 Carla Barbosa Nonino1*
Carla Barbosa Nonino1* Natália Yumi Noronha1
Natália Yumi Noronha1 Maysa de Araújo Ferreira-Julio2
Maysa de Araújo Ferreira-Julio2 Lígia Moriguchi Watanabe1
Lígia Moriguchi Watanabe1 Karen Francislaine Cassia2
Karen Francislaine Cassia2 Carolina Ferreira Nicoletti1
Carolina Ferreira Nicoletti1 Caroline Rossi Welendorf1
Caroline Rossi Welendorf1 Wilson Salgado Junior3
Wilson Salgado Junior3 Dorotéia Rossi Silva Souza2
Dorotéia Rossi Silva Souza2 Marcela Augusta de Souza Pinhel1,2
Marcela Augusta de Souza Pinhel1,2- 1Department of Health Science, Ribeirao Preto Medical School, University of São Paulo, Ribeirao Preto, Brazil
- 2Department of Molecular Biology, São José do Rio Preto Medical School, São José do Rio Preto, Brazil
- 3Department of Surgery and Anatomy, Ribeirao Preto Medical School, University of São Paulo, Ribeirao Preto, Brazil
Matrix metalloproteinases (MMP) and their endogenous inhibitor, the tissue inhibitor of metalloproteinases (TIMP), are expressed in many different cell types and play an important role in physiologic and pathological degradation of extracellular matrix (ECM). Starting from these observations and considering the activation state of peripheral blood mononuclear cells (PBMCs) in obesity, we investigated the gene expression of metalloproteinases before and after Roux-en-Y gastric bypass (RYBG). The study was performed in the Ribeirão Preto Medical School University Hospital. Seventy-three women were divided into a study group (SG), composed of 53 individuals with severe obesity before and after 6 months of RYGB, and a control group (CG), composed of 20 normal-weight individuals. Anthropometric and body composition data were collected, and peripheral blood for ribonucleic acid (RNA) extraction. The biological samples were submitted to a quantitative real-time polymerase chain reaction to evaluate the expression of MMP2 and TIMP2 genes. Alterations in weight loss, body mass index (BMI), and fat mass (FM) were observed after 6 months of RYGB (p < 0.05). A reduction of gene expression of TIMP2 was observed after 6 months of RYGB, contributing positively to the weight loss (R2 = 0.33 p = 0.04). The enrichment analyses highlighted the interaction between TIMP2 and MMP2 genes and the molecular pathways involving the ECM remodeling in the obesity condition. RYGB contributes significantly to weight loss, improved BMI, reduced FM, and reduced TIMP2 expression in PBMCs, which might contribute to the ECM remodeling in the obesity and could be useful as a circulating biomarker.
Introduction
Obesity is one of the most critical public health problems, and the prevalence has reached epidemic proportions worldwide (1, 2). According to the World Health Organization (WHO), obesity is defined as “abnormal or excessive adipose tissue accumulation that offers a risk to health” (2).
In the development of overweight and obesity, adipose tissue is changed with hypertrophic adipocytes, infiltration of macrophages, and other pro-inflammatory immune cells. Also, the occurrence of the extracellular matrix (ECM) dynamic remodeling is fundamental for the expansion of the adipose tissue to allow necessary and proper structural changes (3). In adipose tissue, ECM is composed of several components, including matrix metalloproteases (MMPs) and tissue inhibitors of metalloproteinases (TIMPs), that play an essential role in the ECM remodeling and adipose tissue function (4). The activity of MMPs is regulated by tissue inhibitors of MMPs (TIMPs), which comprise a family of four protease inhibitors: TIMP-1, -2, -3, and -4 (4). Circulating levels of TIMP-1 and -2 are increased in patients with metabolic syndrome and type 2 diabetes (T2D), while MMPs imbalance is associated with obesity and T2D (4).
In obesity management, bariatric surgery is currently the most effective obesity treatment, resulting in significant weight loss and improving whole-body metabolic function (5). One of the most common bariatric surgeries performed worldwide is Roux-en-Y gastric bypass (RYBG), which is considered a gold standard procedure due to its safety and low complication rate (6).
