
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Neurol. , 29 January 2025
Sec. Neurorehabilitation
Volume 16 - 2025 | https://doi.org/10.3389/fneur.2025.1506889
This article is part of the Research Topic New approaches for central nervous system rehabilitation - Volume II View all 4 articles
 Giovanni Morone1,2
Giovanni Morone1,2 Marco Tramontano3,4
Marco Tramontano3,4 Stefano Paolucci5
Stefano Paolucci5 Antonio Cerasa6,7
Antonio Cerasa6,7 Irene Ciancarelli1
Irene Ciancarelli1 Alex Martino Cinnera5
Alex Martino Cinnera5 Marco Iosa5,8*
Marco Iosa5,8* Rocco Salvatore Calabrò9
Rocco Salvatore Calabrò9Robot-assisted arm training (RAAT) has demonstrated promising potential in improving rehabilitation outcomes for individuals with neurological conditions, particularly stroke. Despite 20 years of their use in clinical and research settings, there are still significant needs to be made concerning clinical indications. In the present perspective manuscript, we provide some hypotheses of the suitability of different RAAT according to the features of the available devices and clinical characteristics, showing their limitations and strengths. Several factors were considered in the optimization of RAAT intervention, including the technological characteristics of the devices (e.g., support and constriction), the residual upper limb motor function, and the clinical phase of stroke. Finally, we outline key areas for improvement to advance the field in the near future and provide neuroscientific bases for hypotheses of tailored RAAT training to improve the outcome of robotic rehabilitation.
Robot Assisted Arm Training (RAAT) has long been envisaged as a strategy to enhance arm motor recovery after a stroke (1). Significant efforts have been made toward identifying the neural mechanisms underlying RAAT and their relationship with improved motor recovery (2–5). The rationale behind the application of robots in stroke rehabilitation is that RAAT involves areas of the brain that govern movement planification and execution by early, standardized, repeatable and intense mobilization of the patient’s arm (6, 7). Such reiterated engagement of motor areas is intended to influence brain plasticity phenomena, improving functional outcomes (8). The role of an early mobilization after stroke is well recognized in literature to reduce acute phase complications and improve functional outcomes, especially to more severely affected people (9).
Interestingly, to be task-oriented the RAAT often embedded a system for serious-game technology on which a digital task runs allowing the patient to interact with it, for providing to him/her the execution of task oriented movements and giving visual and acoustic feedback of his/her performance. Despite robots and serious videogames (implemented using virtual reality or on a screen) are two clearly distinct technologies, the common combination in RAAT implies some motor and cognitive links that contribute to enhancing hand and arm sensory-motor areas (10), as well as cognitive functions (11) but makes more difficult to discriminate the specific effect attributed to the robotic system itself, leading to observe cognitive effects of upper limb robotic therapy (12, 13).
Nowadays, evidence for a clinical benefit of RAAT is consolidated as per Cochrane collaboration and in several stroke national guidelines (14, 15). Nonetheless a recent large, randomized, controlled trial in people with subacute stroke reported no significant clinical improvement of RAAT vs. enhanced upper limb therapy (16).
There are different devices for the upper limb that can be distinguished firstly in electromechanical devices vs. robots (being the second adaptable to the patient’s motor behavior during the task), on the basis of clinical characteristics (interactive/assistive), based on technical characteristics (Exoskeleton/End-effector, number of active and/or passive degree of Freedom, Bilateral/Uilateral, distal/proximal, feedback, Wearability, Environment [Real, Virtual], Assistance modality, Recorded parameters [Range of motion, Force, Kinematics], Control system [Force, Range of motion, Impedance, EMG] and Movement dimension [1D/2D/3D]) (17–19).
The main point to be improved regarding the RAAT, and in general to the translational sciences of the robots applied to rehabilitation, is to define the best practices related to the clinical characteristics of individuals that might benefit from a specific type of robot (i.e., exoskeleton/end effector, constrictive characteristics, degree of freedom, cognitive load, movement intention detection, and more).
Although physicians and customers have been looking for solutions to the robotic clinical protocol problem for decades, it is still challenging to find the best candidates for RAAT. Actually, assessing the literature by itself is insufficient to reach this conclusion because each RCT is biased by its design, which assesses overall efficacy rather than the beneficiary’s functional characteristics. According to the Precision Medicine Initiative, that promotes an emerging approach for disease treatment and prevention that considers individual variability (20), and to previous studies that changed the research question from “is robotic treatment effective?” into “who may benefit from robotic therapy?” (21–23), we hypothesized possible indications on the use of RAAT considering rehabilitation objectives, persons functional characteristics, and time from stroke acute event. This manuscript aims to provide neuroscientific bases for hypotheses of personalized robotic training.
Specifically, we will analyze some fundamental aspects that need to be considered from researchers and clinicians for a better integration of robotic training in the rehabilitation project of individuals with stroke. We will analyze the characteristics of the machine according to the patient’s motor possibilities, the cognitive-motor interactions during the execution of robotic functional tasks (24), the continuum of care through the different settings, the importance of contrasting the phenomenon of non-use learning, the functional cross talk between hand and upper limb recovery and finally the personalization of robotic therapy.
The term “machine constriction” in the context of robotic devices for motor recovery in people with stroke likely refers to the physical and functional limitations that a machine, like a robotic rehabilitation device, can impose on a patient during therapy (17). These constrictions could involve:
1. Physical restraints: The robotic device might physically limit or guide the movement of a patient’s limb to ensure it follows a controlled range of motion. This can prevent unsafe or incorrect movements but may also feel restrictive if the machine over constrains the motion (17).
2. Assistance level or weight support: Some robotic devices may constrict the amount of assistance or resistance they provide during therapy. For instance, they may limit how much they aid or oppose the patient’s movements, depending on the patient’s ability to move on their own (17–19).
3. Degree of freedom: Robotic systems may have a limited number of degrees of freedom (DoF), meaning they allow motion only in certain directions or planes. This is a form of “constriction” that simplifies the movement patterns for rehabilitation but may not fully mimic the complexity of human movements (17–19).
4. Best candidate: Even if robotic devices have a wide margin of adaptability based on the functionality of the patient, they are built taking in mind a specific type of patient, which is the best candidate. That is, the ideal patient who, due to the specific phase of the event, cognitive and motor functional condition, can benefit from a specific robotic treatment (23).
In the context of stroke recovery:
• Device constriction can ensure safe rehabilitation by guiding a patient’s movement in a specific, therapeutically beneficial way. It can help train specific muscles and neural pathways damaged by the stroke.
• However, too much constriction can prevent the patient from using their muscles and motor control fully, limiting the effectiveness of the therapy and possibly hindering the recovery of motor independence.
A balance between assistance and freedom of movement is critical for optimizing motor recovery in people with stroke using robotic devices (23).
Using the “from efficacy for all to all for efficacy” approach (23, 25, 26), in this section we report the best practice for addressing patients to the best RAAT-related treatment. First, to maintain an intensive exercise with specific and timely tasks, in more compromised persons it is useful to use an exoskeleton that guarantees better motor control. When the patient recovers or if he/she already has some degree of muscle activity, end-effectors (that move the hand for moving the whole kinematic chain of the upper limb) can also be used (27, 28). In case of persons with mild to moderate impairment, sensor-based devices can be used (29). If the patient has a very mild disability, a conventional/ occupational approach with dedicated functional exercises in an ecological environment (without typical constriction provided by the robots) is often the best solution (2). This hypothesis of robot uses according to persons’ functionality is in line with the principles that in the face of a lower possibility of voluntary movement of the patient, a greater possibility of the robot to control and implement the movements of the upper limb and hand must correspond to a greater possibility of the robot (23, 26). Furthermore, this theory is consistent with recent research showing that persons who are more severely affected are the ones who stand to gain the most from robotic therapy (27, 30, 31).
