 Rafael Bastos Gonçalves Pessoa1
Rafael Bastos Gonçalves Pessoa1 Weslley Felix de Oliveira1Maria Tereza dos Santos Correia1
Weslley Felix de Oliveira1Maria Tereza dos Santos Correia1 Adriana Fontes2
Adriana Fontes2 Luana Cassandra Breitenbach Barroso Coelho1*
Luana Cassandra Breitenbach Barroso Coelho1*- 1Departamento de Bioquímica, Centro de Biociências, Universidade Federal de Pernambuco, Recife, Brazil
- 2Departamento de Biofísica e Radiobiologia, Centro de Biociências, Universidade Federal de Pernambuco, Recife, Brazil
The genus Aeromonas comprises more than 30 Gram-negative bacterial species and naturally inhabitants from aquatic environments. These microorganisms, commonly regarded as pathogens of fish and several other animals, have been gaining prominence on medical trial due to its ability to colonize and infect human beings. Besides water, Aeromonas are widely spreaded on most varied sources like soil, vegetables, and food; Although its opportunistic nature, they are able to cause infections on immunocompromised or immunocompetent patients. Aeromonas species regarded as potential human pathogens are usually A. hydrophila, A. caviae, and A. veronii biovar sobria. The main clinical manifestations are gastrointestinal tract disorders, wound, and soft tissue infections, as well as septicemia. Regarding to antibiotic responses, the bacteria present a diversified susceptibility profile and show inherence resistance to ampicillin. Aeromonas, as an ascending genus in microbiology, has been carefully studied aiming comprehension and development of methods for detection and medical intervention of infectious processes, not fully elucidated in medicine. This review focuses on current clinical knowledge related to human health disorders caused by Aeromonas to contribute on development of efficient approaches able to recognize and impair the pathological processes.
Introduction
When thinking about Aeromonas, the first thing that comes to our minds might be “water” or “fish.” Indeed, bacteria from this genus naturally inhabit aquatic environments and are known as a threat for aquaculture systems (Barger et al., 2021). The hazardousness of Aeromonads for several fish species as well as other waterborne animals has been strongly discussed (Beaz-Hidalgo and Figueras, 2013; Dallaire-Dufresne et al., 2014; Fernández-Bravo and Figueras, 2020). However, the potential of these microorganisms to cause human health disorders must be highlighted.
Worldwide distributed, Aeromonas were already isolated from a broad range of sources like fresh water, sewage, soil, fruits, vegetables, and processed food (McMahon and Wilson, 2001; Gonçalves Pessoa et al., 2019; Barger et al., 2021). Thus, contact between these bacteria and human beings can be easily established. Aeromonads are considered emergent pathogens and its detection in various diarrheal stool samples clearly shows they are not as far from clinical routine as other enteric microorganisms (Li et al., 2015; Mohan et al., 2017; Mbuthia et al., 2018). Consequently, interest about the genus Aeromonas, which embraces 36 recognized species, has risen over the past years (Fernández-Bravo and Figueras, 2020; Ahmed et al., 2021; Conte et al., 2021).
Several case reports involving Aeromonads infections brought up the diversity of clinical manifestations that these bacteria can provoke to human health. Symptoms range from acute self-limiting diarrhea to lethal sepsis; however, wounds, skin, bones, heart, lungs, eyes, and other organs can be potentially affected (Parker and Shaw, 2011; Ahmed et al., 2021; Meng et al., 2021). Most reports classify Aeromonas’s human infections as events caused by “rare” or “uncommon” microorganisms (Lai et al., 2007; Khalil et al., 2013; Hasan et al., 2018; Salehi et al., 2019). Indeed, other bacterial genus causing the same clinical symptoms are more frequent at hospital level. For example, Campylobacter spp., Salmonella spp., Shigella spp., and Escherichia coli are listed as the main pathogens in clinical cases of acute gastroenteritis (Fleckenstein et al., 2021). Moreover, Staphylococcus aureus and Streptococcus pyogenes are frequently detected in skin and wound infections reports (Cefalu et al., 2017; Clebak and Malone, 2018).
Noteworthy, one of the peculiar characteristics of the Aeromonas genus is the unreliable phenotypical identification by conventional biochemical tests or commercial systems, like Vitek, API20, and Microscan, which are commonly used in the quotidian of most hospital laboratories (Lamy et al., 2010; Jin et al., 2011; Gonçalves Pessoa et al., 2019; Meng et al., 2021). It is known that Aeromonas strains show similarities to other bacterial genera, and accurate data still lies on molecular biology techniques aiming amplification of housekeeping genes for phylogenetic differentiation (Yáñez et al., 2003; Beaz-Hidalgo and Figueras, 2013; Hoel et al., 2017).
The Aeromonas possess wide spectra of antibiotic resistance profile and occurrence of multi-resistant strains have already been reported (Galler et al., 2018; Conte et al., 2021). As inhabitants of aquatic environments, these microorganisms can be used as ecological indicators of water pollution since they harbor antibiotic resistance genes obtained from wastewater effluents (Baron et al., 2017; Grilo et al., 2020). Furthermore, the global indiscriminate use of antimicrobials has changed the perspective of medicine regarding bacterial infections for the next years. The incidence of multidrug-resistant microorganisms has increased and it is expected to be the main public health problem in the future (Dimopoulos et al., 2016). Aeromonads are prone to be susceptible to fluoroquinolones but usually resistant to ampicillin and other beta-lactams (Parker and Shaw, 2011; Fernández-Bravo and Figueras, 2020). In a clinical scenario, however, the execution of an antibiogram test must not be dispensed so as to ensure suitable antibiotic prescriptions (Abbott et al., 2003).
In this review, information about the main clinical features of Aeromonas infections will be provided to highlight how dangerous these bacteria can be for human beings. The knowledge about epidemiology, differential diagnosis, and strategies for antibiotic therapy are also explored.
Aeromonas Epidemiological Profile
Aeromonas species generally associated with human infections include A. caviae, A. schubertii, A. hydrophila, A. veronii (biovars veronii and sobria), and A. jandaei (Lamy et al., 2010). These microorganisms have been isolated in hospitals worldwide, and different types of clinical samples, especially fecal, have been used for this investigation. Moreover, the frequency of the species may differ according to the region where they were isolated.
A study performed with diarrheal stool from 1,595 patients identified Aeromonas in 50 samples in India; the biochemical speciation was made on 35 strains showing that the most common species were A. caviae (34%), A. veronii biovar veronii (29%), A. veronii biovar sobria (26%), and A. hydrophila (9%; Mohan et al., 2017). In Kenya, 188 fecal samples were studied to determine the etiological agents of diarrhea, of which only five were caused by A. hydrophila and three by A. caviae (Mbuthia et al., 2018). In 16 hospitals in the city of Shanghai, China, 4,529 specimens from diarrheal patients were collected, in which 193 cases were related to Aeromonas infection: A. veronii (42.5%), A. caviae (25.3%), A. aquariorum (14.5%), A. hydrophila (5.7%), A. enteropelogenes (4.7%), A. media (3.1%), unknown (1.6%), A. salmonicide (2.1%), and A. allosaccharophila (0.5%; Li et al., 2015). While a study at a hospital in Beijing city, China, 1,286 stool samples were analyzed from people with acute diarrhea, and 17 strains of Aeromonas causing extra-intestinal infections were identified in blood or bile. The distribution of Aeromonas species in these isolates obtained from intestinal and extra-intestinal samples followed A. veronii (31.3%), A. caviae (41.7%), A. dhakensis (13.9%), A. media (1.7%), A. hydrophila (5.2%), A. sanarellii (1.7%), A. enteropelogenes (1.7%), A. bivalvium (0.9%), and unknown (1.7%; Zhou et al., 2019).
During the period from January 2015 to December 2017 at Hospital Galdakao-Usansolo, Spain, 98 patients (having a median age of 62 years, and 51% of the cases were women) with positive stool cultures for Aeromonas were counted, being 85 cases of A. caviae, 12 of A. veronii, and 1 of A. hydrophila; estimating an occurrence of 32 cases for every 105 inhabitants per year (Elorza et al., 2020).
Different biological samples, such as stool, eye, sputum, and blood, were tested in microbiological laboratories in Australia for Aeromonas search. From 100 isolates, 39 were A. dhakensis, 21 A. veronii, 20 A. hydrophila, 14 A. caviae, 4 A. jandaei, 1 A. bestiarum, and 1 A. sanarellii (Sinclair et al., 2016). A study of 109 Aeromonas clinical isolates from diarrhea patients was conducted in Mexico and Spain, and the most common species in both countries were A. caviae, A. hydrophila, and A. veronii (Aguilera-Arreola et al., 2007). A retrospective analysis from January 2006 to December 2012, carried out at the Hospital del Mar in Barcelona, Spain, detected 221 clinical samples positive for Aeromonas spp. in 204 patients. Gastroenteritis was the most common form of infection, comprising of 78.4% from patients. It was found that age above 80 years, admission to the intensive care unit, and malignancy were associated with increased mortality rate during the 1-year follow-up of infected patients (Nolla-Salas et al., 2017).
Regarding extra-intestinal infections caused by Aeromonas, there are varieties of sites that can be affected. A range of non-gastrointestinal infections can involve Aeromonas species, some have been associated with contaminated water, for example, soft tissue infection due to injury to an aquatic environment (Lujan-Hernandez et al., 2020), and wound infection after medical leech therapy that may have occurred due to contamination of the water where the leeches were bred (Masters et al., 2020).
Aeromonas wound or pus isolates were collected from a medical center in southern Taiwan, and 76 species were reported, A. dhakensis (37), A. veronii (14), A. hydrophila (13), A. caviae (11), and A. media (1; Chen et al., 2014b). Another study was conducted at this same medical center, in which among 514 stools from adults with diarrhea, 13 had Aeromonas detected, and of the 167 asymptomatic persons, only six were isolated. The most common species in these isolates were A. veronii, A. caviae, A. sanarelli, and A. dhakensis (Chen et al., 2014b). These data show that, although Aeromonas infections may occur in the same region, the difference in anatomical sites may reflect a distinct distribution among their isolate species.
Pathological Processes and Clinical Manifestations
Bacteria belonging to the Aeromonas genus are known as the main pathogens of fish and other marine animals, being responsible for deleterious outbreaks in aquaculture systems due to their wide distribution in various aquatic environments (Beaz-Hidalgo and Figueras, 2013; Liu, 2015; Figueras and Ashbolt, 2019). Moreover, they were already detected in bugs, reptiles, amphibians, birds, and other vertebrates (Percival and Williams, 2014; Praveen et al., 2016; Gonçalves Pessoa et al., 2019). Despite being firstly reported in 1891, the Aeromonas were only recognized as potential human pathogens about 60 years later, in 1954, when these microorganisms were detected in clinical samples obtained from an immunosuppressed woman who died due to a fulminant metastatic myositis (Parker and Shaw, 2011; Liu, 2015; Fernández-Bravo and Figueras, 2020). Currently, it is known that these bacteria can cause predominantly gastrointestinal tract disorders as well as infections in wounds, soft tissues, muscles, lungs, bones, and septicemia, to name a few (Parker and Shaw, 2011; Bhowmick and Bhattacharjee, 2018; Fernández-Bravo and Figueras, 2020). The main illnesses provoked by Aeromonads are shown in Figure 1.