As obesity is a multifactorial disease, weight loss also involves several factors, including environmental, behavioral, and genetic (7). Genetic variants explain the predisposition to obesity, the facility or resistance to weight loss after interventions, as well as the maintenance of weight loss (7, 8). Thus, regardless of the strategy used for obesity control/treatment, individual response to interventions is highly variable, and inter-individual genetic variation may explain the variety of physiological responses in the same environment (9).
Gene expression in blood cells may reflect a systemic response to altered metabolism (10). Peripheral blood mononuclear cells (PBMCs), comprising lymphocytes and monocytes, play crucial roles in the immune system, and they also participate in pathological processes associated with obesity or metabolic syndrome (11). Also, different studies have suggested that the gene expression profile of PBMC reflects the visceral fat amount and may be representative of the inflammatory status in obesity (10, 12).
Thus, this brief research article aimed to evaluate whether alterations in the gene expression of matrix metalloproteinases-2 (MMP2) and tissue inhibitor of metalloproteinases 2 (TIMP2) whose regulation is altered in adipose tissue in obesity are equally manifested in PBMC, before and after RYGB, and the association of these genes with weight loss and body composition.
Methods
Study Population
This was an open, single-center, prospective study conducted at Ribeirão Preto Medical School University Hospital, University of São Paulo (HCFMRP, USP), Brazil, and enrolled participants from a mixed population (13). The inclusion criteria were being women, between 18 and 60 years of age, with a normal weight according to body mass index (BMI) for Control Group (CG), and with obesity grade III (BMI ≥ 40 kg/m2) before and 6 months after RYGB for Study Group (SG). The CG was composed of 20 participants, and SG was composed of 53 participants. All patients from SG were submitted to RYGB according to criteria established by the Brazilian Society of Bariatric and Metabolic Surgery (14) with follow-up at the bariatric surgery outpatient clinic at the HCFMRP USP. Patients who were not operated on by the standard surgical technique; patients who lost follow-up with the multidisciplinary team, pregnant women; and patients with thyroid disease, cancer, and psychiatric disorders were excluded.
All procedures followed in this study have been performed following the ethical standards as laid down in Helsinki's Declaration. The study protocol was approved by the Ethics Committee of the Ribeirão Preto Medical School at the University of São Paulo, Brazil (protocol number CAAE: 15614813.0.0000.5440). Informed consent was obtained from all individual participants.
Study Design
Clinical evaluation and interviews were conducted at the beginning of the study to obtain general information for anamnesis. Participants in CG were evaluated in a single moment, while participants in SG were evaluated in the preoperative period and 6 months after RYGB. We assessed the nutritional assessment, including anthropometric and body composition analysis. We also collected venous blood samples for genetic analysis.
Phenotypic Analysis
For anthropometric evaluation, the following indicators were used: weight (kg), height (m), BMI (kg/m2), and abdominal circumference (cm). Weight was measured with an electronic platform (Filizola, São Paulo, Brazil) scale with a precision of 0.1 kg and a maximum capacity of 300 kg. Height was measured with a vertical shaft with 0.5 cm graduation. The abdominal circumference was measured by passing an inextensible metric tape with graduation of 0.1 mm on the largest circumference. Body composition measurements, fat-free mass (FFM), and fat mass (FM) were evaluated with a Bioelectric Impedance Quantum 450 analyzer (RJL Systems, Clinton Township, USA), after 12-h fasting, with bladder empty.
Four measures were used to assess weight loss after RYGB: absolute weight loss (kg and %); percentage of excess weight loss (%EWL) [%EWL = weight loss (kg) ×100/excess weight (kg)]; and percentage of total weight loss (%TWL) [%TWL = weight loss (kg) ×100/pre-operative weight (kg)].
RNA Extraction and cDNA Synthesis
Peripheral blood was collected after 12-h fasting. Total RNA was extracted from peripheral blood mononuclear cells (PBMCs) using the previously described phenol-chloroform extraction method (15). According to manufacturer instructions, RNA was converted to cDNA using the High-Capacity cDNA Reverse Transcription Kit (Life Technologies, California, USA). Subsequently, cDNA was kept at −20°C until used for polymerase chain reaction (PCR) amplification. MMP-2 and TIMP-2 gene expression were measured by real-time quantitative reverse transcription-PCR (RT-PCR) using specific TaqMan FAM/MGB assays (Applied Biosystems, ID assay Hs01548727_m1 for MMP-2 and Hs00234278_m1 for TIMP-2). Reactions were performed in an Applied Biosystems 7500 Real-Time PCR System, directly detecting the PCR product without downstream processing. Relative quantification used the Δ-CT method, normalized to β-actin (Applied Biosystems, ID assay Hs99999903_m1) and GAPDH (Applied Biosystems, ID assay Hs99999905_m1) expression levels.