It is of note that the relationship between intensity of training and recovery is not linear. Pila et al. recently analyzed responders vs. non-responder after RAAT noting that non responders do not improve arm functionality even in presence of an increase of RAAT intensity. Authors concluded that probably it is important to match training dose with robot parameters to allow a better functional recovery mediated by robot therapy (32). It is hypothesized that, despite the high intensity attained even in the more severely affected persons, the robot’s constriction is insufficient to achieve a clinically significant improvement in light of these results and the fact that arm sensory motor recovery depends on more than just training intensity.
It is also important to underline that a correct stratification of patients must inevitably consider the adaptability of the device to administer an exercise that leads to better performance during the exercise (i.e., increased participation, intra-session functional increase). Correct patient stratification and/or better robot identification will be the basis for creating evidence of greater robustness in the near future to avoid the mistakes made in the recent past. This section is well-articulated but could benefit from a more explicit discussion on patient stratification and device adaptability, particularly for future research directions.
Figure 1 presents a graphical representation of a possible hypothesis of treating arm paresis with a robot, allowing adequate intensity even for more severe persons and according to stroke phase, thanks to the robot characteristics. The functional status of the upper limb was stratified using the Fugl-Meyer Assessment scale for the Upper Extremity (FMA-UE), where a higher score indicates better functionality. The classification of stroke phases followed the ESO guidelines for stroke rehabilitation.
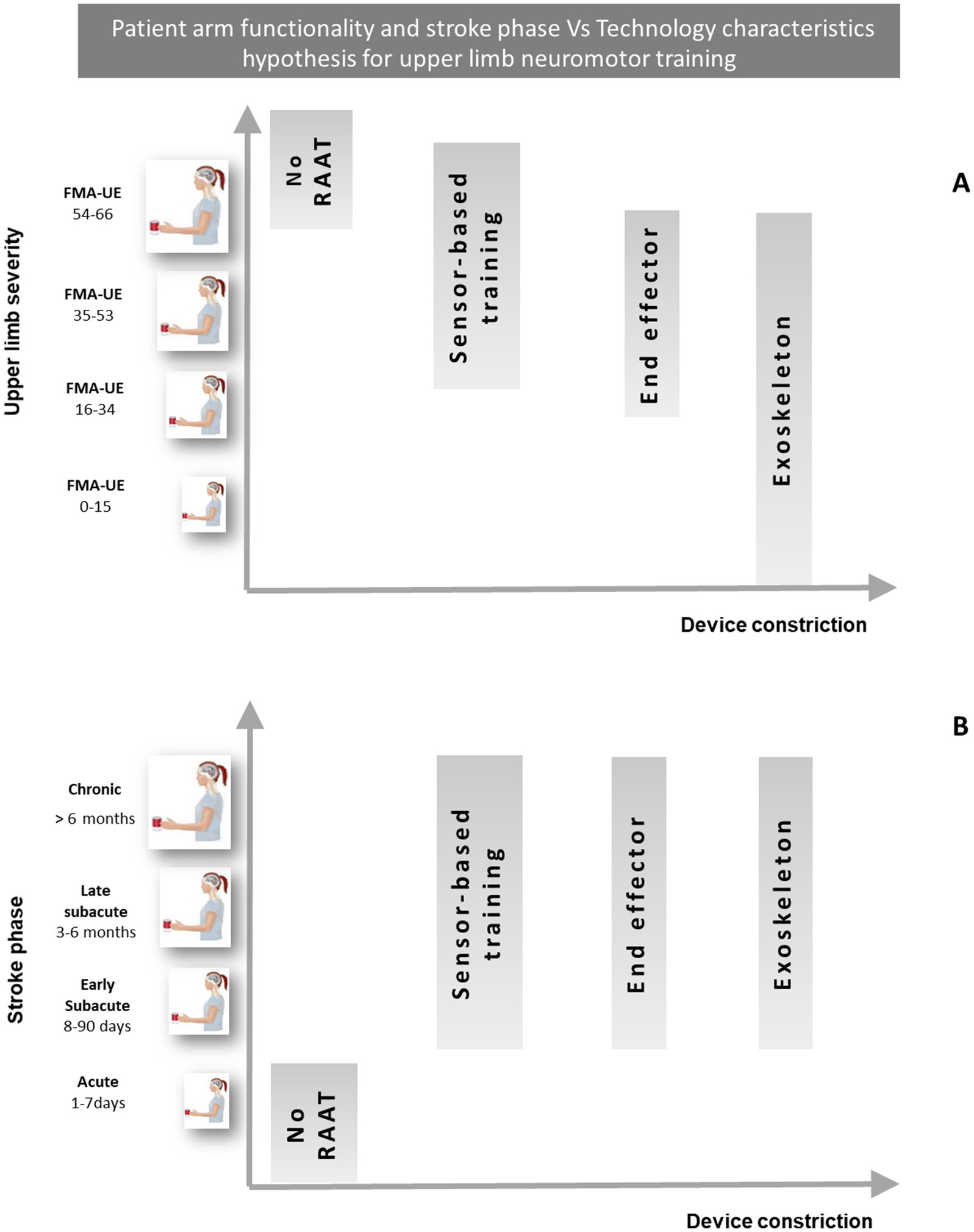
Figure 1. Hypothesis for the selection of RAAT to allow an adequate intensity of training, based on the technological characteristics of the devices and the functional status of the upper limb (A), and on the clinical phase of stroke (B). Adapted from Morone et al. (23). RAAT, robot assisted arm therapy; FMA-UE, Fugl Mayer assessment—upper extremities.
To develop our treatment hypothesis, we stratified the arm severity presented in Figure 1A according the FMA-UE cut-offs proposed by Woytowicz et al. (33) clustering the UL functional level as follow:
• Severe (0–15): no hand, wrist, or multi-joint movements and limited to no movement from single joint extensor and flexor muscle synergies.
• Severe–Moderate (16–34): marked impairment with no movement out of synergy and limited movement from single joint extensor and flexor synergies, hand, wrist, or multi-joint movements.
• Moderate–Mild (35-53): moderate impairment with limited movements out of synergy and partial impairment of single joint extensor and flexor synergies, hand, wrist, and multi-joint movements.
• Mild (54-66): minimal impairment and able to perform movements out of synergy with full movement of the arm.
Figure 1B shows the classification of stroke clinical phases following the ESO guidelines for stroke rehabilitation (34). It should be considered that in the acute and early subacute phase, functional impairment is certainly greater and therefore in this phase the use of robotic devices could be important, as it is crucial for the execution of complex tasks, and not only because neuroplasticity processes are more active (14, 15).
