 Kelsey A. Clayback
Kelsey A. Clayback Ann M. Partee
Ann M. Partee Amanda P. Williford
Amanda P. Williford Jason T. Downer
Jason T. Downer Kyra Parker
Kyra Parker Ann S. Lhospital
Ann S. Lhospital
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Educ., 10 January 2025
Sec. Special Educational Needs
Volume 9 - 2024 | https://doi.org/10.3389/feduc.2024.1494378
This article is part of the Research TopicInclusion of Children with Social-Emotional or Behavioral Needs in Early Childhood EducationView all 6 articles
Introduction: Early childhood educators continue to need support to build their capacity to promote positive social and emotional development and address challenging behavior when it occurs, without resorting to exclusion. One approach to improve the experiences and outcomes of young children through better support to educators is Early Childhood Mental Health Consultation (ECMHC). ECMHC is an evidence-based intervention that pairs a mental health professional (i.e., “consultant”) with early childhood educators to build the capacity of providers to promote inclusion by supporting young children's social and emotional development.
Methods: In this paper, we describe a model of ECMHC that combines data-driven action planning and an individualized approach to build educators' capacity to implement social and emotional teaching practices with fidelity. The model begins with in-context classroom observations of child engagement and teaching practices, as well as a teacher-report of child behavior. Based on this observational baseline data, a standardized formula selects a personalized set of social and emotional teaching strategies recommended for the focus of consultation, based on the strengths and challenges of the teacher and child. Strategies included foundational strategies (e.g., fostering strong teacher-child relationships), flexible strategies (e.g., using cues and visuals), and targeted strategies (e.g., supporting problem-solving skills). Consultants and teachers then collaboratively work together to select strategies to focus on in consultation, allowing for flexibility and individualization based on individual teacher and child strengths and challenges.
Results: We address the following two aims: (1) examine teaching practices and children's behavior at the beginning of consultation and how these data resulted in different recommended teaching strategies, based on our standardized formula, (2) present three case examples to further illustrate how these data guided consultation to improve social and emotional teaching practices during the 2023 to 2024 school year. We found that this baseline data collection and the subsequent data-driven process for selecting strategies was feasible in that all consultants and teachers served by ECMHC were able to use it. We also found variability in baseline data and the associated ECMHC teaching strategies recommended, suggesting that the measures were sensitive to unique classroom needs and individualized recommended strategies accordingly.
Discussion: We discuss how this approach allowed consultants to tailor ECMHC services to the unique strengths and challenges of each child and teacher dyad, while being firmly grounded in empirical research and previously validated assessments.
Early childhood educators continue to need support to build their capacity to promote positive social and emotional development and address challenging behavior when it occurs, without resorting to exclusion. One approach to improve the experiences and outcomes of young children through better support to educators is Early Childhood Mental Health Consultation (ECMHC). ECMHC pairs a mental health professional (i.e., “consultant”) with educators to build the capacity of early childhood education providers to support young children's social and emotional development. In this paper, we describe how a model of ECMHC in Virginia was designed to support consultants to collect and use observational data of classroom practices and child engagement to build the capacity of educators to implement social and emotional teaching practices and reduce exclusionary discipline and disproportionality in these practices. This ECMHC model balances a data-driven approach with flexibility for consultants to individualize their services based on teacher and child needs. We address the following two aims: (1) examine teaching practices and children's behavior at the beginning of consultation and how these data resulted in different recommended teaching strategies, based on our standardized formula, (2) present three case examples to further illustrate how these data guided consultation to improve social and emotional teaching practices during the 2023–2024 school year.
Early childhood educators foster strong teacher-child relationships, help children positively engage in the classroom, and model and explicitly teach social and emotional skills. Some children experience social, emotional, and behavioral challenges and need more intensive and individualized support from their educators (Blewitt et al., 2021; Hemmeter et al., 2021; McClelland et al., 2017; Bulotsky-Shearer et al., 2008). Educators and program directors report needing more support and professional development to adequately address children's social and emotional development and behavior (Garrity et al., 2019; Obee et al., 2023; Snell et al., 2012). In fact, teachers report finding children's behavior to be extremely stressful (Berlin et al., 2020), and research has found that higher challenging behavior is consistently predictive of lower teacher wellbeing (Clayback and Williford, 2022; Friedman-Krauss et al., 2014; Jeon et al., 2018). These challenges are compounded, as early childhood educators face low wages (McLean et al., 2021; Whitebook et al., 2014), struggle to access meaningful support and professional development (Lang et al., 2024; Obee et al., 2023), and experience high rates of depression (Whitaker et al., 2013; Roberts et al., 2019) and turnover (Bassok et al., 2021; Doromal et al., 2022).
Teacher stress, lack of support for the field, and child behavior make fostering high-quality and inclusive learning environments difficult. These challenges are all related to the high rates of exclusionary discipline in early childhood (Clayback et al., 2024; O'Grady and Ostrosky, 2021; Silver and Zinsser, 2020; Zinsser et al., 2022). Exclusionary discipline includes a spectrum of practices, ranging from removals from activities within a classroom to expulsion from a program (Williford et al., 2023). These practices are most commonly used in response to teachers' and leaders' perceptions of children's externalizing behavior, including tantrums, biting, hitting, not listening to instructions, and disrupting the classroom (Mondi et al., 2022; Yoder and Williford, 2019). Further, previous research has shown that early childhood settings are more likely to exclude Black children, boys, and children with disabilities (Giordano et al., 2021; U. S. Department of Education Office for Civil Rights, 2014; Zeng et al., 2020), demonstrating the systematic racism and ableism that undermine efforts to increase inclusion. As such, recent practice and policy efforts have begun to address these inequities to support the inclusion of children with social, emotional, and behavioral challenges in early childhood classrooms (Buell et al., 2022; Loomis et al., 2022).
When early childhood educators feel stressed and lack support to meaningfully prevent and respond to children's challenging behavior, they frequently resort to exclusionary discipline practices, including suspension and expulsion (Gilliam and Reyes, 2018; Zinsser et al., 2019, 2022). The past 20 years of research has consistently shown that exclusionary practices are being used at alarming rates in early childhood settings, are applied disproportionally to children of color and children with disabilities, and result in young children with behavioral needs missing out on learning opportunities during critical developmental windows (Alamos and Williford, 2023; Clayback and Hemmeter, 2021; Williford et al., 2023; Wymer et al., 2022).
When children are excluded, they miss out on not only academic learning, but also social interactions and opportunities to problem solve, manage their emotions, and form positive relationships with peers and teachers. This is especially detrimental for young children with social and emotional needs, who benefit from these social and emotional learning opportunities the most. Unfortunately, for children perceived by their teacher as challenging, negative and conflictual interactions often become cyclical and result in teachers using harsh and exclusionary discipline practices (Alamos and Williford, 2023). Improving teacher-child relationships and equipping educators with the knowledge and skills to keep children in the classroom rather than being suspended and expelled and actively engaged in learning and social activities is key to promoting inclusion (Schoch et al., 2024; Sutherland et al., 2018).
Researchers, practitioners, and policymakers have increasingly made efforts to better support educators and young children and address exclusion in early childhood. One approach to address teacher stress and prevent exclusionary discipline is early childhood mental health consultation (ECMHC). ECMHC is an intervention that pairs a mental health professional (i.e., “consultant”) with adults (i.e., caregivers, teachers, and families) who support young children in the settings where they grow and learn (Cohen and Kaufmann, 2005; Partee et al., 2023). Previous research has found that ECMHC is effective at improving teacher-child interactions and classroom practices, lowering teacher stress, and decreasing young children's externalizing behavior (Albritton et al., 2019; Downer et al., 2018; Silver et al., 2023; Spielberger et al., 2024). Dosage of consultation may be particularly important, as a recent study found that teachers who received consultation for longer durations (i.e., 20 vs. 10 weeks) showed greater improvements in classroom climate (Mathis et al., 2025). ECMHC is also associated with a reduction in exclusionary discipline and expulsion risk (Conners Edge et al., 2021; Davis et al., 2020b) and is increasingly encouraged in policies to support the inclusion of children with social and emotional needs (Loomis et al., 2022).
This growing body of work has found that ECMHC is generally associated with more positive outcomes for teachers and children, though ECMHC can be hard to define, and little empirical research has been conducted to explore mechanisms and theories of change. Best practice guidance on ECMHC recommends that consultation and associated activities be adapted depending on the unique needs of the individual (e.g., teacher or child) and setting being served. As such, specific activities vary greatly, though the relationship between the consultant and individual is considered a central mechanism of change (Davis et al., 2020a). One recent study identified several essential elements of ECMHC, including building strong, equitable relationships between consultants and teachers; supporting teachers to use new ways of thinking and acting; and helping teachers embrace equity in their roles (Schoch et al., 2024).
