 Jinfeng Yang
Jinfeng Yang Junhai Zhou2†
Junhai Zhou2† Chen Liu
Chen Liu Jian Chen
Jian Chen
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Educ., 31 January 2025
Sec. Higher Education
Volume 10 - 2025 | https://doi.org/10.3389/feduc.2025.1461718
Medical humanities are the soul of health education. Humanistic education proposes to improve the conscious and practical activities of educated people and promote their humanity, realize personal and social values, cultivate ideal personalities, and develop a trans-cultural humanistic spirit. The development of higher education has considerably strengthened the integration of scientific and humanistic education in China. This study analyzed the up-to-date teaching situation of medical humanities courses in medical schools considering the following aspects: teachers’ team construction, teaching mode, practical teaching, assessment and evaluation systems, and inadequate platforms. Relevant reforms based on life education were proposed, including improving the integrity of the teaching team, building suitable curriculum system and teaching theory, setting proper evaluation standard for both students and teachers, and providing adequate platforms for practice of humanistic medicine. This study aimed to promote the students’ medical humanities literacy, thus providing potential strategy and reference for improving medical humanistic education.
The reform of medical humanistic education and its curriculum is an important issue in international higher medical education. The educational goal of medical humanities courses is to encourage students to care for life and patients and enhance their sense of responsibility toward the medical profession (Chen et al., 2023). Medical humanities courses are designed by the intersection and integration of medicine, humanities, and social sciences. The development of medical humanities is crucial for promoting the development of a healthy China (Zhao et al., 2023). Psychology, sociology, social medicine, behavioral medicine, ethics, and medical law are core courses in medical humanities (Liou et al., 2016). In physician qualification examinations, medical psychology, law, and ethics are included as mandatory courses, which are assessed as special modules (Chang et al., 2021). This is essential for cultivating students’ humanistic spirit, establishing appropriate values, and improving doctor-patient relationships. Studies have shown that the abundance of medical humanities courses can affect medical students’ humanistic qualities (Centeno et al., 2016). However, problems persist due to the lack of unified standards and coherence in current medical humanities courses, insufficient understanding of trans-cultural humanistic education among medical students, and focus on theoretical teaching over humanistic practice (Rodríguez et al., 2012). Therefore, this study focused on the following aspects: teacher team development, teaching mode, practical teaching, assessment and evaluation systems, platform preparation, and life cherish education, to analyze the problems in teaching medical humanities courses and propose targeted recommendations for establishing these courses and cultivating high-level composite medical talents with an international perspective. This can provide a basis for further studies to deepen the reform of medical education teaching content, teaching evaluation, and curriculum system optimization.
The basic aim of humanistic education is to transmit humanistic qualities via teaching about the significance of life and its meanings through cases (Jung et al., 2016). Humanistic behavior, knowledge, and spirit are united and complementary. Humanistic behavior, which is usually exhibited as social behavior, is the external expression of humanistic knowledge and spirit. It refers to care and reverence for the lives of almost everything. It means to promote the harmonious unity of people with each other, nature, and society, as well as the aspirations of value and meaning (Friedman et al., 2016).
The demand for humanistic-quality education for medical students originated from the United States. Researchers first proposed that the concept of humanistic education should be included in medical education (Rabinowitz, 2021). Since the initial publication of Cultivating Doctors for the 21st Century, American scholars began to demonstrate this idea systemically (Miller, 2004). Around 1980, in the United States, research on the theme of cultivating healthcare workers for the future began to emerge, and research on humanistic quality education for medical students came to the forefront (Miller, 2004). Relevant curriculum reforms appeared, and within 10 years, a relatively systematic medical humanistic education system was established (Wartman, 2019). In 1992, France issued its first macro-guidance document on humanities and social science courses, which has been continuously improved and optimized in practice, giving France a leading background in medical humanistic education in Europe (Boudreau and Fuks, 2015). The demand for humanistic quality education is also common among medical students. In the late 1980s, medical students in Germany called for relevant educational courses to introduce various advanced concepts and innovative practical methods, including medical humanities learning modules (Custers and Cate, 2018). In Belgium, experts in medical education state that talent cultivation and disciplinary development should be equally emphasized. Medicine cannot be regarded as an isolated field; thus, comprehensive education is required (Custers and Cate, 2018).
The first work on humanistic education for medical students by Chinese scholars was published in 1996. Research on humanistic education for medical students went from an initial exploratory stage to gradually taking shape and eventually becoming established (Qian et al., 2018). Medical humanistic education and related curriculum reforms have been increasingly emphasized in China. The General Office of the State Council issued Guiding Opinions on Accelerating the Innovative Development of Medical Education in September 2020 (Liu and Liu, 2024). In the report, they emphasized that a high-level medical talent training system with deep cross-integration of medical science and multiple disciplines will be established by 2025 (Liu and Liu, 2024). Professor Zhang Daqing from Peking University has edited works such as Chinese Medical Humanities Education - History, Current Situation and Prospects and Introduction to Medical Humanities, which comprehensively explore the current situation and curriculum design of medical humanities (Liu and Liu, 2024). In recent years, some domestic universities have established research and teaching institutions for the medical humanities, aiming to cultivate medical students with both medical professional skills and international humanistic spirits (Yi et al., 2024).
Medical schools provide a wide range of medical humanities curricula to undergraduate and graduate students. The core courses are medical ethics, law, and psychology, supplemented by English courses. Medical psychology is an interdisciplinary field that focuses on investigating the roles and patterns of psychological factors in health and disease (Cohen and Herbert, 1996), helping students apply positive psychological interventions and other measures to cope with and adapt to new changes in the medical environment (Cohen and Herbert, 1996). Medical law mainly teaches about legal issues related to new medical technologies, such as building harmonious doctor-patient relationships, handling medical damage, preventive medicine, and human organ transplantation, and explains legal solutions to medical practice problems (Dickinson, 1970). Medical ethics mainly teaches about doctor-patient conflicts, ethical dilemmas in medical behavior choices, and doctor-patient integrity. It can help students comprehensively identify ethical issues in medical practice and research. Medical ethics can also cultivate students’ ethical awareness and decision-making abilities (Caldicott and Danis, 2009). This aims to enable them to deal calmly with thorny ethical issues in medical practice and research. Medical history courses are an interdisciplinary field of medicine and history. Medical students who understand and master the history and laws of medical development can better understand medical science from historical perspectives. By learning and mastering the ideological changes of historical medical figures, they can understand their role and significance in medical development, evaluate their impact on human society, and cultivate a spirit of independent thinking and criticism (Albert et al., 2020). Medical humanistic English has become increasingly prominent due to the increasing internationalization of medical education. It not only helps students master professional English vocabulary in the medical field and improve English communication skills, but also helps students better understand medical concepts and practices in different cultural backgrounds, so as to cultivate medical talents with an international perspective (Daher-Nashif and Kane, 2016).
The practical teaching content and forms of medical humanities courses include early clinical practice, anatomy course humanities practice, medical volunteer service, skill training in medical professional courses, humanities practice in internships, graduation skills assessment and humanities practice exams, social (community health) practice activities, campus medical humanities activities, and medical-related special practice activities (Chen et al., 2023). To enhance students’ medical humanities literacy and strengthen their contact with society and patients, cultivating students’ emotions of caring for patients and life is essential. Accordingly, improving the construction of medical humanities courses has received increasing attention from many universities (Kumagai, 2012). However, certain problems still need to be solved to enhance medical humanistic education.
