 Zeinab Khademi1,2
Zeinab Khademi1,2 Parvane Saneei3,4Ammar Hassanzadeh-Keshteli5,6Hamed Daghaghzadeh6Hamid Tavakkoli6
Parvane Saneei3,4Ammar Hassanzadeh-Keshteli5,6Hamed Daghaghzadeh6Hamid Tavakkoli6 Peyman Adibi6
Peyman Adibi6 Ahmad Esmaillzadeh2,4,7*
Ahmad Esmaillzadeh2,4,7*- 1Students' Scientific Research Center, Tehran University of Medical Sciences, Tehran, Iran
- 2Department of Community Nutrition, School of Nutritional Sciences and Dietetics, Tehran University of Medical Sciences, Tehran, Iran
- 3Food Security Research Center, Isfahan University of Medical Sciences, Isfahan, Iran
- 4Department of Community Nutrition, School of Nutrition and Food Science, Isfahan University of Medical Sciences, Isfahan, Iran
- 5Department of Medicine, University of Alberta, Edmonton, AB, Canada
- 6Integrative Functional Gastroenterology Research Center, Isfahan University of Medical Sciences, Isfahan, Iran
- 7Obesity and Eating Habits Research Center, Endocrinology and Metabolism Molecular -Cellular Sciences Institute, Tehran University of Medical Sciences, Tehran, Iran
Background/Aim: Despite the inflammatory nature of inflammatory bowel disease (IBD), limited data are available on the association of inflammatory potential of the diet and risk of ulcerative colitis (UC). We aimed to investigate the association of inflammatory potential of the diet (IPD) score and odds of UC in a case-control study.
Methods: Patients with UC were enrolled from Iranian IBD registry, whose disease was confirmed by a gastroenterologist. Controls were selected randomly from the Study of the Epidemiology of Psycho Alimentary Health and Nutrition (SEPAHAN) study, a large population-based study on more than 8,000 apparently healthy individuals. Dietary intakes of 28 food items obtained from a validated dish-based food frequency questionnaire (FFQ), were used to compute IPD score.
Results: This case-control study was carried out among 109 cases and 218 randomly chosen controls. Mean age of cases and controls was 39.5 ± 10.0 and 41.5 ± 11.8 y, respectively. Totally, 52% of study participants were female and 48% were male. After controlling for age, sex, and body mass index (BMI), we found that the patients with UC were more likely to be in the highest quartile of IPD score compared with controls (OR: 2.83; 95% CI: 1.41–5.69, P-trend < 0.001). This association strengthened after additional adjustment for education, smoking, medical history, and physical activity (OR: 3.48; 95% CI: 1.32–9.10, P-trend = 0.003). When we took dietary habits into account, the association was slightly attenuated (OR: 3.33; 95% CI: 1.20–9.20, P-trend = 0.005).
Conclusions: We found that adherence to a pro-inflammatory diet was positively associated with greater odds of UC. Further studies are required to confirm these findings.
Introduction
Ulcerative colitis (UC), as an inflammatory bowel disease (IBD), is a multifactorial disorder characterized by chronic, relapsing, and progressive inflammatory condition (1, 2). It starts from the rectum and may involve the entire colon (3). In UC, inflammation is typically superficial and limited to the mucosa and submucosa (3, 4). According to a national survey in Iran, the prevalence of UC has been estimated to be 40.67 per 100,000 subjects (5).
Although the exact etiology is yet unknown, it seems that UC may be the result of an inappropriate and continuing inflammatory response to altered gut microbiota in a genetically susceptible host (2, 4). However, the role of environmental factors including smoking, stress, and diet cannot be ignored (2, 6, 7). Concerning the inflammatory nature of UC, dietary components can play a role in UC pathogenesis through modulation of inflammation (8, 9). For instance, adherence to Western dietary pattern, which is low in food items with anti-inflammatory and anti-oxidant proprieties, was linked to an increased risk of UC (10), while consumption of Mediterranean dietary pattern, rich in anti-inflammatory agents including fruits, vegetables, fish, and nuts, decreased the risk of UC (11).
One of the emerging indices to determine the inflammatory potential of the whole diet is dietary inflammatory index (DII). DII is a literature-derived population-based index, developed and construct validated (12–14) by Shivappa et al. (15, 16). This index has widely been used to examine the link between inflammatory potential of the diet and odds of many chronic conditions, even gastrointestinal disorders. For instance, a greater empirically derived food-based dietary inflammatory index (FDII) was associated with an increased risk of irritable bowel syndrome (IBS) in an Iranian study (17). Adherence to a pro-inflammatory diet was also related to the risk of reflux esophagitis (18). With regards to UC, we are aware of only one report in which 62 patients with UC and 124 hospitalized controls were enrolled. In that case-control study, consumption of a more pro-inflammatory diet was associated with 1.5 times greater odds of UC (19). However, a limitation of that study was the use of hospital-based controls, in whom dietary habits may differ from the general population. Additionally, some potential confounders were not considered.
Limited studies that investigated the association between diet and UC risk are conducted in western countries. Dietary patterns in western countries differ from those in Middle Eastern countries. High intakes of refined carbohydrates and saturated fatty acids and low intake of fiber are common in the Middle East. Such dietary intakes might be associated with increased risk of UC. Accordingly, assessing the relationship between diet and IBD is particularly relevant in these countries. Therefore, we conducted a case-control study that aimed to evaluate the association between inflammatory potential of the diet and risk of UC in Iran.