Models also use research-based assessments like classroom observations and teacher rating scales to varying degrees. While many models do not take an explicit data-driven approach, Mathis et al. (2025) developed a model of consultation that used data to select classrooms most in need of consultation, track classroom progress, and help determine when services should end. Our paper adds to the research literature by describing how one state ECMHC model incorporated data use into the consultation process. In the ECMHC model used in Virginia, consultants individualize their approach based on classroom needs but also use standardized assessments to understand child behavior and teaching practices in-context. We focus this paper on describing the process of using data to guide early decisions in consultation.
ECMHC prioritizes the consultant-teacher relationship and is designed to be highly flexible and individualized, based on the individual needs of teachers, children, and classrooms (Schoch et al., 2024). At the same time, there is a need for consultants to implement evidence-based ECMHC services with fidelity, necessitating a need for guidance on what to focus on in consultation and how to best build capacity of educators and programs. This is especially true as states are scaling-up their ECMHC models, offering services to more and more educators and needing scalable ways to measure intervention fidelity and outcomes across settings.
Related areas of research have also grappled with this tension between flexibility and fidelity, including early intervention for children with disabilities (Lee et al., 2023; Pickard et al., 2022), child welfare (Bromley, 2023), and mental health treatment (Galovski et al., 2024; Kendall et al., 2023). For example, Pickard et al. (2021) found that early intervention providers wanted more training in manualized evidence-based practices but also wanted support in adapting and tailoring services based on family needs. Further, in clinical psychology, there is a movement toward measurement-based care (MBC) to support a data-informed, client-centered, and shared decision-making approach to mental health treatment (Connors et al., 2024). In an MBC approach, clinicians assess mental health symptoms initially and on an ongoing basis to inform treatment and measure effectiveness (Lewis et al., 2019; Scott and Lewis, 2015). This data-based approach has shown to be more effective in reducing youth's internalizing and externalizing symptoms in community mental health settings than services that do not utilize data in systematic ways (Williams et al., 2023).
Evidence-based interventions, including ECMHC, need to be implemented with high implementation fidelity while also adapting to support children and families with varying needs to ensure social and cultural relevance. Our model of ECMHC aims to bridge the gap between individualizing and manualizing an intervention. We do so by combining an individualized approach with data-driven action planning to build educators' capacity. In doing so, the Virginia model of ECMHC is innovative as it integrates both standardized data-driven processes and the ability to individualize the model through data collected by multiple, multi-informant sources on both teacher and child strengths and challenges. This allows consultants to tailor ECMHC services to the unique strengths and challenges of each child and teacher dyad, while being firmly grounded in empirical research and previously validated assessments. In this paper, we illustrate our process of using data to drive consultation.
The current paper describes how a model of ECMHC uses consultant observations of teaching practices and child engagement in-context to build the capacity of early childhood providers to equitably promote social and emotional skills and address challenging behavior to promote inclusion of young children with behavioral needs. We focus on how baseline data collected directly in the classroom context from different perspectives (i.e., teacher and consultant) and using distinct formats (i.e., surveys and observations) informed the focus of consultation. First, we briefly describe the state context and our partnership with the Virginia Department of Education (VDOE). We then focus our paper on describing our service model for providing ECMHC, with an emphasis on how consultants use data in-context to support teachers and children with social, emotional, and behavioral needs. We then illustrate this approach with data collected related to ECMHC cases for preschool children ages three to five who are served in publicly funded programs. We present data collected at the beginning of consultation and provide case examples to illustrate how data guided consultation during pilot year 3 (2023–2024). The current study contributes to the literature on ECMHC by describing specific components (i.e., pre-consultation data collection) and processes (i.e., systematic data use) used in the Virginia ECMHC model to facilitate individualized consultation. Detailed descriptions of the components of various ECMHC models will help the field move toward more refined theories of change for ECMHC and ultimately better supports provided to educators and children.
ECMHC in Virginia is situated in a broader context of ongoing policy efforts to improve quality in early childhood education. This includes a state-wide quality measurement and improvement system, VQB5. In partnership with the Virginia Department of Education (VDOE), our team at the Center for Advanced Study of Teaching and Learning (CASTL) spent the past 4 years developing and piloting a model of ECMHC. In fall 2020, state legislation in Virginia required that a workgroup composed of stakeholders in infant and early childhood mental health study the feasibility of adopting an ECMHC program to prevent suspensions and expulsions of young children attending ECE programs. Based on recommendations made by this workgroup, VDOE allocated federal relief dollars to fund an ECMHC pilot in early care and education classrooms starting in the 2021–2022 school year (pilot year 1). Funding was reallocated for 2022–2023 (pilot year 2) and 2023–2024 (pilot year 3).
The pilot brought together two partners—Child Development Resources (CDR) and CASTL at the University of Virginia—to design, implement, and evaluate an ECMHC model for children from birth to five. CDR provided consultation to settings serving infants and toddlers (children ages birth to 35 months of age), and CASTL provided consultation to settings serving preschoolers (children 36–60 months of age). Virginia's ECMHC pilot was guided by three goals: (1) Assist ECE teachers in supporting children's social and emotional needs in response to COVID-19, particularly among communities with access to the fewest resources, (2) Prevent suspensions and expulsions of young children attending early care and education programs, (3) Explore the feasibility of expanding the pilot to an eventual statewide ECMHC model.
Our model used an open referral system, wherein leaders, teachers, and families could refer classrooms or individual children needing support. For classroom-level referrals, teachers completed a self-assessment to reflect on their social and emotional teaching practices. Teachers then engaged with consultants in four consultation cycles that included action planning with the consultant, teacher implementation of the action plan (videotaped when possible), and feedback sessions between the consultant and teacher after observing action plan implementation (for a more detailed model description, see Partee et al., 2023). For child-level referrals, consultants conducted baseline observations of social and emotional teaching practices and the referred child's engagement in the classroom. Teachers also completed ratings of the child's behavior. Teachers then engaged with consultants in seven consultation cycles, similar to the cycles described above, guided by consultants' initial observations. Consultants also supported teacher-family collaboration and facilitated referrals to community services as needed for child-level cases. This included family engagement sessions, where the consultant met with the family and teacher at least once toward the beginning of consultation to include the family in the consultation process, gain more information about the child's behavior, and inform decision-making. In this paper, we focus on child-level ECMHC cases and describe how data were used formatively to guide consultation.
We focus our analyses on the 100 preschool teachers and 109 preschool children who participated in child-level consultation from 2023 to 2024 and had baseline data, which included a teacher rating of child behavior, observational measure of child behavior, and observational measure of teaching practices described below. Teacher and child demographics are displayed in Table 1. In 2023–2024, there were six full-time and three part-time consultants. All nine consultants were women; 89% had held Master's degrees; 44% were Black, 56% were White, and 11% were Hispanic.