Over the past ten years, many paradigms for upper limb robotic rehabilitation have been completely or partially shifted from Bottom-up to Top-down training (3, 35, 36). This evolution can be attributed to the integration of visual interfaces, both immersive and non-immersive, with robotic systems. These interfaces enable the conversion of passive movements into a diverse array of task-oriented exercises that offer performance feedback, thereby engaging multiple cognitive functions during the learning process. These real-time and goal-directed feedback are well known key components to guide motor relearning (36). Furthermore, feedback can be manipulated in different ways, e.g., with error-based or positive-reinforcement mechanisms, by augmented or multiple feedback, real-time or after-performance feedback (37). It is also possible to insert during therapy a biofeedback/neurofeedback, a powerful means to modulate dependent on the activity of sensorimotor cortical networks (38). The cognitive trigger is often allowed thanks to the countless feedback provided by the 2D screen (non-immersive virtual reality) or even sometimes with serious game content that elicits executive functions (memory tasks, attention, working memory, task switching) and helps to make rehabilitation more salient and motivating, eliciting neuroplasticity (39).
Patients’ interest can be further increased by combining immersive VR with RAAT (40). This scenario suggests that there will be more natural 3D feedback to the 3D arm workspace, together with a genuine sense of presence in the virtual world and the corresponding neurophysiological reactions (as shown by physiological reactions in terms of heart rate, blood pressure etc.) (41). During a training performed in a VR scenario, the first perspective of the avatar induces an embodiment and hence a sense of body ownership that might impact the way in which persons perform an action (42). Immersive VR has the potential to influence motor brain networks thanks to the possibility of modifying the perception of reality (43).
One unique and fascinating way to manipulate attention in addition to visual and auditory stimuli is through dual tasking, which can be done during robotic therapy. Because the patient struggles to manage two activities at once, this approach creates more challenging working conditions for them, but it has been demonstrated to be highly helpful for functional recovery (44). However, Ranzani and colleagues have recently shown that an equivalent dosage of neurocognitive training in people with subacute stroke does not result in less motor skills improvement than robot-assisted therapy of hand function using a neurocognitive approach (i.e., combining motor training with somatosensory and cognitive tasks) (45).
Dual tasking training is of particular interest in persons with disability from neurological origins for its role in motor performances and for predict cognitive decline (46–49), however in people with stroke and with cognitive deficits it might lead to a global improvement of the cognitive function, which was supported by the improved neural efficiency of associated brain areas (50).
An early discharge from hospital wards is necessary for the reduction of costs per individual patient and for an optimization of resources in rehabilitation of neurological conditions (51). Then, there is a need to treat patients at home or on the territory, once discharged from the subacute neurorehabilitation hospital, in continuity with what was done in the hospital. Telerehabilitation programs, for example, gave the opportunity to continue at home the task oriented and intensive training that was undertake in hospital (52). To this aim, robots can help, but smaller and more economic versions are needed to continue reaching the goals stated during the in-hospital training (53). The importance of continuum of care in upper limb and hand recovery is even greater than for other functions such as walking and balance. Indeed, upper limb function and the related activities of daily living may need clinically more time to recover, and important improvement may be observed also in the chronic phase. This scenario is supported by recent evidence that even in the chronic phase, intensive and task-oriented robotic training can lead to an improvement in motor control, and in some cases even a slight improvement in functionality (54–57). Continuing treatment is not only important from an economic point of view because it saves economic resources and makes care more efficient, but it is important from an ethical point of view, since patients can further improve functionally and in their quality of life. For technologies and robotics to play an important role in the scenario of the continuum of care, it will be necessary to plan easy-to-use, less expensive and more usable devices with simpler human-robot interfaces.
In the 1990s, Taub thoroughly explained the phenomenon of learning that has since allowed us to understand various mechanisms of maladaptive plasticity (58). Clinically, this maladaptive plasticity manifests as non-use, pain, and spasticity. This phenomenon is significantly more noticeable in the upper limbs because many daily activities can be performed with just one arm, supplying affected arm/hand reduced functionality (59, 60). Starting from these neuroscientific principles, robotic rehabilitation should be promoted as soon as possible and with adequate intensity, affected arm movement with goal-oriented functional exercises (61). Furthermore, the addition of other devices such as virtual reality, transcranial stimulations, should provide highly personalized rehabilitation exercises to counteract the phenomenon of maladaptive plasticity and promote the recovery of bimanual activities (62). In fact, bimanual activities recovery depends on the extent of corticospinal tract injury and initial sensory and cognitive impairments (63) and are directly related to the patient’s return to work and to the people community life. This should be promoted not only thanks to bimanual robots (Exoskeleton or end-effector) (5), but even implementing, for example, unilateral robots with appropriate Augmented Reality/Virtual Reality bimanual training. Bimanual cooperation, in fact, plays a vital role in functions of the upper extremity and daily activities and re-training bimanual force coordination in stroke survivors could facilitate a higher degree of participation in daily activities (64, 65). It is of note that the integration of both hands in a rehabilitation task led to cross-education and bilateral transfer of sensory motor learning phenomena between less affected hand (i.e., non-affected hand) to more affected hand that might increase functional recovery (66, 67).
The hand and the upper limb are two very distinct body structures with very distinct functionality (mainly grasping and reaching, respectively) (68). To improve distal part of the arm (hand and wrist) and decrease spasticity of the whole upper limb, the treatment based on distal-proximal approach is more effective than that of proximo-distal one (69, 70) and even better if the treatment is enriched with cognitive contents and bilateral training (71). Although this assumption is so true and easy to understand, it is often neglected to be applied in clinical practice (72). Indeed, when using either conventional rehabilitation or robots, especially during subacute phase, we train mainly the lower limb and the proximal upper limb, and little space is dedicated to the hand (73).
However, hand function is complex, and manipulation is a distinct important feature of human beings. This is why the cortical representation of the hand is proportionally larger than those related to other body parts, as described recently following Penfield’s findings (74).
According to conventional rehabilitation techniques, supporting distal functions is essential. However, outcomes for hand recovery are generally poor and often not detailed in clinical trials. Recent evidence suggests that starting rehabilitation distally, particularly with advanced technologies, could immediately stimulate the cognitive and sensory-motor networks of the hand, leading to better representation and potentially improved outcomes. Our hypothesis is corroborated by the study of Calabrò and coworkers. They demonstrated that the treatment of distal part of the arm with a robot, in people affected by chronic stroke, improves motor function by rebalancing interhemispheric connectivity (8).
During neuromotor rehabilitation, it will undoubtedly be essential to construct an increasing number of hand-specific robots and devices and use them either in parallel or in series. In any case, an individual and personalized rehabilitation project must be able to provide the possibility of training the distal or proximal part of the limb depending more on the characteristics of the patient. In fact, they should not be understood as antithetical but synergistic approaches.
Robots and technology aim to provide neuromotor rehabilitation for arm and hand recovery. They hold great potential for advancements and improvements in patient care (Figure 2) (14, 75, 76).