Materials and Methods
Study Participants
This case-control study was done between 2015 and 2019 in Isfahan, Iran. Cases were patients diagnosed with UC by a gastroenterologist that had been registered in Iranian IBD registry. Before enrolment, the study design and aims were explained to all registered patients (n = 140) during an educational class on lifestyle, then patients were requested to participate in this study. Out of these 140 patients, 109 people agreed to participate. It is noteworthy that there was no diversity concerning general characteristics including age, physical activity, and residence area between those who agreed to participate, and those who did not. Controls were randomly selected from the Study of the Epidemiology of Psycho-Alimentary Health and Nutrition (SEPAHAN) project, a large population-based study on more than 8,000 apparently healthy individuals, conducted in the same region. Detailed information about SEPAHAN project can be found elsewhere (20). Before selection of controls, all individuals with gastrointestinal disorders (including Crohn's disease, ulcerative colitis, irritable bowel syndrome, functional dyspepsia, gastro-esophageal reflux disorder) were excluded from the SEPAHAN dataset. Finally, two age- (±2 y) and sex-matched controls for each case were randomly chosen.
Assessment of Dietary Intakes
A validated self-administrated dish-based Food Frequency Questionnaire (DS-FFQ), that included 106 food items, was used to determine participants' usual dietary intakes. Further information on the design, food list, and validity of this questionnaire has been reported before (21). This questionnaire included five domains of foods and dishes (mixed dishes, potatoes and grain-based foods, dairy products, fruits and vegetables, miscellaneous foods and beverages). We asked each subject to determine his/her usual intakes of these food items in the previous year. They were able to choose one choice from nine multiple-choice options. These choices ranged from “never or less than once a month” to “12 or more times per day.” Subjects' reported intakes were then converted to grams per day, for doing that we used household measures. To calculate nutrient intakes for each person in the study, we applied the US Department of Agriculture nutrient database. However, some parts of this database were modified for Iranian local foods based on Iranian food composition table. Earlier studies on a subgroup of 200 participants indicated that this questionnaire works well in estimating long-term dietary intakes of people (21).
Construction of Inflammatory Potential of the Diet Score
The DSFFQ-derived data were used to calculate the IPD scores for all subjects. In the current study, we used the method developed by Shivappa et al. (15) to construct IPD score. The development (15) and construct validation of the DII has been described elsewhere (12, 13). Shivappa et al. (15) identified 45 specific foods or nutrients, according to published literature, that were linked with several inflammatory biomarkers: Interleukin-1β (IL-1β), Interleukin-6 (IL-6), Tumor Necrosis Factor-α (TNF-α), C-reactive protein (CRP), Interleukin-4 (IL-4), and Interleukin-10 (IL-10). Moreover, they gave each food or nutrient a specific inflammatory effect score based on its positive or negative association with inflammatory biomarkers in previous publications. If a food or nutrient was positively associated with pro-inflammatory biomarkers, the score of +1 was given to that food parameter. In case of a negative association, the food parameter was given the score of −1, and in case of null association, the score of 0 was given. They also provided world mean and standard deviations for all these 45 food items using data from 11 different countries around the world. Considering lack of consumption of some of these food items in Iranian food culture and having some missing food components (like polyphenols) in Irannian nutrient database, we included the following 28 food items (instead of 45) to calculate the IPD score: energy, carbohydrate, fat, protein, cholesterol, saturated fat, vitamin B12, and iron (pro-inflammatory items) and mono-unsaturated fatty acids (MUFA), polyunsaturated fatty acids (PUFA), fiber, vitamin B6, folic acid, niacin, riboflavin, thiamin, vitamin A, vitamin C, vitamin D, vitamin E, β-carotene, caffeine, pepper, onion, green/black tea, zinc, selenium, and magnesium (anti-inflammatory items). In present study, we calculate z-score for each food parameter by subtracting the “standard global mean” from participants' reported intake for each item and dividing this value by “global standard deviation,” which we took from the paper of Shivappa et al. (15). To reduce the skewness, all z-scores were then converted to percentiles, as earlier studies did (15). Then, we multiplied the percentile scores by the inflammatory effect score of each food parameter derived from the study of Shivappa et al. (15). Finally, we summed up all foods' IPD scores to construct the final IPD score for each participant. A greater IPD score (more positive) represents a more pro-inflammatory diet. Previous studies in Iran has shown the validity of this modified DII index against circulating levels of inflammatory biomarkers (22).
Assessment of UC
Patients with UC were identified by an experienced gastroenterologist according to international criteria (23) including physical, colonoscopic, and histological examinations. To confirm the diagnosis, we reviewed medical records.
Assessment of Other Variables
Using a self-administered demographic and medical questionnaire, subjects were able to report required information including age, sex (male/female), marital status (single/married), education (high school graduated or below/ academic education), smoking status (yes/no), family size, homeownership (owner/ non-owner), and medical history including existence of hyperlipidemia, hypertension, gallstone, Crohn's disease, and diabetes. Data on dietary habits including meal regularity (never or occasionally/often or always), fluid consumption during meals (<3 glasses/≥3 glasses), chewing efficiency (not a lot/ a lot), fried foods intake (<4 per week/≥4 per week), and fatty meals intake (non-fatty meal/fatty meal) were collected through a pretested dietary habit questionnaire. To examine physical activity of study participants, General Practice Physical Activity Questionnaire (GPPAQ) was applied. Based on the guideline of this questionnaire, we classified study subjects as having no activity, having activity as <3 h per week, 3–5 h per week, 5–7 h per week, and ≥7 h per week. Required information about anthropometric variables was collected through the use of a self-administered questionnaire. Body mass index (BMI) was calculated as weight divided by height squared. Our previous study had shown that self-administered questionnaire of anthropometric measures provides valid information compared with actual measured values (24).
