 Bertil Delsaut
Bertil Delsaut Anissa Abderrakib2
Anissa Abderrakib2 Noémie Ligot
Noémie Ligot Gilles Naeije
Gilles Naeije- 1Department of Neurology, Tivoli Hospital, La Louvière, Belgium
- 2Department of Neurology, CUB Hôpital Erasme, Université libre de Bruxelles (ULB), Brussels, Belgium
Introduction: Large vessel occlusions (LVO) account for over 60% of stroke-related mortality and disability. Lean body mass (LBM) represents metabolically active body tissue and has been associated with reduced mortality. This study aimed to investigate whether body composition influences LVO stroke perfusion volumes and whether this effect is sex-specific.
Methods: Data were retrospectively collected from all patients admitted between January 2017 and January 2022 with LVO ischemic stroke at the Erasmus Hospital (Brussels), for whom anthropometric and perfusion data were available. Body mass index (BMI) and LBM were calculated using, respectively, the Quetelet’s and the James’ formula. Correlations between body composition and stroke volumes were investigated using Spearman correlations.
Results: A total of 152 patients were included in this study. Mean age 72 ± 14y, female ratio 62.5%, core volume 26 ± 38 mL, penumbra volume 104 ± 61 mL. LBM correlated significantly with stroke volumes (penumbra and core) in the entire group (core: p = 0.001; penumbra: p = 0.001). There was a significant sex-effect, with a significant correlation observed only in women (core: p = 0.008; penumbra: p = 0.007). BMI did not correlate with perfusion volumes at the group level nor at the sex-level.
Conclusion: LBM significantly impacts LVO stroke volumes, but this effect is observed only in women. LBM may serve as a superior indicator of body composition compared to BMI.
Introduction
Large vessel occlusions of the anterior circulation (LVO) account for over 60% of stroke-related mortality and disability (1, 2). In stroke, sexes are not equals. Women bear a disproportionate burden from stroke compared to men: women display higher rates of large territorial infarcts, higher mortality, are less likely to achieve functional independence after ischemic stroke in general and after endovascular treatment (EVT) for LVO in particular. Those differences are not entirely accounted for the average older age at stroke onset, the elevated pre-stroke disability level or the higher prevalence of cardio-embolic stroke that are associated with the female sex (3–5) hinting that sex-specific factors may influence LVO outcomes.
Patients with LVO stand to derive optimal benefit from thrombectomy when presenting with a small core infarction and a substantial volume of salvageable brain tissue at the time of baseline imaging evaluation (6). These conditions exhibit a positive correlation with enhanced collateral circulation at both the arterial and cerebral brain tissue levels (7), thereby underscoring their significant role in predicting favorable outcomes in thrombectomy intervention. In women, a discernible paradox is observed in terms of prognosis following an LVO. Despite exhibiting ostensibly superior collaterals (8), diminished ischemic stroke core volumes and better mismatch ratios (MMR) between penumbra and core volumes compared to their male counterparts (9), the prognostic outcomes for women following an LVO are notably poorer. One underexplored explanation may lie in the difference in body composition between male and female sexes. The body mass, indexed by the body mass index (BMI), is composed of the lean body mass (LBM), that comprises metabolically active tissues, including water, skeletal and smooth muscle mass and bone (10) and the fat mass (FM). Women have a lower proportion of LBM than men. Epidemiologically, an excess of FM is associated with greater cardiovascular morbidity (11) while higher LBM confers lower cardiovascular risk in both sexes (12) and is a protective factor for ischemic stroke (13). However, in female individuals, it has been observed that a heightened level of FM exerts a distinct mitigating effect on cardiovascular disease risk, irrespective of their level of LBM (12). These sex differences may contribute to the obesity paradox found in some studies that described better stroke and cardiovascular outcomes in patients with high BMI (14–17) while others fail to find such association (18). Similarly, in LVO, higher salvageable penumbra brain tissue was associated with a higher BMI in the data from The Acute STroke Registry and Analysis of Lausanne (19). In those studies, BMI was analysed as a whole and no distinctions were made between LBM, FM nor sexes which have blurred potentially relevant associations.
Here, we aimed to clarify the effects of gender and LBM on LVO strokes volumes and outcome in a large cohort of LVO using validated anthropometric prediction equations and perfusion volume assessment.
