
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Med., 14 April 2022
Sec. Rheumatology
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.871744
This article is part of the Research TopicGlobal Excellence in Rheumatology: EuropeView all 7 articles
 Jan-Gerd Rademacher1†Björn Tampe1†Angela Borisch1Rosa Marie Buschfort1Andrea von Figura1Thomas Asendorf2Peter Korsten1*
Jan-Gerd Rademacher1†Björn Tampe1†Angela Borisch1Rosa Marie Buschfort1Andrea von Figura1Thomas Asendorf2Peter Korsten1*
Introduction: Raynaud’s phenomenon (RP) and digital ulcers (DU) are frequent manifestations of Systemic Sclerosis (SSc). Despite being very common in SSc patients, both conditions have proven to be notoriously difficult to study. There are very few available approved drugs with varying efficacy. It has been shown that the presence of DU is associated with increased whole blood viscosity (WBV). Rheopheresis (RheoP) is an extracorporeal apheresis technique used to treat microcirculatory disorders by improving blood viscosity. Improved blood flow and wound healing after RheoP treatments have been reported in single case reports.
Methods and Analysis: We report the clinical trial protocol of “A randomized controlled prospective single-center feasibility study of Rheopheresis for Raynaud’s syndrome and Digital Ulcers in Systemic Sclerosis (RHEACT).” RHEACT aims to investigate the efficacy of RheoP on the Raynaud Condition Score (RCS) as the primary efficacy outcome measure after 16 weeks from baseline. Thirty patients will be randomized in a 1:1:1 ratio to one of two RheoP treatment groups or assigned to the standard of care (SoC) control group (intravenous iloprost). Secondary endpoints include changes in DU, changes in nailfold video capillaroscopy and patient-reported-outcomes (Scleroderma Health Assessment Questionnaire, FACIT-Fatigue, and the Disability of Arm, Shoulder, and Hand, quick version).
Discussion: Apheresis techniques have been investigated in SSc but mainly in observational, retrospective studies, or single case reports. RheoP is a pathophysiologically driven potential new therapy for heavily burdened patients with SSc-associated secondary RP with or without DU.
Ethics and Dissemination: The study was registered at clinicaltrials.gov (Identifier: NCT05204784). Furthermore, the study is made publicly available on the website of the German network of Systemic Sclerosis “Deutsches Netzwerk Systemische Sklerodermie (DNSS).”
Systemic Sclerosis (SSc) is an autoimmune disease of unknown etiology characterized by organ fibrosis and vasculopathy (1). The latter manifests clinically as Raynaud’s phenomenon (RP), present in 90–100% of patients with SSc (2). While primary RP, in which the cause is unknown, is usually benign, secondary RP occurs in the context of distinct disorders, and one should suspect a predisposing disease (3). In its classic form, Raynaud’s phenomenon leads to pallor, cyanosis, and reactive hyperemia of affected fingers and toes. A critical complication of RP is the development of digital ulcers (DU), and skin necrosis, digital (auto-)amputation, and functional impairment may occur subsequently (4). Current standard of care (SoC) treatment options aim at vasodilation. They include conservative procedures such as cold exposure prevention and hand-warming but also medical therapy with antihypertensive drugs, such as calcium-channel blockers (CCB) or the intravenous application of the vasodilating agent iloprost (1, 2, 4). However, these antihypertensive or vasodilating drugs are often not well tolerated by patients with reported side effects, including hypotension, migraine-type headache, or chest pain in up to 92% of patients (5). Further, intravenous iloprost infusions are typically performed in hospitalized patients for five to seven consecutive days and may require repeat administrations.
Other treatments, such as phosphodiesterase 5 (PDE5) inhibitors or endothelin receptor antagonists (ERA), have been studied (6) but have not been approved either for RP or DU in many countries. Bosentan, an ERA family member, has been approved for the prevention of new DU (7) but not for RP. Therefore, there is a clear need for additional treatment options.
Recently, whole blood viscosity (WBV) has been shown to be increased in a pilot study of SSc patients with DU compared to patients with a history of DU or without DU (8). Therefore, treatments that can positively affect blood viscosity might be a potential therapeutic option for patients with SSc-associated RP or DU. Plasma exchange (PEX) or variants thereof have been used in SSc with mixed results (9). In this regard, rheopheresis (RheoP) is an extracorporeal therapeutic intervention and a variant of PEX without needing a replacement fluid (fresh frozen plasma or albumin) using an additional rheofilter. It is, therefore, also referred to as double-filtration plasmapheresis (DFPP). In addition, RheoP has been investigated in other conditions affecting the microvascular circulation, such as age-related macular degeneration, sensorineural hearing loss, critical limb ischemia, or diabetic foot syndrome after failure of standard treatments (10–13).
This feasibility study aims to explore therapeutic RheoP as a novel treatment option for SSc-associated RP and DU and compare it to SoC treatment (iloprost). However, RheoP has thus far only been used in single case reports or case series (14, 15). Therefore, the optimal treatment modality, duration, or frequency of RheoP in SSc has not been established yet.
