
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Nutr. , 30 June 2021
Sec. Nutrition and Metabolism
Volume 8 - 2021 | https://doi.org/10.3389/fnut.2021.637267
This article is part of the Research Topic What Level of Added or Free Sugar Is Commensurate with Good Health Outcomes? View all 12 articles
 Lisa Te Morenga1,2,3*
Lisa Te Morenga1,2,3* Devonia Kruimer1,2
Devonia Kruimer1,2 Rachael McLean3,4
Rachael McLean3,4 Amandine J. M. Sabadel5
Amandine J. M. Sabadel5 Robert van Hale5
Robert van Hale5 Xavier Tatin6Jennié Harre Hindmarsh7Jim Mann1,2,3,8
Xavier Tatin6Jennié Harre Hindmarsh7Jim Mann1,2,3,8 Tony Merriman3,9
Tony Merriman3,9Determining the extent to which added sugars intake contribute to non-communicable disease in various populations is challenging because it is difficult to accurately measure intakes. Biomarkers may provide a reliable and easily measured method of assessing intakes. In a predominantly Māori population we compared various sugars intake estimates derived from a 36 item sugar-specific food frequency questionnaire (FFQ) with biomarkers of sugars intake; urinary sugars excretion in random spot collections (n = 153) and carbon stable isotope ratios (n = 36) in red blood cells (RBCs, δ13CRBC) and in the alanine fraction of the RBCs (δ13Calanine). Estimated 24 h urinary sucrose+fructose excretion was statistically significantly correlated with intakes of total sugars (r = 0.23), sucrose (r = 0.26) and added sugars from sugar-sweetened beverages (SSBs; r = 0.26). δ13Calanine was correlated with added sugars (r = 0.40). In log linear multiple regression models adjusted with HbA1C and eGFR δ13Calanine predicted added sugars intakes (r2 = 0.29) and estimated 24 h urinary sucrose+fructose excretion predicted intakes of total sugars (r2 = 0.14), sucrose (r2 = 0.17), added sugars (r2 = 0.17) and sugars from SSBs (r2 = 0.14). These biomarkers have potential for improving assessment of sugars intake in New Zealand populations enabling monitoring of the effectiveness of sugar reduction strategies designed to reduce risk of NCDs. However, further validation is required to confirm these preliminary findings.
Sugars added to the diet are often referred to as added sugars or free sugars. Added sugars are defined as “all monosaccharides and disaccharides added by manufacturer, cook or consumer to sweeten foods or drinks including, sucrose, glucose, honey, syrups, but excludes fruit juices and fruit concentrates. Free sugars include added sugars plus fruit juices and fruit juice concentrates.” (1). There is widespread consensus that intakes of added or free sugars should be limited to <10% of total energy intake (1–3) based on evidence that high intakes contribute to excess weight gain (4) and dental caries (5), and are associated with increased risk of non-communicable diseases including type 2 diabetes (6) and cardiovascular disease (CVD) (7, 8). Māori are disproportionally affected by obesity, diabetes and CVD. While socioeconomic factors are major determinants (9), it is likely that excess consumption of added sugars in sugar-sweetened drinks and processed foods contribute to this disease burden. However, determining the extent to which added sugars contribute to disease in various populations is challenging because it is difficult to accurately measure intakes. Dietary assessment at a population level is still largely dependent on self-report methods such as 24 h diet recalls or food frequency questionnaires which are subject to reporting biases (10). Previous research has shown that self-reported intakes of sugars are particularly prone to misreporting (11). Biomarkers of dietary sugars intake may provide an alternative and more reliable method of assessing intakes. This will improve our understanding of the contribution of added sugars intakes to non-communicable diseases in different population groups and our ability to monitor the effectiveness of strategies to reduce added sugars intakes.
Two promising biomarkers of sugars intake have been identified, and validation studies of these biomarkers have developed regression equations to enable these measures to be converted into estimates of sugars intakes (12, 13). The first predictive biomarker assessed sugars excreted in 24-h urine samples. Results from controlled-feeding studies showed that 24-h urinary excretion of fructose and sucrose provided a valid method of measuring intake of total sugars in controlled-feeding studies (13–15), findings supported in cross-sectional studies (16). Applied in the Norfolk cohort of the European Prospective Investigation into Cancer and Nutrition (EPIC), sugars concentrations in spot urine collections were associated with the development of obesity (17, 18). Twenty-four hour urinary fructose excretion has also been used to a limited extent in studies of children, showing moderate correlations between the biomarker and dietary sugars intake assessed by 3 day weighed food records (19).
The second biomarker of sugars intake are carbon stable isotope ratios (13C/12C ratio expressed as δ13C) measured in various tissues. The δ13C composition of foods reflects the isotope composition of the plant and animals it originates from (20) and the δ13C composition of corn- and cane-derived sugars is distinctive from other foods and sweeteners. Since humans are unable to change the δ13C composition of their tissues, the δ13C in various tissues may reflect the level of consumption of sweetened foods and drinks (21) In studies conducted in the USA δ13C values were shown to be moderately correlated with intakes of sweeteners derived from corn and cane in cross-sectional analyses in tissues including whole blood (22–24), serum (25–27), plasma (25, 28), red blood cells (RBCs) (12, 29–31) and hair (24, 29, 32). Precision may be further improved by two different approaches. The first involves measuring the δ13C in the alanine component of the target tissue (29). Such measurements are more complex and time consuming but have increased specificity for sugars intake because alanine is directly involved in sugars metabolism via the Cahill cycle, a shuttle of carbon between plasma glucose and alanine (33). Up to ~60% of alanine in blood tissues is estimated to originate from intake of dietary sugars. The second approach takes into account that dietary proteins from meat and fish are also an important source of 13C, and could confound the association between δ13C and sugars intake (31, 34). Nitrogen stable isotope ratios (15N/14N; expressed as δ15N) are increased with intakes of fish and meat but not with consumption of cane and corn-derived sugars. Therefore, a dual isotope model, using δ13C with inclusion of δ15N, has been proposed to control for these confounding dietary effects (12, 30, 31).
In the USA, sugars added to foods are commonly derived from sugar cane, corn and sugar beet (35) with only cane and corn sugars being isotopically distinct from all other plant-derived sweeteners. In contrast, the main sweetener used in foods and drinks commonly available in New Zealand is derived from sugar cane. Thus, δ13C is a promising biomarker for assessing sugars in New Zealand populations. To date no research has been published on the comparative performance of the urinary sugars excretion and δ13C as biomarkers for sugars intake in populations like New Zealand where cane sugars predominate.
The ongoing Gout and Related Conditions in Tairāwhiti: Genes and Environment Study is examining the genetic relationship between gout and other metabolic diseases such as type 2 diabetes and heart disease and the role environmental factors play in combination with the predisposing genetic factors. As part of this broader study we compared three biomarkers of sugars intake, urinary sugars excretion in random spot collections, carbon stable isotope ratios in red blood cells, and carbon stable isotope ratios in red blood cell alanine against sugars estimates derived from a culturally-appropriate validated semi-quantitative food frequency questionnaire (FFQ) in a predominantly Māori population.
This cross-sectional study recruited a total of 175 participants aged 16 years and over, with and without gout, who were able to give written consent. Participants were recruited via the patients register of Ngāti Porou Hauora Charitable Trust (NPH), the Māori primary health organization (PHO) and health care provider for all in the Ngāti Porou rohe (tribal territory) on the largely rural East Coast area of the Tairāwhiti/Gisborne region in the North Island of New Zealand. Potential participants were either contacted by the research nurse via telephone or mail or approached in person at NPH health centres at Tawhiti, Ruatoria, Tokomaru Bay, Matakaoa, Uawa, and Puhi Kaiti (Gisborne). Further participants were recruited at community centres and through community groups, events and by word of mouth. The study protocol, risks and benefits were explained to each subject and written consent was given. The study was approved by the University of Otago Human Ethics Committee (13/117). The study was overseen by the NPH Research Coordinator Dr. Harré Hindmarsh, and the research team was advised by the NPH Gout and Related Conditions Research Advisory Group, chaired by Research Coordinator and consisting of a NPH general practitioner, nurse, manager, two community representatives, Professor Merriman, and the research nurse (study recruiter).
