 Mylène Laforest1,2
Mylène Laforest1,2 Stéphane Bouchard
Stéphane Bouchard
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. ICT, 05 September 2016
Sec. Virtual Environments
Volume 3 - 2016 | https://doi.org/10.3389/fict.2016.00018
This article is part of the Research TopicVirtual and Augmented Reality for Education and TrainingView all 10 articles
Obsessive–compulsive disorder (OCD) is characterized by the presence of unwanted and repetitive thoughts triggering significant anxiety, as well as the presence of ritual behaviors or mental acts carried out in response to obsessions to reduce the associated distress. In the contamination subtype, individuals are scared of germs and bacteria, are excessively concerned with cleaning, fear contamination and the spread of disease, and may have a very strong aversion to bodily secretions. A few studies on virtual reality (VR) have been conducted with people suffering from OCD, but they all focus on the subtype characterized by checking rituals. The goal of this study is to confirm the potential of a “contaminated” virtual environment in inducing anxiety in 12 adults suffering from contamination-subtype OCD compared to 20 adults without OCD (N = 32) using a within–between protocol. Subjective (questionnaire) and objective (heart rate) measurements were compiled. Participants were immersed in a control virtual environment (empty and clean room) and a “contaminated” virtual environment (filthy public restroom) designed for the treatment of OCD. Immersions were conducted in a 6-wall CAVE-like system. As hypothesized, the results of repeated-measures ANCOVAs revealed the significant impact of immersion in a filthy public restroom for participants suffering from OCD on both measures. Presence was correlated with anxiety in OCD participants and no difference in presence was observed between groups. Unwanted negative side effects induced by immersions in VR were higher in the OCD group. The clinical implications of the results and directions for further studies are discussed.
The DSM-5 (American Psychiatric Association, 2013) defines obsessive–compulsive disorder (OCD) as characterized by the presence of thoughts, images, or urges perceived as unwanted and inappropriate and causing considerable distress, as well as behavioral or mental rituals used to cope with these obsessions and lessen the associated anxiety. Obsessions and compulsions can be classified in various subtypes. Examples of obsessive thoughts are fear of contamination, pathological doubt, fear of hurting others, symmetry and exactness concern, unacceptable sexual thoughts, and religious obsessions. Compulsive rituals may include such practices as a need to clean, verify, count, or put things away or in order. The contamination subtype is the most prevalent among people suffering from OCD, affecting 47.6% of these individuals (Ball et al., 1996). It is characterized by obsessions, such as fear of germs and filth, fear of disease, and fear of chemicals, as well as by compulsive cleaning, washing, and avoidance of situations where one can be contaminated (e.g., toilet seats). No matter the subtype, people who suffer from OCD often see their ability to function impaired by this disorder as a result of their obsessions and compulsions interfering in their interpersonal and professional lives (Moritz et al., 2005).
The research conducted over the past few decades established cognitive behavioral therapy (CBT), and more specifically the exposure and response prevention technique, as the treatment of choice for this disorder (Meyer, 1966; Lang, 1977; Fals-Stewart et al., 1993). This type of treatment effectively helps patients to face their anxiogenic triggers rather than continue to avoid them or cope with them temporarily using compulsive rituals. For the exposure to be effective, patients must not give in to their compulsions during or after exposure (Stankovic, 2004) and tolerate their anxiety (as defined as an emotion characterized by an increase in physiological arousal and subjective reactions of perceived threat and discomfort).
The exposure and response prevention technique is generally practiced based on real (i.e., in vivo) situations (e.g., exposure to a public restroom) or situations imagined by the patient (McKay et al., 2015). However, there are a number of drawbacks associated with this, such as the potential for actual contamination and contraction of a disease, the costs associated with any travel required, the potential breach of confidentiality, or the patient having trouble envisioning anxiogenic stimuli. A survey of 56 Canadian clinicians treating patients suffering from OCD conducted to document the limitations associated with using in vivo exposure and response prevention (Labonté-Chartrand, 2011) showed that clinicians (a) are aware of the usefulness and safety of exposure, (b) use exposure when they feel they possess the necessary knowledge and skills to do so, and (c) perceive significant challenges in creating, graduating, and standardizing exposure stimuli if they are not experts in treating OCD. As such, there is a certain appeal in developing an alternative tool to address the limitations inherent to in vivo exposure (Labonté-Chartrand, 2011).
Virtual reality (VR) is an emerging technology that can be used to counter the limitations of in vivo exposure (Labonté-Chartrand, 2011; Wiederhold and Bouchard, 2014). VR can be defined as the use of computer and behavioral interfaces to simulate the behavior of 3D entities that interact in real time with each other and with a user immersed via sensorimotor channels (Fuch et al., 2011). Although the specific role of immersion (i.e., the properties of the system stimulating the senses and blocking sensations form the physical environment) and presence on the induction of anxiety and treatment outcome remains to be clarified (Bouchard et al., 2012), research has shown exposure conducted while immersed in VR, or in virtuo exposure, is effective in the treatment of many anxiety disorders [e.g., phobias, social anxiety, post-traumatic stress; see Wiederhold and Bouchard (2014) for an exhaustive review of literature].
Research is now focusing on more complex disorders, such as OCD, to examine the anxiety-inducing potential of VR, with the goal of using this technology for treatments using exposure and response prevention. For example, Kim et al. (2008) examined VR’s ability to induce anxiety in the OCD subtype characterized by checking rituals. Participants were immersed with a head-mounted display in a virtual apartment where they had to turn on and off light switches, gas burners, and water faucets and, after a distraction phase, were invited to check what they did before leaving the virtual apartment. Anxiety and presence (i.e., the feeling of being there in the virtual environment) were assessed with questionnaires. The results were promising and showed that participants suffering from OCD reported significantly higher levels of anxiety than the controls, and the anxiety level reported was positively correlated with the symptoms score and immersion tendencies. The study hints at the value of VR as a tool for inducing anxiety and, accordingly, supports its usefulness as an exposure medium during CBT.
As mentioned earlier, OCD symptoms and avoidance behaviors are heterogeneous (McKay et al., 2004), such as patients predominantly concerned by contamination and washing, checking and verifying, or hoarding. Subtyping OCD symptoms does not necessarily imply the need to develop different theoretical models and treatments for each subtype (McKay et al., 2004; Radomsky and Taylor, 2005), but is very important in terms of clarifying which stimuli will be targeted when using exposure in psychotherapy. Indeed, in order to use VR with success in the context of CBT with exposure and response prevention, virtual environments with subtype-specific triggers must be designed. To the best of our knowledge, no study has taken a look at VR’s inductive potential in connection with contamination-subtype OCD. Researchers have already begun scripting some virtual environments, but these still need to be validated. For example, Cardenas-Lopez et al. (2010) created and are testing virtual environments for the treatment of OCD, developed with the goal of targeting obsessional fears, such as contamination, disorder, and symmetry with VR scenarios that include a public restroom, a bus, and a restaurant.
