 Hugo Peslier
Hugo Peslier
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med. , 17 March 2025
Sec. Nuclear Medicine
Volume 12 - 2025 | https://doi.org/10.3389/fmed.2025.1538507
This article is part of the Research Topic Innovative Approaches in Precision Radiation Oncology View all 4 articles
Introduction: Metastatic castration-resistant prostate cancer (mCRPC) is an aggressive disease with a poor prognosis and few therapeutic options. In recent years, 177Lu-PSMA, a novel radioligand therapy, has shown promising results in patients who have failed conventional therapies. However, around 30% of patients do not respond adequately to this treatment. In this retrospective cohort study, we examined clinical, biological, and 68Ga-PSMA PET/CT-derived factors associated with poor treatment response.
Materials and methods: We conducted a retrospective cohort study including 63 patients treated at ICO Angers for progressive mCRPC following Novel Hormonal Agents and taxane-based chemotherapy. The primary endpoint was early treatment discontinuation, defined as stopping therapy at or before the 4th cycle. Secondary endpoints included PSA response and overall survival.
Results: A total of 63 patients were included in the study. Factors associated with early treatment discontinuation included a BMI < 25 kg/m2, PSA doubling time < 2 months, hemoglobin levels <10 g/dL, albumin levels <35 g/L, lactate dehydrogenase (LDH) levels >250 IU/L and alkaline phosphatase (ALP) levels >125 IU/L. On 68Ga-PSMA PET/CT imaging, low SULmax, high Total Tumor Volume, and a low PSG score were also linked to early treatment discontinuation.
Conclusion: This study identified several clinical, biological, and 68Ga-PSMA PET/CT-derived factors associated with early treatment discontinuation. Patients with poor overall health, aggressive or extensive disease, or low PSMA expression are at higher risk of treatment failure.
According to the Global Cancer Observatory, prostate cancer is the second most common cancer and the fifth leading cause of cancer-related deaths in men worldwide in 2020, with an incidence rate of 30.7 per 100,000 and a mortality rate of 7.7 per 100,000 (1).
In France, according to 2018 data from INCA (Institut National du Cancer), prostate cancer is the most common cancer and the third leading cause of cancer-related deaths in men. The median age at diagnosis is 69 years. It is a condition with a favorable prognosis, with a 5-year survival rate of 93%. Indeed, 80% of cases are diagnosed at a localized stage, and the stage of the disease at diagnosis is a major prognostic factor (2). Notably, the 5-year survival rate of de novo metastatic prostate cancer is around 30% (3).
In the natural evolution of untreated prostate cancer, initial localized disease slowly progresses to locoregional involvement, and subsequently to a metastatic stage with bone, lymph node or visceral metastases. Following definitive local therapy for localized forms through radical prostatectomy or external beam radiotherapy, recurrence is observed in 27–53% of patients (4).
At the metastatic castration-resistant stage defined by biochemical or radiological disease progression in an environment with very low serum testosterone concentration (< 50 ng/dL), prostate cancer is characterized by a poor prognosis and the available therapeutic options are currently limited to anti-hormonal deprivation therapy (ADT) in combination with novel hormonal agents (NHA) (e.g., enzalutamide, abiraterone) or taxane-based chemotherapies (e.g., docetaxel and cabazitaxel). For patients with metastatic castration-resistant prostate cancer (mCRPC) with alteration in BRCA 1 or 2, Olaparib can be considered after NHA (5).
For several decades, extensive research has sought to identify cellular targets for the development of novel targeted therapies in prostate cancer. In 1987, Horoszewicz et al. first described Prostate-Specific Membrane Antigen (PSMA) (6). This is a type II transmembrane protein involved in tumor proliferation and neoangiogenesis through the metabolism of glutamate and folates. PSMA is overexpressed in most prostate cancers, approximately 1,000 times more than in normal prostatic tissue, but is also physiologically expressed in various other tissues, particularly the salivary glands. Importantly, PSMA is not exclusive to prostate cancer; it is also present on endothelial cells of neovessels in other tumors, including colon adenocarcinoma, renal cell carcinoma, lung cancer, and melanoma. Studies have shown that PSMA expression correlates with tumor grade and the presence of metastatic disease, with higher levels associated with poorer prognosis.
In the field of nuclear medicine, several synthetic ligands of PSMA have been developed with the aim of creating radiopharmaceutical drugs both for imaging and therapy (7, 8). This refers to the concept of theranostics, a term derived from the combination of ‘therapy’ and ‘diagnostics.’ Theranostics involves using the same specific ligand for a cellular target, initially labeled with an isotope dedicated to imaging (e.g., 99mTc for SPECT imaging, or 68Ga and 18F for PET/CT imaging). In a subsequent step, the ligand is combined with an alpha or beta- emitting radioisotope capable of destroying the previously targeted tumor cells (for exemple 177Lu wich is a beta- emitter, or 225Ac wich is an alpha emitter) (9).
Among the radioisotopes suitable for therapy, 177Lu is a beta-emitting radionuclide with a half-life of 6.65 days, a maximum β- particle energy of 497 keV and a maximum tissue penetration of 1.8 mm. This makes it particularly suitable for targeted treatment of prostate cancer tumors and their microenvironment, minimizing damage to surrounding healthy tissue. Gamma emission with 113 and 208 keV photons allows for whole-body scintigraphy after each treatment cycle to verify the proper uptake of the radiopharmaceutical drug to all tumor targets, ensure the absence of extravasation and to perform personalized dosimetry. Comparison of each post-therapy scintigraphy also allows tracking treatment efficacy and detecting any potential disease progression that would necessitate modification of the therapeutic approach (10, 11).
The international open-labeled phase 3 trial VISION involving 831 patients, investigating the efficacy and safety of 177Lu-PSMA-617 (commercialized under the name PLUVICTO®), has shown significant promise in extending imaging-based progression-free survival (median: 8.7 vs. 3.4 months) and overall survival (median: 15.3 vs. 11.3 months) when administered alongside standard-care therapy in patients with advanced and progressive PSMA-positive mCRPC, 177Lu-PSMA-617 was associated with a low incidence of serious adverse events. In this study, patients were required, among other criteria, to have previously received one NHA, at least one but no more than two taxane regimens, a positive 68Ga-PSMA-11 PET-CET scan, an Eastern Cooperative Oncology Group (ECOG) Performance Status score of 0 through 2, a life expectancy >6 months and an adequate organ function. The positivity criteria for 68Ga-PSMA PET/CT in the VISION study are presented below in Table 1 (12). Based on PSMA PET/CT criteria, patients who were classified as screen failures in the VISION trial had worse short-term outcomes than those who were classified as eligible (13).
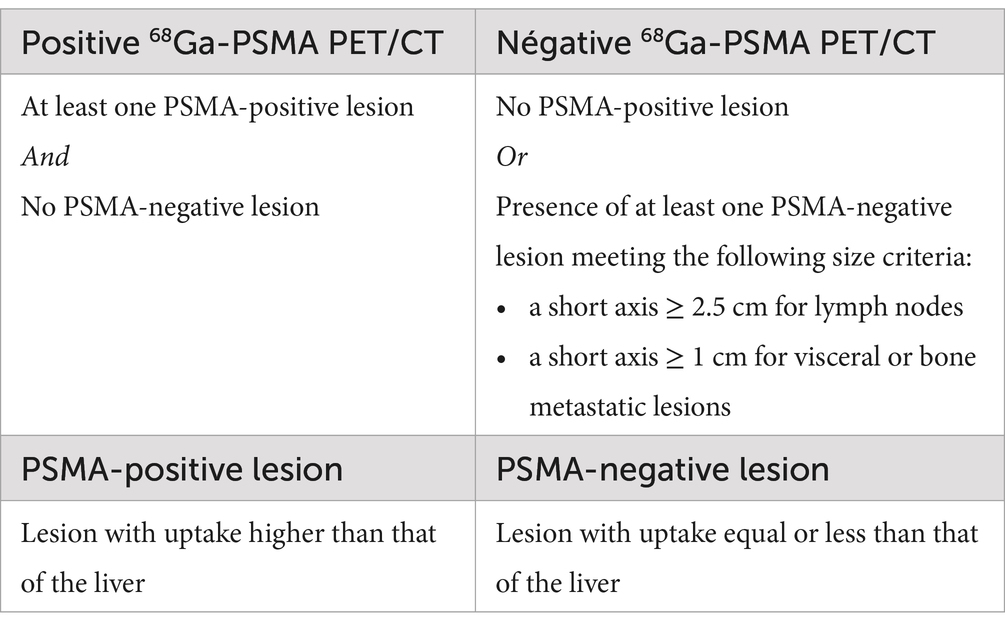
Table 1. Interpretation criteria for 68Ga-PSMA PET in the VISION study.
In France, PLUVICTO® was first used in 2021 under a Temporary Authorization for Use. Since May 2023, it has been granted Marketing Authorization and is now routinely available for the treatment of adult patients with mCRPC who have progressive disease and are positive for PSMA, and who have been treated with androgen pathway inhibitor hormone therapy and taxane-based chemotherapy (14).
The initiation of treatment with PLUVICTO® is complex and requires the expertise of a nuclear medicine physician in collaboration with an oncologist. Joint recommendations have been issued by the European Association of Nuclear Medicine (EANM) and the Society of Nuclear Medicine and Molecular Imaging (SNMMI) (15).
Before starting treatment, several eligibility criteria must be confirmed. In a theranostic approach, a PET scan with 68Ga-PSMA is required to identify PSMA-positive tumor targets and ensure there are no PSMA-negative lesions meeting the specified size criteria. Additionally, a standard biological assessment including a complete blood count, liver function tests and renal function tests must be conducted to rule out contraindications such as cytopenias or severe renal or hepatic insufficiency. A thorough evaluation of the patient’s general health and comorbidities should be performed on a case-by-case basis during a pre-treatment consultation. Relative contraindications established by nuclear medicine societies include: a life expectancy of less than 3 months, an ECOG Performance Status of ≥3, uncontrollable urinary incontinence, acute urinary obstruction, severe comorbidities (e.g., psychiatric or cardiovascular conditions affecting hydration), severe renal or hepatic insufficiency (GFR < 30 mL/min, creatinine > twice the upper limit of normal, liver enzymes > five times the upper limit of normal), active infection, and significant cytopenias (WBC < 2.5 G/L, ANC < 1.5 G/L PLT < 75 G/L).