Currently, most humanities courses in medical schools are performed in traditional classrooms. The main assessment criteria are based on theoretical examinations (Jung et al., 2016; Qian et al., 2018). Although this format helps students acquire systemic humanistic education knowledge effectively, it provides less training on applying what they have learned in real life. This usually leads to a greater emphasis on humanistic knowledge and spirit while ignoring humanistic behavior. Although humanistic education has increased humanistic attitudes, it has not ensured the subsequent change in students’ behavior (Buck et al., 2021; Arnold et al., 1987). Medical students understand the knowledge of humanistic education superficially and are rarely satisfied with it. This has decreased the students’ learning interest and motivation greatly (Macnaughton, 2011; Friedman, 2002).
Most teachers in medical humanities courses have either medical or humanistic educational backgrounds (Isaac, 2023). The knowledge structure of teachers in medical humanities courses tends to lean toward the humanities and social sciences while lacking comprehensive medical knowledge and clinical practice experience with a complete medical professional background (Mangione et al., 2018). Some teachers also lack knowledge systems and practical experience in handling related medical disputes, and most have transitioned from medical, legal, and health management professional backgrounds (Mangione et al., 2018). This leads to difficulties for teachers to explain risk prevention issues in clinical practice (Hakim, 2023; Wang et al., 2023). For example, in terms of the makeup of teaching staff for medical law courses, most domestic law and medical school students are not familiar with legal knowledge in the field of health and even consider it as a marginal discipline (Campbell, 2012; Chen et al., 2022). This subject has not yet developed a complete and independent disciplinary system in China, and there are few degree authorization institutes. Students are unclear about the specific content of their studies and the employers’ prospects (Qian et al., 2018).
Hence, it is crucial to analyze the independent and real participatory experiences of students to solve problems derived from medical humanistic education. This will help students better understand medical humanities and develop medical humanistic education as well (Moyer et al., 2010). Despite a sufficient sense of ethical awareness and morality in Chinese students, the basic humanistic competencies, i.e., compassion, empathy, and communication skills, are still lacking. Therefore, complementary humanistic education is urgently needed. For further development, novel rather than traditional teaching methods must be adopted to improve their effectiveness (Ozair et al., 2021; Brazeau et al., 2011; Carrard et al., 2022).
The curriculum setting is the basis for medical humanistic education. Teaching objectives are guidance of the teaching direction and mode (Swick et al., 1999; Doukas et al., 2022). The teaching objectives of the medical humanities curriculum are to improve clinical medical students’ humanistic literacy, establish appropriate values, and cultivate humanistic sentiments (Isaac, 2023; Howick et al., 2022). However, issues remain exist in the curriculum setting for medical humanities courses. These include a single teaching mode, a shortage of integration and innovation of humanities knowledge with professional medical courses, and insufficient utilization of professional characteristics and advantages (Mitchell and Kan, 2019; Guo, 2022). Compared to high-level universities abroad, there is still room to investigate the diversified, information-based, and flexible classrooms in China (Table 1; Qian et al., 2018). The advantage of the health law course is not significant as the learning content is, which is currently “broad” rather than “deep.” In the limited class time, there is more single-direction indoctrination than bidirectional interaction. Under these conditions, the quality of students’ learning is relatively low. Research has shown that 65% of students are not very satisfied or are dissatisfied with the current situation of medical and legal integration in their study (Woolston, 2022). In a random survey, researchers found that when selecting courses, students care more about obtaining credits than about grasping humanistic concepts (Woolston, 2022).
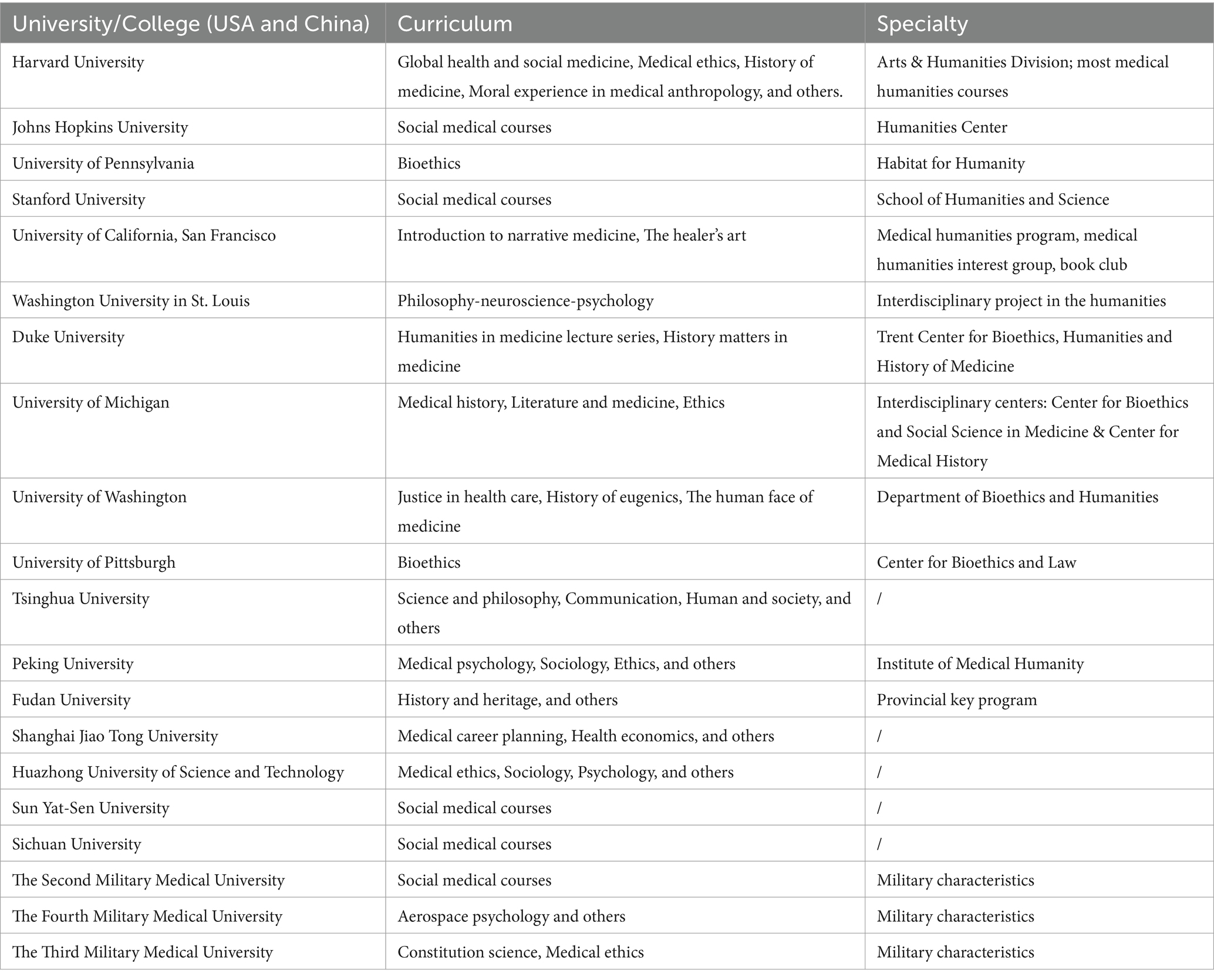
Table 1. Medical humanities courses in top medical colleges in the United States and China.