The study from Kim et al. (2008) paved the way for the current study, although the current project’s differs somewhat from Kim et al. (2008). First, we will be examining the effectiveness of inducing anxiety in a different subtype of OCD (i.e., contamination obsession and cleaning compulsion, rather than checking). Second, we will assess anxiety levels using an objective physiological measure. Third, the participants will be immersed in a virtual environment using a CAVE-like system instead of using head-mounted display.
The primary goal of this research was to assess how effectively a virtual environment could induce anxiety in individuals with contamination-subtype OCD. A large interaction effect was expected (0.40 Cohen’s f or 0.80 d), and two measures were used, one physiological and one subjective. The hypothesis postulated was that exposure to a “contaminated” virtual environment would induce a higher level of anxiety in people suffering from contamination-subtype OCD than in those from the control group, controlling for potential baseline differences.
Once we obtained the approval of the ethics committees of the universities involved in the project, participants were recruited through ads targeting the general population and others posted in hospitals and local community service centers to establish a representative sample of individuals with OCD.
In total, 32 adults between the ages of 18 and 65 years were recruited, including 12 participants with OCD and 20 participants with no mental health disorder. A short telephone interview was conducted before the first meeting to assess whether or not the symptoms of the OCD participants were consistent with those of the contamination subtype. The following exclusion criteria were applied to those individuals with OCD: (a) a primary diagnosis other than OCD; (b) a primary OCD subtype other than contamination; and (c) OCD duration of less than 12 months, to ensure a chronic disorder. The following exclusion criteria applied to both the OCD participants and the non-OCD control participants: (d) a secondary diagnosis of schizophrenia, bipolar disorder, neurobiological disorders, intellectual disability, substance abuse or addiction, or suicidal ideation; and (e) presence of a physical condition contraindicating participation in the study (e.g., epilepsy, visual disorders).
Upon arrival, participants were asked to read and sign the consent form and fill out a short sociodemographic questionnaire (assessing age, gender, socioeconomic status). After providing written consent, the participants were interviewed with semi-structured diagnostic interviews to confirm the presence or absence of OCD and assess for other comorbid disorders as defined in the DSM-IV-TR (American Psychiatric Association, 2000) and DSM-5 (American Psychiatric Association, 2013). The interviews were conducted by three trained therapists and supervised by a licensed psychologist. The participants then filled out other questionnaires (described in the following section) to quantitatively assess OCD and were assigned to either the clinical (OCD) or the control group (non-OCD), depending on the symptoms they presented.
The experimentation was carried out by three research assistants with experience in using VR, the equipment and in conducting CBT. The experiment lasted about 120 min. Prior to each immersion, the participants were outfitted with 3D glasses, an inertial tracking sensor held in the dominant hand, and headphones. Participants were immersed twice in VR and each immersion lasted about 5 min (the exact duration varied slightly depending on participants’ ability to explore the VE and reluctance to approach feared stimuli). The immersions were conducted with two different virtual environments: (a) a training virtual environment (Control) and (b) a virtual environment depicting a filthy public restroom (Contaminated). The first environment was used to familiarize participants with the technology and moving around in the virtual environment. The second environment was used to induce anxiety in participants going through the restroom with various degrees of cleanliness (i.e., the first stall is relatively clean, the second presents filthy walls and toilet seat, and the third adds more filth with an unflushed toilet). Participants were asked to progressively visit each restroom stall, and “touch” the walls and the toilet seat each time with their hands (no touch feedback was provided). The verbal instructions were standardized and similar for each participant. After each immersion, participants were asked to complete a self-assessment of their anxiety level and virtual experience.
Structured Clinical Interview for DSM-IV
This semi-structured diagnostic interview was used to confirm the presence or absence of OCD or a disorder included in the exclusion criteria (First et al., 1997). This tool is recognized for determining the presence of diagnoses established by the DSM-IV (American Psychiatric Association, 2000). For example, with previous versions of the tool, the interrater agreement for OCD ranges in terms of kappa value from average to very high (1.00) (Williams et al., 1992; Steketee et al., 1996). Individuals classified as control were also assessed using the structured clinical interview for DSM-IV (SCID) to make sure they did not present OCD or any of the disorders included in the exclusion criteria.
Yale–Brown Obsessive–Compulsive Scale
The semi-structured Yale–Brown Obsessive–Compulsive Scale (YBOCS) interview helps to provide a more detailed measure of the frequency, severity, and variety of OCD symptoms (Goodman et al., 1989a,b). For this study, the French–Canadian version of this tool was used (Mollard et al., 1989). In validation studies, this version of the tool scored well for internal consistency (Cronbach’s alpha of 0.89–0.96) and fidelity (correlations between the total score and each of the 10 items vary between 0.80 and 0.98) (Bouvard et al., 1992; Ladouceur et al., 1996). Generally, studies call for a total score of 16 or higher as a criterion for inclusion (Shear et al., 2000), which was the threshold used for this study.
State-Trait Anxiety Inventory, State Anxiety Subscale
This measure examines the subjective symptoms of anxiety and serves as the main subjective indicator for the presence of anxiety following immersion in the virtual environment (Spielberger et al., 1970). The first subscale focuses on situational anxiety (i.e., the level of anxiety experienced when completing the questionnaire). The French-language version presents psychometric qualities similar to those of the State-Trait Anxiety Inventory (STAI) (Gauthier and Bouchard, 1993). The questionnaire’s internal consistency was established for a French-speaking Canadian population with a Cronbach’s alpha of 0.90 on the situational anxiety scale and 0.91 on the anxiety trait scale. It was administered before the immersions (pre-experiment) and after each immersion in VR.
Before and after each virtual immersion, the participants were asked to fill out a questionnaire related to their experience in VR. A French version of each measurement tool was translated and validated by a team from the Laboratoire de Cyberpsychologie de l’UQO.
Immersive Tendencies Questionnaire
This tool helps measure a participant’s susceptibility to feel strongly immersed in a virtual environment by evaluating this susceptibility with other activities (e.g., reading a book, watching a movie) (Witmer and Singer, 1998). This questionnaire was translated in French and has a Cronbach’s alpha of 0.83 (N = 483).