Subjects and method
Population
The studied population is derived from the stroke registry of Erasmus Hospital in Brussels (Belgium) where all case of acute stroke since January 2015 are recorded, and our analysis included patients admitted between January 2017 and April 2022. The inclusion criteria were as follows: confirmed LVO-stroke, performance of a perfusion-CT during the acute stroke phase, recorded weight and height, and age > 18 years. Data were collected retrospectively from the patients’ medical records.
BMI was calculated using Quetelet’s formula. LBM was determined using James’ formula (20):
Imaging
Pre-interventional imaging included non-contrast CT, CT angiography and CT perfusion (CTP). Ischemic core was defined as brain volume with cerebral blood flow (CBF) under 30% of the CBF of the homologous zone in the contralateral hemisphere. Ischemic penumbra was defined as brain volumes where the Tmax of contrast product arrival exceeded 6 s. Those volume were automatically computed with the Rapid software (21) on which the cut-offs were based on (22).
Statistical analysis
Clinical characteristics were reported using descriptive statistics. Correlations between body composition and stroke volumes were investigated using Spearman correlations. A Linear regression was performed for parameters that correlated with LBM. Finally, to further characterize the relationship between sex, stroke volumes, outcome and LBM, a median-split analysis of the LBM was performed as in (23). For group comparisons, when variables were continuous, a Mann–Whitney U test was applied. When they were discrete, a χ2 test was applied.
Ethics