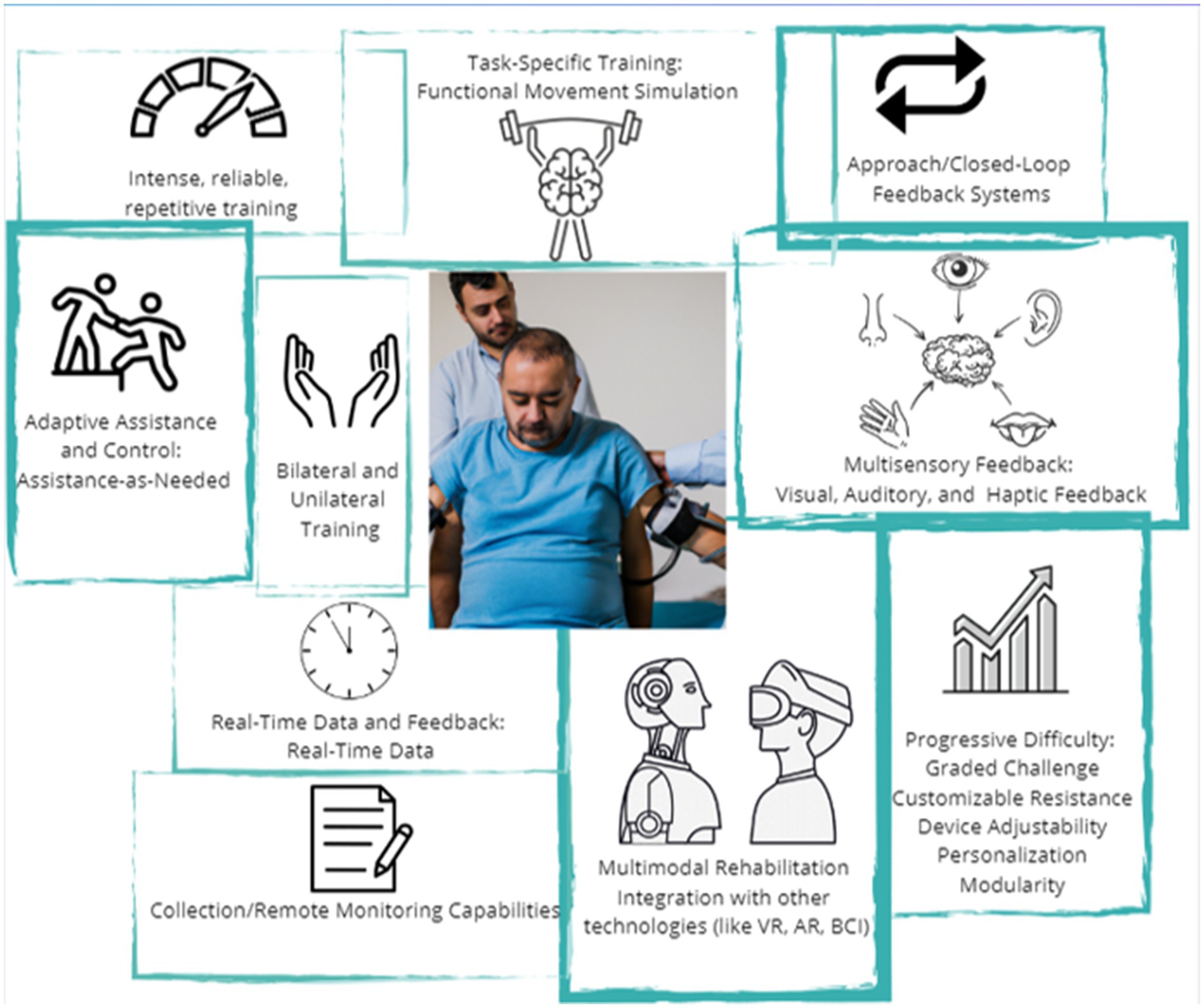
Figure 2. Key features of robotic devices for upper limb rehabilitation. Choosing the device based on its characteristics is fundamental to personalizing the treatment (this original figure was generated using AI tools).
Therefore, comparing neuromotor therapy administered with robotic or electromechanical devices and conventional neuromotor therapy for the upper limb in people with stroke, current evidence affirms that: RAAT improves activities of daily living scores; improves arm function and arm muscle strength, and did not increase the risk of participant dropout (18).
Aspects to be investigated in the future concern the possibility of achieving the objectives earlier, which is important for the improvement of the cost-effectiveness parameters of healthcare and of the whole Health technology Assessment, HTA process. Clinicians as well as bioengineers should shape the future of this field before that trade decides products and markets. To reduce the machine constraint, which in some subgroups of persons represent a limitation, the use of wearable devices with semi-rigid or soft fabrics could broaden the range of patients who could benefit from RAAT. To date, the soft-robots and exosuit are not meeting the needs of their users (77), requiring future advancements in this way. Moreover, many robotic devices can be integrated into a closed-loop system, combining the robot with biosignal acquisition (e.g., EEG, EMG), allowing for reinforced learning by generating robotic movement when a functional activity is detected. Other aspects to carefully consider for this purpose include the integration of other technologies, particularly the virtual reality/augmented reality (VR/AR) and the artificial Intelligence (78) and the modularity of the new robot devices for the more patient centered adaptability.
The personalization of motor and cognitive rehabilitation therapy must not only be implemented on the patient’s impairment/functionality aspects but must also consider factors such as age (79), gender (80) and psychological and behavioral aspects (81) that are decisive for the acceptability and effectiveness of the therapy. Artificial intelligence can adapt exercises following the motor and behavioral information captured by the robot’s sensors during therapy (inertial sensor unit, force detection, facial expression recognition). The integration of robots with AR and VR technologies can enhance rehabilitation training improving the engagement, the motivation, and the interaction during training. Additionally, AR and VR can simulate real-life personalized scenarios (ad hoc per function to be improved, persons’ cognitive resources and persons’ behavioral issues), allowing patients to practice functional movements in a safe and supervised environment before discharge (82, 83). It is important to note that these technologies are always supervised by physiotherapists or occupational therapists (84) and incorporated into the individual rehabilitation program. RAAT will continue to evolve to provide more personalized and adaptive therapy. They will be able to assess a patient’s abilities and adjust the rehabilitation therapy, tailoring it to their specific needs in terms of motor and function assistance and cognitive load (85). The robot or therapeutic technological device should inform the therapist of a rapid decrease in performance to allow him/her to re-modulate the type of training or to limit the training, suspending it, in unsuitable therapeutic conditions. The robots should also provide information on the patient’s state of stress by means of sensors for recording autonomic parameters (86, 87). This is particularly suitable when robots are used with populations with reduced communication skills and/or with children. Continuous monitoring and assessment: Robots equipped with sensors and wearable devices will enable continuous monitoring of patients’ progress and functional abilities. This real-time data can be used to track changes, identify potential issues, and adjust therapy plans accordingly. Continuous monitoring can also facilitate early intervention and prevent complications (5). The integration of RAAT in the clinical practice will continue to complement the conventional training rather than replace them. They will assist therapists in delivering therapy, providing objective data, and automating repetitive tasks (85, 88). This integration will allow therapists to provide more supervised sessions of treatments and focus on more complex and individualized aspects of patient care. Robot adaptability for severity and for setting: for less affected patients to show that they are doing more salient therapy and for the most severe patients to demonstrate a better ability to intercept movement intentions (5). Economic sustainability: healthcare managers and insurance must give credit to robot-assisted neuromotor therapy by increasing financial reimbursements, as it improves outcomes or reduces hospitalization time. At the same time, rehabilitation processes and rehabilitation spaces need to be adapted, as robots require large spaces and trained personnel. Finally, there is the urgent need of a greater accessibility in terms of costs of robots and an increasing of the clinicians’ knowledge regarding robot integration in the rehabilitation process.
