 Shazia Rehman1†
Shazia Rehman1† Zhang Jianglin2,3*†
Zhang Jianglin2,3*†- 1Department of Biomedical Sciences, Pak-Austria Fachhochschule, Institute of Applied Sciences and Technology, Haripur, Pakistan
- 2Department of Dermatology, Shenzhen People's Hospital, The Second Clinical Medical College, Jinan University, The First Affiliated Hospital, Southern University of Science and Technology, Shenzhen, China
- 3Candidate Branch of National Clinical Research Center for Skin Diseases, Shenzhen, China
Inadequate diet and nutritional quality are potentially correlated with an escalated risk of cardiac-related morbidity and mortality. A plethora of knowledge is available regarding the influence of heart-healthy dietary patterns in response to disability-adjusted life years (DALYs), yet little is known regarding the best approaches to adopt. In response, the present investigation aims to bridge this knowledge gap by implementing mathematical machine learning grey methodology to assess the degree of influence and the potential contributing factors in DALYs due to ischemic heart disease and stroke, in conjunction with the Hurwicz (Min-Max) criterion. The outcomes highlighted that a diet low in fruits is a potential contributor to IHD-related DALYS, whereas a diet low in vegetables is a more grounded contributor to stroke-related DALYs in Spain, among others. Moreover, the Hurwicz approach highlighted IHD to be more impacted due to dietary and nutritional factors than stroke. In conclusion, our investigation strongly supports a balanced diet and precision nutrition guidelines as a strategy for reducing cardiac-related diseases in the Spanish population. It is a public health primary consideration to build an ambiance that encourages, rather than hinders, compliance with cardioprotective dietary practices among all people.
Introduction
Cardiovascular disease (CVD) continues to be the major cause of mortality and disability in industrialized nations, although its worldwide burden has progressively declined over recent years (1). In actuality, one in three fatalities in the United States (US) and one in every four in Europe are caused by CVD (2, 3). Among the non-communicable diseases, CVDs are the leading driver of deaths in Spain and account for ~33% of the total mortality. In this demographic, ischemic heart disease is the primary cause in men whereas cerebrovascular disease (stroke) is the main cause of death in women (4–7). In addition, cardiac incidence has sharply increased in developing economies over the past 25 years, becoming the second leading cause of years lost from premature death in the majority of these nations (8, 9), partly as a result of their adoption of Western dietary habits. Despite advancements in treatment, the substantial global burden of CVDs highlights the need for efficient preventative and therapeutic measures to slow the progression of this prevalent chronic disease. The dietary risk appears to be a key focus for cardiac prevention and therapy since it accounts for ~one-third of worldwide mortality (10).
Considerable evidence claims to support the cardiac advantages of healthy eating practices. Nutrition and dietary behaviors are critical to maintaining cardiac health. They are also essential in the prevention and management of CVDs and chronic illnesses. Globally, dietary variables were responsible for about 11 million fatalities and ~255 million disability-adjusted life years (DALYs) during the year 2017 (11). Dietary behaviors include the balance, diversity, and mixture of foods and drinks ingested regularly. This covers all foods and fluids, whether they are cooked or eaten at home or elsewhere. Adherence to heart-healthy eating behaviors is strongly linked to potential cardioprotective effects (12). Since CVD develops throughout neonatal development and premature infancy, it is imperative to develop cardioprotective eating behaviors early in our lifespan, particularly preconception, as well as to sustain them throughout one's life (13). Food-based dietary behavior assistance is intended to promote nutrient sufficiency, heart health, and overall well-being while taking into account personal preferences, cultural and religious customs, and life phases. Cardioprotective dietary habits, or those linked to lower risk of cardiac disorders, usually focus on fruit, and vegetable intake, whole-grain meals, lean protein resources, vegetable oils, and negligibly processed meals. Additionally, these behaviors include a minimal intake of salty and sugary beverages and meals.
Multiple studies integrate healthy eating practices to lower plasmatic levels of pro-inflammatory indicators (14), whereas a Western-style diet (a diet heavy in protein) is linked to greater levels of low-grade inflammatory activation (15). Therefore, a healthy diet is recommended by cardiovascular guidelines. A better blending of various meals and minerals is possible with dietary intervention. Due to the obvious synergistic health impacts among them, healthy eating habits ultimately promote a stronger amplitude of positive benefits than the prospective benefits of nutrient supplementation. As per the existing scientific literature, healthy eating habits are characterized by a high intake of fiber, vitamins, antioxidants, minerals, monounsaturated fatty acids/polyunsaturated fatty acids, low intakes of sodium chloride, refined sugar, saturated and trans fats, polyphenols, and high intakes of complex carbs with minimal glycemic loads (16). This equates to significant consumption of fresh produce, such as fruits, vegetables, lentils, fish, and shellfish, as well as nuts, seeds, whole grains, vegetable oils, primarily extra virgin olive oil, including dairy products, while consuming less sugary snacks, red and processed meat, and carbonated drinks. For Cardiac outcomes, the Mediterranean and DASH diets have received considerable attention. The descending of reduced inflammation and improved body weight management, which both enhance other potential parameters and are associated with fewer clinical occurrences, may both lessen the prevalence of CVD (16, 17).
The significance of dietary behaviors concerning public healthcare has spurred consumer interest in food and nutraceutical constituents, particularly fruits and vegetables. The American Heart Association (AHA) Nutrition Committee and the European Society of Cardiology (ESC) potentially recommend the regular intake of both fruits and vegetables in multiple servings to reduce cardiovascular risk (18, 19). These guidelines are mostly founded on epidemiological research and meta-analyses (19–22). A meta-analysis of 71 clinical and 12 epidemiological investigations revealed a significant inverse relationship between vegetable and fruit consumption (with CRP and TNF levels) and a direct relationship with an elevated accretion of T cells (22). Likewise, in another cohort investigation of 792 subjects (age 70 years), the interconnections between particular single meals (inclusive of fruits and vegetables) and indicators of systemic inflammation were found. According to the investigators, consuming more fresh fruits was potentially proven to reduce CRP levels. No substantial linkage was revealed against vegetables. Comparable findings were observed between fibrinogen levels and fruit intake independently or in conjunction with vegetables (23).