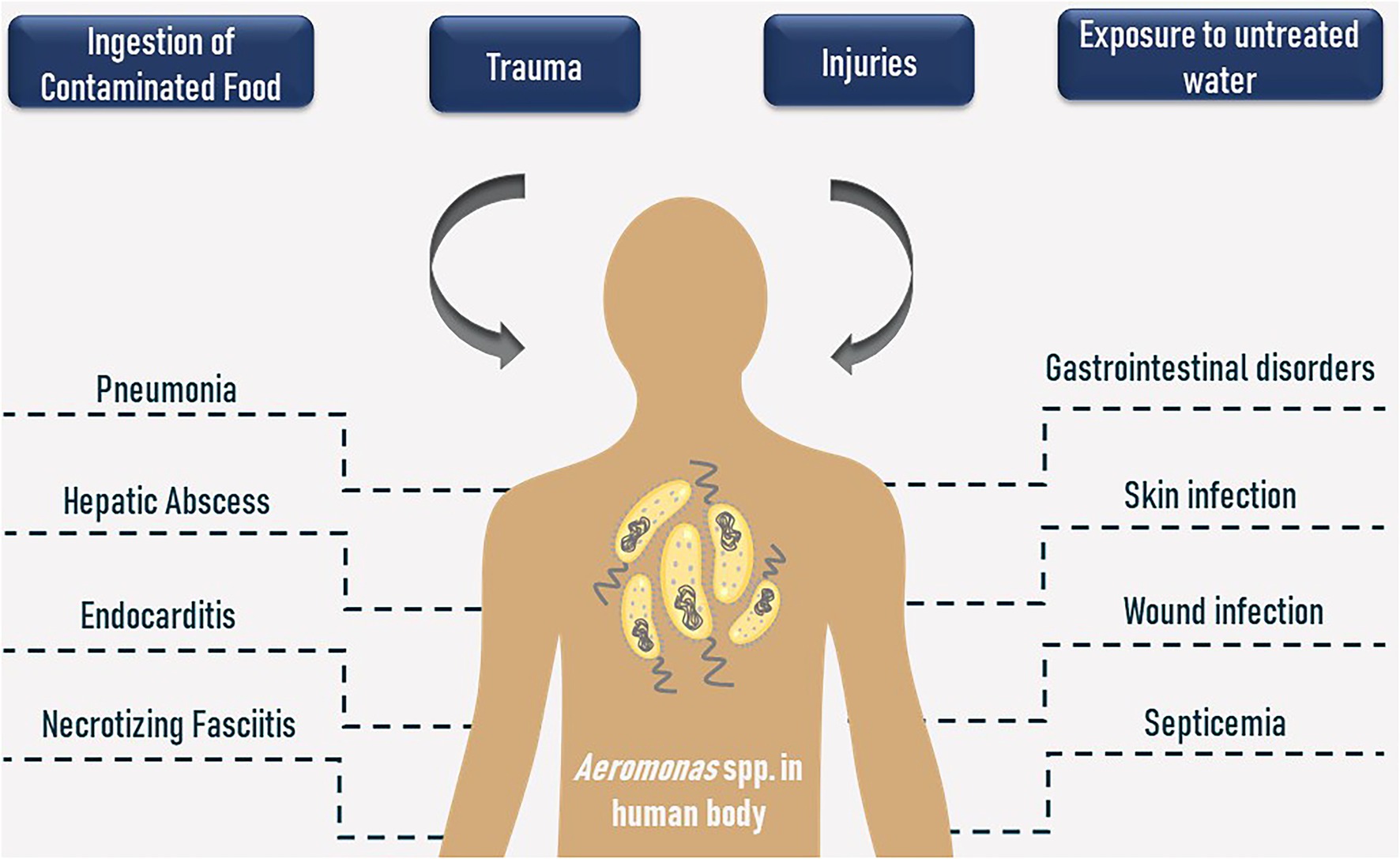
Figure 1. Contamination routes and human health disorders caused by Aeromonas spp.
Aeromonas species are classified into two main groups: (i) psychrophilic, usually non-motile strains which grow well between 22°C and 28°C, and (ii) mesophilic, motile with desirable growth temperature into 35°C–37°C or higher (Parker and Shaw, 2011; Percival and Williams, 2014; Liu, 2015; Fernández-Bravo and Figueras, 2020). The psychrophilic group is represented by the Aeromonas salmonicida, which is described as an important cold-water fish pathogen (Fernández-Bravo and Figueras, 2020; Pérez-García et al., 2021). However, this bacterium has already been detected from blood samples of an infected 20-year-old man diagnosed with endocarditis (Salehi et al., 2019). On the other hand, the mesophilic group is often related to both fish and human infections and is mainly represented by A. hydrophila, A. caviae, and A. veronii, but it embraces the other Aeromonas’s species excepting the psychrophilic A. salmonicida (Percival and Williams, 2014; Pérez-García et al., 2021).
Broadly described as opportunistic bacteria, pathological processes generated by these microorganisms are frequently reported in immunosuppressed patients. However, even healthy persons, from any age, can be potential hosts to illnesses caused by Aeromonas (Chuang et al., 2011; Silva et al., 2017). The wide range of diseases generated by Aeromonads is characterized as a joint action of several virulence factors, such as lipases, proteases, hemolysins, aerolysins, cytotoxins, and enterotoxins, that contribute both to its survival and environmental adaptation as well as to the multifactorial and complexity of its pathogenesis, whose mechanisms and processes are usually not evident (Pemberton et al., 1997; Zhou et al., 2013; Rasmussen-Ivey et al., 2016; Hoel et al., 2017).
Aforementioned, Aeromonas are natural habitants from aquatic environments and could be detected in samples obtained from different sources (Praveen et al., 2016; Harnisz and Korzeniewska, 2018). Furthermore, these bacteria can resist potable water treatment processes for human consumption, representing a potential contamination route (Janda and Abbott, 2010). Phylogenetic studies previously performed suggest feasible relations between Aeromonas strains isolated from both municipal water and clinical samples within the same geographic region (Pablos et al., 2009, 2011). The intake of contaminated food like animal-derived proteins (meat, chicken, and, mainly, fisheries), vegetables, and, additionally, the preparation methods of some culinary recipes are reported as the main cause for Aeromonads infections (Castro-Escarpulli et al., 2003; Pablos et al., 2009; Hoel et al., 2017). Environmental factors can influence outbreaks caused by these microorganisms. Studies have shown that temperatures over 22°C might provoke loss of virulence factors in A. salmonicida strains (Fernández-Bravo and Figueras, 2020). On the other hand, it has been reported that different temperatures modulate the expression of virulence genes in distinct isolates of A. hydrophila; most of the assessed genes were expressed by culturing the strains at 28°C (Pattanayak et al., 2020). Moreover, it was demonstrated that an A. hydrophila strain endured under low temperatures and starvation by shaping its virulence factors content (Bruscolini et al., 2014). Other Aeromonas species related to human health disorders grow well in higher temperatures and, consequently, lead to an increase in the number of infections under warm seasons due to the high bacterial cell count in the environment, especially in water (Bhowmick and Bhattacharjee, 2018).
Herein, based on case reports, the main clinical manifestations developed during infectious processes generated by Aeromonas will be discussed; reinforcing its relevance in public health and the importance of researches involving this bacterial genus in the field of medical microbiology.
Gastrointestinal Diseases
Acute gastroenteritis is one of the most common diseases faced by physicians in emergency medical services around the world. It is presented as a sudden diarrheal process that may be followed by other symptoms like vomiting, abdominal pain, fever, nausea, and malaise, which are results from infectious processes, with inflammatory nature or not, involving the small intestine or the colon (Duman et al., 2015; Barrett and Fhogartaigh, 2017; Fleckenstein et al., 2021). In general, it is mainly caused by a viral infection, but several bacterial species have been associated with gastroenteritis episodes, representing from 15% to 40% of the reported cases, approximately (Barrett and Fhogartaigh, 2017; Schuetz, 2019).
The classification of Aeromonas as true enteropathogens has been under discussion for a long time. Among the main controversial arguments were (i) the lack of reliable identification of Aeromonas strains related to specific outbreaks, (ii) non-compliance with the criteria proposed in the Henle–Koch postulates, in regards to the isolation of the microorganism from the diseased body and reproduction of the infection using animal models, and (iii) lack of consistent evidence related to the induction of pathological processes in humans by these bacteria, which would confirm their pathogenicity (Janda and Abbott, 2010; Chen et al., 2015; Schuetz, 2019). Since previous outbreaks in which Aeromonads were detected on stool samples—obtained from infected patients—had already been reported, persisting on classifying these bacteria as true enteropathogens seem to be an obvious and logic conduct (Janda and Abbott, 2010). Such fact conflicted with the results of an experimental test involving the administration of oral solutions containing a high concentration of Aeromonas strains, where just two from a group of 57 tested humans experienced diarrhea, questioning the enteropathogenicity of these microorganisms (Morgan et al., 1985). However, according to different analysis of data obtained from different outbreaks involving Aeromonads and humans with diverse exposure profile, the potential of these bacteria on developing gastrointestinal disorders was finally proved. It was showed that the ingestion of low concentrations of these bacteria can develop infection even if asymptomatically; what attributed to the genus Aeromonas the classification of true enteropathogen, which severity of infections can be equally compared to those developed by other bacterial genus like Campylobacter and Salmonella (Teunis and Figueras, 2016).
Bacterial enteritis commonly originates from the ingestion of contaminated food, and microorganisms develop gastrointestinal disorders through the production of pre-toxins, adhesion to the epithelium, secretion of virulence factors, and the invasion of the intestinal mucosa, resulting in different symptoms (Barrett and Fhogartaigh, 2017; Fleckenstein et al., 2021). Several risk factors are associated, such as age group, immunological condition, and access to proper basic sanitation (Barrett and Fhogartaigh, 2017). When caused by Aeromonas, cases of gastroenteritis commonly present as episodes of self-limiting watery diarrhea, but they can also occur manifest more severely in the form of dysentery-like and cholera-like disease (Parker and Shaw, 2011; Harnisz and Korzeniewska, 2018). It has been reported a case of two women with a history of diarrhea, vomiting, and abdominal pain in a cholera endemic area. Although stool cultures and Gram staining indicated a possible infection by Vibrio cholerae, genomic analysis of the samples identified A. caviae, revealing Aeromonads enteritis mimicking cholera disease (Van Zwetselaar et al., 2018). Practically the same symptoms were presented by a 69-year-old patient who reported eating raw fish. Imaging examinations and physical evaluation revealed possible appendix perforation, but both the incompatibility of symptoms and detection of A. hydrophila/caviae by stool culture led to the final diagnosis of enteritis with evident mimicry of acute appendicitis (Kishimoto and Watari, 2018). Although considered common and usually simple to treat, gastroenteritis is one of the causes of bacterial gut translocation, which potentially leads to even more severe complications, such as peritonitis and colitis (Kim et al., 2018).
Peritonitis is an inflammatory process on the peritoneum, serous membrane that covers intra-abdominal organs, usually caused by bacterial infection (Lippi et al., 2014). In this case, it is classified mainly as primary, or spontaneous, and secondary. The former is a common complication of cirrhotic patients, contamination of the ascitic fluid (AF) as a result of overgrowing enteric bacteria and posterior translocation due to reduced motility of the intestine and low host defenses (Strauss and Caly, 2006). It was reported a case of a 57-year-old man, with a history of alcoholism and suffering from cirrhosis that came to death after developing septic shock from A. hydrophila, which was detected in blood cultures and ascetic fluid (Lin and Lin, 2019). In Taiwan, it was analyzed that, over 16 years, around 31 cases of cirrhotic patients developed spontaneous Aeromonas peritonitis. The main symptoms were fever and abdominal pain; these cases had a mortality rate of 56% (Wu et al., 2009). Secondary bacterial peritonitis is related to the presence of injuries or intestinal lesions caused basically by surgical procedures or trauma (Miyashita et al., 2019). This kind of infection has been reported in humans undergoing peritoneal dialysis (PD), a technique used in the management of patients suffering from end-stage renal disease (Gillis and Wilkie, 2019). Given that it is a home-based therapy, proper training of the patient for the correct handling of the device and also execution of fluid exchange is extremely important to avoid bacterial infections (Cho and Johnson, 2014; Gillis and Wilkie, 2019). A rare case of peritonitis related to PD due to Aeromonas infection has been reported. A 54-year-old man in the course of PD had washed a disposable part of the automated device with tap water and developed acute abdominal pain. Peritoneal dialysate culture detected A. hydrophila, and the patient was treated without device removal (Kim et al., 2018). Compared with the main Gram-negative bacteria that can cause peritonitis, Aeromonas cases are still considered uncommon, but not less lethal (Lippi et al., 2014).
Ulcerative colitis (UC), which compounds the group of inflammatory disorders involving the colon, does not have an exact pathogenesis (Cheng and Fischer, 2020). However, it is represented by an imbalance in the host’s immune system response to external antigens, such as food and commensal microorganisms (Cheng and Fischer, 2020; Du and Ha, 2020). A wide range of bacterial enteropathogens can develop infection through invading intestinal mucosa or secreting toxins that induce inflammation, causing tissue damage, such as erosions, ulcers, and even mimicking other chronic inflammatory bowel diseases, as a consequence of the persistence of the infectious process (Bhaijee et al., 2015). A case of a 34-year-old woman who developed abdominal pain and diarrhea about 3 days after eating fish was reported. The histopathological analysis detected inflammatory infiltrate and colon ulcers were found using endoscopy, which led to the diagnosis of UC. Molecular tests using fecal samples detected Aeromonas spp. (Morales-Fuentes et al., 2014).
Skin, Soft Tissues and Wound Infections
Human skin consists of two layers that act as a physical barrier, protecting the body against external threats (Cefalu et al., 2017). Infections involving this extensive organ are one of the main disabling disorders in the world (Jabbour and Kanj, 2021). Characterized as invasions of the epidermis and adjacent tissues by virulent microorganisms, due to the presence of injuries and other risk factors, they initially generate common signs of local inflammation with a potential risk of evolution to various pathological processes, depending on the nature of the invading microbe (DiNubile and Lipsky, 2004; Dryden, 2010; Clebak and Malone, 2018). Naturally, the epidermis is colonized by several types of microorganisms and, when it comes to bacteria, the ones most commonly detected on the skin of adult individuals belong to the Staphylococcus, Streptococcus, and Corynebacterium genera (Cefalu et al., 2017; Byrd et al., 2018; Vasagar et al., 2018). Among the main bacterial skin infections are impetigo, erysipelas, cellulitis, folliculitis, abscesses, and necrotizing fasciitis (Clebak and Malone, 2018). Noteworthy, when such diseases are contracted through prior exposure to aquatic environments, the polymicrobial etiology of the infection must be taken into account, especially with regards to the presence of unusual microorganisms, such as Aeromonas (Vasagar et al., 2018).