Statistical Analysis
Required sample size for this study was calculated based on prior evidence indicating that approximately 60% of Iranian adults are following non-healthy dietary patterns (25). According to previous publications, we assumed that consumption of unhealthy dietary patterns would double the risk of IBD (19). Therefore, considering type I error of 5%, the study power of 80%, and 2 controls per case, we needed at least 101 cases and 202 controls for the current study. To categorize study participants, we defined quartile cut-offs points of IPD score in the control group: Q1: <−1.70; Q2: between −1.70 and −0.41; Q3: between −0.41 and 0.97; Q4: >0.97. Comparisons between cases and controls were performed by applying student's t-test for quantitative variables and chi-square for categorical variables. Significant differences across categories of IPD score were examined using one-way analysis of variance (ANOVA). However, chi-square test was applied to assess the distribution of participants in terms of categorical variables across quartiles of IPD score. We applied analysis of covariance (ANCOVA) to obtain energy, sex, and age-adjusted dietary intakes of subjects across categories of IPD score. Binary logistic regression was used to find the association of IPD score with UC, in crude and multivariable-adjusted models. Potential confounders were selected according to previous studies, in which intended variable was found to be associated with UC (26, 27). In the first model, BMI (continuous), age (continuous), and sex (male/female) were controlled for. Then, in the second model, we additionally adjusted for smoking (yes/no), having diabetes (yes/no), education (high school graduated or below/ academic education), and physical activity (no activity/<3 h per week/3–5 h per week/5–7 h per week/≥7 h per week). In the last model, regular meal consumption (never or occasionally/often or always), fluid consumption during meals (<3 glasses/≥3 glasses), chewing efficiency (not a lot/a lot), fried foods intake (<4 per week/≥4 per week), and consumption of fatty meals (non-fatty meal/fatty meal) were also adjusted for. In all analyses, the first quartile of IPD score was considered as the reference category. In the logistic regression models, we treated quartiles of IPD score as an ordinal variable to determine P for trends. SPSS software version 19 was used to carry out all statistical analyses. P-values were considered statistically significant at < 0.05.
Results
Characteristics of UC Cases and Controls
In the present study, 327 people (109 cases and 218 controls) were included. Mean age of cases and controls was 39.5 ± 10.0 and 41.5 ± 11.8 y, respectively. Totally, 52% of study participants were female and 48% were male. Participants with UC were less likely to be physically active and university graduates. No significant differences in mean age and BMI were observed between cases and controls. There was also no significant difference in the distribution of subjects when considering them in terms of sex, smoking status, marital status, and history of diabetes. Comparing participants across quartiles of IPD score, we failed to find any significant difference in mean age and BMI as well as sex, marital status, smoking status, history of diabetes, education, and physical activity (Table 1).
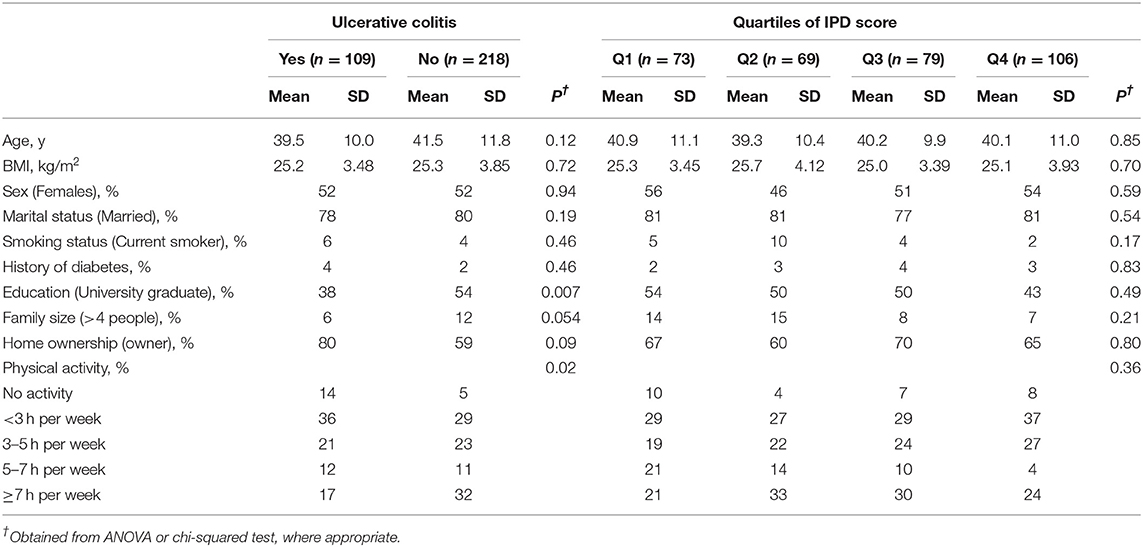
Table 1. Characteristics of patients with ulcerative colitis (UC) and controls across quartiles of inflammatory potential of the diet (IPD) score.
Dietary Habits of UC Cases and Controls
No significant difference was observed between cases and controls in terms of dietary habits including regular meal pattern, chewing efficiency, fluid consumption during meals, fried foods intake, and fatty meals intake. This was also the case when we compared the distribution of subjects in terms of above-mentioned variables across quartiles of IPD score (Table 2).
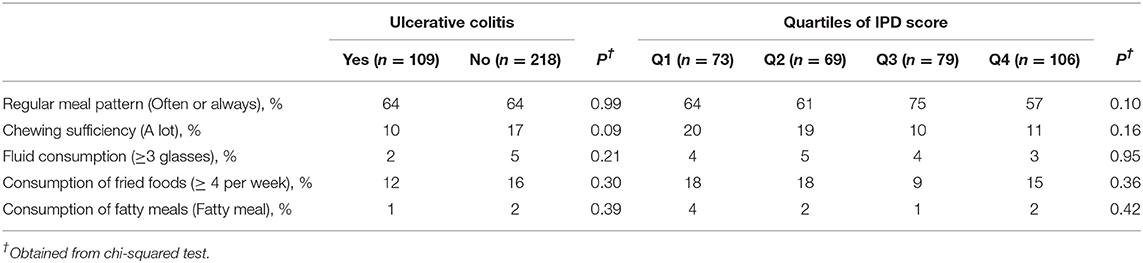
Table 2. Distribution of patients with ulcerative colitis (UC) and controls in terms of dietary habits across quartiles of inflammatory potential of the diet (IPD) score.
