 Çetin Kürşad Akpınar1
Çetin Kürşad Akpınar1 Erdem Gurkas2
Erdem Gurkas2 Atilla Ozcan Ozdemir3
Atilla Ozcan Ozdemir3 Hasan Doğan1*Ayşenur Önalan2Serhan Yıldırım4Zülfikar Memiş5Emrah Aytaç6Bilgehan Atılgan Acar7Muhammed Nur Öğün8
Hasan Doğan1*Ayşenur Önalan2Serhan Yıldırım4Zülfikar Memiş5Emrah Aytaç6Bilgehan Atılgan Acar7Muhammed Nur Öğün8 Özlem Aykaç3
Özlem Aykaç3 Zehra Uysal Kocabaş3Türkan Acar7Halil Alper Eryılmaz7Berkhan Topaktaş9
Zehra Uysal Kocabaş3Türkan Acar7Halil Alper Eryılmaz7Berkhan Topaktaş9- 1Samsun Tranining and Research Hospital, Stroke Center, Department of Neurology, Samsun University, Samsun, Türkiye
- 2Kartal Dr. Lütfi Kırdar City Hospital, Stroke Center, Department of Neurology, Health Sciences University, İstanbul, Türkiye
- 3Eskisehir Osmangazi University Hospital, Stroke Center, Department of Neurology, Eskişehir Osmangazi University, Eskişehir, Türkiye
- 4Kocaeli City Hospital, Stroke Center, Kocaeli, Türkiye
- 5Haseki Training and Research Hospital, Stroke Center, Department of Neurology, Health Sciences University, İstanbul, Türkiye
- 6Fırat University Hospital, Stroke Center, Department of Neurology, Elazığ, Türkiye
- 7Sakarya University Hospital, Stroke Center, Department of Neurology, Sakarya, Türkiye
- 8Abant İzzet Baysal University Hospital, Stroke Center, Department of Neurology, Bolu, Türkiye
- 9Department of Public Health, Amasya University, Amasya, Türkiye
Introduction: While the Thrombite device differs from the Solitare stent with its Helical open-side structure feature, it shows great similarity with its other features. We assessed the Thrombite device’s effectiveness and safety in this study.
Materials and methods: The study was a retrospective analysis of patients who were included in the Turkish Interventional Neurology database and who had mechanical thrombectomy with the Thrombite device as the first choice between January 2020 and January 2023. The type of study is descriptive research.
Result: Using the Thrombite thrombectomy device, 525 patients received treatment. The median baseline National Institutes of Health Stroke Scale (NIHSS) score was 13, the median initial Alberta Stroke Program Early Computed Tomography (ASPECT) score was 8, and the mean patient age was 68.6+11.7 years. Between the groin puncture and the successful recanalization, the median time was 34 minutes (interquartile range [IQR]: 15–45). 48.2% (modified treatment in cerebral infarction; mTICI) 2b/3% and 33.9% (mTICI 2c/3) were the first-pass recanalization rates. In the end, 87.7% of patients had effective recanalization (thrombolysis in cerebral infarction 2b/3). In the “first-pass” subgroup, the favorable functional result (modified Rankin Scale 0–2) was 51.8%, while it was 41.6% for the entire patient population. The rate of embolization into new territory/different territory were 2.1/0.1%. 23 patients (4.5%) had symptomatic hemorrhage.
Conclusion: The Thrombite device showed a good safety profile and high overall successful recanalization rates in our experience.
Introduction
The aim of mechanical thrombectomy is to open the vessel quickly and at one time and achieve a successful clinical outcome. Tortuosity of the aortic and/or supra-aortic vessels, the number of passes, clot characteristics and clot load, the techniques and materials used, and the experience of the surgeon affect the rate of vessel opening and clinical outcome (1, 2). An isolated stent retriever, ADAPT, or combined technique can be used as a mechanical thrombectomy technique (3). In randomized clinical studies using third-generation stent retriever devices, both high vessel opening rates (up to 58.7%–88%) and successful clinical outcome rates (32.6%–71.4%) could be achieved (4, 5). In retrospective studies, the rate of opening the vessel with a stent retriever has increased to 97% (6). Also, in studies conducted with 3rd generation thrombectomy devices with different design structures, high vessel opening rates of up to 90–96% have been reported (7–11). The Thrombite device is featured with an S-shaped helical open-side structure, overlapping design, and self-expanding feature, which aims to obtain more efficient clot removal and a higher acute recanalization rate. In the pre-marketing study of the Thrombite device, the acute recanalization rate was reported as 86.5% and 92.3% before and after angioplasty, and the symptomatic intracranial hemorrhage (sICH) within 24 h was as low as 1.9% (12). Our objective in this study is to present the outcomes of patients included in the Turkish Interventional Neurology database who had mechanical thrombectomy with the Thrombite device as the first option.