Robotic devices have been introduced into clinical practice, but they are not always used in accordance with the patient’s characteristics, resulting in reduced efficacy. Despite, the recent literature reported a significant general efficacy of using robots in rehabilitation of patients with stroke in adjunction, partial or total substitution of conventional therapy (14, 15, 18), some contrasting results is still observed (16) and it could be due to the selection of patients as candidates for robotic therapy. According to our mentioned hypotheses, we proposed that the choice of using a specific device should be based on the patient’s functional level, carefully taking into account both motor (e.g., exoskeletons for more severe patients and end-effectors for less severe patients) and cognitive (e.g., challenges in feedback) domains. In motor recovery, the different levels of weight support offered by various types of robots (complete, partial, counter-resistance) or the type of device (exoskeleton, end-effector, sensor-based) make it possible to personalize the treatment and optimize outcomes. The determining factors in the choice of devices are, from one side the objective of the robot/device assisted therapy and for another side the patient’s characteristics (i.e., residual motor-cognitive functionality, and phase of stroke, subacute or chronic). For devices, the characteristics to consider are the degree of constraint of the machine and the level of movement support, the kind and the scope of feedback interaction, the type of mobilization (distal-proximal or proximal-distal), and whether the robot is unilateral or bilateral. In our view, the matching of patient and device characteristics is the key to a personalized approach to RAAT. Looking to the future, the implementation of virtual reality, artificial intelligence, and wearable sensors, alongside the development of wearable soft-robots and closed-loop systems, could advance the use of RAAT with protocols tailored to individual needs. At the same time the merge of these different technologies will require specific researches to discriminate the combined effect of robotic devices with other systems (virtual reality, feedback, artificial intelligent control) vs. simple robotic devices. Finally, a large multicenter randomized trial with an appropriate stratification of people with stroke functionality for a given robot device to validate the proposed hypotheses is needed.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
GM: Conceptualization, Validation, Writing – original draft. MT: Supervision, Validation, Visualization, Writing – review & editing. SP: Conceptualization, Supervision, Writing – review & editing. AC: Supervision, Writing – review & editing. IC: Supervision, Validation, Writing – review & editing. AMC: Validation, Visualization, Writing – review & editing. MI: Methodology, Supervision, Validation, Visualization, Writing – original draft. RC: Funding acquisition, Methodology, Supervision, Validation, Visualization, Writing – original draft.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
The authors declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Cramer, SC, Sur, M, Dobkin, BH, O'Brien, C, Sanger, TD, Trojanowski, JQ, et al. Harnessing neuroplasticity for clinical applications. Brain. (2011) 134:1591–609. doi: 10.1093/brain/awr039
2. Dimyan, MA, and Cohen, LG. Neuroplasticity in the context of motor rehabilitation after stroke. Nat Rev Neurol. (2011) 7:76–85. doi: 10.1038/nrneurol.2010.200
3. Belda-Lois, JM, Mena-del Horno, S, Bermejo-Bosch, I, Moreno, JC, Pons, JL, Farina, D, et al. Rehabilitation of gait after stroke: a review towards a top-down approach. J Neuroeng Rehabil. (2011) 8:66. doi: 10.1186/1743-0003-8-66
4. Poli, P, Morone, G, Rosati, G, and Masiero, S. Robotic technologies and rehabilitation: new tools for stroke patients' therapy. Biomed Res Int. (2013) 2013:153872. doi: 10.1155/2013/153872
5. Gassert, R, and Dietz, V. Rehabilitation robots for the treatment of sensorimotor deficits: a neurophysiological perspective. J Neuroeng Rehabil. (2018) 15:46. doi: 10.1186/s12984-018-0383-x
6. Zeiler, SR, and Krakauer, JW. The interaction between training and plasticity in the poststroke brain. Curr Opin Neurol. (2013) 26:609–16. doi: 10.1097/WCO.0000000000000025
7. Johnston, M, Pollard, B, Morrison, V, and MacWalter, R. Functional limitations and survival following stroke: psychological and clinical predictors of 3-year outcome. Int J Behav Med. (2004) 11:187–96. doi: 10.1207/s15327558ijbm1104_1
8. Calabrò, RS, Accorinti, M, Porcari, B, Carioti, L, Ciatto, L, Billeri, L, et al. Does hand robotic rehabilitation improve motor function by rebalancing interhemispheric connectivity after chronic stroke? Encouraging data from a randomised-clinical-trial. Clin Neurophysiol. (2019) 130:767–80. doi: 10.1016/j.clinph.2019.02.013
9. Di Carlo, A, Lamassa, M, Franceschini, M, Bovis, F, Cecconi, L, Pournajaf, S, et al. Impact of acute-phase complications and interventions on 6-month survival after stroke. A prospective observational study. PLoS one. (2018) 13:e0194786. doi: 10.1371/journal.pone.0194786
10. De Bartolo, D, Spitoni, GF, Iosa, M, Morone, G, Ciancarelli, I, Paolucci, S, et al. From movement to thought and back: a review on the role of cognitive factors influencing technological neurorehabilitation. Funct Neurol. (2019) 34:131–44.
11. Torrisi, M, Maggio, MG, De Cola, MC, Zichittella, C, Carmela, C, Porcari, B, et al. Beyond motor recovery after stroke: the role of hand robotic rehabilitation plus virtual reality in improving cognitive function. J. Clin. Neurosci. (2021) 92:11–6. doi: 10.1016/j.jocn.2021.07.053
12. Aprile, I, Guardati, G, Cipollini, V, Papadopoulou, D, Mastrorosa, A, Castelli, L, et al. Robotic rehabilitation: an opportunity to improve cognitive functions in subjects with stroke. An explorative study. Front. Neurol. (2020) 11:1498. doi: 10.3389/fneur.2020.588285
13. Bui, KD, Lyn, B, Roland, M, Wamsley, CA, Mendonca, R, and Johnson, MJ. The impact of cognitive impairment on robot-based upper-limb motor assessment in chronic stroke. Neurorehabil Neural Repair. (2022) 36:587–95. doi: 10.1177/15459683221110892
14. Morone, G, Palomba, A, Martino Cinnera, A, Agostini, M, Aprile, I, Arienti, C, et al. Systematic review of guidelines to identify recommendations for upper limb robotic rehabilitation after stroke. Eur J Phys Rehabil Med. (2021) 57:238–45. doi: 10.23736/S1973-9087.21.06625-9
