 Santiago Navas-Carretero1,2,3*†
Santiago Navas-Carretero1,2,3*† Rodrigo San-Cristobal1*†‡Pia Siig Vestentoft4
Rodrigo San-Cristobal1*†‡Pia Siig Vestentoft4 Jennie C. Brand-Miller5
Jennie C. Brand-Miller5 Elli Jalo6
Elli Jalo6 Margriet Westerterp-Plantenga7
Margriet Westerterp-Plantenga7 Elizabeth J. Simpson8
Elizabeth J. Simpson8 Teodora Handjieva-Darlenska9
Teodora Handjieva-Darlenska9 Gareth Stratton10Maija Huttunen-Lenz11
Gareth Stratton10Maija Huttunen-Lenz11 Tony Lam12
Tony Lam12 Roslyn Muirhead5
Roslyn Muirhead5 Sally Poppitt13
Sally Poppitt13 Kirsi H. Pietiläinen14,15Tanja Adam7Moira A. Taylor8Svetoslav Handjiev9
Kirsi H. Pietiläinen14,15Tanja Adam7Moira A. Taylor8Svetoslav Handjiev9 Melitta A. McNarry10Sylvia Hansen16Shannon Brodie5
Melitta A. McNarry10Sylvia Hansen16Shannon Brodie5 Marta P. Silvestre13,17Ian A. Macdonald8Nadka Boyadjieva9
Marta P. Silvestre13,17Ian A. Macdonald8Nadka Boyadjieva9 Kelly A. Mackintosh10Wolfgang Schlicht18Amy Liu13Thomas M. Larsen4
Kelly A. Mackintosh10Wolfgang Schlicht18Amy Liu13Thomas M. Larsen4 Mikael Fogelholm6
Mikael Fogelholm6 Anne Raben4,19
Anne Raben4,19 J. Alfredo Martinez1,2,3‡
J. Alfredo Martinez1,2,3‡- 1Center for Nutrition Research, University of Navarra, Pamplona, Spain
- 2Centro de Investigación Biomédica en Red (CIBER) obn, Instituto de Salud Carlos III, Madrid, Spain
- 3IdiSNA, Navarra Institute for Health Research, Pamplona, Spain
- 4Department of Nutrition, Exercise and Sports, Faculty of Science, University of Copenhagen, Copenhagen, Denmark
- 5School of Life and Environmental Sciences and Charles Perkins Centre, The University of Sydney, Sydney, NSW, Australia
- 6Department of Food and Nutrition, University of Helsinki, Helsinki, Finland
- 7Department of Nutrition and Movement Sciences, NUTRIM, School of Nutrition and Translational Research in Metabolism, Maastricht University, Maastricht, Netherlands
- 8Division of Physiology, Pharmacology and Neuroscience, MRC/ARUK Centre for Musculoskeletal Ageing Research, ARUK Centre for Sport, Exercise and Osteoarthritis, National Institute for Health Research (NIHR) Nottingham Biomedical Research Centre, School of Life Sciences, Queen's Medical Centre, Nottingham, United Kingdom
- 9Department of Pharmacology and Toxicology, Medical University of Sofia, Sofia, Bulgaria
- 10Applied Sports Technology, Exercise and Medicine (A-STEM) Research Centre, College of Engineering, Swansea, United Kingdom
- 11Institute of Nursing Science, University of Education, Schwäbisch Gmünd, Germany
- 12NetUnion Sarl, Lausanne, Switzerland
- 13Human Nutrition Unit, Department of Medicine, School of Biological Sciences, University of Auckland, Auckland, New Zealand
- 14Obesity Research Unit, Diabetes and Obesity Research Program, University of Helsinki and Endocrinology, Helsinki, Finland
- 15Abdominal Center, Helsinki University Hospital and University of Helsinki, Helsinki, Finland
- 16Cologne Center for Ethics, Rights, Economics, and Social Sciences of Health, University of Cologne, Cologne, Germany
- 17Center for Health Technology Services Research (CINTESIS), NOVA Medical School, NMS, Universidade Nova de Lisboa, Lisboa, Portugal
- 18Exercise and Health Sciences, University of Stuttgart, Nobelstraße, Germany
- 19Steno Diabetes Centre Copenhagen, Gentofte, Denmark
Background: Individuals with pre-diabetes are commonly overweight and benefit from dietary and physical activity strategies aimed at decreasing body weight and hyperglycemia. Early insulin resistance can be estimated via the triglyceride glucose index {TyG = Ln [TG (mg/dl) × fasting plasma glucose (FPG) (mg/dl)/2]} and the hypertriglyceridemic-high waist phenotype (TyG-waist), based on TyG x waist circumference (WC) measurements. Both indices may be useful for implementing personalized metabolic management. In this secondary analysis of a randomized controlled trial (RCT), we aimed to determine whether the differences in baseline TyG values and TyG-waist phenotype predicted individual responses to type-2 diabetes (T2D) prevention programs.
Methods: The present post-hoc analyses were conducted within the Prevention of Diabetes through Lifestyle intervention and population studies in Europe and around the world (PREVIEW) study completers (n = 899), a multi-center RCT conducted in eight countries (NCT01777893). The study aimed to reduce the incidence of T2D in a population with pre-diabetes during a 3-year randomized intervention with two sequential phases. The first phase was a 2-month weight loss intervention to achieve ≥8% weight loss. The second phase was a 34-month weight loss maintenance intervention with two diets providing different amounts of protein and different glycemic indices, and two physical activity programs with different exercise intensities in a 2 x 2 factorial design. On investigation days, we assessed anthropometrics, glucose/lipid metabolism markers, and diet and exercise questionnaires under standardized procedures.
Results: Diabetes-related markers improved during all four lifestyle interventions. Higher baseline TyG index (p < 0.001) was associated with greater reductions in body weight, fasting glucose, and triglyceride (TG), while a high TyG-waist phenotype predicted better TG responses, particularly in those randomized to physical activity (PA) of moderate intensity.
Conclusions: Two novel indices of insulin resistance (TyG and TyG-waist) may allow for a more personalized approach to avoiding progression to T2D.
Clinical Trial Registration: https://clinicaltrials.gov/ct2/show/NCT01777893 reference, identifier: NCT01777893.
Introduction
Pre-diabetes and type 2 diabetes (T2D) with accompanying metabolic complications, such as hyperglycemia, insulin resistance, disturbances in lipid metabolism, and pro-inflammatory processes, are associated with the obesity pandemic (1, 2). Pre-diabetes is defined as impaired fasting glucose and/or glucose intolerance or/and elevated glycosylated hemoglobin (HbA1c) with or without overweight or obesity. More targeted preventive and management interventions require investigation with the aim of improved metabolic outcomes (3). Individuals with obesity, pre-diabetes, and T2D benefit from lifestyle interventions involving dietary and physical activity (PA) programs, in which macronutrient distribution, glycemic index (GI), and fiber consumption are prescribed, within energy-restricted diets (4–6). In addition, various PA programs incorporating different exercise types are also beneficial (7, 8).
Indeed, clinical and epidemiological evidence highlights independent or combined beneficial effects of manipulating dietary patterns (quantity and composition of the nutritional intake) and/or PA (type, intensity, and/or frequency) to improve glucose homeostasis and reduce diabetes incidence in people with pre-diabetes (9–11). Specifically, previous lifestyle interventions, such as the Chinese Da Qing study, the Finnish Diabetes Prevention Study, and the US, Indian, and Japanese programs have demonstrated evidence in precluding and delaying progression to T2D and associated morbidities (12). Furthermore, a lifestyle approach was shown to reduce all-cause mortality after 30 years of follow-up (13).
Clinical trials implementing tailored dietary and PA prescriptions for T2D prevention and management have shown inter-individual differences depending on the pre-diabetes grade and associated phenotypes (3). Differences in pretreatment fasting glucose and insulin status have been reported to be associated with weight loss success in patients consuming low GI or fat-rich diets (14). Additionally, data-driven cluster analysis using variables related to glucose utilization identified five subgroups within adult-onset diabetes populations providing some potential for precision nutritional management based on personalized phenotypes (15).