Data collection took place between November 2013 and March 2015. To reduce attrition rates, data were collected at a time and location convenient to the participant, usually during daytime working hours and either at local health clinics or in the participants' homes.
Participants completed a sugars-specific FFQ in the presence of the research nurse who was able to provide clarification of questions if necessary. Two 10 ml urine specimen collection containers were provided to the participants for a spot urine collection at the clinic appointment. One container was for analyses of urinary creatinine and urate. The other for urinary sugars analyses and contained 30 mg boric acid as a preservative. Four blood samples were collected in two serum separator vacutainers, for serum analysis, and two vacutainers containing EDTA (an anticoagulant for blood samples) for analysis of plasma and RBCs. A general questionnaire was administered by the research nurse, registered and trained in rural health care, to elicit information on variables including age; sex; educational attainment; employment status; smoking habits; previous diagnosis of metabolic disorders; medical therapies including uric acid-lowering medication, cholesterol lowering medications, diuretics and other antihypertensive medication; family history of gout and diabetes; alcohol and seafood consumption; and physical activity level. Height (m), weight (kg), and waist circumference (cm) were also measured by the research nurse. Missing data were obtained from patient medical records with participant permission.
Participants completed a 34-item, semi-quantitative FFQ to assess sugars intake over the past month, which was developed and validated previously in this Māori community (36). Usual daily intakes of total available sugars; added sugars; added sugars in sugar-sweetened beverages; and sugars from fruits were calculated via a pre-developed spreadsheet estimated using Kaiculator© 2013 analysis software and New Zealand food composition data [2010 NZ FOODfiles; (37)].
The FFQ was validated is a previous study conducted by Masters of Dietetics students. Cross-classification agreement of sugars intake quartiles from FFQ and repeated 24-h recalls in 72 participants showed that 95–97% of participants were classified into the same or adjacent quartiles, with weighted kappa values (Kw) ranging from 0.43 to 0.51, which suggests a moderate agreement between the two dietary assessment techniques (36). Correlation coefficients between the FFQ and repeated 24-h recalls ranged from 0.59 for total fructose intake, to 0.76 for total sugars from SSBs intakes.
Sugars intakes were defined six ways using data collected from the FFQ:
1. Total sugars: the sum of all sugars from all foods and beverages
2. Sucrose: the sum of sucrose from all foods and beverages.
3. Added sugars: the sum of all sugars minus lactose derived from beverages except 100% fruit juice, the sum of glucose, fructose and sucrose from dairy foods and total sugars in breakfast cereals, iceblocks, cakes, biscuits, confectionary and chocolate.
4. Added sugars from sugar-sweetened beverages (SSBs): the sum of total of fructose, glucose and sucrose from all beverages including fruit juices and alcoholic beverages.
5. Total sugars from sweetened foods (all food items in which sugars are added as a sweetener)
6. Totals sugars from all fresh raw fruit items.
For serum analyses (lipids, urate, creatinine) blood samples were centrifuged in the field for 15 min at 3,000 rpm at 4°C. The samples were couriered to Dunedin and analysed by Southern Community Laboratories (SLC), an accredited diagnostic laboratory. Haemoglobin A1C (HbA1C) was obtained from whole blood using ion-exchange HPLC (BioRad D-10™, Haemoglobin A1C Program) at TLab, Gisborne. After analysis, the remaining blood sample was centrifuged and RBCs were washed twice with a saline solution (0.9 g sodium chloride (NaCl) with 100 mL deionised water) before transport to the Department of Human Nutrition at the University of Otago in Dunedin at 0°C and after arrival transferred to −20°C until analysis. Serum creatinine was measured by SCL using the 'Roche Cobas 8000 system. Estimated glomerular filtration rate (eGFR) was calculated using the Modification of Diet in Renal Disease formula (38).
Urine samples were preserved by adding boric acid (30 mg). Urine samples were returned to the Department of Biochemistry at the University of Otago in Dunedin at room temperature. They were then temporarily stored (<2 days) at 4°C and transferred to long-term storage at −20°C in the Department of Human Nutrition laboratories until analysis. Spot urine collections samples were defrosted at room temperature for analysis. Urinary sucrose, fructose and glucose concentrations were estimated using spectrophotometry with an enzymatic kit (K-SUFRG, Megazyme International Ireland). The UV-method is based on the determination of D-glucose before and after hydrolysis of sucrose by β-fructosidase. D-fructose was determined after isomerization by phosphoglucose isomerase. The smallest differentiating absorbance for the assay is 0.010 absorbance units, corresponding to a concentration of 0.69 mg/L of glucose, fructose or sucrose. The initial protocol was modified to run on a microplate reader in 96-well plates. Each run included fructose, glucose and sucrose standards (50, 100, 200, 300, and 400 mg/L) and samples were measured in duplicates (R2 for the standard curve was 0.999 for fructose and 0.999 for sucrose for each of the plates measured). When the coefficient of variance (CV%) was more than 10%, samples were re-analysed. Urinary creatinine concentrations were measured using a Roche Modular P (Hitachi) analyser by SLC.
We estimated 24 h urinary excretion of the sum of sucrose and fructose from spot urine samples by creatinine adjustment with spot urinary creatinine concentration using the following formula:
where 24 h creatinine was assumed to be 1.7 and 1.0 g for males and females, respectively.
Stable isotope ratios were determined in a convenience sub-sample (the final 36 participants recruited for the study, and from whom we had RBCs) to pilot test the suitability of the method for assessing sugars intakes in New Zealand population. Bulk carbon (δ13CRBC) and nitrogen (δ15NRBC – measured to adjust for potential confounding by meat and fish intakes) isotopic compositions were determined on ~0.8 mg of freeze-dried RBCs, weighed into tin capsules. δ13CRBC and δ15NRBC were determined by combustion in a NA 1500 Elemental Analyser (CE Instruments, Milan), and measurement of the resulting CO2 or N2 gases (respectively) by a Thermo Finnigan Delta Advantage Isotopic Ratio Mass Spectrometer (EA-IRMS) at the Isotrace lab facility (Dunedin, New Zealand). The conventional method of expressing δ13C or δ15N at natural abundance is in per mil (‰) abundance of 13C or 15N relative to an international standard (Vienna PeeDee Belemnite, VPDB or atmospheric N2, respectively), as follows:
The instrument precision was 0.2‰ for C and 0.2‰ for N, based on multiple measurements of laboratory control material (EDTA). Data were calibrated to the international scales using triplicate measurements of two reference materials (USGS41 and 41) run with each batch of samples.
Stable carbon isotope ratios of alanine in RBCs (δ13Calanine) were determined after extraction and derivatization of alanine using adapted protocols (39, 40). In brief, aliquots of 50 μL RBCs and 50 μL of internal standard were pipetted into a Kimax tube. Samples were hydrolysed with 1 mL 6 M HCl. The tube was then filled with N2, sealed (to prevent drying while heated), shaken, and heated at 150°C for 70 min. Samples were cooled down to room temperature, and centrifuged at 3,000 rpm for 7 min. The supernatant was transferred into a clean Kimax© tube and evaporated to dryness at 60°C in a heating block under a gentle stream of N2. Alanine was then derivatised following the protocol by Styring et al. (41). δ13Calanine was measured by gas-chromatography combustion isotope-ratio mass-spectrometer (GC-IRMS), using a Thermo Trace gas chromatograph, the GC-IsoLink combustion interface, and a Delta-XP isotope ratio mass spectrometer (Thermo Fisher Scientific). Two hundred nanoliters aliquots of derivitised alanine were injected at 270°C in splitless mode, carried by helium at 1.4 mL min−1 and separated on a VF-35 ms column (0.32 mm ID and a 1.0 μm film thickness). The oxidation reactor was set at 950°C and the reduction reactor was left at room temperature. Samples were analysed in duplicate along with amino acid laboratory standards of known isotopic composition (measured on EA-IRMS). Raw deltas or chromatographic peaks are measured against a CO2 monitoring gas and corrected to PDB with an internal standard of caffeine (δ13C = −26.98‰) (42). Derivatised δ13Calanine was corrected relative to the δ13Calanine of the laboratory standard to account for the exogenous C and kinetic fractionation introduced during derivatisation (42).