Gatineau Presence Questionnaire
This questionnaire measures the feeling of presence experienced in a virtual environment. It has been developed as a brief measure with four items rated on a 0–100 scale assessing: (#1) the impression of being there, (#2) appraising the experience as being real, (#3) awareness of the virtual environment as being artificial, and (#4) the feeling of being in the physical office instead of the virtual environment. The last two items are scored in reverse and an average score in percentage is computed. The Cronbach’s alpha for this instrument is 0.69 (N = 84, mean age 33.5, 76% females) and a factorial analysis with Promax rotation revealed a two-factor solution explaining 82% of variance with positively and negatively scored items leading on distinct factors (being present/being absent). The immersive tendencies questionnaire (ITQ) and Gatineau Presence Questionnaire (GPQ) correlated significantly (r = 0.26, p < 0.01).
Simulator Sickness Questionnaire
This questionnaire measures unwanted negative side effects induced by immersions in VR (e.g., nausea, eye fatigue, and dizziness) (Kennedy et al., 1993). The revised French-language version of this questionnaire has an alpha of 0.87 (N = 371) (Bouchard et al., 2007a, 2011). The Simulator Sickness Questionnaire (SSQ) was administered upon arrival in the lab and after both immersions, and scored following the procedures recommended by Kennedy et al. (1993).
Heart rate was used as an objective measure of anxiety using an electrocardiogram (ECG). To measure the heart rate, we installed a Polar® T31 heart rate transmitter belt coded to a 256 Hz frequency, worn under clothing, just below the chest. The ECG sensors were connected to a ProComp Infinity and the computer using a wireless Tele-Infiniti Compact Flash T9600 interface. The standard measurement error for this measure is calculated at 2.26.
A baseline was taken at rest, before completing the questionnaires to provide a physiological reference for each participant. Physiological data were recorded over the entire duration of the experiment, starting with the baseline, throughout completion of the questionnaires and the immersions, and finishing after the immersion in the “contaminated” virtual environment.
The experiment took place in a six-sided wireless immersion chamber (CAVE-like), called Psyche, located at the Laboratoire de Cyberpsychologie de l’Université du Québec en Outaouais, Gatineau, QC, Canada (Figure 1). This VR immersion system is made of six projected surfaces: four walls, the floor, and the ceiling. The back wall is mounted on rails and can be closed once the participant is inside the cube. Each wall measures 8.6′ and receives images from a Viztek 1 projector (modified from Electrohome Marquee 8500) located 15 ft away. Each CRT projector projects 225 ANSI lumens in 1280 × 1024 @ 100 Hz resolution, providing a seamless active stereoscopic display. Psyche is operated with a wireless keyboard through a cluster of six computers controlled by a master computer, all running Virtool VPPublisher Unlimited 5.0 and built with the following specifications: Intel® Core 2 Quad Q6600@2.40GHz with 4 GB of RAM, NVidia® Quadro FX 5500G frame-locked graphics card with 1024 MB of VRAM, an Intel® D975XBX2 motherboard, and Windows® XP Pro 32 Bit Service Pack 2. The library uses OpenGL 2.0 Stereo. The master computer also has a Creative® SoundBlaster X-Fi sound card. The computer cluster includes one more computer to link the IS-900 VET Intersense® wireless inertial tracking sensor with the virtual environment on VRPN 7.18 using a Pentium 4 3.20 GHz CPU with 512 MB of RAM. All of the computers are linked in a cluster by a Cysco® Systems Catalyst 2950 100MBITs/s switch.
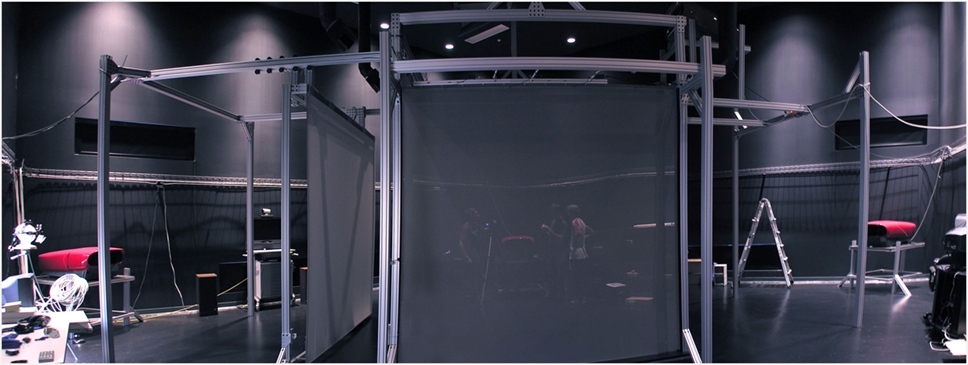
Figure 1. Psyche, the six-wall immersion chamber at UQO’s Cyberpsychology Lab (Gatineau, QC, Canada).
Users wore wireless 3D glasses (NuVision®), wireless headphones, and a wireless microphone. Participants could navigate through the virtual environments using the Intersense wireless hand-held device (“wand”). The experimenter controlled Psyche and the computer used to process physiological measurement from outside the chamber (i.e., the user was alone in the enclosed cube).
As mentioned earlier, two virtual environments were used: a training environment (Control) and an experimental environment (Contaminated). The training environment consisted of a clean empty room with three windows, a glass door, and a cat on a table behind the glass door. Users could hear the relaxing sounds of a gentle breeze and birds chirping through the window. The goal of this environment was to (a) help participants familiarize themselves with immersion in Psyche and (b) take base physiological readings to control for the effect of being immersed in a virtual environment. The experimental environment represented a filthy public restroom (Figures 2 and 3). The restroom represented a very unclean environment (e.g., toilet used but not flushed, graffiti on the walls, and water around a leaking faucet and on the floor), although some areas were cleaner than others. The restroom contained nothing that could be used to clean or eliminate germs (e.g., cleaning products, soap, hands sanitizer). Participants could hear ambient sounds in the restroom (e.g., water pipes, air conditioning). This environment was created to align the VR exposure with the specific obsessions and compulsions of people who suffer from the contamination-subtype OCD. Trained technicians from the Laboratoire de Cyberpsychologie de l’UQO designed the virtual environments using Virtools and 3D StudioMax® [see Wiederhold and Bouchard (2014) for more details].

Figure 2. Screenshot of the women’s restroom in the “contaminated” virtual environment.

Figure 3. Two toilet stalls featuring different levels of dirtiness in the “contaminated” virtual environment.