A scenario of tailored treatment also requires the availability of simple, reliable, and inexpensive tests to detect insulin resistance. A novel index based on glucose and TG measurements (the TyG index), has shown high sensitivity and specificity for identifying participants with disturbed insulin function (16), as well as early diabetes onset in patients with normal fasting glucose (17). Waist circumference (WC) has also emerged as a useful clinical marker to distinguish patients according to cardiometabolic risks (18). A phenotype characterized by both high WC and high TyG index has been associated consistently with abnormal glucose and insulin metabolism, with a potential for timely detection of diabetes and more personalized interventions (19).
The PREVIEW trial (20) explored whether a nutritional intervention based on different protein intakes and dietary GI in combination with PA at different intensities, after an initial weight loss produced long-term benefits for T2D prevention. All participants had pre-diabetes and were overweight or obese at baseline. While the incidence of T2D after 3 years of intervention was very low in all four-intervention groups, reversion to normal glucose status varied significantly between the two diet groups (21). In the current post-hoc analysis, the TyG index and the high WC high TyG phenotype were tested as a potential predictor of clinical responses concerning lifestyle modification at the end (3 years) of the PREVIEW intervention. In addition, we aimed to specifically identify inter-individual differences in order to personalize lifestyle prescriptions with a focus on precision nutrition. We hypothesized that different intervention patterns may have differential effects depending on the baseline phenotype.
Materials/Subjects and Methods
The present post-hoc analyses were conducted within the PREVIEW study (NCT01777893) which has been described elsewhere (20). In summary, this study was a multi-center randomized trial conducted at eight sites in eight different countries, aiming to reduce the incidence of T2D in a population with pre-diabetes (21). The 3-year randomized intervention trial was implemented in two phases. First, a 2-month weight loss phase using a commercial low-energy diet (LED) (~3.4 MJ ≪800 kcal≫ per day) to achieve an ≥ 8% bodyweight reduction (22). Second, a 34-month intervention for weight loss maintenance encompassing four intervention arms with two diets and two PA programs using a 2 x 2 factorial design (21). Given the nature of the study, and the final outcome, it was decided that no control group would be needed, and benefits of participating in the intervention were expected in the four intervention arms (20).
The sample size was calculated to be 2,403 subjects, taking into account data from the Finnish Diabetes Prevention Study (DPS) and US Diabetes Prevention Program (DPP), and anticipating a 3-year incidence of T2D in our population of 21%, as described in detail in the Methods article of the PREVIEW Study (20). Once the potential participants were confirmed eligible, they were enrolled in the trial and randomized to one of the four treatment groups. Randomization was stratified by gender and age group (25–54, and 55–70 years of age), and sequentially assigned from each stratum to different interventions, hence, securing an even distribution of gender and age group over the four intervention arms in each center (20).
A total of 2,326 participants were enrolled in the intervention; of those 2,223 started the trial, and completed CID7 899. These participants were adults (25–70 years), overweight [body mass index (BMI) ≥ 25 kg/m2] men and women with pre-diabetes as defined by the American Diabetes Association (ADA): fasting plasma glucose (FPG) of 5.6-−6.9 mmol/L and/or of 7.8-−11.0 mmol/L 2 h after an oral glucose tolerance test (OGTT) of 75 g glucose when FPG <7.0 mmol/L (23).
Clinical investigation days (CID) were conducted in the facilities of the intervention centers at baseline (CID1), 2 months (CID2, end of the first phase), 6 months (CID3), 12 months (CID4), 18 months (CID5), 24 months (CID6), and 36 months (CID7, end of the trial). In the present study, only data from the first and the last visits were used in the analyses. At each CID, anthropometry, blood samples, 24-h urine samples, 7-days accelerometer data, dietary records, and questionnaires were collected. In addition, participants attended 17 group visits led by trained instructors who supported the acquisition of new diet and physical activity (PA) habits. A behavior modification tool (PREMIT) was developed specifically for PREVIEW (24). All centers had approval from their respective Research Ethics Boards before starting the trial, and all participants were required to give written informed consent in their mother tongue before enrollment (20). The study was conducted in accordance with the ethical standards of the appropriate ethics committee of each center, and following the Helsinki Declaration of 1975 as revised in 1983.
Those participants who reached ≥8% body weight loss during the low-energy diet (LED) phase (n = 1,856), proceeded with the 34-month weight maintenance phase in one of the four intervention arms to which they were randomly allocated at the beginning of the study. The two diets were consumed ad libitum having received guidance on the proportion of foods to consume from different food categories in order to achieve the following nutritional composition: (1) Moderate protein (MP) diet (15% of energy – E% - from protein, 30 E% fat, 55 E% carbohydrates, and moderate GI, (2) High protein (HP) diet (25 E% protein, 30 E% fat, 45 E% carbohydrates, and lower GI). The two PA groups, both with a comparable energy expenditure of >4,200 kJ/week, were as follows: high-intensity (HI) PA (75 min/week) and moderate-intensity (MI) PA (150 min/week).
Data Collection and Processing
All measures and samples were collected at the intervention centers during the CIDs following Standard Operation Procedures (SOP) specifically designed for the study (20). Blood samples were collected from the antecubital vein after fasting for 10–12 h. At baseline, month 6, and years 1, 2, and 3, an oral glucose tolerance test (OGTT) with 75 g glucose was performed, with blood sample collection at every 30 min over the subsequent 2 h, although in the present analysis, only data from baseline and 3 years are analyzed. Blood samples were initially stored at −80°C and then sent to the central laboratory of the project in Finland (National Institute for Health and Welfare, Helsinki) for the analysis of FPG, glycosylated hemoglobin (HbA1c), insulin, homeostatic model assessment of insulin resistance (HOMA-IR), lipids (total, HDL and LDL cholesterol, triglycerides -TG-), and C-reactive protein, as previously described (20). Insulin was measured in Denmark (University of Copenhagen) on Siemens Immulite 2000 equipment, Siemens Healthcare, Diagnostic products, Gwynedds, UK following the Immuno-Chemiluminescent method as previously described (21).
During the CIDs, anthropometric and blood pressure measurements were also collected (22). Standardized measures for body weight, body composition (fat mass and fat-free mass by Bioelectrical Impedance Analysis and DEXA, height, waist, and hip and thigh circumference were performed in light clothes by trained researchers, following the guidance described in the specific SOP developed for PREVIEW. Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured on the right arm with a validated automatic device after 5–10 min in a resting position (21). The details concerning the analyses estimating reported energy intake via 4-day food records and actual protein consumption, accelerometer outcomes, and those explanations involving the Baecke questionnaire implementation have been described elsewhere (21).
The triglyceride glucose index (TyG) and the TyG-waist circumference index (TyG-waist) were estimated as surrogate markers of insulin resistance reflecting the individual physiological status (25). The TyG and TyG-Waist were calculated using the following formulas: TyG = Ln [TG (mg/dl) × FPG (mg/dl)/2] (16) and TyG-Waist = TyG index × WC (cm) (26).
Statistical Methods
Baseline descriptive variables of completers are shown as mean ± SD, with ANOVA used to assess the effect of age and sex (Table 1). To determine the influence of the intervention within each arm (diet and PA groups), a 2 x 2 factorial ANOVA was performed on anthropometrical and biochemical measures for participants who provided data at baseline and CID7 (3 years). Linear regression models were fitted to changes in anthropometrical and biochemical measures from baseline to the end of the study. In the first model, we adjusted for age, sex, and baseline values of the dependent variable. Intervention center and change in body mass index (BMI) were added as covariates in Model 2. These regression analyses also considered the interaction between diet (energy and protein intake) and PA (Baecke questionnaires).