All statistical analyses were performed using Stata/IC 14.2 for Mac (StataCorp, College Station, TX, USA). Descriptive data are presented as the mean and standard deviation (SD) unless specified otherwise. Sugars variables were log transformed to account for skewness in correlation and regression analyses. δ13CRBC and δ13Calanine variables were inversed (since the values are expressed as negatives) and then log transformed.
Partial correlation coefficients were calculated for the associations between the six definitions of sugars intakes (described above) as a continuous variable and the additive inverse of δ13CRBC and additive inverse of δ13Calanine. Because the FFQ was designed to rank sugars intakes by quartiles rather than to provide validated estimates of actual intake 2 participants reported very high sugars intake values (e.g., >9 kg/d) therefore intakes were censored at 500 g/d. δ15NRBC was included as the control variable to account for the effect of meat and fish intake on δ13C values.Partial correlation coefficients were also calculated for the associations between 24 h urinary sucrose + fructose and the additive inverses of δ13CRBC and δ13Calanine with δ15NRBC included as the control variable. Finally correlation coefficients were calculated for the associations between 24 h urinary sucrose+fructose and sugars intakes.
Log linear multiple regression models were used to determine whether the three sugars intake biomarkers could predict the various measures of dietary sugars intakes. Single variable regression analyses were conducted to test for an association between sugars intake measures and each biomarker. Stepwise regression was used to identify whether covariates for δ15NRBC, age, sex, BMI, HbA1c and EGFR should be included in multivariate log regression models, up to a maximum of two covariates for the carbon stable isotope models and four covariates for the 24 h urinary sucrose + fructose model with p < 0.1. EGFR and HbA1C were selected to account for potentially abnormal urinary sugars excretion in people with impaired glycaemic control. We also tested the associations between the three biomarkers with regression analyses.
The study included 175 participants of whom 122 had a previous diagnosis of gout. Table 1 describes the participant characteristics. The mean (SD) age of the group was 60 (15) years and mean BMI was 35.2 (9.7) kg/m2 (Table 1). Seventy-three percent were obese (BMI >30 kg/m2). Eighteen percent of participants had hypertension stage 2 (systolic blood pressure ≥145 or diastolic blood pressure ≥90 mm Hg), 79% had high total cholesterol (>4 mmol/L), 32% had impaired glucose tolerance [HbA1C between 40 and 50 mmol/mol; (43)] and 18% had HbA1C above 50 mmol/mol, consistent with a diagnosis of diabetes (43), indicating a high level of comorbidities in the population. There were no statistically significant differences in variables between the complete sample population and the RBC subset (n = 36).
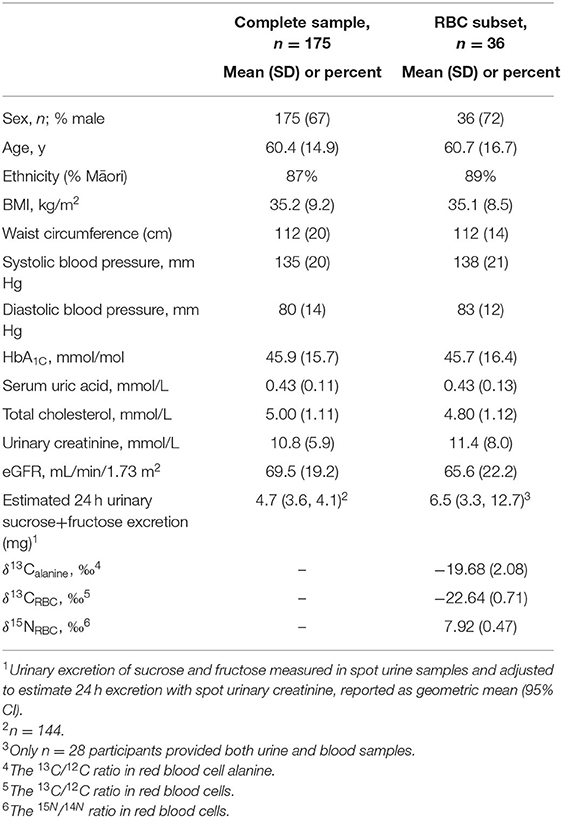
Table 1. Characteristics of study participants of the complete sample and the subset of participants with red blood cell samples.
Sugars intakes estimated by the food frequency questionnaire for six definitions for sugars are provided in Table 2. Extreme values reported by 2 individuals were truncated to a maximum value of 500g/day. Spot urine samples were available for 150 of the 175 participants recruited for the study and urinary creatinine was available for 144 of these. Excretion of estimated 24 h urinary sucrose + fructose was statistically significantly correlated with self-reported intakes of sucrose, added sugars, total sugars from SSBs and total sugars (p = 0.051) (Figure 1).
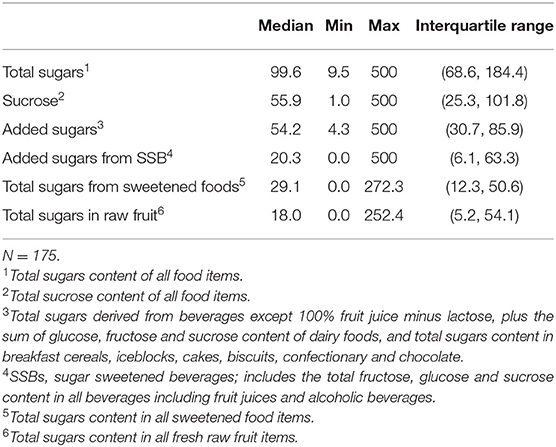
Table 2. Sugars intakes reported by six definitions estimated from a 36 item food frequency questionnaire (g/day).