Dietary Intakes of UC Cases and Controls
Cases reported higher intakes of energy, PUFA, vitamin A, vitamin C, and vitamin B12 and lower intakes of protein, MUFA, vitamin B1, vitamin B2, vitamin B3, iron, zinc, magnesium, β-carotene, folate and, dietary fiber compared to controls. Participants in the highest quartile of IPD score had lower energy, vitamin E, vitamin C, vitamin B6, riboflavin, niacin, β-carotene, folate, dietary fiber, MUFA, PUFA, Fe, Mg, Zn, and, Se as well as higher vitamin B12 and PUFA intake compared with those in lowest quartile (Table 3). In addition, patients with UC had lower intakes of fruits and refined grains than controls, whereas there were no significant differences in consumption of whole-grains, white meats, red and processed meats, fish, vegetables dairy products, nuts and legumes, green/black tea and coffee. Higher IPD score was associated with lower intakes of red and processed meat, and green/black tea and coffee, and higher intake of refined grains (Table 4).
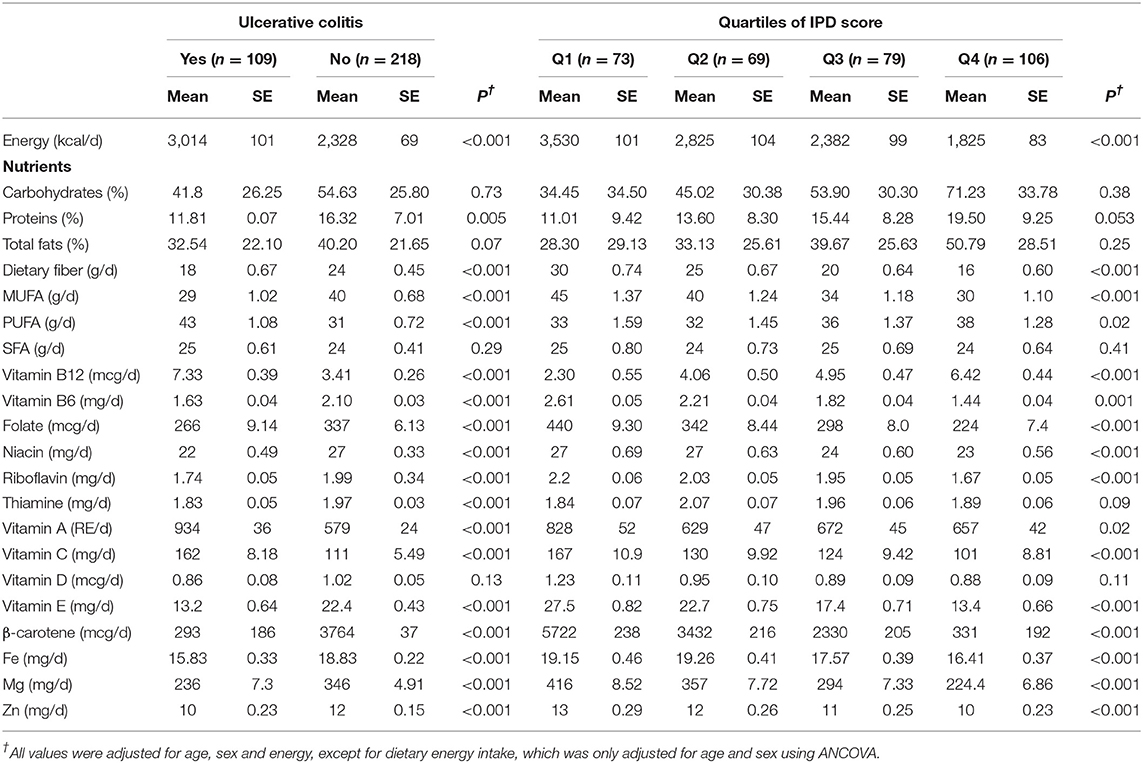
Table 3. Dietary intakes of selected nutrients for patients with ulcerative colitis (UC) and controls across quartiles of inflammatory potential of the diet (IPD) score.
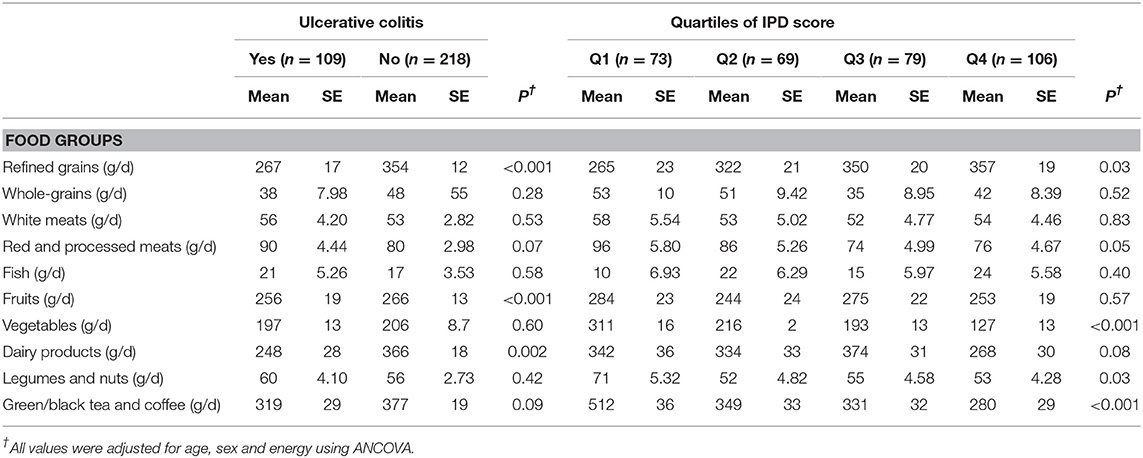
Table 4. Dietary intakes of selected food groups for patients with ulcerative colitis (UC) and controls across quartiles of inflammatory potential of the diet (IPD) score.