Multiple objectives are a typical challenge with systemic issues, which makes decisions more ambiguous. Discovering methodologies that incorporate the strongest criteria in the decision-making procedure that directly affect decisions is essential in this context to reduce inaccuracies (24–26). However, usually, this technique is challenging to implement since the decision-making criteria parameters fluctuate elevating the level of ambiguity in the final response. In the sphere of health, these protocols are far more challenging since they encompass not only technological issues as well as the human aspect, which generates conflicts of interest and impedes the ultimate decision. In consequence, multi-criteria decision analysis (MCDA) has been employed in its various forms to strengthen healthcare structures overall (27–29). The association between cardiac-related prevalence and related dietary and nutritional variables has been explored in these researches via a variety of methodologies. The greatest ways to improve the caliber of research work and its application are, however, scarcely understood.
In response to the above-stated research query, we integrated the grey machine learning approach with Hurwicz's approach to seek a comprehensive understanding of dietary and nutritional patterns on ischemic heart disease (IHD) and stroke prevalence in the Spanish population. Therefore, by targeting a broad variety of dietary and nutritional factors together with the prevalence of major cardiac-related disorders, we may be able to construct a more comprehensive and potential continuum of correlations. Ultimately, our work seeks to explore the missing gaps in the existing body of literature by measuring the nexus between vitamin A deficiency, a diet low in vegetables, a diet high in sodium, zinc deficiency, iron deficiency, and a diet low in fruits, with disability-adjusted life years (DALYs) of ischemic heart disease (IHD) and stroke. We implemented mathematical machine learning grey modeling of grey system theory to investigate potential interactions, these include Deng GRA, absolute GRA, and the second synthetic GRA. The purpose of the absolute GRA model is to provide integral closeness or proximity between two variables whereas Deng's GRA model just reveals partial closeness or proximity. The second synthetic GRA model, on the flip side, incorporates the characteristics of both Deng's GRA and absolute GRA models to offer a more comprehensive closeness also known as inclusive proximity. This closeness or proximity is also known as correlation in the current literature. The core idea behind GRA models is to evaluate the degree of relationships between the study variables based on how comparable their geometric curves are to one another. To put it simply, the fundamental goal of GRA models is to quantify the proximity or closeness of two data sequences that indicate two curves from a distinct perspective. These insights set one GRA model apart from another. Dependent on the notion of an association between the reference series and the comparability series of the data, GRA can ascertain the potential factors of the given inputs. These models have higher precision and could produce more reliable solutions though with limited data.
Also, Hurwicz's (Min-Max) criterion was applied to perform a comparative evaluation of all the chosen dietary and nutritional variables with IHD and stroke DALYs within the Spanish population to ascertain which dietary and nutritional variable is potentially contributing to DALYs of IHD and stroke.
Materials and methods
Data source
All of the data analyzed in the current analysis is derived from the Global Burden of Disease (GBD 2019) study. DALYs were chosen as the unit of measurement for IHD and stroke, and dietary and nutritional components (vitamin A deficiency, a diet low in vegetables, a diet high in sodium, zinc deficiency, iron deficiency, and a diet low in fruits) were also chosen as DALYs. The collected data were for both sexes (male and female) and were expressed as percentages of the total population. All data were normalized as the first step before proceeding with the analysis.
Grey analyses
Grey relational analyses (GRA)
GRA methods are one of the fundamental aspects of grey system theory, which was presented in 1982 by Chinese scholar Deng Julong to deal with ambiguous processes with partial information (30). The basic principle behind grey modeling is that the measure of closeness (or correlation) of the multilateral pattern of a given dataset representing the structural properties, could be adapted to foresee the closeness of a linkage among variables within the systems. A detailed description of the GRA method can be found in (31). The incorporation and effective application of grey approaches have been demonstrated in the literature in several scientific disciplines (32–36). The present investigation is carried out by engaging GRA methodologies. The GRA models are designed using SAS (2019), whereas Microsoft Excel software (2019) was used to solve the Hurwicz (Min-Max) criterion. The proposed analyses and modeling approaches are used in the paper to measure the level of influence and linkage between dietary and nutritional variables and IHD and stroke DALYs in a multifaceted way. The accompanying section summarizes the computing algorithms for grey relational models.
Deng's grey relational analysis (GRA) model
Let 𝕐i be the reference series of the given data set denoting a dependent parameter and 𝕐j be the comparative sequences of the given data set denoting an independent parameter, then, the grey relational gradient (GRG), (the output of the GRA model) is depicted as γij or γ(𝕐i, 𝕐j) and can be accompanied by Rehman and Rehman (37)and Xuerui et al. (38):
Where,
In this case, ζ ϵ (0, 1) denotes the distinguishing coefficient, and is generally assumed to be at 0.5.
Absolute grey relational analysis (GRA) model
If 𝕐i(dependent) and 𝕐j(independent) are two distinct data series connected within a system, so the algorithm for computing the absolute GRA model is shown below (31).
Where,
Second synthetic grey relational analysis (SSGRA) model
The SSGRA model can be produced by incorporating the given equation (39).
Where, ′′ indicates the SSGRA model, indicates the absolute GRA model whereas ′γ′ indicates the Deng GRA model outcomes across the two grey data series i.e., Yi and Yj. Whenever a decision-maker seeks an inclusive evaluation that combines the pros of both ′ϵ′ and ′γ′ without endorsing one over another and so sets ϑ at 0.5. We assumed ϑ at 0.5 for our analysis. The detailed literature on grey modeling can be obtained from (31, 40). A graphical roadmap for the grey framework employed in our research is displayed in Figure 1.