Aeromonads potentially generates a variety of skin and soft tissue disorders, most often affecting healthy people, aging ≥10 years, who have suffered some type of injury (such as burns and trauma) and/or exposure to contaminated water (Janda and Abbott, 2010; Parker and Shaw, 2011; Fernández-Bravo and Figueras, 2020). Aeromonas species have been detected by the pus culture of infected wounds contained in a 12-year-old boy that had injured his knees after falling on rocks while swinging over water (Rutteman, 2017). Likewise, A. hydrophila and E. cancerogenus were also identified in the pus culture of an elderly patient who suffered a traffic accident and fell into a pool of contaminated water (Hadano et al., 2017). Traumatic events involving sharp objects have also been the cause of infections by these bacteria (Larka et al., 2003). Burn wounds have a high risk of contamination when not treated properly, mainly because they are exposed to water as a first-aid measure (Ribeiro et al., 2010). Although uncommon, some Aeromonas spp. have been reported as the cause of infection and worsening prognosis of patients in this situation (Kienzle et al., 2000; Chim and Song, 2007; Lai et al., 2007).
Although the vast majority of skin infections involving Aeromonas have been reported as a consequence of a previously caused injury, objects that are eventually filled with contaminated water and used for domestic or recreational purposes can also be a source of infection. Cases of Aeromonas folliculitis have been reported in children after playing in inflatable swimming pools filled with tap water without any purification or disinfection system. One of them, the 11-year-old girl, developed symptoms related to systemic inflammatory syndrome due to a left sinus infection that was not completely resolved until Aeromonas was detected in the purulent fluid collected (Olszewski et al., 2017). The other kids, a 15-year-old girl and an 8-year-old boy, complained of just pruritus due to the presence of multiple follicular lesions. Pustular fluid cultures detected A. hydrophila in the two patients, who used the inflatable pool for 5 days without water change (Manresa et al., 2009). Severely, a 34-year-old man developed folliculitis in the pubic region potentially caused by Aeromonads that resulted in rashes, swelling, and local alopecia. Since her partner had also developed similar symptoms and both denied extramarital relationships and sexually transmitted diseases, the possible cause of the infection was related to the use of a spa bath with no regular maintenance (Mulholland and Yong-Gee, 2008).
Regarding musculoskeletal and soft tissue infections, the Aeromonas are recognized to generate disorders in both healthy and immunocompromised patients (Voss et al., 1992; Janda and Abbott, 2010). Necrotizing fasciitis (NF), a disease associated with a high mortality rate, which usually needs surgical intervention, is characterized by a progressive infection that starts in the fascia and extends to the subcutaneous tissues, impairing local blood circulation, generating deep necrosis (Ali and Lateef, 2016; Narayan and McCoubrey, 2019; Stevens et al., 2021). NF is subdivided into four categories, depending on the type and number of microorganisms detected, and has several etiologies, risk factors, and pathogenic mechanisms (Narayan and McCoubrey, 2019; Stevens et al., 2021). Some Aeromonas species have been identified causing NF. A case involving an 8-year-old boy who injured his right foot while swimming and developed fever, as well as a general malaise in addition to progressive pain and edema in the affected region, was reported. During surgery, fascial necrosis was detected, and cultures of collected samples identified the presence of A. hydrophila and S. pyogenes (Fletscher Covaleda et al., 2013). On the other hand, the 80-year-old man with no previous trauma or exposure to contaminated water died from NF caused by Aeromonads, which led to multiple organ dysfunctions (Cui et al., 2007). Aeromonas hydrophila, A. caviae, and A. dhakensis were distinctly found causing fatal NF in immunocompromised patients suffering from a wide range of underlying diseases like heart failure, hypertension, leukemia, aplastic anemia, cirrhosis, and diabetes (Spadaro et al., 2014; Hong et al., 2018; Ugarte-Torres et al., 2018) as well as acting as secondary pathogens in dengue patients (Chang et al., 2018). Aeromonas caviae was also detected in a case of a 22-year-old woman that developed NF after an aesthetic surgical procedure in both calves (Park et al., 2010).
Aeromonas Bacteremia and Sepsis
When searching through the literature, it is easy to identify differences in the application of the expressions “bacteremia” and “sepsis” concerning systemic infections caused by bacteria and other microorganisms (Søgaard et al., 2012). Bacteremia refers to the presence of bacteria in the bloodstream, while sepsis is characterized as a systemic inflammatory syndrome involving components of the innate immune system, which can be caused by bacterial pathogens as well as fungi, viruses, and parasites; resulting in other metabolic disorders which lead to multiple organ failure and patient death (Girard and Ely, 2007; Perner et al., 2016; Minasyan, 2019). Aeromonas are recognized in the group of Gram-negative bacteria causing bacteremia/sepsis, but they do not cause any signs or symptoms that distinguishes their systemic infections from cases involving other bacterial genera (Janda and Abbott, 2010). The incidence of Aeromonas septicemia is relatively low. Its mortality rate can vary between 25% and 30% and it is commonly related to immunocompromised patients or those suffering from underlying diseases (Parker and Shaw, 2011; Fernández-Bravo and Figueras, 2020). Aeromonas hydrophila was reported in a rare case of fulminant septicemia in a child in the course of acute lymphoblastic leukemia therapy, generating tissue necrosis and requiring extensive surgical debridement (Papadakis et al., 2012). Aeromonas sobria was the cause of fatal septicemia in a patient living with HIV. The infection developed rapidly, the patient’s health condition has severely deteriorated and the pathogen was discovered in post-mortem tests (Stano et al., 2009). In cases of sepsis, rapid diagnosis and the initiation of appropriate empirical antibiotic therapy have been cited as crucial measures to preserve the life of the affected patient (Minasyan, 2019; Sweeney et al., 2019).
Hepatobiliary and Pancreatic System Infections
Infectious diseases affecting the liver and the biliary tract trigger the development of other complications of human health, which demand rapid and accurate diagnosis (Hynes et al., 2020). The potential of Aeromonas in generating disorders in these systems has already been described, with cases of acute suppurative cholangitis (ASC), an obstructive and infectious complication of the biliary tract, being one of the most common reports (Janda and Abbott, 2010; Sulzer and Ocuin, 2019). In a general evaluation of patients diagnosed with ASC, symptoms, such as fever, jaundice, abdominal pain, and the presence of several underlying conditions, were verified. Aeromonas hydrophila was the most detected species in bile cultures, A. caviae and A. veronii biotype sobria were also found (Chan et al., 2000). In another analysis, the same species were also isolated from bile samples collected from 750 patients suffering from biliary tract infections. The authors highlighted the tendency of cases to occur frequently in patients with immunosuppressive conditions due to diseases, such as cancer, diabetes, cirrhosis, and other liver illnesses, in addition to therapy with immunosuppressive agents (Chao et al., 2013b). Invasive clinical procedures also pose a risk of bile system infections by Aeromonas. A case of a 64-year-old woman who developed sepsis and other complications from A. veronii biovar veronii after biliary drainage catheter insertion was reported (Monti et al., 2019). Aeromonas were also the cause of liver and pancreas abscesses (Kratzke and Golenbock, 1987; De Gascun et al., 2007).
Other Infections
Bacteria belonging to the genus Aeromonas have been uncommonly reported generating disorders in several other organs, such as eyes, lungs, bones, and kidneys, for example, (Bhowmick and Bhattacharjee, 2018; Fernández-Bravo and Figueras, 2020).
Regarding eye infections, a case of a 35-year-old man who developed keratitis related to the use of contact lenses, which was occasionally exposed to tap water, was reported. A. caviae was detected by culturing eye swabs and contact lens case (Pinna et al., 2004). Aeromonads were also the cause of conjunctivitis, contracted in a nosocomial route, in a diabetic patient (Gonzales et al., 1989). Such disorders can also occur as a consequence of other previously developed diseases. It was reported a case of a 79-year-old woman who developed endogenous endophthalmitis, eye infection involving the vitreous and/or aqueous humor, after developing Aeromonas-related gastroenteritis with progression to sepsis (Durand, 2013; Ryan et al., 2017).
The species A. veronii and A. hydrophila have been related to cases of pneumonia in both immunocompromised and immunocompetent patients with or without prior contact with suspicious water samples (David Reines and Cook, 1981; Ku and Yu, 2017). Such complication was also reported as a consequence of a near-drowning case of a 43-year-old man, whose clinical course evolved to multiple organ failure and death (Ender et al., 1996).
Cases involving genitourinary tract infections by Aeromonas species have been generally described as infrequent episodes, usually reported in patients with reduced immunity or undergoing invasive therapeutical procedures (Chao et al., 2012). Aeromonas hydrophila was found to be the cause of hematuria in a 42-year-old patient with a history of kidney transplantation (Hussain et al., 2018). The same species was isolated by peripheral veins and dialysis catheter cultures of a 55-year-old man that experienced kidney failure and was initiated on hemodialysis (Khalil et al., 2013). The insertion of these medical devices has been related to a large percentage of cases of bloodstream infections, and the treatment duration has been one of the risk factors for contamination by microorganisms (Kumbar and Yee, 2019). It was reported a case of a 42-year-old woman who died of bacteremia involving A. hydrophila in the course of hemodialysis sessions due to chronic kidney failure (Lin et al., 1996). Aeromonas caviae and A. veronii have also been detected as the cause of genitourinary tract infections in both healthy and immunosuppressed patients (Chao et al., 2012).
The involvement of the bones and joints due to infections represents a serious health problem, which can mainly culminate in the patient’s disability (Bejon, 2017). The potential of Aeromonads to colonize and infect these organs has already been reported, especially as a consequence of a previous wound or exposure trauma contamination (Janda and Abbott, 2010). Aeromonas sobria was the cause of ethmoiditis in a 16-year-old boy who experienced fever, eye swelling, vomiting, and headache after playing in a river (Couturier et al., 2017). Aeromonas hydrophila was detected from blood cultures of a cirrhotic patient who developed bacteremia followed by acute osteomyelitis (Lee et al., 2003). Similarly, the same species was found to be the cause of chronic osteomyelitis in a 50-year-old diabetic patient (Agrawal et al., 2017).
Differential Diagnosis
Although Aeromonas species can cause extraintestinal infections, such as skin and soft-tissue infections, one of the main consequences of Aeromonas infection is gastroenteritis, as observed according to the epidemiological data presented. Microbiology laboratories do not usually investigate Aeromonas spp. in diarrheal stools. The most commonly searched bacteria are Salmonella, Shigella, Campylobacter, and Escherichia coli (Schuetz, 2019).
Gastroenteritis may be caused by viral, bacterial, and parasitic pathogens whose clinical symptoms may be similar, so analysis with the patients’ stool becomes indispensable to promote differential diagnosis. Aeromonas spp. can grow in routine culture media commonly used in clinical laboratories, such as sheep blood agar (SBA) and chocolate agar. In addition, these microorganisms also grow in specific culture media for the isolation of enteropathogenic bacteria, for example, hektoen enteric agar, xylose deoxycholate agar (XLD) agar, and MacConkey agar (Carr, 2016). Moreover, Aeromonas recovery has been facilitated using enrichment broths, for example, alkaline peptone water under overnight incubation and subcultured onto blood ampicillin and cefsulodin irgasan novobiocin (CIN) agars (Igbinosa et al., 2012).
In addition to growth in culture medium, it is important to perform other phenotypic tests, such as different biochemical tests, for more accurate identification. For example, the fact that most Aeromonas organisms have a positive oxidase reaction, resistance to the vibriostatic compound O/129, absence of ornithine decarboxylase activity, and no growth in 6% NaCl allows their differentiation with the genera Vibrio and Plesiomonas (Batra et al., 2016). Aeromonas can grow on selective and differential enteric agars; however, the carbohydrate contained in these agars can influence the growth of these microorganisms and is therefore not ideal for primary isolation in fecal samples of Aeromonas. For example, the ability to ferment carbohydrates can depend on the species, carbohydrates, such as xylose and lactose, can inhibit the growth of some Aeromonas, and a false-negative oxidase reaction can occur due to an acidification process in the medium (Oliveira et al., 2020).
However, the laboratory screening using phenotypic tests can still generate doubts about the correct diagnosis of the bacteria causing the infection; for example, the distinction between V. cholera and Aeromonas spp. in stool samples from patients with diarrheal episodes can only be achieved with genome sequencing analysis (Van Zwetselaar et al., 2018). The molecular identification of Aeromonas species can be performed through 16S rRNA gene analysis, housekeeping genes, genotyping techniques, the latter includes different methods, such as multilocus sequence typing (MLST) and enterobacterial repetitive intergenic consensus-PCR (ERIC-PCR; Fernández-Bravo and Figueras, 2020). Aeromonas specification is not commonly performed clinically, although its species can be identified quickly, for example by employing matrix-assisted laser desorption–ionization time-of-flight mass spectrometry (MALDI-TOF; Benagli et al., 2012; Akyar and Can, 2013; Chen et al., 2014a).