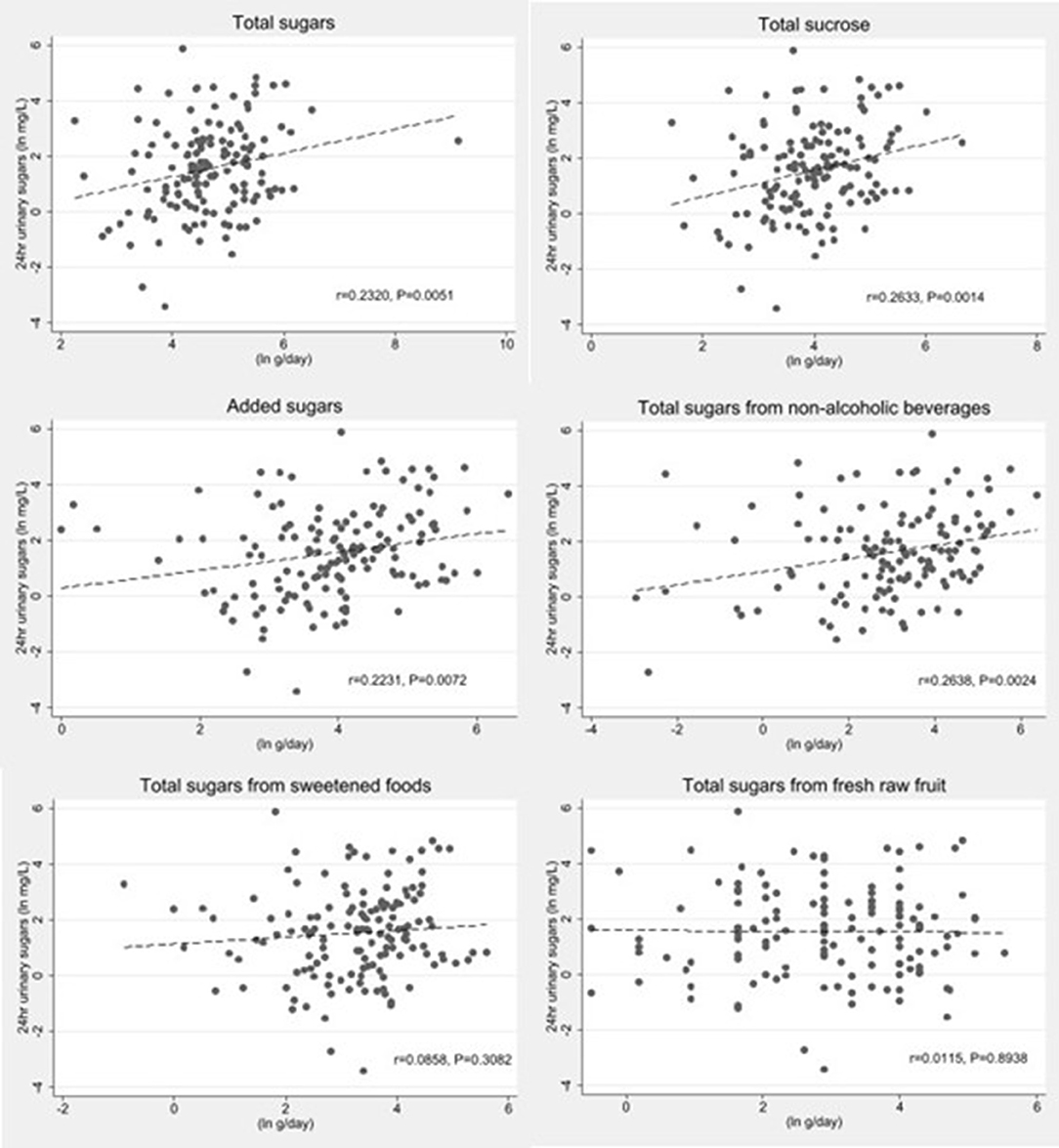
Figure 1. Scatter plots of log transformed estimated 24 h urinary sucrose+fructose excretion by log transformed sugars intakes estimated by a sugar specific FFQ (n = 140). The dashes lines represent the linear fit models.
We conducted isotope analyses on RBCs from a subsample of 36 participants. δ13CRBC correlated with δ15NRBC (r = 0.348, p = 0.038) but not with δ13Calanine (r = 0.012, p = 0.948). δ13Calanine correlated with intakes of total added sugars after controlling for δ15NRBC but not for any other definitions of sugar intakes (Figure 2). δ13CRBC was not correlated with any sugars intake variables. Estimated 24 h urinary sugars excretion correlated with δ13CRBC (r = 0.41; p = 0.0385) but did not correlate with δ13Calanine (r = 0.07; p = 0.7275) after controlling for δ15NRBC. Correlation coefficients between sugars intake variables and biomarkers are presented in Table 3.
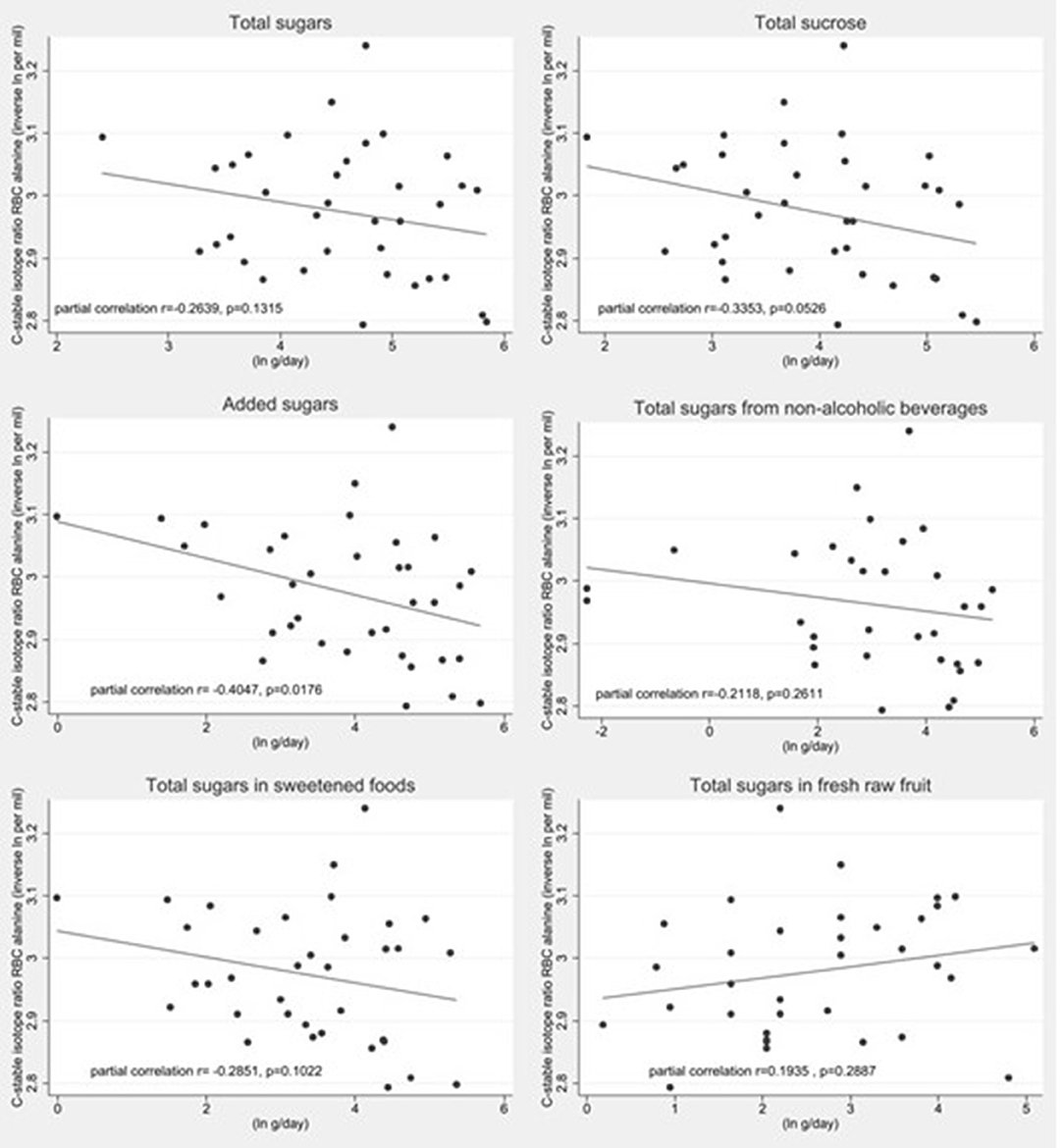
Figure 2. Scatter plots of the log transformed additive inverse δ13Calanine values by log transformed sugars intake estimates estimated by a sugar specific FFQ (n = 36). The dashed represents the linear fit model. Partial correlation values after controlling for δ15NRBC are presented within each plot.