The study was reviewed and approved by the Ethics Committee of Erasmus Hospital, Route de Lennik, 808, Brussels, Belgium.
Due to the retrospective and non-interventional nature of this study, written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirement of the Ethics Committee of Erasmus Hospital, Route de Lennik, 808, Brussels, Belgium.
All methods were performed in accordance with the relevant guidelines and regulations.
Results
Population
Of an initial population of 310 LVO, 152 patients were included in the final analysis (Figure 1). Mean age of patients was 72 years old (62.5% female). Population characteristics are detailed in Table 1.

Figure 1. Flow chart.

Table 1. Data summary.
Correlations
Significant correlations were observed between LBM and stroke volumes. This correlation between LBM and stroke volumes was sex-specific in the female sex. There was the expected negative correlation between LBM and age. Admission NIHSS was significantly correlated with lean body mass, only in the entire group. These correlations were not observed with BMI or 3 months modified Rankin Score (mRS).
Correlation analysis are summarized in Table 2.
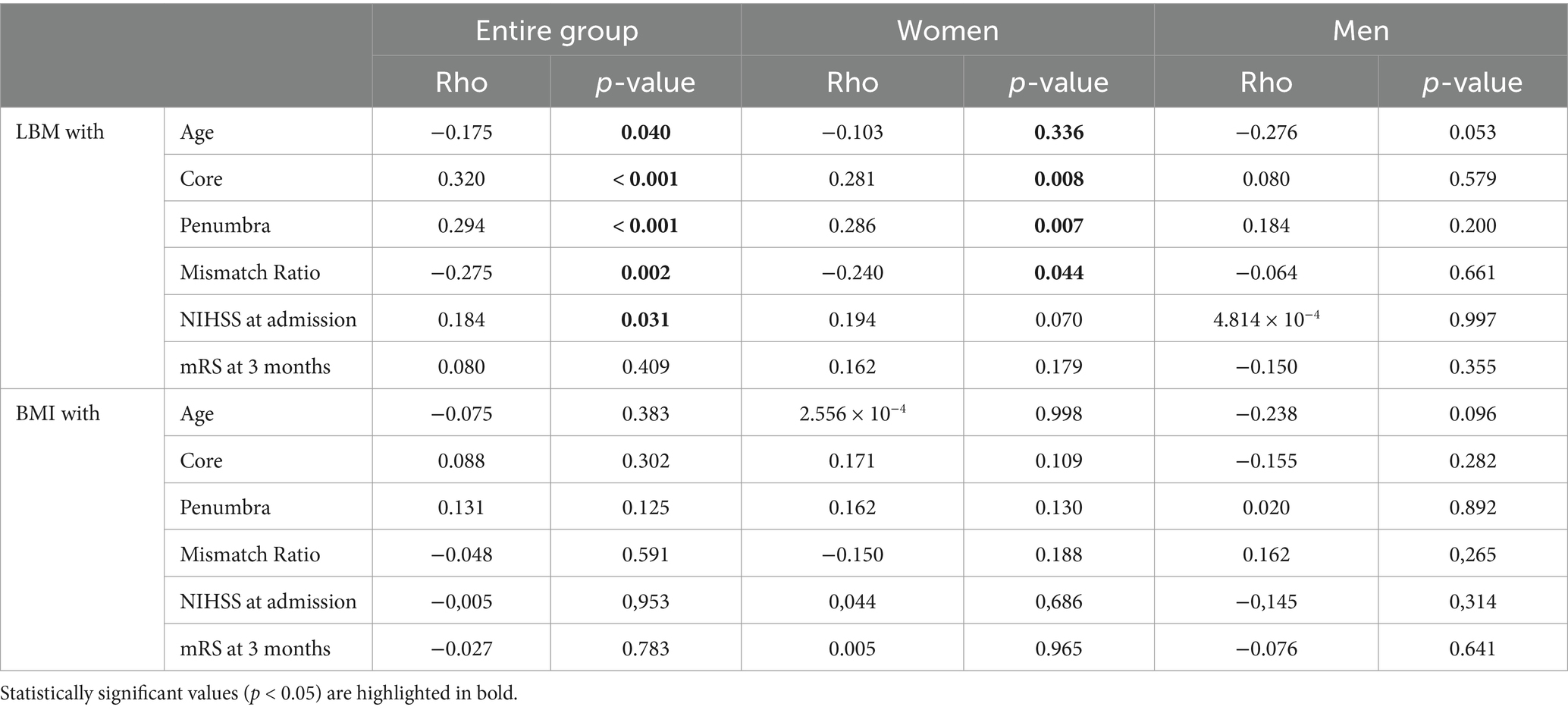
Table 2. Spearman’s correlations between LBM or BMI and age, core, penumbra, mismatch ratio, NIHSS at admission and mRS at 3 months.
Lean body mass median-split
The LBM median split showed that higher LBM is associated to higher stroke volume in women. High LBM in women erases sex-differences in stroke characteristics with similar stroke volumes than men.
Table 3 details the LBM median-split analysis according to sex.
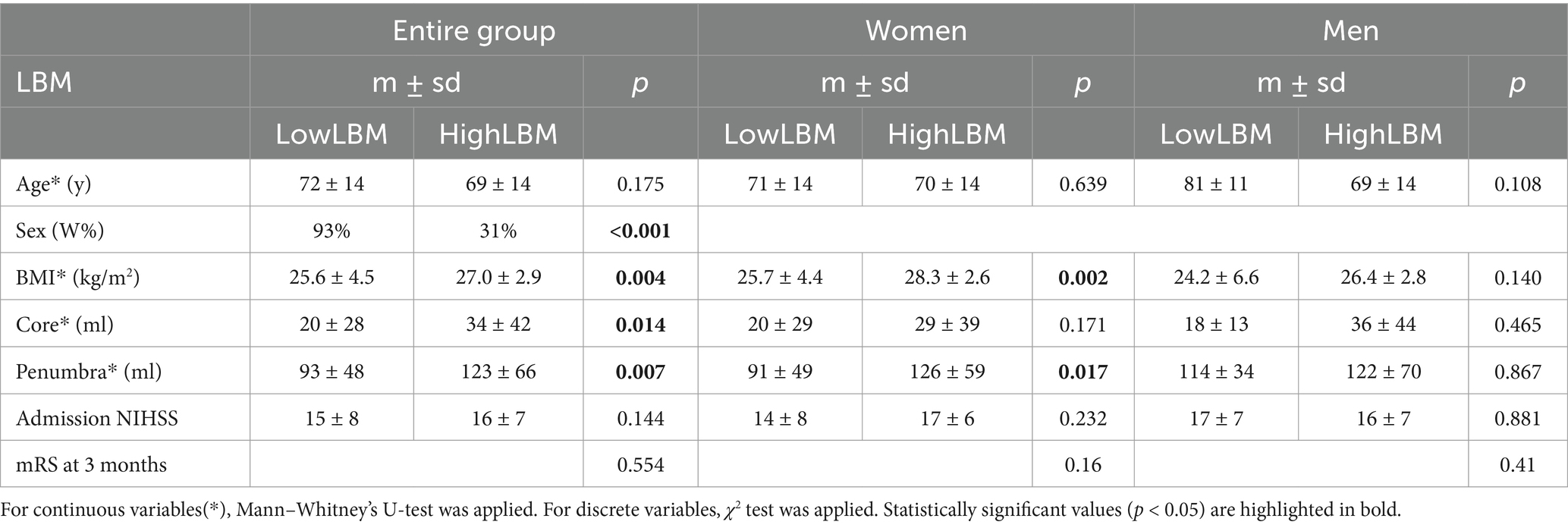
Table 3. Median split according to LBM’s median and comparisons of clinical characteristics.