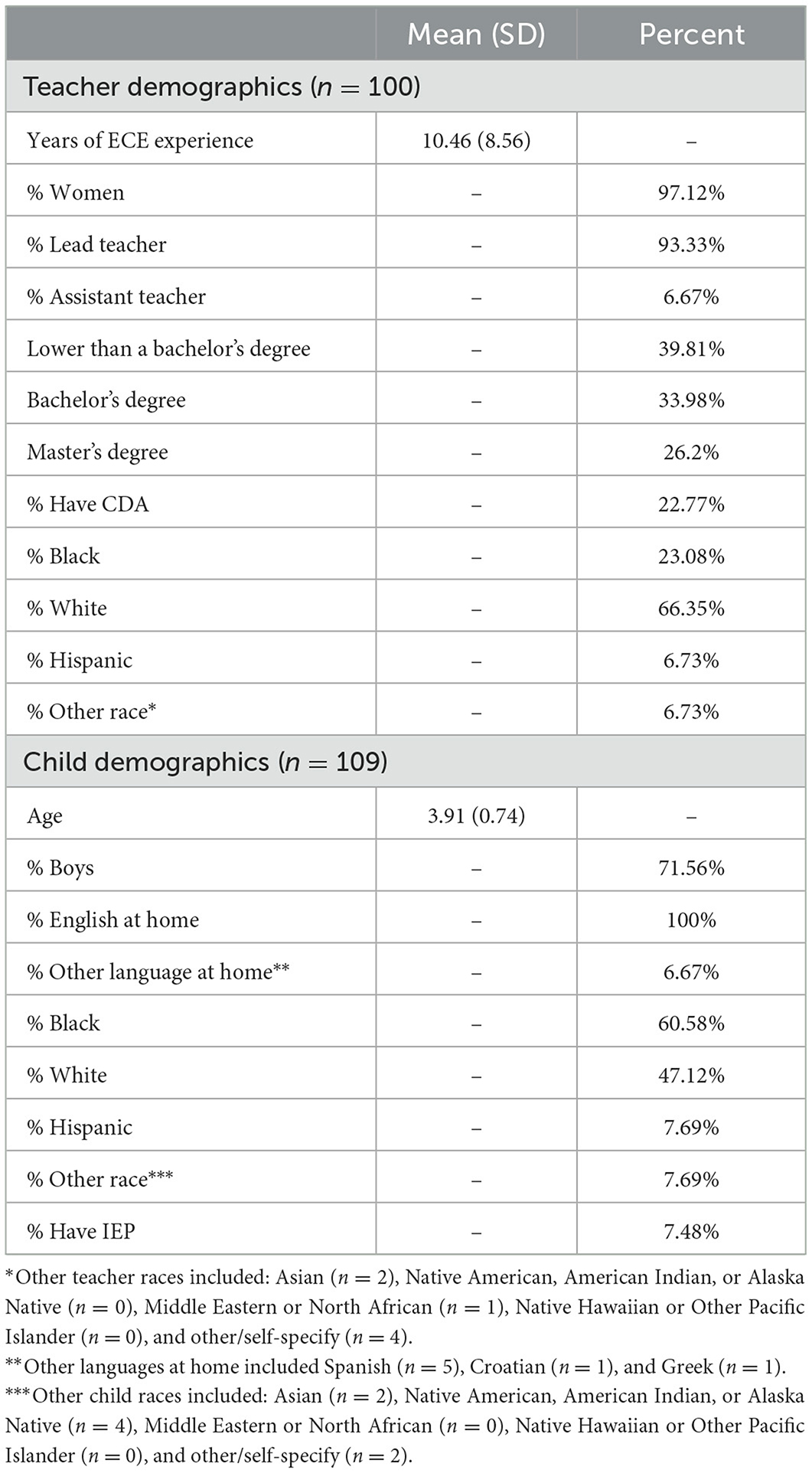
Table 1. Demographics of ECMHC teachers and children with baseline data.
At the beginning of consultation, teachers completed the Strengths and Difficulties Questionnaire (SDQ; Goodman, 1997) about the referred child's behavior, and consultants conducted classroom observations of child engagement, using the Individualized Classroom Assessment Scoring System (inCLASS; Downer et al., 2010), and teaching practices, using the Teaching Pyramid Observation Tool-Short Form (TPOT-S; Artman et al., 2008).
The SDQ measures challenging behaviors with 25 items across four subscales: emotional problems (e.g., “nervous or clingy in new situations, easily loses confidence”), conduct problems (e.g., “often fights with other children or bullies them”), hyperactivity (e.g., “restless, overactive, cannot stay still for long”), and peer problems (e.g., “rather solitary, tends to play alone”). Teachers rated each SDQ item on a scale of 0 (not true) to 2 (certainly true). Higher scores on the SDQ indicate more challenging child behavior (i.e., higher scores are worse).
The inCLASS is an observational measure of children's positive engagement with teachers, peers, and tasks and negative engagement (i.e., conflict) in the classroom. Scores are rated on a 7-point scale, with higher scores reflecting more positive engagement. To transform inCLASS scores into subscales consultants could easily use with teachers, we followed scoring procedures outlined by Williford et al. (2018) in the LOOK consultation model, described further below. Scores were generated for the following subscales of children's engagement in the classroom: Positive Teacher; Negative Teacher; Positive Peer; Negative Peer; Positive Task; Negative Task.
Consultants completed a 2-day inCLASS training and demonstrated reliability on the coding system before conducting inCLASS observations. Consultants conducted about 2 h of live classroom observation to collect four 15-min inCLASS cycles (10 min of observation and note taking, 5 min of coding) on the referred child. After the observation, consultants entered their raw inCLASS scores into a database (SmartSheet). Raw scores (averages across the four cycles) were converted into t-scores, and strengths and challenges were identified for high (t > 60) and low (t < 40) t-scores in line with previous use of the inCLASS for consultation purposes (Williford et al., 2018).
In addition to these child-level measures, consultants conducted an observation of classroom-wide behavioral support practices, using the Teaching Pyramid Observation Tool-Short Form (TPOT-S; Artman et al., 2008; Fox and Hemmeter, 2009). The TPOT-S was adapted from the full Teaching Pyramid Observation Tool (TPOT; Hemmeter et al., 2018), and we follow scoring procedures outlined by Artman et al. (2008). The TPOT-S includes 35 items across eight groups of strategies that support social and emotional development (e.g., classroom arrangement; transitions and routines; supporting emotion regulation). Eight items were indicator variables (consultants rated yes/no), and 27 items were rated on a scale from never (1) to almost always (4). If a consultant rated the frequency of a positive teaching practice (e.g., “Teachers adapt group directions to give additional help to children who need more support”; “Teachers support children in learning how to solve problems”) as occurring never or rarely, this teaching strategy was flagged. If a consultant rated a practice that was not desirable (e.g., “Transitions are chaotic”; “Teachers appear frustrated or frazzled in managing challenging child behaviors”) as occurring sometimes or almost always, that strategy would be flagged. For the purpose of consultation, areas of need were indicated when at least two TPOT-S items in a subscale were flagged.
Consultants were trained on the TPOT-S through a presentation and manual. Consultants completed the TPOT-S during the same inCLASS observation. Consultants scored the TPOT-S based on strategies observed during the previous inCLASS cycle, as well as ten additional minutes of observation at the classroom-level. After the observation, consultants entered their raw TPOT-S scores into a database.
Central to the Virginia ECMHC model, the scope and sequence of selected strategies depended on the observations of the classroom and child and teacher choice, supported by the consultant. Using data collected from key measures (described above), consultants supported teachers to strategically select from a list of recommended strategies (see Table 2), drawn from a menu of thirteen evidence-based teaching strategies. These strategies are organized into three categories: (1) Foundational Strategies designed to promote well-organized, engaging, warm, inclusive, and culturally responsive classroom environments (e.g., transitions and routines, teacher-child relationships), (2) Flexible Strategies that address challenging behavior and promote positive engagement across many contexts/settings (e.g., cues and visuals, effective instructions), and (3) Targeted Strategies that focus on skill-building (e.g., problem solving skills, emotion regulation). When multiple types of strategies were linked to the pre-consultation observation data, consultants were guided to begin with Foundational and Flexible strategies, before helping teachers implement Targeted strategies.
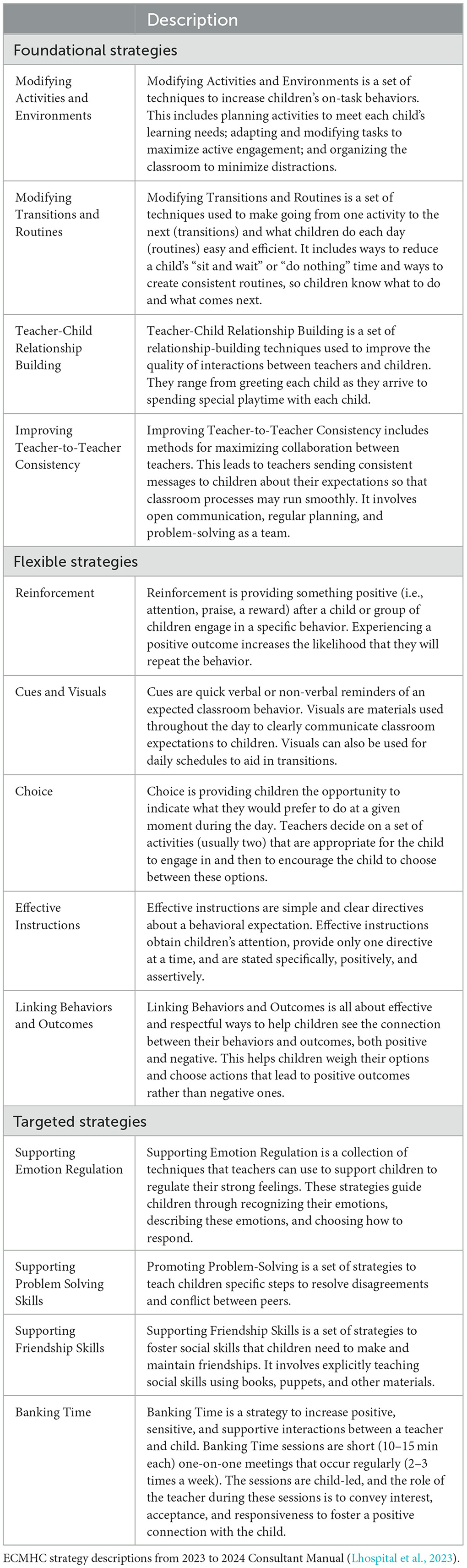
Table 2. ECMHC teaching strategies.