Statistical Analysis
Continuous variables were tested for normality using the Shapiro-Wilk test, and non-parametric tests were used when appropriate. Data are presented as mean and standard deviation. Analysis of variance (ANOVA) with Tukey's post hoc or Kruskal-Wallis non-parametric test was used to verify differences between groups regarding the study's clinical variables. A paired t-test or Wilcoxon test was used for comparisons between pre-and-post-RYGB. Spearman's rank correlation analysis was also applied. Statistical significance was set at p < 0.05, and all analyzes were performed using the Statistical Package for Social Science software (SPSS version 22.0).
Results
Seventy-three individuals were included in the study protocol, divided into a study group (SG), n = 53, and control group (CG), n = 20. The mean age, anthropometric characteristics, and body composition of participants are shown in Table 1. For the SG, the measurements occurred in the preoperative period and 6 months after RYGB. We also evaluated parameters of weight loss after RYGB (Table 1).
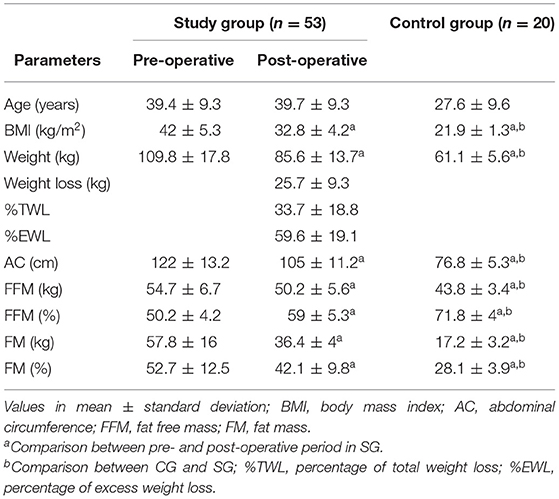
Table 1. The study group's age, anthropometric characteristics, and body composition in pre- and post-operative periods and control group.
According to BMI, in the preoperative period, patients in SG were classified with class III obesity (BMI ≥ 40 kg/m2). After the RYGB, we observed a significant weight loss of 25.7 ± 9.3 kg, which corresponded to a TWL of 33.7 ± 18.8 and 59.6 ± 19.1% of EWL and, consequently, a change in the BMI classification to overweight (BMI = 30.0–34.9 kg/m2). The body composition was also significantly different after RYGB when compared with the pre-operative period. However, while the fat mass decreased in absolute (kg) and relative (%) measurements, the absolute measurement of fat-free mass decreased, but the relative increased after body weight adjustment.
CG participants were classified with normal weight (BMI = 18.5–24.9 kg/m2) and presented a better metabolic profile according to all anthropometric and body composition parameters than SG before and after 6 months of RYGB.
Figure 1 illustrates gene expression analysis of Tissue matrix metalloproteinase-2 inhibitor (TIMP2) (Figure 1A) and Matrix metalloproteinase-2 (MMP2) (Figure 1B) of patients with obesity pre- and post-operative period in PBMC. PBMCs seem to reflect hepatic regulation of cholesterol metabolism and can migrate through the blood circulation and infiltrate various tissues such as the endothelium and adipose tissue (16). Since the present study aimed to evaluate the gene expression of metalloproteinases involved in adipose tissue remodeling, we deliberated that PBMC gene expression might reflect adipocytes' metabolic responses. Thus, we observed a decreased in the expression of TIMP2 postoperative when compared with preoperative (pre = 1.73 ± 0.9; post = 1.43 ± 0.9; p = 0.03). No differences were found for MMP2 expression postoperative (p = 0.19). We did not find differences between CG and SG, pre-and-post-RYGB in the expression of TIMP2: pre x control (p = 0.1582); post × control (p = 0.9574) and MMP2 pre × control (p = 0.5970); post × control (p = 0.6490). Logistic regression analysis indicated the expression of TIMP2 as an independent factor for absolute (kg), R2 = 0.33; p = 0.04, and relative (%), R2 = 0.32; p = 0.04) weight loss (Table 2). We did not find the relation between MMP2 expression and parameters of weight loss or body composition.