The standard treatment regimen consists of 6 cycles administered every 6 weeks, each involving an intravenous injection of 7.4 GBq of 177Lu-PSMA-617. Due to the co-emission of a 208 keV gamma ray by 177Lu, a whole-body scan is performed within 48 h after each injection to confirm proper radiopharmaceutical binding to tumor targets, check for tumor progression that might impact treatment continuation and ensure there is no extravasation at the injection site or contamination.
During and after PLUVICTO® administration, radioprotection measures must be implemented to prevent radioactive waste from contaminating the environment and to protect both healthcare staff and the patient’s close contacts. Specifically, patients should be hospitalized for 6 to 24 h to collect their urine in decay containers. Radioprotection guidelines for home care can be adjusted based on dose rate measurements taken at the end of hospitalization.
Ongoing clinical and biological monitoring is essential during treatment, including assessing general health, screening for hematological and non-hematological toxicities and tracking PSA levels with tests conducted every 3 weeks. In cases of severe toxicity, adjustments to the dose, delays or discontinuation of treatment may be considered on an individual basis. Efficacy should be evaluated with Computed Tomography (CT) scans and bone scintigraphy every 12 weeks and at the end of the 6 treatment cycles. Indeed, as per the 2024 EAU – EANM – ESTRO – ESUR – SIOG Guidelines on Prostate Cancer, 68Ga-PSMA PET/CT is not yet recommended as imaging modality for therapeutic assessment in clinical practice. The treatment regimen for 177Lu-PSMA administered at ICO Angers is presented below in Figure 1.
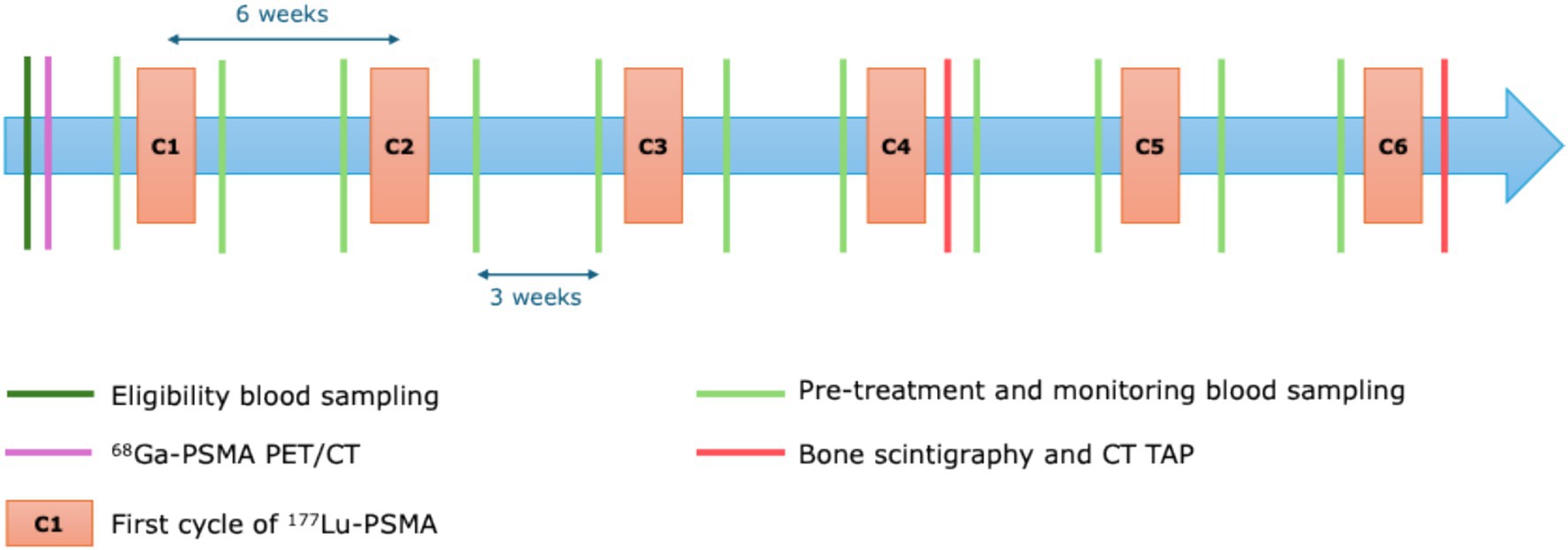
Figure 1. 177Lu-PSMA treatment regimen and monitoring at ICO Angers.
Despite initial patient selection based on VISION study criteria, several retrospective studies indicate that approximately 30% of patients treated with 177Lu-PSMA-617 do not respond favorably (PSA decline <50% during treatment), and there is limited knowledge regarding predictive factors for treatment success (16).
To prevent administering a complex, costly, and potentially side-effect-laden treatment to patients who are unlikely to benefit, it is crucial to identify the patient groups most likely to respond to 177Lu-PSMA therapy. The aim of this study was to pinpoint clinical, biological and nuclear-imaging parameters in the pretherapeutic phase that are associated with a poor response to treatment.
We conducted a single-center, retrospective cohort including all consecutive patients treated at ICO Angers for mCRPC who received at least one cycle of 177Lu-PSMA between February 2022 and December 2023.
Inclusion criteria encompassed the presence of mCRPC, progression following at least one line of taxane chemotherapy and second-generation hormone therapy, and a positive 68Ga-PSMA PET/CT scan according to the VISION study criteria mentioned above.
Exclusion criteria included severe cytopenias and severe renal or hepatic insufficiency, as outlined in the PLUVICTO® product’s Summary of Product Characteristics. Additionally, patients involved in clinical research protocols receiving experimental treatments during the 177Lu-PSMA therapy period, and those who did not consent to the use of their health data for research purposes, were also excluded.
The following data were collected from the patient’s electronic medical records: characteristics related to the initial disease and previously received treatments, clinical and biological characteristics at the start of 177Lu-PSMA treatment, and characteristics of the 68Ga-PSMA PET/CT scan before the first treatment cycle (C1).
Each treatment decision was made during a multidisciplinary tumor board meeting including oncologists and nuclear medicine physicians. During a pre-therapeutic consultation, patients were informed about the treatment modalities, expected benefits, and potential adverse effects. Written consent was systematically obtained. A consent form for the use of health data for research purposes was provided and completed by each patient who started treatment during the inclusion period. The study protocol was previously approved by an independent ethics committee.
68Ga-PSMA PET/CT scans were performed in accordance with the 2017 European Association of Nuclear Medicine and Society of Nuclear Medicine and Molecular Imaging (EANM and SNMMI) standard recommendations. The first 15 patients underwent their scans at the ICO site in Nantes: 7 on a 2019 Siemens Biograph Vision PET scanner and 8 on a 2020 Siemens Biograph Vision PET scanner. 1 patient had his scan at the Institut Gustave Roussy in Paris on a Siemens Biograph Vision 600 PET scanner, and 47 patients underwent their scans at ICO Angers: 24 on a Philips VEREOS PET scanner and 23 on a GE Discovery IQ PET scanner.
Each scan was interpreted by an experienced nuclear medicine physician on a Syngo.via platform (Siemens Healthineers, Erlangen, Germany), including both visual and quantitative analyses. Lesions were considered PSMA-positive if their uptake intensity was equal to or greater than that of healthy liver tissue.
Measurements of Maximum Standardized Uptake Value – Lean body mass (SULmax) and Total Tumor Volume (TTV) were performed using the automatic segmentation module of the Syngo.via software, which allowed for automatic segmentation of all PSMA-positive lesions with a segmentation threshold of 41% of each lesion’s SULmax (this threshold is the commonly used in the literature for lesion segmentation on PET images). To quantify the uptake of tumor lesions, we chose to use SULmax, a semi-quantitative index that accounts for lean body mass, as opposed to SUVmax which is based on the total body weight. Indeed, due to significant differences in body morphotypes within the study population, the use of SULmax allows for better interindividual comparability.
Patients were categorized into three groups based on the tracer uptake pattern for the definition of the PSG (PET Tumor-to-Salivary Gland) score, based on a visual analysis of the Maximum Intensity Projection image: patients whose more than 80% of lesions had higher uptake than the salivary glands were classified in the ‘High’ group; patients whose more than 80% of lesions had lower uptake than the salivary glands were classified in the ‘Low’ group; the remaining patients who did not fit into the first two categories were classified in the ‘Intermediate’ group. In an international multicenter retrospective study including 237 men, Hotta et al. demonstrated that this new visual score is predictive of the response to 177Lu-PSMA treatment with better PSA reduction and longer overall survival for ‘High’ scores, and with a substantial interreader reproducibility (17).
The 177Lu-PSMA treatment protocol consisted of administering 6 cycles of 7,4 GBq, each spaced 6 weeks apart, in the context of day hospitalization. At the end of each cycle, whole-body scintigraphy was performed to verify the proper distribution of the radiopharmaceutical to the tumor targets, the absence of extravasation at the injection site or contamination, and the absence of new uptake sites that could suggest disease progression during treatment.
Regular clinical and biological monitoring was established, with laboratory tests performed within 7 days before each cycle and 3 weeks after each treatment cycle. These tests included PSA level measurement to track changes, complete blood counts, comprehensive liver and kidney function tests, and albumin levels to ensure the treatment’s tolerability. Each patient was regularly consulted by both their treating oncologist and the nuclear medicine physician overseeing the treatment. In cases of severe adverse effects, such as cytopenias detected during monitoring, decisions regarding the spacing, postponement or permanent discontinuation of treatment cycles were made on a case-by-case basis by the multidisciplinary medical team.
At the end of the fourth cycle (C4) and the sixth cycle (C6), bone scintigraphy and CT scans of the thorax, abdomen, and pelvis (TAP) were performed to evaluate therapeutic efficacy. An earlier interim evaluation could be requested in case of suspected disease progression during treatment, before C4 or C6.
The primary endpoint was poor response to 177Lu-PSMA, defined by early discontinuation of treatment between the first dose and post-C4 therapeutic assessment for any reason (e.g., progression objectively confirmed by CT or bone scan, or early treatment interruption due to severe hematological toxicity or deterioration in general condition, where continuing treatment was considered unreasonable). Secondary endpoints included a lack of treatment response as measured by PSA levels and the description of overall survival in treated patients. The lack of response based on PSA levels was defined as the proportion of patients who did not achieve a reduction of more than 50% from their baseline PSA level, as measured on the last biological assessment performed prior to C1.