RHEACT (ClinicalTrials.gov Identifier: NCT05204784) is a randomized controlled, prospective single-center study conducted at the Department of Nephrology and Rheumatology of the University Medical Center (UMG) in Göttingen, Germany. RHEACT will compare two different RheoP treatment regimens with iloprost over 24 weeks. The primary endpoint will be assessed at 16 weeks. The decision to evaluate the primary endpoint at 16 weeks was chosen to maximize patient retention in the trial until the primary endpoint assessment. A total of 30 patients will be allocated at random to one of three treatments.
Patients will be randomized using block randomization with random block length, stratified for the month of inclusion (October to March or April to August) to minimize bias due to ambient temperatures on the primary outcome measure. Randomization will be performed electronically after the assessment of eligibility.
All patients ≥ 18 years of age fulfilling the ACR/EULAR Classification Criteria for SSc (Supplementary File 1) (16) are eligible. The presence of RP with or without DU is required. Furthermore, the failure of at least one SoC therapy has to be reported. The Raynaud Condition Score (RCS), a patient-reported outcome measure used in many studies assessing RP, has to have a value ≥ 4 (17–19). To perform the RheoP procedure, appropriate venous access, either through a peripherally or centrally inserted catheter, must be established.
Exclusion criteria include significant anemia (hemoglobin < 8 g/dL), clinically relevant hemorrhagic diathesis or coagulopathy, diabetes mellitus, and severe acute or chronic kidney (eGFR < 30 ml/min/1.73 m2) or liver failure. In addition, patients with hypotension (systolic blood pressure < 100 mmHg) are not considered eligible. Chronic viral infections like HIV and Hepatitis B and C also preclude participation in this study. Patients with relevant neurological diseases like epilepsy, psychosis, dementia, or other relevant neurologic conditions are also excluded from participation. Other general exclusion criteria include a life expectancy of fewer than 12 months, abuse of alcohol, drugs, and a reported long-term serious tobacco abuse with documented consequential damage like severe vascular disease (Fontaine stage III or higher). Furthermore, patients with severe hyperlipoproteinemia, defined as a significant elevation of LP(a) or LDL cholesterol despite standard doses of medical therapy, are also not eligible for participation in this study. The main inclusion and exclusion criteria are summarized in Table 1.
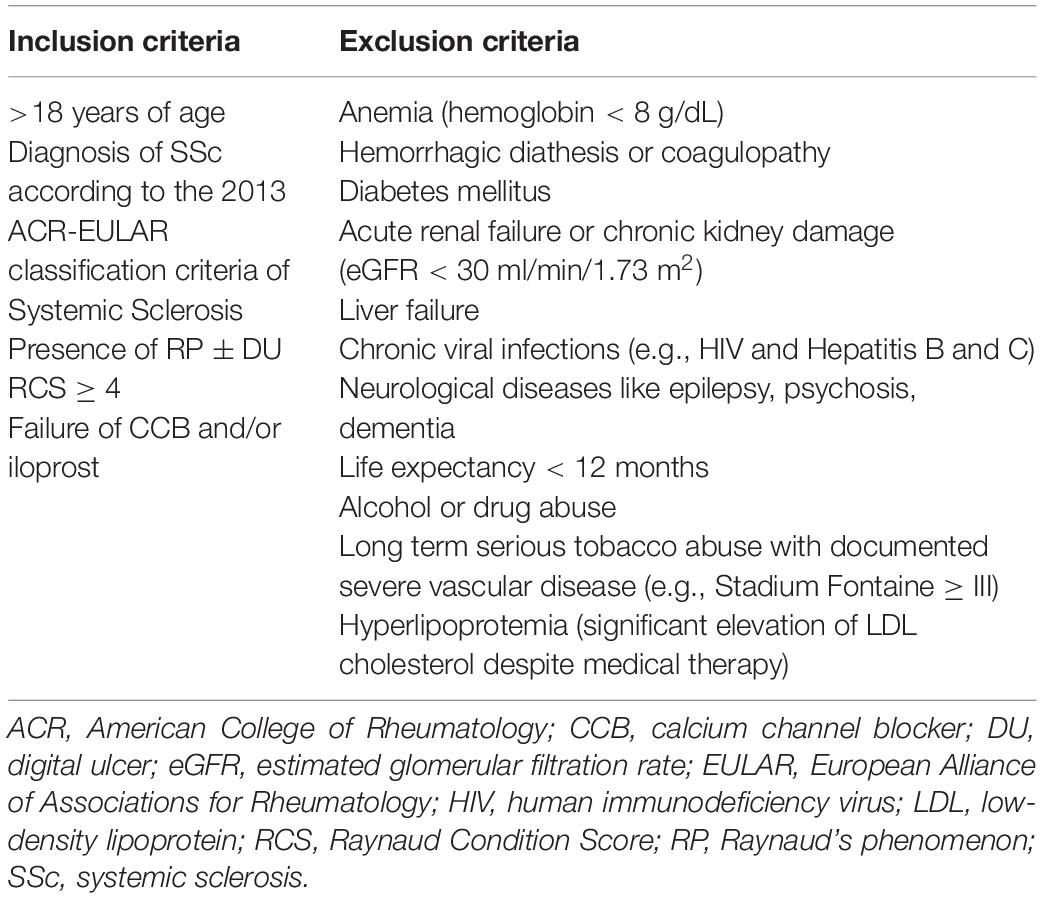
Table 1. Inclusion and exclusion criteria.