Furthermore, students and teachers have separate evaluation systems for medical humanities courses. Students’ assessments are mainly composed of regular grades and final exams (Lee et al., 2019; Hoang et al., 2022). The final assessment content is mostly limited to course theory, not including theoretical application ability, humanistic literacy, or humanistic spirit (Hoang et al., 2022; Chen et al., 2023). When evaluating students’ humanistic literacy and spirit, problems arise such as difficulty in formulating assessment standards, strong subjective judgment, and difficult implementation paths. This leads to the phenomenon of “last-minute cramming” and reduces the significance of mastering the curriculum theory. Moreover, questionnaires and other similar forms are usually used to evaluate teachers. However, the evaluation is more important than the form (Chen and Zhang, 2022). Therefore, the authenticity, objectivity, and comprehensiveness of the evaluation content must be studied. In addition, the relevant departments of the school typically do not pay enough attention to the evaluation opinions, resulting in failure to form a closed loop of “evaluation feedback improvement” (Saga et al., 2023; Rubins et al., 2022). This not only hinders the improvement of the quality of medical humanities courses but also affects the long-term development of teachers themselves.
Societies and economic environments create various habits and lifestyles, in which humanities are one product. Humanities often appear following the progression of society and the economy (Costa, 2019). The development of humanistic education follows that of the humanities as well. Therefore, its development lags behind that of the humanities. Moreover, general medical education is derived from multiple clinical tests, whereas humanistic education is entirely different (Wang, 2021). Currently, medicine is undergoing a highly developing phase, whereas the general medical education substance remains static. Therefore, the medical humanistic education progression inevitably falls behind that of humanities (Doukas et al., 2022). Although more attention has been paid to medical humanities by medical education reform, the gap between China and Western countries in the integration of the medical humanities remains substantial (Wang, 2021). This is mainly caused by a lack of independent organization, dis-unified medical humanities courses, and insufficient teaching faculties. Overall, there is an urgent need for well-organized medical humanistic education courses in medical schools (Song and Tang, 2017).
Unlike traditional education, humanistic education contains a variety of content, such as the relationship of individuals with their will and emotions and the relationship between different individuals, society, and nature (Song and Tang, 2017). These contents indicate a person’s theoretical and ideological level, as well as esthetic qualities. Different individuals have various insights regarding the same event; therefore, it is difficult for humanistic education to apply universal answers to the same condition. The value judgment standard based on moral education serves as the value orientation for humanistic education.
An effective medical humanistic education comprises a comprehensive and explicit curriculum system as well as a campus cultural atmosphere influenced by an implicit humanistic spirit. This cultural atmosphere, rich in humanistic values, can subtly steer students toward establishing sound values and enhancing their medical humanities literacy. The integration of explicit and implicit curricula is paramount for medical humanistic education to achieve its intended value and efficacy (Smydra et al., 2022; Pfeiffer et al., 2016).
A survey revealed that students perceived social practice as the most effective means to enhance their medical humanities qualities; however, their satisfaction with the school’s practical teaching platform for medical humanistic education was comparatively low (Li et al., 2022; Huss et al., 2020). Currently, medical humanistic education in universities lacks practical platforms and other supporting resources, which hinders the cultivation of an international humanistic atmosphere in academic institutions and subsequently impacts the students’ position in medical humanistic education (Daher-Nashif and Kane, 2016). A comparative analysis of students’ familiarity with medical humanities courses from various institutions suggests that those from comprehensive colleges have a higher level of familiarity compared to students from independent medical schools (Fanwei et al., 2019). This disparity could be attributed to the comprehensive nature of disciplines, the variety of cultural and sports activities, club-based practical engagements, and interdisciplinary academic lectures offered by comprehensive colleges, all of which contribute to a more robust implicit medical humanistic education atmosphere.
A stable campus humanistic environment necessitates hardware support from dedicated medical humanistic education platforms (Liu and Liu, 2024). The construction of curricula, teacher teams, student cultivation, and resource allocation all rely heavily on these platforms as crucial carriers. Consequently, strengthening the development of medical humanistic education platforms is of utmost importance.
Ensuring health is the first and final goal of medical practitioners. Life cherish concept has been taken as a new connotation and new medical discipline by medical schools. Life education is the true nature of medical ethics, achieving a shift in medical education from knowledge-based to life-oriented. Over years, life education has demonstrated promising application in improving medical humanistic education. Several reforms have been performed based on this concept. Therefore, it is crucial for medical institutions to conduct research based on life education to improve teaching efffcacy for medical humanities education (Figure 1).
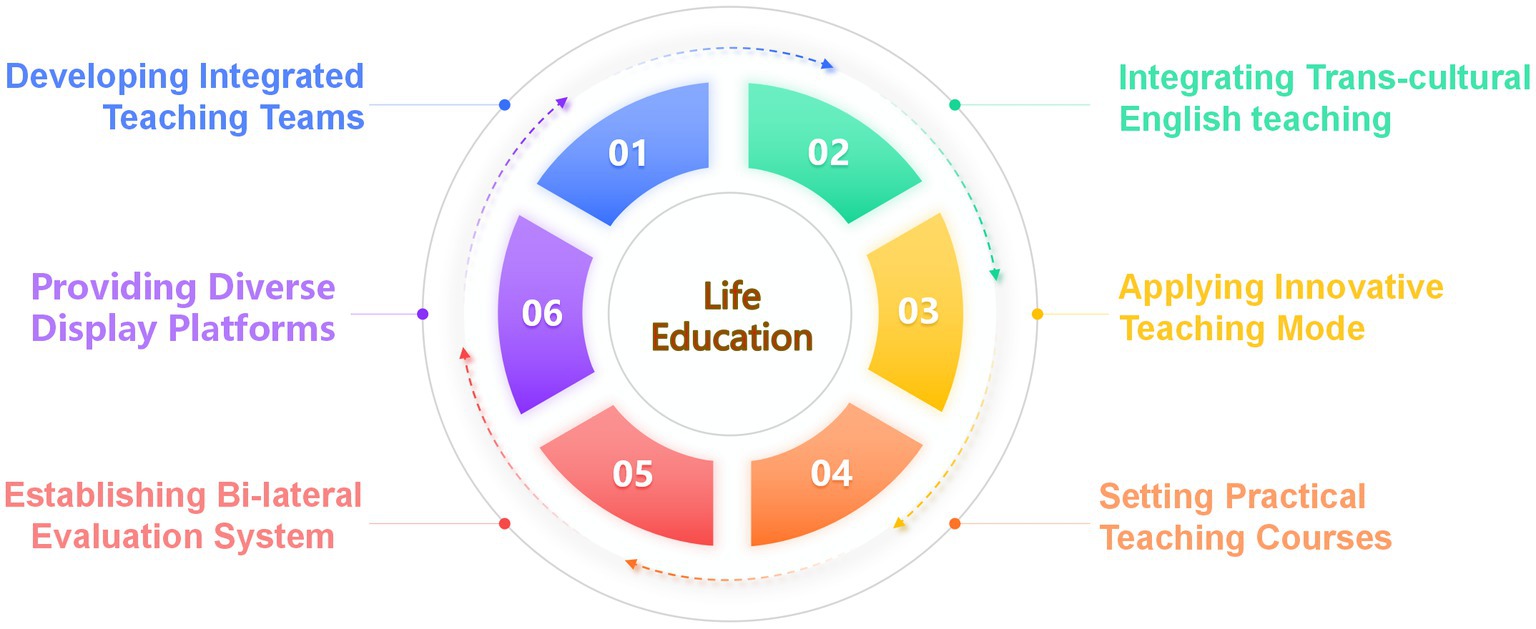
Figure 1. Reforms for improving medical humanities course quality in medical schools.