This study applied a repeated-measure covariance analyses1 (with the baseline score as a covariable) with two Groups (OCD/non-OCD) × two Environments (Control and Contaminated) to test the effectiveness of the virtual environment in inducing anxiety in OCD individuals with a dominant contamination subtype. Chi-square analyses and a Student’s t-test were performed on the descriptive variables (e.g., gender, nationality, schooling, marital status) to determine whether there were any pre-existing differences between the groups before the experiment. The analyses revealed no significant difference. As can be seen in Table 1, most of the participants were Canadian-born women with university-level education. As for marital status, most of the participants were single or in a common-law relationship. The average YBOCS for the OCD group was 25.04 (SD = 6.31), representing an average score that falls within the “severe” end of the scale.
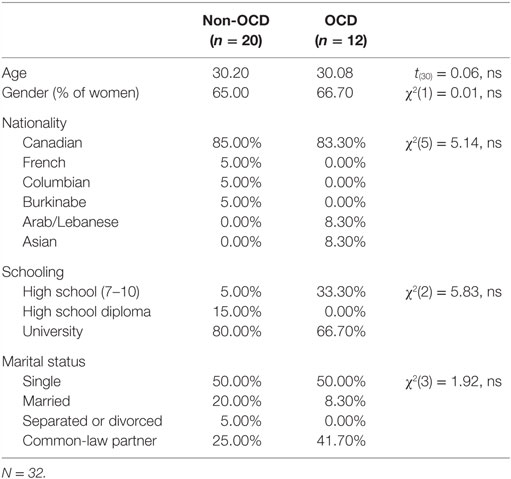
Table 1. Description of the sociodemographic variables of the sample.
The questionnaires on the participants’ VR experience showed that propensity for immersion did not differ between the two groups (see Table 2). The feeling of presence did not differ between OCD and non-OCD participants, regardless of the virtual environment (and for both factors of the GPQ, data not shown). A repeated-measure ANOVA revealed a significant increase in presence in the “contaminated” environment immersion [F(1,29) = 9.13, p < 0.01] and no significant statistical interaction [F(1,29) = 0.9, ns]. Correlating presence with the mean STAI scores showed a positive and significant relationship within the OCD group (r(12) = 0.67, p < 0.05) after the immersion in the “contaminated” environment. However, the correlation was not significant for the non-OCD group (r(20) = 0.15, ns) or for either group following the immersion in the control environment (OCD: r(12) = 0.20, ns; non-OCD: r(20) = −0.23, ns). Finally, the negative unwanted side effects were significantly higher for participants in the OCD group (see Table 2), both prior the experiment and following immersion in the “contaminated” environment. Comparisons for each subscale of the SSQ provided similar results (data not shown).
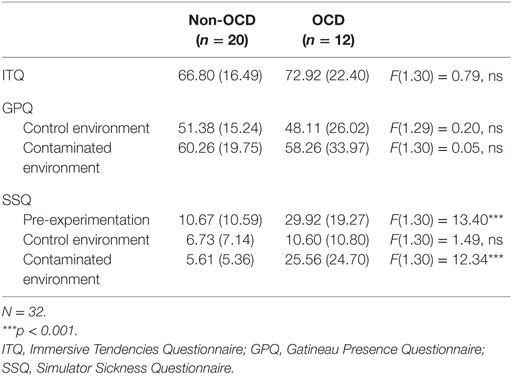
Table 2. Results of questionnaires associated with the virtual reality experience.
The repeated-measure covariance analyses were performed on the two dependent variables (i.e., the STAI situational anxiety scale and mean heart rate). As a preliminary step, the data were examined to make sure the parametric analyses were aligned with the required postulates. The Shapiro–Wilk omnibus test of normality highlighted a few significant indicators (STAI score following neutral immersion for the control and experimental group) pointing to a data distribution that did not quite line up with the normal curve. In these cases, the Shapiro–Wilk indicator was elevated as a result of a few extreme values. Eliminating these extreme numbers corrected the problem detected by the Shapiro–Wilk test, but this in no way affected the materiality of the results. Furthermore, given the low number of participants and the strength of the repeated-measures ANCOVAs, we felt it would be better to proceed with the parametric analyses without eliminating those few, more extreme values. Parametric analyses were applied to the STAI, even though the data came from a Likert scale, given the simulations documenting the strength of this type of analysis when used with ordinal data (Velleman and Wilkinson, 1993; Davidson and Sharma, 1994; Stiger et al., 1998; Carifio and Perla, 2008; Norman, 2010). The homogeneity postulates for the regression slopes were respected [F(1.28) = 1.03 for heart rate, 1.23 for the STAI, all ns]. The Greenhouse–Geisser correction was systematically applied to the repeated-measures ANCOVAs to counter issues with the heterogeneity of variance and, to correct for Type I errors, a Bonferroni adjustment was applied (i.e., critical alpha set a 0.025).
First, the results point to a statistically significant Condition by Time interaction for the heart rate (see Table 3). OCD participants presented a higher heart rate following immersion in the “contaminated” restroom environment compared to the heart rate reported for the control group. This difference remained statistically significant even after the Bonferroni adjustment was applied for the significance threshold. Figure 4 illustrates the results of this interaction. Loftus and Masson’s method (Loftus and Masson, 1994) was used to calculate the confidence intervals in the case of repeated measurements. The interaction proved statistically significant. Breaking down the interaction using Dunn’s procedure revealed that the only significant single effect is the pre/post-immersion effect on the OCD participants [t(11) = −3.06, p < 0.025, 95% confidence interval between −26.21 and −4.29].
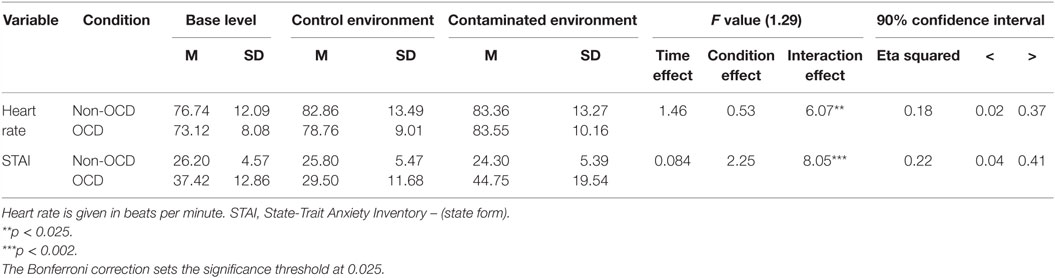
Table 3. Results following ANCOVAs on the dependent variables.