Standardized formulas used the TPOT-S and inCLASS scores to recommend strategies. This process of using data to guide consultation and formulas were adapted from the Learning to Objectively Observe Kids (LOOK) model of consultation (Downer et al., 2018; Williford et al., 2018). Scoring procedures were adapted from the way these measures are used for research purposes (Williford et al., 2018), and standardized inCLASS scores were generated for the following subscales of engagement: Positive Teacher; Negative Teacher; Positive Peer; Negative Peer; Positive Task; Negative Task. By looking at positive and negative engagement and using standardized scores comparing to a LOOK norm group, consultants assessed each child's areas of strength (i.e., high positive engagement or low negative engagement) and areas of challenge (i.e., low positive engagement or high negative engagement) relative to 3- to 5-year-old peers.
This process was designed such that different combinations of inCLASS and TPOT-S scores resulted in different teaching strategies being focused on in ECMHC. For example, if a child was observed to have low positive engagement and high negative engagement with peers (on the inCLASS) and the teacher was rated low on supporting peer interactions (on the TPOT-S), the consultant was provided the linked Targeted strategy of Supporting Friendship Skills. Based on this recommendation, the consultant and teacher may decide to focus on implementing this strategy (after covering any relevant Foundational Strategies, if recommended, such as Modifying Transitions and Routines). In contrast, another child may be doing well with their peers but have lower observed task engagement (on the inCLASS) and in a classroom where the teacher was rated low on the promoting and maintaining engagement (on the TPOT-S). In this case, the consultant and teacher may start with strategies that support higher child engagement with tasks, such as Modifying Activities and Environments (a Foundational strategy) as well as Choice and Reinforcement (Flexible strategies). We provide examples in the Results section to further illustrate how data were used to select teaching strategies of focus for consultation.
Consultants were supported to use data to select teaching strategies, while also individualizing based on the unique context and needs of teachers and children. For example, though the SDQ was not used in formulas to generate recommended teaching strategies, consultants were encouraged to examine teacher ratings and use this information in consultation. Consultants were encouraged to compare teacher ratings with their observations of child engagement, noting areas of similarity in child challenges to help guide goal setting. Consultants could also comment to teachers on differences noticed between ratings and observations as a foray into helping support teachers to reflect on their “lenses” for (i.e., perceptions of) children's behavior (Partee et al., 2023).
After the observation, consultants entered their raw inCLASS and TPOT-S scores into a database (i.e., SmartSheet). Within 24 h of consultants' data entry into the Smartsheet forms, a member of the research team entered data into an individualized ECMHC Data workbook in Excel. Each child-level referral had a workbook, where data were analyzed using the same standardized formula, and teaching strategies were recommended based on these scores in a user-friendly format. This included averages and t-scores of the adapted inCLASS domains and the number of flags for each TPOT-S dimension. Areas of strength (color-coded green) and areas of need (color-coded red) were identified for the inCLASS, TPOT-S, and SDQ. The workbook then auto-generated a “Recommended Strategies” table based on the needs identified, reflected in Table 3.
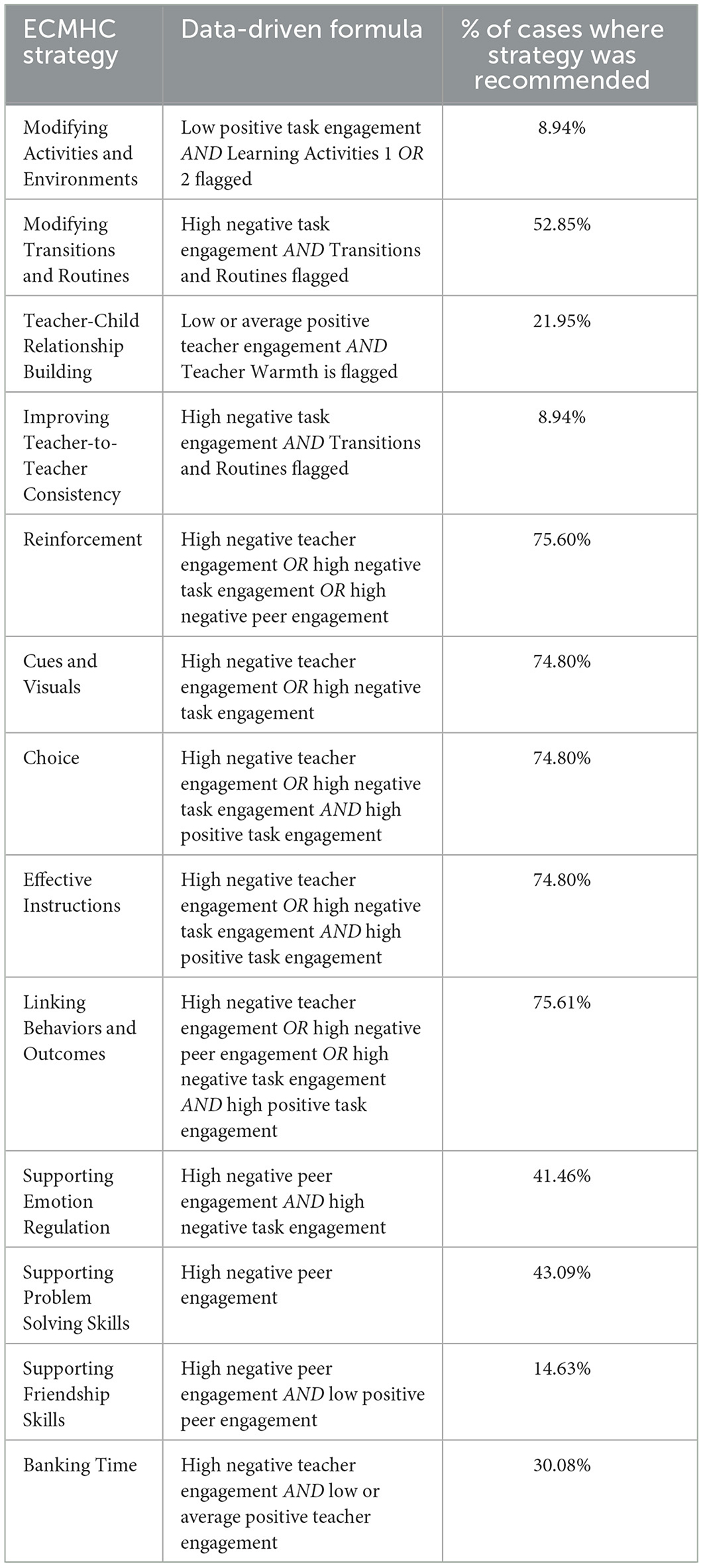
Table 3. Strategy selection in ECMHC cases.
In our results, we provide descriptive information on child and teacher measures before services began and how these scores resulted in different recommended strategies (aim 1) and present individual examples of how pre-consultation data resulted in different strategies being targeted in ECMHC (aim 2). We discuss strategy selection patterns in the data and highlight three specific case examples of different pre-consultation scores and how initial teaching strategies covered in consultation varied as a result.
We examined descriptive statistics of baseline SDQ, inCLASS, and TPOT-S (see Table 4). In terms of teacher reports of child behavior, scores were highest for hyperactivity and conduct problems and lowest for emotional problems. Correlations between the subdomains were positive and low to moderate in strength, ranging from 0.06 (p = 0.48; hyperactivity and emotional problems) to 0.32 (p < 0.001; hyperactivity and conduct problems). In terms of inCLASS scores, observed positive engagement was highest for task engagement and lowest for peer engagement. Observed negative engagement was also highest for task engagement and lowest for peer engagement. Domain scores were positively and moderately correlated for positive engagement, ranging from 0.39 (p < 0.001; teacher and peer) to 0.54 (p < 0.001; peer and task). For negative engagement, correlations ranged from 0.50 (p < 0.001; teacher and peer) to 0.58 (p < 0.001; peer and task). These correlations suggest that children with high positive engagement tended to be high on all three positive domains, and children with high negative engagement tended to be high on all three negative domains.