The development of a teaching staff team for medical humanities courses primarily focuses on talent recruitment and cultivation (Cohen and Sherif, 2014). First, medical schools should strengthen their emphasis on medical humanistic education, deepen cooperation and exchange in talent cultivation among high-level universities, research institutes, tertiary hospitals, and high-quality enterprises, and leverage the professional advantages of medical schools. Specific attention has to be paid to establish medical humanities centers, internship bases, and student exchange programs, with a focus on promoting talent recruitment mechanisms in scientific research and teaching at high-level universities and research institutes (Liu and Liu, 2024). In addition, talent exchange mechanisms for employment with hospitals and enterprises should be implemented (Umair et al., 2024). Second, attention should be paid to continuing education of teachers with multidisciplinary backgrounds. Long-term cooperation mechanisms should be established with hospitals and enterprises. Teachers of humanities courses can provide theoretical training and guidance on medical professional knowledge in hospitals and enterprises, exchange knowledge with industry experts, and establish cooperation platforms to further deepen continuing education and learning, thereby achieving resource sharing among schools, teachers, hospitals, and enterprises (Kemp and Day, 2014; Dong et al., 2021). In medical ethics and law classes, medical teachers and healthcare workers can be invited to exchange and share information about ethical events and legal disputes during medical work.
Due to the internationalization of medical education, medical students today should possess an international vision, being able to participate in international medical scientific research exchanges with language skills, cross-cultural communication skills as well as inclusive and dialectical thinking. Therefore, integrating trans-cultural medical humanities education with English teaching enables students to understand the advanced concepts of international medical humanities in English context, cultivating students’ critical and creative thinking (Daher-Nashif and Kane, 2016). In Medical humanistic English classes, under the guidance of both English and medical teachers, students are required to read the latest reports of medical humanities in English, make comparative analysis with Chinese medical humanistic concepts by collecting and analyzing medical humanistic cases from different cultural backgrounds and participate in international volunteering activities (Chen et al., 2023). We distributed a questionnaire to 300 s-year students of clinical medicine on integrating trans-cultural medical humanities education with English teaching and 235 of them were recovered (Table 2). The results showed students’ approval of the integrated courses of trans-cultural medical humanities education and English teaching.

Table 2. Students’ attitudes toward the integrated courses of trans-cultural medical humanities education and English teaching.
First, medical humanities courses should innovate their teaching modes, combine the characteristics of different disciplines, apply Internet-based teaching tools, and combine project-based learning with traditional teaching according to local conditions. Problem-based learning (PBL) is an approach that cultivates innovative thinking and enhances the ability to discover and solve problems of the students (Chen and Zhang, 2022; Chen et al., 2020). PBL teaching is problem-solving oriented and helps cultivate students’ humanistic spirit, literacy, and beliefs. This helps students focus on patients’ needs and respect their various rights (Jones, 2006; Arruzza et al., 2023). Medical psychology, medical law, and doctor-patient communication can stimulate students’ thinking and discussion through a series of related topics, such as doctor values, doctor-patient relationships, nurse–patient relationships, medical disputes, and responsibility determination, improving students’ classroom participation and enthusiasm. Case-based learning (CBL) focuses on bidirectional communication between teachers and students and is also an interactive, heuristic, and guided classroom teaching method (Thistlethwaite et al., 2012; Cen et al., 2021). Medical law and ethics courses can be combined with relevant cases to use CBL teaching to inspire students to understand events and enhance their problem-solving abilities (Chen et al., 2022).
Second, medical humanities teachers should update their teaching methods in a timely manner with the development and transformation of educational technology, particularly the application of various teaching methods (Bastola et al., 2024). For example, modernization and informatization of teaching methods have been shown to effectively enhance students’ independent study abilities. Teachers can use conditioned classrooms and practical-based learning to conduct virtual experiments or situational teaching in medical-humanities courses (Chen et al., 2020). This can help students enhance their internalization of relative medical humanities knowledge and improve their humanistic practice abilities.
Finally, various teaching patterns can help increase student participation in class. The five characteristics of the humanistic curriculum in U.S. medical schools are randomness, effectiveness, flexibility, intersectionality, and continuity (Figure 2; Qian et al., 2018). Many teaching models that are used in humanistic education programs are worth considering at the University of California as well. For example, students can attend a humanistic book club to improve their spiritual development, a medical humanistic group to support their mutual self-improvement, and multiple group seminars to train their supervised ability or independence.
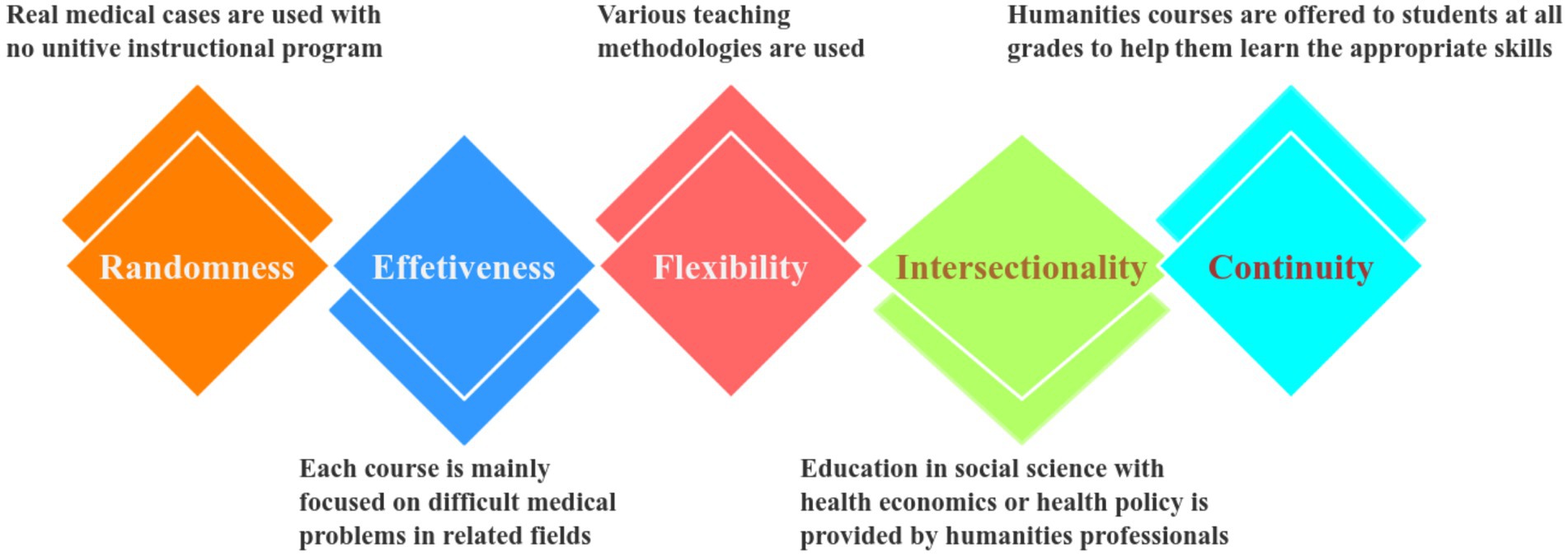
Figure 2. Five specialties of humanistic courses in American medical colleges.