The RheoP procedure will be performed and supervised by experienced technical and nursing staff using a Plasauto Sigma blood purification machine (DIAMED Medizintechnik GmbH, Cologne, Germany, and Asahi Kasei Medical Co., Ltd., Tokyo, Japan). The RheoP circuit is depicted in Figure 1. When patients are cannulated peripherally, a blood flow of ∼70–80 ml/min will be used. A maximum blood flow of 100 ml/min will be used in centrally cannulated patients. The plasma flow is aimed at around 25% of the blood flow (∼25 ml/min). The target treatment volume is calculated using the formula: 42 ml × kg body weight (Example: 42 mL × 70 kg BW = 2,940 mL [∼3,000 mL]). A treatment is considered technically appropriate if a target volume of 0.8–1.0 is reached. Heparin is used as an anticoagulant to prevent blood clotting during the procedure. Typical doses are 2500 IU given as a bolus at treatment initiation and 2000 IU per hour as continuous infusion given through the apheresis machine. All products used in this study are CE certified as per regulatory requirements.
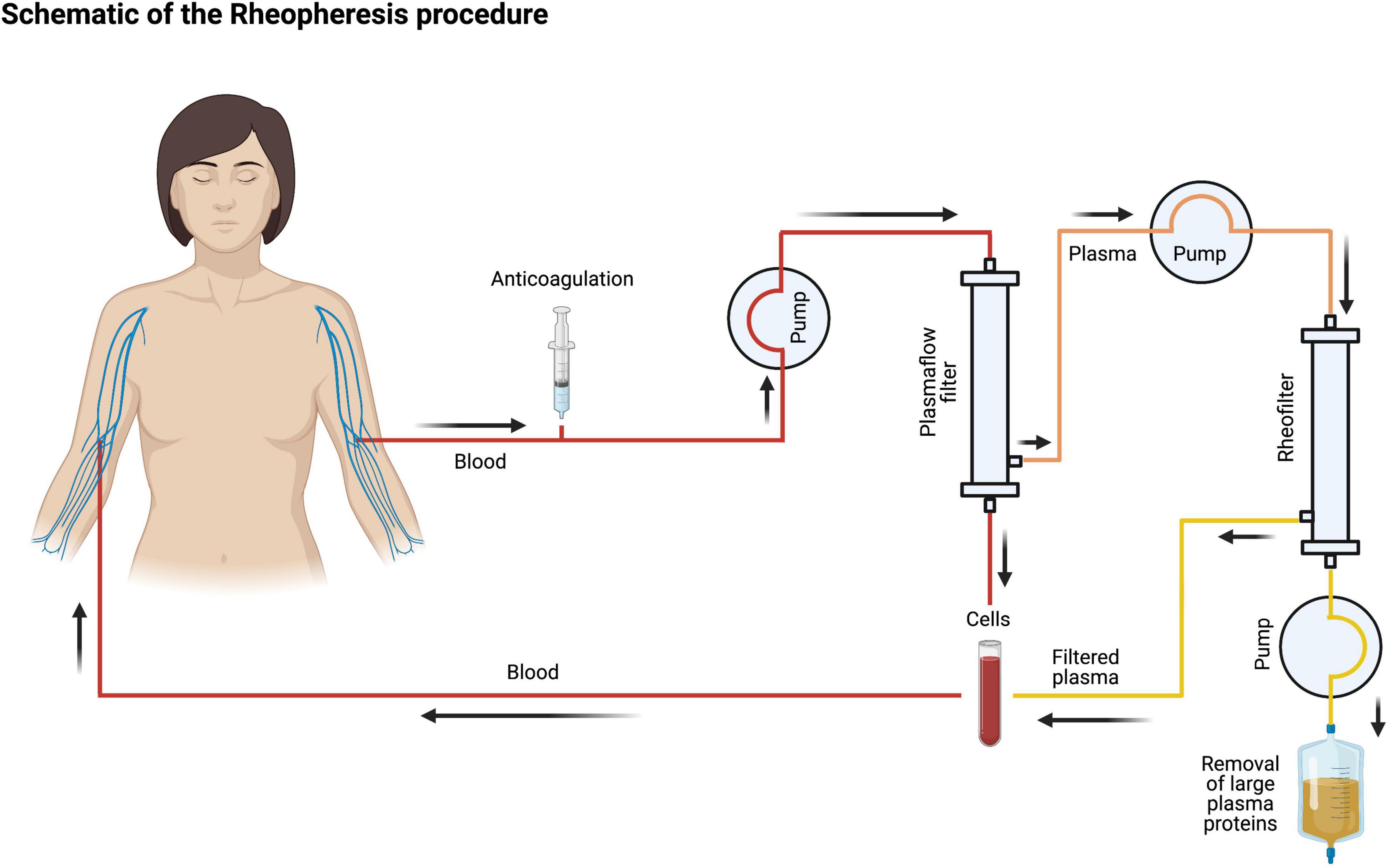
Figure 1. Schematic of the rheopheresis procedure. After obtaining venous access, anticoagulated blood is pumped through a plasma filter. The plasma is then run through the rheofilter, and large plasma proteins are removed. Finally, cells are reinfused, and blood is returned to the patient. The figure was created with biorender.com.