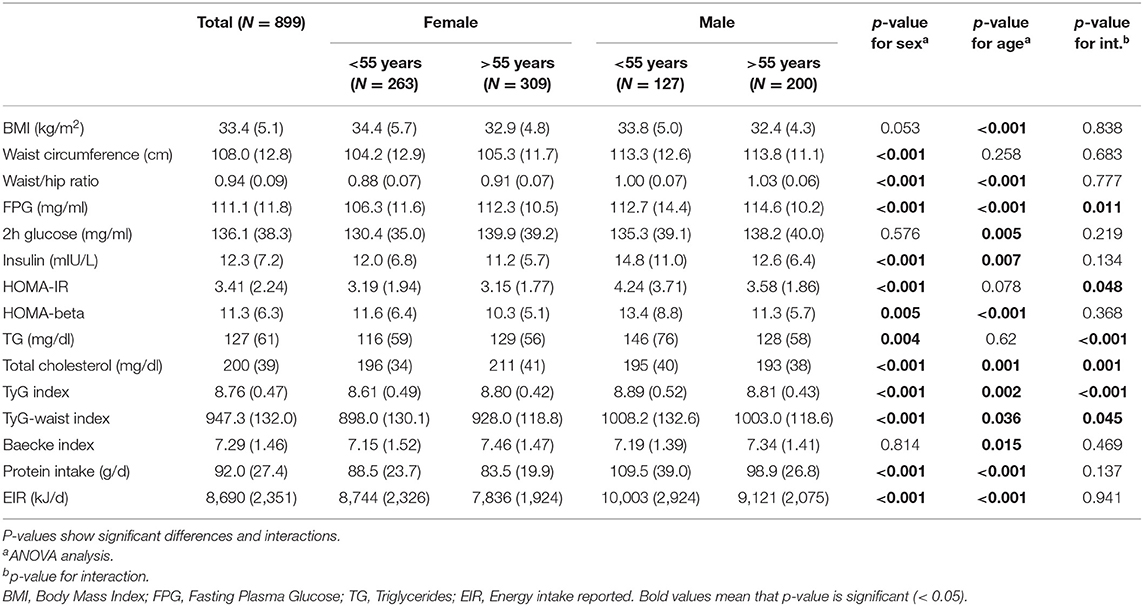
Table 1. Baseline characteristics of PREVIEW completer participants categorized by age and sex.
Participants were subsequently categorized into two groups according to the median values of the TyG and TyG-waist index (8.8 for TyG and 943.6 for TyG-waist, respectively) in order to assess independently the predictive value of these trygliceride-related markers and the interaction with the intervention arms. Linear regression analyses for the difference between baseline and endpoint were carried out to assess the estimated marginal means for the anthropometric and metabolic markers. The regression model included the interaction term of the two TyG categories and each one of the intervention arms (in separate models) adjusted for age, sex, baseline BMI, and intervention center.
The results of per protocol analysis were preferred because they better reflect the effects of the intervention when considered optimally, decreasing the probability of incurring a type II error, as described elsewhere (27, 28). The statistical per protocol analyses and calculations were carried out using the statistical program, R version 4.0.2 (R Core Team, Vienna, Austria) using the following packages “dplyr,” “psych,” “DescTools,” “tidyr,” “ggplot2,” “ggpubr,” “MASS,” “multcomp,” “emmeans,” and RStudio version 1.2.1335. The P < 0.05 was considered statistically significant.
Results
Baseline characteristics of the completers (n = 899) in the analysis are shown in Table 1. Sex, age, body mass index (BMI), and WC correlated as expected with specific metabolic markers of glucose homeostasis and insulin resistance. Energy intake and physical activity (PA) (assessed by Baecke estimation) were also significant predictors. The TyG (p < 0.001) and the TyG-waist index (p = 0.045) showed significant interactions with age and sex with a modification of the effects mediated by both factors (Table 1).
Changes in adiposity, glucose, and TG markers in the intervention arms from baseline to the end of the study are shown in Table 2. There were no differences in changes in glucose, BMI, and WC among the four interventions groups (Table 2). However, there were greater reductions in TG (P = 0.004), TyG (p = 0.023), and TyG-waist (p = 0.061) in the moderate PA group. The Baecke scores showed that protein intake and energy intake varied as expected according to the intervention group (Table 2).
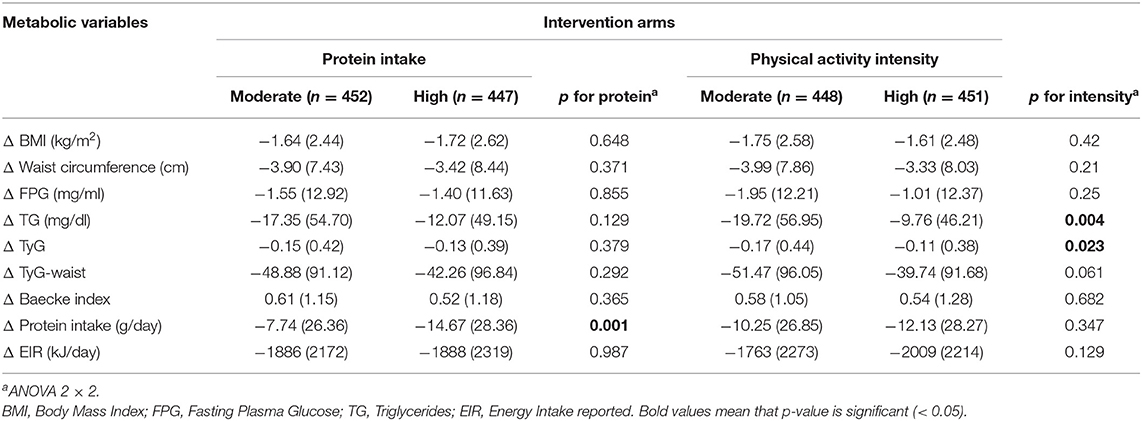
Table 2. Change in anthropometrical and biochemical variables during the PREVIEW intervention between baseline and after 36-months of intervention (CID7), categorized by intervention arm.
The regression models when adjusted by age, sex, baseline value of the dependent variable, intervention center, and BMI changes did not demonstrate any favorable effects of a high protein diet compared with a moderate protein diet on changes in fasting glucose (p = 0.242) or circulating TG (p = 0.181) concentrations (Table 3).
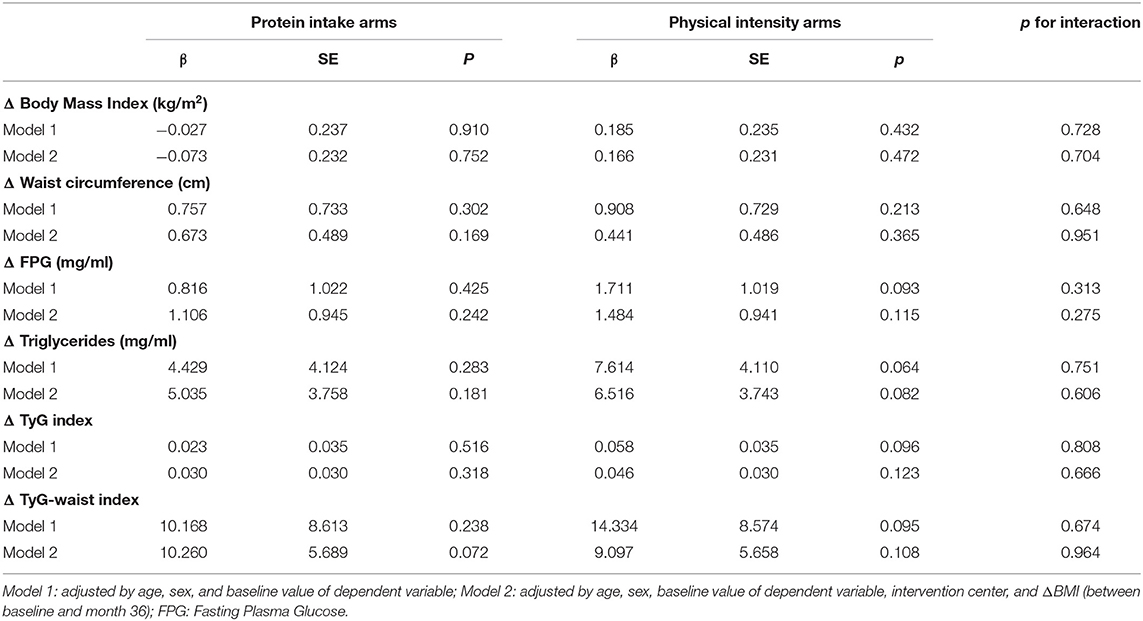
Table 3. Regression models concerning the effect of intervention arms (diet and PA groups) on the variation of anthropometrical and biochemical markers as dependent variables after 36 months of intervention.