Linear regressions
Patients with an admission mRS score < 3, anterior LVO, and treated with mechanical thrombectomy were included in this study.
Significant correlations were observed between LBM and stroke volumes in both the entire group and the female subgroup (women’s core: t = 0.042, women’s penumbra: t = 0.005). In this model, LBM explains 6% (R2 entire group = 0.064 - R2 women = 0.096 - R2 men = 0.005) of penumbra’s variability, while age explains only 0.6% (R2 = 0.006) of penumbra’s variability. A variation of 10 kg in LBM correlates with a proportional variation of 17 mL in penumbra.
Linear regressions of stroke volumes by BMI were evaluated. Slope for both penumbra (t = 0.259) and core (t = 0.827) were found to be statistically non-significant.
Figure 2 illustrates the regression curves for LBM and stroke volume.
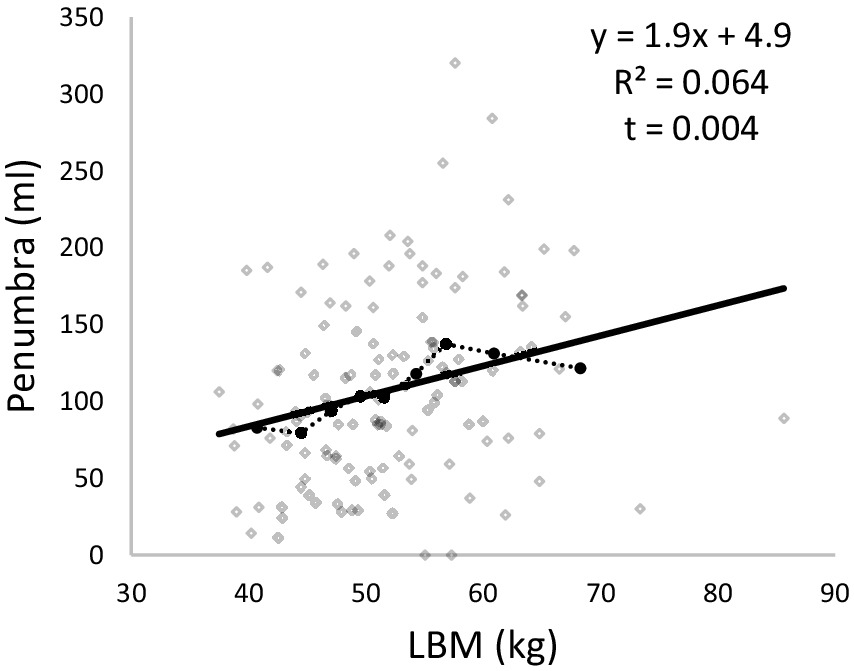
Figure 2. Penumbra according to LBM. In continuous line, regression curve. In dotted line, croissant class of LBM curve.
Discussion
The main findings of this study are that higher LBM is associated with higher stroke volumes in LVO and that the association between LBM and stroke volume is specific of the female sex.
Although based on a monocentric cohort, our findings are likely to be valid in LVO populations. Indeed, our cohort closely matches the clinical characteristics of other large LVO cohorts in term of age, sex, stroke risk factors, admission NIHSS and functional outcomes (1, 24–26). Similarly, perfusion parameters were within the same range in term of core and penumbra volume as in the meta-analysis performed under the HERMES collaboration that pooled patient-level data from all randomized controlled trials that compared endovascular thrombectomy with standard medical therapy (27). Furthermore, the clinical and imaging characteristics from our population also parallels the characteristics from studies that compared LVO perfusion parameters and outcomes in men and women (8, 9, 28, 29). Finally, the LBM values we report in our study correspond to the normative data for 70 years old male and females (30–32). All those facts concur to suggest that our observation apply to LVO cohorts in general.