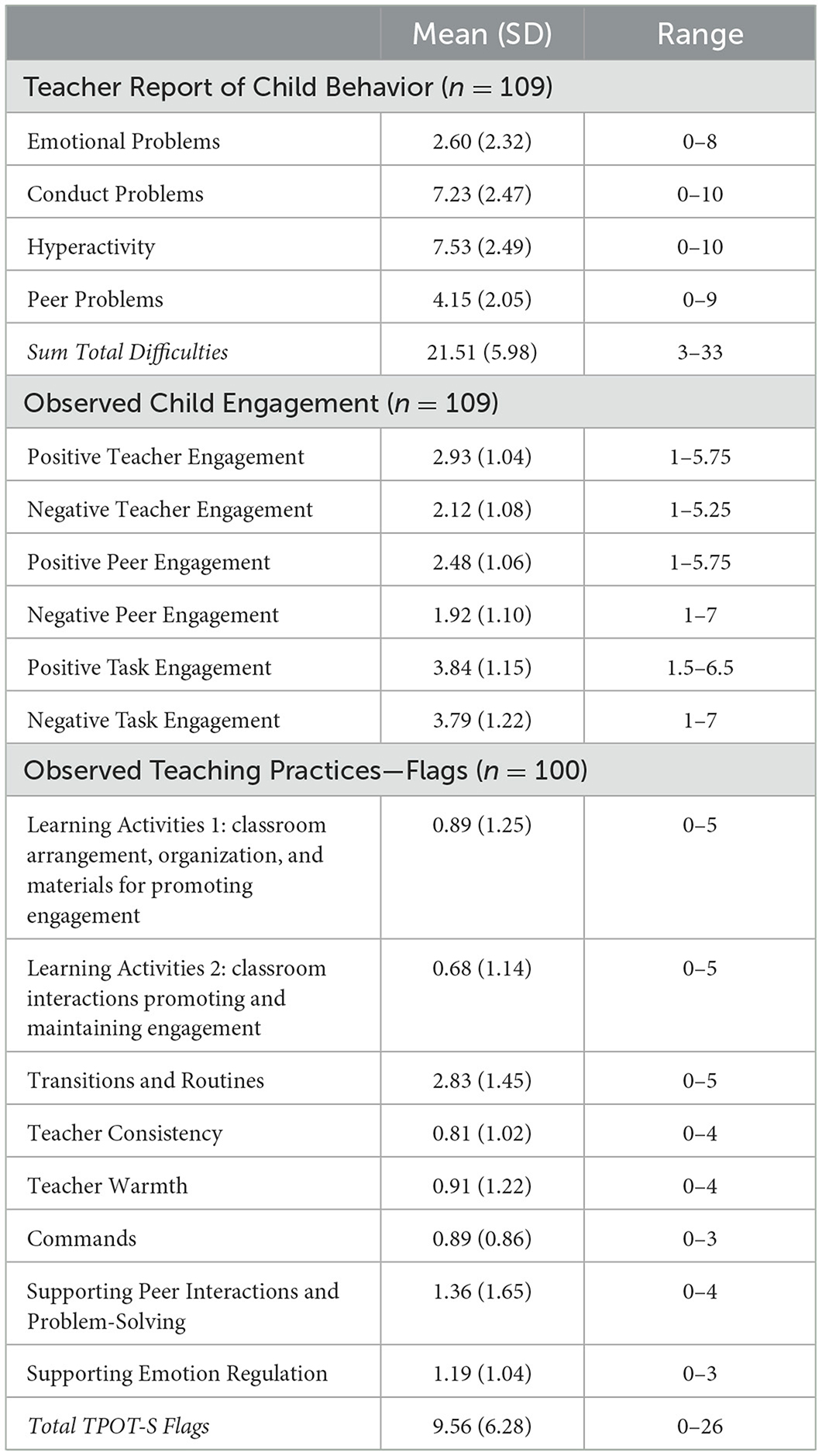
Table 4. Pre-consultation descriptive statistics.
For TPOT-S observations, the subdomain Transitions and Routines had the highest average flags, followed by Supporting Peer Interactions and Problem-Solving, and Supporting Emotion Regulation. This suggests that these domains were the most in need of attention during consultation, compared to other TPOT-S domains. Most TPOT-S domains were significantly correlated, except for the first learning activities domain which was only correlated with Learning Activities 2 and Transitions and Routines. For the other domains, correlations ranged from 0.19 (p = 0.05; Teacher Consistency and Supporting Emotion Regulation) to 0.52 (p < 0.001; Teacher Warmth and Supporting Peer Interactions and Problem-Solving).
We next examined how often each strategy was recommended in the full sample of cases served. On average, 5.98 (SD = 3.68, range 0–13) strategies were recommended based on baseline data. A breakdown of how often each strategy was recommended is presented in Table 3. The five Flexible strategies (Reinforcement, Cues and Visuals, Choice, Effective Instructions, Linking Behaviors and Outcomes) were most commonly recommended, with each being recommended in over 70% of cases. These strategies tended to be recommended together, with 74.80% of cases being recommended all five. Modifying Transitions and Routines was also commonly recommended in over half of cases. Modifying Activities and Environments and Improving Teacher-to-Teacher Consistency were recommended the least often, in fewer than 9% of cases.
To provide examples of how data guided consultation, we selected three real case examples served by three different consultants. Each example was selected based on pre-consultation z-scores on the SDQ, inCLASS, and TPOT-S to maximize variability in examples presented (i.e., z-scores around 1, 0, and −1). Example 1 includes a child with consistently low positive engagement, high negative engagement, and a teacher with a very high number of flagged teaching strategies. Example 2 includes a child with high negative engagement in combination with high positive engagement and a teacher with a moderate number of flagged teaching strategies. Finally, example 3 includes a child with a mix of low and high positive engagement and a teacher with an average number of flagged teaching strategies. Averages for each case are shown in Table 5. Each pre-consultation profile is described in more detail below, and recommended strategies based on these data are also provided.
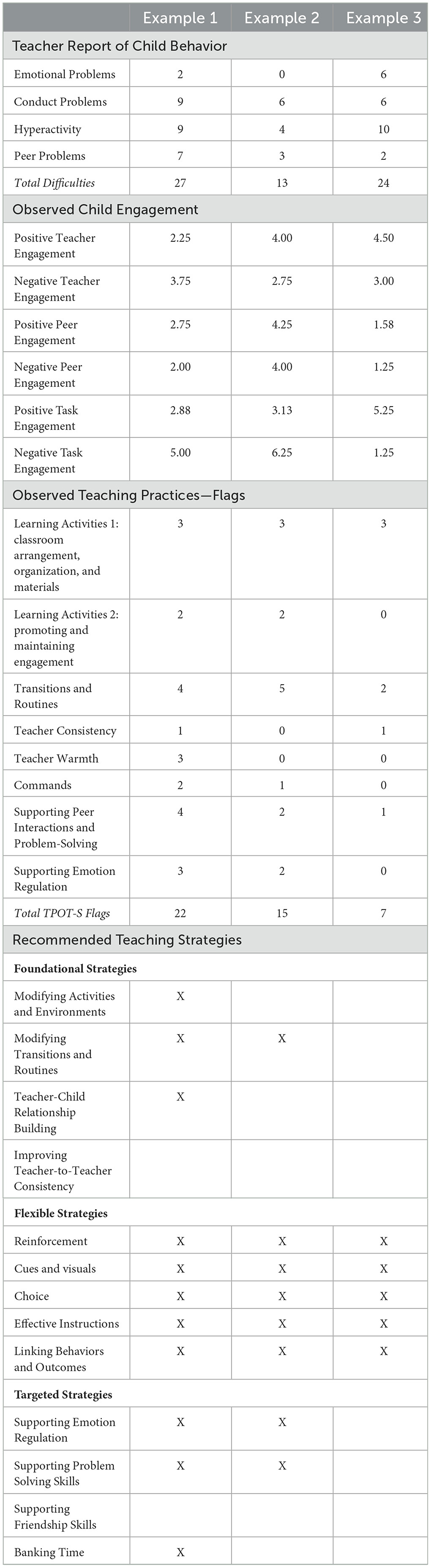
Table 5. Pre-consultation descriptive statistics for selected cases.
The case presented in example 1 focused on a 3.2-year-old boy referred to consultation for being “disruptive, defiant to teachers and parents, no remorse for actions and doesn't listen to adults.” Before consultation, this child had low positive engagement and high negative engagement with his teacher, peers, and tasks. His teacher also had a very high number of teaching strategies flagged on the TPOT-S. Based on this pre-consultation data, 11 of the 13 ECMHC strategies were recommended. His teacher engaged in consultation from January to June 2024. Over these months, the teacher and consultant engaged in a kickoff meeting and seven focused consultation sessions. During the first ECMHC meeting, the consultant and teacher collaboratively chose to focus on the foundational strategy Modifying Transitions and Routines, in line with the data-driven recommendations. Based on consultation report, the following additional teaching strategies were covered during consultation: Modifying Activities and Environments, Effective Instructions, Linking Behaviors and Outcomes, Supporting Emotion Regulation, Supporting Problem Solving Skills, and Supporting Friendship Skills.