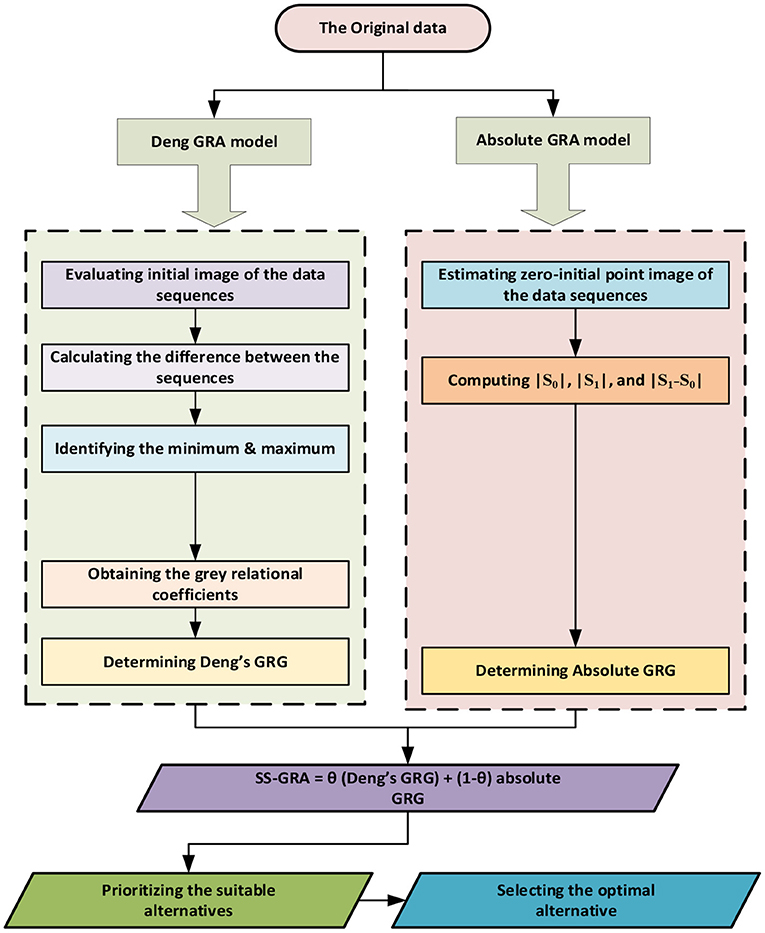
Figure 1. The methodological roadmap of grey modeling.
Results
The estimated outcomes for IHD based on the three grey relational models are shown in Table 1. A Diet low in vegetables (Deng GRA:0.9889, Absolut GRA: 0.9935, SS-GRA:0.9912) is shown to be highly associated with the number of DALYs attributable to IHD against Deng, absolute GRA, and SS-GRA models and ranked top as compared to the rest of the chosen variables. In addition, the variable diet low in fruits also appeared to be significantly associated with a very slight difference in strength. These data imply that a diet poor in vegetables and fruits has a significant impact on the occurrence of IHD. Furthermore, in all three grey relational models, the variables zinc (absolute GRA: 0.8014, Deng GRA:0.7806, SS-GRA:0.7910) and iron deficiency (Deng GRA:0.6931, absolute GRA:0.7083, SS-GRA:0.7007) had less effect on morbidity from IHD. A low-vegetable-and-fruit diet has been demonstrated to be a significant predictive risk factor for the higher incidence of IHD in the Spanish population. In Spain, the prevalence of IHD is considerably high and rising, but the control rate is lower than the needed threshold. These findings are consistent with previous epidemiological studies conducted in Spain, which discovered that a diet poor in vegetables is significantly associated with a frequent incidence of IHD (41–43). The graphical relationship between the cardiac DALYs and nutritional factors can be seen in Figures 2, 3.
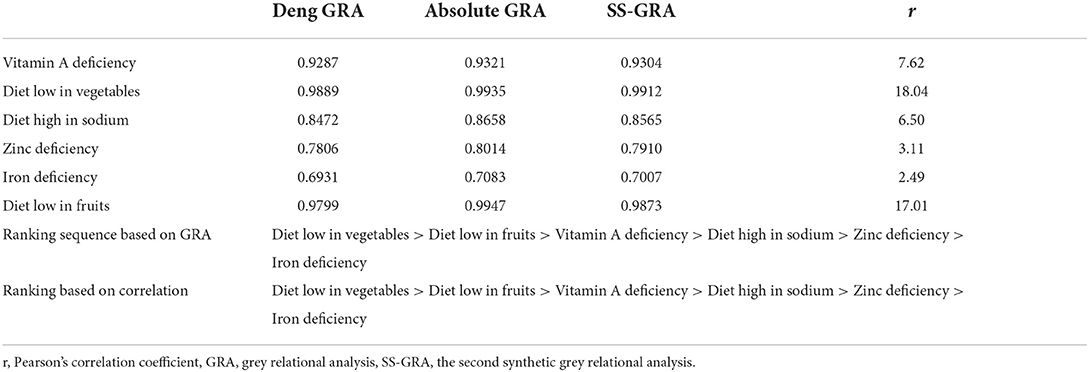
Table 1. Grey relational assessment for IHD morbidity with nutritional risk factors.
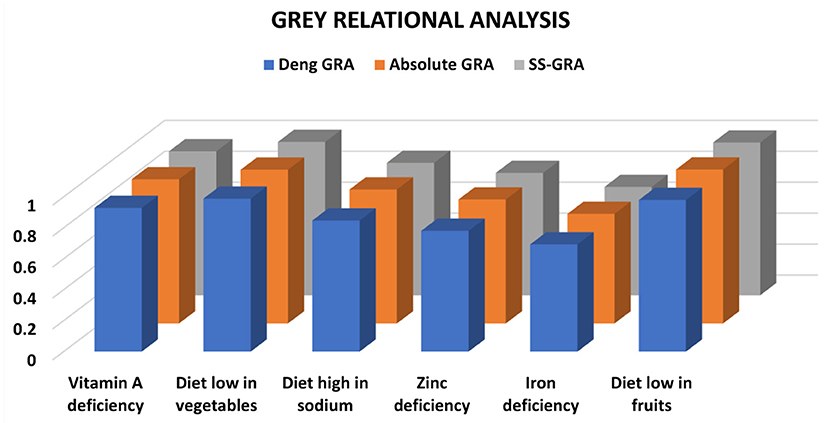
Figure 2. GRA assessment between IHD and nutritional variables.