Antibiotic Responses and Therapeutic Efficacy
Prescribing antibiotics in clinical practice was undoubtedly a revolutionary milestone in medicine regarding therapy against bacterial infections (Baron et al., 2017). The antibiotics era, which began around 1930 until the current days, has saved countless lives throughout the story. However, it brought one of the major and unavoidable public health problems of the modern world: the generation of multi-resistant bacteria (Dimopoulos et al., 2016; Baron et al., 2017; Dodds, 2017; Sánchez and Demain, 2017). The uncontrolled usage and irregular disposal of antibiotics, among other chemical compounds, that is, several drugs and personal use products, promote a propitious environment for the development of hard-to-treat microorganisms that become a threat to human health by sharing and acquiring resistance mechanisms which they naturally might not have (Chaturvedi et al., 2021). Although there has been great concern in recent years about environmental contamination by chemical and antimicrobial compounds, with a consequent increase in resistant microorganisms (Figueira et al., 2011), the history of humanity’s relationship with antibiotics has established a cycle of dependence that—apparently—will no sooner end. These medicines are still our front line in the fight against bacterial infections, and their consumption is estimated to globally increase approximately 200% by 2030 (Klein et al., 2018; Zheng et al., 2021).
Wastewater effluents derived from hospitals, veterinary clinics, industries, and aquaculture farms make aquatic environments great spreaders of multi-resistant pathogens (Baquero et al., 2008; Baron et al., 2017). Thus, Aeromonas, as natural inhabitants of these ecosystems, have a wide antibiotic resistance profile and are constantly isolated from several species of fish and other animals (Beaz-Hidalgo and Figueras, 2013). Aeromonads acquire and share antibiotic resistance genes by transmitting mobile elements like plasmids, integrons, insertion sequences, and transposons (Piotrowska and Popowska, 2015; Stratev and Odeyemi, 2016). These genetic compounds are known as the “mobilome” and are permanently subjected to evolution according to changes in the environment (Piotrowska and Popowska, 2015).
It has been described the production of 4 main groups of beta-lactamases, divided from Class A to Class D, which confer to the Aeromonas a potential defense against the action of beta-lactam drugs (Stratev and Odeyemi, 2016; Fernández-Bravo and Figueras, 2020). The antimicrobial resistance of 24 strains of Aeromonas isolated from Nile tilapia and domestic fowl was evaluated. The strains showed to be invulnerable to the beta-lactams amoxicillin and ampicillin/sulbactam, as well as to streptomycin, from aminoglycoside’s class (Abu-Elala et al., 2015). Aeromonads isolates from cow fecal samples from different farms also showed complete resistance to a large group of beta-lactam antibiotics and susceptibility to cephamycin, tetracycline, ciprofloxacin, and gentamicin (Igbinosa et al., 2015). In addition, sensitivity to cefepime was also observed in strains obtained from commercialized/farmed shellfish as well as aquatic environment samples (Chen et al., 2021). Aeromonads from cultured freshwater fishes showed main resistance to ampicillin and amoxicillin and absolute sensitivity to levofloxacin (Azzam-Sayuti et al., 2021). Besides beta-lactams, resistance against colistin can also be chromosomally mediated or transferred by the mobilome. This antibiotic can disrupt the membrane of gram-negative bacteria by interacting with surface LPS and is used as last resort for infections cause by multi-drug resistant microorganisms (MDR). Reports showed the existence of colistin-resistant Aeromonads, especially among the isolates obtained from clinical samples (Gonzalez-Avila et al., 2021).
Aeromonas are also capable of colonizing water treatment plants and, consequently, contaminate both the content intended for human consumption and the environment in which effluents are disposed (Figueira et al., 2011). Strains obtained from a domestic and hospital treatment system have been shown to resist three or more classes of antibiotics, including tigecycline, another drug used as a last line in cases involving MDR (Harnisz and Korzeniewska, 2018). The hazardousness of the dissemination of these microorganisms in the environment, arising from the addition of hospital waste to domestic effluents in municipal water treatment systems, has already been reported (Varela et al., 2016).
Although the wide antibiotic resistance and susceptibility profiles within the Aeromonas genus, it is believed that the therapeutic administration of these drugs should not be restricted to specific species (Janda and Abbott, 2010). Strains of A. trota obtained from clinical samples were susceptible to ampicillin, an antibiotic generally not recommended for the treatment of infections caused by this genus (Carnahan et al., 1991; Janda and Abbott, 2010; Bhowmick and Bhattacharjee, 2018). In addition, (Hughes et al., 2016) isolated A. veronii from a stool culture and found that this strain was resistant to ertapenem and susceptible to imipenem and meropenem. These same authors also identified in perirectal isolates from two different patients the species A. veronii and A. hydrophila, which were resistant to all carbapenems previously cited. Carbapenems are widely used for therapy against MDR infections and resistance to this antibiotic is a global concern (Nordmann and Poirel, 2019; Kaluba et al., 2021). Previous detection of carbapenem-resistant bacteria is extremely important to improve the patient’s prognosis and thus reduce mortality. Noteworthy, the execution of the antibiogram test in clinical practice is crucial in prescribing antibiotics able to contribute to the therapeutic process (Hughes et al., 2016; Nordmann and Poirel, 2019).
Symptoms of acute gastroenteritis present commonly as self-limiting within approximately 5 days (Graves, 2013). Dehydration, caused by successive diarrheal episodes, is reversed by oral or intravenous rehydration techniques to balance body fluids and electrolytes (Graves, 2013; Mosegui et al., 2019). In these cases, antibiotics have been prescribed to quickly reduce the frequency of diarrhea, shorten the recovery time, and control the contagion, since it reduces the release of the pathogen in stools (Graves, 2013; Cohen et al., 2017). When dealing with antibiotics, the appropriate choice of empirical treatment before antibiogram results is very important, especially for reducing bacterial resistance (Zhu et al., 2021). Aeromonas spp. isolates from stool samples from children in a diarrheal outbreak demonstrated susceptibility to gentamicin, amicin, and cefepime (Soltan Dallal et al., 2016). Ciprofloxacin was used empirically in association with rehydration therapy in cases of gastroenteritis by A. hydrophila (Van Zwetselaar et al., 2018). Oral prescription of the same antibiotic was reported according to the results of the antibiogram performed with an A. hydrophila strain detected by stool culture from a patient experiencing gastroenteritis (Ahishali et al., 2007). Empirical infusion of sulbactam/ampicillin was used to treat enteritis by Aeromonas, with subsequent change of therapy by oral levofloxacin (Kishimoto and Watari, 2018).
Considering the therapy against peritonitis associated with PD, it is recommended by the International Society for Peritoneal Dialysis that antibiotics should be prescribed even if the infection is only a suspect; being administrated preferably by intraperitoneal route (Al Sahlawi et al., 2020). Vancomycin and ceftazidime were used empirically in a case of peritonitis involving a PD patient. Based on susceptibility testing, only ceftazidime was continued in the course of treatment of A. hydrophila infection (Kim et al., 2018). In a similar case involving A. sobria, the PD patient was treated with empirical teicoplanin and cefotiam. According to the antibiogram, therapy was replaced by intraperitoneal and intravenous infusion of amikacin and levofloxacin, respectively (Song et al., 2019).
Skin infections are classified according to the location of the lesion, analysis of its extension, and degree of involvement of the adjacent superficial and deep tissues (Ramakrishnan et al., 2015; Jabbour and Kanj, 2021). Thus, the therapeutic strategy can range from topical treatment to administrate antibiotics and surgical procedures to remove necrotic tissues (Jabbour and Kanj, 2021). Due to the multiple causes and origins of lesions and skin contamination, emergencies usually require rapid administration of empirical antibiotics, before susceptibility testing, to preserve the patient’s life and eventually reduce the need for invasive approaches (Abrahamian et al., 2008). Aeromonas hydrophila has been frequently reported in several cases of skin infection with previous trauma. Gentamicin and carbenicillin were used empirically to treat an infection in a puncture wound. Culture of purulent material and subsequent susceptibility testing isolated a strain of A. hydrophila sensitive to the aminoglycoside class, tetracycline, and chloramphenicol (Katz and Smith, 1980). The same species was detected in a case of postoperative sepsis due to a hand injury. Antibiogram revealed strain sensitivity to different classes of antibiotics, but resistance to amoxicillin/clavulanic acid, erythromycin, and clindamycin (Yang et al., 2004). Aeromonas hydrophila was also detected in purulent samples collected during surgical incision at sites of foot trauma infection. Levofloxacin and ampicillin/sulbactam were used empirically for adult and pediatric patients, respectively. After test results, the strains obtained from the cultures demonstrated susceptibility to levofloxacin and trimethoprim/sulfamethoxazole (Larka et al., 2003). Aeromonas species were detected in a study involving 129 cancer patients who experienced polymicrobial skin and soft tissue infections without previous exposure to water. Therapeutic administration of ceftazidime, ciprofloxacin, and ceftriaxone was reported (Chao et al., 2013a).
The management of other skin and soft tissue infections has also been reported. Aforementioned, A. hydrophila has been the underlying cause of folliculitis (Mulholland and Yong-Gee, 2008; Manresa et al., 2009; Olszewski et al., 2017). In these cases, the main therapeutical strategy has been using topical drugs and oral antibiotics have been chosen as a second-line treatment if there is no improvement in the infectious scenario (Clebak and Malone, 2018). Topical administration of gentamicin was prescribed to treat pediatric patients experiencing Aeromonas folliculitis (Manresa et al., 2009). The isolated strain of A. hydrophila has also been shown to be susceptible to other antibiotics. In the case of spa bath folliculitis, oral dicloxacillin was used empirically, being later replaced by oral ciprofloxacin according to antibiogram (Mulholland and Yong-Gee, 2008). Empirical use of ampicillin/sulbactam did not contain the progression of infection in a patient suffering from NF by A. sobria. Therapy was initially changed to ceftriaxone and levofloxacin and then to meropenem and linezolid. Susceptibility testing revealed resistance of the strain to meropenem, which was discontinued and replaced by ceftazidime (Spadaro et al., 2014). On the other hand, the prescription of meropenem was crucial in the prognosis of a patient diagnosed with NF by A. caviae, whose infection was also not controlled by empirical administration of antibiotics (Park et al., 2010). In these cases, in addition to drug therapy, surgical procedures of debridement and fasciotomies are also critical in the treatment and survival of the affected patient (Clebak and Malone, 2018). Other therapeutical strategies for uncommon Aeromonas human infections are summarized in Table 1.
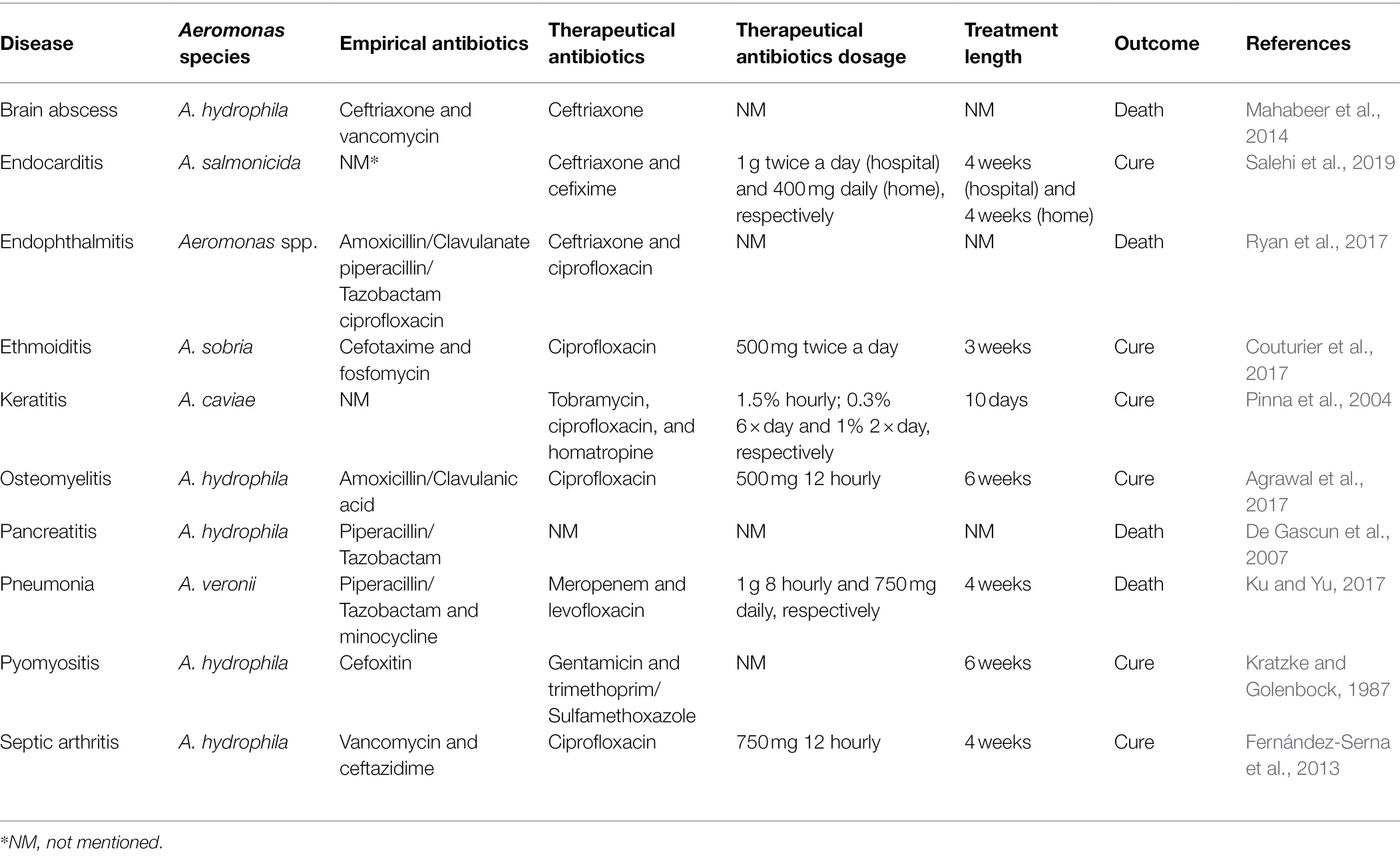
Table 1. Antimicrobial strategies and respective outcomes for uncommon Aeromonas human health disorders.