Association of IPD With UC
After controlling for age, sex, and BMI, we found that participants in highest quartile of IPD score had 183% increased chance of UC compared with those in the lowest quartile (OR: 2.83; 95% CI: 1.41–5.69, P-trend < 0.001). More adjustment for education, smoking, medical history, and physical activity strengthened this association (OR: 3.48; 95% CI: 1.32–9.10, P-trend = 0.003). After we took dietary habits into account, the association did not change much (OR: 3.33; 95% CI: 1.20–9.20, P-trend = 0.005) (Table 5).
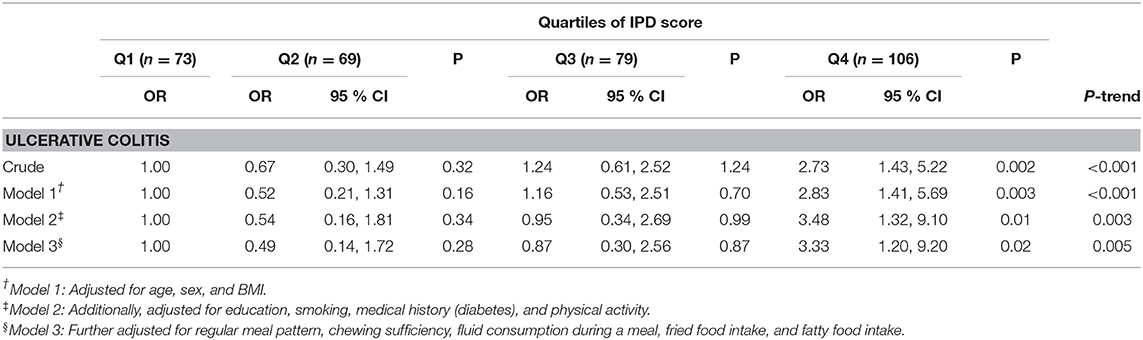
Table 5. Crude and multivariable-adjusted ORs and 95% CIs for UC across quartiles of inflammatory potential of the diet (IPD) score.
Discussion
We found that patients with UC were more likely to consume pro-inflammatory diets compared with controls. This association remained significant after taking potential confounders into account. To the best of our knowledge, this is among the first studies in which the link between inflammatory potential of the diet and UC was assessed.
UC prevalence has rapidly increased in developing countries over recent decades. It causes an enormous cost on the healthcare system and has been shown to negatively affect general health, mental health, and social function of patients (26). Chronic inflammation is an underlying physiological process that has been associated with numerous gastrointestinal disorders including IBS (17), reflux esophagitis (18), and UC (19). In fact, there are several lines of evidence linking inflammation to UC. For instance, consumption of fruits and vegetables, known as anti-inflammatory food parameters (28), was linked to decreased risk of UC (29). While intake of pro-inflammatory foods such as red and processed meats and refined carbohydrates was associated with elevated risk of UC (30–32).
We found that adherence to a pro-inflammatory diet was associated with greater odds of UC. It has been shown that higher diet quality was associated with a lower chance of UC. In a cohort study, higher Healthy Eating Index-2015 (HEI-2015) score was associated with 66% reduced risk of UC (33). This was also reported about dietary TAC score; such that higher dietary total antioxidant capacity (TAC) score was associated with lower odds of UC in a case-control study (34). Only one previous study has examined the relationship between literature-derived nutrient-based DII and UC. Our findings are similar to this hospital-based case-control study, in which consuming a pro-inflammatory diet was associated with 1.5 times increased risk of UC (19). However, a recent prospective cohort study investigating the relation between empirical dietary inflammatory pattern (EDIP) score and IBD incidence, found no significant association between a pro-inflammatory dietary pattern with UC risk (35). The difference in studies' design might help to explain discrepant findings. Prospective studies, especially in developing countries are needed to confirm these findings.
The potential mechanisms through which might a pro-inflammatory diet contributes to UC pathogenesis are yet to be determined. Chronic inflammation is an underlying physiological process associated with inflammatory bowel disease, UC. Certain dietary components may induce inflammation by altering inflammatory gene expression (36, 37). Results from a recent publication showed that a pro-inflammatory diet is associated with greater proinflammatory gene expression among non-obese individuals (38). Considering the role of inflammatory mediators including cytokines in the regulation of intestinal immune responses and intestinal mucosal barrier homeostasis (39), cytokines play a critical role in causing the chronic inflammatory condition in IBD (40). Therefore, consumption of a pro-inflammatory diet can contribute to UC pathogenesis through increasing serum levels of inflammatory cytokines. Moreover, there is growing evidence showing that gut microbiota is associated with a lot of immune and inflammatory disorders. Gut microbiota can influence intestinal immunity by promoting the development and maintenance of the mucosal immune system, protecting against pathogen invasion, and maintaining gastrointestinal tract barrier integrity (41). Abnormalities of the gut microbiome are common in different intestinal conditions, including IBD. In fact, an altered microbiota has been reported in IBD (10, 39). Diet can affect the gut microbiota (42, 43), as a recent publication revealed a correlation between intakes of energy and micronutrients such as vitamin A, vitamin D and, vitamin C, all contributed to IPD score, with fecal and mucosal communities in UC patients (44). Therefore, a pro-inflammatory diet might increase risk of UC through its influence on gut flora composition.