Clinical and biological characteristics, disease extent at the start of 177Lu-PSMA treatment, and prior treatments received are described for all patients included in this study, based on the nature of the variable studied, with the number of missing data presented where applicable. Quantitative or discrete data are summarized with median, 25th-75th percentiles, minimum, maximum, mean and standard deviation. Categorical and binary data are described by the number and percentage of data points for each modality.
To study the factors associated with early treatment discontinuation (primary endpoint), we distinguish between two groups of patients: those who were unable to receive more than 4 cycles and those who received 5 or 6 cycles of 177Lu-PSMA. We compare characteristics related to initial disease and prior treatments, clinical characteristics at the start of 177Lu-PSMA treatment and PET characteristics using 68Ga-PSMA before the initiation of 177Lu-PSMA treatment between these two groups using logistic regression models.
To investigate factors associated with progression or disease-related death, we used a semi-parametric Cox proportional hazards model to estimate the hazard ratios and associated p-values. In this model, time corresponds to the treatment regimen (C1 to C6). The event of interest is disease progression or death related to cancer. Patients who complete all 6 cycles without progression are censored at C6. Patients who discontinue treatment before C6 without progression and without disease-related death are censored at the date of their last received cycle. Risk estimation and its 95% confidence interval are performed using the Kaplan–Meier method.
All baseline variables are analyzed univariately first, and variables associated with survival with a p-value <0.2 are eligible for inclusion in the multivariate model. In cases of high correlation between two variables, the one most significantly associated with survival is preferred. Essential clinical characteristics for interpreting the multivariate analysis are also included in the model, regardless of their univariate significance.
For factors related to receiving 4 or fewer cycles, logistic regression models are employed. For factors associated with progression or disease-related death, Cox proportional hazards models are used.
Characteristics of patients who experience a reduction in PSA levels of more than 50% after the start of treatment (compared to before treatment) are compared using logistic regression models. Individual PSA trajectories are graphically represented.
Analyses are conducted under the responsibility of the Clinical Research Department of ICO, Promotion Unit, using appropriate statistical software (R or SAS). No imputation of missing data is planned in the protocol. A p-value <0.05 is considered statistically significant. In this exploratory study, no correction for alpha inflation is planned.
In this retrospective study, 63 patients were enrolled between February 2022 and December 2023. The average age at initial diagnosis was 62.2 ± 8.2 years and the average age at C1 was 71.8 ± 8.0 years.
At the time of diagnosis, 37 patients (58.7%) had metastatic disease, 16 patients (25.4%) had locally advanced disease and 10 patients (15.9%) had localized disease. A total of 34 patients (54%) had an ISUP (International Society of Urological Pathology) score of 4 or higher while 29 patients (46%) had an ISUP score below 4.
Before starting treatment, 56 patients (88.9%) had bone metastases, 35 patients (55.6%) had lymph node involvement, and 3 patients (7.9%) had visceral metastases (affecting the liver, lungs or brain). Of the group, 35 patients (55.6%) had received one line of NHA, 26 patients (41.3%) had received two lines, and 2 patients (3.2%) had received three lines. Additionally, 26 patients (41.3%) had undergone one line of taxane chemotherapy (Docetaxel only) while 37 patients (58.7%) had received two lines (Docetaxel followed by Cabazitaxel). The median initial PSA level was 67.7 ng/mL (95% CI: [19.8; 257.7]) and the median PSA doubling time before C1 was 2.2 months (95% CI: [1.4; 3.8]). On 68Ga-PSMA PET/CT scans, the median SULmax was 23.7 (95% CI: [18.5; 53.1]) and the median TTV was 82.2 mL (95% CI: [18.0; 251.8]). Among these patients, 18 (28.6%) had a high PSG score, 26 (41.3%) had an intermediate PSG score and 19 (30.2%) had a low PSG score.
The average time from initial diagnosis to the start of the first treatment cycle was 8.3 ± 5.8 years. The average time between the 68Ga-PSMA PET/CT scan and the first treatment cycle was 1 ± 0.6 months. Resumed characteristics of the study population are presented in Table 2 and Supplementary Material.
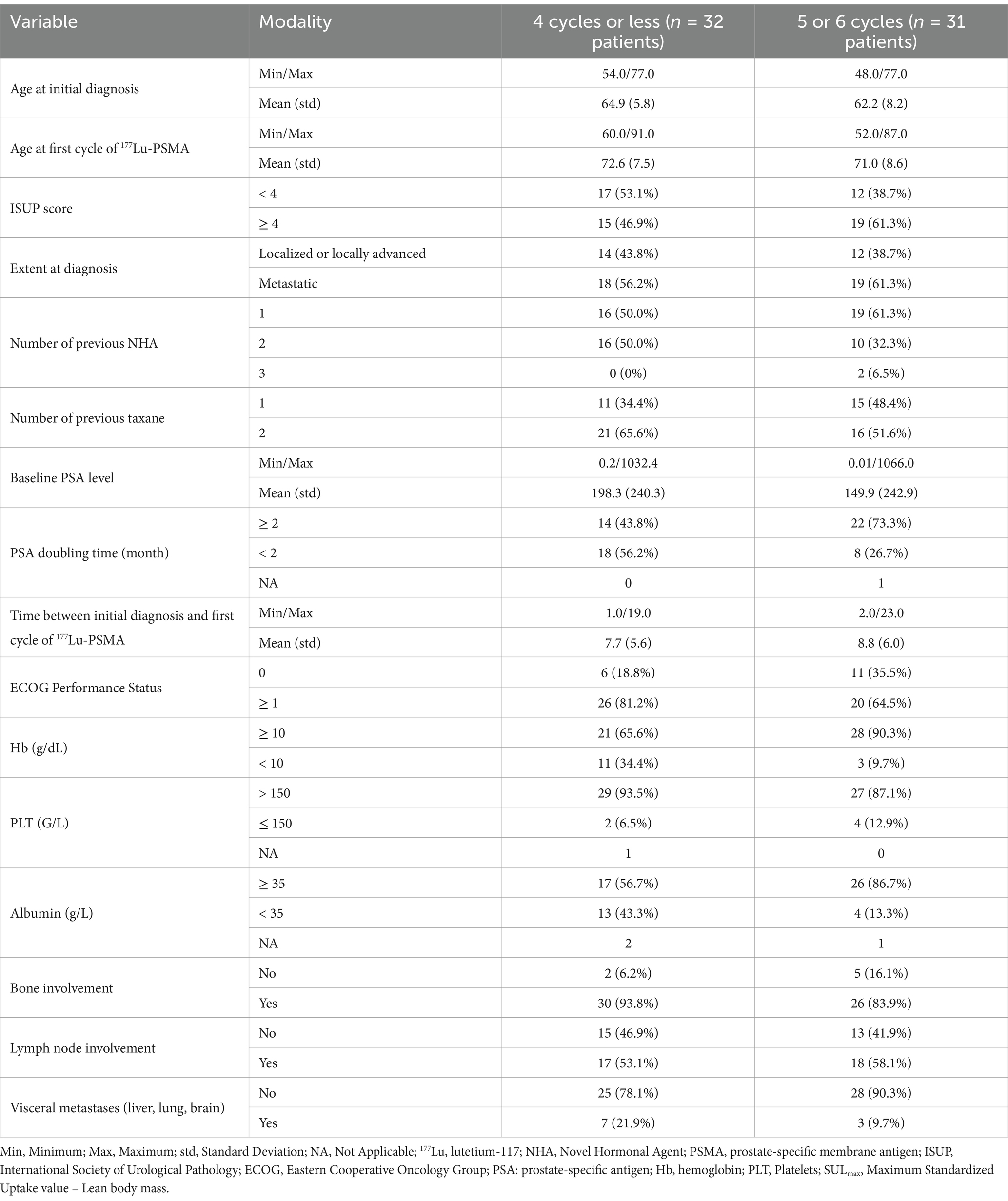
Table 2. Resumed characteristics of the study population.
By the end of the study period, patients had received a median of 4 cycles of 177Lu-PSMA therapy. Of these, 32 patients (50.7%) received between 1 and 4 cycles and 31 patients (49.2%) received 5 or 6 cycles. Among those who received one to four cycles, 26 discontinued treatment due to disease progression (objectively confirmed by imaging: CT or bone scan), while 6 stopped for other reasons: 3 due to hematotoxicity, 1 due to death related to heart failure, 1 due to severe hyponatremia and 1 patient who opted to discontinue despite a favorable therapeutic response.
Among patients who received five or six cycles, 4 (6.3%) experienced disease progression (objectively confirmed by imaging) and 4 were awaiting their C6. Overall, 38 patients (60.3%) saw a reduction in PSA levels of 50% or more during treatment.
In univariate analysis, the factors associated with early treatment discontinuation (four cycles or fewer) were as follows: a BMI < 25 vs. ≥ 25 kg/m2 (OR: 3.85; 95% CI [1.30–11.11]; p = 0.0148), a PSA doubling time < 2 months vs. ≥ 2 months (OR: 3.57; 95% CI [1.22–10.00]; p = 0.0206), hemoglobin <10 g/dL vs. ≥ 10 g/dL (OR: 4.89; 95% CI [1.21–19.75]; p = 0.0259), albumin <35 g/L vs. ≥ 35 g/L (OR: 4.97; 95% CI [1.39–17.82]; p = 0.0138), LDH > 250 IU/L vs. ≤ 250 IU/L (OR: 5.96; 95% CI [1.99–17.86]; p = 0.0014), and ALP > 125 IU/L vs. ≤ 125 IU/L (OR: 4.07; 95% CI [1.42–11.7]; p = 0.0091). On 68Ga-PSMA PET/CT, a lower SULmax (per unit decrease: OR: 1.02; 95% CI [1.00–1.04]; p = 0.0361), a higher TTV compared to the median (OR: 4.62; 95% CI [1.60–13.35]; p = 0.0047) and a low vs. high PSG score (OR: 5.63; 95% CI [1.37–23.17]; p = 0.0166) were also associated with early treatment discontinuation. In multivariate analysis, BMI, PSA doubling time, PSG score, and TTV remained significantly associated with early treatment discontinuation.