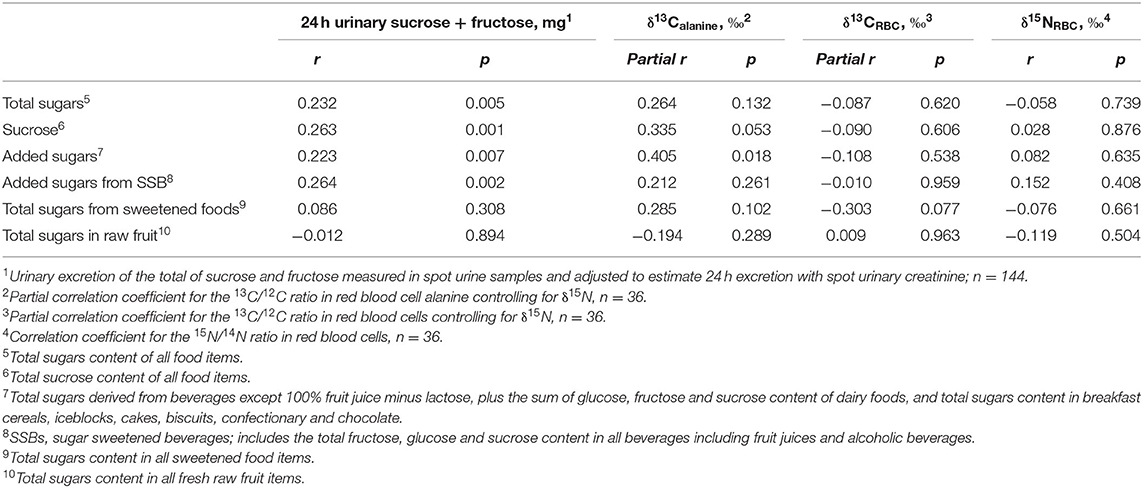
Table 3. Correlation coefficients between dietary sugars intakes estimated by food frequency questionnaire (g/d) and biomarkers for sugars intake from spot urinesamples and red blood cells.
Unadjusted, single variable, log regression analyses showed a significant association between estimated 24 h urinary sucrose + fructose excretion and total sugars (p = 0.002), sucrose (p = 0.001), added sugars (p = 0.007) and sugars in SSBs (p = 0.003). There was also a statistically significant association between δ13Calanine and added sugars (P = 0.025) and sucrose at the 90% confidence level (P = 0.08). There were no statistically significant associations between δ13CRBC or δ15NRBC and any sugars intake variables. There was a significant association between δ13CRBC and 24 h urinary sucrose+fructose excretion (p = 0.049).
In multivariate log linear regression analyses including HbA1C and eGFR as covariates, estimated 24 h urinary sucrose + fructose excretion was a significant predictor of intakes of total sugars, sucrose, added sugars and sugars in SSBs (Table 4). The best predictive model was between 24 h urinary sucrose+fructose excretion and sucrose (p < 0.001) with the model explaining 17.4% of the variation in sucrose intake. For each 1% increase in 24 h urinary sucrose+fructose there was a 0.17% increase in sucrose intake (P < 0.0001).
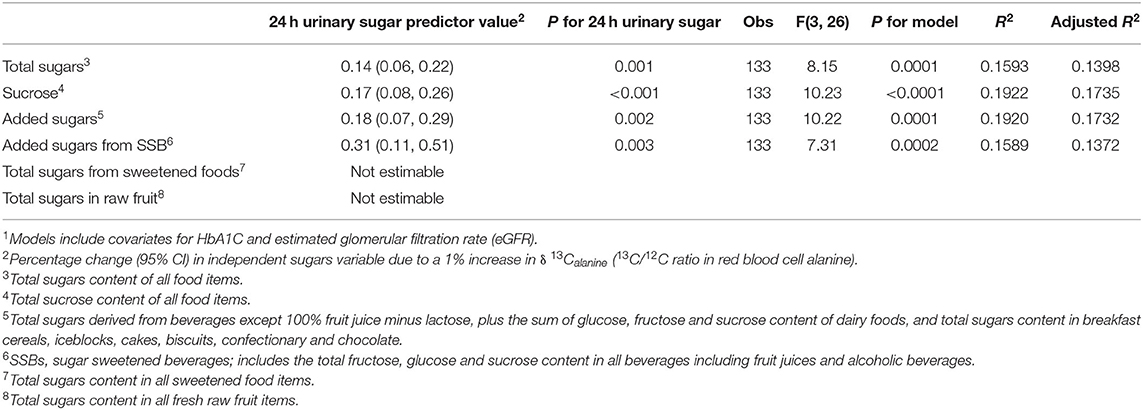
Table 4. Associations between dietary sugars intakes (g/d) and estimated 24 h urinary sucrose+fructose excretion from a multivariate log linear regression model1.
In multivariate log linear regression analyses including HbA1C and eGFR as covariates, δ13Calanine was a significant predictor of added sugars intakes (Table 5). For each 1% increase in δ13Calanine an increase in added sugars intake of 4.9% is predicted. The adjusted model explained 28.5% of the variation in added sugars intakes estimated by the FFQ also predicted total sugars intake from sweetened foods at the 90% confidence level (p = 0.072) in the HBA1c and eGFR adjusted model which was statistically significant (p = 0.0065) explaining 30% of the variation in sugars intake. δ13CRBC did not predict sugars intakes in multivariate log regressions models (Table 6).
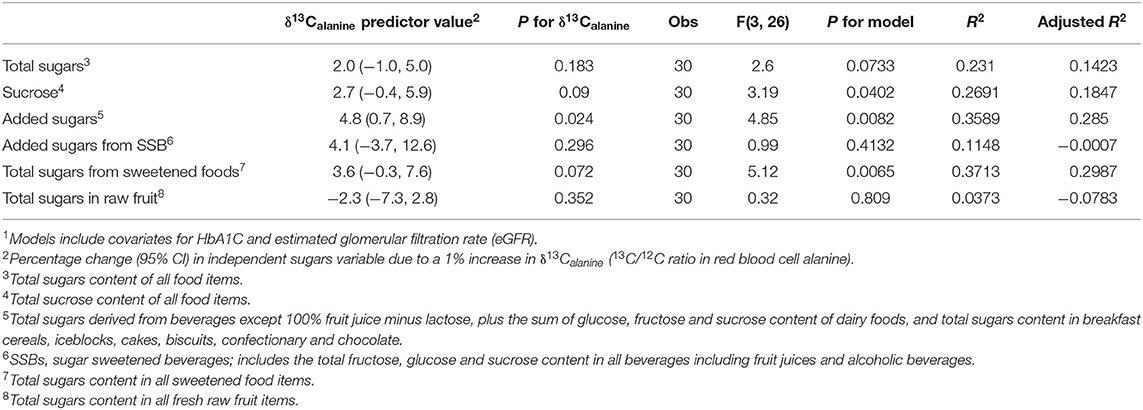
Table 5. Associations between dietary sugars intakes (g/d) and δ 13Calanine from a multivariate log linear regression model1.
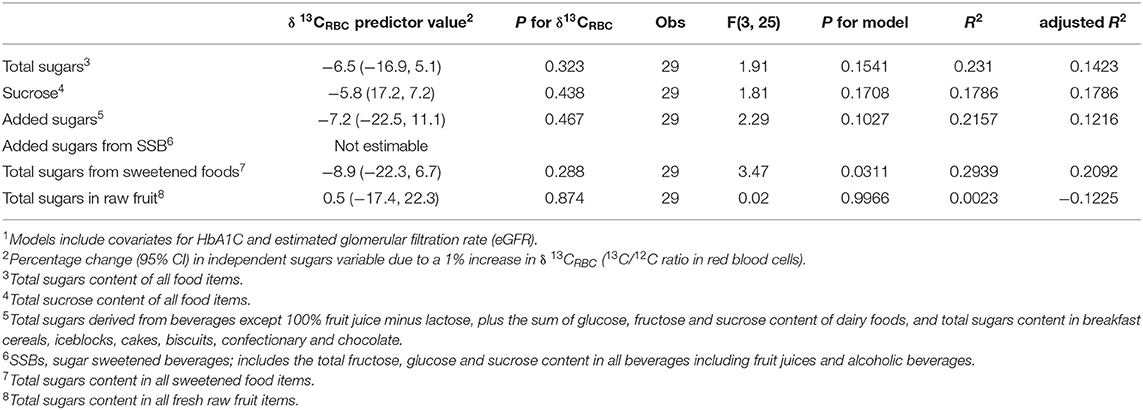
Table 6. Associations between dietary sugars intakes (g/d) and δ 13CRBC from a multivariate log linear regression model1.