Patients will receive one of three treatments in a 1:1:1 ratio. The treatment groups (RheoP) will be randomized to two treatment schedules (Figure 2).
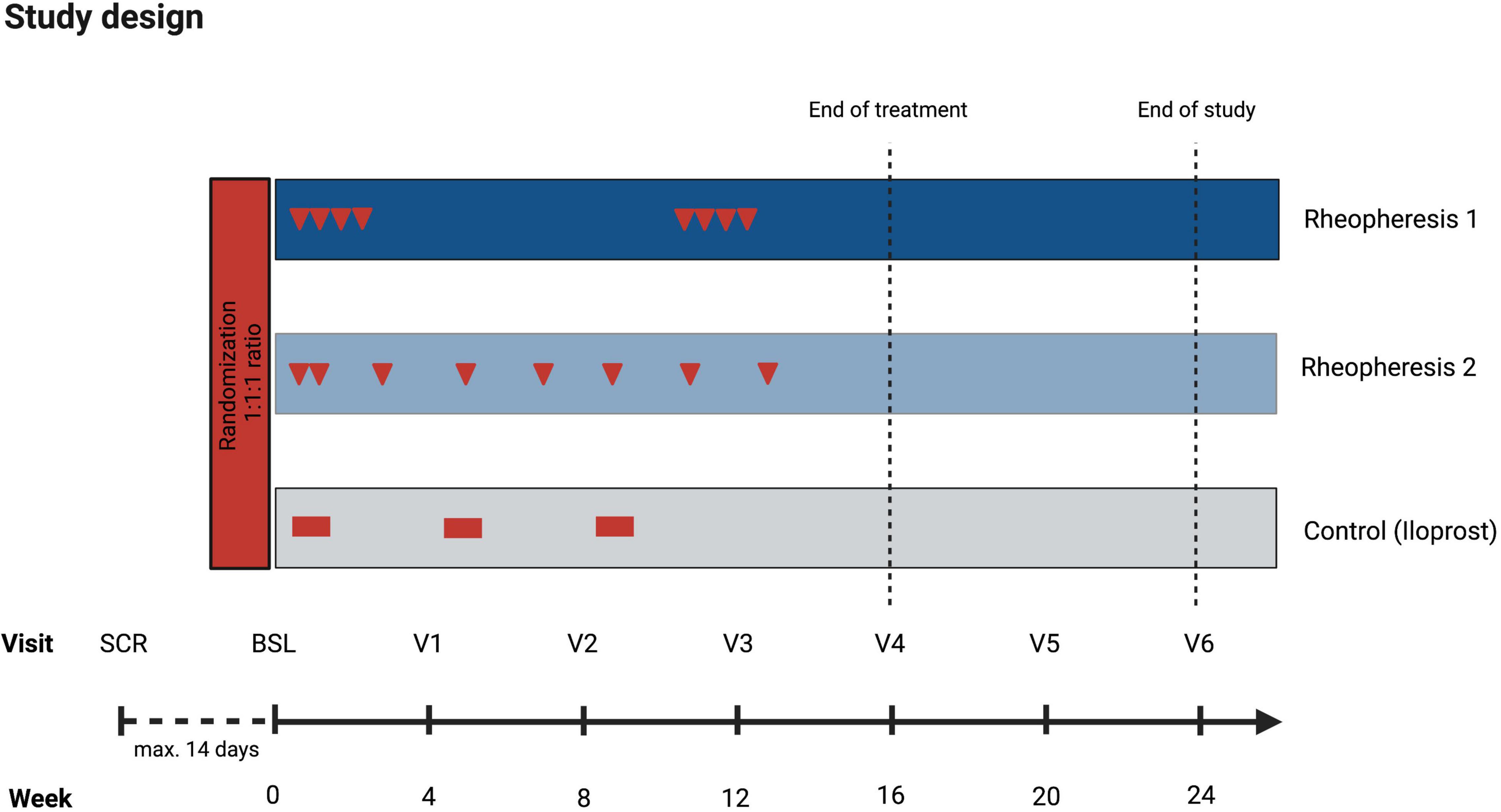
Figure 2. Study design. Treatment schedule (red arrows or blocks) and intervention and control groups assessments. The figure was created with biorender.com. BSL, baseline; SCR, screening; V, visit.