The results of the statistical analyses are presented below in Tables 3, 4.
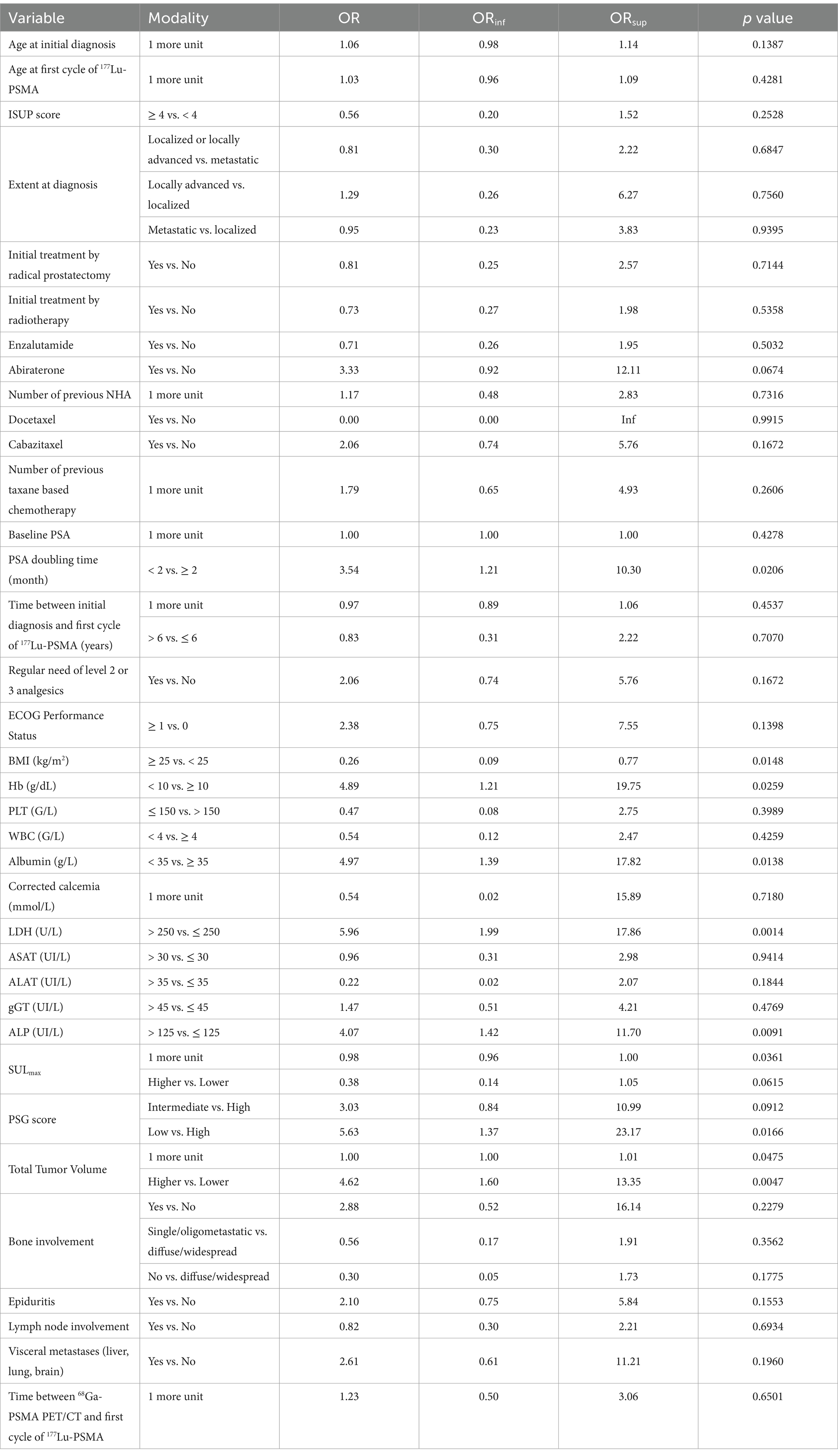
Table 3. Risk of early treatment discontinuation – univariate analysis.
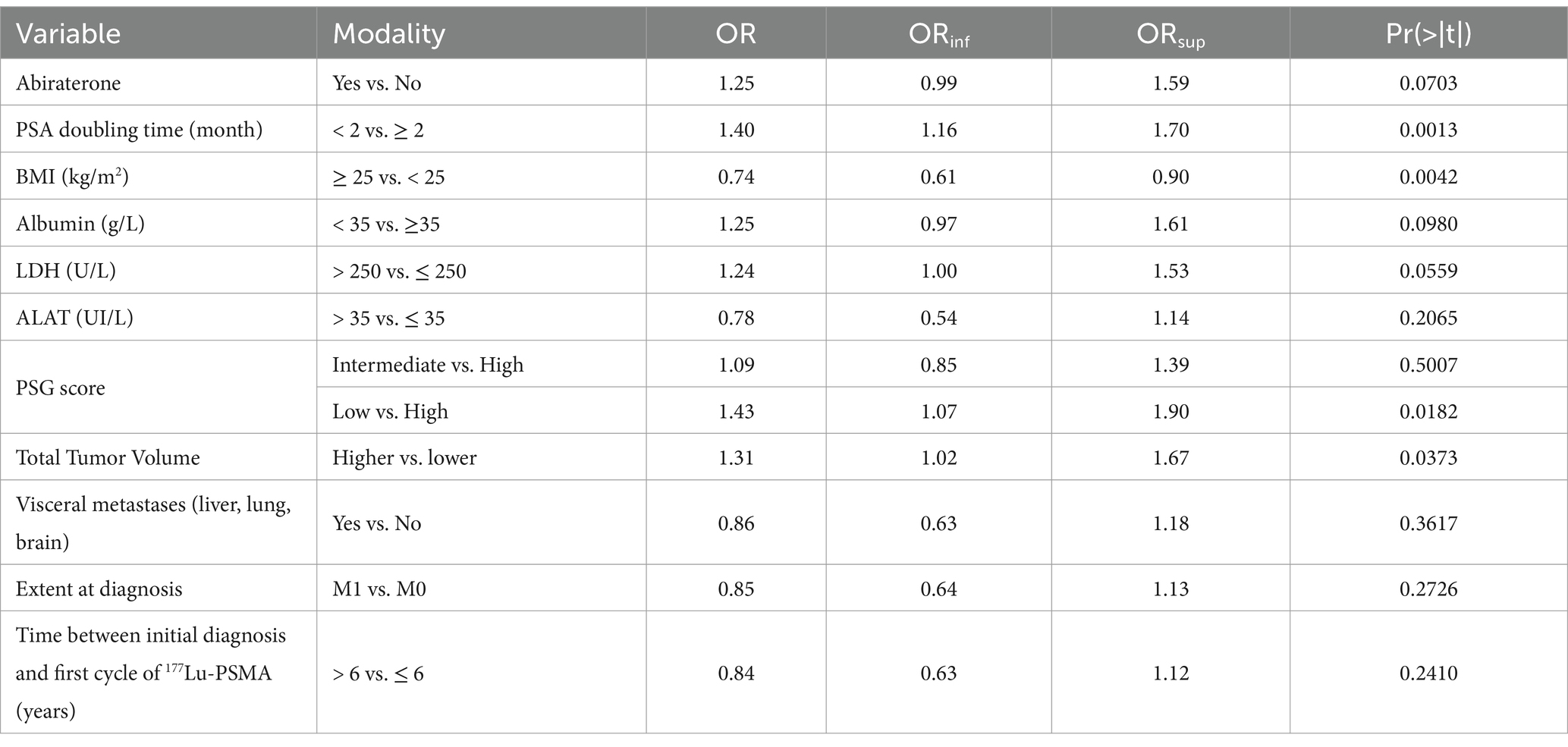
Table 4. Risk of early treatment discontinuation – multivariate analysis.
Additionally, aside from the PSG score, all these factors are significantly associated with disease progression and prostate cancer-specific mortality. This includes the presence of widespread bone involvement (HR: 2.34; 95% CI [1.14–4.78]; p = 0.0198) and pulmonary metastases (HR: 2.63; 95% CI [1.00–6.89]; p = 0.0493). In the multivariate analysis, BMI, PSA doubling time, albumin levels and TTV remain significant predictors. However, metastatic status at initial diagnosis (HR: 3.33; 95% CI [1.09–10.00]; p = 0.0357) and ECOG Performance Status ≥1 versus 0 (HR: 3.47; 95% CI [1.25–9.68]; p = 0.0173) also emerge as significant.
Detailed results are presented in the Appendix Tables 1, 2.
In univariate analysis, the clinico-biological factors associated with a reduction in PSA of less than 50% during treatment were as follows: BMI < 25 vs. ≥ 25 kg/m2 (OR: 3.85; 95% CI [1.30–11.11]; p = 0.0148), PSA doubling time < 2 vs. ≥ 2 months (OR: 3.54; 95% CI [1.21–10.30]; p = 0.0206), hemoglobin <10 g/dL vs. ≥ 10 g/dL (OR: 4.89; 95% CI [1.21–19.75]; p = 0.0259), albumin <35 g/L vs. ≥ 35 g/L (OR: 4.97; 95% CI [1.39–17.82]; p = 0.0138), LDH > 250 IU/L vs. ≤ 250 IU/L (OR: 5.96; 95% CI [1.99–17.86]; p = 0.0014), and ALP > 125 IU/L vs. ≤ 125 IU/L (OR: 4.07; 95% CI [1.42–11.7]; p = 0.0091). On 68Ga-PSMA PET/CT, a higher SULmax (per unit increase: OR = 0.98; 95% CI [0.96–1.00]; p = 0.0361), a higher TTV compared to the median (OR: 4.62; 95% CI [1.60–13.35]; p = 0.0047) and a low vs. high PSG score (OR: 5.63; 95% CI [1.37–23.17]; p = 0.0166) were associated with a reduction in PSA of less than 50%.
In multivariate analysis, BMI, PSA doubling time, LDH levels, and PSG score remained significantly associated with PSA response. However, ECOG Performance Status ≥1 vs. 0 (HR: 1.34; 95% CI [1.05–1.71]; p = 0.0246) also became significant.