Elevated TyG index at baseline independently and significantly predicted greater reductions in BMI, FPG, and TG, but not WC, within each intervention group (Figure 1). Furthermore, a higher baseline TyG-waist phenotype was associated with greater decreases in WC, FPG, and circulating TG, irrespective of the protein level (Figure 2). Moderate intensity PA (Figure 3) predicted more favorable metabolic effects than more intensive PA. Remarkably, those participants with higher baseline TyG-waist values responded better overall to all lifestyle interventions (Figures 2, 3).
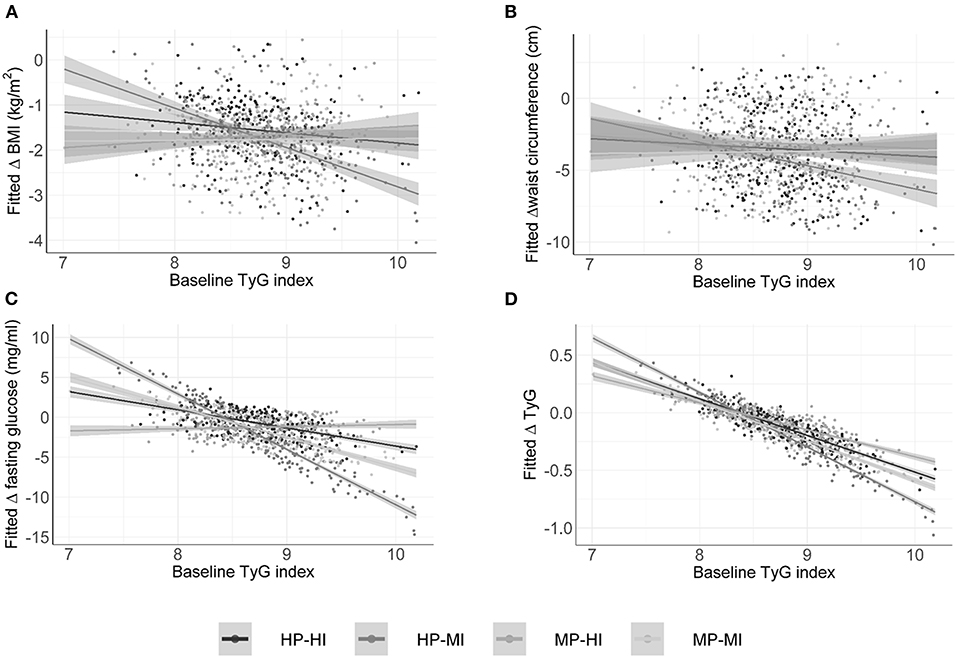
Figure 1. Baseline triglyceride glucose index (TyG) prediction value for changes in anthropometric and metabolic outcomes categorized by the intervention groups of the PREVIEW study. HP, high protein; MP, moderate protein; HI, high intensity; MI, moderate intensity. (A) Fitted change in BMI; (B) Fitted change in waist circumference; (C) Fitted change in fasting glucose; (D) Fitted change in triglycerides.
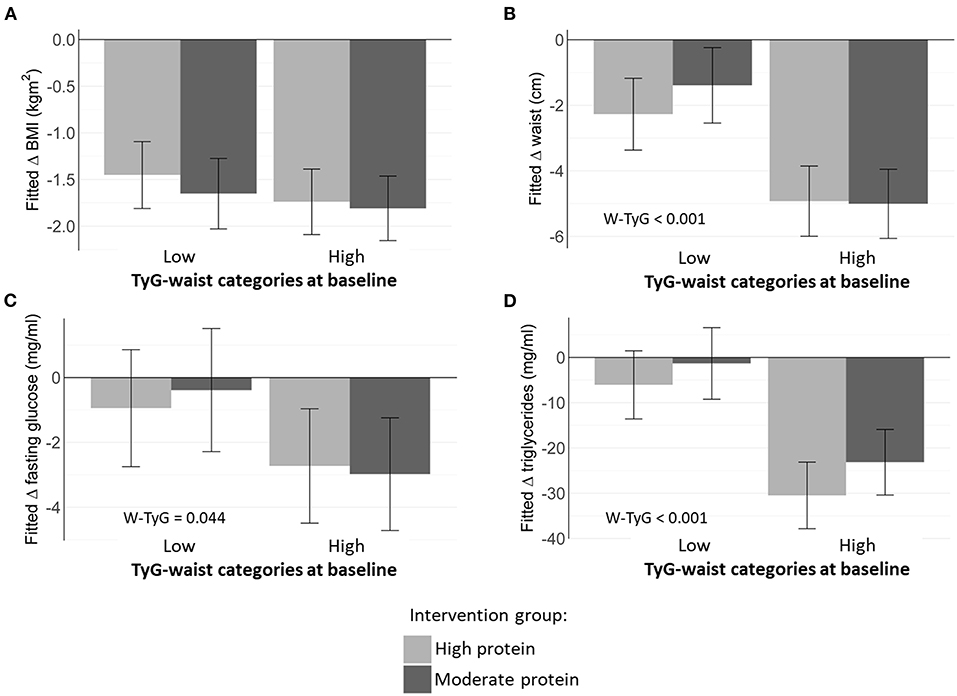
Figure 2. Estimated marginal means of changes in metabolic markers depending on baseline TyG-waist categories and dietary protein intake (high vs. moderate intervention group). (A) Fitted change in BMI; (B) Fitted change in waist circumference; (C) Fitted change in fasting glucose; (D) Fitted change in triglycerides.
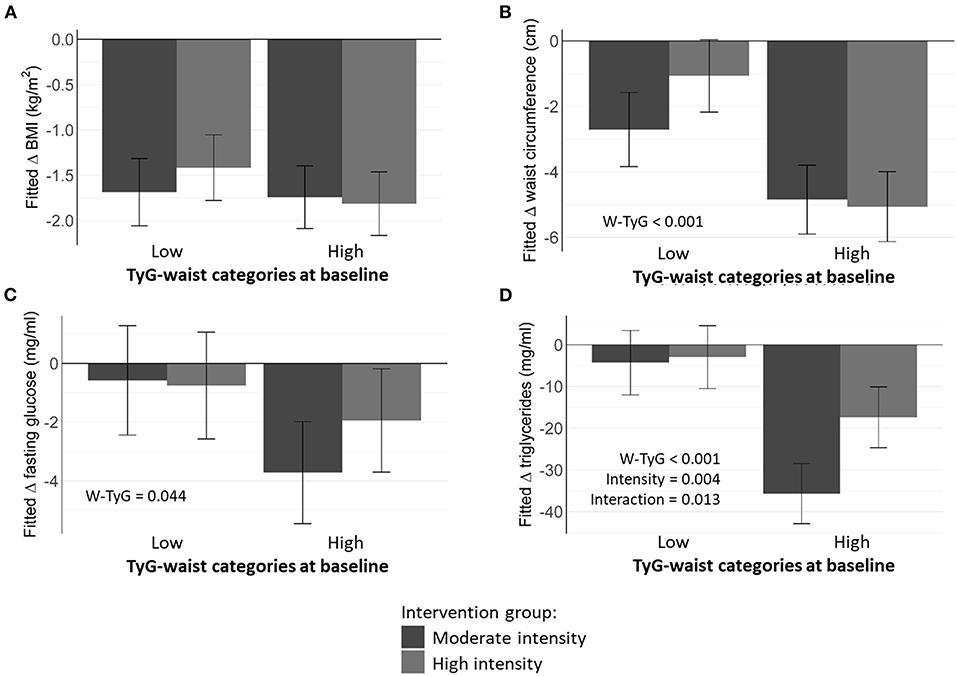
Figure 3. Estimated marginal means of metabolic markers depending on baseline TyG- waist categories and physical activity (high vs. moderate). (A) Fitted change in BMI; (B) Fitted change in waist circumference; (C) Fitted change in fasting glucose; (D) Fitted change in triglycerides.
Discussion
Individuals with pre-diabetes and higher baseline TyG and TyG-waist phenotypes had superior outcomes in all four intervention groups in this secondary analysis of the PREVIEW Study. An elevated TyG index at baseline independently predicted greater reductions in body mass index (BMI), FPG, and TG, but not WC, within all four intervention groups. Furthermore, a higher baseline TyG-waist phenotype was associated with greater decreases in WC, FPG, and circulating TG, irrespective of the protein intake. Moderate physical activity (PA) intensity also appeared to be more efficacious than high intensity (HI) PA intervention arms with respect to improvements in TG and WC. However, we did not find any association between the baseline phenotypes (TyG index or TyG-waist phenotype) and response to different treatments.