The predictive equation for added sugars intake based on δ13Calanine is defined as follows:
Where δ13Calanineis measured in mg, HbA1C in mmol/mol and eGFR in mL/min/1.73 m2
This is the first study to assess the association between self-reported sugars intake and two different biomarkers of sugars intake in a population of New Zealand Māori adults; urinary sucrose and fructose excretion, δ13Calanine and δ13CRBC. We found that urinary sugars in spot urine samples were very weakly correlated with self-reported intakes of total sugars, sucrose, total added sugars and added sugars in SSBs. In the subset of the population in which we were able to conduct carbon stable isotope analyses we found that δ13Calanine in RBCs was weakly correlated with self-reported intake of added sugars after partial adjustment for δ15N to account for potential confounding by meat and fish intake. In log linear multiple regression models adjusted with HbA1C and eGFR δ13Calanine some predicted added sugars intakes and estimated 24 h urinary sucrose+fructose excretion predicted sucrose and added sugars intakes.
Several studies have shown 24 h urinary sucrose and fructose to be valid predictive biomarkers of sugars intake. In a 30 day controlled-feeding crossover study involving with 12 participants living in a metabolic unit and consuming three different diets varying in sugars content for 10 days each Tasevska et al. (13) showed a strong correlation (r = 0.89) between total sugars intake and urinary sucrose and fructose excretion measured from twelve 24 h urine collections per participant. In a study involving twelve subjects living in a metabolic unit and consuming their habitual diets for 30 days Tasevska et al. (15) found that mean daily urinary sucrose and fructose excretion was most strongly associated with intakes of extrinsic sugars (r = 0.84) compared to intrinsic sugars (r = 0.43). In contrast a recent cohort study of 477 participants in the U.S. self-reported intakes of total sugars were not associated with biomarker-predicted intakes based on single 24-h urine collections (r = −0.06) (44). The biomarker predicted intakes were calculated using the formulas developed by Tasevska and colleagues based on feeding studies in a U.K population (13), and were not adapted to a U.S. population. Different sources of sugar, i.e., beet sugars, corn-derived sugars or cane-derived sugars, in the two countries may explain the inconsistent findings.
In our study urinary sugars excretion was assessed using random spot urine collections rather than 24 h urine to reduce respondent burden and we used a sugar specific limited item FFQ that was designed to rank sugar intakes rather to assess actual intakes. More intensive and accurate dietary assessment and 24 h urine collections were not possible in this population study of older Maori adults due to limited funding and our desire to minimize participant burden. It is therefore not surprising that we found weaker correlations between measures than those demonstrated in studies by Tasevska et al. (14, 16) study where multiple days of complete urine samples were collected and analysed. Nevertheless that fact that our analyses showed that are urinary sucrose + fructose biomarker was most strongly associated with sucrose and added sugars, in which glucose and the disaccharides sucrose and fructose would predominate, strengthens our confidence that the biomarker reflects the level of sugars intakes in our population group. The first study reporting on the spot urinary excretion of sucrose and fructose, showed in nine participants in Italy, that the average urinary sucrose excretion of four timed spot urine collections (collected at 8 a.m., 10 a.m., 3 p.m., and 8 p.m.) was correlated with dietary sucrose intake (r = 0.70) (45). In a cross-sectional analysis of data from free living participants in the EPIC-Norfolk study (n = 475), sucrose intake assessed by FFQ was positively associated with urinary sucrose and fructose excretion in single spot urine samples of individuals with normal body weight (BMI <25 kg/m2) (p < 0.001). There were, however, no associations shown between urinary sucrose and fructose excretion and self-reported sucrose intake in obese participants (17). Further prospective analysis of prospective data from EPIC Norfolk participants (n = 1,734) where sucrose intake was assessed using 7-day diet diaries showed a negative association between sucrose and BMI, whereas sugar intake estimated from baseline spot urine samples was positively associated with BMI. Given that our systematic review of dietary intervention studies showed that sugars intakes are associated with weight gain (8) these findings suggest suggests that urinary excretion of sugars may be a more reliable objective measure of sugars intake than self-report methods in both obese and lean participants. Further previously reported discrepant findings [such as those reported by Bingham et al. (17)] may be due to misreporting of intakes, particularly by obese participants (18). Supporting this theory previous research by Joosen and colleagues, assessing the effect of BMI on urinary sugars excretion, showed that urinary sugars excretion is not affected by BMI (14).
Participants in our study had a high prevalence of overweight and obesity, gout, and dysglycaemia (HbA1C > 40 mmol/mol). Metabolic comorbidities may alter urinary excretion of sugars, affecting the suitability of this biomarker in this group of people. Both diabetes and hyperuricaemia are associated with chronic kidney disease (46, 47) and it is possible that urinary sugars excretion patterns are different for people with these conditions. Furthermore, the mechanism by which sucrose and fructose occurs in the urine is not well-understood (13) except in the case of glucosuria, which is a direct result of elevated blood glucose. Therefore, further research is needed to assess the validity of urinary sugars excretions as a biomarker of sugars intake in participants with metabolic comorbidities such as obesity, diabetes and gout.
Stable isotope ratios in blood have been proposed previously as a biomarker of sugars intake in the U.S. Most of this research evaluated the use of δ13C in whole blood or serum (12, 20, 22–28, 30). However, Choy et al. (29) evaluated carbon stable isotope ratios in RBC's alanine as a more precise marker of sugars intake compared to δ13CRBC (29). As high intakes of animal proteins also tend to elevate δ13C, this approach attempts to account for confounding of the association between sugar and δ13C by dietary protein (31, 34, 48). Choy et al. (29) found in a Native Alaskan population (n = 68) that RBC's δ13Calanine was strongly correlated with self-reported SSBs intake (r = 0.70), added sugars intake (r = 0.59) and total sugars intake (r = 0.57) independent of animal protein intake. Our study showed weaker but statistically significant associations between RBC δ13Calanine and added sugars, sucrose and added sugars in sweetened food in multivariate log linear regression models, but not with total sugars, and sugars from SSBs and raw fruit. While the findings are weak this likely reflects the small sample size and the limitations of our dietary assessment method. Further the lack of association with sugars definitions that included sugars from fruit and dairy sources supports the theory that δ13Calanine has promise as a marker of sugar-sweetened foods in New Zealand where cane sugar is the predominant sweetener. The lack of association, however, between RBC δ13Calanine and the urinary sugars biomarker is not unexpected at the two biomarkers measure sugars intakes over different timeframes; urinary sugars measure recent intake whereas RBC δ13Calanine is hypothesized to represent intakes over the previous months.
There are a number of limitations to our study. The primary limitation of this study was its small sample size. Urinary measures were obtained for 153 participants recruited, however we only obtained RBC samples from 36 participants for measurement of δ13Calanine and δ13CRBC as this was an initial exploratory analysis. The collection of a single spot urine sample rather than a 24 h urine sample is a major limitation as it assumes that sugars excretion is consistent throughout the day. Spot urine samples must thus be corrected for urine concentration. This is typically achieved by correction with urinary creatinine or specific gravity assuming consistent daily excretion values across a population. We corrected for urine dilution with urinary creatinine concentrations however the high level of comorbidity and obesity in our older Maori population means this assumption may not be valid. Even with correction for urine concentration spot samples are not particularly reliable and bias will attenuate the true association between urinary sugars and dietary intakes. On the other hand 24 h urine collections place a high burden on study participants, are frequently incomplete, and are challenging to collect in large population studies. Additionally dietary assessment by self-report is also affected by a high degree of reporting bias further attenuating potential associations between self-reported intakes and the biomarkers of interest. We assessed dietary intakes using a sugar-specific FFQ that had been previously validated for use among Māori in NZ as our reference method (36). FFQs are limited to a finite list of foods and are constrained by the ability of participants to accurately report their food intake retrospectively over a long period of time, and are therefore subject to reporting errors (49). Further research including controlled feeding studies, or free-living participants using dietary measures such as 7-day weighed food records is needed to further study these associations. Because our FFQ instrument was designed specifically to estimate sugars intakes we were not able to assess intakes of other sources of 13C-enriched foods such as meat and fish intake that may have confounded the associations between δ13Calanine and δ13CRBC with sugars intake. Additionally, the FFQ was not designed to distinguish between cane and corn-derived sugars and other sweeteners such as honey, maple syrup and beet sugars that are not enriched in 13C. However, consumption of these other sugar sources in New Zealand is relatively low (50) and thus is unlikely to substantially affect the association between stable isotope ratios and dietary sugars intake.