15. Martino Cinnera, A, Palomba, A, Paci, M, Marino, D, LA Rosa, G, Gimigliano, F, et al. A three-year update on guidelines for upper limb robotic rehabilitation after stroke. Eur J Phys Rehabil Med. (2024) 60:556–8. doi: 10.23736/S1973-9087.24.08451-X
16. Rodgers, H, Bosomworth, H, Krebs, HI, van Wijck, F, Howel, D, Wilson, N, et al. Robot assisted training for the upper limb after stroke (RATULS): a multicentre randomised controlled trial. Lancet. (2019) 394:51–62. doi: 10.1016/S0140-6736(19)31055-4
17. Gandolfi, M, Valè, N, Posteraro, F, Morone, G, Dell'orco, A, Botticelli, A, et al. State of the art and challenges for the classification of studies on electromechanical and robotic devices in neurorehabilitation: a scoping review. Eur J Phys Rehabil Med. (2021) 57:831–40. doi: 10.23736/S1973-9087.21.06922-7
18. Mehrholz, J, Pohl, M, Platz, T, Kugler, J, and Elsner, B. Electromechanical and robot-assisted arm training for improving activities of daily living, arm function, and arm muscle strength after stroke. Cochrane Database Syst Rev. (2018) 9:CD006876. doi: 10.1002/14651858.CD006876.pub5
19. Maciejasz, P, Eschweiler, J, Gerlach-Hahn, K, Jansen-Troy, A, and Leonhardt, S. A survey on robotic devices for upper limb rehabilitation. J Neuroeng Rehabil. (2014) 11:3. doi: 10.1186/1743-0003-11-3
20. Hartl, D, de Luca, V, Kostikova, A, Laramie, J, Kennedy, S, Ferrero, E, et al. Translational precision medicine: an industry perspective. J Transl Med. (2021) 19:245. doi: 10.1186/s12967-021-02910-6
21. Morone, G, Bragoni, M, Iosa, M, De Angelis, D, Venturiero, V, Coiro, P, et al. Who may benefit from robotic-assisted gait training? A randomized clinical trial in patients with subacute stroke. Neurorehabil Neural Repair. (2011) 25:636–44. doi: 10.1177/1545968311401034
22. Morone, G, Iosa, M, Bragoni, M, De Angelis, D, Venturiero, V, Coiro, P, et al. Who may have durable benefit from robotic gait training?: a 2-year follow-up randomized controlled trial in patients with subacute stroke. Stroke. (2012) 43:1140–2. doi: 10.1161/STROKEAHA.111.638148
23. Morone, G, Paolucci, S, Cherubini, A, De Angelis, D, Venturiero, V, Coiro, P, et al. Robot-assisted gait training for stroke patients: current state of the art and perspectives of robotics. Neuropsychiatr Dis Treat. (2017) 13:1303–11. doi: 10.2147/NDT.S114102
24. Da Silva-Grigoletto, ME, Pereira-Monteiro, MR, Aragão-Santos, JC, Vasconcelos, ABS, Marcos-Pardo, PJ, and Fortes, LS. Brain functional training: a perspective article. Front. Aging. (2024) 5:1368878. doi: 10.3389/fragi.2024.1368878
25. Micera, S, Caleo, M, Chisari, C, Hummel, FC, and Pedrocchi, A. Advanced Neurotechnologies for the restoration of motor function. Neuron. (2020) 105:604–20. doi: 10.1016/j.neuron.2020.01.039
26. Lambercy, O, Dovat, L, Yun, H, Wee, SK, Kuah, CW, Chua, KS, et al. Effects of a robot-assisted training of grasp and pronation/supination in chronic stroke: a pilot study. J Neuroeng Rehabil. (2011) 8:63. doi: 10.1186/1743-0003-8-63
27. Timmermans, A. A., Lemmens, R. J., Geers, R. P., Smeets, R. J., and Seelen, H. A. (2011). A comparison of treatment effects after sensor- and robot-based task-oriented arm training in highly functional stroke patients. Annual International Conference of the IEEE Engineering in Medicine and Biology Society. Boston, MA, USA: IEEE, 3507–3510.
28. Franceschini, M, Goffredo, M, Pournajaf, S, Paravati, S, Agosti, M, De Pisi, F, et al. Predictors of activities of daily living outcomes after upper limb robot-assisted therapy in subacute stroke patients. PLoS One. (2018) 13:e0193235. doi: 10.1371/journal.pone.0193235
29. Jakob, I, Kollreider, A, Germanotta, M, Benetti, F, Cruciani, A, Padua, L, et al. Robotic and sensor Technology for Upper Limb Rehabilitation. PM R. (2018) 10:S189–97. doi: 10.1016/j.pmrj.2018.07.011
30. Duret, C, Hutin, E, Lehenaff, L, and Gracies, JM. Do all sub acute stroke patients benefit from robot-assisted therapy? A retrospective study. Restor Neurol Neurosci. (2015) 33:57–65. doi: 10.3233/RNN-140418
31. Saita, K, Morishita, T, Hyakutake, K, Ogata, T, Fukuda, H, Kamada, S, et al. Feasibility of robot-assisted rehabilitation in Poststroke recovery of upper limb function depending on the severity. Neurol Med Chir. (2020) 60:217–22. doi: 10.2176/nmc.oa.2019-0268
32. Pila, O, Duret, C, Koeppel, T, and Jamin, P. Performance-based robotic training in individuals with subacute stroke: differences between responders and non-responders. Sensors (Basel). (2023) 23:4304. doi: 10.3390/s23094304
33. Woytowicz, EJ, Rietschel, JC, Goodman, RN, Conroy, SS, Sorkin, JD, Whitall, J, et al. Determining levels of upper extremity movement impairment by applying a cluster analysis to the Fugl-Meyer assessment of the upper extremity in chronic stroke. Arch Phys Med Rehabil. (2017) 98:456–62. doi: 10.1016/j.apmr.2016.06.023
34. Kwakkel, G, Stinear, C, Essers, B, Munoz-Novoa, M, Branscheidt, M, Cabanas-Valdés, R, et al. Motor rehabilitation after stroke: European stroke organisation (ESO) consensus-based definition and guiding framework. Eur Stroke J. (2023) 8:880–94. doi: 10.1177/23969873231191304
35. Morone, G, Spitoni, GF, De Bartolo, D, Ghanbari Ghooshchy, S, Di Iulio, F, Paolucci, S, et al. Rehabilitative devices for a top-down approach. Expert Rev Med Devices. (2019) 16:187–95. doi: 10.1080/17434440.2019.1574567
36. Levin, MF. Can virtual reality offer enriched environments for rehabilitation? Expert Rev Neurother. (2011) 11:153–5. doi: 10.1586/ern.10.201
37. Morone, G, Ghanbari Ghooshchy, S, Palomba, A, Baricich, A, Santamato, A, Ciritella, C, et al. Differentiation among bio- and augmented- feedback in technologically assisted rehabilitation. Expert Rev Med Devices. (2021) 18:513–22. doi: 10.1080/17434440.2021.1927704
38. Mihara, M, Fujimoto, H, Hattori, N, Otomune, H, Kajiyama, Y, Konaka, K, et al. Effect of neurofeedback facilitation on Poststroke gait and balance recovery: a randomized controlled trial. Neurology. (2021) 96:e2587–98. doi: 10.1212/WNL.0000000000011989
39. Pignolo, L, Basta, G, Carozzo, S, Bilotta, M, Todaro, MR, Serra, S, et al. A body-weight-supported visual feedback system for gait recovering in stroke patients: a randomized controlled study. Gait Posture. (2020) 82:287–93. doi: 10.1016/j.gaitpost.2020.09.020
40. Walker, M, Phung, T, Chakraborti, T, Williams, T, and Szafir, D. Virtual, augmented, and mixed reality for human-robot interaction: a survey and virtual design element taxonomy. ACM Trans. Hum. Robot Interact. (2023) 12:1–39. doi: 10.1145/3597623