Obesity and accompanying inflammatory phenomena are associated with hyperglycemia and insulin resistance, providing early manifestations that often lead to type-2 diabetes (T2D) and cardiovascular events (29, 30). Evidence suggests that there are also differences in prognosis associated with diabetes prevention and treatment that are due to inter-individual heterogeneity in glucose tolerance (3). We hypothesized that novel markers of insulin resistance, the TyG index and the TyG-waist phenotype, may help to define and individually categorize patients. Trait differences among patients may appear depending on personal (epi)genotype, microbiota, and phenotypic characteristics. A better understanding of these effects may contribute to tailoring more effective therapeutic interventions for each individual (31). Indeed, the growing emphasis on precision nutrition is based on the premise that clinical variability may require personalized management (32).
Individualized approaches could be supported by “omics” technologies (33, 34) and by clustering patients according to pretreatment weight-for-height, WC, homeostasis model assessment (HOMA), TyG, and other phenotype-based algorithms (15, 35, 36). Recently, a machine-learning approach integrating anthropometrics, blood biochemistry, diet, PA, and gut microbiota composition accurately forecasted personalized post-prandial glycemic response to a meal (37). Precision medicine methodologies may also demonstrate that similar dietary prescriptions cause different weight loss outcomes depending on pre-treatment FPG levels (38), while the precision of clinical monitoring of glucose tolerance and glycosylated hemoglobin (HbA1c) may be useful for pre-diabetes management (39).
The implementation of supervised lifestyle interventions in individuals with pre-diabetes usually focuses on weight loss (5–10% of body mass) by prescribing energy-controlled dietary regimes and increases in exercise expenditure in order to reduce blood glucose levels (40). Less is known about the prescription of dietary patterns with different macronutrient distribution, glycemic loads, or restriction of specific foods. Similarly, we are yet to learn whether the different forms of PA, including moderate vs. vigorous intensity, resistance training, or other health behaviors will differentially improve markers of the metabolic syndrome, including diabetes (41, 42).
Diabetes risk scores and diagnostic algorithms for personalized precision medicine often use factors, such as age, sex, family clinical history, WC, BMI, smoking, and alcohol consumption, dietary and PA habits, as well as blood pressure, lipid and glucose markers (3, 43). Distinctive pathophysiological profiles in pre-diabetes phenotypes have been described based on insulin secretion, insulin sensitivity, and beta-cell dysfunction assessed by IFG, IGT, and Hb1Ac measurements (40). More recently, HOMA, TyG, and TyG-waist phenotypes have been considered with the goal of categorizing different degrees of insulin resistance and glucose status (17) across different patients. Circulating fatty acids and TG have been associated with insulin sensitivity and glucose tolerance, via the generation of toxic lipids and inflammatory molecules. Changes in cellular membranes have also been implicated through alterations in glucose transport and the insulin signaling cascade, endoplasmic reticulum stress, and reactive oxygen species (44). The glucose-fatty acid cycle may also be disturbed via circulating lipid species and inflammatory mediators (45).
Most randomized trials have focused on weight lowering under energy restriction or dietary recommendations concerning the nutritional quality of the consumed foods with an emphasis on fat and carbohydrate/fiber intake as well as general non-personalized instructions for PA of different types and intensities (12). However, less scientific evidence is available on the role of protein intake and its interactions with the level of PA after weight loss is achieved.
The impact of higher protein intake on TG (a marker of lipid metabolism) and the TyG index (as an affordable surrogate of insulin resistance) requires further study. Previous clinical and lifestyle intervention trials have combined multidisciplinary prescriptions, including dietary modifications, with or without energy restriction, with approaches to enhance daily PA or exercise training, making it difficult to separately discriminate the role of each factor (diet vs. PA). These difficulties were overcome in the PREVIEW project (21), where four experimental arms were designed: two levels of protein consumption and two intensities of PA after following a low energy diet (LED) to induce at least 8% weight loss in 2 months (22). Regarding protein intake, the main limitation encountered was that the group following a high protein intake pattern reduced their protein consumption toward the end of the study, which makes it difficult to interpret the results. These findings build on previous studies that suggest replacing sitting with low intensity PA to produce metabolic benefits that contribute to the prevention and management of T2D (46). However, despite differences in instruction [moderate intensity (MI) vs. high intensity (HI) PA], there were no actual differences in PA intensity. Furthermore, total PA was as strongly associated with cardiometabolic risk markers as moderate- to vigorous-intensity physical activity (MVPA), which implies that the accumulation of total PA over the day is more important than the intensity of PA in this population (47).
Secondary analyses in the Look AHEAD and PREDIMED studies, which were focused on reducing cardiometabolic events by means of lifestyle interventions revealed improvements in circulating glucose and TG even after corrections for the degree of weight change (48, 49). And vice versa, most of the previous trials revealed that weight loss seems to be an independent predictor for the prevention of type 2 diabetes mellitus (T2DM), even after adjustments for diet and PA. The PREVIEW project showed that after a period of weight loss, there were no separate effects of diet composition or PA intensity on the risk of developing T2D within 3 years. An unexpected finding in PREVIEW was that significantly fewer participants achieved normoglycemia in the high protein high intensity (HPHI) PA group, compared to the other three groups. However, a limitation of the PREVIEW study is the high attrition rate and the possibility of selection bias (e.g., in the recruitment of more health-conscious participants). Nonetheless, the results appear robust and plausible, providing new evidence that clinicians should consider in a personalized fashion.
Several clinical and epidemiological studies have reported that the TyG index was superior to FPG and TG alone in predicting metabolically unhealthy individuals with fasting glucose levels under 5.5 mmol/L (16, 17, 36), as well as a role for TyG-waist for categorizing the hypertriglyceride phenotype (18, 19). Our findings suggest that the intensity of PA has a role in the management of glucose and lipid status. Furthermore, the conceptual framework underlying precision medicine is founded on assessing inter-individual heterogeneity (50). Accounting for phenotypic variability requires an understanding of the markers to be considered (51) and the characteristics of the intervention (52). In summary, both TyG indices count with sufficient scientific evidence as markers of insulin resistance, which showed similar or better precision than FPG, TG, or WC alone (16, 53). Indeed, these indices are as reliable as homeostatic model assessment for insulin resistance (HOMA-IR) regarding insulin resistance, but additionally are simpler, easier to interpret, and inexpensive than analyzing insulin or HOMA, as well as more informative than glucose measurements (16, 54).
In conclusion, individuals with pre-diabetes and higher baseline TyG and TyG-waist had better outcomes in all four PREVIEW intervention arms. This is in agreement with the commonly accepted clinical practice that patients with extreme features of the metabolic syndrome respond earlier and better to diverse dietary or pharmacological treatments. In contrast, we did not find any association between the baseline phenotype (TyG-index of TyG-waist) and response to different treatments. A goal of this research was to prospectively analyze the value of the baseline insulin resistance status based on both serviceable TyG tools to characterize patients at baseline and explain future outcomes, in order to facilitate a personalized prescription for application in subjects with pre-diabetes based on glucose tolerance status.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Denmark: the Research Ethics Committees of the Capital Region; Finland: Coordinating Ethical Committee of HUS (Helsinki and Uusimaa Hospital District); the UK: UK National Research Ethics Service (NRES) and East Midlands (Leicester) Ethics Committee; Netherlands: Medical Ethics Committee of the Maastricht University Medical Centre; Spain: Research Ethics Committee of the University of Navarra; Bulgaria: Commission on Ethics in Scientific Research with the Medical University-Sofia (KENIMUS); Australia: The University of Sydney, Human Research Ethics Committee (HREC); and New Zealand: Health and Disability Ethics Committees (HDEC). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
AR, JM, MF, JB-M, MW-P, IM, NB, SH, GS, WS, and SP participated in the study design. Specifically, AR and JM were coordinators and led the objectives of this manuscript. SN-C, RS-C, PS, EJ, LS, TH-D, MH-L, TL, RM, KP, TA, MT, MM, SH, SB, MS, KM, AL, and TML conducted the study and provided data necessary for the study. JM and RS-C conducted the statistical analyses. SN-C, RS-C, and JM performed the preliminary writing of the manuscript. All authors read and approved the final version of the manuscript.