To the best of our knowledge, no previous studies have evaluated the effect of LBM on LVO clinical and perfusion parameters at the acute phase. The finding that higher LBM is associated with higher stroke volumes seems paradoxical. Indeed increased LBM is associated with lower mortality rates in older individuals (33) as well as to larger brain grey matter volume (34) and lower rates of brain atrophy (35). In LVO, the level of brain atrophy is predictive of futile recanalization (36) and functional outcome (37). So, a variable usually associated with better brain trophicity would be expected to be beneficial instead of detrimental. The reason why LBM is associated with higher LVO stroke volume in women is probably not to be found in brain leptomeningeal collaterality as arterial collaterality scores are better in women than men in LVO (8) but could relate to tissular collaterality issues. Indeed, brain tissular collaterality is reflected by LVO stroke core and penumbra volumes and while women tend to have lower LVO stroke volumes, women with higher LBM in our study showed similar stroke volumes than men. Thus, higher LBM in women seems to erase the sex-effect in LVO stroke volumes. This observation is not due to the age difference between men and women in our study, as regression models showed that LBM explained a ten times higher proportion of penumbra volume variability than age. A possible explanation as to why higher LBM lessens the positive female sex-effect on LVO stroke volumes could relate to blood pressure levels. Increased LBM is positively correlated with elevated mean blood pressure (38, 39). Furthermore, heightened blood pressure levels exhibit an adverse association with functional outcomes following LVO and an augmented burden of white matter lesions (WML). Cerebral blood flow is more impaired with higher burden of WML (40) and WML burden is significantly higher in women compared to men (41). This cascade of events may serve as a circumstantial elucidation for the observed correlation wherein elevated LBM in females correlates with heightened perfusion parameters in both male and female subjects.
Different cerebral self-regulation mechanisms in relation to LBM could also contribute to the sex difference we report. Previous research has reported differences in the adaptability of the cardiovascular system to exercise, particularly in women, that were strongly correlated with LBM (42). Decreased LBM is associated with decreased cardiac output (CO) and increased peripheral vascular resistance, while increased LBM has shown the opposite effects on CO and peripheral vascular resistance (42). This raises the question of whether a similar phenomenon occurs at the intracranial level, influencing the myogenic tone of the arteries. During acute ischaemia, the fall in CBF induces hypoxia which favors vasodilatation, while the fall in pressure causes myogenic vasodilatation (43). In these patients, whose tone is already reduced, additional myogenic vasodilatation could be limited, effectively increasing the penumbra volume. To assess this hypothesis, it would be of interest to evaluate CBF using transcranial Doppler during the acute phase of LVO stroke as well as post-stroke, considering potential gender differences in CBF, and their association with varying levels of LBM.
Finally, BMI, owing to its role in defining obesity, is widely used to describe the weight status of patients. However, its utility is limited when it comes to assessing stroke volume or predicting the functional outcome of patients. This limitation may be attributed, at least in part, to the lack of representativeness of body composition in its calculation (44).The use of LBM could potentially serve as a more suitable tool for assessing body composition in stroke patients. One could object that in our study, we used James’ equation to compute LBM and not Dual X-ray Absorptiometry (DXA) that is the gold-standard to assess body composition. However, DXA is not suited for acute stroke settings and LBM estimation equations, such as James’, displays 0.948 Pearson rank correlation with DXA measures (45) suggesting that LBM equation are effective surrogates to estimate LBM.
In summary, we showed that LBM has a sex specific effect on LVO stroke volumes in women. This observation warrants further studies to understand the pathophysiology behind this association and help understand why women fare worse after an LVO stroke than men in order to provide tailored care.
Data availability statement
Data can be shared upon reasonable request. Requests to access the data should be directed to Gilles Naeije (Z2lsbGVzLm5hZWlqZUBodWJydXhlbGxlcy5iZQ==).
Ethics statement
The studies involving humans were approved by Comité d’éthique de l’Hôpital Erasme-Bruxelles. The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because this study is a retrospective study.