Methods
Six stroke sites were identified using prospective data collection from the Interventional Neurology Database between January 2020 and January 2023. We performed a retrospective analysis on 505 consecutive LVO stroke patients. who underwent thrombectomy using a first-line Thrombite device. Patient demographic information, risk factors, procedural details were saved. The type of study is descriptive research.
Each participating site’s institutional review board or ethics committee accepted the study protocol. Prior to enrollment, each patient or their legal representative gave written consent.
Imaging and patient selection
The study comprised individuals with LVO stroke who were 18 to 96 years old. Noncontrast computed tomography (CT) and contrast-enhanced neck-brain CT angiography were used to confirm LVO. Patients with intracranial hemorrhage were excluded from the study
We established inclusion criteria as follows: pre-stroke modified Rankin Scale (mRS) of 0–1, Alberta Stroke Program Early Computed Tomography (ASPECT) score above 4, angiographically verified LVO in the anterior system, and baseline National Institutes of Health Stroke Scale (NIHSS) score of 4–25. Mechanical thrombectomy was carried out on eligible patients within six hours after the beginning of symptoms (13). Intravenous (IV) tissue-type plasminogen activator (tPA) was given to patients who arrived within 4.5 hours. Patients undergoing CT perfusion were excluded from the study.
Clinical assessment
Modified thrombolysis in cerebral infarction (mTICI) 2b-3 was used to determine successful recanalization. The mRS was determined at 90 days from discharge. A follow-up CT scan performed within the first 24 hours was used to evaluate the existence of intracerebral bleeding (hemorrhagic infarction type 1, hemorrhagic infarction type 2, parenchymal hematoma type 1, and parenchymal hematoma type 2).
Thrombectomy device
Different sizes of the Thrombite™ thrombectomy device are available to accommodate varying anatomical and procedural constraints.
The Thrombite™ “3 mm (3 × 15, 3 × 20, 3 × 25, 3 × 30 mm) and 4 mm (4 × 15, 4 × 20, 4 × 25, 4 × 30” sizes are compatible with microcatheters with a minimum internal diameter of 0.021 inch.
The Thrombite™ “5 mm (5 × 15, 5 × 20, 5 × 25, 5 × 30 mm) and 6 mm (6 × 15, 6 × 20, 6 × 25, 6 × 30” sizes are compatible with microcatheters with a minimum internal diameter of 0.027 inch. In our series, the Headway 21–27 catheter (MicroVention, Valencia, USA) and the excelsior 27 catheter (Stryker Neurovascular, California, USA) were routinely used with all sizes.
The Thrombite™ device is intended for more effective clot removal and optimal revascularization in a variety of vessels. It has an S-shaped helical open-side structure and an overlapped stent that effectively entwine and clamp the clot, assure clot retention, and increase contact surface with thrombus.
A new generation of stent retrievers, the Thrombite has a hybrid closed and open cell architecture that forms a spiral opening along the tubular surface of the device in a longitudinal configuration.
Thrombectomy technique
Depending on the stroke patient’s health, either local anesthetic or conscious sedation was used throughout the treatment.
For access and flow control in the anterior circulation LVO, either proximal flow arrest or mixed aspiration techniques were applied. Under proximal flow arrest, the Thrombite™ thrombectomy device (Stryker Neurovascular, California, USA) was utilized alone in certain instances. When it was possible to advance the Terumo Destination (Terumo, Shibuya-ku, Japan) into the ICA or the Common carotid artery (CCA), combined aspiration using the Thrombite™ device (Solumbra technique or ADVANCE technique) and a 5 Fr or 6 Fr large-bore catheter was carried out. Depending on the stroke patient’s neurological status, either local anesthetic or conscious sedation was used throughout the treatment.
There were three methods employed: aspiration with large-diameter aspiration catheters, thrombectomy using stent retrievers, or a combination of stent and aspiration approaches.
Using the Thrombite™ thrombectomy device, up to three passes were permitted during the procedure. In the event that effective recanalization was not possible, rescue therapy was permitted. The use of an alternative method (ADAPT), an alternative device (Trevo, EmboTrap, Neva, etc.), balloon angioplasty, or permanent stenting were all considered forms of rescue therapy.
Statistical analysis
Following encoding, the data were loaded into the SPSS (Version 22 for Windows, SPSS Inc., Chicago, IL, USA) application for analysis. Data with a normal distribution were represented as mean (standard deviation) for continuous variables, whereas data with an irregular distribution were represented as median (interquartile range) for continuous variables and frequency (%) for categorical variables.