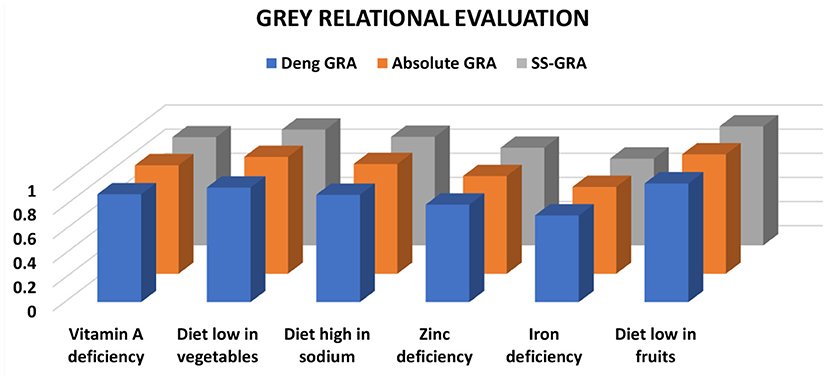
Figure 3. GRA assessment between stroke and nutritional variables.
The findings in the case of stroke demonstrated that all risk variables maintained their positions against all grey relational models (Table 2). The risk factor diet low in fruits (Deng GRA:0.9848, absolute GRA:0.9904, SS-GRA:0.9876) ranked top while a diet low in vegetables (Deng GRA:0.9509, absolute GRA:0.9701, SS-GRA:0.9605) ranked second. The degree of association for the risk factor diet low in fruits was stronger than the rest of the risk factors. Considering the effect of zinc (Deng GRA:0.8090, absolute GRA:0.8112, SS-GRA:0.8101) and iron deficiency (Deng GRA:0.7192, absolute GRA:0.7212, SS-GRA:0.7202) on prevalence from stroke, the estimates against all grey relational models are found to show a comparatively frail linkage when compared with the rest of the risk factors. However, as compared to vitamin A deficiency, a diet high in sodium, zinc, and iron deficiency, a diet low in nutrients (vegetables and fruits) depicted a potential impact on increased DALYs from stroke as it holds 1st place throughout the analyses. The substantial associations between a diet low in fruits with stroke morbidity illustrated that it may be regarded as the strongest predictive risk factor to foresee DALYs and ultimately fatality from a stroke in the Spanish population. An abundance of evidence has shown stroke is the second leading cause of death and a top leading cause of disability in the Spanish population, with a stroke incidence of 187 cases per 100,000 persons per year (44). Our study's three grey relationship conclusions are congruent with a plethora of other stroke-related dietary and nutritional risk variables in Spain, where the incidence of stroke is growing and primary and secondary prevention should likely be fundamental health policy goals soon (45–47).
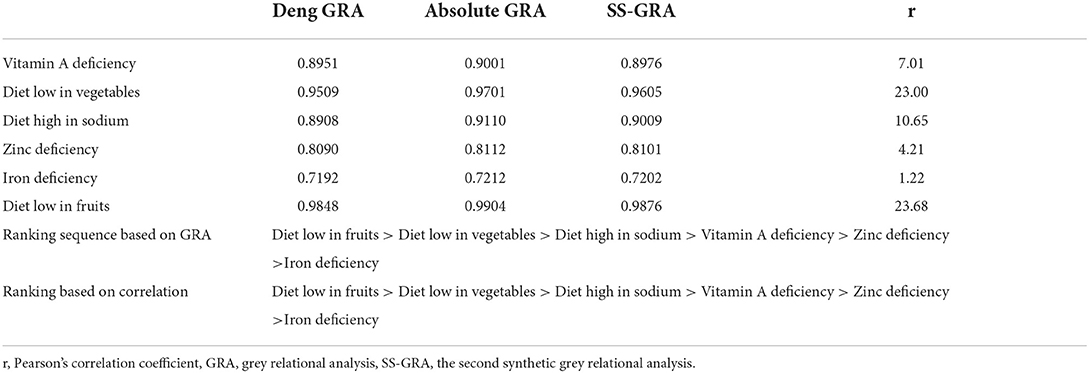
Table 2. Grey relational assessment for stroke morbidity with nutritional risk factors.
We also employed Pearson's correlation coefficient to correlate our results to the SS-GRA model. As shown, the sequences derived by the two methods are nearly identical. Their respective strengths, however, were the major point of distinction. Although the GRA model dimensions and Pearson's correlational coefficient are not identical, their judgments may be contrasted since both scales allow the decision-maker to assess if the association is moderate, significant, or extremely powerful.
The Hurwicz's (Min-Max) approach
The Hurwicz (Min-Max) metrics have been referred to as the realism criterion. This method is used to make judgments (decisions) in conditions of uncertainty. It is commonly used in decision-making when we are challenged with several alternatives and an uncertain natural context. This procedure followed the stages outlined by Sikdar (48). We need to reduce cardiac DALYs for the current study, hence the decision would be as follows:
The metric is classified as an optimism index, and its magnitude ranges from [0–1]. In this case, we'll use 0.8. The following are the outcomes of a minimization approach:
A1 (IHD): (0.8 × 0.9912) + (0.2 × 0.7007) = 0.9331
A2 (Stroke): (0.8 × 0.9876) + (0.2 × 0.7202) = 0.9341
The results indicated that the prevalence of IHD is more likely to be affected by the risk factors attributable to nutrition in the Spanish population as compared to stroke. As an aggregate, the projected outputs of both decision-making approaches demonstrated that low-vegetable-and-fruits are strongly related to an upsurge in overall cardiac prevalence, specially IHD.
Discussion
Health professionals and policymakers are tremendously concerned about the fact that CVDs are the leading cause of morbidity and death in Spain. Chronic illnesses, particularly CVD, are greatly influenced by poor nutrition. To reduce the prevalence and mortality from CVDs, much research has been done on the role of dietary variables in morbidity linked with cardiovascular disorders. However, our research takes a step further by assessing the degree of association and effect between the selected variables (nutritional risk factors) and morbidity spurred on CVDs, particularly IHD and stroke, in the Spanish population from 2010 to 2019. In the current investigation, we implemented three grey relational models (Deng GRA, absolute GRA, and SS-GRA models), which might potentially replace conventional data analysis techniques. The estimated statistics confirmed the suitability and effectiveness of the grey relational model technique.