Author contributions
BD: Conceptualization, Formal analysis, Investigation, Methodology, Visualization, Writing – original draft. AA: Writing – review & editing. NL: Writing – review & editing. GN: Conceptualization, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Malhotra, K, Gornbein, J, and Saver, JL. Ischemic strokes due to large-vessel occlusions contribute disproportionately to stroke-related dependence and death: a review. Front Neurol. (2017) 8:651. doi: 10.3389/fneur.2017.00651
2. Smith, WS, Lev, MH, English, JD, Camargo, EC, Chou, M, Johnston, SC, et al. Significance of large vessel intracranial occlusion causing acute ischemic stroke and TIA. Stroke. (2009) 40:3834–40. doi: 10.1161/STROKEAHA.109.561787
3. Benjamin, EJ, Muntner, P, Alonso, A, Bittencourt, MS, Callaway, CW, Carson, AP, et al. Heart disease and stroke statistics—2019 update: a report from the American Heart Association. Circulation. (2019) 139:e56–e528. doi: 10.1161/CIR.0000000000000659
4. Reeves, MJ, Bushnell, CD, Howard, G, Gargano, JW, Duncan, PW, Lynch, G, et al. Sex differences in stroke: epidemiology, clinical presentation, medical care, and outcomes. Lancet Neurol. (2008) 7:915–26. doi: 10.1016/S1474-4422(08)70193-5
5. Gall, S, Phan, H, Madsen, TE, Reeves, M, Rist, P, Jimenez, M, et al. Focused update of sex differences in patient reported outcome measures after stroke. Stroke. (2018) 49:531–5. doi: 10.1161/STROKEAHA.117.018417
6. Warach, SJ, Luby, M, Albers, GW, Bammer, R, Bivard, A, Campbell, BCV, et al. Acute stroke imaging research roadmap III imaging selection and outcomes in acute stroke reperfusion clinical trials: consensus recommendations and further research priorities. Stroke. (2016) 47:1389–98. doi: 10.1161/STROKEAHA.115.012364
7. Faizy, TD, Kabiri, R, Christensen, S, Mlynash, M, Kuraitis, GM, Broocks, G, et al. Favorable venous outflow profiles correlate with favorable tissue-level collaterals and clinical outcome. Stroke. (2021) 52:1761–7. doi: 10.1161/STROKEAHA.120.032242
8. Lagebrant, C, Ramgren, B, Hassani Espili, A, Marañon, A, and Kremer, C. Sex differences in collateral circulation and outcome after mechanical Thrombectomy in acute ischemic stroke. Front Neurol. (2022) 13:878759. doi: 10.3389/fneur.2022.878759
9. Dula, AN, Mlynash, M, Zuck, ND, Albers, GW, and Warach, SJfor the DEFUSE 3 Investigators. Neuroimaging in ischemic stroke is different between men and women in the DEFUSE 3 cohort. Stroke. (2020) 51:481–8. doi: 10.1161/STROKEAHA.119.028205
10. Merchant, RA, Seetharaman, S, Au, L, Wong, MWK, Wong, BLL, Tan, LF, et al. Relationship of fat mass index and fat free mass index with body mass index and association with function, cognition and sarcopenia in pre-frail older adults. Front Endocrinol. (2021) 12:765415. doi: 10.3389/fendo.2021.765415
11. Wilczyński, J, Mierzwa-Molenda, M, and Habik-Tatarowska, N. Differences in body composition among patients after hemorrhagic and ischemic stroke. IJERPH. (2020) 17:4170. doi: 10.3390/ijerph17114170
12. Srikanthan, P, Horwich, TB, Calfon Press, M, Gornbein, J, and Watson, KE. Sex differences in the Association of Body Composition and Cardiovascular Mortality. JAHA. (2021) 10:e017511. doi: 10.1161/JAHA.120.017511
13. Larsson, SC, Bäck, M, Rees, JMB, Mason, AM, and Burgess, S. Body mass index and body composition in relation to 14 cardiovascular conditions in UK biobank: a Mendelian randomization study. Eur Heart J. (2020) 41:221–6. doi: 10.1093/eurheartj/ehz388
14. Chaudhary, D, Khan, A, Gupta, M, Hu, Y, Li, J, Abedi, V, et al. Obesity and mortality after the first ischemic stroke: is obesity paradox real? PLoS One. (2021) 16:e0246877. doi: 10.1371/journal.pone.0246877
15. Oesch, L, Tatlisumak, T, Arnold, M, and Sarikaya, H. Obesity paradox in stroke – myth or reality? A systematic review. PLoS One. (2017) 12:e0171334. doi: 10.1371/journal.pone.0171334
16. Kim, BJ, Lee, SH, Jung, KH, Yu, KH, Lee, BC, and Roh, JK. Dynamics of obesity paradox after stroke, related to time from onset, age, and causes of death. Neurology. (2012) 79:856–63. doi: 10.1212/WNL.0b013e318266fad1
17. Sang-Hun, L, Jin-Man, J, and Park, M-H. Obesity paradox and stroke outcomes according to stroke subtype: a propensity score-matched analysis. Int J Obes. (2023) 47:669–76. doi: 10.1038/s41366-023-01318-0
18. Hoffman, H, Cote, JR, Wood, J, Jalal, MS, Draytsel, DY, and Gould, GC. The influence of body mass index on outcomes in patients undergoing mechanical Thrombectomy for anterior circulation large vessel occlusion: institutional experience and Meta-analysis. Neurocrit Care. (2023) 40:654–63. doi: 10.1007/s12028-023-01801-6
19. Sirimarco, G, Strambo, D, Nannoni, S, Labreuche, J, Cereda, C, Dunet, V, et al. Predicting penumbra salvage and infarct growth in acute ischemic stroke: a multifactor survival game. J Clin Med. (2023) 12:4561. doi: 10.3390/jcm12144561