41. Chheang, V, Lokesh, R, Chaudhari, A, Wang, Q, Baron, L, Kiafar, B, et al. Immersive virtual reality and robotics for upper extremity rehabilitation. arXiv. (2023) arXiv:2304.11110. doi: 10.48550/arXiv.2304.11110
42. Tieri, G, Morone, G, Paolucci, S, and Iosa, M. Virtual reality in cognitive and motor rehabilitation: facts, fiction and fallacies. Expert Rev Med Devices. (2018) 15:107–17. doi: 10.1080/17434440.2018.1425613
43. Buetler, KA, Penalver-Andres, J, Özen, Ö, Ferriroli, L, Müri, RM, Cazzoli, D, et al. "tricking the brain" using immersive virtual reality: modifying the self-perception over embodied avatar influences motor cortical excitability and action initiation. Front Hum Neurosci. (2022) 15:787487. doi: 10.3389/fnhum.2021.787487
44. Hass, J, Blaschke, S, and Herrmann, JM. Cross-modal distortion of time perception: demerging the effects of observed and performed motion. PLoS One. (2012) 7:e38092. doi: 10.1371/journal.pone.0038092
45. Ranzani, R, Lambercy, O, Metzger, JC, Califfi, A, Regazzi, S, Dinacci, D, et al. Neurocognitive robot-assisted rehabilitation of hand function: a randomized control trial on motor recovery in subacute stroke. J Neuroeng Rehabil. (2020) 17:115. doi: 10.1186/s12984-020-00746-7
46. Johansson, H, Folkerts, AK, Hammarström, I, Kalbe, E, and Leavy, B. Effects of motor-cognitive training on dual-task performance in people with Parkinson's disease: a systematic review and meta-analysis. J Neurol. (2023) 270:2890–907. doi: 10.1007/s00415-023-11610-8
47. Kim, J, Rider, JV, Zinselmeier, A, Chiu, YF, Peterson, D, and Longhurst, JK. Dual-task gait has prognostic value for cognitive decline in Parkinson's disease. J. Clin. Neurosci. (2024) 126:101–7. doi: 10.1016/j.jocn.2024.06.006
48. Pang, MYC, Yang, L, Ouyang, H, Lam, FMH, Huang, M, and Jehu, DA. Dual-task exercise reduces cognitive-motor interference in walking and falls after stroke. Stroke. (2018) 49:2990–8. doi: 10.1161/STROKEAHA.118.022157
49. Martino Cinnera, A, Bisirri, A, Leone, E, Morone, G, and Gaeta, A. Effect of dual-task training on balance in patients with multiple sclerosis: a systematic review and meta-analysis. Clin Rehabil. (2021) 35:1399–412. doi: 10.1177/02692155211010372
50. Sun, R, Li, X, Zhu, Z, Li, T, Zhao, M, Mo, L, et al. Effects of dual-task training in patients with post-stroke cognitive impairment: a randomized controlled trial. Front Neurol. (2022) 13:1027104. doi: 10.3389/fneur.2022.1027104
51. DiCarlo, J. A., Gheihman, G., Lin, D. J., & 2019 Northeast Cerebrovascular Consortium Conference Stroke Recovery Workshop Participants. Reimagining stroke rehabilitation and recovery across the care continuum: results from a design-thinking workshop to identify challenges and propose solutions. Arch Phys Med Rehabil. (2021) 102:1645–57. doi: 10.1016/j.apmr.2021.01.074
52. Cramer, SC, Young, BM, Schwarz, A, Chang, TY, and Su, M. Telerehabilitation following stroke. Phys Med Rehabil Clin N Am. (2024) 35:305–18. doi: 10.1016/j.pmr.2023.06.005
53. Lambercy, O, Lehner, R, Chua, K, Wee, SK, Rajeswaran, DK, Kuah, CWK, et al. Neurorehabilitation from a distance: can intelligent technology support decentralized access to quality therapy? Front. Robot. AI. (2021) 8:612415. doi: 10.3389/frobt.2021.612415
54. Conroy, SS, Wittenberg, GF, Krebs, HI, Zhan, M, Bever, CT, and Whitall, J. Robot-assisted arm training in chronic stroke: addition of transition-to-task practice. Neurorehabil Neural Repair. (2019) 33:751–61. doi: 10.1177/1545968319862558
55. Klamroth-Marganska, V, Blanco, J, Campen, K, Curt, A, Dietz, V, Ettlin, T, et al. Three-dimensional, task-specific robot therapy of the arm after stroke: a multicentre, parallel-group randomised trial. Lancet Neurol. (2014) 13:159–66. doi: 10.1016/S1474-4422(13)70305-3
56. Calabrò, RS, Morone, G, Naro, A, Gandolfi, M, Liotti, V, D'aurizio, C, et al. Robot-assisted training for upper limb in stroke (ROBOTAS): an observational, multicenter study to identify determinants of efficacy. J Clin Med. (2021) 10:5245. doi: 10.3390/jcm10225245
57. Morone, G, Capone, F, Iosa, M, Cruciani, A, Paolucci, M, Martino Cinnera, A, et al. May dual transcranial direct current stimulation enhance the efficacy of robot-assisted therapy for promoting upper limb recovery in chronic stroke? Neurorehabil Neural Repair. (2022) 36:800–9. doi: 10.1177/15459683221138743
58. Mark, VW, and Taub, E. Constraint-induced movement therapy for chronic stroke hemiparesis and other disabilities. Restor Neurol Neurosci. (2004) 22:317–36. doi: 10.3233/RNN-2004-00264
59. Barth, J, Geed, S, Mitchell, A, Lum, PS, Edwards, DF, and Dromerick, AW. Characterizing upper extremity motor behavior in the first week after stroke. PLoS One. (2020) 15:e0221668. doi: 10.1371/journal.pone.0221668
60. Allred, RP, Cappellini, CH, and Jones, TA. The “good” limb makes the “bad” limb worse: experience-dependent interhemispheric disruption of functional outcome after cortical infarcts in rats. Behav Neurosci. (2010) 124:124–32. doi: 10.1037/a0018457
61. Lang, CE, Wagner, JM, Edwards, DF, and Dromerick, AW. Upper extremity use in people with hemiparesis in the first few weeks after stroke. J. Neurol. Phys. Ther. (2007) 31:56–63. doi: 10.1097/NPT.0b013e31806748bd
62. Sakabe, N, Altukhaim, S, Hayashi, Y, Sakurada, T, Yano, S, and Kondo, T. Enhanced visual feedback using immersive VR affects decision making regarding hand use with a simulated impaired limb. Front Hum Neurosci. (2021) 15:677578. doi: 10.3389/fnhum.2021.677578
63. Plantin, J, Verneau, M, Godbolt, AK, Pennati, GV, Laurencikas, E, Johansson, B, et al. Recovery and prediction of bimanual hand use after stroke. Neurology. (2021) 97:e706–19. doi: 10.1212/WNL.0000000000012366
64. Patel, P, and Lodha, N. Functional implications of impaired bimanual force coordination in chronic stroke. Neurosci Lett. (2020) 738:135387. doi: 10.1016/j.neulet.2020.135387
65. Gerardin, E, Bontemps, D, Babuin, NT, Herman, B, Denis, A, Bihin, B, et al. Bimanual motor skill learning with robotics in chronic stroke: comparison between minimally impaired and moderately impaired patients, and healthy individuals. J Neuroeng Rehabil. (2022) 19:28. doi: 10.1186/s12984-022-01009-3
66. Iosa, M, Morone, G, Ragaglini, MR, Fusco, A, and Paolucci, S. Motor strategies and bilateral transfer in sensorimotor learning of patients with subacute stroke and healthy subjects. A randomized controlled trial. Eur J Phys Rehabil Med. (2013) 49:291–9.