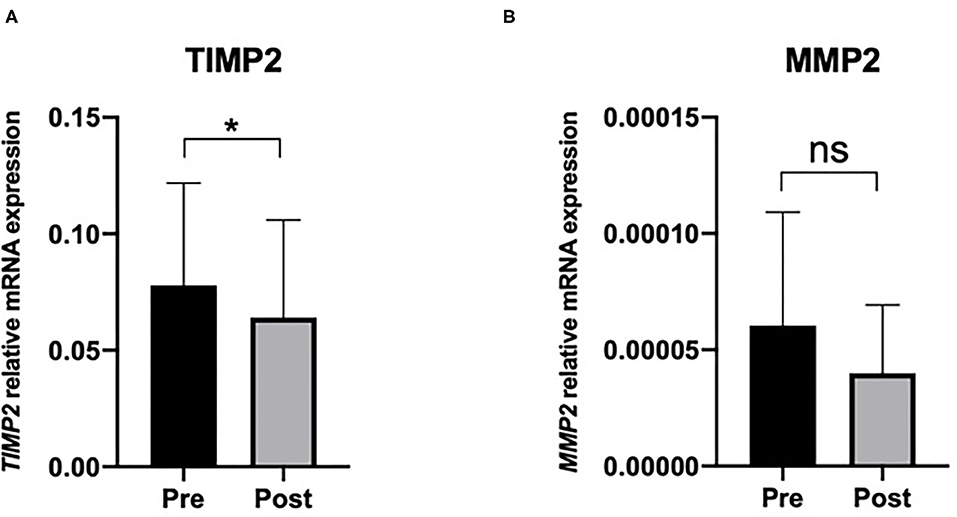
Figure 1. Peripheral blood mononuclear cells expression. Of (A) Tissue inhibitor of metalloproteinase 2 (TIMP2) and (B) Matrix metalloproteinase 2 (MMP2), relative to GAPDH/P-actin. Values are mean and standard deviation. *Wilcoxon matched-pairs signed-rank test p < 0.05. Pre, pre-operative; post, post-operative; ns, non-significant.
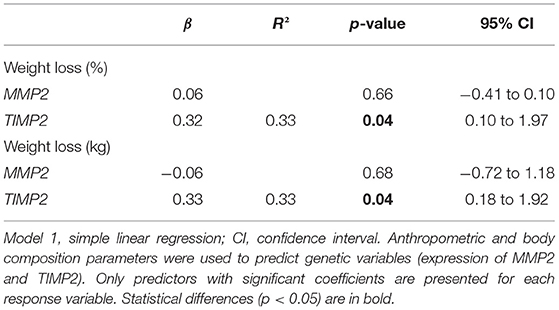
Table 2. Linear regression analysis for matrix metalloproteinase-2 (MMP2) and tissue inhibitor of metalloproteinases 2 (TIMP2) expression with Study Group participants, after RYGB.
Considering the biological role of TIMP2 as an endogenous inhibitor of MMP2, we analyzed the correlation of these genes' expression in CG and SG before and after RYGB surgery. We found a significant positive correlation between TIMP2 and MMP2 in CG (Supplementary Figure 1A). In SG, we did not find a correlation for these genes pre-RYGB (Supplementary Figure 1B), but interestingly, after RYGB, we found a positive correlation between TIMP2 and MMP2 as observed in CG (Supplementary Figure 1C).
The network's functional enrichment analysis revealed three top pathways (Supplementary Table 1) that could be related to the remodeling of adipose tissue: collagen metabolic process, extracellular matrix disassembly, and extracellular matrix organization. The primary gene ontologies (GO) revealed a co-expression network among TIMP2 and MMP2 (Figure 2), indicating that they could be functionally related and involved in a common biological process.