Conclusion
For a long time, the genus Aeromonas was erroneously dissociated from the group of bacterial pathogens that have caused infections in humans. Some signs, like several diarrheal outbreaks around the world and widespread distribution of the Aeromonas in the environment reveal that these microorganisms were present in the medical routine for a very long time. Moreover, a great number of lives were taken under the consequences of its infectious processes. Given the diversity of clinical manifestations that Aeromonads can cause in both immunocompromised and immunocompetent patients, physicians should not underestimate this bacterial genus. As emergent pathogens, Aeromonas species are as common as other bacterial pathogens and are more prone to acquire multi-drug resistance, representing a severe threat to human health in the future. Therefore, progress in scientific studies aiming at new methods for Aeromonas identification as well as appropriate antimicrobial strategies will be a potential help for clinical approaches.
Author Contributions
RBGP and LCBBC designed the structure of the manuscript. RBGP and WFdO wrote the review. MTdSC, AF, and LCBBC reviewed and approved the final version of the manuscript. All authors contributed to the article and approved the submitted version.
Funding
Conselho Nacional de Desenvolvimento Científico e Tecnológico, Fundação de Amparo à Ciência e Tecnologia do Estado de Pernambuco, and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior were responsible for fellowship.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) is acknowledged for fellowships (MTdSC, AF, and LCBBC) and grants. Authors are also grateful to the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) and to the Fundação de Amparo à Ciência e Tecnologia do Estado de Pernambuco (FACEPE) for financial supports. Authors pay homage to victims of the SARS-CoV-2 virus pandemic. In addition, to all scientific community and health professionals that were and are on the front line in the combat against COVID-19; may your efforts never be forgotten by humanity.
References
Abbott, S. L., Cheung, W. K. W., and Janda, J. M. (2003). The genus Aeromonas: biochemical characteristics, atypical reactions, and phenotypic identification schemes. J. Clin. Microbiol. 41, 2348–2357. doi: 10.1128/JCM.41.6.2348-2357.2003
Abrahamian, F. M., Talan, D. A., and Moran, G. J. (2008). Management of skin and soft-tissue infections in the emergency department. Infect. Dis. Clin. N. Am. 22, 89–116. doi: 10.1016/j.idc.2007.12.001
Abu-Elala, N., Abdelsalam, M., Marouf, S., and Setta, A. (2015). Comparative analysis of virulence genes, antibiotic resistance and gyrB-based phylogeny of motile Aeromonas species isolates from Nile tilapia and domestic fowl. Lett. Appl. Microbiol. 61, 429–436. doi: 10.1111/lam.12484
Agrawal, S., Srigyan, D., Nag, H. L., Kapil, A., and Dhawan, B. (2017). Chronic osteomyelitis by Aeromonas hydrophila: a silente cause of concern. J. Lab. Physicians 9, 264–268. doi: 10.4103/JLP.JLP
Aguilera-Arreola, M. G., Hernández-Rodríguez, C., Zúñiga, G., Figueras, M. J., Garduño, R. A., and Castro-Escarpulli, G. (2007). Virulence potential and genetic diversity of Aeromonas caviae, Aeromonas veronii, and Aeromonas hydrophila clinical isolates from Mexico and Spain: a comparative study. Can. J. Microbiol. 53, 877–887. doi: 10.1139/W07-051
Ahishali, E., Pinarbasi, B., Akyuz, F., Ibrisim, D., Kaymakoglu, S., and Mungan, Z. (2007). A case of Aeromonas hydrophila enteritis in the course of ulcerative colitis. Eur. J. Intern. Med. 18, 430–431. doi: 10.1016/j.ejim.2006.12.008
Ahmed, R. M., Ismaiel, A. A., Abou Zeid, A., Ibrahim, R. A., and Enan, G. (2021). Biological characteristics of enteropathogenic Aeromonas species isolated from different Egyptian foods. Biologia 76, 1577–1586. doi: 10.1007/s11756-021-00696-y
Akyar, I., and Can, S. (2013). Rapid identification of Aeromonas species in stool samples with chromogenic media and matrix-assisted laser desorption ionization-time of flight mass spectrometry: an institutional experience. Turkish J. Med. Sci. 43, 388–392. doi: 10.3906/sag-1203-63
Al Sahlawi, M., Bargman, J. M., and Perl, J. (2020). Peritoneal dialysis–associated peritonitis: suggestions for management and mistakes to avoid. Kidney Med. 2, 467–475. doi: 10.1016/j.xkme.2020.04.010
Ali, S. S., and Lateef, F. (2016). Laboratory risk indicators for acute necrotizing fasciitis in the emergency setting. J. Acute Dis. 5, 114–116. doi: 10.1016/j.joad.2015.11.003
Azzam-Sayuti, M., Ina-Salwany, M. Y., Zamri-Saad, M., Yusof, M. T., Annas, S., Najihah, M. Y., et al. (2021). The prevalence, putative virulence genes and antibiotic resistance profiles of Aeromonas spp. isolated from cultured freshwater fishes in peninsular Malaysia. Aquaculture 540:736719. doi: 10.1016/j.aquaculture.2021.736719
Baquero, F., Martínez, J. L., and Cantón, R. (2008). Antibiotics and antibiotic resistance in water environments. Curr. Opin. Biotechnol. 19, 260–265. doi: 10.1016/j.copbio.2008.05.006
Barger, P. C., Liles, M. R., Beck, B. H., and Newton, J. C. (2021). Differential production and secretion of potentially toxigenic extracellular proteins from hypervirulent Aeromonas hydrophila under biofilm and planktonic culture. BMC Microbiol. 21, 1–16. doi: 10.1186/s12866-021-02088-3
Baron, S., Granier, S. A., Larvor, E., Jouy, E., Cineux, M., Wilhelm, A., et al. (2017). Aeromonas diversity and antimicrobial susceptibility in freshwater: an attempt to set generic epidemiological cut-off values. Front. Microbiol. 8:503. doi: 10.3389/fmicb.2017.00503
Barrett, J., and Fhogartaigh, C. N. (2017). Bacterial gastroenteritis. Medicine 45, 683–689. doi: 10.1016/j.mpmed.2017.08.002
Batra, P., Mathur, P., and Misra, M. C. (2016). Aeromonas spp.: an emerging nosocomial pathogen. J. Lab. Physicians 8, 001–004. doi: 10.4103/0974-2727.176234
Beaz-Hidalgo, R., and Figueras, M. J. (2013). Aeromonas spp. whole genomes and virulence factors implicated in fish disease. J. Fish Dis. 36, 371–388. doi: 10.1111/jfd.12025
Benagli, C., Demarta, A., Caminada, A. P., Ziegler, D., Petrini, O., and Tonolla, M. (2012). A rapid MALDI-TOF MS identification database at genospecies level for clinical and environmental aeromonas strains. PLoS One 7, e48441–e48446. doi: 10.1371/journal.pone.0048441
Bhaijee, F., Arnold, C., Lam-Himlin, D., Montgomery, E. A., and Voltaggio, L. (2015). Infectious mimics of inflammatory bowel disease. Diagn. Histopathol. 21, 267–275. doi: 10.1016/j.mpdhp.2015.06.015
Bhowmick, U. D., and Bhattacharjee, S. (2018). Bacteriological, clinical and virulence aspects of Aeromonas-associated diseases in humans. Pol. J. Microbiol. 67, 137–149. doi: 10.21307/pjm-2018-020
Bruscolini, F., Barbieri, F., Battistelli, M., Betti, M., Dominici, S., Manti, A., et al. (2014). A multi-approach study of influence of growth temperature and nutrient deprivation in a strain of Aeromonas hydrophila. Int. J. Food Microbiol. 188, 1–10. doi: 10.1016/j.ijfoodmicro.2014.07.005
Byrd, A. L., Belkaid, Y., and Segre, J. A. (2018). The human skin microbiome. Nat. Rev. Microbiol. 16, 143–155. doi: 10.1038/nrmicro.2017.157
Carnahan, A. M., Chakraborty, T., Fanning, G. R., Verma, D., Ali, A., Janda, J. M., et al. (1991). Aeromonas trota sp. nov., an ampicillin-susceptible species isolated from clinical specimens. J. Clin. Microbiol. 29, 1206–1210. doi: 10.1128/jcm.29.6.1206-1210.1991
Carr, F. J., (2016). Microbiology: A Fundamental Introduction, Journal of Microbiology and Experimentation Microbiology. MedCrave Group LLC. 1–34.