Medical humanities courses should advocate a student-centered educational philosophy, optimize and conduct subject-specific clinical practice teaching, and enhance students’ clinical practice and job competence (Petrou et al., 2021). Outcome-based education (OBE) refers to results-oriented education that uses an opposite approach and provides a targeted and detailed teaching design (Gonzalo et al., 2018). First, schools can invite hospitals and enterprise managers to give special lectures on topics, such as medical humanistic education practices. Second, schools can cooperate with nursing homes, welfare homes, rehabilitation institutions, and communities to establish volunteer services and teaching practice platforms. Finally, most medical students enter hospitals for internships; thus, schools should pay attention to conducting internship assessments in the medical humanities field, such as doctor-patient communication skills, teamwork skills, and ethical ward rounds (Liu and Liu, 2024; Wang et al., 2019).
The cultivation of humanistic education of medical students accompanies their learning and work careers, helping them establish sustained humanistic care for patients, reverence for life, and a sense of noble mission for their careers. Medical humanistic education in the United States offers the standardized training and continuing education stage of resident physicians after graduation, which even extends to their entire careers as doctors (Anil et al., 2023). Therefore, employment units and society should continue to assume the role of educators after students graduate and put more effort into providing continuing education. Students can share their experiences and insights into medical practice through seminars, special lectures, and popular education. Experts in relevant fields can be invited to discuss ethical and medical disputes and legal liability determination and further enhance their humanistic literacy in work practice. This approach will substantially bolster the teaching quality of medical humanistic education.
Moreover, studies have demonstrated that applying the “patient-as-teacher” strategy in medical schools is a reliable way to influence medical students (Kumagai, 2008; Wilson et al., 2015). In this approach, students are exposed to patients who experience illness and must handle the procedures of the healthcare system like teachers when patients share their stories. The “patient-as-teacher” approach enhances the communication between patients and students, which enables medical students to foster a better understanding of medical humanism (Wilson et al., 2015). This is entirely different from traditional medical education which only focuses on the treatment of patients and relative diseases. This pattern helps students interact with suffering patients with more empathy and prompts more humane medical practice in advance (Simpson et al., 2020). The “patient-as-teacher” approach is worth trying in medical schools as it emphasizes the social and humanistic role of physicians and the humanity of patients, thus providing patient-centered care effectively (Boyde et al., 2021).
Medical humanities courses should improve formative evaluation and assessment systems and pay more attention to students’ emotions, attitudes, thinking patterns, and value orientations rather than just their level of objective knowledge mastery (Lee et al., 2019; Elwy et al., 2020). Some researchers stated that the assessment of medical humanities courses should adhere to the principles of development, student-centeredness, comprehensiveness, process, practicality, timeliness, and feasibility (Carr et al., 2021). This is similar to formative assessments guided by student development. Formative evaluation is a developmental evaluation aimed at promoting the comprehensive development of students’ knowledge, abilities, skills, emotions, attitudes, and other aspects (Elwy et al., 2020). In a survey of 5,996 students, 79.02% thought that closed-book exams were the most commonly used assessment method for medical humanities courses (Cor and Brocks, 2021). The closed-book exam, guided by assessment scores, examines students’ mastery of knowledge and theory (Cor and Brocks, 2021). However, it is difficult to assess their medical humanities literacy and knowledge transfer ability. Therefore, teachers can incorporate formative assessments into the comprehensive evaluation system of students, including routine tests, thematic discussions, and case sharing as process assessments (Kingston et al., 2023). Group presentations, scenario simulations, and skill tests can be used as final assessments for medical law and medical ethics courses with a focus on examining students’ general ability to apply knowledge (Melguizo-Garín et al., 2022; Thammasitboon and Brand, 2022). This can help cultivate innovative and critical thinking abilities. At the same time, students’ humanistic literacy and spirit in the classroom and clinical practice should also be evaluated. To reduce the occurrence of free riding and other similar situations, the degree of contribution of each individual in the group must also be assessed.
In the evaluation of teachers’ efforts, the diversification of evaluation subjects, content, and forms are the main aspects. Evaluation content can be combined with teaching objectives, teaching processes and methods, mastery of basic theories, student-classroom feedback, online teaching participation, and other comprehensive evaluations (Davis et al., 2022). The score-only model for students, as well as the employment rate-only model for teachers, must be avoided. Various forms of evaluation can be adopted, such as semester reports and course summaries, evaluation groups conducting in-depth classroom observations of student learning outcomes, and simulating situational assessments of teachers’ clinical practice abilities (Cai et al., 2022). The results of teaching evaluations and shortcomings in teaching should also be promptly fed back to teachers. This result can be used as an indicator of teacher performance evaluation, promoting the development of an evaluation and feedback system of evaluation improvement optimization, effectively improving the quality of education and teaching (Thirumoorthy, 2017).
People’s health represents the country’s national prosperity and strength. Ensuring health is the first and final goal of medical practitioners (Elrod and Fortenberry, 2020). Medical schools should take the life cherish concept as a new connotation and new medical discipline. A systemic curriculum system should be built for life education, which could continuously increase the proportion of life education content. In addition, inspiring students to consider the life-cherishing concept by delving into the elements of life education in both on and off-campus resources contributes to integrating life education content into humanistic education. Meanwhile, by creating a case library of medical humanistic education, an integrated life education course could be well established and applied to a wide range of students (Wershof Schwartz et al., 2009). Life education should be taken as the true nature of medical ethics, achieving a shift in medical education from knowledge-based to life-oriented.
The medical humanistic education platform serves as the cornerstone for the implementation of medical humanistic education. Hence, it is imperative to prioritize and enhance the infrastructure of medical humanities disciplines, gradually create favorable conditions for establishing humanities laboratories, and consolidate and expand the medical humanistic education platform through various avenues. Medical schools can build a strong campus cultural atmosphere for life education, which breaks through time and space limitations, creates immersive multi-scenario experiential teaching, and strengthens the influence of life education. These would help students understand the true nature of life and enhance their awareness of it.
Furthermore, guiding students to remember the original intention of doctors and cultivating their positive and optimistic attitude toward life is critical to improving humanistic spirit as well. The students’ medical literacy would be well-formed by setting up a life education lecture hall, performing life education ceremonies such as paying tribute to the cadavers, and establishing an art performance to cherish life. These would help students enhance their humanistic spirit and life literacy effectively.
Medical humanistic education is critical for cultivating qualified medical practitioners with international perspectives. This can guide physicians’ clinical performance and promote their empathy toward patients. In contrast, disharmonious doctor-patient relationships can lead to misunderstandings and even medical disputes between physicians and patients. Therefore, the medical humanities should be taken as a core process in clinical training. Thus, it is important to promote experiential learning and cooperation between the communities and medical schools. Meanwhile, an assessment of medical humanistic education must be established to improve harmonious mutual relationships and enhance physician-patient trust in medical care (Hoang et al., 2022; Huang et al., 2023). Medical humanistic education should be brought into medical education as early as possible because students must understand the need to be qualified and humane physicians before they study any professional courses.