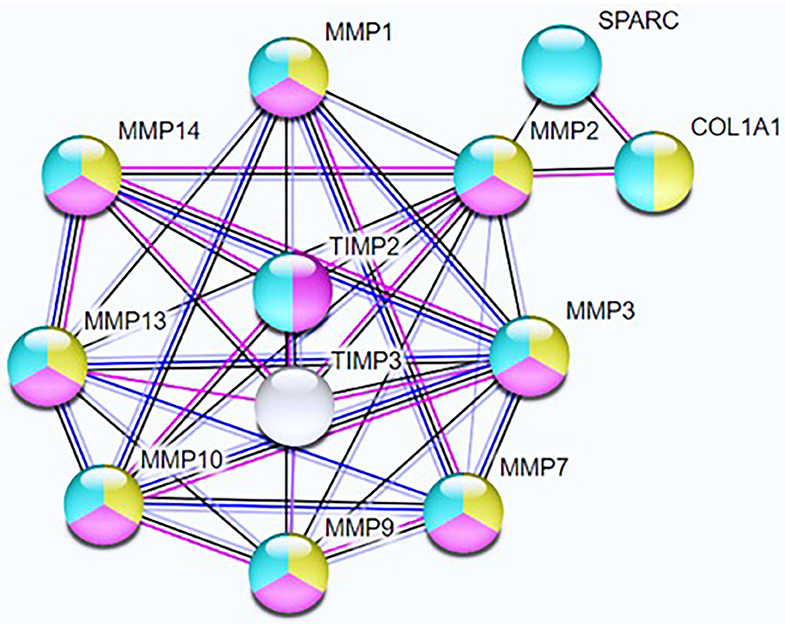
Figure 2. Network nodes represent query proteins and first shell of interactors; yellow nodes = collagen metabolic process; pink nodes = extracellular matrix disassembly; blue nodes = extracellular matrix organization. Line color indicates the type of interaction evidence; Blue lines represent gene co-occurrence, black lines represent co-expression, and pink lines represent experiment determined relations. Number of nodes = 12; number of edges = 36; average node degree = 6; average local clustering coefficient = 0.814; expected number of edges = 10; PPI enrichment p = 2.16e–10.
Discussion
In the present study, our patients had a successful weight loss after RYGB, with consequently decrease in body mass index (BMI) and fat mass (FM), evidencing one of the most noticeable effects of bariatric surgery: the loss of up to half of the total adipose tissue mass (5). Bariatric surgery is the most effective therapeutic option to reach long-term significant weight loss and improve control or even achieve remission of the associated comorbidities for severe obesity or those with BMI > 35 kg/m2 and other comorbidities (17). Weight loss is considered one of the main parameters to define bariatric surgery's success, and the criterion for this evaluation is the loss of at least 50% of the excess weight (% EWL) (17).
A balance mediates the organization of the growth and remodeling of cells to their extracellular environment between MMPs activities and concentrations of their endogenous inhibitors (18, 19). Consequently, the balance between TIMP2 and MMP2 is crucial to cellular homeostasis. In the present study, we found a positive correlation between TIMP2 and MMP2 in CG, indicating a similar expression pattern of TIMP2 and MMP2, culminating in a possible balance between these genes.
On the other side, the disruption of the MMP/TIMP balance influences the improper ECM remodeling, a process that takes place during obesity-mediated adipose tissue formation (18, 19), and influences the development of obesity and associated complications (19). Patients in SG preoperative period were classified with severe obesity according to body mass index (BMI), and under the condition of morbid obesity, we did not find a correlation between TIMP2 and MMP2 expression in PBMC. This result could indicate a possible imbalance between TIMP2 and MMP2 in these patients. Available data about MMPs in obese subjects have often shown an increase in their plasma levels and their inhibitors' erratic behavior (20). Indeed, previous studies observed a variation in the circulating levels of TIMP-1 and -2 (21) and plasma concentrations of MMP-2 and -9 (22) in patients with metabolic syndrome and T2D (4).