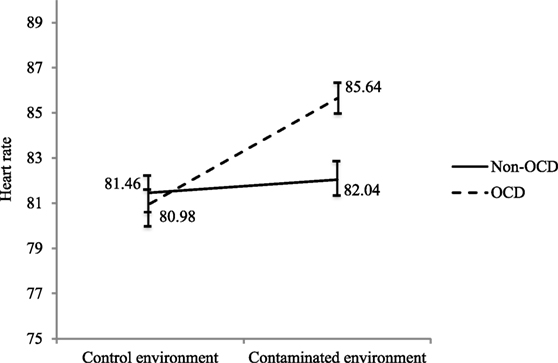
Figure 4. Estimated marginal means after controlling for base levels and 95% confidence intervals of the measured heart rate in both virtual environments for the OCD and non-OCD groups.
Second, and similar to the results for the heart rate, the ANCOVA for the state anxiety measure with a Bonferroni adjustment shows a statistically significant interaction between the Control environment and Contaminated environment, which confirms that the OCD participants felt a subjectively higher level of anxiety following immersion in the virtual restroom than those in the control group. Figure 5 illustrates this interaction, which remains statistically significant when using confidence intervals. The breakdown of the interaction using Dunn’s procedure revealed two significant effects: the pre/post-immersion effect on the OCD participants [t(11) = −3.38, p < 0.025, 95% confidence interval between −7.91 and −1.67], and the post-immersion comparison between the two groups [t(30) = −3.55, p < 0.025, 95% confidence interval between −3.02 and −7.88].
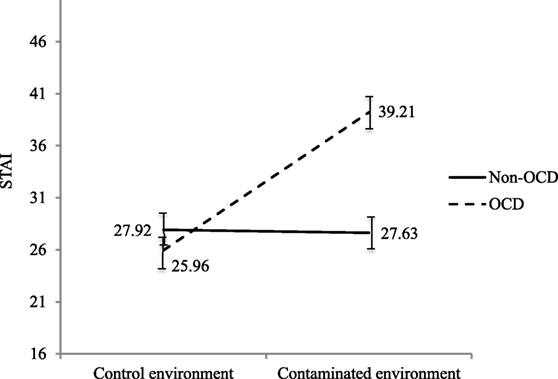
Figure 5. Estimated marginal means after controlling for base levels and 95% confidence intervals of the STAI after immersions in both virtual environments for the OCD and non-OCD groups.
The goal of this study was to determine the potential for a virtual environment to induce an anxiety response in individuals suffering from a contamination obsession/cleaning compulsion-subtype OCD. It was hypothesized that individuals suffering from OCD with dominant fears of contaminations would be more anxious than non-OCD controls when immersed in a disgusting public restroom. The anxiety reported by the participants was studied following immersion in a neutral environment and in a “contaminated” environment. The results confirmed our hypothesis: exposure to a “contaminated” virtual environment induced a higher anxiety level in the OCD group compared to the control group, demonstrated by objective (heart rate) and subjective (state anxiety measured with the STAI) measures. These results are consistent with previous studies (Meehan, 2001; Moore et al., 2002; Robillard et al., 2003; Kim et al., 2008), which contributes to validating the impact of immersion in virtual environments created for OCD.
When establishing the methodology, heart rate was selected as the main measure of anxiety because it is more objective than self-reports. Note that the methodology did not control for individual differences that can alter physiological responses, such as weight, health status, smoking, etc. Nevertheless, this corroborates the results of other studies using objective measures (Côté and Bouchard, 2005; Simeonov et al., 2005; Slater et al., 2006). The subjective anxiogenic response in OCD individuals was also significantly higher, with a mean difference of about 29 points on the STAI. The effect size of the interaction was greater than for the heart rate, as also confirmed by examining the confidence intervals. Note that the aim of the study was not to maximize the level of anxiety felt – in other words, to induce a panic response in participants – but simply to show the potential for increasing the level of anxiety felt from one immersion to the other. Stated otherwise, the goal of the study was not to show how frightening the environment could be, but rather to show that it does elicit the expected emotional response required to use it in psychotherapy.
A few words must be devoted to variance observed in the data. This variance is evident in the large size of the SDs, the explained variance percentage, and the extent of the confidence intervals. There may be various reasons for this. First, because the study was conducted using a clinical sample, differences in sensitivity to stimuli are to be expected. For example, although all OCD participants manifested a fear of contamination, they varied on other characteristics that may have tainted their responses, including broad clinical features of OCD (e.g., inflated responsibility or perfectionism), and differences in feared contaminants (e.g., some were more concerned about food than restrooms). Because it is a tedious process to create virtual environments that target the specific fears of all participants, differing responses between patients are to be expected with generic scenarios. It is also important to recognize that even in the control population, touching a toilet bowl in a filthy restroom is likely to cause some discomfort. That means that there is a good chance that the results for the control participants will vary from person to person. From the methodological point of view of purely experimental research, it might have been worthwhile to recruit control participants with zero concerns regarding restroom cleanliness and OCD participants with only fears of restroom-related contaminations. However, this might have biased the results in favor of the hypotheses (i.e., increase the likelihood of finding significant differences) and lowered the potential for the generalization of results to clinical research and settings. Of note, the correlation between the level of presence and self-reported anxiety in the OCD group accounted for about 45% of the variance.
The lack of significant difference in presence among the two groups is worth further examination, as this runs counter to studies that report a higher degree of presence in clinical samples compared to control groups. For example, Robillard et al. (2003) showed that participants suffering from snake phobia reported a greater sense of presence compared to the non-phobic group following immersion in a virtual environment. It may be that presence was more disrupted in OCD participants than in controls because OCD participants were more distracted by not feeling the virtual walls when touching them. In Robillard et al. (2003), the researchers reported a significant correlation between anxiety and presence. Other studies highlighted the bidirectionality of this correlation (Michaud et al., 2004; Riva et al., 2007), illustrating that not only could the level of anxiety reported predict the degree of presence, but that the sense of presence could predict the level of anxiety experienced. Here, despite recording a lower average presence than the control group, the OCD individuals still reported a higher level of anxiety than the controls following immersion in the filthy environment. This brings into question the importance of the extent of presence when attempting to induce an emotion using VR. It is possible that our results show that a certain minimum level of presence is necessary to induce an anxiety response, but once this level has been reached, the extent of the feeling of presence will have little influence over the emotional response [i.e., a non-linear relationship (Bouchard et al., 2012)]. It is accordingly possible that our results support the idea that quality is more important than quantity when it comes to users’ sense of presence in a virtual environment (Bouchard et al., 2007b). The role of presence in the development of clinical applications of VR for anxiety disorders also deserves a brief mention. As it is the case for the therapeutic alliance in the CBT of anxiety disorders, feeling present may be a prerequisite yet a poor predictor of treatment outcome. Further research is needed to document whether presence allows for, or is associated with, virtual stimuli to be perceived and processed as real, which then leads to the core process associated with treatment success, namely “developing new associations with lack of threat” (Bouchard et al., 2012; Craske et al., 2014).