Castro-Escarpulli, G., Figueras, M. J., Aguilera-Arreola, G., Soler, L., Fernández-Rendón, E., Aparicio, G. O., et al. (2003). Characterisation of Aeromonas spp. isolated from frozen fish intended for human consumption in Mexico. Int. J. Food Microbiol. 84, 41–49. doi: 10.1016/S0168-1605(02)00393-8
Cefalu, J. E., Barrier, K. M., and Davis, A. H. (2017). Wound infections in critical care. Crit. Care Nurs. Clin. North Am. 29, 81–96. doi: 10.1016/j.cnc.2016.09.009
Chan, F. K. L., Ching, J. Y. L., Ling, T. K. W., Chung, S. C. S., and Sung, J. J. Y. (2000). Aeromonas infection in acute suppurative cholangitis: review of 30 cases. J. Inf. Secur. 40, 69–73. doi: 10.1053/jinf.1999.0594
Chang, H.-L., Chen, P.-L., Lin, S.-Y., Chen, T.-C., Chang, K., Ko, W.-C., et al. (2018). Two fatal cases of Aeromonas dhakensis bacteremia and necrotizing fasciitis in severe dengue patients. J. Microbiol. Immunol. Infect. 51, 692–694. doi: 10.1016/j.jmii.2018.03.003
Chao, C. M., Gau, S. J., and Lai, C. C. (2012). Aeromonas genitourinary tract infection. J. Inf. Secur. 65, 573–575. doi: 10.1016/j.jinf.2012.06.012
Chao, C. M., Lai, C. C., Gau, S. J., and Hsueh, P. R. (2013a). Skin and soft tissue infection caused by Aeromonas species in cancer patients. J. Microbiol. Immunol. Infect. 46, 144–146. doi: 10.1016/j.jmii.2013.02.006
Chao, C. M., Lai, C. C., Tang, H. J., Ko, W. C., and Hsueh, P. R. (2013b). Biliary tract infections caused by Aeromonas species. Eur. J. Clin. Microbiol. Infect. Dis. 32, 245–251. doi: 10.1007/s10096-012-1736-1
Chaturvedi, P., Shukla, P., Giri, B. S., Chowdhary, P., Chandra, R., Gupta, P., et al. (2021). Prevalence and hazardous impact of pharmaceutical and personal care products and antibiotics in environment: a review on emerging contaminants. Environ. Res. 194:110664. doi: 10.1016/j.envres.2020.110664
Chen, J. S., Hsu, G. J., Hsu, B. M., Yang, P. Y., Kuo, Y. J., Wang, J. L., et al. (2021). Prevalence, virulence-gene profiles, antimicrobial resistance, and genetic diversity of human pathogenic Aeromonas spp. from shellfish and aquatic environments. Environ. Pollut. 287:117361. doi: 10.1016/j.envpol.2021.117361
Chen, P. L., Lee, T. F., Wu, C. J., Teng, S. H., Teng, L. J., Ko, W. C., et al. (2014a). Matrix-assisted laser desorption ionization-time of flight mass spectrometry can accurately differentiate Aeromonas dhakensis from A. hydrophila, A. caviae, and A. veronii. J. Clin. Microbiol. 52, 2625–2628. doi: 10.1128/JCM.01025-14
Chen, P. L., Tsai, P. J., Chen, C. S., Lu, Y. C., Chen, H. M., Lee, N. Y., et al. (2015). Aeromonas stool isolates from individuals with or without diarrhea in southern Taiwan: predominance of Aeromonas veronii. J. Microbiol. Immunol. Infect. 48, 618–624. doi: 10.1016/j.jmii.2014.08.007
Chen, P. L., Wu, C. J., Chen, C. S., Tsai, P. J., Tang, H. J., and Ko, W. C. (2014b). A comparative study of clinical Aeromonas dhakensis and Aeromonas hydrophila isolates in southern Taiwan: A. dhakensis is more predominant and virulent. Clin. Microbiol. Infect. 20, 0428–0434. doi: 10.1111/1469-0691.12456
Cheng, Y. W., and Fischer, M. (2020). Fecal microbiota transplantation for ulcerative colitis. Are we ready for primetime? Gastroenterol. Clin. N. Am. 49, 739–752. doi: 10.1016/j.gtc.2020.08.006
Chim, H., and Song, C. (2007). Aeromonas infection in critically ill burn patients. Burns 33, 756–759. doi: 10.1016/j.burns.2006.10.389
Cho, Y., and Johnson, D. W. (2014). Peritoneal dialysis-related peritonitis: towards improving evidence, practices, and outcomes. Am. J. Kidney Dis. 64, 278–289. doi: 10.1053/j.ajkd.2014.02.025
Chuang, H. C., Ho, Y. H., Lay, C. J., Wang, L. S., and Tsai, Y. S. (2011). Different clinical characteristics among Aeromonas hydrophila, Aeromonas veronii biovar sobria and Aeromonas caviae monomicrobial bacteremia. J. Korean Med. Sci. 26, 1415–1420. doi: 10.3346/jkms.2011.26.11.1415
Clebak, K. T., and Malone, M. A. (2018). Skin infections. Prim. Care 45, 433–454. doi: 10.1016/j.pop.2018.05.004
Cohen, R., Raymond, J., and Gendrel, D. (2017). Antimicrobial treatment of diarrhea/acute gastroenteritis in children. Arch. Pediatr. 24, S26–S29. doi: 10.1016/S0929-693X(17)30515-8
Conte, D., Palmeiro, J. K., Bavaroski, A. A., Rodrigues, L. S., Cardozo, D., Tomaz, A. P., et al. (2021). Antimicrobial resistance in Aeromonas species isolated from aquatic environments in Brazil. J. Appl. Microbiol. 131, 169–181. doi: 10.1111/jam.14965
Couturier, A., Chidiac, C., Truy, E., and Ferry, T. (2017). Ethmoiditis with subperiosteal and retro-ocular abscesses due to Aeromonas sobria in a 16-year-old boy exposed to the Ardèche river. BMJ Case Rep. 2017:bcr2017219505. doi: 10.1136/bcr-2017-219505
Cui, H., Hao, S., and Arous, E. (2007). A distinct cause of necrotizing fasciitis: Aeromonas veronii biovar sobria. Surg. Infect. 8, 523–528. doi: 10.1089/sur.2006.046
Dallaire-Dufresne, S., Tanaka, K. H., Trudel, M. V., Lafaille, A., and Charette, S. J. (2014). Virulence, genomic features, and plasticity of Aeromonas salmonicida subsp. salmonicida, the causative agent of fish furunculosis. Vet. Microbiol. 169, 1–7. doi: 10.1016/j.vetmic.2013.06.025
David Reines, H., and Cook, F. V. (1981). Pneumonia and bacteremia due to Aeromonas hydrophila. Chest 80, 264–267. doi: 10.1378/chest.80.3.264
De Gascun, C. F., Rajan, L., O’Neill, E., Downey, P., and Smyth, E. G. (2007). Pancreatic abscess due to Aeromonas hydrophila. J. Inf. Secur. 54, e59–e60. doi: 10.1016/j.jinf.2006.03.037
Dimopoulos, G., Kollef, M. H., and Cohen, J. (2016). In 2035, will all bacteria be multiresistant? Yes. Intensive Care Med. 42, 2014–2016. doi: 10.1007/s00134-016-4310-y
DiNubile, M. J., and Lipsky, B. A. (2004). Complicated infections of skin and skin structures: when the infection is more than skip deep. J. Antimicrob. Chemother. 53, ii37–ii50. doi: 10.1093/jac/dkh202
Dodds, D. R. (2017). Antibiotic resistance: a current epilogue. Biochem. Pharmacol. 134, 139–146. doi: 10.1016/j.bcp.2016.12.005
Dryden, M. S. (2010). Complicated skin and soft tissue infection. J. Antimicrob. Chemother. 65, 35–44. doi: 10.1093/jac/dkq302
Du, L., and Ha, C. (2020). Epidemiology and pathogenesis of ulcerative colitis. Gastroenterol. Clin. N. Am. 49, 643–654. doi: 10.1016/j.gtc.2020.07.005
Duman, M., Gencpinar, P., Biçmen, M., Arslan, N., Özden, Ö., Üzüm, Ö., et al. (2015). Fecal calprotectin: can be used to distinguish between bacterial and viral gastroenteritis in children? Am. J. Emerg. Med. 33, 1436–1439. doi: 10.1016/j.ajem.2015.07.007
Durand, M. L. (2013). Endophthalmitis. Clin. Microbiol. Infect. 19, 227–234. doi: 10.1111/1469-0691.12118
Elorza, A., Rodríguez-Lago, I., Martínez, P., Hidalgo, A., Aguirre, U., and Cabriada, J. L. (2020). Gastrointestinal infection with Aeromonas: incidence and relationship to inflammatory bowel disease. Gastroenterol. Hepatol. 43, 614–619. doi: 10.1016/j.gastrohep.2020.04.014
Ender, P. T., Dolan, M. J., Dolan, D., Farmer, J. C., and Melcher, G. P. (1996). Near-drowning associated Aeromonas pneumonia. J. Emerg. Med. 14, 737–741. doi: 10.1016/S0736-4679(96)00183-7
Fernández-Bravo, A., and Figueras, M. J. (2020). An update on the genus Aeromonas: taxonomy, epidemiology, and pathogenicity. Microorganisms 8, 1–39. doi: 10.3390/microorganisms8010129
Fernández-Serna, M., Arboleya, L., Alonso, S., Queiro, R., and Alperi, M. (2013). Dropped head syndrome in a patient with scleromyositis. J. Clin. Rheumatol. 19, 32–34. doi: 10.1097/RHU.0b013e31827d8778
Figueira, V., Vaz-Moreira, I., Silva, M., and Manaia, C. M. (2011). Diversity and antibiotic resistance of Aeromonas spp. in drinking and waste water treatment plants. Water Res. 5, 5599–5611. doi: 10.1016/j.watres.2011.08.021
Figueras, M. J. S., and Ashbolt, N. (2019). In: Global Water Pathogen Project. eds. J.B. Rose and B. Jiménez-Cisneros, Michigan State University, E. Lansing, MI, UNESCO. 1–34. doi: 10.14321/waterpathogens.21
Fleckenstein, J. M., Kuhlmann, F. M., and Sheik, A. (2021). Acute bacterial gastroenteritis. Gastroenterol. Clin. N. Am. 50, 283–304. doi: 10.1016/j.gtc.2021.02.002
Fletscher Covaleda, G., Martínez González, C., and Galván-Villamarín, F. (2013). Fascitis necrotizante por Aeromona hydrophila en un niño inmunocompetente: reporte de caso y revisión de la literatura. Rev. Colomb. Ortop. y Traumatol. 27, 222–226. doi: 10.1016/S0120-8845(13)70023-3
Galler, H., Feierl, G., Petternel, C., Reinthaler, F. F., Haas, D., Habib, J., et al. (2018). Multiresistant bacteria isolated from activated sludge in Austria. Int. J. Environ. Res. Public Health 15, 1–11. doi: 10.3390/ijerph15030479
Gillis, L., and Wilkie, M. (2019). Peritoneal dialysis. Medicine 47, 603–608. doi: 10.1016/j.mpmed.2019.06.003
Girard, T. D., and Ely, E. W. (2007). Bacteremia and sepsis in older adults. Clin. Geriatr. Med. 23, 633–647. doi: 10.1016/j.cger.2007.05.003
Gonçalves Pessoa, R. B., de Oliveira, W. F., Marques, D. S. C., dos Santos Correia, M. T., de Carvalho, E. V. M. M., and Coelho, L. C. B. B. (2019). The genus Aeromonas: a general approach. Microb. Pathog. 130, 81–94. doi: 10.1016/j.micpath.2019.02.036
Gonzales, A. C., Denamur, E., and Orfila, J. (1989). Conjonctivite a Aeromonas sp. Med. Mal. Infect. 19, 415–417. doi: 10.1016/S0399-077X(89)80232-X
Gonzalez-Avila, L. U., Loyola-Cruz, M. A., Hernández-Cortez, C., Bello-López, J. M., and Castro-Escarpulli, G. (2021). Colistin resistance in Aeromonas spp. Int. J. Mol. Sci. 22, 1–10. doi: 10.3390/ijms22115974
Grilo, M. L., Sousa-Santos, C., Robalo, J., and Oliveira, M. (2020). The potential of Aeromonas spp. from wildlife as antimicrobial resistance indicators in aquatic environments. Ecol. Indic. 115:106396. doi: 10.1016/j.ecolind.2020.106396
Hadano, Y., Tamagawa, K., and Ohkusu, K. (2017). Trauma wound related infection caused by Enterobacter cancerogenus and Aeromonas hydrophila. Intern. Med. 57, 131–133. doi: 10.2169/internalmedicine.9171-17
Harnisz, M., and Korzeniewska, E. (2018). The prevalence of multidrug-resistant Aeromonas spp. in the municipal wastewater system and their dissemination in the environment. Sci. Total Environ. 626, 377–383. doi: 10.1016/j.scitotenv.2018.01.100
Hasan, O., Khan, W., Jessar, M., Pathan, A. Z., and Lakdawala, R. H. (2018). Bone graft donor site infection with a rare organism, Aeromonas hydrophila. A typical location, presentation and organism with 2 years follow-up. Case report. Int. J. Surg. Case Rep. 51, 154–157. doi: 10.1016/j.ijscr.2018.08.037
Hoel, S., Vadstein, O., and Jakobsen, A. N. (2017). Species distribution and prevalence of putative virulence factors in mesophilic Aeromonas spp. isolated from fresh retail sushi. Front. Microbiol. 8:931. doi: 10.3389/fmicb.2017.00931
Hong, C. K., Chen, H. C., Su, W. R., and Lee, P. Y. (2018). Rapid progression and mortality of necrotizing fasciitis caused by Aeromonas hydrophila in a patient with type I open tibial fracture. Kaohsiung J. Med. Sci. 34, 307–309. doi: 10.1016/j.kjms.2017.12.001
Hughes, H. Y., Conlan, S. P., Lau, A. F., Dekker, J. P., Michelin, A. V., Youn, J. H., et al. (2016). Detection and whole-genome sequencing of carbapenemase- producing Aeromonas hydrophila isolates from routine perirectal surveillance culture. J. Clin. Microbiol. 54, 1167–1170. doi: 10.1128/JCM.03229-15
Hussain, S., Farhat, S., and Jasuja, S. (2018). Hematuria secondary to Aeromonas infection in a kidney transplant recipient. Saudi J. Kidney Dis. Transplant. 29, 976–978. doi: 10.4103/1319-2442.239635
Hynes, D., Duffin, C., and Catanzano, T. (2020). Infections of the hepatobiliary system. Semin. Ultrasound CT MR 41, 46–62. doi: 10.1053/j.sult.2019.10.003
Igbinosa, I. H., Igbinosa, E. O., and Okoh, A. I. (2015). Detection of antibiotic resistance, virulence gene determinants and biofilm formation in Aeromonas species isolated from cattle. Environ. Sci. Pollut. Res. 22, 17596–17605. doi: 10.1007/s11356-015-4934-4