The findings exhibited that, among the variables chosen, a diet poor in fruits tended to be highly grounded when compared with stroke morbidity in Spain, but a diet low in vegetables is the most likely contributor to the occurrence of IHD. Contrarily, in our analyses, zinc and iron insufficiency were the factors that had the least impact on morbidity from IHD and stroke. Additionally, we contrasted the outcomes of our advanced mathematical grey modeling analysis with those of a more conventional statistical technique, i.e., Pearson's correlation. The ranking order derived from the grey technique and that derived from the correlation was found to be identical, confirming the reliability of the grey analyses. Moreover, leveraging the statistics from the SS-GRA, a decision analysis technique (Hurwicz's criterion) was also applied to verify the robustness of the results. This approach confirmed a strong relationship between nutritional variables and the prevalence of IHD. Interestingly, we also examined a strong relationship between IHD and stroke morbidity caused by nutritional risk factors, which highlights nutritional factors as a potential contributor to improving heart health among the Spanish population.
Prior research has established a nexus between a diet poor in fruits and vegetables and the development of heart diseases, particularly IHD and stroke, in patients (49, 50). The best dietary practices for cardiac protection receive less attention than other dietary factors that may affect IHD and stroke risk. The findings of our study make it abundantly evident that a diet low in fruits and vegetables has a significant impact on the onset and progression of IHD and stroke, and they emphasize that one of the best dietary patterns for prevention is to increase the consumption of fruits and vegetables. It is challenging to specify an individual food component a pathophysiological function due to the great diversity of nutritional research. There may be intricate relationships between the various diet components, and any influences cannot be attributable to a single diet component but rather to a conjunction of dietary elements (51). Our results are aligned with the previous investigations which have been conducted to investigate the role of diet in cardiac health (52–56). An abundance of observational and experimental data suggests that practicing the Mediterranean diet (MD) is strongly correlated with a reduced risk of cardiac-related disorders (57). In particular, no other dietary pattern has accumulated as much data as the MD. Numerous observational analyses have explored the association between mortality and the incidence of MD and CVD (58–60). Several meta-analyses that compiled their risk assessments revealed an overarching inverse correlation (61–64).
In the going era, it has become more challenging to maintain heart-healthy dietary behaviors since the food environment has a considerable impact on people's food preferences, nutrition quality, and ergo cardiac health in several aspects. There are several systematic federal, state, and municipal activities and regulations that hinder the acquisition of these dietary behaviors against the backdrop of widespread nutrition ignorance. In this scientific claim, aspects such as specific food advertising, compositional racial prejudice, neighborhood discrimination, unpleasant built environmental conditions, and dietary and nutritional uncertainty all contribute to environments where unhealthy diets are predefined choices where we ingest, work, and reside. Furthermore, differences in product access, affordability, pricing, advertising, and placement in various locations sometimes make it convenient to consume harmful food as compared to healthier options. Improving food and nutrition quality, as well as chronic health issues across all communities will necessitate resolving these underlying structural issues, especially among persons of marginalized races and nationalities (2, 65). One significant adjuvant technique is to vigorously combat dietary myths among the general public and medical professionals, in conjunction with significant environmental improvements. Such endeavors may be aided by the inclusion of food and nutrition awareness in elementary and medical school curricula (66, 67).
The National Institutes of Health (NIH) (2020–2030 Strategic Plan for Nutrition Research) emphasizes precision nutrition to identify the influence on the health of not just what people consume, but also when, why, and how they consume throughout their lives (68). Precision nutrition is based on mounting data on those individual disparities in food consumption, habits, genetic history, microbial, and demographic and physical settings that impact disease susceptibility. The proactive goal of the NIH intends to deepen awareness of the synergies among these determinants to enable the establishment of significant clinical treatments to optimize food ingestion and the wellness of individuals. Precision nutrition integrates bioinformatics, genomics, and artificial intelligence with operational and cognitive disciplines (68–70). Multiplex precision nutrition techniques may significantly eradicate demographic, racial, and cultural differences in food consumption and CVD outcomes in the coming decades (71). Nonetheless, while precision nutrition can deliver tailored diets for cardiac prevention in the future, the discipline is still in its early stages. As a result, the present emphasis on public health nutrition endeavors to strengthen the food environment is substantial.
Since it facilitates clarity, resilience, and consistency in the presence of numerous and conflicting criteria, scientists have concluded that the MCDA paradigms are efficacious in the public health care contexts and are a viable decision-making technique [12, 45]. The findings of the present study suggest that when challenged with several options of comparable significance in healthcare decision-making scenarios, experts should leverage MCDA approaches and tools. The results of this study could assist researchers with mixed-method research guidance to aid in improving the excellence of their works and their comprehension of how to employ multi-method approaches to assess and prioritize the contributing variables of disease fatality in healthcare analytics. Such studies may aid in enhancing our ability to get key perspectives into the complex structure of the variables in a framework. Moreover, the recommended techniques also offer policy and decision-makers a useful tool and more in-depth practical information to aid in generating meaningful conclusions.
Conclusion
In conclusion, a balanced diet, particularly fruits and vegetables, has a direct influence on IHD and stroke disorders and lowers the risk of cardiac events. This investigation strongly supports a balanced diet and precision nutrition guidelines as a strategy for reducing cardiac-related diseases in the Spanish population. It is a public health primary consideration to build an ambiance that encourages, rather than hinders, compliance with cardioprotective dietary practices among all people.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found here: https://www.healthdata.org/gbd/2019.