The PSA level trends and detailed statistical analysis results are presented in Appendix Figure 1 and Appendix Tables 3, 4.
The median follow-up period was 13.7 months (95% CI: 10.5–20.9). A total of 34 deaths were observed in the cohort with a median overall survival of 12.8 months (95% CI: 9.4–18.1). The overall survival of the cohort is depicted in Figure 2.
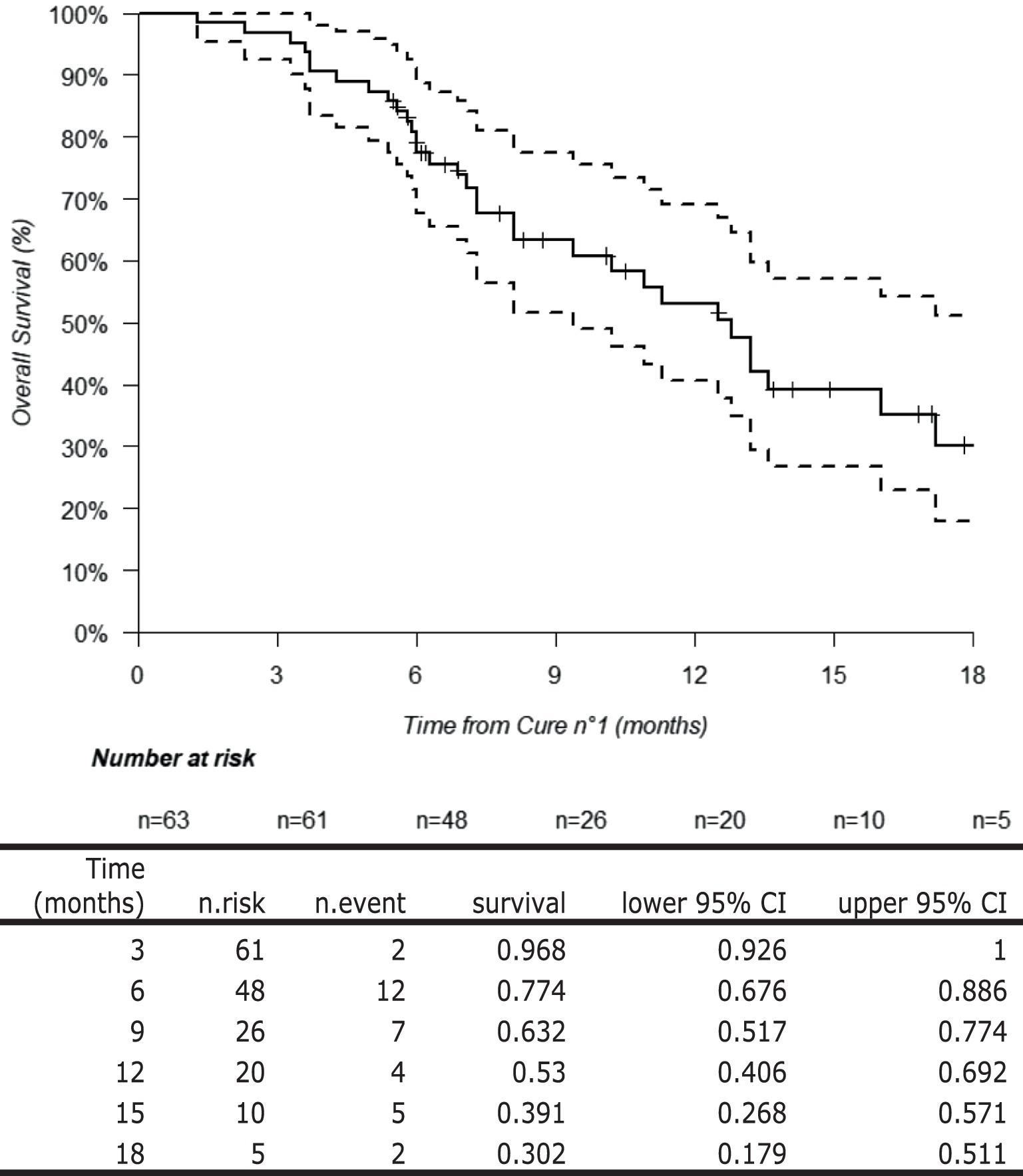
Figure 2. Overall survival of the study population.
In this study, we assessed the impact of various clinico-biological factors and 68Ga-PSMA PET/CT findings on the response to 177Lu-PSMA treatment in patients with metastatic castration-resistant prostate cancer who had progressed after at least one line of taxane chemotherapy and NHA. We categorized the study population into two groups: patients who received 4 cycles or fewer of treatment versus those who received 5 to 6 cycles. We defined the group receiving 4 or fewer cycles as having a poor therapeutic response. This group also included 6 patients who discontinued treatment for reasons other than disease progression, allowing us to account for potential adverse effects of 177Lu-PSMA, comorbidities, and practical management issues.
Our analysis identified several clinico-biological factors associated with an early treatment discontinuation, early progression and low PSA response rate: BMI < 25 kg/m2, short PSA doubling time, decreased hemoglobin and albumin level and increased LDH and ALP levels. While ECOG Performance Status ≥1 does not appear to be a predictor of early treatment discontinuation, it is associated with early progression and a poorer PSA response in multivariate analysis.
A low BMI, low serum albumin, and a high ECOG Performance Status generally reflect a state of malnutrition and are associated with a deterioration of the patient’s overall condition. Cancer-associated malnutrition is known to impair response to chemotherapy (18–20). Based on our findings, we suggest that malnutrition may be linked to a poorer response to 177Lu-PSMA. Further prospective studies are needed to confirm the impact of malnutrition on treatment outcomes with 177Lu-PSMA. Nonetheless, close monitoring of patient’s nutritional status before and during treatment is crucial. In cases of confirmed malnutrition, initiating a re-nutrition strategy could potentially improve therapeutic efficacy and survival.
Interestingly, higher BMI has been linked to better overall survival in cancer patients (21). This finding is paradoxical given that obesity is generally associated with increased all-cause mortality in the general population (22). This discrepancy might be due to one or more confounding factors, as BMI alone is not a reliable indicator of body composition or nutritional status. Body composition can vary widely by age and ethnicity, and individuals with the same BMI can have different distributions of lean and fat mass, which affects prognosis differently (23). For instance, a malnourished individual with sarcopenia but a normal BMI may have a worse prognosis compared to someone with a high BMI but without sarcopenia (24–26). Additionally, our study did not consider recent weight loss before treatment, which could be another confounding factor (27, 28).
While metastatic versus non-metastatic status at initial diagnosis is not a predictor of early treatment discontinuation, it is associated with early progression in multivariate analysis. In a retrospective study, Francini et al. demonstrated improved overall survival in patients with metachronous versus synchronous hormone-sensitive metastatic prostate cancer (29). Similarly, Bajeot et al. reported that synchronous metastatic patients were more symptomatic and had a higher metastatic burden compared to their metachronous counterparts (30). This leads us to hypothesize that the synchronous metastatic patients in our cohort likely had a more aggressive disease, which may have adversely affected their therapeutic response.
PSA doubling time is a dynamic measure of PSA progression and is widely recognized as one of the most reliable biological markers of prostate cancer aggressiveness. In a prospective study of 1,804 men with localized prostate cancer, D’Amico et al. showed that a PSA velocity exceeding 2 ng/mL per year in the year before diagnosis was associated with a tenfold higher risk of prostate cancer-specific mortality compared to those with a PSA velocity of 2 ng/mL per year or less, following radical prostatectomy (31). Likewise, in a retrospective study of 8,669 patients treated with surgery or radiotherapy, D’Amico et al. demonstrated that a PSA doubling time of less than 3 months was linked to significantly shorter prostate cancer-specific survival after biochemical recurrence, with a Hazard Ratio of 19.6 (32). Consistent with our findings, other studies have shown a significant link between PSA doubling time and progression-free survival after 177Lu-PSMA, with a short or negative doubling time predicting poor therapeutic response (33, 34). Based on our results and the existing literature, PSA doubling time also appears to reflect disease aggressiveness in the metastatic castration-resistant stage, with an impact on the response to 177Lu-PSMA. However, the initial PSA level before 177Lu-PSMA treatment does not appear to predict treatment response (35, 36).
In metastatic prostate cancer, elevated LDH levels are linked to shorter overall survival and poorer progression-free survival (PFS) (37). Similarly, in cases of bone metastatic prostate cancer, elevated ALP levels indicate increased osteoblastic activity and greater disease burden (38, 39), with a negative impact on overall survival (40). Other studies have confirmed that an elevation of these two markers is associated with a reduction in PFS after 177Lu-PSMA (34, 36, 41–45). In our cohort, elevation of these two biological markers also predict a poor therapeutic response to 177Lu-PSMA, as they are associated with earlier discontinuation of treatment. Thus, the elevation of these markers may also reflect aggressive metastatic disease.
A decrease in hemoglobin levels is frequently observed in cancer patients and is often due to multiple factors. These can include disease-related issues such as marrow infiltration, nutritional deficiencies, the inflammatory syndrome induced by the disease, or chemotherapy-induced toxicity affecting hematopoietic precursors. Low hemoglobin levels are known to be associated with reduced overall survival and lower treatment efficacy (46, 47). In our study, a hemoglobin level below 10 g/dL was strongly linked to early treatment discontinuation, early disease progression and a poorer PSA response with significant findings across all multivariate analyses. Therefore, investigating and addressing treatable causes of anemia may be beneficial for improving the response to 177Lu-PSMA.
Contrary to several previous reports, we did not find a significant association between regular use of analgesics of levels 2 or 3 and early treatment discontinuation, early progression or PSA response (36, 48).
Lastly, we could not demonstrate a significant association between previous treatments received at the metastatic castration-resistant stage and response to 177Lu-PSMA. However, the recent phase 3 clinical trial PSMAFore demonstrated that 177Lu-PSMA-617 treatment prolonged radiographic PFS versus androgen receptor pathway inhibitor change in taxane-naïve mCRPC patients (49). Moreover, another phase 2 clinical trial, UpFrontPSMA, demonstrated that a sequential treatment including 177Lu-PSMA followed by docetaxel resulted in a better therapeutic response based on PSA reduction compared to docetaxel alone (50). Finally, the TheraP clinical trial, which included 200 patients, found that 177Lu-PSMA was more effective than Cabazitaxel in reducing PSA levels in progressive mCRPC patients eligible for Cabazitaxel. This suggests that earlier use of 177Lu-PSMA before taxane chemotherapy failure may improve therapeutic response (51).