67. Smyth, C, Broderick, P, Lynch, P, Clark, H, and Monaghan, K. To assess the effects of cross-education on strength and motor function in post stroke rehabilitation: a systematic literature review and meta-analysis. Physiotherapy. (2023) 119:80–8. doi: 10.1016/j.physio.2023.02.001
68. Borghese, NA, Essenziale, J, Mainetti, R, Mancon, E, Pagliaro, R, and Pajardi, G. Hand rehabilitation and telemonitoring through smart toys. Sensors (Basel). (2019) 19:5517. doi: 10.3390/s19245517
69. Qian, Q, Nam, C, Guo, Z, Huang, Y, Hu, X, Ng, SC, et al. Distal versus proximal – an investigation on different supportive strategies by robots for upper limb rehabilitation after stroke: a randomized controlled trial. J Neuroeng Rehabil. (2019) 16:64. doi: 10.1186/s12984-019-0537-5
70. Hsieh, YW, Lin, KC, Wu, CY, Shih, TY, Li, MW, and Chen, CL. Comparison of proximal versus distal upper-limb robotic rehabilitation on motor performance after stroke: a cluster controlled trial. Sci Rep. (2018) 8:2091. doi: 10.1038/s41598-018-20330-3
71. Hung, CS, Lin, KC, Chang, WY, Huang, WC, Chang, YJ, Chen, CL, et al. Unilateral vs bilateral hybrid approaches for upper limb rehabilitation in chronic stroke: a randomized controlled trial. Arch Phys Med Rehabil. (2019) 100:2225–32. doi: 10.1016/j.apmr.2019.06.021
72. Kwakkel, G, Kollen, BJ, and Krebs, HI. Effects of robot-assisted therapy on upper limb recovery after stroke: a systematic review. Neurorehabil Neural Repair. (2008) 22:111–21. doi: 10.1177/1545968307305457
73. Wodu, CO, Sweeney, G, and Kerr, A. Exploring the reasons behind the low focus on upper limb rehabilitation in the early stages after a stroke: a qualitative study. J. Hand Ther. (2024) S0894-1130:00064–4. doi: 10.1016/j.jht.2024.08.005
74. Roux, FE, Djidjeli, I, and Durand, JB. Functional architecture of the somatosensory homunculus detected by electrostimulation. J Physiol. (2018) 596:941–56. doi: 10.1113/JP275243
75. Everard, G, Declerck, L, Detrembleur, C, Leonard, S, Bower, G, Dehem, S, et al. New technologies promoting active upper limb rehabilitation after stroke: an overview and network meta-analysis. Eur J Phys Rehabil Med. (2022) 58:530–48. doi: 10.23736/S1973-9087.22.07404-4
76. Franceschini, M, Mazzoleni, S, Goffredo, M, Pournajaf, S, Galafate, D, Criscuolo, S, et al. Upper limb robot-assisted rehabilitation versus physical therapy on subacute stroke patients: a follow-up study. J Bodyw Mov Ther. (2020) 24:194–8. doi: 10.1016/j.jbmt.2019.03.016
77. Morris, L, Diteesawat, RS, Rahman, N, Turton, A, Cramp, M, and Rossiter, J. The-state-of-the-art of soft robotics to assist mobility: a review of physiotherapist and patient identified limitations of current lower-limb exoskeletons and the potential soft-robotic solutions. J Neuroeng Rehabil. (2023) 20:18. doi: 10.1186/s12984-022-01122-3
78. Faria, AL, Almeida, Y, Branco, D, Câmara, J, Cameirão, M, Ferreira, L, et al. NeuroAIreh@b: an artificial intelligence-based methodology for personalized and adaptive neurorehabilitation. Front Neurol. (2024) 14:1258323. doi: 10.3389/fneur.2023.1258323
79. Morone, G, Iosa, M, Marinozzi, F, D’Antonio, E, Poli, P, Masiero, S, et al. Effectiveness of robotic assisted walking therapy: the role of age and sex. In: W Jensen, O Andersen, and M Akay, editors. Replace, repair, restore, relieve – Bridging clinical and engineering solutions in neurorehabilitation. Biosystems & Biorobotics, vol. 7. Cham: Springer (2014)
80. Lamberti, N, Manfredini, F, Lissom, LO, Lavezzi, S, Basaglia, N, and Straudi, S. Beneficial effects of robot-assisted gait training on functional recovery in women after stroke: a cohort study. Medicina (Kaunas). (2021) 57:1200. doi: 10.3390/medicina57111200
81. Bragoni, M, Broccoli, M, Iosa, M, Morone, G, De Angelis, D, Venturiero, V, et al. Influence of psychologic features on rehabilitation outcomes in patients with subacute stroke trained with robotic-aided walking therapy. Am J Phys Med Rehabil. (2013) 92:e16–25. doi: 10.1097/PHM.0b013e3182a20a34
82. Martino Cinnera, A, Bisirri, A, Chioccia, I, Leone, E, Ciancarelli, I, Iosa, M, et al. Exploring the potential of immersive virtual reality in the treatment of unilateral spatial neglect due to stroke: a comprehensive systematic review. Brain Sci. (2022) 12:1589. doi: 10.3390/brainsci12111589
83. Martino Cinnera, A, Verna, V, Marucci, M, Tavernese, A, Magnotti, L, Matano, A, et al. Immersive virtual reality for treatment of unilateral spatial neglect via eye-tracking biofeedback: RCT protocol and usability testing. Brain Sci. (2024) 14:283. doi: 10.3390/brainsci14030283
84. Iwamoto, Y, Imura, T, Suzukawa, T, Fukuyama, H, Ishii, T, Taki, S, et al. Combination of exoskeletal upper limb robot and occupational therapy improve activities of daily living function in acute stroke patients. J Stroke Cerebrovasc Dis. (2019) 28:2018–25. doi: 10.1016/j.jstrokecerebrovasdis.2019.03.006
85. Garro, F, Chiappalone, M, Buccelli, S, De Michieli, L, and Semprini, M. Neuromechanical biomarkers for robotic neurorehabilitation. Front Neurorobot. (2021) 15:742163. doi: 10.3389/fnbot.2021.742163
86. Calatrava-Nicolás, FM, Gutiérrez-Maestro, E, Bautista-Salinas, D, Ortiz, FJ, González, JR, Vera-Repullo, JA, et al. Robotic-based well-being monitoring and coaching system for the elderly in their daily activities. Sensors (Basel). (2021) 21:6865. doi: 10.3390/s21206865
87. Chen, J, Abbod, M, and Shieh, JS. Pain and stress detection using wearable sensors and devices-a review. Sensors (Basel). (2021) 21:1030. doi: 10.3390/s21041030
Keywords: robotic devices, exoskeleton devices, stroke, rehabilitation, upper extremity
Citation: Morone G, Tramontano M, Paolucci S, Cerasa A, Ciancarelli I, Martino Cinnera A, Iosa M and Calabrò RS (2025) Tailoring robot-assisted arm training to individuals with stroke: bridging neuroscience principles and clinical practice. Front. Neurol. 16:1506889. doi: 10.3389/fneur.2025.1506889
Edited by:
Carlos Luque-Moreno, University of Seville, SpainReviewed by:
Sanaz Pournajaf, IRCCS San Raffaele, ItalyCopyright © 2025 Morone, Tramontano, Paolucci, Cerasa, Ciancarelli, Martino Cinnera, Iosa and Calabrò. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marco Iosa, bS5pb3NhQGhzYW50YWx1Y2lhLml0
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.