This study focused on the current situation and proposed reforms for teaching medical humanities courses, which can help solve problems related to the teaching staff, teaching mode, practical teaching, assessment and evaluation systems, and other aspects. In the future, empirical research methods can be used to investigate the problems that exist in the entire process of medical humanities curriculum education, combined with the teaching system of medical humanities courses abroad and the current development status of medical humanities courses in China, to continuously improve the quality of classroom teaching and cultivate high-quality medical talent.
JY: Writing – review & editing, Funding acquisition. JZ: Writing – original draft, Writing – review & editing. YP: Writing – original draft. CL: Writing – original draft. HD: Supervision, Writing – review & editing. JC: Writing – review & editing, Supervision.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work was supported by Guangxi Higher Education Teaching Reform Projects (Nos. 2023JAG267 and 2022JGZ154), Degree and Graduate Education Reform Program of Guilin Medical University (Nos. JGY2024236 and JGY2024242), and Guilin Medical University Teaching Research and Reform Program (No. JG202220 and No. JG202402).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Albert, M., Rowland, P., and Friesen, F. (2020). Interdisciplinarity in medical education research: myth and reality. Advan. Health Sci. Educ. Theory Prac. 25, 1243–1253. doi: 10.1007/s10459-020-09977-8
Anil, J., Cunningham, P., and Dine, C. J. (2023). The medical humanities at United States medical schools: a mixed method analysis of publicly assessable information on 31 schools. BMC Med. Educ. 23:620. doi: 10.1186/s12909-023-04564-y
Arnold, R. M., Povar, G. J., and Howell, J. D. (1987). The humanities, humanistic behavior, and the humane physician: a cautionary note. Ann. Intern. Med. 106, 313–318. doi: 10.7326/0003-4819-106-2-313
Arruzza, E., Chau, M., and Kilgour, A. (2023). Problem-based learning in medical radiation science education: A scoping review. Radiography (London, England: 1995) 29, 564–572. doi: 10.1016/j.radi.2023.03.008
Bastola, P., Atreya, A., Bhandari, P. S., and Parajuli, S. (2024). The evolution of anesthesiology education: embracing new technologies and teaching approaches. Health Sci. Reports 7:e1765. doi: 10.1002/hsr2.1765
Boudreau, J. D., and Fuks, A. (2015). The humanities in medical education: ways of knowing, doing and being. J. Med. Humanit. 36, 321–336. doi: 10.1007/s10912-014-9285-5
Boyde, M., Tuckett, A., and Ty, J. (2021). Teacher-as-actor: investigating the barriers and facilitators of patient education among hospitalized patients in a cardiology clinical unit[J]. Nurs. Health Sci. 23, 871–879. doi: 10.1111/nhs.12874
Brazeau, C. M. L. R., Schroeder, R., Rovi, S., and Boyd, L. (2011). Relationship between medical student service and empathy. Academic Med.: J. Association of American Medical Colleges 86, S42–S45. doi: 10.1097/ACM.0b013e31822a6ae0
Buck, E., Billingsley, T., McKee, J., Richardson, G., and Geary, C. (2021). The physician healer track: educating the hearts and the minds of future physicians. Med. Educ. Online 26:1844394. doi: 10.1080/10872981.2020.1844394
Cai, B., Shafait, Z., and Chen, L. (2022). Teachers’ adoption of emotions-based learning outcomes: significance of teachers’ competence, creative performance, and university performance. Front. Psychol. 13:812447. doi: 10.3389/fpsyg.2022.812447
Caldicott, C. V., and Danis, M. (2009). Medical ethics contributes to clinical management: teaching medical students to engage patients as moral agents. Med. Educ. 43, 283–289. doi: 10.1111/j.1365-2923.2008.03277.x
Campbell, A. T. (2012). Teaching law in medical schools: first, reflect. J. Law, Med. Ethics: J. American Society of Law, Med. Ethics 40, 301–310. doi: 10.1111/j.1748-720X.2012.00665.x
Carr, S. E., Noya, F., and Phillips, B. (2021). Health humanities curriculum and evaluation in health professions education: a scoping review. BMC Med. Educ. 21:568. doi: 10.1186/s12909-021-03002-1
Carrard, V., Bourquin, C., Berney, S., Schlegel, K., Gaume, J., Bart, P. A., et al. (2022). The relationship between medical students’ empathy, mental health, and burnout: a cross-sectional study. Med. Teach. 44, 1392–1399. doi: 10.1080/0142159X.2022.2098708
Cen, X. Y., Hua, Y., Niu, S., and Yu, T. (2021). Application of case-based learning in medical student education: a meta-analysis. Eur. Rev. Med. Pharmacol. Sci. 25, 3173–3181. doi: 10.26355/eurrev_202104_25726
Centeno, C., Ballesteros, M., Carrasco, J. M., and Arantzamendi, M. (2016). Does palliative care education matter to medical students? The experience of attending an undergraduate course in palliative care. BMJ Support. Palliat. Care 6, 128–134. doi: 10.1136/bmjspcare-2014-000646
Chang, J., Qi, Z., Jiang, S., Li, L., and Sun, Q. (2021). The impact of palliative care education and training program on the resident physicians. Annals of Palliative Med. 10, 2758–2752765. doi: 10.21037/apm-20-1625
Chen, W. T., Fu, C. P., and Chang, Y. D. (2022). Developing an innovative medical ethics and law curriculum-constructing a situation-based, interdisciplinary, court-based learning course: a mixed methods study. BMC Med. Educ. 22:284. doi: 10.1186/s12909-022-03349-z
Chen, J., and Zhang, Z. (2022). Editorial: public health promotion and medical education reform. Front. Public Health 10:918962. doi: 10.3389/fpubh.2022.918962
Chen, L., Zhang, J., and Zhu, Y. (2023). Exploration and practice of humanistic education for medical students based on volunteerism. Medical Educ. 28:2182691. doi: 10.1080/10872981.2023.2182691
Chen, J., Zhou, J., Wang, Y., Qi, G., Xia, C., Mo, G., et al. (2020). Blended learning in basic medical laboratory courses improves medical students’ abilities in self-learning, understanding, and problem solving. Adv. Physiol. Educ. 44, 9–14. doi: 10.1152/advan.00076.2019
Cohen, S., and Herbert, T. B. (1996). Health psychology: psychological factors and physical disease from the perspective of human psychoneuroimmunology. Annu. Rev. Psychol. 47, 113–142. doi: 10.1146/annurev.psych.47.1.113
Cohen, L. G., and Sherif, Y. A. (2014). Twelve tips on teaching and learning humanism in medical education. Med. Teach. 36, 680–684. doi: 10.3109/0142159X.2014.916779
Cor, M. K., and Brocks, D. R. (2021). Does a sudden shift of testing format from closed-book to open-book change the characteristics of test scores on summative final exams? Curr. Pharm. Teach. Learn. 13, 1174–1179. doi: 10.1016/j.cptl.2021.06.039
Costa, R. C. (2019). The place of the humanities in today’s knowledge society. Palgrave Communications 5, 1–5. doi: 10.1057/s41599-019-0245-6