We were also unable to identify a significant link between initial disease characteristics at diagnosis (e.g., initial stage, histopathological grade), disease duration, type of local treatment (if any), and response to 177Lu-PSMA.
In our analysis of 68Ga-PSMA PET/CT, we identified that a low SULmax, a low PSG score, and a high TTV are associated with a poorer therapeutic response.
SULmax measures the maximum activity within the most intense tumor voxel on 68Ga-PSMA PET/CT, adjusted for injected activity and the patient’s lean body mass. This unitless value reflects the tumor’s avidity for the tracer and thus the expression of membranous PSMA. Consequently, a lesion with high uptake of 68Ga-PSMA results in intense binding and a high SULmax. Other related measures include SUVmax, which quantifies the activity of the most intense voxel relative to total body weight, and SUVmean, which measures the average activity within a segmented tumor volume, also relative to total body weight.
Our findings are consistent with those reported by Kuo et al. in their analysis of patients from the VISION study, which showed that high SUVmean is associated with better PFS and overall survival (52). Similarly, Eisazadeh et al. found that a high SULmax /Liver SULmean ratio was associated with longer PFS in patients treated with 177Lu-PSMA I&T (53). Additionally, a prospective study by Emmett et al. which included 14 patients, demonstrated that high SUVmax or SUVmean values correlate with a better PSA response (54).
Our results also confirm the predictive value of the PSG score, as described by Hotta et al., which considers the overall intensity of PSMA expression across all tumor lesions. An uptake higher than that of the salivary glands for most lesions predicts a better response to 177Lu-PSMA. Conversely, an uptake lower than that of the salivary gland and, even more so, lower than that of the liver for most lesions predicts a poor response, with earlier treatment discontinuation and a less favorable PSA response (17). These results suggest that the intensity and homogeneity of lesions are key factors influencing the therapeutic response to 177Lu-PSMA.
Furthermore, a high TTV is a predictive factor for poor response, associated with early treatment discontinuation, early progression and a worse PSA response. This finding corroborates Kuo et al.’s results in their analysis of VISION data (55) and Wang et al.’s findings, which showed an association between high tumor volume and poorer PSA response (56). In line with this, we also observed that diffuse osteomedullary infiltration on 68Ga-PSMA PET/CT is associated with early progression.
In our study population, a low proportion of patients had undergone 18F − FDG PET/CT in addition to 68Ga-PSMA PET/CT before starting PLUVICTO® to detect dedifferentiated tumor lesions. Consequently, we were unable to assess the impact of the presence of FDG-avid and PSMA-low lesions (FDG+/PSMA−) on therapeutic response. Rosar et al. demonstrated in their retrospective study that the FDG SUVmax /PSMA SUVmax ratio calculated across multiple target lesions per patient was predictive of therapeutic response after 2 cycles of 177Lu-PSMA. Specifically, an increase in this ratio (e.g., the presence of FDG+/PSMA− lesions) was associated with a poorer therapeutic response (57).
Several studies have demonstrated the adverse impact of visceral metastases, particularly hepatic involvement, on PFS and overall survival. A meta-analysis involving 1,504 patients indicated that the presence of visceral metastases is linked to both poorer biochemical response and shorter PFS and overall survival (58). We were unable to show this negative association in our cohort, likely due to limited statistical power: only 10 out of 63 patients had visceral involvement, and of these, only 3 received more than four cycles. However, we did find that pulmonary or pleural metastatic involvement was associated with early progression.
The observed overall survival in our study (median: 12.8 months) is lower than that reported in the VISION study (median: 15.3 months). This difference may be due to our more permissive inclusion criteria, which allowed us to include patients who were more severely impaired and had more extensive metastatic involvement. For instance, patients with a Superbonescan were excluded from the VISION study but were included in our cohort. Our study aimed to evaluate factors associated with the response to 177Lu-PSMA in real-world conditions, which naturally differ from those in a clinical trial setting. Moreover, a higher proportion of patients in our cohort received Cabazitaxel (60.3% compared to 41.8% in the VISION study). Indeed, according to the prospective TheraP trial, prior treatment with Cabazitaxel is associated with poorer PFS when followed by 177Lu-PSMA. Additionally, our study had a shorter median follow-up (13.7 months vs. 20.9 months), which could lead to an underestimation of overall survival. However, it is noteworthy that the proportion of patients achieving a PSA reduction of ≥50% during treatment was higher in our study compared to the VISION study (60.3% vs. 46.0%).
Additionally, it is interesting to note that the incidence of progression by C4 or earlier was higher among the initial patients treated in our cohort. This may be due to the overrepresentation of high tumor volumes and low PSG scores among these early patients. These patients also exhibited the most severe clinical and biological impairment. We can hypothesize that the latter patients were better selected, leading to more favorable therapeutic outcomes.
The primary limitations of this study include its retrospective design, which may introduce recall bias, the small sample size that limits statistical power, and its monocentric nature, which could introduce selection bias and center-specific effects. Specifically, this cohort consists of patients treated at a center specialized in cancer care (Centre de Lutte Contre le Cancer - CLCC) with management practices that might differ from those at other hospital settings, including conventional hospitals.
Additionally, we were unable to investigate the impact of molecular biomarkers on treatment response due to their limited use in routine practice. For example, androgen receptor gene amplification, determined through blood sampling, is associated with reduced PFS in several studies (59–61). Moreover, there are rare cases of patients with lesions showing high 68Ga-PSMA avidity and no FDG+/PSMA− lesions, who nevertheless exhibit a poor therapeutic response to 177Lu-PSMA. Some data suggest that genomic alterations such as BRCA2 mutation or neuroendocrine differentiation, could play a key role in treatment resistance (62).
A summarized comparison of our results with those of the previously mentioned studies is available in Appendix Table 5.
Currently, most studies focusing on predictive and prognostic factors associated with response to 177Lu-PSMA have a low level of evidence due to their retrospective design, often monocentric nature, small sample sizes, and highly heterogeneous methodologies. Conducting prospective studies to validate the predictive value of already identified factors would be beneficial. Such studies could facilitate the development of nomograms that could be used in clinical practice to more objectively select patients who are most likely to benefit from treatment. For instance, Gafita et al. developed nomograms to predict response to 177Lu-PSMA. However, this study is limited by its retrospective nature and the small size of the validation cohort (35).
Due to the high cost of treatment, its radiative nature, the complexity of its implementation, and potential adverse effects, patient selection is crucial.
This issue becomes even more significant considering that 177Lu-PSMA could potentially be used at earlier stages of prostate cancer in the future, significantly increasing the number of patients who would require treatment. This raises the important question of how to select between 177Lu-PSMA and other therapies based on the characteristics of the patients and their disease. Several clinical trials are currently investigating the efficacy of 177Lu-PSMA in earlier stages of prostate cancer. For instance, the PSMAfore trial which included 468 patients demonstrated that 177Lu-PSMA is superior to an androgen receptor pathway inhibitor change in taxane-naïve patients with mCRPC (63). Additionally, the ongoing PSMAddition trial is assessing the effectiveness of 177Lu-PSMA combined with standard of care (SoC) versus SoC alone in patients with metastatic hormone-sensitive prostate cancer (64).
Similarly, new radiopharmaceuticals using alpha-emitting isotopes, such as actinium-225 (225Ac − PSMA), have shown promising results in patients who have progressed after 177Lu-PSMA treatment (65).
Our study identifies several predictive factors associated with a poor response to 177Lu-PSMA. Clinico-biologically, these factors include a body mass index (BMI) < 25 kg/m2, a PSA doubling time < 2 months, hemoglobin levels <10 g/dL, albumin levels <35 g/L, LDH > 250 IU/L and ALP > 125 IU/L. These factors are associated with a reduced likelihood of achieving a satisfactory therapeutic response and an increased risk of early treatment discontinuation.
On 68Ga-PSMA PET imaging, poor predictors include a low SULmax, high tumor volume (TTV) and a low PSG score.
The study’s findings underscore the importance of integrating clinico-biological parameters and advanced imaging results in the patient selection process for 177Lu-PSMA therapy. These predictive factors can aid in identifying patients who are less likely to benefit from the treatment, thereby optimizing patient management and potentially guiding the use of alternative or additional therapeutic strategies.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Comité d’Ethique - CHU Angers - 4, rue Larrey - 49933 Angers Cedex 9; comite-ethique@chu-angers.fr. The studies were conducted in accordance with the local legislation and institutional requirements. A consent form for the use of health data for research purposes was provided and completed by each patient who started treatment during the inclusion period. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
HP: Conceptualization, Data curation, Writing – original draft, Writing – review & editing. VS: Formal analysis, Methodology, Writing – original draft. P-AD: Supervision, Writing – original draft.
The author(s) declare that no financial support was received for the research and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2025.1538507/full#supplementary-material
1. GCO. (2023). Cancer today. Available online at: http://gco.iarc.fr/today/home (Accessed November 29, 2023).
2. Institut National du Cancer. (2023). Panorama des cancers en France - édition 2023 - Ref: PANOKFR2023B. Available online at: https://www.e-cancer.fr/Expertises-et-publications/Catalogue-des-publications/Panorama-des-cancers-en-France-edition-2023 (Accessed November 29, 2023).
3. Siegel, DA, O’Neil, ME, Richards, TB, Dowling, NF, and Weir, HK. Prostate Cancer incidence and survival, by stage and race/ethnicity — United States, 2001–2017. Morb Mortal Wkly Rep. (2020) 69:1473–80. doi: 10.15585/mmwr.mm6941a1
4. Artibani, W, Porcaro, AB, De Marco, V, Cerruto, MA, and Siracusano, S. Management of biochemical recurrence after primary curative treatment for prostate Cancer: a review. Urol Int. (2017) 100:251–62. doi: 10.1159/000481438
5. Parker, C, Castro, E, Fizazi, K, Heidenreich, A, Ost, P, Procopio, G, et al. Prostate cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. (2020) 31:1119–34. doi: 10.1016/j.annonc.2020.06.011
6. Horoszewicz, JS, Kawinski, E, and Murphy, GP. Monoclonal antibodies to a new antigenic marker in epithelial prostatic cells and serum of prostatic cancer patients. Anticancer Res. (1987) 7:927–35.