Finally, there was a significantly higher instance of unwanted negative side effects induced by immersions in VR in the OCD group before the first immersion and following immersion in the “contaminated” environment, while there was no significant difference between the two groups following immersion in the control environment. These results were also replicated for all three SSQ subscales. It is possible that the anxiety felt by the OCD group before the experiment, likely induced by apprehension, caused symptoms similar to cybersickness (e.g., nausea, difficulty concentrating). In this regard, Bouchard et al. (2007a, 2011) questioned the use of the SSQ with anxious participants. In a series of studies, they (Bouchard et al., 2011) examined the correlation between cybersickness symptoms and anxiety levels and found that SSQ items associated with nausea (general discomfort, increased salivation, perspiration) and oculomotor function (difficulty focusing, difficulty concentrating) significantly correlated with the anxiety levels reported by participants, both following immersion in VR and in situation where no immersions in VR were involved. These results support those of the current study as well as the possibility that the phenomenon observed will be repeated in subsequent studies. As for the results following immersion in the “contaminated” environment, it is possible that the environment itself triggered a physical response comparable to cybersickness (e.g., general discomfort, nausea) which would explain the higher rating for these items. In other words, it is plausible that participants had trouble differentiating between some of the physical symptoms they felt and actual cybersickness when they filled out the SSQ.
One might think that the feeling of being contaminated would cause the person to want to “decontaminate” themselves, especially in the case of OCD individuals, who view contamination as a major threat. To be rigorous, it is important to also mention that the experimental environment did not display any actual germ, microbes, or explicit mention that the restroom was contaminated. With this in mind, and with the goal of observing the compulsive rituals of the OCD group, participants were asked to complete a qualitative questionnaire post-immersion. The results suggest that the OCD participants reported a greater need to wash their feet and needed to wash their hands and feet more thoroughly following immersion compared to the control group. They also revealed that the “contaminated” virtual environment succeeded in triggering cleaning compulsions in the OCD group. These observations deserve to be studied more rigorously.
To the best of our knowledge, this study is the first to validate a virtual environment created specifically to induce an anxiety response in contamination-subtype OCD patients. As mentioned earlier, the only set of studies to have examined the inductive potential of VR for OCD was conducted with respect to the checking subtype, with promising results that were expanded in a few studies (Kim et al., 2012). As things stand, the research shows that the anxiety-inducing potential of VR immersion has been assessed in other clinical populations, and its capacity to trigger an anxiety response has been repeatedly and reliably documented (Wiederhold and Bouchard, 2014). To date, most studies have focused on simpler anxiety disorders, such as specific phobias. Among others, the study lead by Robillard et al. (2003) using a sample of phobic (suffering from claustrophobia, acrophobia, and arachnophobia) and non-phobic individuals demonstrated the capacity to trigger a significantly greater subjective anxiety response in phobics compared to the control group, using a virtual environment created using a video game editor. Behaviorally, Renaud et al. (2002) detected considerably more pronounced patterns of avoidance in arachnophobic participants compared to the control group when confronted with a virtual spider.
In addition to the subjective and behavioral measures of anxiety, studies have shown the inductive potential of environments using physiological measurements. Among others, Moore et al. (2002) showed significant changes in heart rate and electrical conductance following immersion in a potentially anxiogenic environment (e.g., elevator, grocery store with avatars) in a sample of non-phobic individuals. Similarly, Diemer et al. (2014) documented major and significant changes in heart rate and other psychophysiological parameters when phobic and non-phobic participants were immersed in VR. In short, these results are congruent with ours and confirm that a virtual environment is capable of inducing an anxiety response in people suffering from anxiety disorders and OCD. The next studies should be pilot [e.g., Laforest et al. (2016)] and larger scale control trials to design and test treatment programs using this virtual environment.
As for the limitations of this study, the first would the sample size. Given the low prevalence of contamination-subtype OCD, and the fact that we sought to engage Francophones, recruitment proved difficult. It would be worthwhile to reproduce this study with a larger sample to obtain more representative and generalizable results. Furthermore, the variability of the results obtained, as manifested by the size of the confidence intervals, could be lessened through greater control over individual differences between the participants in the sample and even more anxiogenic experimental manipulation.
Immersing people suffering from fears of contamination as severe as to meet the diagnostic criteria of OCD can be immersed in VR and feel the emotions CBT therapists expect from stimuli used to conducted exposure-based therapy. The next steps involve conducting pilot and large control outcome trial, address the use of VR with other OCD subtypes (e.g., religious/moral obsessions, aggressive obsessions, symmetry/order obsessions) and with other populations (e.g., children, adolescents, elders). Finally, the addition of more interfaces (e.g., smell, touch, taste) combined with the three-dimensional view should be part of future studies on this topic. In fact, several individuals who took part in this study (control and OCD) anecdotally suggested that adding smell or touch interfaces would make the scenario used feel even more real.
This study is part of the doctoral thesis of ML, Ph.D. SB was the thesis supervisor. They both conceptualized the study. ML did the recruitment and treatment. A-MC and OM were involved in conceptual decisions leading to the final version of this document.
The second author holds share in Clinique et Developpement In Virtuo.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors wish to thank Tanya Guitard and Geneviève Robillard for their contribution in conducting this study.
The study was funded by grants from the Canada Research Chair program awarded to the second author and was conducted at the Laboratoire de Cyberpsychologie de l’UQO (http://w3.uqo.ca/cyberpsy), where the first author completed her Ph.D. research.
American Psychiatric Association. (2000). Diagnostic and Statistical Manual of Mental Disorders, 4th Edn. Washington, DC: American Psychiatric Association.
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders, 5th Edn. Washington, DC: American Psychiatric Association.
Ball, S. G., Baer, L., and Otto, M. W. (1996). Symptom subtypes of obsessive-compulsive disorder in behavioural treatment studies: a quantitative review. Behav. Res. Ther. 34, 47–51.
Bouchard, S., Robillard, G., Larouche, S., and Loranger, C. (2012). “Description of a treatment manual for in virtuo exposure with specific phobia,” in Virtual Reality in Psychological, Medical and Pedagogical Applications, ed. C. Eichenberg (Rijeka, Croatia: InTech), 82–108.