Funding
This work was supported by the EU framework program 7 (FP7/2007-2013) grant agreement # 312057, National Health and Medical Research Council - EU Collaborative Grant, AUS 8, ID 1067711), the Glycemic Index Foundation Australia through royalties to the University of Sydney, the New Zealand Health Research Council (14/191) and University of Auckland Faculty Research Development Fund, the Cambridge Weight Plan© donated all products for the 8-weeks LED period, the Danish Agriculture & Food Council, the Danish Meat and Research Institute, National Institute for Health Research Biomedical Research Centre (NIHR BRC) (UK), Biotechnology and Biological Sciences Research Council (BBSRC) (UK), Engineering and Physical Sciences Research Council (EPSRC) (UK), Nutritics (Dublin) donated all dietary analyses software used by UNOTT. Juho VainioFoundation (FIN), Academy of Finland (Grant Numbers: 272376, 314383, 266286, 314135), Finnish Medical Foundation, Gyllenberg Foundation, Novo Nordisk Foundation, Finnish Diabetes Research Foundation, University of Helsinki, Government Research Funds for Helsinki University Hospital (FIN), Jenny and Antti Wihuri Foundation (FIN), Emil Aaltonen Foundation (FIN). CIBEROBN of Spain is also gratefully acknowledged. RS-C acknowledges financial support from the Juan de la Cierva Program Training Grants of the Spanish State Research Agency of the Spanish Ministerio de Ciencia e Innovación y Ministerio de Universidades (FJC2018-038168- I). The funders of the study had no role in the study design, data collection, data analysis, data interpretation, or writing of the report.
Conflict of Interest
TL was employed by company NetUnion Sarl. PS has received travel grants from the Cambridge Weight Plan, UK. JB-M is the President and Director of the Glycemic Index Foundation, oversees a glycemic index GI testing service at the University of Sydney and is a co-author of books about diet and diabetes. IM is a member of the UK Government Scientific Advisory Committee on Nutrition, Treasurer of the Federation of European Nutrition Societies, Treasurer of the World Obesity Federation, member of the Mars Scientific Advisory Council, member of the Mars Europe Nutrition Advisory Board, and Scientific Adviser to the Waltham Centre for Pet Nutrition. He is also a member of the Nestle Research Scientific Advisory Board and of the Novozymes Scientific Advisory Board. SP was the Fonterra Chair in Human Nutrition and Principle Investigator for NZ National Science Challenge High Value Nutrition during the PREVIEW intervention. TML is an advisor for the “Sense” diet program. AR has received honorariums from Novo Nordisk A/S, the International Sweeteners Association, Nordic Sugar and Unilever. JM is the President of IUNS.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The PREVIEW consortium would like to thank all the study participants at all intervention centers for their time and commitment and all scientists, advisors, and students for their dedication and contributions to the study. Specifically, we would like to thank Louise Dye (chairman of the Scientific Advisory Board, SAB), University of Leeds, UK, Richard Atkinson (Ethical Officer of the SAB), Virginia Commonwealth University, USA, and medical expert and consultant Stephen Colagiuri (University of Sydney, Australia). Meyers Madhus A/S is acknowledged for providing training and producing 2 cooking books. Furthermore, we gratefully thank the research staff from each center. From UCPH: Laura Pastor-Sanz, Grith Møller, Lone Vestergaard Nielsen, Kasper Nowak, Arne Astrup, Finn Sandø-Pedersen, Morten Bo Johansen, Ulla Skovbæch Pedersen, Maria Roed Andersen, Marianne Juhl Hansen, Jane Jørgensen, Sofie Skov Frost, and Lene Stevner. From HEL: Heikki Tikkanen, Saara Kettunen, Tiia Kunnas, Sanna Ritola, Laura Korpipää, Heini Hyvärinen, Karoliina Himanen, Tiina Pellinen, Elina Malkamäki, Heidi Jokinen, Pauliina Kokkonen, Liisi Korhonen, Jaana Valkeapää, Heli Pikkarainen, Martta Nieminen, Tuulia Ingman, Pihla Mäkinen, and Sonja Toijonen. From UNOTT: Clare Randall, Nicky Gilbert, Shelley Archer, Sally Maitland, Melanie Marshall, Cheryl Percival, Jakki Pritchard, Laura Helm, and Peter Mansell. From UNAV: Blanca Martinez de Morentin, Maria Hernandez Ruiz de Eguilaz, Salome Perez Diez, Veronica Ciaurriz, Angels Batlle, and Maria Jose Cobo. From MU: Georgi Bogdanov, Pavlina Gateva, Rossica Metodieva, and Galia Dobrevska. From SU: Nils Swindell, Jeff Stephens, Gareth Dunseath, Steve Luzio, and Masoumeh Minou. From THL: Jouko Soundvall, Laura Ramån, Merja Tukiainen, Ira Greinert, Laura Karjalainen, and Jukka Lauronen. From UNSYD: Fiona Atkinson, Michele Whittle, Jessica Burke, Kylie Simpson, Kimberley Way, Sally McClintock, Radhika Seimon, Shelly Keating, Kirsten Bell, Tania Markovic, Cathy Corry, Evalyn Eldering, and Ian Caterson. From UOA: Lindsay Plank, Nicholas Gant, Jon Woodhead, Anne-Thea McGill, Katya Volkova, Madhavi Bollineni, Clarence Vivar, Kelly Storey, Niamh Brennan, and Audrey Tay.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2021.733697/full#supplementary-material
Supplementary Table 1. CONSORT Statement checklist, as required by the ICMJE.
Supplementary Figure 1. Flowchart of the volunteers involved in the study, and whose data were analysed in the present article (Screened, Eligible and Completers, as well as those with valid full data).
Abbreviations
ADA, American Diabetes Association; BMI, body mass index; CID, Clinical Investigation Day; DP, diabetes prevention; EIR, energy intake reported; FPG, fasting plasma glucose; GI, glycemic index; HbA1c, glycosylated hemoglobin; HDL cholesterol, high-density lipoprotein cholesterol; LDL cholesterol, low-density lipoprotein cholesterol; HI, high-intensity; HOMA-IR, homeostatic model assessment of insulin resistance; HP, high protein; LED, low-energy diet; MI, moderate intensity; MP, moderate protein; OGTT, oral glucose tolerance test; PA, physical activity; SOP, Standard Operation Procedure; SBP, systolic blood pressure; DBP, diastolic blood pressure; T2D, Type 2 diabetes mellitus; TG, Triglyceride; TyG, Triglyceride glucose index; TyG-Waist, Triglyceride waist circumference index.