Results
From January 2020 to January 2023, a total of 575 patients—245 men (48.5%) and 260 women (51.5%)—were treated with Thrombite™, the first-line thrombectomy device. The baseline NIHSS was 14.7 ± 5.1, and the mean age was 68.6 ± 11.7 years. Initial ASPECT score median was 7 (IQR: 5–9). Out of the 505 patients, 105 patients (38.6%) had IV tPA prior to endovascular surgery. We found that 213 patients (42.2%) had M1 occlusion, 127 patients (25.1%) had M2 occlusion, 55 patients (10.9%) had tandem ICA–MCA occlusion, 101 patients (20%) had carotid I, L, and T occlusion, and 9 patients (1.8%) had anterior cerebral artery A1 occlusion. Table 1 summarizes the baseline and demographic features of the patient.
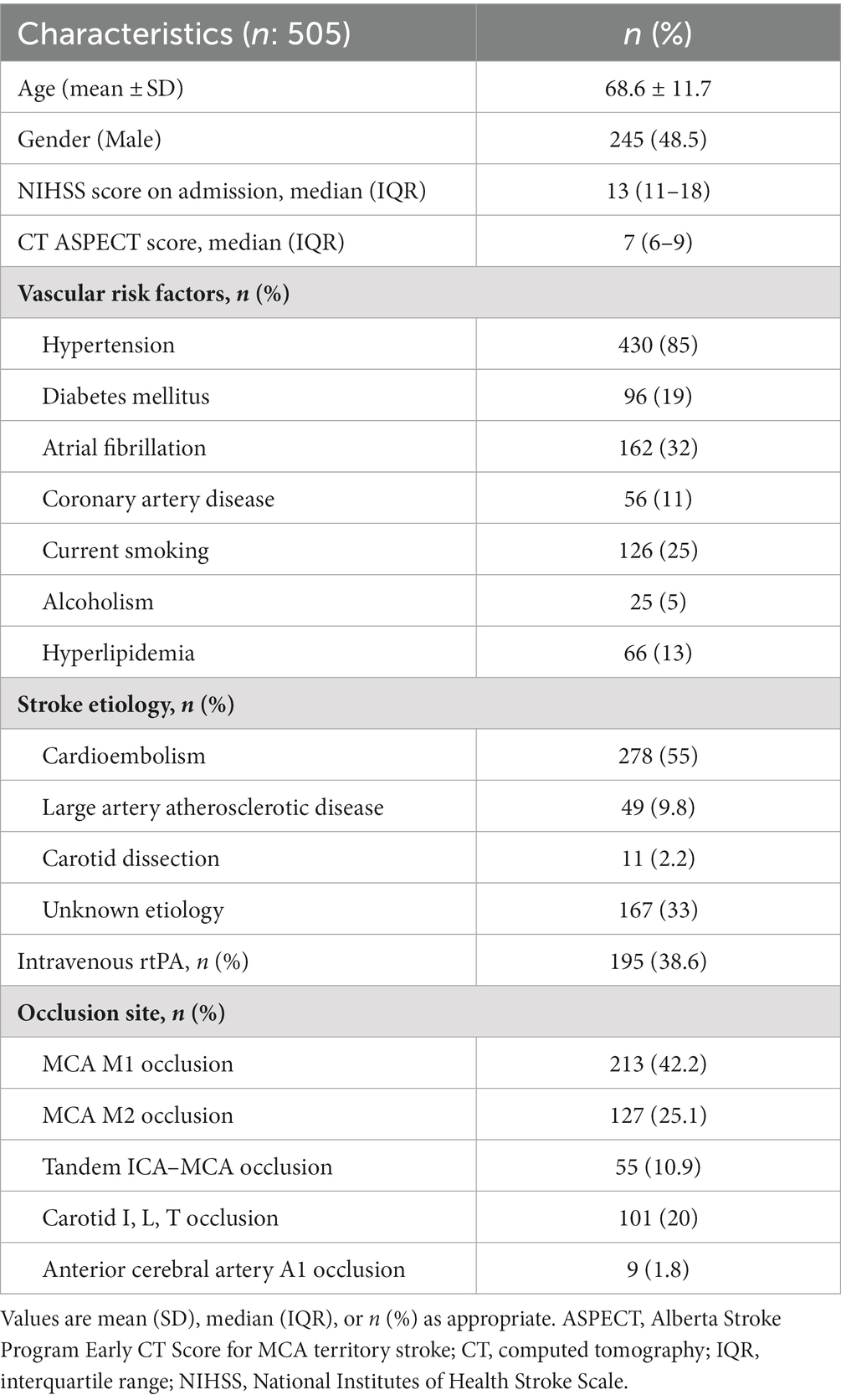
Table 1. Baseline characteristics of patients.