7. Hawkey, NM, Sartor, AO, Morris, MJ, and Armstrong, AJ. Prostate-specific membrane antigen–targeted Theranostics: past, present, and future approaches. Clin Adv Hematol Oncol. (2022) 20:227–38.
8. Shahrokhi, P, Farahani, AM, Tamaddondar, M, and Rezazadeh, F. The utility of radiolabeled PSMA ligands for tumor imaging. Chem Biol Drug Des. (2022) 99:136–61. doi: 10.1111/cbdd.13946
9. Langbein, T, Weber, WA, and Eiber, M. Future of Theranostics: an outlook on precision oncology in nuclear medicine. J Nucl Med. (2019) 60:13S–9S. doi: 10.2967/jnumed.118.220566
10. IAEA. (2024). Livechart - Table of nuclides - nuclear structure and decay data. Available online at: https://www-nds.iaea.org/relnsd/vcharthtml/VChartHTML.html (Accessed January 20, 2024).
11. Sjögreen Gleisner, K, Chouin, N, Gabina, PM, Cicone, F, Gnesin, S, Stokke, C, et al. EANM dosimetry committee recommendations for dosimetry of 177Lu-labelled somatostatin-receptor- and PSMA-targeting ligands. Eur J Nucl Med Mol Imaging. (2022) 49:1778–809. doi: 10.1007/s00259-022-05727-7
12. Sartor, O, de Bono, J, Chi, KN, Fizazi, K, Herrmann, K, Rahbar, K, et al. Lutetium-177-PSMA-617 for metastatic castration-resistant prostate Cancer. N Engl J Med. (2021) 385:1091–103. doi: 10.1056/NEJMoa2107322
13. Hotta, M, Gafita, A, Czernin, J, and Calais, J. Outcome of patients with PSMA PET/CT screen failure by VISION criteria and treated with 177Lu-PSMA therapy: a multicenter retrospective analysis. J Nucl Med. (2022) 63:1484–8. doi: 10.2967/jnumed.121.263441
14. Haute Autorité de Santé. (2024). PLUVICTO (lutécium (177Lu) vipivotide tétraxétan) - Cancer de la prostate. Available online at: https://www.has-sante.fr/jcms/p_3443283/fr/pluvicto-lutecium-177lu-vipivotide-tetraxetan-cancer-de-la-prostate (Accessed August 14, 2024).
15. Kratochwil, C, Fendler, WP, Eiber, M, Hofman, MS, Emmett, L, Calais, J, et al. Joint EANM/SNMMI procedure guideline for the use of 177Lu-labeled PSMA-targeted radioligand-therapy (177Lu-PSMA-RLT). Eur J Nucl Med Mol Imaging. (2023) 50:2830–45. doi: 10.1007/s00259-023-06255-8
16. Rasul, S, Hartenbach, M, Wollenweber, T, Kretschmer-Chott, E, Grubmüller, B, Kramer, G, et al. Prediction of response and survival after standardized treatment with 7400 MBq 177Lu-PSMA-617 every 4 weeks in patients with metastatic castration-resistant prostate cancer. Eur J Nucl Med Mol Imaging. (2021) 48:1650–7. doi: 10.1007/s00259-020-05082-5
17. Hotta, M, Gafita, A, Murthy, V, Benz, MR, Sonni, I, Burger, IA, et al. PSMA PET tumor–to–salivary gland ratio to predict response to [177Lu]PSMA Radioligand therapy: an international multicenter retrospective study. J Nucl Med. (2023) 64:1024–9. doi: 10.2967/jnumed.122.265242
18. Gioulbasanis, I, Baracos, VE, Giannousi, Z, Xyrafas, A, Martin, L, Georgoulias, V, et al. Baseline nutritional evaluation in metastatic lung cancer patients: Mini nutritional assessment versus weight loss history. Ann Oncol. 22:835–41. doi: 10.1093/annonc/mdq440
19. Dewys, WD, Begg, C, Lavin, PT, Band, PR, Bennett, JM, Bertino, JR, et al. Prognostic effect of weight loss prior tochemotherapy in cancer patients. Am J Med. (1980) 69:491–7. doi: 10.1016/S0149-2918(05)80001-3
20. Andreyev, HJN, Norman, AR, Oates, J, and Cunningham, D. Why do patients with weight loss have a worse outcome when undergoing chemotherapy for gastrointestinal malignancies? Eur J Cancer. (1998) 34:503–9. doi: 10.1016/S0959-8049(97)10090-9
21. Shachar, SS, and Williams, GR. The obesity paradox in cancer – moving beyond BMI. Cancer Epidemiol Biomark Prev. (2017) 26:13–6. doi: 10.1158/1055-9965.EPI-16-0439
22. Flegal, KM, Kit, BK, Orpana, H, and Graubard, BI. Association of all-cause mortality with overweight and obesity using standard body mass index categories: a systematic review and meta-analysis. JAMA. (2013) 309:71–82. doi: 10.1001/jama.2012.113905
23. Shah, AD, Kandula, NR, Lin, F, Allison, MA, Carr, J, Herrington, D, et al. Less favorable body composition and adipokines in south Asians compared with other US ethnic groups: results from the MASALA and MESA studies. Int J Obes. (2016) 40:639–45. doi: 10.1038/ijo.2015.219
24. Cruz-Jentoft, AJ, Baeyens, JP, Bauer, JM, Boirie, Y, Cederholm, T, Landi, F, et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age and Ageing. (2010) 39:412–23. doi: 10.1093/ageing/afq034
25. Cruz-Jentoft, AJ, Landi, F, Schneider, SM, Zúñiga, C, Arai, H, Boirie, Y, et al. Prevalence of and interventions for sarcopenia in ageing adults: a systematic review. Report of the international sarcopenia initiative (EWGSOP and IWGS). Age Ageing. (2014) 43:748–59. doi: 10.1093/ageing/afu115
26. Cruz-Jentoft, AJ, Landi, F, Topinková, E, and Michel, JP. Understanding sarcopenia as a geriatric syndrome. Curr Opin Clin Nutr Metab Care. (2010) 13:1–7. doi: 10.1097/MCO.0b013e328333c1c1
27. Wallace, JI, and Schwartz, RS. Involuntary weight loss in elderly outpatients: recognition, etiologies, and treatment. Clin Geriatr Med. (1997) 13:717–36. doi: 10.1016/S0749-0690(18)30146-0
28. Newman, AB, Yanez, D, Harris, T, Duxbury, A, Enright, PL, Fried, LP, et al. Weight change in old age and its association with mortality. J Am Geriatr Soc. (2001) 49:1309–18. doi: 10.1046/j.1532-5415.2001.49258.x
29. Francini, E, Gray, KP, Xie, W, Shaw, GK, Valença, L, Bernard, B, et al. Time of metastatic disease presentation and volume of disease are prognostic for metastatic hormone sensitive prostate cancer (mHSPC). Prostate. (2018) 78:889–95. doi: 10.1002/pros.23645
30. Bajeot, AS, Roumiguié, M, Rébillard, X, Descotes, JL, Duguet, C, Lebret, T, et al. Prise en charge des cancers de la prostate métastatiques synchrones et métachrones en France: étude observationnelle à partir des “RCP sentinelles” de l’AFU. Prog En Urol. (2022) 32:691–701. doi: 10.1016/j.purol.2022.04.013
31. D’Amico, AV, Chen, MH, Roehl, KA, and Catalona, WJ. Preoperative PSA velocity and the risk of death from prostate Cancer after radical prostatectomy. N Engl J Med. (2004) 351:125–35. doi: 10.1056/NEJMoa032975
32. D’Amico, AV, Moul, JW, Carroll, PR, Sun, L, Lubeck, D, and Chen, MH. Surrogate end point for prostate cancer–specific mortality after radical prostatectomy or radiation therapy. JNCI J Natl Cancer Inst. (2003) 95:1376–83. doi: 10.1093/jnci/djg043
33. Suman, S, Parghane, RV, Joshi, A, Prabhash, K, Bakshi, G, Talole, S, et al. Therapeutic efficacy, prognostic variables and clinical outcome of 177Lu-PSMA-617 PRLT in progressive mCRPC following multiple lines of treatment: prognostic implications of high FDG uptake on dual tracer PET-CT Vis-à-Vis Gleason score in such cohort. Br J Radiol. (2019) 92:20190380. doi: 10.1259/bjr.20190380
34. Telli, T, Tuncel, M, Karabulut, E, Aksoy, S, Erman, M, Akdogan, B, et al. Prognostic factors of overall and prostate-specific antigen-progression-free survival in metastatic castration-resistant prostate cancer patients treated with 177Lu-PSMA-617. A single-center prospective observational study. Prostate. (2023) 83:792–800. doi: 10.1002/pros.24518
35. Gafita, A, Calais, J, Grogan, TR, Hadaschik, B, Wang, H, Weber, M, et al. Nomograms to predict outcomes after 177Lu-PSMA therapy in men with metastatic castration-resistant prostate cancer: an international, multicentre, retrospective study. Lancet Oncol. (2021) 22:1115–25. doi: 10.1016/S1470-2045(21)00274-6
36. Ferdinandus, J, Eppard, E, Gaertner, FC, Kürpig, S, Fimmers, R, Yordanova, A, et al. Predictors of response to Radioligand therapy of metastatic castrate-resistant prostate Cancer with 177Lu-PSMA-617. J Nucl Med. (2017) 58:312–9. doi: 10.2967/jnumed.116.178228
37. Li, F, Xiang, H, Pang, Z, Chen, Z, Dai, J, Chen, S, et al. Association between lactate dehydrogenase levels and oncologic outcomes in metastatic prostate cancer: a meta-analysis. Cancer Med. (2020) 9:7341–51. doi: 10.1002/cam4.3108
38. Nishimori, H, Ehata, S, Suzuki, HI, Katsuno, Y, and Miyazono, K. Prostate Cancer cells and bone stromal cells mutually interact with each other through bone morphogenetic protein-mediated signals*. J Biol Chem. (2012) 287:20037–46. doi: 10.1074/jbc.M112.353094