References
1. Carbone S, Del Buono MG, Ozemek C, Lavie CJ. Obesity, risk of diabetes and role of physical activity, exercise training and cardiorespiratory fitness. Prog Cardiovasc Dis. (2019) 62:327–33. doi: 10.1016/j.pcad.2019.08.004
2. Christ A, Lauterbach M, Latz E. Western diet and the immune system: an inflammatory connection. Immunity. (2019) 51:794–811. doi: 10.1016/j.immuni.2019.09.020
3. Campbell MD, Sathish T, Zimmet PZ, Thankappan KR, Oldenburg B, Owens DR, et al. Benefit of lifestyle-based T2DM prevention is influenced by prediabetes phenotype. Nat Rev Endocrinol. (2020) 16:395–400. doi: 10.1038/s41574-019-0316-1
4. Navas-Carretero S, Holst C, Saris WH, van Baak MA, Jebb SA, Kafatos A, et al. The impact of gender and protein intake on the success of weight maintenance and associated cardiovascular risk benefits, independent of the mode of food provision: the DiOGenes randomized trial. J Am Coll Nutr. (2016) 35:20–30. doi: 10.1080/07315724.2014.948642
5. Reynolds AN, Akerman AP, Mann J. Dietary fibre and whole grains in diabetes management: systematic review and meta-analyses. PLoS Med. (2020) 17:e1003053. doi: 10.1371/journal.pmed.1003053
6. Tay J, Thompson CH, Luscombe-Marsh ND, Wycherley TP, Noakes M, Buckley JD, et al. Effects of an energy-restricted low-carbohydrate, high unsaturated fat/low saturated fat diet versus a high-carbohydrate, low-fat diet in type 2 diabetes: a 2-year randomized clinical trial. Diabetes Obes Metab. (2018) 20:858–71. doi: 10.1111/dom.13164
7. Luan X, Tian X, Zhang H, Huang R, Li N, Chen P, et al. Exercise as a prescription for patients with various diseases. J Sport Health Sci. (2019) 8:422–41. doi: 10.1016/j.jshs.2019.04.002
8. Way KL, Hackett DA, Baker MK, Johnson NA. The effect of regular exercise on insulin sensitivity in type 2 diabetes mellitus: a systematic review and meta-analysis. Diabetes Metab J. (2016) 40:253–71. doi: 10.4093/dmj.2016.40.4.253
9. Hrubeniuk TJ, Bouchard DR, Goulet EDB, Gurd B, Senechal M. The ability of exercise to meaningfully improve glucose tolerance in people living with prediabetes: a meta-analysis. Scand J Med Sci Sports. (2020) 30:209–16. doi: 10.1111/sms.13567
10. Jeong Y, Lee E, Park YJ, Kim Y, Kwon O, Kim Y, et al. Review of recent evidence from meal-based diet interventions and clinical biomarkers for improvement of glucose regulation. Prev Nutr Food Sci. (2020) 25:9–24. doi: 10.3746/pnf.2020.25.1.9
11. Senechal M, Slaght J, Bharti N, Bouchard DR. Independent and combined effect of diet and exercise in adults with prediabetes. Diabetes Metab Syndr Obes. (2014) 7:521–9. doi: 10.2147/DMSO.S62367
12. Dagogo-Jack S. Prevention begets prevention - lessons from the Da Qing Study. Nat Rev Endocrinol. (2019) 15:442–3. doi: 10.1038/s41574-019-0227-1
13. Gong Q, Zhang P, Wang J, Ma J, An Y, Chen Y, et al. Morbidity and mortality after lifestyle intervention for people with impaired glucose tolerance: 30-year results of the Da Qing Diabetes Prevention Outcome Study. Lancet Diabetes Endocrinol. (2019) 7:452–61. doi: 10.1016/S2213-8587(19)30093-2
14. Hjorth MF, Ritz C, Blaak EE, Saris WH, Langin D, Poulsen SK, et al. Pretreatment fasting plasma glucose and insulin modify dietary weight loss success: results from 3 randomized clinical trials. Am J Clin Nutr. (2017) 106:499–505. doi: 10.3945/ajcn.117.155200
15. Ahlqvist E, Storm P, Karajamaki A, Martinell M, Dorkhan M, Carlsson A, et al. Novel subgroups of adult-onset diabetes and their association with outcomes: a data-driven cluster analysis of six variables. Lancet Diabetes Endocrinol. (2018) 6:361–9. doi: 10.1016/S2213-8587(18)30051-2
16. Guerrero-Romero F, Simental-Mendia LE, Gonzalez-Ortiz M, Martinez-Abundis E, Ramos-Zavala MG, Hernandez-Gonzalez SO, et al. The product of triglycerides and glucose, a simple measure of insulin sensitivity. Comparison with the euglycemic-hyperinsulinemic clamp. J Clin Endocrinol Metab. (2010) 95:3347–51. doi: 10.1210/jc.2010-0288
17. Navarro-Gonzalez D, Sanchez-Inigo L, Pastrana-Delgado J, Fernandez-Montero A, Martinez JA. Triglyceride-glucose index (TyG index) in comparison with fasting plasma glucose improved diabetes prediction in patients with normal fasting glucose: the Vascular-Metabolic CUN cohort. Prev Med. (2016) 86:99–105. doi: 10.1016/j.ypmed.2016.01.022
18. Ross R, Neeland IJ, Yamashita S, Shai I, Seidell J, Magni P, et al. Waist circumference as a vital sign in clinical practice: a Consensus Statement from the IAS and ICCR Working Group on Visceral Obesity. Nat Rev Endocrinol. (2020) 16:177–89. doi: 10.1038/s41574-019-0310-7
19. Ma CM, Liu XL, Lu N, Wang R, Lu Q, Yin FZ. Hypertriglyceridemic waist phenotype and abnormal glucose metabolism: a system review and meta-analysis. Endocrine. (2019) 64:469–85. doi: 10.1007/s12020-019-01945-6
20. Fogelholm M, Larsen TM, Westerterp-Plantenga M, Macdonald I, Martinez JA, Boyadjieva N, et al. PREVIEW: prevention of diabetes through lifestyle intervention and population studies in Europe and around the World. Design, methods, and baseline participant description of an adult cohort enrolled into a three-year randomised clinical trial. Nutrients. (2017) 9:632. doi: 10.3390/nu9060632
21. Raben A, Vestentoft PS, Brand-Miller J, Jalo E, Drummen M, Simpson L, et al. PREVIEW - Results from a 3-year randomised 2 x 2 factorial multinational trial investigating the role of protein, glycemic index and physical activity for prevention of type-2 diabetes. Diabetes Obes Metab. (2020) 23:324–37. doi: 10.1111/dom.14219
22. Christensen P, Meinert Larsen T, Westerterp-Plantenga M, Macdonald I, Martinez JA, Handjiev S, et al. Men and women respond differently to rapid weight loss: metabolic outcomes of a multi-centre intervention study after a low-energy diet in 2500 overweight, individuals with pre-diabetes (PREVIEW). Diabetes Obes Metab. (2018) 20:2840–51. doi: 10.1111/dom.13466
23. American Diabetes A. Diagnosis and classification of diabetes mellitus. Diabetes Care. (2010) 33(Suppl 1):S62–9. doi: 10.2337/dc10-S062
24. Kahlert D, Unyi-Reicherz A, Stratton G, Meinert Larsen T, Fogelholm M, Raben A, et al. Behavior modification intervention toolbox (PREMIT): a study protocol for a psychological element of a multicenter project. Front Psychol. (2016) 7:1136. doi: 10.3389/fpsyg.2016.01136
25. Zheng S, Shi S, Ren X, Han T, Li Y, Chen Y, et al. Triglyceride glucose-waist circumference, a novel and effective predictor of diabetes in first-degree relatives of type 2 diabetes patients: cross-sectional and prospective cohort study. J Transl Med. (2016) 14:260. doi: 10.1186/s12967-016-1020-8
26. Er LK, Wu S, Chou HH, Hsu LA, Teng MS, Sun YC, et al. Triglyceride glucose-body mass index is a simple and clinically useful surrogate marker for insulin resistance in nondiabetic individuals. PLoS ONE. (2016) 11:e0149731. doi: 10.1371/journal.pone.0149731
27. Tripepi G, Chesnaye NC, Dekker FW, Zoccali C, Jager KJ. Intention to treat and per protocol analysis in clinical trials. Nephrology. (2020) 25:513–7. doi: 10.1111/nep.13709