Author contributions
Both authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Funding
This work was supported by the Union Program of Science and Health of Hunan Province, China (2019JJ80011).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Rehman S, Rehman E, Mumtaz A, Jianglin Z. Cardiovascular disease mortality and potential risk factor in china: a multi-dimensional assessment by a grey relational approach. Int J Public Health. (2022) 67. Available online at: https://www.ssph-journal.org/articles/10.3389/ijph.2022.1604599
2. Lichtenstein AH, Appel LJ, Vadiveloo M, Hu FB, Kris-Etherton PM, Rebholz CM, et al. 2021 dietary guidance to improve cardiovascular health: a scientific statement from the American heart association. Circulation. (2021) 144:e472–87. doi: 10.1161/CIR.0000000000001031
3. Perak AM, Ning H, Khan SS, Van Horn L V, Grobman WA, Lloyd-Jones DM. Cardiovascular health among pregnant women, aged 20 to 44 years, in the United States. J Am Heart Assoc. (2020) 9:e015123. doi: 10.1161/JAHA.119.015123
4. ISGlobal Barcelona Institute of Global H. Leading Causes of Deaths In Spain. 2018. Available online at: https://www.isglobal.org/en_GB/-/cardiopatia-isquemica-demencias-e-ictus-se-situan-como-las-principales-causas-de-muerte-en-espana
5. Jagannathan R, Patel SA, Ali MK, Narayan KM. Global updates on cardiovascular disease mortality trends and attribution of traditional risk factors. Curr Diab Rep. (2019) 19:1–12. doi: 10.1007/s11892-019-1161-2
6. Meier T, Gräfe K, Senn F, Sur P, Stangl GI, Dawczynski C, et al. Cardiovascular mortality attributable to dietary risk factors in 51 countries in the WHO European Region from 1990 to 2016: a systematic analysis of the Global Burden of Disease Study. Eur J Epidemiol. (2019) 34:37–55. doi: 10.1007/s10654-018-0473-x
7. Soriano JB, Rojas-Rueda D, Alonso J, Antó JM, Cardona P-J, Fernández E, et al. The burden of disease in Spain: results from the global burden of disease 2016. Med Clínica (English Ed. (2018) 151:171–90. doi: 10.1016/j.medcle.2018.05.043
8. Rehman S, Rehman E, Ikram M, Jianglin Z. Cardiovascular disease (CVD): assessment, prediction and policy implications. BMC Public Health. (2021) 21:1–14. doi: 10.1186/s12889-021-11334-2
9. Rehman S, Li X, Wang C, Ikram M, Rehman E, Liu M. Quality of care for patients with acute myocardial infarction (AMI) in Pakistan: a retrospective study. Int J Environ Res Public Health. (2019) 16:3890. doi: 10.3390/ijerph16203890
10. Micek A, Godos J, Del Rio D, Galvano F, Grosso G. Dietary flavonoids and cardiovascular disease: a comprehensive dose–response meta-analysis. Mol Nutr Food Res. (2021) 65:2001019. doi: 10.1002/mnfr.202001019
11. Casas R, Castro-Barquero S, Estruch R, Sacanella E. Nutrition and cardiovascular health. Int J Mol Sci. (2018) 19:3988. doi: 10.3390/ijms19123988
12. Gomez-Delgado F, Katsiki N, Lopez-Miranda J, Perez-Martinez P. Dietary habits, lipoprotein metabolism and cardiovascular disease: from individual foods to dietary patterns. Crit Rev Food Sci Nutr. (2021) 61:1651–69. doi: 10.1080/10408398.2020.1764487
13. Ravera A, Carubelli V, Sciatti E, Bonadei I, Gorga E, Cani D, et al. Nutrition and cardiovascular disease: finding the perfect recipe for cardiovascular health. Nutrients. (2016) 8:363. doi: 10.3390/nu8060363
14. Centritto F, Iacoviello L, di Giuseppe R, De Curtis A, Costanzo S, Zito F, et al. Dietary patterns, cardiovascular risk factors and C-reactive protein in a healthy Italian population. Nutr Metab Cardiovasc Dis. (2009) 19:697–706. doi: 10.1016/j.numecd.2008.11.009
15. Barbaresko J, Koch M, Schulze MB, Nöthlings U. Dietary pattern analysis and biomarkers of low-grade inflammation: a systematic literature review. Nutr Rev. (2013) 71:511–27. doi: 10.1111/nure.12035
16. Mozaffarian D. Dietary and policy priorities for cardiovascular disease, diabetes, and obesity: a comprehensive review. Circulation. (2016) 133:187–225. doi: 10.1161/CIRCULATIONAHA.115.018585
17. Silveira BKS, Oliveira TMS, Andrade PA, Hermsdorff HHM, Rosa C de OB, Franceschini S do CC. Dietary pattern and macronutrients profile on the variation of inflammatory biomarkers: scientific update. Cardiol Res Pract. (2018) 2018:2575. doi: 10.1155/2018/4762575
18. Dauchet L, Amouyel P, Dallongeville J. Fruits, vegetables and coronary heart disease. Nat Rev Cardiol. (2009) 6:599–608. doi: 10.1038/nrcardio.2009.131
19. Dauchet L, Amouyel P, Hercberg S, Dallongeville J. Fruit and vegetable consumption and risk of coronary heart disease: a meta-analysis of cohort studies. J Nutr. (2006) 136:2588–93. doi: 10.1093/jn/136.10.2588
20. Arouca A, Michels N, Moreno LA, González-Gil EM, Marcos A, Gómez S, et al. Associations between a Mediterranean diet pattern and inflammatory biomarkers in European adolescents. Eur J Nutr. (2018) 57:1747–60. doi: 10.1007/s00394-017-1457-4
21. Lichtenstein AH, Appel LJ, Brands M, Carnethon M, Daniels S, Franch HA, et al. Diet and lifestyle recommendations revision 2006: a scientific statement from the American heart association nutrition committee. Circulation. (2006) 114:82–96. doi: 10.1161/CIRCULATIONAHA.106.176158
22. Hosseini B, Berthon BS, Saedisomeolia A, Starkey MR, Collison A, Wark PAB, et al. Effects of fruit and vegetable consumption on inflammatory biomarkers and immune cell populations: a systematic literature review and meta-analysis. Am J Clin Nutr. (2018) 108:136–55. doi: 10.1093/ajcn/nqy082
23. Corley J, Kyle JAM, Starr JM, McNeill G, Deary IJ. Dietary factors and biomarkers of systemic inflammation in older people: the Lothian Birth Cohort 1936. Br J Nutr. (2015) 114:1088–98. doi: 10.1017/S000711451500210X
24. Rehman S, Rehman N, Naz M, Mumtaz A, Jianglin Z. Application of grey-based SWARA and COPRAS techniques in disease mortality risk assessment. J Healthc Eng. (2021) 2021:2157. doi: 10.1155/2021/7302157
25. Hansen P, Devlin N. Multi-criteria decision analysis (MCDA) in healthcare decision-making. Oxford Res Encyclopedia Econ Finance. (2019) 3:98. doi: 10.1093/acrefore/9780190625979.013.98
26. Durbach IN, Stewart TJ. Modeling uncertainty in multi-criteria decision analysis. Eur J Oper Res. (2012) 223:1–14. doi: 10.1016/j.ejor.2012.04.038