In conclusion, these results show that both urinary sugars excretion and δ13Calanine in red blood cells, but not δ13CRBC, have potential as objective biomarkers of sugars intake in the New Zealand Māori population, where added sugars in foods and beverages are derived predominantly from sugar cane. However, the weak to moderate associations shown indicate that further research is needed in other populations including groups with and without diabetes and pre-diabetes as these conditions may alter the excretion of sugars in urine and sugars metabolism. Further adequately powered research involving more precise methods of dietary assessment such as a 7-day weighed food record is needed in order to confirm these findings.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by University of Otago Human Ethics Committee (13/177). The patients/participants provided their written informed consent to participate in this study.
LT, TM, and DK conceived and designed the study. DK, AS, and XT performed the laboratory analyses. RH and AS contributed expertise and support for the isotope analyses. LT analyzed the data. JH supported the study with access to the community, and guardianship and monitoring of the data collection. LT, JM, and TM provided academic supervision. LT, TM, and JH obtained funding for the study and LT had overall responsibility for the research. LT, DK, and RM wrote the paper. All authors contributed to the article and approved the submitted version.
This research was funded by a New Zealand Lotteries Health Research Grant (326852) and the New Zealand Government funded Riddet Centre of Research Excellence. LM is supported by a Royal Society of New Zealand Rutherford Discovery Fellowship.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We would like to thank Ngāti Porou Hauora Charitable Trust and the Tairāwhiti Ngāti Porou community for enabling this research, and the study research nurse, Carol Ford.
1. World Health Organization. Guideline: Sugars Intake for Adults and Children. Geneva: World Health Organization (2015).
2. Casavale KO, Stoody EE, Rihane C, Olson R. Recommendations of the 2015–2020 dietary guidelines for Americans. FASEB J. (2016) 30:lb423. doi: 10.1096/fasebj.30.1_supplement.lb423
3. Evans CEL. Sugars and health: a review of current evidence and future policy. Proc Nutr Soc. (2017) 76:400–7. doi: 10.1017/S0029665116002846
4. Te Morenga L, Mallard S, Mann J. Dietary sugars and body weight: systematic review and meta-analyses of randomised controlled trials and cohort studies. BMJ. (2013) 345:e7492. doi: 10.1136/bmj.e7492
5. Moynihan P, Kelly S. Effect on caries of restricting sugars intake: systematic review to inform WHO guidelines. J Dent Res. (2014) 93:8–18. doi: 10.1177/0022034513508954
6. Malik VS, Popkin BM, Bray GA, Després J-P, Willett WC, Hu FB. Sugar-sweetened beverages and risk of metabolic syndrome and type 2 diabetes. Diabetes Care. (2010) 33:2477–83. doi: 10.2337/dc10-1079
7. Yang Q, Zhang Z, Gregg EW, Flanders WD, Merritt R, Hu FB. Added sugar intake and cardiovascular diseases mortality among US adults. JAMA. (2014) 174:516–24. doi: 10.1001/jamainternmed.2013.13563
8. Te Morenga LA, Howatson AJ, Jones RM, Mann J. Dietary sugars and cardiometabolic risk: systematic review and meta-analyses of randomized controlled trials of the effects on blood pressure and lipids. Am J Clin Nutr. (2014) 100:65–79. doi: 10.3945/ajcn.113.081521
9. Theodore R, McLean R, TeMorenga L. Challenges to addressing obesity for Māori in Aotearoa/New Zealand. Aust N Z J Public Health. (2015) 39:509–12. doi: 10.1111/1753-6405.12418
11. Poppitt S, Swann D, Black A, Prentice A. Assessment of selective under-reporting of food intake by both obese and non-obese women in a metabolic facility. Int J Obes Relat Metab Disord. (1998) 22:303–11. doi: 10.1038/sj.ijo.0800584
12. Nash SH, Kristal AR, Bersamin A, Hopkins SE, Boyer BB, O'Brien DM. Carbon and nitrogen stable isotope ratios predict intake of sweeteners in a Yup'ik Study Population. J Nutr. (2013) 143:161–5. doi: 10.3945/jn.112.169425
13. Tasevska N, Runswick SA, McTaggart A, Bingham SA. Urinary sucrose and fructose as biomarkers for sugar consumption. Cancer Epidemiol Biomarkers Prev. (2005) 14:1287–94. doi: 10.1158/1055-9965.EPI-04-0827
14. Joosen A, Kuhnle G, Runswick S, Bingham S. Urinary sucrose and fructose as biomarkers of sugar consumption: comparison of normal weight and obese volunteers. Int J Obes. (2008) 32:1736–40. doi: 10.1038/ijo.2008.145
15. Tasevska N, Runswick S, Welch A, McTaggart A, Bingham S. Urinary sugars biomarker relates better to extrinsic than to intrinsic sugars intake in a metabolic study with volunteers consuming their normal diet. Eur J Clin Nutr. (2008) 63:653–9. doi: 10.1038/ejcn.2008.21
16. Song X, Navarro SL, Diep P, Thomas WK, Razmpoosh EC, Schwarz Y, et al. Comparison and validation of 2 analytical methods for measurement of urinary sucrose and fructose excretion. Nutr Res. (2013) 33:696–703. doi: 10.1016/j.nutres.2013.05.017
17. Bingham S, Luben R, Welch A, Tasevska N, Wareham N, Khaw KT. Epidemiologic assessment of sugars consumption using biomarkers: comparisons of obese and nonobese individuals in the European prospective investigation of cancer Norfolk. Cancer Epidemiol Biomarkers Prev. (2007) 16:1651–4. doi: 10.1158/1055-9965.EPI-06-1050
18. Kuhnle GG, Tasevska N, Lentjes MA, Griffin JL, Sims MA, Richardson L, et al. Association between sucrose intake and risk of overweight and obesity in a prospective sub-cohort of the European Prospective Investigation into Cancer in Norfolk (EPIC-Norfolk). Public Health Nutr. (2015) 18:2815–24. doi: 10.1017/S1368980015000300
19. Johner SA, Libuda L, Shi L, Retzlaff A, Joslowski G, Remer T. Urinary fructose: a potential biomarker for dietary fructose intake in children. Eur J Clin Nutr. (2010) 64:1365–70. doi: 10.1038/ejcn.2010.160
20. Jahren AH, Saudek C, Yeung EH, Kao WL, Kraft RA, Caballero B. An isotopic method for quantifying sweeteners derived from corn and sugar cane. Am J Clin Nutr. (2006) 84:1380–4. doi: 10.1093/ajcn/84.6.1380
21. O'Brien DM. Stable isotope ratios as biomarkers of diet for health research. Annu Rev Nutr. (2015) 35:565–94. doi: 10.1146/annurev-nutr-071714-034511
22. Davy BM, Jahren AH, Hedrick VE, Comber DL. Association of δ13 C in fingerstick blood with added-sugar and sugar-sweetened beverage intake. J Am Diet Assoc. (2011) 111:874–8. doi: 10.1016/j.jada.2011.03.019
23. Hedrick VE, Davy BM, Wilburn GA, Jahren AH, Zoellner JM. Evaluation of a novel biomarker of added sugar intake (δ 13 C) compared with self-reported added sugar intake and the Healthy Eating Index-2010 in a community-based, rural US sample. Public Health Nutr. (2016) 19:429–36. doi: 10.1017/S136898001500107X