Our study has several strengths. Being among the first studies in the field, using a validated FFQ to assess subjects' dietary intake and statistical adjustment for several potential covariates are among these strengths. However, there are some limitations as well. Findings from case-control study do not allow conferring causality. Therefore, prospective cohort studies would be required to confirm these findings. Recall and selection bias are inherent in case-control studies, which might affect our findings. Although we used a validated FFQ for dietary assessment, there is still the possibility of measurement errors and misclassification of study participants in terms of exposure. Despite controlling for several potential covariates, the effect of residual confounding cannot be excluded. There was a difference in educational status of cases and controls. This has occurred because cases were selected from IBD registry, while controls were chosen from SEPAHAN project dataset, which was conducted among university employees. This difference might lead to a difference in the household income between cases and controls, which can in turn affect the findings. Additionally, the possibility of changing dietary intake in UC patients as a result of their condition cannot be ignored. We did not collect any information about the duration of disease in UC patients, therefore we could not analyze our data accordingly. In the present study, unlike original DII method, we computed IPD score using data on only 28 nutrient or food items. In total, we did not consider 17 items (saffron, garlic, rosemary, turmeric, ginger, oregano, n-3 fatty acid, trans fatty acid, n-6 fatty acids, flavonols, isoflavones, flavan-3-ol, flavonones, flavones, eugenol, anthocyanidins, and alcohol) in our IPD score calculation due to lacking their information in our dataset. Given that most missing items in our dataset were of anti-inflammatory potential, therefore, studies that include all these items in their DII score calculation might reach a different conclusion than the one we found. Other studies were done in Iran, including the one that has been done on UC patients, have used only 27 foods or nutrients to calculate DII. Finally, in the current study, we had no data on inflammatory biomarkers to examine the validity of IPD; however, previous studies in Iran have shown good correlations between DII and serum concentrations of inflammatory biomarkers, indicating a reasonable validity of this index to predict inflammation (45, 46).
Conclusion
As a conclusion, this case-control study indicated that consuming a diet with high IPD score might be positively associated with UC. Considering the limitations of case-control studies as well as the nutrient-based index we used in the current analysis which cannot capture interactions between nutrients, future studies are required to examine this association. In particular, developing a new index based on all available publications on the association between foods and inflammation is necessary. Designing prospective studies to investigate this association can also shed light on this link in the future.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethical Committee of the Tehran University of Medical Sciences, Tehran, Iran (IR.TUMS.VCR.REC.1398.497). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
ZK and PS contributed in conception, design, search, statistical analyses, data interpretation, and manuscript drafting. AH-K and HD contributed in design and data interpretation. HT and PA contributed in conception, design, statistical analyses, data interpretation, and manuscript drafting. AE supervised the study. All authors approved the final manuscript for submission. All authors contributed to the article and approved the submitted version.
Funding
This study was supported by Research Council of School of Nutritional Sciences and Dietetics, Tehran University of Medical Sciences, Tehran, Iran.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank all participants of the study for their cooperation. We also thank Asma Salari-Moghaddam and Alireza Milajerdi for their scientific consultations.
References
1. Rogler G, Biedermann L, Scharl M. New insights into the pathophysiology of inflammatory bowel disease: microbiota, epigenetics and common signalling pathways. Swiss Med Wkly. (2018) 148:w14599. doi: 10.4414/smw.2018.14599
2. Zhou M, He J, Shen Y, Zhang C, Wang J, Chen Y. New frontiers in genetics, gut microbiota, and immunity: a rosetta stone for the pathogenesis of inflammatory bowel disease. Biomed Res Int. (2017) 2017:8201672. doi: 10.1155/2017/8201672
3. Abraham C, Cho JH. Inflammatory bowel disease. N Engl J Med. (2009) 361:2066–78. doi: 10.1056/NEJMra0804647
4. Khor B, Gardet A, Xavier RJ. Genetics and pathogenesis of inflammatory bowel disease. Nature. (2011) 474:307–17. doi: 10.1038/nature10209
5. Malekzadeh MM, Vahedi H, Gohari K, Mehdipour P, Sepanlou SG, Ebrahimi Daryani N, et al. Emerging epidemic of inflammatory bowel disease in a middle income country: a nation-wide study from Iran. Arch Iran Med. (2016) 19:2–15.