Bouchard, S., Robillard, G., and Renaud, P. (2007a). Revising the factor structure of the simulator sickness questionnaire. Annu. Rev. Cyber. Ther. Telemed. 5, 117–122.
Bouchard, S., Côté, S., and Richards, D. S. (2007b). “Virtual reality application for exposure,” in Handbook of Exposure Therapies, eds D. S. Richards and D. Lauterbach (New York: Academic Press), 347–388.
Bouchard, S., Robillard, G., Renaud, P., and Bernier, F. (2011). Exploring new dimensions in the assessment of virtual reality induced side-effects. J. Comput. Inf. Technol. 1, 20–32.
Bouvard, M., Sauteraud, A., Note, I., Bourgeois, M., Dirson, S., and Cottraux, J. (1992). Étude de validation et analyse factorielle de la version française de l’échelle d’obsession compulsion de Yale-Brown. J. Ther. Comportement. Cogn. 2, 18–22.
Cardenas-Lopez, G., Munoz, S., and Oviedo, P. (2010). “Clinical virtual environments for OCD treatment,” in Journal of Cybertherapy and Rehabilitation, Abstracts from the 15th Annual Cyberpsychology and Cybertherapy Conference (Seoul).
Carifio, J., and Perla, R. (2008). Resolving the 50-year debate around using and misusing Likert scales. Med. Educ. 42, 1150–1152. doi: 10.1111/j.1365-2923.2008.03172.x
Côté, S., and Bouchard, S. (2005). Documenting the efficacy of virtual reality exposure with psychophysiological and information processing measures. Appl. Psychophysiol. Biofeedback 30, 217–232. doi:10.1007/s10484-005-6379-x
Craske, M., Treanor, M., Conway, C. C., Zbozinek, T., and Vervliet, B. (2014). Maximizing exposure therapy: an inhibitory learning approach. Behav. Res. Ther. 58, 10–23. doi:10.1016/j.brat.2014.04.006
Cronbach, L. J., and Furby, L. (1970). How we should measure “change” – or should we? Psychol. Bull. 74, 68–80. doi:10.1037/h0029382
Davidson, M. L., and Sharma, A. R. (1994). ANOVA and ANCOVA of pre- and post-test, ordinal data. Psychometrika 59, 593–600. doi:10.1007/BF02294394
Diemer, J., Mühlberger, A., Pauli, P., and Zwanger, P. (2014). Virtual reality exposure in anxiety disorders: impact on psychophysiological reactivity. World J. Biol. Psychiatry 15, 427–442. doi:10.3109/15622975.2014.892632
Fals-Stewart, W., Marks, A. P., and Schafer, J. (1993). A comparison of behavioral group therapy and individual behavior therapy in treating obsessive-compulsive disorder. J. Nerv. Ment. Dis. 181, 189–193. doi:10.1097/00005053-199303000-00007
First, M. B., Spitzer, R. L., Gibbon, M., and Williams, J. B. W. (1997). Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-I). Washington, DC: American Psychological Association.
Fuch, P., Moreau, G., and Guitton, P. (2011). Virtual Reality: Concepts and Technologies. New York: CRC Press.
Gauthier, J., and Bouchard, S. (1993). Adaptation canadienne-française de la forme révisée du State-Trait Anxiety Inventory de Spielberger. Can. J. Behav. Sci. 25, 559–578. doi:10.1037/h0078881
Goodman, W. K., Price, L. H., Rasmussen, S. A., Mazure, C., Delgado, P., Heninger, G. R., et al. (1989a). The Yale-Brown obsessive-compulsive scale II. Validity. Arch. Gen. Psychiatry 46, 1012–1016. doi:10.1001/archpsyc.1989.01810110054008
Goodman, W. K., Price, L. H., Rasmussen, S. A., Mazure, C., Fleishmann, R. L., Hill, C. L., et al. (1989b). The Yale-Brown obsessive-compulsive scale I. Development, use, and reliability. Arch. Gen. Psychiatry 46, 1006–1011. doi:10.1001/archpsyc.1989.01810110048007
Huck, S. W., and McLean, R. A. (1975). Using a repeated measures ANOVA to analyze the data from a pretest-posttest design: a potentially confusing task. Psychol. Bull. 82, 511–518. doi:10.1037/h0076767
Kennedy, R. S., Lane, N. E., Berbaum, K. S., and Lilienthal, M. G. (1993). Simulator sickness questionnaire: an enhanced method for quantifying simulator sickness. Int. J. Aviat. Psychol. 3, 203–220. doi:10.1207/s15327108ijap0303_3
Kim, K., Kim, C.-H., Cha, K. R., Park, J., Han, K., Kim, Y. K., et al. (2008). Anxiety provocation and measurement using virtual reality in patients with obsessive-compulsive disorder. Cyberpsychol. Behav. 11, 637–641. doi:10.1089/cpb.2008.0003
Kim, K., Roh, D., Kim, C.-H., Cha, K. R., Rosenthal, Z., and Kim, S. I. (2012). Comparison of checking behavior in adults with or without checking symptom of obsessive-compulsive disorder using a novel computer-based measure. Comput. Methods Programs Biomed. 108, 434–441. doi:10.1016/j.cmpb.2012.03.014
Kirk, R. E. (1982). Experimental Design: Procedures for the Behavioral Sciences, 2nd Edn. Pacific Grove, CA: Brooks/Cole.
Labonté-Chartrand, G. (2011). Étude portant sur l’évaluation des attitudes, des croyances négatives et des contraintes rencontrées lors du traitement par exposition de personnes souffrant de trouble obsessionnel-compulsif. Essai de Psy. D. Université du Québec à Montréal, Montréal.
Ladouceur, R., Léger, E., Rhéaume, J., and Dubé, D. (1996). Correction of inflated responsibility in the treatment of obsessive-compulsive disorder. Behav. Res. Ther. 34, 767–774. doi:10.1016/0005-7967(96)00042-3
Laforest, M., Bouchard, S., Bossé, J., and Mesly, O. (2016). Effectiveness of in virtuo exposure and response prevention treatment using cognitive-behavioral therapy for obsessive-compulsive disorder: a study based on a single-case study protocol. Front. Psychiatry 7:99. doi:10.3389/fpsyt.2016.00099
Lang, P. J. (1977). Imagery in therapy: an information processing analysis of fear. Behav. Ther. 8, 862–886. doi:10.1016/S0005-7894(77)80157-3
Loftus, G. R., and Masson, M. E. J. (1994). Using confidence intervals in within-subject designs. Psychon. Bull. Rev. 1, 476–490. doi:10.3758/BF03210951
McKay, D., Abramowitz, J. S., Calamari, J. E., Kyrios, M., Radomsky, A., Sookman, D., et al. (2004). A critical evaluation of obsessive-compulsive disorder subtypes: symptoms versus mechanisms. Clin. Psychol. Rev. 24, 283–313. doi:10.1016/j.cpr.2004.04.003
McKay, D., Sookman, D., Neziroglu, F., Wilhelm, S., Stein, D. J., Kyrios, M., et al. (2015). Efficacy of cognitive-behavioral therapy for obsessive-compulsive disorder. Psychiatry Res. 227, 104–113. doi:10.1016/j.psychres.2015.02.004
Meehan, M. (2001). Physiological Reaction as an Objective Measure of Presence in Virtual Environments. Ph.D. Dissertation, University of North Carolina, Chapel Hill.