Custers, E. J. F. M., and Cate, O. T. (2018). The history of medical education in Europe and the United States, with respect to time and proficiency. Academic Med.: J. Association of American Medical Colleges 93, S49–S54. doi: 10.1097/ACM.0000000000002079
Daher-Nashif, S., and Kane, T. (2016). A culturally competent approach to teaching humanities in an international medical school: potential frameworks and lessons learned. MedEdPublish 2022:6. doi: 10.12688/mep.18938.2
Davis, S., Duane, B., and Loxley, A. (2022). The evaluation of an evidence-based model of feedback implemented on an undergraduate dental clinical learning environment. BMC Med. Educ. 22:588
Dickinson, H. H. (1970). Medical ethics and the law. The position of the medical administrator. Med. J. Aust. 1, 791–794. doi: 10.5694/j.1326-5377.1970.tb116813.x
Dong, H., Lio, J., Sherer, R., and Jiang, I. (2021). Some learning theories for medical educators. Medical Sci. Educator 31, 1157–1172. doi: 10.1007/s40670-021-01270-6
Doukas, D. J., Ozar, D. T., Darragh, M., de Groot, J. M., Carter, B. S., and Stout, N. (2022). Virtue and care ethics & humanism in medical education: a scoping review. BMC Med. Educ. 22:131. doi: 10.1186/s12909-021-03051-6
Elrod, J. K., and Fortenberry, J. L. (2020). Integrated marketing communications: a strategic priority in health and medicine. BMC Health Serv. Res. 20:825. doi: 10.1186/s12913-020-05606-7
Elwy, A. R., Wasan, A. D., and Gillman, A. G. (2020). Using formative evaluation methods to improve clinical implementation efforts: description and an example. Psychiatry Res. 283:112532. doi: 10.1016/j.psychres.2019.112532
Fanwei, Q. U., Jin, H. E., Hua, M. A., Yanling, J. I. A. N. G., Wenlan, Z. H. A. O., Chongsuvivatwong, V., et al. (2019). A comparative analysis of medical education models and curriculums of a medical university and a medical education center. JNMA J. Nepal Med. Assoc. 57, 45–49. doi: 10.31729/jnma.4107
Friedman, L. D. (2002). The precarious position of the medical humanities in the medical school curriculum. Academic Med.: J. Association of American Medical Colleges 77, 320–322. doi: 10.1097/00001888-200204000-00011
Friedman, C. P., Donaldson, K. M., and Vantsevich, A. V. (2016). Educating medical students in the era of ubiquitous information. Med. Teach. 38, 504–509. doi: 10.3109/0142159X.2016.1150990
Gonzalo, J. D., Caverzagie, K. J., Hawkins, R. E., Lawson, L., Wolpaw, D. R., and Chang, A. (2018). Concerns and responses for integrating health systems science into medical education. Academic Med.: J. Association of American Medical Colleges 93, 843–849. doi: 10.1097/ACM.0000000000001960
Guo, X. (2022). A study on cross-media teaching model for college english classroom based on output-driven hypothetical neural network. Comput. Intell. Neurosci. 2022, 1–11. doi: 10.1155/2022/5283439
Hakim, A. (2023). Investigating the challenges of clinical education from the viewpoint of nursing educators and students: a cross-sectional study. SAGE Open Med. 11:20503121221143578. doi: 10.1177/20503121221143578
Hoang, B. L., Monrouxe, L. V., Chen, K. S., Chang, S. C., Chiavaroli, N., Mauludina, Y. S., et al. (2022). Medical humanities education and its influence on students’ outcomes in Taiwan: a systematic review. Front. Med. 9:857488. doi: 10.3389/fmed.2022.857488
Howick, J., Zhao, L., McKaig, B., Rosa, A., Campaner, R., Oke, J., et al. (2022). Do medical schools teach medical humanities? Review of curricula in the United States, Canada and the United Kingdom. J. Eval. Clin. Pract. 28, 86–92. doi: 10.1111/jep.13589
Huang, S. S., Ho, C. C., and Chu, Y. R. (2023). The quantified analysis of the correlation between medical humanities curriculums and medical students’ performance. BMC Med. Educ. 23:571. doi: 10.1186/s12909-023-04073-y
Huss, N., Ikiugu, M. N., Hackett, F., Sheffield, P. E., Palipane, N., and Groome, J. (2020). Education for sustainable health care: from learning to professional practice. Med. Teach. 42, 1097–1101. doi: 10.1080/0142159X.2020.1797998
Isaac, M. (2023). Role of humanities in modern medical education. Curr. Opin. Psychiatry 36, 347–351. doi: 10.1097/YCO.0000000000000884
Jones, R. W. (2006). Problem-based learning: description, advantages, disadvantages, scenarios and facilitation. Anaesth. Intensive Care 34, 485–488. doi: 10.1177/0310057X0603400417
Jung, H. Y., Kim, J. W., Lee, S., Yoo, S. H., Jeon, J. H., Kim, T. W., et al. (2016). A study of core humanistic competency for developing humanism education for medical students. J. Korean Med. Sci. 31, 829–835. doi: 10.3346/jkms.2016.31.6.829
Kemp, S. J., and Day, G. (2014). Teaching medical humanities in the digital world: affordances of technology-enhanced learning. Med. Humanit. 40, 125–130. doi: 10.1136/medhum-2014-010518
Kingston, A. K., Garofalo, E. M., and Cardoza, K. (2023). Designing formative assessments to improve anatomy exam performance. Anat. Sci. Educ. 16, 989–1003. doi: 10.1002/ase.2279
Kumagai, A. K. (2008). A conceptual framework for the use of illness narratives in medical education. Academic Med.: J. Association of American Medical Colleges 83, 653–658. doi: 10.1097/ACM.0b013e3181782e17
Kumagai, A. K. (2012). Perspective: acts of interpretation: a philosophical approach to using creative arts in medical education. Academic Med.: J. Association of American Medical Colleges 87, 1138–1144. doi: 10.1097/ACM.0b013e31825d0fd7
Lee, S. Y., Lee, S. H., and Shin, J. S. (2019). Evaluation of medical humanities course in college of medicine using the context, input, process, and product evaluation model. J. Korean Med. Sci. 34:e163. doi: 10.3346/jkms.2019.34.e163
Li, Y., Jin, Z., Dong, G., Zheng, R., and Wang, T. (2022). A survey of college students’ willingness to participate in social practice with perceived environmental support based on the applied mixed research method. Front. Psychol. 13:972556. doi: 10.3389/fpsyg.2022.972556
Liou, K. T., Jamorabo, D. S., Dollase, R. H., Dumenco, L., Schiffman, F. J., and Baruch, J. M. (2016). Playing in the “gutter”: cultivating creativity in medical education and practice. Acad. Med. 91, 322–327. doi: 10.1097/ACM.0000000000001018
Liu, C., and Liu, S. (2024). Medical students’ knowledge and attitude toward brain death and the influence of medical education: a cross-sectional study. BMC Med. Educ. 24:346. doi: 10.1186/s12909-024-05346-w
Macnaughton, J. (2011). Medical humanities’ challenge to medicine. J. Eval. Clin. Pract. 17, 927–932. doi: 10.1111/j.1365-2753.2011.01728.x
Mangione, S., Chakraborti, C., Staltari, G., Harrison, R., Tunkel, A. R., Liou, K. T., et al. (2018). Medical students’ exposure to the humanities correlates with positive personal qualities and reduced burnout: a multi-institutional U.S. survey. J. Gen. Intern. Med. 33, 628–634. doi: 10.1007/s11606-017-4275-8