Igbinosa, I. H., Igumbor, E. U., Aghdasi, F., Tom, M., and Okoh, A. I. (2012). Emerging Aeromonas species infections and their significance in public health. Sci. World J. 2012. doi: 10.1100/2012/625023
Jabbour, J. F., and Kanj, S. S. (2021). Gram-negative skin and soft tissue infections. Infect. Dis. Clin. N. Am. 35, 157–167. doi: 10.1016/j.idc.2020.10.008
Janda, J. M., and Abbott, S. L. (2010). The genus Aeromonas: taxonomy, pathogenicity, and infection. Clin. Microbiol. Rev. 23, 35–73. doi: 10.1128/CMR.00039-09
Jin, W. Y., Jang, S. J., Lee, M. J., Park, G., Kim, M. J., Kook, J. K., et al. (2011). Evaluation of VITEK 2, MicroScan, and Phoenix for identification of clinical isolates and reference strains. Diagn. Microbiol. Infect. Dis. 70, 442–447. doi: 10.1016/j.diagmicrobio.2011.04.013
Kaluba, C. K., Samutela, M. T., Kapesa, C., Muma, J. B., Hang’ombe, B. M., Hachaambwa, L., et al. (2021). Carbapenem resistance in Pseudomonas aeruginosa and Acinetobacter species at a large tertiary referral hospital in Lusaka, Zambia. Sci. African 13:e00908. doi: 10.1016/j.sciaf.2021.e00908
Katz, D., and Smith, H. (1980). Aeromonas hydrophila infection of a puncture wound. Ann. Emerg. Med. 9, 529–531. doi: 10.1016/S0196-0644(80)80193-4
Khalil, M. A. M., Rehman, A., Kashif, W. U., Rangasami, M., and Tan, J. (2013). A rare case of Aeromonas hydrophila catheter related sepsis in a patient with chronic kidney disease receiving steroids and dialysis: a case report and review of Aeromonas infections in chronic kidney disease patients. Case Rep. Nephrol. 2013, 1–5. doi: 10.1155/2013/735194
Kienzle, N., Muller, M., and Pegg, S. (2000). Aeromonas wound infection in burns. Burns 26, 478–482. doi: 10.1016/S0305-4179(99)00188-6
Kim, H. J., Park, H. S., Bae, E., Kim, H. W., Kim, B., Moon, K. H., et al. (2018). A case of peritoneal dialysis-related peritonitis caused by Aeromonas hydrophila in the patient receiving automated peritoneal dialysis. Electrolytes Blood Press. 16:27. doi: 10.5049/EBP.2018.16.2.27
Kishimoto, K., and Watari, T. (2018). Aeromonas enteritis: a great mimicker of acute appendicitis. QJM 111, 257–258. doi: 10.1093/qjmed/hcx261
Klein, E.Y., Boeckel, T.P.Van, Martinez, E.M., Pant, S., Gandra, S., and Levin, S.A., (2018). Global increase and geographic convergence in antibiotic consumption between 2000 and 2015. Proc. Natl. Acad. Sci. 115, 3463–3470. doi:doi: 10.1073/pnas.1717295115
Kratzke, R. A., and Golenbock, D. T. (1987). Pyomyositis and hepatic abscess in association with Aeromonas hydrophila sepsis. Am. J. Med. 83, 347–349. doi: 10.1016/0002-9343(87)90710-8
Ku, Y. H., and Yu, W. L. (2017). Extensive community-acquired pneumonia with hemophagocytic syndrome caused by Aeromonas veronii in an immunocompetent patient. J. Microbiol. Immunol. Infect. 50, 555–556. doi: 10.1016/j.jmii.2015.06.007
Kumbar, L., and Yee, J. (2019). Current concepts in hemodialysis vascular access infections. Adv. Chronic Kidney Dis. 26, 16–22. doi: 10.1053/j.ackd.2018.10.005
Lai, C. C., Shiao, C. C., Lu, G. D., and Ding, L. W. (2007). Aeromonas hydrophila and Aeromonas sobria bacteremia: rare pathogens of infection in a burn patient. Burns 33, 255–257. doi: 10.1016/j.burns.2006.06.003
Lamy, B., Laurent, F., Verdier, I., Decousser, J. W., Lecaillon, E., Marchandin, H., et al. (2010). Accuracy of 6 commercial systems for identifying clinical Aeromonas isolates. Diagn. Microbiol. Infect. Dis. 67, 9–14. doi: 10.1016/j.diagmicrobio.2009.12.012
Larka, U.-B., Ulett, D., Garrison, T., and Rockett, M. S. (2003). Aeromonas hydrophila infections after penetrating foot trauma. J. Foot Ankle Surg. 42, 305–308. doi: 10.1016/S1067-2516(03)00305-3
Lee, C. H., Liu, M. S., and Hsieh, S. H. (2003). Aeromonas hydrophila bacteremia presenting as non-traumatic acute osteomyelitis in a cirrhotic patient. Chang Gung Med. J. 26, 520–524.
Li, F., Wang, W., Zhu, Z., Chen, A., Du, P., Wang, R., et al. (2015). Distribution, virulence-associated genes and antimicrobial resistance of Aeromonas isolates from diarrheal patients and water, China. J. Inf. Secur. 70, 600–608. doi: 10.1016/j.jinf.2014.11.004
Lin, C.-S., and Lin, C.-W. (2019). Monomicrobial non-neutrocytic bacterascites caused by Aeromonas hydrophila in a patient with liver cirrhosis. Biomedicine 9:13. doi: 10.1051/bmdcn/2019090213
Lin, S. H., Shieh, S. D., Lin, Y. F., De Brauwer, E., Van Landuyt, H. W., Gordts, B., et al. (1996). Fatal Aeromonas hydrophila bacteremia in a hemodialysis patient treated with deferoxamine. Am. J. Kidney Dis. 27, 733–735. doi: 10.1016/S0272-6386(96)90112-2
Lippi, G., Danese, E., Cervellin, G., and Montagnana, M. (2014). Laboratory diagnostics of spontaneous bacterial peritonitis. Clin. Chim. Acta 430, 164–170. doi: 10.1016/j.cca.2014.01.023
Liu, D. (2015). “Aeromonas,” in Molecular Medical Microbiology: 2nd Edn. (eds) Y.-W. Tang, D. Liu, J. Schwartzman, M. Sussman, and I. Poxton (USA: Elsevier Ltd.), 1099–1110.
Lujan-Hernandez, J., Schultz, K. S., and Rothkopf, D. M. (2020). Rapidly progressive soft tissue infection of the upper extremity with Aeromonas veronii biovar sobria. J. Hand. Surg. Am. 45, 1091.e1–1091.e4. doi: 10.1016/j.jhsa.2020.02.003
Mahabeer, Y., Khumalo, A., Kiratu, E., and Mlisana, K. (2014). Posttraumatic brain abscess caused by Aeromonas hydrophila. J. Clin. Microbiol. 52, 1796–1797. doi: 10.1128/JCM.00267-14
Manresa, M. J., Villa, A. V., Giralt, A. G., and González-Enseñat, M. A. (2009). Aeromonas hydrophila folliculitis associated with an inflatable swimming pool: mimicking Pseudomonas aeruginosa infection. Pediatr. Dermatol. 26, 601–603. doi: 10.1111/j.1525-1470.2009.00993.x
Masters, M. C., Gupta, A. R., Rhodes, N. J., Flaherty, J. P., Zembower, T. R., Alghoul, M., et al. (2020). Multidrug resistant Aeromonas infection following medical leech therapy: a case report and development of a joint antimicrobial stewardship and infection prevention protocol. J. Glob. Antimicrob. Resist. 23, 349–351. doi: 10.1016/j.jgar.2020.10.010
Mbuthia, O. W., Mathenge, S. G., Oyaro, M. O., and Ng’ayo, M. O. (2018). Etiology and pathogenicity of bacterial isolates: a cross sectional study among diarrheal children below five years in central regions of Kenya. Pan Afr. Med. J. 31, 1–15. doi: 10.11604/pamj.2018.31.88.15644
McMahon, M. A. S., and Wilson, I. G. (2001). The occurrence of enteric pathogens and Aeromonas species in organic vegetables. Int. J. Food Microbiol. 70, 155–162. doi: 10.1016/S0168-1605(01)00535-9
Meng, S., Du, X. L., Wang, Y. L., Qu, F. T., Xie, G. L., Zhou, H. J., et al. (2021). Comparative study of the genetic diversity, antimicrobial resistance, and pathogenicity of Aeromonas isolates from clinical patients and healthy individuals. Biomed. Environ. Sci. 34, 454–464. doi: 10.3967/bes2021.062
Minasyan, H. (2019). Sepsis: mechanisms of bacterial injury to the patient. Scand. J. Trauma Resusc. Emerg. Med. 27, 1–22. doi: 10.1186/s13049-019-0596-4
Miyashita, H., Okamoto, K., Kobayashi, T., Wakabayashi, Y., Kitaura, S., Ikeuchi, K., et al. (2019). Bacterial peritonitis in a patient with malignant ascites caused by pancreatic carcinoma: case report and review of literature. J. Infect. Chemother. 25, 473–476. doi: 10.1016/j.jiac.2019.01.007
Mohan, B., Sethuraman, N., Verma, R., and Taneja, N. (2017). Speciation, clinical profile & antibiotic resistance in Aeromonas species isolated from cholera-like illnesses in a tertiary care hospital in North India. Indian J. Med. Res. 146, 517–520. doi: 10.4103/ijmr.IJMR
Monti, M., Torri, A., Amadori, E., Rossi, A., Bartolini, G., Casadei, C., et al. (2019). Aeromonas veronii biovar veronii and sepsis-infrequent complication of biliary drainage placement: a case report. World J. Clin. Cases 7, 759–764. doi: 10.12998/wjcc.v7.i6.759
Morales-Fuentes, G. A., Páez-Zayas, V. M., García-de la Rosa, Y. P., Villar-Chávez, S., Ramírez-Cisneros, D. A., Carballo-Zarate, A. A., et al. (2014). Colitis ulcerosa infecciosa por Aeromonas spp. Endoscopia 26, 19–22. doi: 10.1016/j.endomx.2014.04.004
Morgan, D. R., Johnson, P. C., Dupont, H. L., Satterwhite, T. K., and Wood, L. V. (1985). Lack of correlation between known virulence properties of Aeromonas hydrophila and enteropathogenicity for humans. Infect. Immun. 50, 62–65. doi: 10.1128/iai.50.1.62-65.1985
Mosegui, G. G., Vianna, C. M., Rodrigues, M. S., Valle, P. M., and Silva, F. V. (2019). Cost-effectiveness analysis of oral rehydration therapy compared to intravenous rehydration for acute gastroenteritis without severe dehydration treatment. J. Infect. Public Health 12, 816–821. doi: 10.1016/j.jiph.2019.05.001
Mulholland, A., and Yong-Gee, S. (2008). A possible new cause of spa bath folliculitis: Aeromonas hydrophila. Aust. J. Dermatol. 49, 39–41. doi: 10.1111/j.1440-0960.2007.00418.x
Narayan, N., and McCoubrey, G. (2019). Necrotizing fasciitis: a plastic surgeon’s perspective. Surgery 37, 33–37. doi: 10.1016/j.mpsur.2018.11.009
Nolla-Salas, J., Codina-Calero, J., Vallés-Angulo, S., Sitges-Serra, A., Zapatero-Ferrándiz, A., Climent, M. C., et al. (2017). Clinical significance and outcome of Aeromonas spp. infections among 204 adult patients. Eur. J. Clin. Microbiol. Infect. Dis. 36, 1393–1403. doi: 10.1007/s10096-017-2945-4
Nordmann, P., and Poirel, L. (2019). Epidemiology and diagnostics of carbapenem resistance in gram-negative bacteria. Clin. Infect. Dis. 69, S521–S528. doi: 10.1093/cid/ciz824
Oliveira, W. F., Santos, N. R. M., Cabrera, M. P., Ferreira, S. A. O., Raposo, B. L., Napoleão, T. H., et al. (2020). Bauhinia monandra leaf lectin (BmoLL) conjugated with quantum dots as fluorescent nanoprobes for biological studies: application to red blood cells. Methods Appl. Fluoresc. 8, 1–7. doi: 10.1088/2050-6120/ab9694
Olszewski, A. E., Karandikar, M. V., and Surana, N. K. (2017). Aeromonas as a cause of purulent folliculitis: a case report and review of the literature. J. Pediatric Infect. Dis. Soc. 6, e1–e3. doi: 10.1093/jpids/piw073
Pablos, M., Huys, G., Cnockaert, M., Rodríguez-Calleja, J. M., Otero, A., Santos, J. A., et al. (2011). Identification and epidemiological relationships of Aeromonas isolates from patients with diarrhea, drinking water and foods. Int. J. Food Microbiol. 147, 203–210. doi: 10.1016/j.ijfoodmicro.2011.04.006
Pablos, M., Rodríguez-Calleja, J. M., Santos, J. A., Otero, A., and García-López, M. L. (2009). Occurrence of motile Aeromonas in municipal drinking water and distribution of genes encoding virulence factors. Int. J. Food Microbiol. 135, 158–164. doi: 10.1016/j.ijfoodmicro.2009.08.020
Papadakis, V., Poniros, N., Katsibardi, K., Charissiadou, A. E., Anastasopoulos, J., and Polychronopoulou, S. (2012). Fulminant Aeromonas hydrophila infection during acute lymphoblastic leukemia treatment. J. Microbiol. Immunol. Infect. 45, 154–157. doi: 10.1016/j.jmii.2011.09.008
Park, S. Y., Jeong, W. K., Kim, M. J., Lee, K. M., Lee, W. S., and Lee, D. H. (2010). Necrotising fasciitis in both calves caused by Aeromonas caviae following aesthetic liposuction. J. Plast. Reconstr. Aesthet. Surg. 63, e695–e698. doi: 10.1016/j.bjps.2010.04.006
Parker, J. L., and Shaw, J. G. (2011). Aeromonas spp. clinical microbiology and disease. J. Inf. Secur. 62, 109–118. doi: 10.1016/j.jinf.2010.12.003
Pattanayak, S., Priyadarsini, S., Paul, A., Kumar, P. R., and Sahoo, P. K. (2020). Diversity of virulence-associated genes in pathogenic Aeromonas hydrophila isolates and their in vivo modulation at varied water temperatures. Microb. Pathog. 147:104424. doi: 10.1016/j.micpath.2020.104424
Pemberton, J. M., Kidd, S. P., and Schmidt, R. (1997). Secreted enzymes of Aeromonas. FEMS Microbiol. Lett. 152, 1–10. doi: 10.1111/j.1574-6968.1997.tb10401.x
Percival, S. L., and Williams, D. W. (2014). “Aeromonas,” in Microbiology of Waterborne Diseases (eds) S. L. Percival, D. W. Williams, N. F. Gray, M. V. Yates, and R. M. Chalmers (USA: Elsevier), 36, 49–64.