24. Hedrick VE, Zoellner JM, Jahren AH, Woodford NA, Bostic JN, Davy BM. A dual-carbon-and-nitrogen stable isotope ratio model is not superior to a single-carbon stable isotope ratio model for predicting added sugar intake in southwest Virginian Adults. J Nutr. (2015) 145:1362–9. doi: 10.3945/jn.115.211011
25. Cook CM, Alvig AL, Liu YQD, Schoeller DA. The natural 13C abundance of plasma glucose is a useful biomarker of recent dietary caloric sweetener intake. J Nutr. (2010) 140:333–7. doi: 10.3945/jn.109.114777
26. Fakhouri TH, Jahren AH, Appel LJ, Chen L, Alavi R, Anderson CA. Serum carbon isotope values change in adults in response to changes in sugar-sweetened beverage intake. J Nutr. (2014) 144:902–5. doi: 10.3945/jn.113.186213
27. Yeung EH, Saudek CD, Jahren AH, Kao WHL, Islas M, Kraft R, et al. Evaluation of a novel isotope biomarker for dietary consumption of sweets. Am J Epidemiol. (2010) 172:1045–52. doi: 10.1093/aje/kwq247
28. Nash SH, Kristal AR, Hopkins SE, Boyer BB, O'Brien DM. Stable isotope models of sugar intake using hair, red blood cells, and plasma, but not fasting plasma glucose, predict sugar intake in a Yup'ik Study Population. J. Nutr. (2014) 144:75–80. doi: 10.3945/jn.113.182113
29. Choy K, Nash SH, Kristal AR, Hopkins S, Boyer BB, O'Brien DM. The carbon isotope ratio of alanine in red blood cells is a new candidate biomarker of sugar-sweetened beverage intake. J Nutr. (2013) 143:878–84. doi: 10.3945/jn.112.172999
30. Nash S, Kristal A, Bersamin A, Choy K, Hopkins S, Stanhope K, et al. Isotopic estimates of sugar intake are related to chronic disease risk factors but not obesity in an Alaska native (YupÄôik) study population. Eur J Clin. Nutr. (2014) 68:91–6. doi: 10.1038/ejcn.2013.230
31. Nash SH, Bersamin A, Kristal AR, Hopkins SE, Church RS, Pasker RL, et al. Stable nitrogen and carbon isotope ratios indicate traditional and market food intake in an indigenous circumpolar population. J Nutr. (2012) 142:84–90. doi: 10.3945/jn.111.147595
32. Chi DL, Hopkins S, O'Brien D, Mancl L, Orr E, Lenaker D. Association between added sugar intake and dental caries in Yup'ik children using a novel hair biomarker. BMC Oral Health. (2015) 15:121. doi: 10.1186/s12903-015-0101-z
33. Bender DA. Energy nutrition – the metabolism of carbohydrates and fat. In: Bender DA, editors. Introduction to Nutrition and Metabolism. Boca Raton, FL: CRC Press (2014).
34. Petzke KJ, Boeing H, Klaus S, Metges CC. Carbon and nitrogen stable isotopic composition of hair protein and amino acids can be used as biomarkers for animal-derived dietary protein intake in humans. J Nutr. (2005) 135:1515–20. doi: 10.1093/jn/135.6.1515
35. Pomeranz JL. The bittersweet truth about sugar labeling regulations: they are achievable and overdue. Am J Public Health. (2012) 102:e14–20. doi: 10.2105/AJPH.2012.300732
36. Furter E. The Māori Kai Semi-Quantitative Food Frequency Questionnaire: Relative Validity and Reliability for Assessing Usual Sugar Intakes in New Zealand East Coast Māori. University of Otago (2014). Available online at: http://hdl.handle.net/10523/4662 (accessed June 14, 2021).
37. The New Zealand Institute for Plant & Food Research Limited. New Zealand Food Composition Database: New Zealand FOODfiles 2010. The New Zealand Institute for Plant & Food Research Limited and Ministry of Health (2010). Available online at: https://www.foodcomposition.co.nz/foodfiles/ (accessed June 14, 2021).
38. Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Ann Intern Med. (1999) 130:461–70. doi: 10.7326/0003-4819-130-6-199903160-00002
39. Popp BN, Graham BS, Olson RJ, Hannides CC, Lott MJ, López-Ibarra GA, et al. Insight into the trophic ecology of yellowfin tuna, Thunnus albacares, from compound-specific nitrogen isotope analysis of proteinaceous amino acids. Terrestrial Ecol. (2007) 1:173–90. doi: 10.1016/S1936-7961(07)01012-3
40. Walsh RG, He S, Yarnes CT. Compound-specific δ13C and δ15N analysis of amino acids: a rapid, chloroformate-based method for ecological studies. Rapid Commun Mass Spectrom. (2014) 28:96–108. doi: 10.1002/rcm.6761
41. Styring AK, Kuhl A, Knowles TD, Fraser RA, Bogaard A, Evershed RP. Practical considerations in the determination of compound-specific amino acid δ15N values in animal and plant tissues by gas chromatography-combustion-isotope ratio mass spectrometry, following derivatisation to their N-acetylisopropyl esters. Rapid Commun Mass Spectrom. (2012) 26:2328–34. doi: 10.1002/rcm.6322
42. Sabadel A, Woodward E, Van Hale R, Frew R. Compound-specific isotope analysis of amino acids: a tool to unravel complex symbiotic trophic relationships. Food Webs. (2016) 6:9–18. doi: 10.1016/j.fooweb.2015.12.003
43. Braatvedt G, Cundy T, Crooke M, Florkowski C, Mann JI, Lunt H, et al. Understanding the new HbA1c units for the diagnosis of Type 2 diabetes. N Z Med J. (2012) 125:70–80.
44. Beasley J, Jung M, Tasevska N, Wong W, Siega-Riz A, Sotres-Alvarez D, et al. Biomarker-predicted sugars intake compared with self-reported measures in US Hispanics/Latinos: results from the HCHS/SOL SOLNAS study. Public Health Nutr. (2016) 19:3256–64. doi: 10.1017/S1368980016001580
45. Luceri C, Caderni G, Lodovici M, Spagnesi MT, Monserrat C, Lancioni L, et al. Urinary excretion of sucrose and fructose as a predictor of sucrose intake in dietary intervention studies. Cancer Epidemiol Biomarkers Prev. (1996) 5:167–71.
46. Min T, Stephens M, Kumar P, Chudleigh R. Renal complications of diabetes. Br Med Bull. (2012) 104:113–27. doi: 10.1093/bmb/lds030
47. Bellomo G, Venanzi S, Verdura C, Saronio P, Esposito A, Timio M. Association of uric acid with change in kidney function in healthy normotensive individuals. Am J Kidney Dis. (2010) 56:264–72. doi: 10.1053/j.ajkd.2010.01.019
48. Patel PS, Cooper AJ, O'Connell TC, Kuhnle GG, Kneale CK, Mulligan AM, et al. Serum carbon and nitrogen stable isotopes as potential biomarkers of dietary intake and their relation with incident type 2 diabetes: the EPIC-Norfolk study. Am J Clin Nutr. (2014) 100:708–18. doi: 10.3945/ajcn.113.068577
Keywords: added sugars, free sugars, carbon stable isotope ratio, urinary sugars, urinary excretion, Māori, New Zealand, dietary biomarker
Citation: Te Morenga L, Kruimer D, McLean R, Sabadel AJM, van Hale R, Tatin X, Hindmarsh JH, Mann J and Merriman T (2021) Associations Between Sugars Intakes and Urinary Sugars Excretion and Carbon Stable Isotope Ratios in Red Blood Cells as Biomarkers of Sugars Intake in a Predominantly Māori Population. Front. Nutr. 8:637267. doi: 10.3389/fnut.2021.637267
Received: 03 December 2020; Accepted: 21 May 2021;
Published: 30 June 2021.
Edited by:
Anette E. Buyken, University of Paderborn, GermanyReviewed by:
Gunter Kuhnle, University of Reading, United KingdomCopyright © 2021 Te Morenga, Kruimer, McLean, Sabadel, van Hale, Tatin, Hindmarsh, Mann and Merriman. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lisa Te Morenga, bC50ZW1vcmVuZ2FAbWFzc2V5LmFjLm56
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.