Melguizo-Garín, A., Ruiz-Rodríguez, I., and Peláez-Fernández, M. A. (2022). Relationship between group work competencies and satisfaction with project-based learning among university students. Front. Psychol. 13:811864. doi: 10.3389/fpsyg.2022.811864
Miller, J. L. (2004). From "building" to "cultivating": changing the way we educate doctors and nurses in the 21st century. Creat. Nurs. 10, 6–8. doi: 10.1891/1078-4535.10.3.6
Mitchell, M., and Kan, L. (2019). Digital technology and the future of health systems. Health Syst. Reform 5, 113–120. doi: 10.1080/23288604.2019.1583040
Moyer, C. A., Arnold, L., and Quaintance, J. (2010). What factors create a humanistic doctor? A nationwide survey of fourth-year medical students. Academic Med.: J. Association of American Medical Colleges 85, 1800–1807. doi: 10.1097/ACM.0b013e3181f526af
Ozair, A., Singh, K. K., and Kumar, P. (2021). Decline of empathy during medical education. Academic Med.: J. Association of American Medical Colleges 96:317. doi: 10.1097/ACM.0000000000003748
Petrou, L., Mittelman, E., Osibona, O., Panahi, M., Harvey, J. M., Patrick, Y. A. A., et al. (2021). The role of humanities in the medical curriculum: medical students’ perspectives. BMC Med. Educ. 21:179. doi: 10.1186/s12909-021-02555-5
Pfeiffer, S., Chen, Y., and Tsai, D. (2016). Progress integrating medical humanities into medical education: a global overview. Curr. Opin. Psychiatry 29, 298–301. doi: 10.1097/YCO.0000000000000265
Qian, Y., Han, Q., and Yuan, W. (2018). Insights into medical humanities education in China and the west. J. Int. Med. Res. 46, 3507–3517. doi: 10.1177/0300060518790415
Rabinowitz, D. G. (2021). On the arts and humanities in medical education. Philosophy, ethics, and humanities in medicine: PEHM 16:4. doi: 10.1186/s13010-021-00102-0
Rodríguez, C., Tellier, P. P., and Bélanger, E. (2012). Exploring professional identification and reputation of family medicine among medical students: a Canadian case study. Education for primary care: an official publication of the Association of Course Organisers, National Association of GP Tutors, World Organisation of Family Doctors 23, 158–168. doi: 10.1080/14739879.2012.11494099
Rubins, D., McCoy, A. B., and Dutta, S. (2022). Real-time user feedback to support clinical decision support system improvement. Appl. Clin. Inform. 13, 1024–1032. doi: 10.1055/s-0042-1757923
Saga, T., Tanaka, H., Matsuda, Y., Morimoto, T., Uratani, M., Okazaki, K., et al. (2023). Automatic evaluation-feedback system for automated social skills training. Sci. Rep. 13:6856. doi: 10.1038/s41598-023-33703-0
Simpson, J. S., Ng, S., and Kangasjarvi, E. (2020). Humanistic education in surgery: a “patient as teacher” program for surgical clerkship. Canadian J. Surg. J. Canadien De Chirurgie 63, E257–E260. doi: 10.1503/cjs.005319
Smydra, R., May, M., Taranikanti, V., and Mi, M. (2022). Integration of arts and humanities in medical education: a narrative review. J. Cancer Educ.: Official J. American Association for Cancer Education 37, 1267–1274. doi: 10.1007/s13187-021-02058-3
Song, P., and Tang, W. (2017). Emphasizing humanities in medical education: promoting the integration of medical scientific spirit and medical humanistic spirit. Biosci. Trends 11, 128–133. doi: 10.5582/bst.2017.01092
Swick, H. M., Szenas, P., Danoff, D., and Whitcomb, M. E. (1999). Teaching professionalism in undergraduate medical education. JAMA 282, 830–832. doi: 10.1001/jama.282.9.830
Thammasitboon, S., and Brand, P. L. P. (2022). The physiology of learning: strategies clinical teachers can adopt to facilitate learning. Eur. J. Pediatr. 181, 429–433. doi: 10.1007/s00431-021-04054-7
Thirumoorthy, T. (2017). The ethics of medical education - the ethical and professional issues in teaching and learning medicine. Ann. Acad. Med. Singap. 46, 331–332. doi: 10.47102/annals-acadmedsg.V46N9p331
Thistlethwaite, J. E., Davies, D., and Ekeocha, S. (2012). The effectiveness of case-based learning in health professional education. A BEME systematic review: BEME guide no. 23. Med. Teach. 34, e421–e444. doi: 10.3109/0142159X.2012.680939
Umair, S., Waqas, U., and Mrugalska, B. (2024). Cultivating sustainable environmental performance: the role of green talent management, transformational leadership, and employee engagement with green initiatives. Work (Reading, Mass.) 78, 1093–1105. doi: 10.3233/WOR-230357
Wang, W. (2021). Medical education in China: progress in the past 70 years and a vision for the future. BMC Med. Educ. 21:453. doi: 10.1186/s12909-021-02875-6
Wang, T., Tan, J. Y. B., Liu, X. L., et al. (2023). Barriers and enablers to implementing clinical practice guidelines in primary care: an overview of systematic reviews. BMJ Open 13:e062158. doi: 10.1136/bmjopen-2022-062158
Wang, Q., Wang, L., and Shi, M. (2019). Empathy, burnout, life satisfaction, correlations and associated socio-demographic factors among Chinese undergraduate medical students: an exploratory cross-sectional study. BMC Med. Educ. 19:341. doi: 10.1186/s12909-019-1788-3
Wartman, S. A. (2019). The empirical challenge of 21st-century medical education. Academic Med.: J. Association of American Medical Colleges 94, 1412–1415. doi: 10.1097/ACM.0000000000002866
Wershof Schwartz, A., Abramson, J. S., and Wojnowich, I. (2009). Evaluating the impact of the humanities in medical education. Mount Sinai J. Med. New York 76, 372–380. doi: 10.1002/msj.20126
Wilson, R., Godfrey, C. M., Sears, K., Medves, J., Ross-White, A., and Lambert, N. (2015). Exploring conceptual and theoretical frameworks for nurse practitioner education: a scoping review protocol. JBI Database System Rev. Implement. Rep. 13, 146–155. doi: 10.11124/jbisrir-2015-2150
Woolston, C. (2022). Stress and uncertainty drag down graduate students’ satisfaction. Nature 610, 805–808. doi: 10.1038/d41586-022-03394-0
Yi, S., Yam, E. L. Y., Cheruvettolil, K., Linos, E., Gupta, A., Palaniappan, L., et al. (2024). Perspectives of digital health innovations in low- and middle-income health care systems from south and Southeast Asia. J. Med. Internet Res. 26:e57612. doi: 10.2196/57612
Keywords: medical humanities, medical education, trans-cultural humanistic education, teaching mode, ethics, life education
Citation: Yang J, Zhou J, Pan Y, Liu C, Deng H and Chen J (2025) Exploring and practicing trans-cultural humanistic education for medical students based on life education. Front. Educ. 10:1461718. doi: 10.3389/feduc.2025.1461718
Edited by:
Mainul Haque, National Defence University of Malaysia, MalaysiaReviewed by:
Huan Ren, Southern University of Science and Technology, ChinaCopyright © 2025 Yang, Zhou, Pan, Liu, Deng and Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Honglin Deng, MTEyMDAyMDA1QGdsbWMuZWR1LmNu; Jian Chen, Y2hlbmppYW5AZ2xtYy5lZHUuY24=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.