Treatment group 1: This group initially receives two rheopheresis treatments per week for 2 weeks, followed by 8 weeks without treatment. After 8 weeks, the patients will receive another 2 weeks of two treatments per week. Patients in this group will receive a total of eight RheoP treatments.
Treatment group 2: Patients in this group will receive two rheopheresis treatments in week one, followed by treatment intervals of one treatment every 2 weeks. In total, this group also receives eight treatments.
Control group: The control group is supplied with standard medical therapy for RP, consisting of intravenous iloprost therapy given as continuous infusion via an infusion pump over a minimum of 6 h (dose range 10–40 μg per day).
All patients will be advised to comply with general recommendations to avoid RP attacks, such as smoking cessation, avoidance of cold temperatures, stress reduction, and optimized skin care.
Study visits are performed on eight occasions: An initial screening visit to assess eligibility and a baseline visit for randomization. Then, study visits are conducted every 4 weeks up to week 24 (Figure 2). Each study visit consists of a physical examination with vital signs and evaluation of the RCS and modified Rodnan skin score (mRSS). The laboratory analyses include a complete blood count, fibrinogen, antithrombin, d-dimers, uric acid, blood urea nitrogen, creatinine, creatine kinase, nt-pro brain natriuretic peptide, troponin-I, erythrocyte sedimentation rate, low-density lipoprotein (LDL) cholesterol, immunoglobulins, protein electrophoresis, C-reactive protein (CRP), complement factor C3 and C4, and SSc-associated antibodies. All these values are either part of the routine assessment or required to evaluate the technical adequacy of the RheoP procedure (fibrinogen, albumin, IgG, IgM, LDL cholesterol).
The baseline visit and end of treatment visits include a nailfold video capillaroscopy (NVC). Other non-invasive assessments include a transthoracic echocardiography, pulmonary function testing (PFT), and a pulse wave analysis (PWA). An overview of the scheduled assessments is given in Table 2.
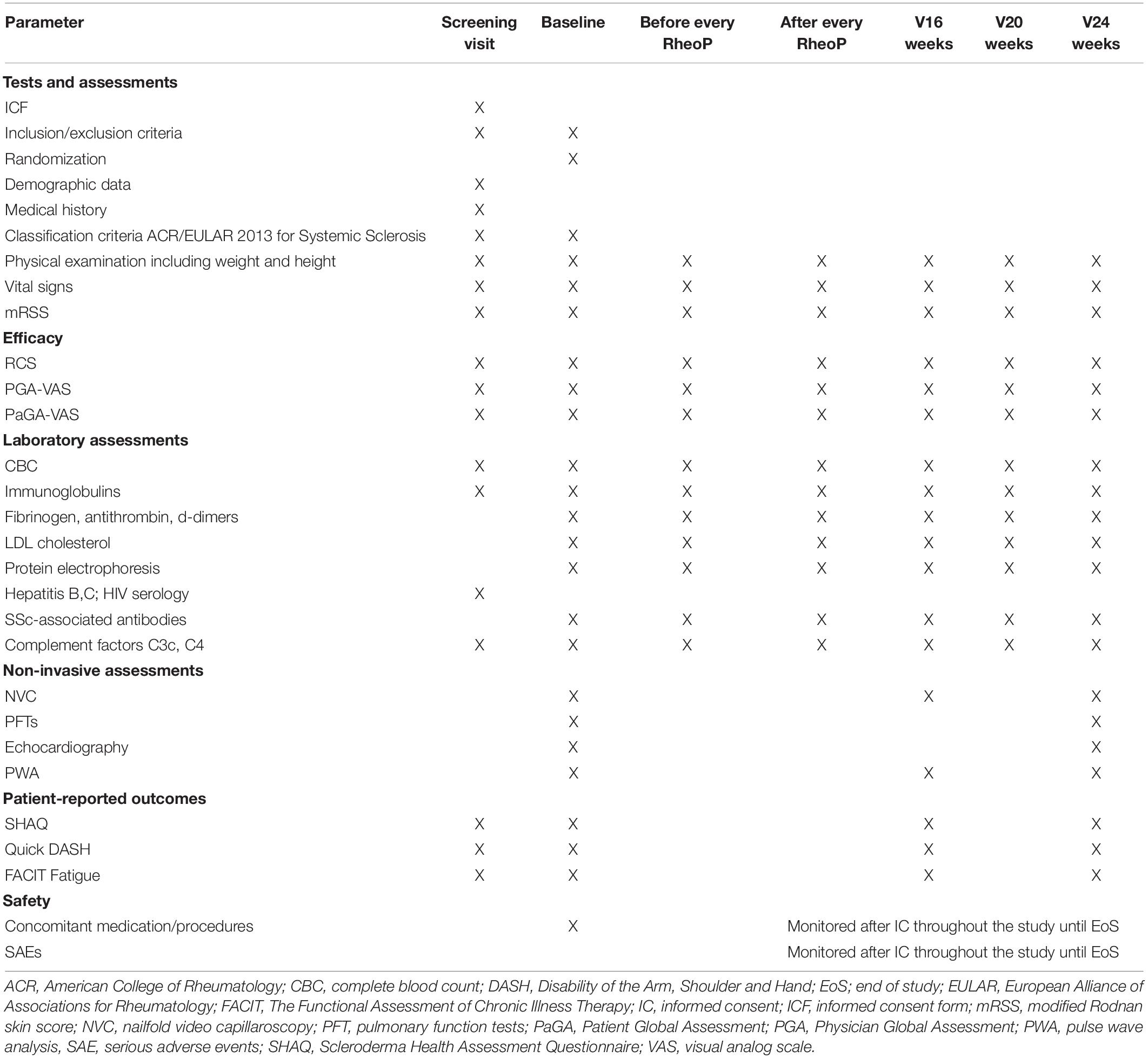
Table 2. Visit schedule and assessments.