27. Mumtaz A, Rehman E, Rehman S, Hussain I. Impact of environmental degradation on human health: an assessment using multicriteria decision making. Front Public Heal. (2022) 9:2743. doi: 10.3389/fpubh.2021.812743
28. Huang IB, Keisler J, Linkov I. Multi-criteria decision analysis in environmental sciences: Ten years of applications and trends. Sci Total Environ. (2011) 409:3578–94. doi: 10.1016/j.scitotenv.2011.06.022
29. Rehman S, Rehman E, Hussain I, Jianglin Z. Socioeconomic influence on cardiac mortality in the South Asian Region: new perspectives from grey modeling and G-TOPSIS. J Healthc Eng. (2021) 2021:246. doi: 10.1155/2021/6866246
30. Ng DKW, Deng J. Contrasting grey system theory to probability and fuzzy. ACM Sigice Bull. (1995) 20:3–9. doi: 10.1145/202081.202082
31. Liu S, Xie N, Forrest J. Novel models of grey relational analysis based on visual angle of similarity and nearness. Grey Syst Theory Appl. (2011) 54:6696 doi: 10.1108/20439371111106696
32. Rehman S, Rehman E, Mumtaz A, Jianglin Z. A multicriteria decision-making approach in exploring the nexus between wind and solar energy generation, economic development, fossil fuel consumption, and CO2 emissions. Front Environ Sci. (2022) 659:9384. doi: 10.3389/fenvs.2021.819384
33. Javed SA, Liu S. Evaluation of outpatient satisfaction and service quality of Pakistani healthcare projects: application of a novel synthetic grey incidence analysis model. Grey Syst Theory Appl. (2018) 8:462–80. doi: 10.1108/GS-04-2018-0018
34. Mahmoudi A, Javed SA, Zhang Z, Deng X. Grey group Qualiflex method: application in project management. In: 2019 IEEE 14th International Conference on Intelligent Systems and Knowledge Engineering (ISKE). IEEE (2019). p. 189–95. doi: 10.1109/ISKE47853.2019.9170357
35. Javed SA, Mahmoudi A, Khan AM, Javed S, Liu S, A. critical review: shape optimization of welded plate heat exchangers based on grey correlation theory. Appl Therm Eng. (2018) 144:593–9. doi: 10.1016/j.applthermaleng.2018.08.086
36. Rehman E, Rehman S. Modeling the nexus between carbon emissions, urbanization, population growth, energy consumption, and economic development in Asia: Evidence from grey relational analysis. Energy Reports. (2022) 8:5430–42. doi: 10.1016/j.egyr.2022.03.179
38. Xuerui T, Julong D, Hongxing P, Sifeng L. Grey system and grey data management in medicine. In: 2007 IEEE International Conference on Grey Systems and Intelligent Services. IEEE (2007). p. 163–6.
39. Diba S, Xie N. Sustainable supplier selection for Satrec Vitalait Milk Company in Senegal using the novel grey relational analysis method. Grey Syst Theory Appl. (2019) 45:3 doi: 10.1108/GS-01-2019-0003
40. Kalyon A, Günay M, Özyürek D. Application of grey relational analysis based on Taguchi method for optimizing machining parameters in hard turning of high chrome cast iron. Adv Manuf. (2018) 6:419–29. doi: 10.1007/s40436-018-0231-z
41. Cambeses-Franco C, González-García S, Feijoo G, Moreira MT. Is the Paleo diet safe for health and the environment? Sci Total Environ. (2021) 781:146717. doi: 10.1016/j.scitotenv.2021.146717
42. Beltrá M, Borrás F, Ropero AB. Sodium content of foods sold in the Spanish market. Results from the BADALI project. Nutrients. (2021) 13:3410. doi: 10.3390/nu13103410
43. Greene MW, Roberts AP, Frugé AD. Negative association between Mediterranean diet adherence and COVID-19 cases and related deaths in Spain and 23 OECD countries: an ecological study. Front Nutr. (2021) 8:591964. doi: 10.3389/fnut.2021.591964
44. de Leciñana MA, Morales A, Martínez-Zabaleta M, Ayo-Martín Ó, Lizán L, Castellanos M. Characteristics of Stroke Units and Stroke Teams in Spain in 2018. Pre2Ictus project. Neurol English Ed. (2022).
45. Ozturk S. Cerebrovascular Risk Factors in Migrants and Refugees. In: Neurology in Migrants and Refugees. Springer (2022). p. 165–74. doi: 10.1007/978-3-030-81058-0_14
46. Feigin VL, Stark BA, Johnson CO, Roth GA, Bisignano C, Abady GG, et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet Neurol. (2021) 20:795–820. doi: 10.1016/S1474-4422(21)00252-0
47. Cayuela A, Cayuela L, Belmonte MJO, Rodríguez-Domínguez S, Escudero-Martínez I, González A. Has stroke mortality stopped declining in Spain? Neurol. (2021) 59:7. doi: 10.1016/j.nrleng.2019.06.007
49. Sotomayor CG, Gomes-Neto AW, Eisenga MF, Nolte IM, Anderson JLC, De Borst MH, et al. Consumption of fruits and vegetables and cardiovascular mortality in renal transplant recipients: a prospective cohort study. Nephrol Dial Transplant. (2020) 35:357–65. doi: 10.1093/ndt/gfy248
50. Towfighi A, Markovic D, Ovbiagele B. Impact of a healthy lifestyle on all-cause and cardiovascular mortality after stroke in the USA. J Neurol Neurosurg Psychiatry. (2012) 83:146–51. doi: 10.1136/jnnp-2011-300743
51. Rodríguez-Campello A, Jiménez-Conde J, Ois Á, Cuadrado-Godia E, Giralt-Steinhauer E, Schroeder H, et al. Dietary habits in patients with ischemic stroke: a case-control study. PLoS ONE. (2014) 9:e114716. doi: 10.1371/journal.pone.0114716
52. Rodríguez-Rodríguez E, Aparicio A, Aranceta-Bartrina J, Gil Á, González-Gross M, Serra-Majem L, et al. Low adherence to dietary guidelines in Spain, especially in the overweight/obese population: The ANIBES Study. J Am Coll Nutr. (2017) 36:240–7. doi: 10.1080/07315724.2016.1248246
53. Martínez-González MÁ, de la Fuente-Arrillaga C, López-del-Burgo C, Vázquez-Ruiz Z, Benito S, Ruiz-Canela M. Low consumption of fruit and vegetables and risk of chronic disease: a review of the epidemiological evidence and temporal trends among Spanish graduates. Public Health Nutr. (2011) 14:2309–15. doi: 10.1017/S1368980011002564
54. Krishnamurthi R V, Barker-Collo S, Barber PA, Tippett LJ, Dalrymple-Alford JC, Tunnage B, et al. Community knowledge and awareness of stroke in New Zealand. J Stroke Cerebrovasc Dis. (2020) 29:104589. doi: 10.1016/j.jstrokecerebrovasdis.2019.104589
55. Pastor AG, Martínez EL-C, Rodríguez-Yáñez M, de Lecinana MA, Amaro S, Arenillas JF, et al. Recommendations of the Spanish society of neurology for the prevention of stroke. Interventions Lifestyle Air Pollut Neurol. (2021) 36:377–87.