A groin puncture was performed on average 215 (IQR:155-325) minutes after the last known well or the symptom onset.
A successful recanalization occurred after a groin puncture in 29 (IQR/15-65) minutes on average.
In 48.1% of cases, first-pass recanalization was successful (mTICI 2b/3) and in 33.9% of cases, it was exceptional (mTICI 2c/3). Forty-seven percent of patients (443/505) had successful final recanalization (mTICI 2b/3). The mTICI scores of these patients were 3, 2c, and 2b for 21.6%, 31.5%, and 34.7% of the patients, respectively. Table 2 provides a summary of the reperfusion result.
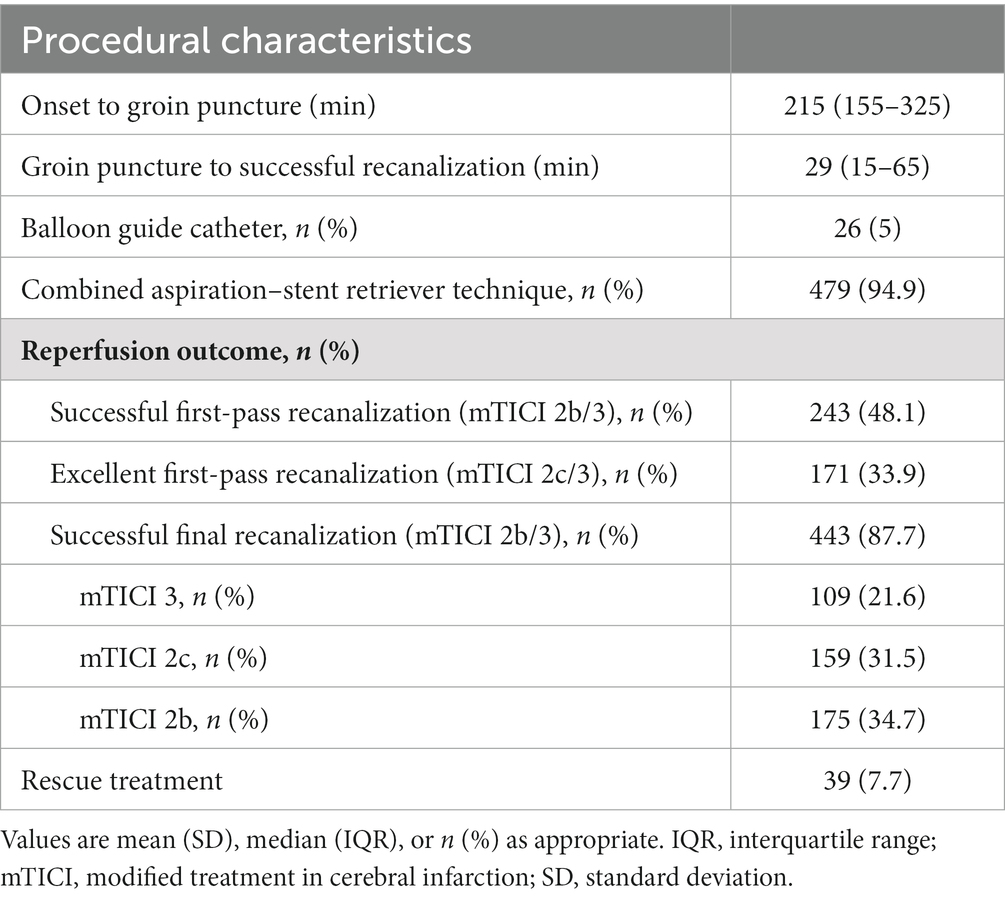
Table 2. Details of endovascular treatment.
In 94.9% of patients, the combined aspiration–stent retriever approach was employed, whereas 5.1% of patients underwent BGC. 39 patients (7.7%) required rescue therapy. In these patients, either trombectomy technique or stentretriever device change was performed.
Complications
The rate of embolization into new territory was 2.2%. A total of 165 (32.7%) patients had ICH in brain CT at 24th hour. SICH (type 2 parenchymal hematoma) occured in 23 (4.6%) patients. Type 1 parenchymal hematoma was present in thirty-three patients (6.5%), petechial type 1 hemorrhage was present in 39 patients (7.7%), and petechial type 2 hemorrhage was present in 61 patients (12.1%).