6. Asakura H, Suzuki K, Kitahora T, Morizane T. Is there a link between food and intestinal microbes and the occurrence of Crohn's disease and ulcerative colitis? J Gastroenterol Hepatol. (2008) 23:1794–801. doi: 10.1111/j.1440-1746.2008.05681.x
7. Ruemmele FM. Role of diet in inflammatory bowel disease. Ann Nutr Metab. (2016) 68(Suppl 1):33–41. doi: 10.1159/000445392
8. Santos S, Oliveira A, Lopes C. Systematic review of saturated fatty acids on inflammation and circulating levels of adipokines. Nutr Res. (2013) 33:687–95. doi: 10.1016/j.nutres.2013.07.002
9. Bordoni A, Danesi F, Dardevet D, Dupont D, Fernandez AS, Gille D, et al. Dairy products and inflammation: a review of the clinical evidence. Crit Rev Food Sci Nutr. (2017) 57:2497–525. doi: 10.1080/10408398.2014.967385
10. Rizzello F, Spisni E, Giovanardi E, Imbesi V, Salice M, Alvisi P, et al. Implications of the Westernized diet in the onset and progression of IBD. Nutrients. (2019) 11:1033. doi: 10.3390/nu11051033
11. Whalen KA, McCullough ML, Flanders WD, Hartman TJ, Judd S, Bostick RM. Paleolithic and mediterranean diet pattern scores are inversely associated with biomarkers of inflammation and oxidative balance in adults123. J Nutr. (2016) 146:1217–26. doi: 10.3945/jn.115.224048
12. Shivappa N, Steck SE, Hurley TG, Hussey JR, Ma Y, Ockene IS, et al. A population-based dietary inflammatory index predicts levels of C-reactive protein in the Seasonal Variation of Blood Cholesterol Study (SEASONS). Public Health Nutr. (2014) 17:1825–33. doi: 10.1017/s136898001300.2565
13. Tabung FK, Steck SE, Zhang J, Ma Y, Liese AD, Agalliu I, et al. Construct validation of the dietary inflammatory index among postmenopausal women. Ann Epidemiol. (2015) 25:398–405. doi: 10.1016/j.annepidem.2015.03.009
14. Ruiz-Canela M, Zazpe I, Shivappa N, Hebert JR, Sanchez-Tainta A, Corella D, et al. Dietary inflammatory index and anthropometric measures of obesity in a population sample at high cardiovascular risk from the PREDIMED (PREvencion con DIeta MEDiterranea) trial. Br J Nutr. (2015) 113:984–95. doi: 10.1017/s0007114514004401
15. Shivappa N, Steck SE, Hurley TG, Hussey JR, Hébert JR. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. (2014) 17:1689–96. doi: 10.1017/S1368980013002115
16. Cavicchia PP, Steck SE, Hurley TG, Hussey JR, Ma Y, Ockene IS, et al. A new dietary inflammatory index predicts interval changes in serum high-sensitivity C-reactive protein. J Nutr. (2009) 139:2365–72. doi: 10.3945/jn.109.114025
17. Salari-Moghaddam A, Hassanzadeh Keshteli A, Esmaillzadeh A, Adibi P. Empirically derived food-based inflammatory potential of the diet, irritable bowel syndrome and its severity. Nutrition. (2019) 63–64:141–7. doi: 10.1016/j.nut.2019.02.004
18. Shivappa N, Hebert JR, Anderson LA, Shrubsole MJ, Murray LJ, Getty LB, et al. Dietary inflammatory index and risk of reflux oesophagitis, Barrett's oesophagus and oesophageal adenocarcinoma: a population-based case-control study. Br J Nutr. (2017) 117:1323–31. doi: 10.1017/s0007114517001131
19. Shivappa N, Hebert JR, Rashvand S, Rashidkhani B, Hekmatdoost A. Inflammatory potential of diet and risk of ulcerative colitis in a case-control study from Iran. Nutr Cancer. (2016) 68:404–9. doi: 10.1080/01635581.2016.1152385
20. Adibi P, Keshteli AH, Esmaillzadeh A, Afshar H, Roohafza H, Bagherian-Sararoudi R, et al. The study on the epidemiology of psychological, alimentary health and nutrition (SEPAHAN): overview of methodology. J Res Med Sci. (2012) 17:S292–S8.
21. Keshteli A, Esmaillzadeh A, Rajaie S, Askari G, Feinle-Bisset C, Adibi P. A Dish-based Semi-quantitative food frequency questionnaire for assessment of dietary intakes in epidemiologic studies in Iran: design and development. Int J Prev Med. (2014) 5:29–36.
22. Farhangi MA, Najafi M. Dietary inflammatory index: a potent association with cardiovascular risk factors among patients candidate for coronary artery bypass grafting (CABG) surgery. Nutrition J. (2018) 17:20. doi: 10.1186/s12937-018-0325-2
23. Lennard-Jones JE. Classification of inflammatory bowel disease. Scand J Gastroenterol Suppl. (1989) 170:2–6; discussion 16–9. doi: 10.3109/00365528909091339
24. Aminianfar A, Saneei P, Nouri M, Shafiei R, Hassanzadeh-Keshteli A, Esmaillzadeh A, et al. Validity of self-reported height, weight, body mass index and waist circumference in Iranian adults. Int J Prev Med. (2019).
25. Kimiagar SM, Ghaffarpour M, Houshiar Rad A, Hormozdyari H, Zellipour L. Food consumption pattern in the Islamic Republic of Iran and its relation to coronary heart disease. East Mediterr Health J. (1998) 4:539–47.