After 6 months of the RYGB, patients lost a significant amount of weight but still are classified with obesity according to BMI. Interestingly, we verified a positive correlation between TIMP2 and MMP2, and the expression of MMP2 did not change when compared with the preoperative period. Berg et al. (23) pointed out that the impact of bariatric surgery on MMPs is controversial. It has been reported that in morbidly obese patients, serum MMP2 and MMP9 levels significantly decrease after bariatric surgery (24). Otherwise, in obese non-diabetic patients, (25) reported an increase in collagen I and III degradations in subcutaneous AT 1 year after bariatric surgery, accompanied by increased MMP2 and MMP9 activity; however, these differences were not observed in obese diabetic patients.
On the other side, after RYGB, we observed a decreased expression of TIMP2 and a positive relation between TIMP2 and weight loss. These results could indicate that decreased TIMP2 expression in PBMC could be a marker of improvement of obesity, corroborating with Yasmeen et al. (26), in which the alteration or increase in serum levels of TIMP2 resulted in the accumulation of extracellular matrix cells, tissue fibrosis and an imbalance of metalloproteinases in the obesity condition. Moreover, the authors also observed a positive association between TIMP2 and the percentage of weight loss, abdominal circumference, and blood glucose levels. Although TIMPs are recognized as inhibitors of MMPs, several studies have revealed that these proteins may also perform biological activities distinct from their interactions with MMPs (27, 28). It is noteworthy that TIMP2 modulates the extracellular matrix in adipocyte growth and expansion during excess caloric intake (26).
The enrichment analysis confirmed the interaction between TIMP2 and MMP2 genes and their involvement in the ECM remodeling. Several lines of evidence suggest a potential role of MMPs during obesity-mediated fat mass development, especially in the control of proteolysis and adipogenesis (3). The balance between MMPs and TIMPs is a critical determinant of ECM integrity and function, and alterations in MMP/TIMP- mediated proteolysis may contribute to many pathological states, including obesity (18, 19).
In this report, MMP and TIMP expression were primarily studied at the transcript level, which does not necessarily reflect protein and activity level. However, the MMP activity study in vivo is complex because of a lack of sensitive and specific assays and the activated form. The small sample size could be a limitation. However, this limitation did not compromise the data analysis considering the potential results obtained and the limited data regarding this field in the literature.
In conclusion, RYGB outcomes included a significant weight loss with improved BMI and reduced fat mass 6 months post-procedure. Although the balance between TIMP2 and MMP2 seemed essential for ECM remodeling, we demonstrated that decreased TIMP2 expression in PBMC could be a marker of improvement of obesity after 6 months of RYGB. The enrichment analyses highlighted the interaction between TIMP2 and MMP2 genes and the molecular pathways involving the ECM remodeling in the obesity condition. In this context, elucidating ECM remodeling and obesity mechanisms may reflect in new therapeutic options and intervention pathways and diagnosis and prognosis of chronic diseases. However, further studies are needed to explore the behavior and the balance between TIMPs and MMPs in the context of bariatric surgery.
Data Availability Statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: Gene Expression Omnibus (GEO) - NCBI. Accession number: GSE83223.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics Committee of the Ribeirão Preto Medical School at the University of São Paulo, Brazil (protocol number CAAE: 15614813.0.0000.5440). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
CBN, DRSS, and MASP made conception and design research. NYN, MAFJ, KFC, CFN, and CRW conducted the research. NYN, MASP, KFC, CFN, CRW, MAFJ, WS, and LMW participated in the sample analyses and manuscript revision. CBN had primary responsibility for final content. All authors read and approved the final manuscript.
Funding
This research was supported by the São Paulo Research Foundation (FAPESP) under grants 2018/24069-3, 2018/08784-4, and 2013/12819-4. National Council for Scientific and Technological Development (CNPq) also supported this work under grant 480763/2013-5.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnut.2021.628759/full#supplementary-material
References
1. Engin A. The definition and prevalence of obesity and metabolic syndrome. Adv Exp Med Biol. (2017) 960:1–17. doi: 10.1007/978-3-319-48382-5_1
2. World Health Organization. Obesity and Overweight. (2020). Available online at: http://www.who.int/mediacentre/factsheets/fs311/en/ (accessed October 15, 2020).