39. Mundy, GR. Metastasis to bone: causes, consequences and therapeutic opportunities. Nat Rev Cancer. (2002) 2:584–93. doi: 10.1038/nrc867
40. Heinrich, D, Bruland, Ø, Guise, TA, Suzuki, H, and Sartor, O. Alkaline phosphatase in metastatic castration-resistant prostate cancer: reassessment of an older biomarker. Future Oncol. (2018) 14:2543–56. doi: 10.2217/fon-2018-0087
41. Barber, TW, Singh, A, Kulkarni, HR, Niepsch, K, Billah, B, and Baum, RP. Clinical outcomes of 177Lu-PSMA Radioligand therapy in earlier and later phases of metastatic castration-resistant prostate Cancer grouped by previous Taxane chemotherapy. J Nucl Med. (2019) 60:955–62. doi: 10.2967/jnumed.118.216820
42. Heck, MM, Tauber, R, Schwaiger, S, Retz, M, D’Alessandria, C, Maurer, T, et al. Treatment outcome, toxicity, and predictive factors for Radioligand therapy with 177Lu-PSMA-I&T in metastatic castration-resistant prostate Cancer. Eur Urol. (2019) 75:920–6. doi: 10.1016/j.eururo.2018.11.016
43. Rathke, H, Holland-Letz, T, Mier, W, Flechsig, P, Mavriopoulou, E, Röhrich, M, et al. Response prediction of 177Lu-PSMA-617 Radioligand therapy using prostate-specific antigen, chromogranin a, and lactate dehydrogenase. J Nucl Med. (2020) 61:689–95. doi: 10.2967/jnumed.119.231431
44. Bräuer, A, Grubert, LS, Roll, W, Schrader, AJ, Schäfers, M, Bögemann, M, et al. 177Lu-PSMA-617 radioligand therapy and outcome in patients with metastasized castration-resistant prostate cancer. Eur J Nucl Med Mol Imaging. (2017) 44:1663–70. doi: 10.1007/s00259-017-3751-z
45. Rahbar, K, Ahmadzadehfar, H, Kratochwil, C, Haberkorn, U, Schäfers, M, Essler, M, et al. German multicenter study investigating 177Lu-PSMA-617 radioligand therapy in advanced prostate cancer patients. J Nucl Med. (2017) 58:85–90. doi: 10.2967/jnumed.116.183194
46. Zhang, L, Zhou, G, Li, Y, Tang, L, Mao, Y, Lin, A, et al. Combined prognostic value of pretreatment anemia and cervical node necrosis in patients with nasopharyngeal carcinoma receiving intensity-modulated radiotherapy: a large-scale retrospective study. Cancer Med. (2017) 6:2822–31. doi: 10.1002/cam4.1233
47. Caro, JJ, Salas, M, Ward, A, and Goss, G. Anemia as an independent prognostic factor for survival in patients with cancer. Cancer. (2001) 91:2214–21. doi: 10.1002/1097-0142(20010615)91:12<2214::AID-CNCR1251>3.0.CO;2-P
48. Ahmadzadehfar, H, Eppard, E, Kürpig, S, Fimmers, R, Yordanova, A, Schlenkhoff, CD, et al. Therapeutic response and side effects of repeated radioligand therapy with 177Lu-PSMA-DKFZ-617 of castrate-resistant metastatic prostate cancer. Oncotarget. (2016) 7:12477–88. doi: 10.18632/oncotarget.7245
49. Morris, MJ, Castellano, D, Herrmann, K, de Bono, JS, Shore, ND, Chi, KN, et al. 177Lu-PSMA-617 versus a change of androgen receptor pathway inhibitor therapy for taxane-naive patients with progressive metastatic castration-resistant prostate cancer (PSMAfore): a phase 3, randomised, controlled trial [published correction appears in lancet]. Lancet. (2025) 404:2542. doi: 10.1016/S0140-6736(24)027168
50. Azad, AA, Bressel, M, Tan, H, Voskoboynik, M, Suder, A, Weickhardt, AJ, et al. Sequential [177Lu]Lu-PSMA-617 and docetaxel versus docetaxel in patients with metastatic hormone-sensitive prostate cancer (UpFrontPSMA): a multicentre, open-label, randomised, phase 2 study. Lancet Oncol. (2024) 25:1267–76. doi: 10.1016/S1470-2045(24)00440-6
51. Hofman, MS, Emmett, L, Sandhu, S, Iravani, A, Joshua, AM, Goh, JC, et al. [177Lu]Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): a randomised, open-label, phase 2 trial. Lancet. (2021) 397:797–804. doi: 10.1016/S0140-6736(21)00237-3
52. Kuo, P, Hesterman, J, Rahbar, K, Kendi, AT, Wei, XX, Fang, B, et al. [68Ga]Ga-PSMA-11 PET baseline imaging as a prognostic tool for clinical outcomes to [177Lu]Lu-PSMA-617 in patients with mCRPC: a VISION substudy. J Clin Oncol. (2022) 40:5002–2. doi: 10.1200/JCO.2022.40.16_suppl.5002
53. Eisazadeh, R, Mirshahvalad, SA, Schwieghofer-Zwink, G, Hehenwarter, L, Rendl, G, Gampenrieder, S, et al. Pre-treatment 68 Ga-PSMA-11 PET/CT prognostic value in predicting response to 177Lu-PSMA-I&T therapy and patient survival. Mol Imaging Biol. (2024) 26:360–9. doi: 10.1007/s11307-024-01900-6
54. Emmett, L, Crumbaker, M, Ho, B, Willowson, K, Eu, P, Ratnayake, L, et al. Results of a prospective phase 2 pilot trial of 177Lu–PSMA-617 therapy for metastatic castration-resistant prostate Cancer including imaging predictors of treatment response and patterns of progression. Clin Genitourin Cancer. (2019) 17:15–22. doi: 10.1016/j.clgc.2018.09.014
55. Kuo, PH, Morris, MJ, Hesterman, J, Kendi, AT, Rahbar, K, Wei, XX, et al. Quantitative 68Ga-PSMA-11 PET and clinical outcomes in metastatic castration-resistant prostate Cancer following 177Lu-PSMA-617 (VISION trial). Radiology. (2024) 312:e233460. doi: 10.1148/radiol.233460
56. Wang, G, Zang, J, Jiang, Y, Liu, Q, Sui, H, Wang, R, et al. A single-arm, low-dose, prospective study of 177Lu-EB-PSMA Radioligand therapy in patients with metastatic castration-resistant prostate Cancer. J Nucl Med. (2023) 64:611–7. doi: 10.2967/jnumed.122.264857
57. Rosar, F, Burgard, C, David, S, Marlowe, RJ, Bartholomä, M, Maus, S, et al. Dual FDG/PSMA PET imaging to predict lesion-based progression of mCRPC during PSMA-RLT. Sci Rep. (2024) 14:11271. doi: 10.1038/s41598-024-61961-z
58. Satapathy, S, Mittal, BR, and Sood, A. Visceral metastases as predictors of response and survival outcomes in patients of castration-resistant prostate Cancer treated with 177Lu-labeled prostate-specific membrane antigen Radioligand therapy: a systematic review and Meta-analysis. Clin Nucl Med. (2020) 45:935–42. doi: 10.1097/RLU.0000000000003307
59. Vanwelkenhuyzen, J, Van Bos, E, Van Bruwaene, S, Lesage, K, Maes, A, Üstmert, S, et al. AR and PI3K genomic profiling of cell-free DNA can identify poor responders to Lutetium-177-PSMA among patients with metastatic castration-resistant prostate Cancer. Eur Urol Open Sci. (2023) 53:63–6. doi: 10.1016/j.euros.2023.05.008
60. De Giorgi, U, Sansovini, M, Severi, S, Nicolini, S, Monti, M, Gurioli, G, et al. Circulating androgen receptor gene amplification and resistance to 177Lu-PSMA-617 in metastatic castration-resistant prostate cancer: results of a phase 2 trial. Br J Cancer. (2021) 125:1226–32. doi: 10.1038/s41416-021-01508-5
61. Sun, M, Thomas, C, Orlando, F, Sigouros, M, Osborne, J, Nauseef, J, et al. 1390P circulating tumor DNA (ctDNA) and prognosis with PSMA-targeted radionuclide therapy (TRT). Ann Oncol. (2022) 33:S1179. doi: 10.1016/j.annonc.2022.07.1522
62. Moghrabi, S, Al-Houwari, R, Ruzzeh, S, and Al-Ibraheem, A. Therapeutic challenges in metastatic castration-resistant prostate Cancer: a case study and review of prostate-specific membrane antigen-targeted therapy failures in highly prostate-specific membrane antigen-avid disease. Cureus. (2024) 16:e76224. doi: 10.7759/cureus.76224
63. Sartor, O, Gauna, DEC, Herrmann, K, De, BJS, Shore, ND, Chi, KNN, et al. LBA13 phase III trial of [177Lu]Lu-PSMA-617 in taxane-naive patients with metastatic castration-resistant prostate cancer (PSMAfore). Ann Oncol. (2023) 34:S1324–5. doi: 10.1016/j.annonc.2023.10.085
64. Tagawa, ST, Sartor, AO, Saad, F, Reid, AH, Sakharova, OV, Feng, FY, et al. PSMAddition: a phase 3 trial to compare treatment with 177Lu-PSMA-617 plus standard of care (SoC) and SoC alone in patients with metastatic hormone-sensitive prostate cancer. J Clin Oncol. (2023) 41:TPS5116–6. doi: 10.1200/JCO.2023.41.16_suppl.TPS5116
Keywords: 177Lu-PSMA, mCRPC, predictive factors, therapeutic response, SULmax, total tumor volume, PSG score
Citation: Peslier H, Seegers V and Dufour P-A (2025) Study of predictive factors for response to 177LU-PSMA in patients with metastatic castration-resistant prostate cancer. Front. Med. 12:1538507. doi: 10.3389/fmed.2025.1538507
Edited by:
Abdul K. Parchur, Medical College of Wisconsin, United StatesReviewed by:
Akram Al-Ibraheem, King Hussein Cancer Center, JordanCopyright © 2025 Peslier, Seegers and Dufour. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hugo Peslier, hpeslier@yahoo.fr
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.