28. Intention to treat analysis and per protocol analysis: complementary information. Prescrire Int. (2012) 21:304–6.
29. Gonzalez-Muniesa P, Martinez-Gonzalez MA, Hu FB, Despres JP, Matsuzawa Y, Loos RJF, et al. Obesity. Nat Rev Dis Primers. (2017) 3:17034. doi: 10.1038/nrdp.2017.34
30. Davies MJ, D'Alessio DA, Fradkin J, Kernan WN, Mathieu C, Mingrone G, et al. Management of hyperglycemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. (2018) 41:2669–701. doi: 10.2337/dci18-0033
31. Ramos-Lopez O, Milagro FI, Allayee H, Chmurzynska A, Choi MS, Curi R, et al. Guide for current nutrigenetic, nutrigenomic, and nutriepigenetic approaches for precision nutrition involving the prevention and management of chronic diseases associated with obesity. J Nutrigenet Nutrigenomics. (2017) 10:43–62. doi: 10.1159/000477729
32. Gonzalez-Muniesa P, Martinez JA. Precision nutrition and metabolic syndrome management. Nutrients. (2019) 11:2411. doi: 10.3390/nu11102411
33. Corella D, Ordovas JM. The role of omics in precision nutrition: strengths and weaknesses. Nutr Hosp. (2018) 35:10–8. doi: 10.20960/nh.2119
34. Ferguson LR, De Caterina R, Gorman U, Allayee H, Kohlmeier M, Prasad C, et al. Guide and position of the international society of nutrigenetics/nutrigenomics on personalised nutrition: part 1 - fields of precision nutrition. J Nutrigenet Nutrigenomics. (2016) 9:12–27. doi: 10.1159/000446347
35. Phillips SA, Ali M, Modrich C, Oke S, Elokda A, Laddu D, et al. Advances in health technology use and implementation in the era of healthy living: implications for precision medicine. Prog Cardiovasc Dis. (2019) 62:44–9. doi: 10.1016/j.pcad.2018.12.007
36. Sanchez-Inigo L, Navarro-Gonzalez D, Fernandez-Montero A, Pastrana-Delgado J, Martinez JA. The TyG index may predict the development of cardiovascular events. Eur J Clin Invest. (2016) 46:189–97. doi: 10.1111/eci.12583
37. Zeevi D, Korem T, Zmora N, Israeli D, Rothschild D, Weinberger A, et al. Personalized nutrition by prediction of glycemic responses. Cell. (2015) 163:1079–94. doi: 10.1016/j.cell.2015.11.001
38. Ritz C, Astrup A, Larsen TM, Hjorth MF. Weight loss at your fingertips: personalized nutrition with fasting glucose and insulin using a novel statistical approach. Eur J Clin Nutr. (2019) 73:1529–35. doi: 10.1038/s41430-019-0423-z
39. Buse JB, Wexler DJ, Tsapas A, Rossing P, Mingrone G, Mathieu C, et al. 2019 update to: management of hyperglycemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. (2020) 43:487–93. doi: 10.2337/dci19-0066
40. Bell K, Shaw JE, Maple-Brown L, Ferris W, Gray S, Murfet G, et al. A position statement on screening and management of prediabetes in adults in primary care in Australia. Diabetes Res Clin Pract. (2020) 164:108188. doi: 10.1016/j.diabres.2020.108188
41. Abete I, Astrup A, Martinez JA, Thorsdottir I, Zulet MA. Obesity and the metabolic syndrome: role of different dietary macronutrient distribution patterns and specific nutritional components on weight loss and maintenance. Nutr Rev. (2010) 68:214–31. doi: 10.1111/j.1753-4887.2010.00280.x
42. Galarregui C, Abete I, Navas Carretero S, Reglero G, Ramirez de Molina A, Loria Kohen V, et al. Precision dietary guidelines and ingredients for chronic diseases in pre-senior and senior populations. An Sist Sanit Navar. (2018) 41:227–42. doi: 10.23938/ASSN.0311
43. Noble D, Mathur R, Dent T, Meads C, Greenhalgh T. Risk models and scores for type 2 diabetes: systematic review. BMJ. (2011) 343:d7163. doi: 10.1136/bmj.d7163
44. Sobczak AIS, Blindauer CA, Stewart AJ. Changes in plasma free fatty acids associated with type-2 diabetes. Nutrients. (2019) 11:2022. doi: 10.3390/nu11092022
45. Boden G, Salehi S. Why does obesity increase the risk for cardiovascular disease? Curr Pharm Des. (2013) 19:5678–83. doi: 10.2174/1381612811319320003
46. Swindell N, Rees P, Fogelholm M, Drummen M, MacDonald I, Martinez JA, et al. Compositional analysis of the associations between 24-h movement behaviours and cardio-metabolic risk factors in overweight and obese adults with pre-diabetes from the PREVIEW study: cross-sectional baseline analysis. Int J Behav Nutr Phys Act. (2020) 17:29. doi: 10.1186/s12966-020-00936-5
47. Swindell N, Mackintosh K, McNarry M, Stephens JW, Sluik D, Fogelholm M, et al. Objectively measured physical activity and sedentary time are associated with cardiometabolic risk factors in adults with prediabetes: the PREVIEW study. Diabetes Care. (2018) 41:562–9. doi: 10.2337/dc17-1057
48. Salas-Salvado J, Diaz-Lopez A, Ruiz-Canela M, Basora J, Fito M, Corella D, et al. Effect of a lifestyle intervention program with energy-restricted mediterranean diet and exercise on weight loss and cardiovascular risk factors: one-year results of the PREDIMED-plus trial. Diabetes Care. (2019) 42:777–88. doi: 10.2337/dc18-0836
49. Gibbs BB, Brancati FL, Chen H, Coday M, Jakicic JM, Lewis CE, et al. Effect of improved fitness beyond weight loss on cardiovascular risk factors in individuals with type 2 diabetes in the Look AHEAD study. Eur J Prev Cardiol. (2014) 21:608–17. doi: 10.1177/2047487312462823
50. Hemler EC, Hu FB. Plant-based diets for personal, population, and planetary health. Adv Nutr. (2019) 10(Suppl_4):S275–S83. doi: 10.1093/advances/nmy117
51. O'Donoghue G, Kennedy A, Andersen GS, Carr B, Cleary S, Durkan E, et al. Phenotypic responses to a lifestyle intervention do not account for inter-individual variability in glucose tolerance for individuals at high risk of type 2 diabetes. Front Physiol. (2019) 10:317. doi: 10.3389/fphys.2019.00317
52. Solomon TPJ. Sources of inter-individual variability in the therapeutic response of blood glucose control to exercise in type 2 diabetes: going beyond exercise dose. Front Physiol. (2018) 9:896. doi: 10.3389/fphys.2018.00896
53. Lee J, Kim B, Kim W, Ahn C, Choi HY, Kim JG, et al. Lipid indices as simple and clinically useful surrogate markers for insulin resistance in the U.S population. Sci Rep. (2021) 11:2366. doi: 10.1038/s41598-021-82053-2
Keywords: obesity, pre-diabetes, triglycerides (PubChem CID: 5460048), hypertriglyceridemic-waist phenotype, precision nutrition, diabetes, carbohydrate metabolism, lipid markers
Citation: Navas-Carretero S, San-Cristobal R, Siig Vestentoft P, Brand-Miller JC, Jalo E, Westerterp-Plantenga M, Simpson EJ, Handjieva-Darlenska T, Stratton G, Huttunen-Lenz M, Lam T, Muirhead R, Poppitt S, Pietiläinen KH, Adam T, Taylor MA, Handjiev S, McNarry MA, Hansen S, Brodie S, Silvestre MP, Macdonald IA, Boyadjieva N, Mackintosh KA, Schlicht W, Liu A, Larsen TM, Fogelholm M, Raben A and Martinez JA (2021) Appraisal of Triglyceride-Related Markers as Early Predictors of Metabolic Outcomes in the PREVIEW Lifestyle Intervention: A Controlled Post-hoc Trial. Front. Nutr. 8:733697. doi: 10.3389/fnut.2021.733697
Received: 30 June 2021; Accepted: 24 September 2021;
Published: 01 November 2021.
Edited by:
Rikard Landberg, Chalmers University of Technology, SwedenReviewed by:
Rouzha Zlatanova Pancheva, Medical University of Varna, BulgariaYoshitaka Hashimoto, Kyoto Prefectural University of Medicine, Japan
Stefan Kabisch, Charité–Universitätsmedizin Berlin, Germany
Copyright © 2021 Navas-Carretero, San-Cristobal, Siig Vestentoft, Brand-Miller, Jalo, Westerterp-Plantenga, Simpson, Handjieva-Darlenska, Stratton, Huttunen-Lenz, Lam, Muirhead, Poppitt, Pietiläinen, Adam, Taylor, Handjiev, McNarry, Hansen, Brodie, Silvestre, Macdonald, Boyadjieva, Mackintosh, Schlicht, Liu, Larsen, Fogelholm, Raben and Martinez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Santiago Navas-Carretero, c25hdmFzQHVuYXYuZXM=; Rodrigo San-Cristobal, cm9kcmlnby5zYW5jcmlzdG9iYWxAaW1kZWEub3Jn
†These authors have contributed equally to this work and share first authorship
‡Present Address: Rodrigo San-Cristobal, J. Alfredo Martinez, Cardiometabolic Nutrition Group, Precision Nutrition and Cardiometabolic Health Program, IMDEA Food, CEI UAM + CSIC, Madrid, Spain