26. Windsor JW, Kaplan GG. Evolving epidemiology of IBD. Curr Gastroenterol Rep. (2019) 21:40. doi: 10.1007/s11894-019-0705-6
27. Cui G, Yuan A. A systematic review of epidemiology and risk factors associated with chinese inflammatory bowel disease. Front Med. (2018) 5:183. doi: 10.3389/fmed.2018.00183
28. Defagó MD, Elorriaga N, Irazola VE, Rubinstein AL. Influence of food patterns on endothelial biomarkers: a systematic review. J Clin Hypertens. (2014) 16:907–13. doi: 10.1111/jch.12431
29. Li F, Liu X, Wang W, Zhang D. Consumption of vegetables and fruit and the risk of inflammatory bowel disease: a meta-analysis. Eur J Gastroenterol Hepatol. (2015) 27:623–30. doi: 10.1097/MEG.0000000000000330
30. Buyken AE, Goletzke J, Joslowski G, Felbick A, Cheng G, Herder C, et al. Association between carbohydrate quality and inflammatory markers: systematic review of observational and interventional studies. Am J Clin Nutr. (2014) 99:813–33. doi: 10.3945/ajcn.113.074252
31. Lopez-Garcia E, Schulze MB, Fung TT, Meigs JB, Rifai N, Manson JE, et al. Major dietary patterns are related to plasma concentrations of markers of inflammation and endothelial dysfunction. Am J Clin Nutr. (2004) 80:1029–35. doi: 10.1093/ajcn/80.4.1029
32. Shivappa N, Bonaccio M, Hebert JR, Di Castelnuovo A, Costanzo S, Ruggiero E, et al. Association of pro-inflammatory diet with low-grade inflammation: results from the Moli-sani study. Nutrition. (2018) 54:182–8. doi: 10.1016/j.nut.2018.04.004
33. Rahmani J, Varkaneh HK, Ryan PM, Zarezadeh M, Rashvand S, Clark C, et al. Healthy Eating Index-2015 as a predictor of ulcerative colitis risk in a case–control cohort. J Dig Dis. (2019) 20:649–55. doi: 10.1111/1751-2980.12826
34. Rahmani J, Kord-Varkaneh H, Ryan PM, Rashvand S, Clark C, Day AS, et al. Dietary total antioxidant capacity and risk of ulcerative colitis: a case-control study. J Dig Dis. (2019) 20:636–41. doi: 10.1111/1751-2980.12823
35. Lo C-H, Lochhead P, Khalili H, Song M, Tabung FK, Burke KE, et al. Dietary inflammatory potential and risk of Crohn's Disease and Ulcerative Colitis. Gastroenterology. (2020) 159:873–83.e1. doi: 10.1053/j.gastro.2020.05.011
36. Shivappa N, Hebert JR, Marcos A, Diaz LE, Gomez S, Nova E, et al. Association between dietary inflammatory index and inflammatory markers in the HELENA study. Mol Nutr Food Res. (2017) 61:707. doi: 10.1002/mnfr.201600707
37. Shivappa N, Wirth MD, Hurley TG, Hébert JR. Association between the dietary inflammatory index (DII) and telomere length and C-reactive protein from the National Health and Nutrition Examination Survey-1999–2002. Mol Nutr Food Res. (2017) 61:1600630. doi: 10.1002/mnfr.201600630
38. Padin AC, Hebert JR, Woody A, Wilson SJ, Shivappa N, Belury MA, et al. A proinflammatory diet is associated with inflammatory gene expression among healthy, non-obese adults: can social ties protect against the risks? Brain Behav Immun. (2019) 82:36–44. doi: 10.1016/j.bbi.2019.07.031
39. Witkowski M, Witkowski M, Gagliani N, Huber S. Recipe for IBD: can we use food to control inflammatory bowel disease? Semin Immunopathol. (2018) 40:145–56. doi: 10.1007/s00281-017-0658-5
40. Kunnumakkara AB, Sailo BL, Banik K, Harsha C, Prasad S, Gupta SC, et al. Chronic diseases, inflammation, and spices: how are they linked? J Trans Med. (2018) 16:14. doi: 10.1186/s12967-018-1381-2
41. Minihane AM, Vinoy S, Russell WR, Baka A, Roche HM, Tuohy KM, et al. Low-grade inflammation, diet composition and health: current research evidence and its translation. Br J Nutr. (2015) 114:999–1012. doi: 10.1017/s0007114515002093
42. Castro F, de Souza HSP. Dietary composition and effects in inflammatory bowel disease. Nutrients. (2019) 11:1398. doi: 10.3390/nu11061398
43. Rapozo DC, Bernardazzi C, de Souza HS. Diet and microbiota in inflammatory bowel disease: the gut in disharmony. World J Gastroenterol. (2017) 23:2124–40. doi: 10.3748/wjg.v23.i12.2124
44. Weng Y, Gan H, Li X, Huang Y, Li Z, Deng H, et al. Diet-microbiota-metabolite interaction networks reveal key players in inflammatory bowel disease. J Dig Dis. (2019) 20:447–59. doi: 10.1111/1751-2980.12795
45. Vahid F, Shivappa N, Faghfoori Z, Khodabakhshi A, Zayeri F, Hebert JR, et al. Validation of a dietary inflammatory index (DII) and association with risk of gastric cancer: a case-control study. Asian Pac J Cancer Prev. (2018) 19:1471–7. doi: 10.22034/apjcp.2018.19.6.1471
46. Vahid F, Shivappa N, Hekmatdoost A, Hebert JR, Davoodi SH, Sadeghi M. Association between Maternal Dietary Inflammatory Index (DII) and abortion in Iranian women and validation of DII with serum concentration of inflammatory factors: case-control study. Appl Physiol Nutr Metab. (2017) 42:511–6. doi: 10.1139/apnm-2016-0274
Keywords: ulcerative colitis, inflammatory bowel disease, inflammatory potential of the diet, dietary pattern, case-control study
Citation: Khademi Z, Saneei P, Hassanzadeh-Keshteli A, Daghaghzadeh H, Tavakkoli H, Adibi P and Esmaillzadeh A (2021) Association Between Inflammatory Potential of the Diet and Ulcerative Colitis: A Case-Control Study. Front. Nutr. 7:602090. doi: 10.3389/fnut.2020.602090
Received: 02 September 2020; Accepted: 17 December 2020;
Published: 10 February 2021.
Edited by:
Esther Molina-Montes, University of Granada, SpainReviewed by:
Irina Uzhova, Institute of Technology, Sligo, IrelandAndrew S. Day, University of Otago, New Zealand
Copyright © 2021 Khademi, Saneei, Hassanzadeh-Keshteli, Daghaghzadeh, Tavakkoli, Adibi and Esmaillzadeh. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ahmad Esmaillzadeh, YS1lc21haWxsemFkZWhAdHVtcy5hYy5pcg==