20. James, WPT. Research on obesity: A report of the DHSS/MRC Group. London: Her Majesty’s Stationery Office (1976).
21. Austein, F, Riedel, C, Kerby, T, Meyne, J, Binder, A, Lindner, T, et al. Comparison of perfusion CT software to predict the final infarct volume after Thrombectomy. Stroke. (2016) 47:2311–7. doi: 10.1161/STROKEAHA.116.013147
22. Albers, GW, Marks, MP, Kemp, S, Christensen, S, Tsai, JP, Ortega-Gutierrez, S, et al. Thrombectomy for stroke at 6 to 16 hours with selection by perfusion imaging. N Engl J Med. (2018) 378:708–18. doi: 10.1056/NEJMoa1713973
23. Naeije, G, Wens, V, Coquelet, N, Sjøgård, M, Goldman, S, Pandolfo, M, et al. Age of onset determines intrinsic functional brain architecture in Friedreich ataxia. Ann Clin Transl Neurol. (2020) 7:94–104. doi: 10.1002/acn3.50966
24. Thijs, VN, Lansberg, MG, Beaulieu, C, Marks, MP, Moseley, ME, and Albers, GW. Is early ischemic lesion volume on diffusion-weighted imaging an independent predictor of stroke outcome?: a multivariable analysis. Stroke. (2000) 31:2597–602. doi: 10.1161/01.STR.31.11.2597
25. Sipilä, JOT. Anterior circulation large vessel occlusion outcomes in patients transferred from a peripheral primary stroke Centre. Neurol Res. (2022) 44:554–9. doi: 10.1080/01616412.2021.2024727
26. Shi, Z, Li, J, Zhao, M, Zhang, M, Wang, T, Chen, L, et al. Baseline cerebral ischemic Core quantified by different automatic software and its predictive value for clinical outcome. Front Neurosci. (2021) 15:608799. doi: 10.3389/fnins.2021.608799
27. Campbell, BCV, Majoie, CBLM, Albers, GW, Menon, BK, Yassi, N, Sharma, G, et al. Penumbral imaging and functional outcome in patients with anterior circulation ischaemic stroke treated with endovascular thrombectomy versus medical therapy: a meta-analysis of individual patient-level data. Lancet Neurol. (2019) 18:46–55. doi: 10.1016/S1474-4422(18)30314-4
28. Madsen, TE, DeCroce-Movson, E, Hemendinger, M, McTaggart, RA, Yaghi, S, Cutting, S, et al. Sex differences in 90-day outcomes after mechanical thrombectomy for acute ischemic stroke. J NeuroIntervent Surg. (2019) 11:221–5. doi: 10.1136/neurintsurg-2018-014050
29. Sun, D, Raynald,, Huo, X, Jia, B, Tong, X, Ma, G, et al. Sex-related differences in outcomes of endovascular treatment for anterior circulation large vessel occlusion. Stroke. (2023) 54:327–36. doi: 10.1161/STROKEAHA.122.041195
30. Kirk, B, Bani Hassan, E, Brennan-Olsen, S, Vogrin, S, Bird, S, Zanker, J, et al. Body composition reference ranges in community-dwelling adults using dual-energy X-ray absorptiometry: the Australian body composition (ABC) study. J Cachexia Sarcopenia Muscle. (2021) 12:880–90. doi: 10.1002/jcsm.12712
31. Mitchell, SJ, Kirkpatrick, CMJ, le Couteur, DG, Naganathan, V, Sambrook, PN, Seibel, MJ, et al. Estimation of lean body weight in older community-dwelling men. Br J Clin Pharmacol. (2010) 69:118–27. doi: 10.1111/j.1365-2125.2009.03586.x
32. Coin, A, Sergi, G, Minicuci, N, Giannini, S, Barbiero, E, Manzato, E, et al. Fat-free mass and fat mass reference values by dual-energy X-ray absorptiometry (DEXA) in a 20–80 year-old Italian population. Clin Nutr. (2008) 27:87–94. doi: 10.1016/j.clnu.2007.10.008