A total of 165 (32.7%) patients had ICH in brain CT at the 24th hour. SICH (type 2 parenchymal hematoma) occurred in 23 (4.6%) patients (Table 3).
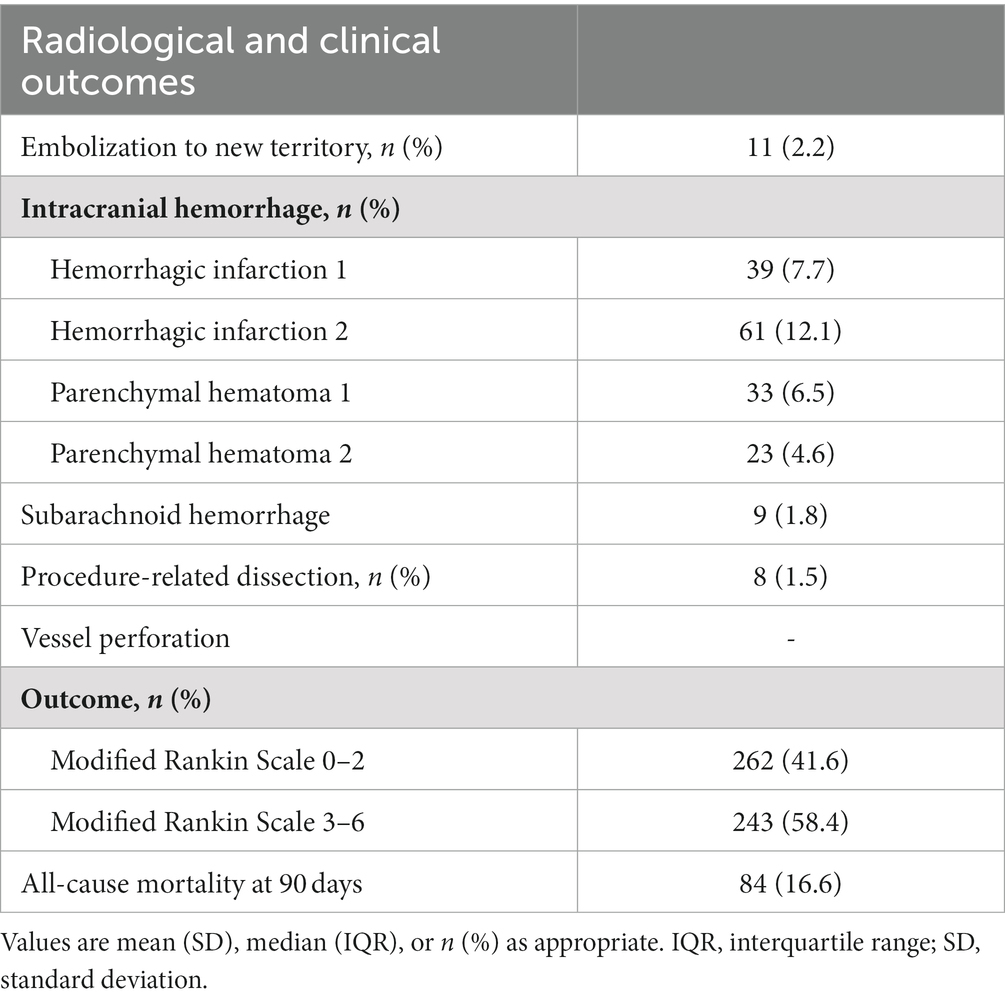
Table 3. Endovascular complications and clinical outcome.
Thirty-three patients (6.5%) had type 1 parenchymal hematoma, 39 patients (7.7%) experienced petechial type 1 hemorrhage, and 61 patients (12.1%) had petechial type 2 hemorrhage.
Clinical outcome
The percentage of patients who had a good functional outcome (mRS 0–2) was 41.6% in the entire patient population (210/505) and 51.8% (262/505) in the “first-pass” (mTICI 2b/3) sub-group. The overall death rate was 16.6%.
Discussion
This study presents our retrospective analysis of 505 patients treated in the Turkey Interventional Neurology Database using Thrombite™ as the first-line device. 48.1% of patients had first-pass success (mTICI 2b-3) and 87.7% of patients had successful recanalization (mTICI 2b-3). At 90 days, there was 4.6% symptomatic bleeding and 51.8% (262/505) of the “first-pass” (mTICI 2b/3) sub-group and 41.6% of all patients (210/505) with good functional result (mRS 0–2). Our analysis revealed that thrombectomy with the Thrombite™ device seems safe without major complications.