Meyer, V. (1966). Modification of expectations in cases with obsessional rituals. Behav. Res. Ther. 4, 273–280. doi:10.1016/0005-7967(66)90023-4
Michaud, M., Bouchard, S., Dumoulin, S., and Zhong, X.-W. (2004). “Manipulating presence and its impact on anxiety,” in Poster Presented at Cybertherapy Conference 2004 (San Diego, CA).
Mollard, E., Cottraux, J., and Bouvard, M. (1989). Version française de l’échelle d’obsessions-compulsions de Yale-Brown. LEncéphale XV, 335–341.
Moore, K., Wiederhold, B. K., Wiederhold, M. D., and Riva, G. (2002). Panic and agoraphobia in a virtual world. Cyberpsychol. Behav. 5, 197–202. doi:10.1089/109493102760147178
Moritz, S., Rufer, M., Fricke, S., Karow, A., Morfeld, M., Jelinek, L., et al. (2005). Quality of life in obsessive-compulsive disorder before and after treatment. Compr. Psychiatry 46, 453–459. doi:10.1016/j.comppsych.2005.04.002
Norman, G. (2010). Likert scales, levels of measurement and the “laws” of statistics. Adv. Health Sci. Educ. Theory Pract. 15, 625–632. doi:10.1007/s10459-010-9222-y
Radomsky, A. S., and Taylor, S. (2005). Subtyping OCD: prospects and problems. Behav. Ther. 36, 371–379. doi:10.1016/S0005-7894(05)80119-4
Renaud, P., Bouchard, S., and Proulx, R. (2002). Behavioral dynamics in the presence of a virtual spider. IEEE Trans. Inf. Technol. Biomed. 6, 235–243. doi:10.1109/TITB.2002.802381
Riva, G., Mantovani, F., Capideville, C. M., Preziosa, A., Morganti, F., Villani, D., et al. (2007). Affective interactions using virtual reality: the link between presence and emotions. Cyberpsychol. Behav. 10, 45–56. doi:10.1089/cpb.2006.9993
Robillard, G., Bouchard, S., Fournier, T., and Renaud, P. (2003). Anxiety and presence during VR immersion: a comparative study of the reactions of phobic and non-phobic participants in therapeutic virtual environments derived from computer games. Cyberpsychol. Behav. 6, 467–476. doi:10.1089/109493103769710497
Shear, M. K., Feske, U., Brown, C., Clark, D. B., Mammen, O., and Scotti, J. (2000). “Anxiety disorders measures,” in Handbook of Psychiatric Measures, ed. Task Force for the Handbook of Psychiatric Measures (Washington, DC: American Psychiatric Association), 549–589.
Simeonov, P. I., Hsiao, H., Dotson, B. W., and Ammons, D. E. (2005). Height effects in real and virtual reality. Hum. Factors 47, 430–438. doi:10.1518/0018720054679506
Slater, M., Pertaub, D. P., Barker, C., and Clark, D. (2006). An experimental study on fear of public speaking using a virtual environment. Cyberpsychol. Behav. 9, 627–633. doi:10.1089/cpb.2006.9.627
Spielberger, C. D., Gorusch, R. L., and Lushene, R. E. (1970). Manual of the State-Trait Anxiety Inventory. Palo Alto, CA: Consulting Psychologists Press.
Stankovic, M. (2004). Quelle est la place de l’émotion dans les approches cognitivo-comportementales des troubles obsessionnels-compulsifs? Sante Ment. Que. 29, 105–114. doi:10.7202/008824ar
Steketee, G., Frost, R., and Bogart, K. (1996). The Yale-Brown obsessive-compulsive scale: interview versus self-report. Behav. Res. Ther. 34, 675–684. doi:10.1016/0005-7967(96)00036-8
Stiger, T. R., Kosinski, A. S., Barhart, H. S., and Kleinbaum, D. G. (1998). ANOVA for repeated ordinal data with small sample size? A comparison of ANOVA, MANOVA, WLS and GEE methods by simulation. Commun. Stat. Simul. Comput. 27, 357–375. doi:10.1080/03610919808813485
Van Breukelen, G. J. P. (2006). ANCOVA versus change from baseline had more power in randomized studies and more bias in nonrandomized studies. J. Clin. Epidemiol. 59, 920–925. doi:10.1016/j.jclinepi.2006.02.007
Velleman, P. F., and Wilkinson, L. (1993). Nominal, ordinal, interval, and ratio typologies are misleading. Am. Stat. 47, 65–72. doi:10.1080/00031305.1993.10475938
Wiederhold, B., and Bouchard, S. (2014). Advances in Virtual Reality and Anxiety Disorders. New York: Springer.
Williams, J. B. W., Gibbon, M., First, M. B., Spitzer, R. L., Davies, M., Borus, J., et al. (1992). The Structured Clinical Interview for DSM_III-R (SCID) II. Multisite test-retest reliability. Arch. Gen. Psychiatry 49, 630–636. doi:10.1001/archpsyc.1992.01820080038006
Keywords: virtual reality, OCD, therapeutic tool, exposure therapy, contamination
Citation: Laforest M, Bouchard S, Crétu A-M and Mesly O (2016) Inducing an Anxiety Response Using a Contaminated Virtual Environment: Validation of a Therapeutic Tool for Obsessive–Compulsive Disorder. Front. ICT 3:18. doi: 10.3389/fict.2016.00018
Received: 15 March 2016; Accepted: 22 August 2016;
Published: 05 September 2016
Edited by:
Ryan Patrick McMahan, University of Texas at Dallas, USAReviewed by:
Ferran Argelaguet, French Institute for Research in Computer Science and Automation (INRIA), FranceCopyright: © 2016 Laforest, Bouchard, Crétu and Mesly. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Stéphane Bouchard, c3RlcGhhbmUuYm91Y2hhcmRAdXFvLmNh
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.