Insulin Foundation, Hjalmar Svenssons Research Foundation, Swedish Society for Medical Research, and the University of Göteborg, Göteborg, Sweden. Fertil Steril. (1993) 59:323–31. doi: 10.1016/S0015-0282(16)55675-1
34. Chen W, Pang Y. Metabolic syndrome and PCOS: pathogenesis and the role of metabolites. Metabolites. (2021) 11:869. doi: 10.3390/metabo11120869
35. Olivares-Reyes JA, Arellano-Plancarte A, Castillo-Hernandez JR. Angiotensin II and the development of insulin resistance: implications for diabetes. Mol Cell Endocrinol. (2009) 302:128–39. doi: 10.1016/j.mce.2008.12.011
36. Xu M, Wang YM, Li WQ, Huang CL, Li J, Xie WH, et al. Ccrl2 deficiency deteriorates obesity and insulin resistance through increasing adipose tissue macrophages infiltration. Genes Dis. (2022) 9:429–42. doi: 10.1016/j.gendis.2020.08.009
37. Hirosumi J, Tuncman G, Chang L, Görgün CZ, Uysal KT, Maeda K, et al. A central role for JNK in obesity and insulin resistance. Nature. (2002) 420:333–6. doi: 10.1038/nature01137
38. Uysal KT, Wiesbrock SM, Marino MW, Hotamisligil GS. Protection from obesity-induced insulin resistance in mice lacking TNF-alpha function. Nature. (1997) 389:610–4. doi: 10.1038/39335
39. Chuang CC, Bumrungpert A, Kennedy A, Overman A, West T, Dawson B, et al. Grape powder extract attenuates tumor necrosis factor alpha-mediated inflammation and insulin resistance in primary cultures of human adipocytes. J Nutr Biochem. (2011) 22:89–94. doi: 10.1016/j.jnutbio.2009.12.002
40. González F, Considine RV, Abdelhadi OA, Acton AJ. Saturated fat ingestion promotes lipopolysaccharide-mediated inflammation and insulin resistance in polycystic ovary syndrome. J Clin Endocrinol Metab. (2019) 104:934–46. doi: 10.1210/jc.2018-01143
41. Xu T, Xu L, Meng P, Ma X, Yang X, Zhou Y, et al. Angptl7 promotes insulin resistance and type 2 diabetes mellitus by multiple mechanisms including SOCS3-mediated IRS1 degradation. FASEB J. (2020) 34:13548–60. doi: 10.1096/fj.202000246RR
42. Zhang R, Liu H, Bai H, Zhang Y, Liu Q, Guan L, et al. Oxidative stress status in Chinese women with different clinical phenotypes of polycystic ovary syndrome. Clin Endocrinol. (2017) 86:88–96. doi: 10.1111/cen.13171
43. González F, Rote NS, Minium J, Kirwan JP. Increased activation of nuclear factor kappaB triggers inflammation and insulin resistance in polycystic ovary syndrome. J Clin Endocrinol Metab. (2006) 91:1508–12. doi: 10.1210/jc.2005-2327
44. González F, Rote NS, Minium J, Kirwan JP. In vitro evidence that hyperglycemia stimulates tumor necrosis factor-alpha release in obese women with polycystic ovary syndrome. J Endocrinol. (2006) 188:521–9. doi: 10.1677/joe.1.06579
45. Spaczynski RZ, Arici A, Duleba AJ. Tumor necrosis factor-alpha stimulates proliferation of rat ovarian theca-interstitial cells. Biol Reprod. (1999) 61:993–8. doi: 10.1095/biolreprod61.4.993
46. Ortega I, Villanueva JA, Wong DH, Cress AB, Sokalska A, Stanley SD, et al. Resveratrol potentiates effects of simvastatin on inhibition of rat ovarian theca-interstitial cells steroidogenesis. J Ovarian Res. (2014) 7:21. doi: 10.1186/1757-2215-7-21
47. Sun Y, Li S, Liu H, Bai H, Hu K, Zhang R, et al. Oxidative stress promotes hyperandrogenism by reducing sex hormone-binding globulin in polycystic ovary syndrome. Fertil Steril. (2021) 116:1641–50. doi: 10.1016/j.fertnstert.2021.07.1203