Pérez-García, D., Larios-Serrato, V., Rojas-Rios, R., Otero-Olarra, J. E., Mendoza-Sanchez, I., Curiel-Quesada, E., et al. (2021). Frequency and diversity of small plasmids in mesophilic Aeromonas isolates from fish, water and sediment. Plasmid 118, 1–10. doi: 10.1016/j.plasmid.2021.102607
Perner, A., Gordon, A. C., De Backer, D., Dimopoulos, G., Russell, J. A., Lipman, J., et al. (2016). Sepsis: frontiers in diagnosis, resuscitation and antibiotic therapy. Intensive Care Med. 42, 1958–1969. doi: 10.1007/s00134-016-4577-z
Pinna, A., Sechi, L. A., Zanetti, S., Usai, D., and Carta, F. (2004). Aeromonas caviae keratitis associated with contact lens wear. Ophthalmology 111, 348–351. doi: 10.1016/j.ophtha.2003.05.012
Piotrowska, M., and Popowska, M. (2015). Insight into the mobilome of Aeromonas strains. Front. Microbiol. 6:494. doi: 10.3389/fmicb.2015.00494
Praveen, P. K., Debnath, C., Shekhar, S., Dalai, N., and Ganguly, S. (2016). Incidence of Aeromonas spp. infection in fish and chicken meat and its related public health hazards: a review. Vet. World 9, 6–11. doi: 10.14202/vetworld.2016.6-11
Ramakrishnan, K., Salinas, R. C., and Higuita, N. I. A. (2015). Skin and soft tissue infections. Am. Fam. Physician 35, xiii–xxiv. doi: 10.1016/j.idc.2020.12.001
Rasmussen-Ivey, C. R., Figueras, M. J., McGarey, D., and Liles, M. R. (2016). Virulence factors of Aeromonas hydrophila: in the wake of reclassification. Front. Microbiol. 7:1337. doi: 10.3389/fmicb.2016.01337
Ribeiro, N. F. F., Heath, C. H., Kierath, J., Rea, S., Duncan-Smith, M., and Wood, F. M. (2010). Burn wounds infected by contaminated water: case reports, review of the literature and recommendations for treatment. Burns 36, 9–22. doi: 10.1016/j.burns.2009.03.002
Rutteman, B. (2017). Aeromonas wound infection in a healthy boy. JMM Case Rep. 4, e005129–e005180. doi: 10.1099/jmmcr.0.005129
Ryan, L., Higgins, G., and Doyle, M. (2017). Aeromonas species endogenous endophthalmitis. JMM Case Rep. 4, e005094–e005096. doi: 10.1099/jmmcr.0.005094
Salehi, M., Shadvar, S., Sadeghian, M., Doomanlou, M., Abdollahi, A., Manshadi, S. A. D., et al. (2019). Endocarditis with Aeromonas salmonicida. IDCases 18:e00625. doi: 10.1016/j.idcr.2019.e00625
Sánchez, S., and Demain, A. L. (2017). The amazing world of antibiotics. Biochem. Pharmacol. 133, 1–3. doi: 10.1016/j.bcp.2017.03.008
Schuetz, A. N. (2019). Emerging agents of gastroenteritis: Aeromonas, Plesiomonas, and the diarrheagenic pathotypes of Escherichia coli. Semin. Diagn. Pathol. doi: 10.1053/j.semdp.2019.04.012
Silva, L.C.A.D, Leal-Balbino, T.C., Melo, B.S.T. De, Mendes-Marques, C.L., Rezende, A.M., Almeida, A.M.P. De, et al. (2017). Genetic diversity and virulence potential of clinical and environmental Aeromonas spp. isolates from a diarrhea outbreak. BMC Microbiol. 17, 1–9. doi:doi: 10.1186/s12866-017-1089-0
Sinclair, H. A., Heney, C., Sidjabat, H. E., George, N. M., Bergh, H., Anuj, S. N., et al. (2016). Genotypic and phenotypic identification of Aeromonas species and CphA-mediated carbapenem resistance in Queensland, Australia. Diagn. Microbiol. Infect. Dis. 85, 98–101. doi: 10.1016/j.diagmicrobio.2016.02.005
Søgaard, M., Andersen, J. P., and Schønheyder, H. C. (2012). Searching PubMed for studies on bacteremia, bloodstream infection, septicemia, or whatever the best term is: a note of caution. Am. J. Infect. Control 40, 237–240. doi: 10.1016/j.ajic.2011.03.011
Soltan Dallal, M. M., Mazaheri Nezhad Fard, R., Kavan Talkhabi, M., Aghaiyan, L., and Salehipour, Z. (2016). Prevalence, virulence and antimicrobial resistance patterns of Aeromonas spp. isolated from children with diarrhea. Germs 6, 91–96. doi: 10.11599/germs.2016.1094
Song, P., Deng, J., Hou, T., Fu, X., Zhang, L., Sun, L., et al. (2019). Aeromonas sobria peritonitis in a peritoneal dialysis (pd) patient: a case report and review of the literature. BMC Nephrol. 20:180. doi: 10.1186/s12882-019-1361-7
Spadaro, S., Berselli, A., Marangoni, E., Romanello, A., Colamussi, M. V., Ragazzi, R., et al. (2014). Aeromonas sobria necrotizing fasciitis and sepsis in an immunocompromised patient: a case report and review of the literature. J. Med. Case Rep. 8:315. doi: 10.1186/1752-1947-8-315
Stano, F., Brindicci, G., Monno, R., Rizzo, C., Ghezzani, F., Carbonara, S., et al. (2009). Aeromonas sobria sepsis complicated by rhabdomyolysis in an HIV-positive patient: case report and evaluation of traits associated with bacterial virulence. Int. J. Infect. Dis. 13, 113–118. doi: 10.1016/j.ijid.2008.08.003
Stevens, D. L., Bryant, A. E., and Goldstein, E. J. (2021). Necrotizing soft tissue infections. Infect. Dis. Clin. N. Am. 35, 135–155. doi: 10.1016/j.idc.2020.10.004
Stratev, D., and Odeyemi, O. A. (2016). Antimicrobial resistance of Aeromonas hydrophila isolated from different food sources: a mini-review. J. Infect. Public Health 9, 535–544. doi: 10.1016/j.jiph.2015.10.006
Strauss, E., and Caly, W. R. (2006). Spontaneous bacterial peritonitis: a therapeutic update. Expert Rev. Anti-Infect. Ther. 4, 249–260. doi: 10.1586/14787210.4.2.249
Sulzer, J. K., and Ocuin, L. M. (2019). Cholangitis: causes, diagnosis, and management. Surg. Clin. North Am. 99, 175–184. doi: 10.1016/j.suc.2018.11.002
Sweeney, T. E., Liesenfeld, O., and May, L. (2019). Diagnosis of bacterial sepsis: why are tests for bacteremia not sufficient? Expert. Rev. Mol. Diagn. 19, 959–962. doi: 10.1080/14737159.2019.1660644
Teunis, P., and Figueras, M. J. (2016). Reassessment of the enteropathogenicity of mesophilic Aeromonas species. Front. Microbiol. 7:1395. doi: 10.3389/fmicb.2016.01395
Ugarte-Torres, A., Perry, S., Franko, A., and Church, D. L. (2018). Multidrug-resistant Aeromonas hydrophila causing fatal bilateral necrotizing fasciitis in an immunocompromised patient: a case report. J. Med. Case Rep. 12:326. doi: 10.1186/s13256-018-1854-1
Van Zwetselaar, M., Nyombi, B., Sonda, T., Kumburu, H., Chamba, N., Dekker, M. C. J., et al. (2018). Aeromonas caviae mimicking vibrio cholerae infectious enteropathy in a cholera-endemic region with possible public health consequences: two case reports. J. Med. Case Rep. 12, 1–6. doi: 10.1186/s13256-018-1603-5
Varela, A. R., Nunes, O. C., and Manaia, C. M. (2016). Quinolone resistant Aeromonas spp. as carriers and potential tracers of acquired antibiotic resistance in hospital and municipal wastewater. Sci. Total Environ. 542, 665–671. doi: 10.1016/j.scitotenv.2015.10.124
Vasagar, B., Jain, V., Germinario, A., Watson, H. J., Ouzts, M., Presutti, R. J., et al. (2018). Approach to aquatic skin infections. Prim. Care 45, 555–566. doi: 10.1016/j.pop.2018.05.010
Voss, L. M., Rhodes, K. H., and Johnson, K. A. (1992). Musculoskeletal and soft tissue Aeromonas infection: an environmental disease. Mayo Clin. Proc. 67, 422–427. doi: 10.1016/S0025-6196(12)60387-5
Wu, C. J., Lee, H. C., Chang, T. T., Chen, C. Y., Lee, N. Y., Chang, C. M., et al. (2009). Aeromonas spontaneous bacterial peritonitis: a highly fatal infectious disease in patients with advanced liver cirrhosis. J. Formos. Med. Assoc. 108, 293–300. doi: 10.1016/S0929-6646(09)60069-3
Yáñez, M. A., Catalán, V., Apráiz, D., Figueras, M. J., and Martínez-Murcia, A. J. (2003). Phylogenetic analysis of members of the genus Aeromonas based on gyrB gene sequences. Int. J. Syst. Evol. Microbiol. 53, 875–883. doi: 10.1099/ijs.0.02443-0
Yang, C. C., Sun, I. F., Liu, C. M., and Lai, C. S. (2004). Aeromonas hydrophila septicemia in acute hand injury: a case report. Kaohsiung J. Med. Sci. 20, 351–356. doi: 10.1016/S1607-551X(09)70170-6
Zheng, D., Yin, G., Liu, M., Chen, C., Jiang, Y., Hou, L., et al. (2021). Science of the total environment a systematic review of antibiotics and antibiotic resistance genes in estuarine and coastal environments. Sci. Total Environ. 777:146009. doi: 10.1016/j.scitotenv.2021.146009
Zhou, Q. L., Wang, Y. J., Xie, J., Ge, X. P., Xi, B. W., and Liu, B. (2013). Distribution and virulence gene comparison of Aeromonas strains isolated from diseased fish and water environment. Pol. J. Microbiol. 62, 299–302. doi: 10.33073/pjm-2013-039
Zhou, Y., Yu, L., Nan, Z., Zhang, P., Kan, B., Yan, D., et al. (2019). Taxonomy, virulence genes and antimicrobial resistance of Aeromonas isolated from extra-intestinal and intestinal infections. BMC Infect. Dis. 19, 1–9. doi: 10.1186/s12879-019-3766-0
Zhu, H., Chen, Y., Hang, Y., Luo, H., Fang, X., Xiao, Y., et al. (2021). Impact of inappropriate empirical antibiotic treatment on clinical outcomes of urinary tract infections caused by Escherichia coli: a retrospective cohort study. J. Glob. Antimicrob. Resist. 26, 148–153. doi: 10.1016/j.jgar.2021.05.016
Keywords: microbiology, bacterial infection, human pathogen, prognosis, antibiotic responses
Citation: Pessoa RBG, Oliveira WF, Correia MTS, Fontes A and Coelho LCBB (2022) Aeromonas and Human Health Disorders: Clinical Approaches. Front. Microbiol. 13:868890. doi: 10.3389/fmicb.2022.868890
Edited by:
Dongsheng Zhou, Beijing Institute of Microbiology and Epidemiology, ChinaReviewed by:
Jose Ramos-Vivas, Universidad Europea del Atlántico, SpainMichael P. Ryan, University of Limerick, Ireland
Po Lin Chen, National Cheng Kung University, Taiwan
Copyright © 2022 Pessoa, Oliveira, Correia, Fontes and Coelho. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luana Cassandra Breitenbach Barroso Coelho, bGNiYmNvZWxob0BnbWFpbC5jb20=