The study’s primary outcome measure is the change in RCS after 16 weeks (Supplementary File 2). The RCS is assessed at baseline and every 4 weeks before and after each RheoP (Table 2); it will also be evaluated in the control group receiving SoC therapy. The RCS incorporates the frequency, duration, severity, and impact of RP attacks on a 0–10 numerical rating scale and can be documented using paper or electronic diaries.
Secondary endpoints are the frequency of new DU, worsening of DU, time to healing of existing DU, changes of laboratory parameters, the proportion of patients with an improvement in non-invasive assessments, and changes in patient report outcome measures.
The assessed patient-reported outcome (PROs) measures include the patient global assessment-visual analog scale (PaGA-VAS), the German versions of the Functional Assessment of Chronic Illness Therapy (FACIT) – Fatigue Scale (Supplementary File 3), the Scleroderma Health Assessment Questionnaire (SHAQ, Supplementary File 4), and the Quick Disabilities of the Arm, Shoulder, and Hand (Quick DASH, Supplementary File 5).
Adverse events will be explicitly assessed at every study visit and throughout the entire after the inclusion of every subject. In addition, adverse events will be reported according to the Common Terminology Criteria for Adverse Events (CTCAE, v5.0, November 2017).
Clinical data for all patients, including frequency and duration of Raynaud attacks and the RCS, is collected during the routine clinic visits at least every 6 months. Study-specific data will be collected at screening, baseline, and the defined study visits (Figure 2). Data will be collected through electronic case report forms (eCRF) and stored in a provided GCP-compliant database (REDCap®). Data is collected in compliance with Good Clinical Practice (GCP) and following standard operating procedures (SOP) of the Clinical Trials Unit UMG to ensure high data quality.
Selection bias is minimized by random allocation in a 1:1:1 ratio stratified by the season of admission. Block randomization with random block length will be performed. Performance and detection bias is reduced as the patient’s treatment group assignment will be concealed to a blinded team of study site investigators. Assessments will be performed before and after the treatments. In order to minimize bias related to outside temperatures, we will record the ambient temperatures during the study periods.
The objective of this study is to gather initial data on the efficacy of different treatment protocols. When the sample size is 10, a two-sided 95% confidence interval for the difference in paired means of RCS will extend 1.178 from the observed mean, assuming that the standard deviation is known to be 1.9 and the confidence interval is based on the large sample z statistic. A standard deviation of 1.9 of the difference of the mean RCS was observed in prior studies on iloprost, e.g., Wigley et al. (5). Sample size calculation was performed using nQuery Version 8.3.1.0.
Although the study has a confirmatory design that intends to test for group differences, the primary aim is to gather initial data on the efficacy of RheoP as a novel treatment option. Therefore, both treatment groups’ Pre-Post treatment effects (baseline vs. 16 weeks) will be reported with 95%-confidence intervals. Further, RCS at the end of treatment (at 16 weeks) will be compared between groups by ANCOVA with treatment group as factor and baseline RCS and season as covariates. The secondary endpoint new DUs will be compared using Poisson regression or, in the case of apparent overdispersion, negative binomial regression. Patient proportions will be summarized in tables and compared between groups using Chi Square-Test. Line plots are evaluated, where possible, to descriptively assess the influence of the intervention on observations. Estimators are calculated following the treatment policy with the intention-to-treat principle. Secondary endpoints are analyzed analogously to the primary endpoint. Finally, a sensitivity analysis with the per-protocol population will be performed. Additional vasoactive therapies, if present, will be considered as potentially confounding variables during the analysis.
RHEACT is the first controlled study to evaluate the efficacy of therapeutic RheoP in RP with or without DU in SSc. With this study, we seek to offer a potential new treatment option in patients with refractory RP or non-healing DU despite standard therapy. Raynaud’s phenomenon is almost universal in SSc. In our experience, most SSc patients can be managed with symptomatic or medical treatment alone. However, a significant proportion of patients require additional treatment, including iloprost, ERA, or PDE-5 inhibitors. This is supported by the latest EULAR recommendations (20), but none of these therapies is licensed for RP in SSc, and results from clinical trials have been mixed (21, 22). We acknowledge that the RCS is not a perfect primary outcome measure because it heavily relies on subjective impressions by the patients.