33. Han, SS, Kim, KW, Kim, KI, Na, KY, Chae, DW, Kim, S, et al. Lean mass index: a better predictor of mortality than body mass index in elderly Asians: lean mass index and mortality. J Am Geriatr Soc. (2010) 58:312–7. doi: 10.1111/j.1532-5415.2009.02672.x
34. Croll, PH, Bos, D, Ikram, MA, Rivadeneira, F, Voortman, T, and Vernooij, MW. Body composition is not related to structural or vascular brain changes. Front Neurol. (2019) 10:559. doi: 10.3389/fneur.2019.00559
35. Yu, JH, Kim, REY, Jung, JM, Park, SY, Lee, DY, Cho, HJ, et al. Sarcopenia is associated with decreased gray matter volume in the parietal lobe: a longitudinal cohort study. BMC Geriatr. (2021) 21:622. doi: 10.1186/s12877-021-02581-4
36. Pedraza, MI, de Lera, M, Bos, D, Calleja, AI, Cortijo, E, Gómez-Vicente, B, et al. Brain atrophy and the risk of futile endovascular reperfusion in acute ischemic stroke. Stroke. (2020) 51:1514–21. doi: 10.1161/STROKEAHA.119.028511
37. Diprose, WK, Diprose, JP, Wang, MTM, Tarr, GP, McFetridge, A, and Barber, PA. Automated measurement of cerebral atrophy and outcome in endovascular Thrombectomy. Stroke. (2019) 50:3636–8. doi: 10.1161/STROKEAHA.119.027120
38. Li, S, Jiao, H, Yang, J, Li, Y, Zhang, J, Liu, X, et al. Association between lean body mass and hypertension: a cross-sectional study of 50 159 NHANES participants. J Clinical Hypertens. (2023) 25:957–64. doi: 10.1111/jch.14710
39. Korhonen, PE, Mikkola, T, Kautiainen, H, and Eriksson, JG. Both lean and fat body mass associate with blood pressure. Eur J Intern Med. (2021) 91:40–4. doi: 10.1016/j.ejim.2021.04.025
40. Shi, Y, Thrippleton, MJ, Makin, SD, Marshall, I, Geerlings, MI, de Craen, AJM, et al. Cerebral blood flow in small vessel disease: a systematic review and meta-analysis. J Cereb Blood Flow Metab. (2016) 36:1653–67. doi: 10.1177/0271678X16662891
41. Alqarni, A, Jiang, J, Crawford, JD, Koch, F, Brodaty, H, Sachdev, P, et al. Sex differences in risk factors for white matter hyperintensities in non-demented older individuals. Neurobiol Aging. (2021) 98:197–204. doi: 10.1016/j.neurobiolaging.2020.11.001
42. Diaz-Canestro, C, Tse, HF, Yiu, KH, and Montero, D. Reduced lean body mass: a potential modifiable contributor to the pathophysiology of heart failure. Eur Heart J. (2023) 44:1386–8. doi: 10.1093/eurheartj/ehad130
43. Cipolla, MJ. The cerebral circulation. San Rafael (CA): Morgan & Claypool Life Sciences (2009) Chapter 4, Regulation of Cerebrovascular Tone.
44. Koh, IS, Minn, YK, and Suk, SH. Body fat mass and risk of cerebrovascular lesions: the PRESENT (prevention of stroke and dementia) project. IJERPH. (2019) 16:2840. doi: 10.3390/ijerph16162840
Keywords: ischemic stroke, lean body mass, sex, core, penumbra
Citation: Delsaut B, Abderrakib A, Ligot N and Naeije G (2025) Lean body mass and stroke volume, a sex issue. Front. Neurol. 15:1443356. doi: 10.3389/fneur.2024.1443356
Edited by:
Jean-Claude Baron, University of Cambridge, United KingdomCopyright © 2025 Delsaut, Abderrakib, Ligot and Naeije. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bertil Delsaut, YmVydGlsLmRlbHNhdXRAZXBpY3VyYS5iZQ== Gilles Naeije, Z2lsbGVzLm5hZWlqZUBodWJydXhlbGxlcy5iZQ==
†Present address: Bertil Delsaut,Department of Neurology, Epicura Hospital, Hornu, Belgium
†ORCID: Bertil Delsaut, orcid.org/0009-0006-8798-1017