The case presented example 2 focused on 3.3-year-old boy referred to consultation by his program leader for “aggression, regression, and fearfulness of adult figures” as well as the family having expressed that they do not have the tools to support him. Before consultation, this child had both high positive engagement and high negative engagement with his teacher, peers, and tasks. His teacher also had a moderate number of teaching strategies flagged on the TPOT-S. Based on this pre-consultation data, eight of the 13 ECMHC strategies were recommended, including a mix of Foundational, Flexible, and Targeted strategies. His teacher engaged in consultation from September 2023 to January 2024. The teacher and consultant engaged in a kickoff meeting and four focused consultation sessions. The consultant also facilitated three family engagement sessions. During the first ECMHC meeting, the consultant and teacher collaboratively chose to focus on the flexible strategy Linking Behaviors and Outcomes, in line with the data-driven recommendations. Based on consultation report, the following additional teaching strategies were covered during consultation: Modifying Activities and Environments, Modifying Transitions and Routines, and Improving Teacher-to-Teacher Consistency.
The case presented example 3 focused on a 2.95-year-old boy referred to consultation by his program leader for being unable to control his behavior and disturbing the classroom. Before consultation, this child had high positive and negative engagement with his teacher, low positive and negative engagement with peers, and high positive engagement with tasks. His teacher also had an average number of teaching strategies flagged on the TPOT-S. Based on this pre-consultation data, five of the 13 ECMHC strategies were recommended. All strategies recommended were Flexible; no Foundational or Targeted strategies were recommended based on the pre-consultation observations. His teacher engaged in consultation from December 2023 to April 2024. Over these 5 months, his teacher and consultant engaged in a kickoff meeting and five focused consultation sessions. The consultant also facilitated two family engagement sessions. During the first ECMHC meeting, the consultant and teacher collaboratively chose to focus on the flexible Cues and Visuals strategy, in line with the data-driven recommendations. Based on consultation report, the following additional teaching strategies were covered during consultation: Effective Instructions and Linking Behaviors and Outcomes.
ECMHC builds the capacity of early childhood educators to support children displaying challenging behaviors in an inclusive way. These efforts directly address the use of exclusionary practices that remove children from the classroom in inequitable ways based on child race, gender, and disability. In this paper, we described how in an ECMHC model used in Virginia, consultants used a data-driven approach to identify teacher, child, and classroom needs and select teaching strategies through baseline observations to guide the consultation process in a way that builds educator capacity to support social and emotional development. In doing so, the model balances standardizing an intervention to ensure high fidelity of implementation as it is scaled up while also encouraging individualization based on teachers' and children's unique strengths and challenges. This paper has implications for how we promote evidence-based strategies to address individual needs in early childhood settings, including through ECMHC and other professional development.
In the Virginia ECMHC pilot, consultants supported educators to learn and use evidence-based teaching strategies to support the inclusion of children with social, emotional, or behavioral challenges in their learning environment. Our model used baseline classroom and child observational data to help consultants and educators identify areas of child and teacher need and aligned teaching strategies. Data was collected using in-context observations and teacher reports, allowing for consultants to have a fuller picture of the child's engagement in the classroom and from the teacher's perspective. Using this data, consultants and teachers selected strategies from a menu of 13 social and emotional teaching strategies to focus on during consultation. This collaborative process allowed for data to guide consultation while also leaving room for flexibility. For example, if four strategies were recommended based on the data, the teacher and consultant would choose one to begin with, providing more autonomy for teachers and increasing buy-in and motivation to engage in ECMHC.
Our data provides evidence that the baseline data collection and subsequent data-driven process for selecting strategies worked as intended. In a sample of children with elevated behavior challenges and at risk of being excluded through suspension or expulsion, we saw a range of scores on the teacher-report and observations of child engagement and classroom practices. This variability led to different recommended strategies, resulting in distinct scopes and sequences of ECMHC strategies covered. Based on our findings, we see this approach to ECMHC as both feasible and effective at resulting in individualized consultation paths. Additional research is needed to replicate this approach, ideally in a larger sample. Future research could also incorporate consultant and teacher feedback to understand qualitatively how the baseline data was used and perceived to support consultation.
We found that flexible strategies (i.e., Reinforcement, Cues and Visuals, Choice, Effective Instructions, and Linking Behaviors and Outcomes) were most commonly recommended. Further, they were usually recommended together, with about 75% of cases being recommended all five. This pattern makes sense, given the similarities in the data-driven guidelines for recommending each. Further, these five strategies are essential strategies for teachers to feel comfortable using and use effectively across situations, especially when young children are engaging in challenging behavior. Modifying Transitions and Routines was also commonly flagged, with over 50% of cases recommended this strategy. With all 13 strategies, teachers were eventually also encouraged to generalize their use to the larger classroom environment to promote inclusion and social and emotional development of all children, not just the child who was the focus of consultation. All of the 13 strategies, when implemented with fidelity, create more organized and predictable classrooms and are associated with more positive child behavior (Downer et al., 2018; Hemmeter et al., 2022).
ECMHC is an evidence-based intervention associated with lower teacher stress (Zinsser et al., 2019), improvements in children's social and emotional skills (Downer et al., 2018), and reductions in exclusionary discipline practices (Conners Edge et al., 2021). In this paper, we describe one model of ECMHC in Virginia and how it was designed to build educator capacity through a data-driven collaborative process that balanced standardization with individualization. This process allowed consultants to support educators to select and implement teaching strategies that support social and emotional development, such as fostering strong teacher-child relationships, using cues and visuals, and supporting problem-solving skills. Central to the ECMHC theory of change, consultants also sought to boost educator capacity to reflect on how they perceived children's behavior, interrupt any biases, and promote more inclusive teaching practices (Partee et al., 2023; Schoch et al., 2024). This ECMHC model supported inclusion by equipping educators with the strategies, confidence, and support to promote children's social and emotional development and address challenging behavior. Future research exploring if, when, and how data are used within large ECMHC initiatives can help the field better understand how data can be leveraged to unpack ECMHC mechanisms of change that result in positive outcomes for educators and children, ultimately increasing ECHMC's impact and use at scale.
The datasets presented in this article are not readily available because the team does not have permission to share externally. Requests to access the datasets should be directed to Kelsey A. Clayback, a2FjNWZkQHZpcmdpbmlhLmVkdQ==.
The studies involving humans were approved by University of Virginia Institutional Review Board for the Social and Behavioral Sciences. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin.
KC: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Visualization, Writing – original draft, Writing – review & editing. AP: Conceptualization, Data curation, Funding acquisition, Investigation, Methodology, Project administration, Writing – review & editing. AW: Conceptualization, Funding acquisition, Methodology, Supervision, Writing – review & editing. JD: Conceptualization, Funding acquisition, Methodology, Supervision, Writing – review & editing. KP: Investigation, Writing – review & editing. AL: Investigation, Project administration, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This paper was produced by the authors as part of the ECMHC initiative, a partnership between the Virginia Department of Education (VDOE) and UVA-CASTL and funded by VDOE. The opinions expressed are those of the authors and do not represent the views of VDOE.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Alamos, P., and Williford, A. P. (2023). A conceptual model to understand and address racial disparities in exclusionary discipline through teacher-child relationships. Early Child. Res. Q. 65, 363–373. doi: 10.1016/j.ecresq.2023.08.003
Albritton, K., Mathews, R. E., and Anhalt, K. (2019). Systematic review of early childhood mental health consultation: implications for improving preschool discipline disproportionality. J. Educ. Psychol. Consult. 29, 444–472. doi: 10.1080/10474412.2018.1541413
Artman, K., Hemmeter, M. L., Feeney-Kettler, K., and Meiler, C. (2008). Observation Toolkit for Mental Health Consultants. Available at: https://www.ecmhc.org/documents/CECMHC_Observation_Toolkit.pdf (accessed August 10, 2024).