In both randomized and non-randomized clinical studies published in 2015 and conducted in subsequent years, the superiority of mechanical thrombectomy to medical treatment has been shown. Because with this treatment, both disability and mortality are significantly reduced (13). A recent meta-analysis of randomized clinical trials found that the mortality rate in the treatment group was 16.1%, whereas the control group experienced a mortality rate of 19.2%. At 90 days, the Number-Needed-to-Treat (NNT) required to prevent one death was 32 (14).
With the advent of advanced thrombectomy devices, (the 2nd and 3rd Stent retrievers, modifications in device design) and improvement in thrombectomy technique, an outstanding increase in the rate of successful recanalization has been achieved (15).
In a meta-analysis involving randomized clinical trials, mTICI 2b-3 rates were reported between 58.7% and 88% in thrombectomies performed with the stent retriver technique, while the good clinical outcome at day 90 was between 33-71% (14).
The Thrombite clot retriever device (Ton-bridge, Guangdong, China) was approved by the EU in January of 2020. It has similar features as the 2nd generation stent retriever, such as the overlapping design and self-expanding stent, whereas the helical open-side structure is a unique design (12).
An in vitro study showed that the the radial force and flexibility of the Thrombite device were better than the other device (16). In a prospective and randomized study comparing both stents, the clinical outcome, bleeding rates, number of passes, and mortality rates were similar, while at a statistically significant level (p < 0.001), the Thrombite device demonstrated a higher rate of successful recanalization (12).
In the same study, the first pass/final mTICI2b/3 rates were 48.1% and 92.3%, respectively, in the group using the Thrombite device. First pass effect was first described by Zaidat et al. (17) and significantly improves clinical outcome. In recent years, the rates of first pass mTICI2b-3 have been increased to 57% with newly-introduced stent retrievers. In the literature, there are different data on the first-pass effect and bleeding complications of different thrombectomy devices (Table 4) (1, 9, 10, 18–22).
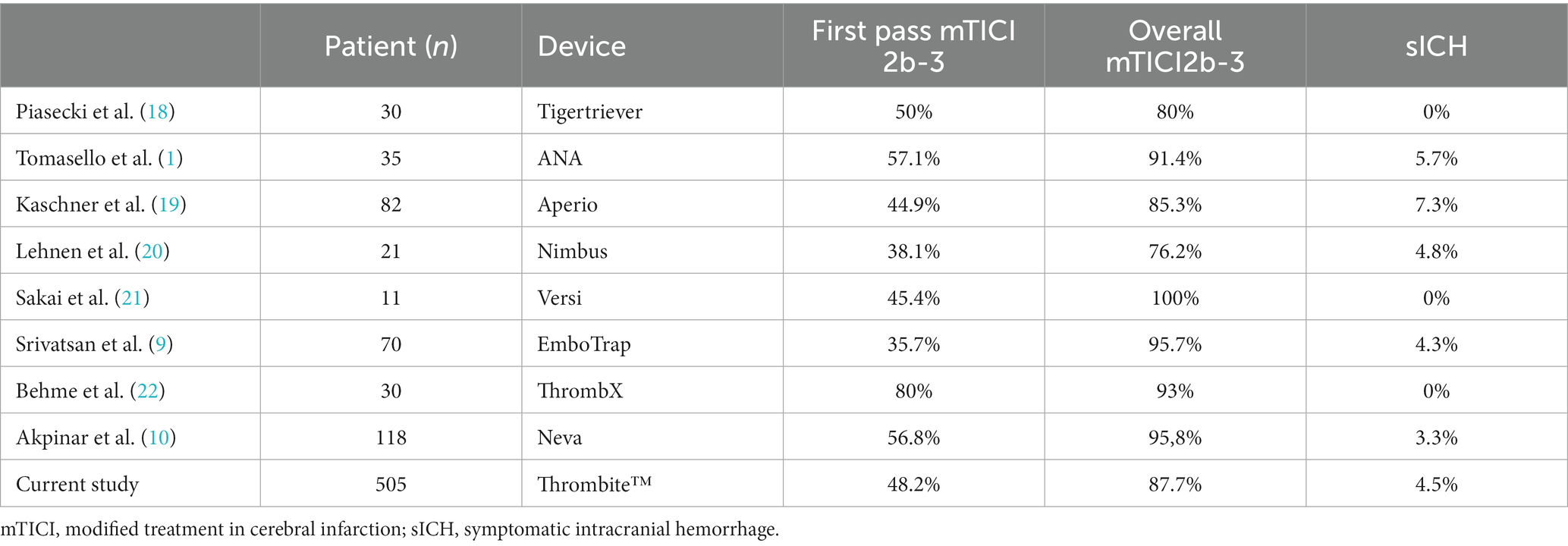
Table 4. Characteristics of reperfusion therapy studies.