48. González F, Nair KS, Daniels JK, Basal E, Schimke JM. Hyperandrogenism sensitizes mononuclear cells to promote glucose-induced inflammation in lean reproductive-age women. Am J Physiol Endocrinol Metab. (2012) 302:E297–306. doi: 10.1152/ajpendo.00416.2011
49. Wang J, Wu D, Guo H, Li M. Hyperandrogenemia and insulin resistance: the chief culprit of polycystic ovary syndrome. Life Sci. (2019) 236:116940. doi: 10.1016/j.lfs.2019.116940
50. Mizgier M, Jarząbek-Bielecka G, Wendland N, Jodłowska-Siewert E, Nowicki M, Brożek A, et al. Relation between inflammation, oxidative stress, and macronutrient intakes in normal and excessive body weight adolescent girls with clinical features of polycystic ovary syndrome. Nutrients. (2021) 13:896. doi: 10.3390/nu13030896
51. Yang R, Yang S, Li R, Liu P, Qiao J, Zhang Y. Effects of hyperandrogenism on metabolic abnormalities in patients with polycystic ovary syndrome: a meta-analysis. Reprod Biol Endocrinol. (2016) 14:67. doi: 10.1186/s12958-016-0203-8
52. Weisberg SP, McCann D, Desai M, Rosenbaum M, Leibel RL, Ferrante AW Jr. Obesity is associated with macrophage accumulation in adipose tissue. J Clin Invest. (2003) 112:1796–808. doi: 10.1172/JCI200319246
53. Puschel GP, Klauder J, Henkel J. Macrophages, low-grade inflammation, insulin resistance and hyperinsulinemia: a mutual ambiguous relationship in the development of metabolic diseases. J Clin Med. (2022) 11:4358. doi: 10.3390/jcm11154358
54. Polak K, Czyzyk A, Simoncini T, Meczekalski B. New markers of insulin resistance in polycystic ovary syndrome. J Endocrinol Invest. (2017) 40:1–8. doi: 10.1007/s40618-016-0523-8
55. Escobar-Morreale HF, San Millan JL. Abdominal adiposity and the polycystic ovary syndrome. Trends Endocrinol Metab. (2007) 18:266–72. doi: 10.1016/j.tem.2007.07.003
56. Mehrabani HH, Salehpour S, Amiri Z, Farahani SJ, Meyer BJ, Tahbaz F. Beneficial effects of a high-protein, low-glycemic-load hypocaloric diet in overweight and obese women with polycystic ovary syndrome: a randomized controlled intervention study. J Am Coll Nutr. (2012) 31:117–25. doi: 10.1080/07315724.2012.10720017
57. Scarfo G, Daniele S, Fusi J, Gesi M, Martini C, Franzoni F, et al. Metabolic and molecular mechanisms of diet and physical exercise in the management of polycystic ovarian syndrome. Biomedicines. (2022) 10:1305. doi: 10.3390/biomedicines10061305
58. Murri M, García-Fuentes E, García-Almeida JM, Garrido-Sánchez L, Mayas MD, Bernal R, et al. Changes in oxidative stress and insulin resistance in morbidly obese patients after bariatric surgery. Obes Surg. (2010) 20:363–8. doi: 10.1007/s11695-009-0021-6
59. Agarwal A, Gupta S, Sharma RK. Role of oxidative stress in female reproduction. Reprod Biol Endocrinol. (2005) 3:28. doi: 10.1186/1477-7827-3-28
60. Freitas C, Neto AC, Matos L, Silva E, Ribeiro Â, Silva-Carvalho JL, et al. Follicular fluid redox involvement for ovarian follicle growth. J Ovarian Res. (2017) 10:44. doi: 10.1186/s13048-017-0342-3
61. Jozwik M, Wolczynski S, Jozwik M, Szamatowicz M. Oxidative stress markers in preovulatory follicular fluid in humans. Mol Hum Reprod. (1999) 5:409–13. doi: 10.1093/molehr/5.5.409
62. Kim JA, Wei Y, Sowers JR. Role of mitochondrial dysfunction in insulin resistance. Circ Res. (2008) 102:401–14. doi: 10.1161/CIRCRESAHA.107.165472