Bassok, D., Markowitz, A. J., Bellows, L., and Sadowski, K. (2021). New evidence on teacher turnover in early childhood. Educ. Eval. Policy Anal. 43, 172–180. doi: 10.3102/0162373720985340
Berlin, L. J., Shdaimah, C. S., Goodman, A., and Slopen, N. (2020). “I‘m literally drowning”: a mixed-methods exploration of infant-toddler child care providers' wellbeing. Early Educ. Dev. 31, 1071–1088. doi: 10.1080/10409289.2020.1766915
Blewitt, C., O'Connor, A., Morris, H., May, T., Mousa, A., Bergmeier, H., et al. (2021). A systematic review of targeted social and emotional learning interventions in early childhood education and care settings. Early Child Dev. Care 191, 2159–2187. doi: 10.1080/03004430.2019.1702037
Bromley, A. R. (2023). Flexibility within fidelity: a narrative review of practitioner modifications to child welfare interventions. Child. Youth Serv. Rev. 149:106908. doi: 10.1016/j.childyouth.2023.106908
Buell, M., Fidel, R., Hustedt, J. T., Kuntz, S., and Slicker, G. (2022). From time-out to expulsion: a national review of states' center-based child care licensing exclusionary discipline regulations. Child Youth Serv. Rev. 141:106623. doi: 10.1016/j.childyouth.2022.106623
Bulotsky-Shearer, R. J., Fantuzzo, J. W., and McDermott, P. A. (2008). An investigation of classroom situational dimensions of emotional and behavioral adjustment and cognitive and social outcomes for head start children. Dev. Psychol. 44, 139–154. doi: 10.1037/0012-1649.44.1.139
Clayback, K. A., and Hemmeter, M. L. (2021). Exclusionary discipline practices in early childhood settings: a survey of child care directors. Early Child. Res. Q. 55, 129–136. doi: 10.1016/j.ecresq.2020.11.002
Clayback, K. A., LoCasale-Crouch, J., and Alamos, P. (2024). A pilot study of a micro-course to promote positive teaching practices and prevent exclusionary discipline in early childhood. Early Child. Res. Q. 67, 182–190. doi: 10.1016/j.ecresq.2023.12.010
Clayback, K. A., and Williford, A. P. (2022). Teacher and classroom predictors of preschool teacher stress. Early Educ. Dev. 33, 1347–1363. doi: 10.1080/10409289.2021.1972902
Cohen, E., and Kaufmann, R. (2005). Early Childhood Mental Health Consultation. DHHS pub. No. CMHS-SVP0151, Center for Mental Health Services, Substance Abuse and Mental Health Services Administration.
Conners Edge, N. A., Kyzer, A., Davis, A. E., and Whitman, K. (2021). Infant and early childhood mental health consultation in the context of a statewide expulsion prevention initiative. J. Educ. Psychol. Consult. 0, 1–22. doi: 10.1080/10474412.2021.1983440
Connors, E. H., Childs, A. W., Douglas, S., and Jensen-Doss, A. (2024). Data-informed communication: how measurement-based care can optimize child psychotherapy. Administr. Policy Mental Health Mental Health Serv. Res. doi: 10.1007/s10488-024-01372-4. [Epub ahead of print].
Davis, A. E., Barrueco, S., and Perry, D. F. (2020a). The role of consultative alliance in infant and early childhood mental health consultation: child, teacher, and classroom outcomes. Infant Mental Health J. 42, 246–262. doi: 10.1002/imhj.21889
Davis, A. E., Perry, D. F., and Rabinovitz, L. (2020b). Expulsion prevention: framework for the role of infant and early childhood mental health consultation in addressing implicit biases. Infant Ment. Health J. 41, 327–339. doi: 10.1002/imhj.21847
Doromal, J. B., Bassok, D., Bellows, L., and Markowitz, A. J. (2022). Hard-to-staff centers: exploring center-level variation in the persistence of child care teacher turnover. Early Child. Res. Q. 61, 170–178. doi: 10.1016/j.ecresq.2022.07.007
Downer, J. T., Booren, L. M., Lima, O. K., Luckner, A. E., and Pianta, R. C. (2010). The individualized classroom assessment scoring system (inCLASS): preliminary reliability and validity of a system for observing preschoolers' competence in classroom interactions. Early Child. Res. Q. 25, 1–16.
Downer, J. T., Williford, A. P., Bulotsky-Shearer, R. J., Vitiello, V. E., Bouza, J., Reilly, S., et al. (2018). Using data-driven, video-based early childhood consultation with teachers to reduce children's challenging behaviors and improve engagement in preschool classrooms. Sch. Ment. Health 10, 226–242. doi: 10.1007/s12310-017-9237-0
Fox, L., and Hemmeter, M. L. (2009). “A programwide model for supporting social emotional development and addressing challenging behavior in early childhood settings. in Handbook of Positive Behavior Support, eds. W. Sailor, G. Dunlap, G. Sugai, and R. Horner (Springer), 177–202. doi: 10.1007/978-0-387-09632-2_8
Friedman-Krauss, A. H., Raver, C. C., Morris, P. A., and Jones, S. M. (2014). The role of classroom-level child behavior problems in predicting preschool teacher stress and classroom emotional climate. Early Educ. Dev. 25, 530–552. doi: 10.1080/10409289.2013.817030
Galovski, T. E., Nixon, R. D. V., and Kehle-Forbes, S. S. (2024). Walking the line between fidelity and flexibility: A conceptual review of personalized approaches to manualized treatments for posttraumatic stress disorder. J. Traum. Stress. 36, 1–10. doi: 10.1002/jts.23073
Garrity, S. M., Longstreth, S. L., Linder, L. K., and Salcedo Potter, N. (2019). Early childhood education centre director perceptions of challenging behaviour: promising practices and implications for professional development. Child. Soc. 33, 168–184. doi: 10.1111/chso.12306
Gilliam, W. S., and Reyes, C. R. (2018). Teacher decision factors that lead to preschool expulsion: scale development and preliminary validation of the preschool expulsion risk measure. Infants Young Child. 31, 93–108. doi: 10.1097/IYC.0000000000000113
Giordano, K., Interra, V. L., Stillo, G. C., Mims, A. T., and Block-Lerner, J. (2021). Correction to: Associations between child and administrator race and suspension and expulsion rates in community childcare programs. Early Childh. Educ. J. 49:135. doi: 10.1007/s10643-020-01057-1
Goodman, R. (1997). The strengths and difficulties questionnaire: A research note. J. Child Psychol. Psychiatry 38, 581–586.
Hemmeter, M. L., Fox, L., Snyder, P., Algina, J., Hardy, J. K., Bishop, C., et al. (2022). Corollary child outcomes from the Pyramid Model professional development intervention efficacy trial. Early Child. Res. Q. 54, 204–218. doi: 10.1016/j.ecresq.2020.08.004
Hemmeter, M. L., Ostrosky, M. M., and Fox, L., (eds.). (2021). Unpacking the Pyramid Model: A Practical Guide for Preschool teachers. Paul H. Brookes.
Hemmeter, M. L., Snyder, P., and Fox, L. (2018). Using the Teaching Pyramid Observation Tool (TPOT) to support implementation of social–emotional teaching practices. Sch. Ment. Health 10, 202–213. doi: 10.1007/s12310-017-9239-y
Jeon, L., Buettner, C. K., and Grant, A. A. (2018). Early childhood teachers' psychological well-being: exploring potential predictors of depression, stress, and emotional exhaustion. Early Educ. Dev. 29, 53–69. doi: 10.1080/10409289.2017.1341806
Kendall, P. C., Ney, J. S., Maxwell, C. A., Lehrbach, K. R., Jakubovic, R. J., McKnight, D. S., et al. (2023). Adapting CBT for youth anxiety: flexibility, within fidelity, in different settings. Front. Psychiatry 14:1067047. doi: 10.3389/fpsyt.2023.1067047
Lang, S. N., Tebben, E., Odean, R., Wells, M. B., and Huang, H. (2024). Inequities in coaching interventions: a systematic review of who receives and provides coaching within early care and education. Child Youth Care For. 53, 141–171. doi: 10.1007/s10566-023-09748-7
Lee, J. D., Meadan, H., Kang, V. Y., and Terol, A. K. (2023). Balancing fidelity and flexibility of manualized interventions in cultural adaptation: issues to consider. Educ. Treat. Child. 46, 263–273. doi: 10.1007/s43494-023-00102-z
Lewis, C. C., Boyd, M., Puspitasari, A., Navarro, E., Howard, J., Kassab, H., et al. (2019). Implementing measurement-based care in behavioral health: a review. JAMA Psychiatry 76:324. doi: 10.1001/jamapsychiatry.2018.3329
Lhospital, A., Altman, S., Clayback, K., Bivona, M., Therber, G., Johnson, M., et al. (2023). Virginia Early Childhood Mental Health Consultation (ECMHC) Consultancy Manual, 2023-2024 (Unpublished manual). University of Virginia.