Nevertheless, it is currently the most widely accepted outcome measure in studies for RP. A recent survey among SSc experts showed that the RCS is mainly used in clinical trial settings and has several limitations (19): it may be subject to seasonal variation and recall bias. Also, an individual patient’s RP characteristics may change over time. We try to overcome the first limitation by block randomization according to the season of inclusion (see Methods section). Due to the relatively short observational period (24 weeks), changes over time secondary to vessel obliteration will likely not influence the results significantly. RCS also has the advantage of being a PRO.
In RHEACT, we try to gain insights regarding other secondary outcomes, such as the healing of existing DU or the development of new DU and additional PRO, including fatigue and daily function. Further, more objective outcome measures to study RP in SSc and other conditions are clearly required. For example, we recently investigated microvascular imaging (MVI) as a novel ultrasound-based method to quantify microvascular blood flow (23). However, our preliminary findings must be confirmed before applying them in clinical practice or a clinical trial setting.
Our first experiences with RheoP in refractory RP showed that it is a feasible and well-tolerated therapy (14), which may offer a novel, pathophysiologically based treatment in heavily burdened patients.
The studies involving human participants were reviewed and approved by the Ethics Committee of the University Medical Center Göttingen, Göttingen, Germany (protocol number 36/7/21). The patients/participants will provide their written informed consent to participate in this study.
J-GR wrote the first draft and edited the manuscript. BT conceived the study and edited the manuscript. AB edited and reviewed the manuscript and is the study coordinator. RB assisted with the writing of the manuscript. AF edited and reviewed the manuscript and helped with the planning of the study. TA planned the statistical analysis and edited the manuscript. PK conceived the study, wrote the manuscript, created the figures, and acquired funding for the study. All authors contributed to the article and approved the submitted version.
This study is financially and technically supported by the DIAMED Medizintechnik GmbH, Cologne, Germany. The funder has no role in the planning or the design of the study. The funder will have no role in collecting, reporting, analyzing, or interpreting the data. We acknowledge support by the Open Access Publication Funds of the Göttingen University.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors acknowledge technical support by Klaus Horn, DIAMED Medizintechnik GmbH, Cologne, Germany, and the nursing staff of the apheresis unit of the University Medical Center Göttingen. In addition, the authors thank Florian Walker and Ralf Tostmann from the Clinical Trials Unit of the University Medical Center Göttingen for their support of the study’s organizational aspects. Sonja Kaaden assisted with the design of the REDCap® database. Finally, the authors appreciate feedback on the study protocol provided by Reinhard Klingel concerning technical aspects of the rheopheresis procedure.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2022.871744/full#supplementary-material
1. Allanore Y, Simms R, Distler O, Trojanowska M, Pope J, Denton CP, et al. Systemic sclerosis. Nat Rev Dis Primers. (2015) 1:15002. doi: 10.1038/nrdp.2015.2
2. Gabrielli A, Avvedimento EV, Krieg T. Scleroderma. N Engl J Med. (2009) 360:1989–2003. doi: 10.1056/NEJMra0806188
3. Wigley FM. Clinical practice. Raynaud’s phenomenon. N Engl J Med. (2002) 347:1001–8. doi: 10.1056/NEJMcp013013
4. Abraham S, Steen V. Optimal management of digital ulcers in systemic sclerosis. Ther Clin Risk Manag. (2015) 11:939–47. doi: 10.2147/TCRM.S82561
5. Wigley FM, Wise RA, Seibold JR, McCloskey DA, Kujala G, Medsger TA, et al. Intravenous iloprost infusion in patients with Raynaud phenomenon secondary to systemic sclerosis. A multicenter, placebo-controlled, double-blind study. Ann Intern Med. (1994) 120:199–206. doi: 10.7326/0003-4819-120-3-199402010-00004
6. Herrick AL. Management of Raynaud’s phenomenon and digital ischemia. Curr Rheumatol Rep. (2013) 15:303. doi: 10.1007/s11926-012-0303-1
7. Matucci-Cerinic M, Denton CP, Furst DE, Mayes MD, Hsu VM, Carpentier P, et al. Bosentan treatment of digital ulcers related to systemic sclerosis: results from the RAPIDS-2 randomised, double-blind, placebo-controlled trial. Ann Rheum Dis. (2011) 70:32–8. doi: 10.1136/ard.2010.130658