63. Perez GI, Acton BM, Jurisicova A, Perkins GA, White A, Brown J, et al. Genetic variance modifies apoptosis susceptibility in mature oocytes via alterations in DNA repair capacity and mitochondrial ultrastructure. Cell Death Differ. (2007) 14:524–33. doi: 10.1038/sj.cdd.4402050
64. Franks S, Stark J, Hardy K. Follicle dynamics and anovulation in polycystic ovary syndrome. Hum Reprod Update. (2008) 14:367–78. doi: 10.1093/humupd/dmn015
65. Chen Z, Zhang D, Sun Z, Yu Q. A proper increasing in the testosterone level may be associated with better pregnancy outcomes for patients with tubal or male infertility during in vitro fertilization/intracytoplasmic sperm injection. Front Physiol. (2021) 12:696854. doi: 10.3389/fphys.2021.696854
66. Vendola KA, Zhou J, Adesanya OO, Weil SJ, Bondy CA. Androgens stimulate early stages of follicular growth in the primate ovary. J Clin Invest. (1998) 101:2622–9. doi: 10.1172/JCI2081
67. Rosenfield RL, Ehrmann DA. The pathogenesis of polycystic ovary syndrome (PCOS): the hypothesis of PCOS as functional ovarian hyperandrogenism revisited. Endocr Rev. (2016) 37:467–520. doi: 10.1210/er.2015-1104
68. Willis DS, Watson H, Mason HD, Galea R, Brincat M, Franks S. Premature response to luteinizing hormone of granulosa cells from anovulatory women with polycystic ovary syndrome: relevance to mechanism of anovulation. J Clin Endocrinol Metab. (1998) 83:3984–91. doi: 10.1210/jcem.83.11.5232
69. Szeliga A, Rudnicka E, Maciejewska-Jeske M, Kucharski M, Kostrzak A, Hajbos M, et al. Neuroendocrine determinants of polycystic ovary syndrome. Int J Environ Res Public Health. (2022) 19:3089.
70. Teede HJ, Misso ML, Costello MF, Dokras A, Laven J, Moran L, et al. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Clin Endocrinol. (2018) 89:251–68.
71. Anjali G, Kaur S, Lakra R, Taneja J, Kalsey GS, Nagendra A, et al. FSH stimulates IRS-2 expression in human granulosa cells through cAMP/SP1, an inoperative FSH action in PCOS patients. Cell Signal. (2015) 27:2452–66. doi: 10.1016/j.cellsig.2015.09.011
72. Chahal N, Geethadevi A, Kaur S, Lakra R, Nagendra A, Shrivastav TG, et al. Direct impact of gonadotropins on glucose uptake and storage in preovulatory granulosa cells: implications in the pathogenesis of polycystic ovary syndrome. Metabolism. (2021) 115:154458. doi: 10.1016/j.metabol.2020.154458
73. Wang D, Weng Y, Zhang Y, Wang R, Wang T, Zhou J, et al. Exposure to hyperandrogen drives ovarian dysfunction and fibrosis by activating the NLRP3 inflammasome in mice. Sci Total Environ. (2020) 745:141049. doi: 10.1016/j.scitotenv.2020.141049
74. Gharaei R, Mahdavinezhad F, Samadian E, Asadi J, Ashrafnezhad Z, Kashani L, et al. Antioxidant supplementations ameliorate PCOS complications: a review of RCTs and insights into the underlying mechanisms. J Assist Reprod Genet. (2021) 38:2817–31. doi: 10.1007/s10815-021-02342-7
75. Jamilian M, Samimi M, Mirhosseini N, Afshar Ebrahimi F, Aghadavod E, Talaee R, et al. The influences of vitamin D and omega-3 co-supplementation on clinical, metabolic and genetic parameters in women with polycystic ovary syndrome. J Affect Disord. (2018) 238:32–8. doi: 10.1016/j.jad.2018.05.027
76. Jamilian M, Shojaei A, Samimi M, Afshar Ebrahimi F, Aghadavod E, Karamali M, et al. The effects of omega-3 and vitamin E co-supplementation on parameters of mental health and gene expression related to insulin and inflammation in subjects with polycystic ovary syndrome. J Affect Disord. (2018) 229:41–7. doi: 10.1016/j.jad.2017.12.049