Loomis, A., Davis, A., Cruden, G., Padilla, C., and Drazen, Y. (2022). Early childhood suspension and expulsion: a content analysis of state legislation. Early Childh. Educ. J. 50, 327–344. doi: 10.1007/s10643-021-01159-4
Mathis, E., Hartz, K., Berkowitz, M., Carlson, A., Kimport, R., Brown, C., et al. (2025). Infant and early childhood mental health consultation: evaluating change in classroom climate and teaching practices by dosage of program exposure. Early Child. Res. Q. 70, 52–64. doi: 10.1016/j.ecresq.2024.08.009
McClelland, M. M., Tominey, S. L., Schmitt, S. A., and Duncan, R. (2017). SEL interventions in early childhood. Fut. Child. 27, 33–47. doi: 10.1353/foc.2017.0002
McLean, C., Austin, L. J. E., Whitebook, M., and Olson, K. L. (2021). Early Childhood Workforce Index – 2020. Berkeley, CA: Center for the Study of Child Care Employment, University of California, Berkeley. Available at: https://cscce.berkeley.edu/workforce-index-2020/report-pdf/ (accessed August 10, 2024).
Mondi, C. F., Rihal, T. K., Magro, S. W., Kerber, S., and Carlson, E. A. (2022). Childcare providers' views of challenging child behaviors, suspension, and expulsion: a qualitative analysis. Infant Ment. Health J. 43, 695–713. doi: 10.1002/imhj.22005
Obee, A. F., Hart, K. C., and Fabiano, G. A. (2023). professional development targeting classroom management and behavioral support skills in early childhood settings: a systematic review. Sch. Ment. Health 15, 339–369. doi: 10.1007/s12310-022-09562-x
O'Grady, C., and Ostrosky, M. M. (2021). Suspension and expulsion: early educators' perspectives. Early Child. Educ. J. 51, 115–125.
Partee, A. M., Sachdeva, S., Bivona, M. A., Clayback, K. A., Miller-Marshall, S., Parker, K., et al. (2023). Implementation of an early childhood mental health consultation pilot in Virginia: critical tensions and implications for scale-up. Front. Educ. 8:1070591. doi: 10.3389/feduc.2023.1070591
Pickard, K., Mellman, H., Frost, K., Reaven, J., and Ingersoll, B. (2021). Balancing fidelity and flexibility: usual care for young children with an increased likelihood of having autism spectrum disorder within an early intervention system. J. Autism Dev. Disord. 53, 656–668. doi: 10.1007/s10803-021-04882-4
Pickard K. Wainer A. Broder-Fingert S. Sheldrick R. C. and Stahmer A. C. (2022). Overcoming tensions between family-centered care and fidelity within early intervention implementation research. Autism 27, 858–863. doi: 10.1177/13623613221133641
Roberts, A. M., Gallagher, K. C., Daro, A. M., Iruka, I. U., and Sarver, S. L. (2019). Workforce well-being: personal and workplace contributions to early educators' depression across settings. J. Appl. Dev. Psychol. 61, 4–12. doi: 10.1016/j.appdev.2017.09.007
Schoch, A. D., Tidus, K. M., Catherine, E., Perry, D. F., Duran, F., and Rabinovitz, L. (2024). Essential elements of infant and early childhood mental health consultation: inside the black box of preschool expulsion prevention. Early Child. Res. Q. 66, 24–33. doi: 10.1016/j.ecresq.2023.08.005
Scott, K., and Lewis, C. C. (2015). Using measurement-based care to enhance any treatment. Cogn. Behav. Pract. 22, 49–59. doi: 10.1016/j.cbpra.2014.01.010
Silver, H. C., Davis Schoch, A. E., Loomis, A. M., Park, C. E., and Zinsser, K. M. (2023). Updating the evidence: a systematic review of a decade of Infant and Early Childhood Mental Health Consultation (IECMHC) research. Infant Ment. Health J. 44, 5–26. doi: 10.1002/imhj.22033
Silver, H. C., and Zinsser, K. M. (2020). The interplay among early childhood teachers' social and emotional well-being, mental health consultation, and preschool expulsion. Early Educ. Dev. 31, 1133–1150. doi: 10.1080/10409289.2020.1785267
Snell, M. E., Berlin, R. A., Voorhees, M. D., Stanton-Chapman, T. L., and Hadden, S. (2012). A survey of preschool staff concerning problem behavior and its prevention in Head Start classrooms. J. Posit. Behav. Interv. 14, 98–107. doi: 10.1177/1098300711416818
Spielberger, J., Burkhardt, T., Carreon, E. D., and Gitlow, E. R. (2024). Fostering healthy social and emotional climates in early childhood classrooms through infant and early childhood mental health consultation. Early Child. Res. Q. 67, 307–319. doi: 10.1016/j.ecresq.2024.01.009
Sutherland, K. S., Conroy, M. A., Algina, J., Ladwig, C., Jessee, G., and Gyure, M. (2018). Reducing child problem behaviors and improving teacher-child interactions and relationships: a randomized controlled trial of BEST in CLASS. Early Child. Res. Q. 42, 31–43. doi: 10.1016/j.ecresq.2017.08.001
U. S. Department of Education Office for Civil Rights (2014). Civil Rights Data Collection: Data Snapshot: Early Childhood Education. Available at: https://www2.ed.gov/about/office~s/list/ocr/docs/crdc-early-learning-snapshot.pdf (accessed August 10, 2024).
Whitaker, R. C., Becker, B. D., Herman, A. N., and Gooze, R. A. (2013). The physical and mental health of head start staff: The Pennsylvania Head Start Staff Wellness Survey, 2012. Prev. Chronic Dis. 10:130171. doi: 10.5888/pcd10.130171
Whitebook, M., Phillips, D., and Howes, C. (2014). Worthy Work, STILL Unlivable Wages: The Early Childhood Workforce 25 Years After the National Child Care Staffing Study. Berkeley, CA: Center for the Study of Child Care Employment, University of California. Available at: https://cscce.berkeley.edu/publications/report/worthy-work-still-unlivable-wages/ (accessed August 10, 2024).
Williams, N. J., Marcus, S. C., Ehrhart, M. G., Sklar, M., Esp, S. M., Carandang, K., et al. (2023). Randomized trial of an organizational implementation strategy to improve measurement-based care fidelity and youth outcomes in community mental health. J. Am. Acad. Child Adolesc. Psychiatry 63, 991–1004. doi: 10.1016/j.jaac.2023.11.010
Williford, A. P., Alamos, P., Whittaker, J. E., and Accavitti, M. R. (2023). Missing out: kindergarten teachers' reports of soft exclusionary discipline practices. Early Educ. Dev. 35, 1827–1846. doi: 10.1080/10409289.2023.2291745
Williford, A. P., Bulotsky-Shearer, R., Bichay, K., Reilly, S., and Downer, J. T. (2018). Adapting assessments of child engagement to develop an early childhood consultation model. J. Appl. Dev. Psychol. 56, 67–78. doi: 10.1016/j.appdev.2018.01.005
Wymer, S. C., Corbin, C. M., and Williford, A. P. (2022). The relation between teacher and child race, teacher perceptions of disruptive behavior, and exclusionary discipline in preschool. J. Sch. Psychol. 90, 33–42. doi: 10.1016/j.jsp.2021.10.003
Yoder, M. L., and Williford, A. P. (2019). Teacher perception of preschool disruptive behavior: Prevalence and contributing factors. Early Educ. Dev. 30, 835–853. doi: 10.1080/10409289.2019.1594531
Zeng, S., Pereira, B., Larson, A., Corr, C. P., O'Grady, C., and Stone-MacDonald, A. (2020). Preschool suspension and expulsion for young children with disabilities. Except. Child. 87, 199–216. doi: 10.1177/0014402920949832
Zinsser, K. M., Silver, H. C., Shenberger, E. R., and Jackson, V. (2022). A systematic review of early childhood exclusionary discipline. Rev. Educ. Res. 92, 743–785. doi: 10.3102/00346543211070047
Keywords: early childhood mental health consultation, data-driven, early childhood education, classroom observation, challenging behavior, social and emotional teaching practices
Citation: Clayback KA, Partee AM, Williford AP, Downer JT, Parker K and Lhospital AS (2025) Using data to promote inclusion through early childhood mental health consultation. Front. Educ. 9:1494378. doi: 10.3389/feduc.2024.1494378
Received: 10 September 2024; Accepted: 05 December 2024;
Published: 10 January 2025.
Edited by:
Huichao Xie, University College Dublin, IrelandReviewed by:
Celene Domitrovich, Georgetown University, United StatesCopyright © 2025 Clayback, Partee, Williford, Downer, Parker and Lhospital. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kelsey A. Clayback, a2FjNWZkQHZpcmdpbmlhLmVkdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.