3. Åkra S, Aksnes TA, Flaa A, Eggesbø HB, Opstad TB, Njerve IU, et al. Markers of remodeling subcutaneous adipose tissue are strongly associated with overweight and insulin sensitivity in healthy non-obese men. Sci Rep. (2020) 10:14055. doi: 10.1038/s41598-020-71109-4
4. Ruiz-Ojeda FJ, Mendez-Gutierrez A, Aguilera CM, Plaza-Diaz J. Extracellular matrix remodeling of adipose tissue in obesity and metabolic diseases. Int J Mol Sci. (2019) 20:4888; doi: 10.3390/ijms20194888
5. Frikke-Schmidt H, O'Rourke RW, Lumeng CN, Sandova LDA, Seeley RJ. Does bariatric surgery improve adipose tissue function? Obes Rev. (2016) 17:795–809. doi: 10.1111/obr.12429
6. Fernández-Ruiz VE, Armero-Barranco D, Xandri-Graupera JM, Paniagua-Urbano JA, Solé-Agustí M, Mulero J. Roux-en-Y Gastric Bypass. Biol Res Nurs. (2017) 19:162–9. doi: 10.1177/1099800416675406
7. Eckel RH, Grundy SC, Zimment PZ. The metabolic syndrome. Lancet. (2005) 365:1415–28. doi: 10.1016/S0140-6736(05)66378-7
8. Still CD, Wood GC, Chu X, Erdman R, Manney CH, Benotti PN, et al. High allelic burden of four obesity SNPs is associated with poorer weight loss outcomes following gastric bypass surgery. Obesity. (2011) 19:1676–83. doi: 10.1038/oby.2011.3
9. Kaput J, Rodriguez RL. Nutritional Genomics: Discovering the Path to Personalized Nutrition. Hoboken, NJ: John Wiley and Sons (2006).
10. Pinhel MAS, Noronha NY, Nicoletti CF, de Oliveira BAP, Cortes-Oliveira C, Pinhanelli VC, et al. Changes in global transcriptional profiling of women following obesity surgery bypass. Obes Surg. (2018) 28:176–86. doi: 10.1007/s11695-017-2828-x
11. Monserrat-Mesquida M, Quetglas-Llabrés M, Bouzas C, Capó X, Mateos D, Ugarriza L, et al. Peripheral blood mononuclear cells oxidative stress and plasma inflammatory biomarkers in adults with normal weight, overweight and obesity. Antioxidants. (2021) 1:813. doi: 10.3390/antiox10050813
12. Catalán V, Gómez-Ambrosi J, Rodríguez A, Ramírez B, Valentí V, Moncada R, et al. Peripheral mononuclear blood cells contribute to the obesity-associated inflammatory state independently of glycemic status: involvement of the novel proinflammatory adipokines chemerin, chitinase-3-like protein 1, lipocalin-2 and osteopontin. Genes Nutr. (2015) 10:460. doi: 10.1007/s12263-015-0460-8
13. Pena SD, Di Pietro G, Fuchshuber-Moraes M, Genro JP, Hutz MH, Kehdy Fde S, et al. The genomic ancestry of individuals from different geographical regions of Brazil is more uniform than expected. PLoS ONE. (2011) 6:e17063. doi: 10.1371/journal.pone.0017063