77. Afshar Ebrahimi F, Foroozanfard F, Aghadavod E, Bahmani F, Asemi Z. The effects of magnesium and zinc co-supplementation on biomarkers of inflammation and oxidative stress, and gene expression related to inflammation in polycystic ovary syndrome: a randomized controlled clinical trial. Biol Trace Elem Res. (2018) 184:300–7. doi: 10.1007/s12011-017-1198-5
78. Rahmani E, Jamilian M, Samimi M, Zarezade Mehrizi M, Aghadavod E, Akbari E, et al. The effects of coenzyme Q10 supplementation on gene expression related to insulin, lipid and inflammation in patients with polycystic ovary syndrome. Gynecol Endocrinol. (2018) 34:217–22. doi: 10.1080/09513590.2017.1381680
79. Mousavi R, Alizadeh M, Asghari Jafarabadi M, Heidari L, Nikbakht R, Babaahmadi Rezaei H, et al. Effects of melatonin and/or magnesium supplementation on biomarkers of inflammation and oxidative stress in women with polycystic ovary syndrome: a randomized, double-blind, placebo-controlled trial. Biol Trace Elem Res. (2022) 200:1010–9.
80. Shokrpour M, Asemi Z. The effects of magnesium and vitamin E co-supplementation on hormonal status and biomarkers of inflammation and oxidative stress in women with polycystic ovary syndrome. Biol Trace Elem Res. (2019) 191:54–60. doi: 10.1007/s12011-018-1602-9
81. Gharaei R, Alyasin A, Mahdavinezhad F, Samadian E, Ashrafnezhad Z, Amidi F. Randomized controlled trial of astaxanthin impacts on antioxidant status and assisted reproductive technology outcomes in women with polycystic ovarian syndrome. J Assist Reprod Genet. (2022) 39:995–1008. doi: 10.1007/s10815-022-02432-0
82. Tauqir S, Israr M, Rauf B, Malik MO, Habib SH, Shah FA, et al. Acetyl-L-carnitine ameliorates metabolic and endocrine alterations in women with PCOS: a double-blind randomized clinical trial. Adv Ther. (2021) 38:3842–56. doi: 10.1007/s12325-021-01789-5
83. Kazemi M, Lalooha F, Nooshabadi MR, Dashti F, Kavianpour M, Haghighian HK. Randomized double blind clinical trial evaluating the ellagic acid effects on insulin resistance, oxidative stress and sex hormones levels in women with polycystic ovarian syndrome. J Ovarian Res. (2021) 14:100. doi: 10.1186/s13048-021-00849-2
84. Khorshidi M, Moini A, Alipoor E, Rezvan N, Gorgani-Firuzjaee S, Yaseri M, et al. The effects of quercetin supplementation on metabolic and hormonal parameters as well as plasma concentration and gene expression of resistin in overweight or obese women with polycystic ovary syndrome. Phytother Res. (2018) 32:2282–9.
Keywords: polycystic ovary syndrome, oxidative stress, hyperandrogenism, insulin resistance, ovulation disorder, antioxidants, overweight/obesity
Citation: Li W, Liu C, Yang Q, Zhou Y, Liu M and Shan H (2022) Oxidative stress and antioxidant imbalance in ovulation disorder in patients with polycystic ovary syndrome. Front. Nutr. 9:1018674. doi: 10.3389/fnut.2022.1018674
Received: 13 August 2022; Accepted: 07 October 2022;
Published: 28 October 2022.
Edited by:
Shuai Chen, Wuhan University, ChinaReviewed by:
Meysam Zarezadeh, Tabriz University of Medical Sciences, IranCopyright © 2022 Li, Liu, Yang, Zhou, Liu and Shan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hongying Shan, aG9uZ3lpbmdzaGFuQGJqbXUuZWR1LmNu
†These authors have contributed equally to this work and share first authorship