56. Amato M, Bonomi A, Laguzzi F, Veglia F, Tremoli E, Werba JP, et al. Overall dietary variety and adherence to the Mediterranean diet show additive protective effects against coronary heart disease. Nutr Metab Cardiovasc Dis. (2020) 30:1315–21. doi: 10.1016/j.numecd.2020.04.002
57. Razquin C, Martinez-Gonzalez MA. A traditional mediterranean diet effectively reduces inflammation and improves cardiovascular health. Nutrients. (2019) 11:1842. doi: 10.3390/nu11081842
58. Mente A, de Koning L, Shannon HS, Anand SS, A. systematic review of the evidence supporting a causal link between dietary factors and coronary heart disease. Arch Intern Med. (2009) 169:659–69. doi: 10.1001/archinternmed.2009.38
59. D'Alessandro A, De Pergola G. Mediterranean diet and cardiovascular disease: a critical evaluation of a priori dietary indexes. Nutrients. (2015) 7:7863–88. doi: 10.3390/nu7095367
60. Liyanage T, Ninomiya T, Wang A, Neal B, Jun M, Wong MG, et al. Effects of the Mediterranean diet on cardiovascular outcomes—a systematic review and meta-analysis. PLoS ONE. (2016) 11:e0159252. doi: 10.1371/journal.pone.0159252
61. Sofi F, Cesari F, Abbate R, Gensini GF, Casini A. Adherence to Mediterranean diet and health status: meta-analysis. Bmj. (2008) 337:1344. doi: 10.1136/bmj.a1344
62. Psaltopoulou T, Sergentanis TN, Panagiotakos DB, Sergentanis IN, Kosti R, Scarmeas N. Mediterranean diet, stroke, cognitive impairment, and depression: a meta-analysis. Ann Neurol. (2013) 74:580–91. doi: 10.1002/ana.23944
63. AlAufi NS, Chan YM, Waly MI, Chin YS, Mohd Yusof B-N, Ahmad N. Application of mediterranean diet in cardiovascular diseases and type 2 diabetes mellitus: motivations and challenges. Nutrients. (2022) 14:2777. doi: 10.3390/nu14132777
64. Petersen KS, Kris-Etherton PM. Diet quality assessment and the relationship between diet quality and cardiovascular disease risk. Nutrients. (2021) 13:4305. doi: 10.3390/nu13124305
65. Kris-Etherton PM, Petersen KS, Velarde G, Barnard ND, Miller M, Ros E, et al. Barriers, opportunities, and challenges in addressing disparities in diet-related cardiovascular disease in the United States. J Am Heart Assoc. (2020) 9:e014433. doi: 10.1161/JAHA.119.014433
66. Aspry KE, Van Horn L, Carson JAS, Wylie-Rosett J, Kushner RF, Lichtenstein AH, et al. Medical nutrition education, training, and competencies to advance guideline-based diet counseling by physicians: a science advisory from the American heart association. Circulation. (2018) 137:e821–41. doi: 10.1161/CIR.0000000000000563
67. Lichtenstein AH, Ludwig DS. Bring back home economics education. Jama. (2010) 303:1857–8. doi: 10.1001/jama.2010.592
68. Rodgers GP, Collins FS. Precision nutrition—the answer to “what to eat to stay healthy. Jama. (2020) 324:735–6. doi: 10.1001/jama.2020.13601
69. De Roos B, Brennan L. Personalised interventions—a precision approach for the next generation of dietary intervention studies. Nutrients. (2017) 9:847. doi: 10.3390/nu9080847
70. Ordovas JM, Ferguson LR, Tai ES, Mathers JC. Personalised nutrition and health. Bmj. (2018) 361:2173. doi: 10.1136/bmj.k2173
Keywords: dietary habits, cardiac disease prevention, IHD, stroke, Spain, dietary and nutritional patterns, cardiovascular disease
Citation: Rehman S and Jianglin Z (2022) Micronutrient deficiencies and cardiac health. Front. Nutr. 9:1010737. doi: 10.3389/fnut.2022.1010737
Received: 03 August 2022; Accepted: 26 September 2022;
Published: 14 October 2022.
Edited by:
Aamir Shehzad, UniLaSalle, FranceReviewed by:
Aftab Alam, University at Buffalo, United StatesUmar Farooq, Northwestern Polytechnical University, China
Faiza Manzoor, Zhejiang University, China
Copyright © 2022 Rehman and Jianglin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zhang Jianglin, emhhbmcuamlhbmdsaW4mI3gwMDA0MDtzemhvc3BpdGFsLmNvbQ==
†ORCID: Shazia Rehman orcid.org/0000-0003-4563-1124
Zhang Jianglin orcid.org/0000-0003-0434-1729