14. Garrido AB Jr. Cirurgia da obesidade. São Paulo: Atheneu; Sociedade Brasileira de Cirurgia Bariátrica (2002).
15. Chomczynski P, Sacchi N. Single-step method of RNA isolation by acid guanidinium thiocyanate-phenol-chloroform extraction. Anal Biochem. (1987) 162:156–9. doi: 10.1006/abio.1987.9999
16. de Mello VD, Kolehmanien M, Schwab U, Pulkkinen L, Uusitupa M. Gene expression of peripheral blood mononuclear cells as a tool in dietary intervention studies: what do we know so far? Mol Nutr Food Res. (2012) 56:1160–72. doi: 10.1002/mnfr.201100685
17. Cadena-Obando D, Ramírez-Rentería C, Ferreira-Hermosillo A, Albarrán-Sanchez A, Sosa-Eroza E, Molina-Ayala M, et al. Are there really any predictive factors for a successful weight loss after bariatric surgery? BMC Endocrine Disord. (2020) 20:20. doi: 10.1186/s12902-020-0499-4
18. Chavey C, Mari B, Monthoue LM, Bonnafous S, Anglard P, Obberghen EV, et al. Matrix metalloproteinases are differentially expressed in adipose tissue during obesity and modulate adipocyte differentiation. J Biol Chem. (2003) 278:11888–96. doi: 10.1074/jbc.M20919620
19. Sakamuri SSVP, Watts R, Takawale A, Wang X, Hernandez-Anzaldo S, Bahitham W, et al. Absence of Tissue Inhibitor of Metalloproteinase-4 (TIMP4) ameliorates high fat diet-induced obesity in mice due to defective lipid absorption. Sci Rep. (2017) 7:6210. doi: 10.1038/s41598-017-05951-4
20. Caimi G, Canino B, Montana M, Urso C, Calandrino V, Presti RL, et al. Lipid peroxidation, protein oxidation, gelatinases, and their inhibitors in a group of adults with obesity. Horm Metab Res. (2019) 51:389–95. doi: 10.1055/a-0887-2770
21. Brew K, Dinakarpandian D, Nagase H. Tissue inhibitors of metalloproteinases: evolution, structure and function. Biochim Biophys Acta. (2000) 1477:267–83. doi: 10.1016/s0167-4838(99)00279-4
22. Hopps E, Presti RL, Montana M, Noto D, Averna MR, Caimi G. Gelatinases and their tissue inhibitors in a group of subjects with metabolic syndrome. J Investig Med. (2013) 61:978–83. doi: 10.2310/JIM.0b013e318294e9da
23. Berg G, Barchuk M, Miksztowicz V. Behavior of metalloproteinases in adipose tissue, liver and arterial wall: an update of extracellular matrix remodeling. Cells. (2019) 8:158. doi: 10.3390/cells8020158
24. Domienik-Karłowicz J, Rymarczyk Z, Dzikowska-Diduch O, Lisik W, Chmura A, Demkow U, et al. Emerging markers of atherosclerosis before and after bariatric surgery. Obes Surg. (2015) 25:486–93. doi: 10.1007/s11695-014-1407-7
25. Liu Y, Aron-Wisnewsky J, Marcelin G, Genser L, Le Naour G, Torcivia A, et al. Accumulation and changes in composition of collagens in subcutaneous adipose tissue after bariatric surgery. J Clin Endocrinol Metab. (2016) 101:293–304. doi: 10.1210/jc.2015-3348
26. Yasmeen S, Khan U, Khan GM, Fatima SS. Association of tissue inhibitor of metalloproteinase 2 with non-alcoholic fatty liver disease in metabolic syndrome. Arch Physiol Biochem. (2019) 125:441–6. doi: 10.1080/13813455.2018.1481095
27. Lambert E, Dassé E, Haye B, Petitfrère E. TIMPs as multifacial proteins. Crit Rev Oncol Hematol. (2004) 49:187–98. doi: 10.1016/j.critrevonc.2003.09.008
Keywords: gene expression, metalloproteinases, MMP2 (matrix metalloproteinase-2), TIMP (tissue inhibitors of metallproteinase), bariatric surgery
Citation: Nonino CB, Noronha NY, de Araújo Ferreira-Julio M, Moriguchi Watanabe L, Cassia KF, Ferreira Nicoletti C, Rossi Welendorf C, Salgado Junior W, Rossi Silva Souza D and Augusta de Souza Pinhel M (2021) Differential Expression of MMP2 and TIMP2 in Peripheral Blood Mononuclear Cells After Roux-en-Y Gastric Bypass. Front. Nutr. 8:628759. doi: 10.3389/fnut.2021.628759
Received: 12 November 2020; Accepted: 16 September 2021;
Published: 13 October 2021.
Edited by:
Lidia Santarpia, University of Naples Federico II, ItalyReviewed by:
Anna Pryczynicz, Medical University of Bialystok, PolandSubhash K. Das, University of Alberta, Canada
Copyright © 2021 Nonino, Noronha, de Araújo Ferreira-Julio, Moriguchi Watanabe, Cassia, Ferreira Nicoletti, Rossi Welendorf, Salgado Junior, Rossi Silva Souza and Augusta de Souza Pinhel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carla Barbosa Nonino, Y2FybGFAZm1ycC51c3AuYnI=