8. Korsten P, Niewold TB, Zeisberg M, Utset TO, Cho D, Zachary LS, et al. Increased whole blood viscosity is associated with the presence of digital ulcers in systemic sclerosis: results from a cross-sectional pilot study. Autoimmune Dis. (2017) 2017:3529214. doi: 10.1155/2017/3529214
9. Harris ES, Meiselman HJ, Moriarty PM, Metzger A, Malkovsky M. Therapeutic plasma exchange for the treatment of systemic sclerosis: a comprehensive review and analysis. J Scleroder Relat Disord. (2018) 3:132–52. doi: 10.1177/2397198318758606
10. Koss MJ, Kurz P, Tsobanelis T, Lehmacher W, Fassbender C, Klingel R, et al. Prospective, randomized, controlled clinical study evaluating the efficacy of Rheopheresis for dry age-related macular degeneration. Dry AMD treatment with Rheopheresis trial-ART. Graefes Arch Clin Exp Ophthalmol. (2009) 247:1297–306. doi: 10.1007/s00417-009-1113-7
11. Kostal M, Drsata J, Bláha M, Lánská M, Chrobok V. Rheopheresis in treatment of idiopathic sensorineural sudden hearing loss. J Otolaryngol Head Neck Surg. (2017) 46:50. doi: 10.1186/s40463-017-0228-9
12. Klingel R, Erdtracht B, Gauss V, Piazolo A, Mausfeld-Lafdhiya P, Diehm C. Rheopheresis in patients with critical limb ischemia–results of an open label prospective pilot trial. Ther Apher Dial. (2005) 9:473–81. doi: 10.1111/j.1744-9987.2005.00276.x
13. Klingel R, Mumme C, Fassbender T, Himmelsbach F, Altes U, Lotz J, et al. Rheopheresis in patients with ischemic diabetic foot syndrome: results of an open label prospective pilot trial. Ther Apher Dial. (2003) 7:444–55. doi: 10.1046/j.1526-0968.2003.00082.x
14. Korsten P, Müller GA, Rademacher J-G, Zeisberg M, Tampe B. Rheopheresis for Digital Ulcers and Raynaud’s phenomenon in systemic sclerosis refractory to conventional treatments. Front Med (Lausanne). (2019) 6:208. doi: 10.3389/fmed.2019.00208
15. Lutze S, Daeschlein G, Konschake W, Jünger M. Rheopheresis as a causal therapy option for systemic scleroderma (SSc). Clin Hemorheol Microcirc. (2017) 67:229–40. doi: 10.3233/CH-179204
16. van den Hoogen F, Khanna D, Fransen J, Johnson SR, Baron M, Tyndall A, et al. 2013 classification criteria for systemic sclerosis: an American college of rheumatology/European league against rheumatism collaborative initiative. Arthritis Rheum. (2013) 65:2737–47. doi: 10.1002/art.38098
17. Merkel PA, Herlyn K, Martin RW, Anderson JJ, Mayes MD, Bell P, et al. Measuring disease activity and functional status in patients with scleroderma and Raynaud’s phenomenon. Arthritis Rheum. (2002) 46:2410–20.
18. Cutolo M, Smith V, Furst DE, Khanna D, Herrick AL. Points to consider—Raynaud’s phenomenon in systemic sclerosis. Rheumatology. (2017) 56:v45–8. doi: 10.1093/rheumatology/kex199
19. Pauling JD, Frech TM, Hughes M, Gordon JK, Domsic RT, Anderson ME, et al. Patient-reported outcome instruments for assessing Raynaud’s phenomenon in systemic sclerosis: a SCTC vascular working group report. J Scleroder Relat Disord. (2018) 3:249–52. doi: 10.1177/2397198318774307
20. Kowal-Bielecka O, Fransen J, Avouac J, Becker M, Kulak A, Allanore Y, et al. Update of EULAR recommendations for the treatment of systemic sclerosis. Ann Rheum Dis. (2017) 76:1327–39. doi: 10.1136/annrheumdis-2016-209909
21. Hachulla E, Hatron P-Y, Carpentier P, Agard C, Chatelus E, Jego P, et al. Efficacy of sildenafil on ischaemic digital ulcer healing in systemic sclerosis: the placebo-controlled SEDUCE study. Ann Rheum Dis. (2016) 75:1009–15. doi: 10.1136/annrheumdis-2014-207001
22. Khanna D, Denton CP, Merkel PA, Krieg T, Le Brun F-O, Marr A, et al. Effect of macitentan on the development of new ischemic digital ulcers in patients with systemic sclerosis: DUAL-1 and DUAL-2 randomized clinical trials. JAMA. (2016) 315:1975–88. doi: 10.1001/jama.2016.5258
Keywords: rheopheresis, therapeutic plasma exchange, systemic sclerosis, Raynaud’s phenomenon, digital ulcers, blood viscosity
Citation: Rademacher J-G, Tampe B, Borisch A, Buschfort RM, von Figura A, Asendorf T and Korsten P (2022) Study Protocol: A Randomized Controlled Prospective Single-Center Feasibility Study of Rheopheresis for Raynaud’s Syndrome and Digital Ulcers in Systemic Sclerosis (RHEACT Study). Front. Med. 9:871744. doi: 10.3389/fmed.2022.871744
Received: 08 February 2022; Accepted: 11 March 2022;
Published: 14 April 2022.
Edited by:
Chris Wincup, University College London, United KingdomReviewed by:
Simone Parisi, University Hospital City of Health and Science of Turin, ItalyCopyright © 2022 Rademacher, Tampe, Borisch, Buschfort, von Figura, Asendorf and Korsten. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Peter Korsten, peter.korsten@med.uni-goettingen.de
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.