The Thrombite mechanical thrombectomy device can be used as the first choice for suitable patients.
The main limitation of our study is its non-randomized design and thus lack of a control group. Furthermore, a comparative assessment of retrieval skills per clot type is also not possible because we did not undertake histological analysis of the retrieved clots.
Conclusion
It is possible to utilize the Thrombite™ thrombectomy device as the first-line option for LVO stroke thrombectomy, given the high rates of first-pass and final recanalization observed in our series. Larger, prospective multi-center trials are necessary to validate our results.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent from the patients/participants or patients/participants' legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Author contributions
ÇA: Writing – original draft. EG: Writing – review & editing. AO: Writing – review & editing. HD: Writing – original draft. AÖ: Writing – review & editing. SY: Writing – review & editing. ZM: Writing – review & editing. EA: Writing – review & editing. BA: Writing – review & editing. MÖ: Writing – review & editing. ÖA: Writing – review & editing. ZU: Writing – review & editing. TA: Writing – review & editing. HE: Writing – review & editing. BT: Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Tomasello, A, Hernandez, D, Piñana, C, Requena, M, Liebeskind, DS, Nogueira, RG, et al. Mechanical thrombectomy with a novel device: initial clinical experience with the ANA thrombectomy device. J Neuroradiol. (2022) 49:324–8. doi: 10.1016/j.neurad.2020.11.003
2. Prajapati, C, Huded, V, Mahajan, N, and Kulkarni, A. Mechanical Thrombectomy: review. Ann Indian Acad Neurol. (2022) 25:606–15. doi: 10.4103/aian.aian_29_22
3. Lapergue, B, Blanc, R, Gory, B, Labreuche, J, Duhamel, A, Marnat, G, et al. Effect of endovascular contact aspiration vs stent retriever on revascularization in patients with acute ischemic stroke and large vessel occlusion: the ASTER randomized clinical trial. JAMA. (2017) 318:443–52. doi: 10.1001/jama.2017.9644
4. Saver, JL, Goyal, M, Bonafe, A, Diener, HC, Levy, EI, Pereira, VM, et al. Stent-retriever thrombectomy after intravenous t-PA vs. t-PA alone in stroke. N Engl J Med. (2015) 372:2285–95. doi: 10.1056/NEJMoa1415061
5. Menon, BK, Hill, MD, Davalos, A, Roos, YBWEM, Campbell, BCV, Dippel, DWJ, et al. Efficacy of endovascular thrombectomy in patients with M2 segment middle cerebral artery occlusions: Meta-analysis of data from the HERMES collaboration. J Neuro Interventional Surg. (2019) 11:1065–9. doi: 10.1136/neurintsurg-2018-014678
6. Hentschel, KA, Daou, B, Chalouhi, N, Starke, RM, Clark, S, Gandhe, A, et al. Comparison of non-stent retriever and stent retriever me-chanical thrombectomy devices for the en-dovascular treatment of acute ischemic stroke. J Neurosurg. (2017) 126:1123–30. doi: 10.3171/2016.2.JNS152086
7. Samaniego, EA, Roa, JA, Limaye, K, and Adams, HP Jr. Mechanical Thrombectomy: emerging technologies and techniques. J Stroke Cerebrovasc Dis. (2018) 27:2555–71. doi: 10.1016/j.jstrokecerebrovasdis.2018.05.025
8. Yoo, AJ, Soomro, J, Andersson, T, Saver, JL, Ribo, M, Bozorgchami, H, et al. Benchmarking the extent and speed of reperfusion: first pass TICI 2c-3 is a preferred endovascular reperfusion endpoint. Front Neurol. (2021) 12:669934. doi: 10.3389/fneur.2021.669934
9. Srivatsan, A, Srinivasan, VM, Starke, RM, Peterson, EC, Yavagal, DR, Hassan, AE, et al. Early Postmarket results with Embo trap II stent retriever for mechanical Thrombectomy: a multicenter experience. AJNR Am J Neuroradiol. (2021) 42:904–9. doi: 10.3174/ajnr.A7067
10. Akpinar, CK, Ozdemir, AO, Gurkas, E, Bilgic, AB, Aykac, O, Inanc, Y, et al. Favorable first-pass recanalization rates with NeVa™ thrombectomy device in acute stroke patients: initial clinical experience. Interv Neuroradiol. (2021) 27:107–13. doi: 10.1177/1591019920938223
11. Seifert, M, Ahlbrecht, A, Dohmen, C, Spuentrup, E, and Moeller-Hartmann, W. Combined interventional stroke therapy using intra-cranial stent and local intraarterial thrombolysis (LIT). Neuroradiology. (2011) 53:273–82. doi: 10.1007/s00234-010-0719-0
12. Zhang, Y, Hua, W, Li, Z, Peng, Y, Han, Z, Li, T, et al. Efficacy and safety of a novel Thrombectomy device in patients with acute ischemic stroke: a randomized controlled trial. Front Neurol. (2021) 12:686253. doi: 10.3389/fneur.2021.686253
13. Goyal, M, Menon, BK, van Zwam, W, Dippel, DWJ, Mitchell, PJ, Demchuk, AM, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet. (2016) 387:1723–31. doi: 10.1016/S0140-6736(16)00163-X
14. Rajkumar, CA, Ganesananthan, S, Ahmad, Y, Seligman, H, Thornton, GD, Foley, M, et al. Mechanical thrombectomy with retrievable stents and aspiration catheters for acute ischaemic stroke: a meta-analysis of randomised controlled trials. Euro Intervention. (2022) 17:e1425–34. doi: 10.4244/EIJ-D-21-00343
15. Bageac, DV, Gershon, BS, and De Leacy, RA. The evolution of devices and techniques in endovascular stroke therapy In: S Dehkharghani, editor. Stroke [Internet]. Brisbane (AU): Exon Publications (2021).
16. Zhou, G, Li, M, Lu, H, Deng, J, Zhao, Y, Wang, YXJ, et al. No inferiority of tonbridge thrombectomy device for acute thrombus retrial compared with solitaire device: an experimental evaluation with a canine distal external carotid-maxillary artery occlusion model. J Neurointerv Surg. (2018) 10:1085–91. doi: 10.1136/neurintsurg-2017-013673
17. Zaidat, OO, Castonguay, AC, Linfante, I, Gupta, R, Martin, CO, Holloway, WE, et al. First pass effect: a new measure for stroke Thrombectomy devices. Stroke. (2018) 49:660–6. doi: 10.1161/STROKEAHA.117.020315
18. Piasecki, P, Wierzbicki, M, and Narloch, J. Safety and efficacy of mechanical Thrombectomy using Tigertriever as a rescue device after failed aspiration—single center experience. Front Neurol. (2020) 11:603679. doi: 10.3389/fneur.2020.603679
19. Kaschner, MG, Weiss, D, Rubbert, C, Lee, J, Gliem, M, Jander, S, et al. One-year single-center experience with the Aperio thrombectomy device in large vessel occlusion in the anterior circulation: safety, efficacy, and clinical outcome. Neurol Sci. (2019) 40:1443–51. doi: 10.1007/s10072-019-03861-z
20. Lehnen, NC, Paech, D, Zülow, S, Bode, FJ, Petzold, GC, Radbruch, A, et al. First experience with the Nimbus Stentretriever a novel device to handle fibrin-rich clots. Clin Neuroradiol. (2023) 33:491–7. doi: 10.1007/s00062-022-01237-z
21. Sakai, N, Imamura, H, Adachi, H, Tani, S, Tokunaga, S, Funatsu, T, et al. First-in-man experience of the Versi retriever in acute ischemic stroke. J Neuro Intervent Surg. (2019) 11:296–9. doi: 10.1136/neurintsurg-2018-014040
Keywords: acute stroke, mechanical thrombectomy, thrombectomy device, first pass complete reperfusion, technique
Citation: Akpınar ÇK, Gurkas E, Ozdemir AO, Doğan H, Önalan A, Yıldırım S, Memiş Z, Aytaç E, Acar BA, Öğün MN, Aykaç Ö, Uysal Kocabaş Z, Acar T, Eryılmaz HA and Topaktaş B (2024) Three years’ interventional neurology experience in Turkey with the Thrombite thrombectomy device in large vessel occlusion in the anterior circulation: safety, efficacy, and clinical outcome. Front. Neurol. 15:1320510. doi: 10.3389/fneur.2024.1320510
Edited by:
Sherief Ghozy, Mayo Clinic, United StatesReviewed by:
Qazi Zeeshan, Mayo Clinic Arizona, United StatesKwon-Duk Seo, National Health Insurance Service Ilsan Hospital, Republic of Korea
Copyright © 2024 Akpınar, Gurkas, Ozdemir, Doğan, Önalan, Yıldırım, Memiş, Aytaç, Acar, Öğün, Aykaç, Uysal Kocabaş, Acar, Eryılmaz and Topaktaş. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hasan Doğan, ZHIuaGFzYW5kb2dhbkBvdXRsb29rLmNvbQ==