 Fanan Ujoh1*
Fanan Ujoh1* Anja Dzunic-Wachilonga2
Anja Dzunic-Wachilonga2 Rafat Noor2
Rafat Noor2 Victoria Gusa3Roseline Ape-aii4Isaac Ohene1Rajan Bola5Jan Christilaw1
Victoria Gusa3Roseline Ape-aii4Isaac Ohene1Rajan Bola5Jan Christilaw1 Stephen Hodgins2
Stephen Hodgins2 Ronald Lett1
Ronald Lett1- 1Canadian Network for International Surgery (CNIS), Vancouver, BC, Canada
- 2School of Public Health, University of Alberta, Edmonton, AB, Canada
- 3School of Midwifery, Makurdi, Nigeria
- 4School of Midwifery, Mkar, Benue, Nigeria
- 5University of British Columbia, Vancouver, BC, Canada
Background: Many health education institutions in African countries such as Nigeria face increasing enrolment of students but lack an adequate number of instructors to train them. If digital learning can be demonstrated effective in augmenting knowledge and skills, this approach could help fill this gap and improve education efficiency. A needs assessment in two Nigerian midwifery schools confirmed that digital learning would be feasible and welcomed. In this study, the Midwifery Active Digitization Empowerment Initiative (MADE-I) program was tested to determine if digital delivery of the Fundamental Interventions, Referral and Safe Transfer (FIRST) course is at least equally effective for training midwifery students compared to conventional small-group delivery.
Methods: A non-inferiority randomized controlled trial design was used, enrolling 130 s-year students from 2 midwifery schools in Benue State, Nigeria. Students were randomly assigned into six cohorts. Each cohort received half of the course on a Learning Management Platform on their mobile phones, the other half through standard small-group teaching. Students’ knowledge, thinking, and technical skills were assessed using a pre-test, post-test, Objective Structured Clinical Exam (OSCE), and daily modular quizzes. The data was analyzed using the difference-in-difference method.
Results: The study revealed that post-intervention student knowledge and thinking skills did not significantly differ between digital learning (75.26%) and small-group learning arms of the trial (75.02%, p = 0.404). Student knowledge improved significantly compared to the pre-test in both groups (by 25.03 points in the digital arm, 26.39, in small-group). Some differences were observed between digital and small-group learning in disaggregated analysis by specific module and midwifery school. Although there was a trend toward small-group learning of technical skills being more effective than digital learning, no significant differences between groups were observed in the post-intervention OSCE. Students in both groups learned equally well regardless of age, gender, and midwifery school entrance exam score.
Conclusion: Digital learning is as effective as small-group learning, for midwifery trainees, in augmenting knowledge, thinking, and technical skills addressed in the FIRST course, and have lighter human resource requirements, an important consideration especially in LMIC. However, similar assessments would be needed to assess effectiveness for other digitally delivered clinical education programs.
1 Introduction
Globally, maternal mortality remains unacceptably high, with 94% of maternal deaths occurring in LMICs. Mortality varies significantly by country due to factors including access to healthcare, education, and socio-economic conditions. Sub-Saharan Africa alone accounts for two-thirds of maternal deaths, with Nigeria recording the largest numbers of such deaths (WHO, UNICEF, UNFPA, World Bank Group, and United Nations Population Division, 2017). Currently, Nigeria has among the highest maternal mortality ratios (MMR) in the world, with 1,047 maternal deaths per 100,000 live births (Macro Trends, 2024). Studies conducted in 2021 and 2022 reveal that the MMR in Benue State, Nigeria—the site of this study—is 1,189 deaths per 100,000 live births (Bola et al., 2022; Ujoh et al., 2021). The Sustainable Development Goal 3 (Target 1) aims at achieving a target of less than 70 deaths per 100,000 live births by year 2030. To achieve this goal, Nigeria must increase the number of healthcare professionals; currently they number only 1.95 per 1,000 (WHO, 2021); this will require training methods that ensure good training outcomes at large scale and a bearable cost, given the current economic challenges facing the country.
Studies (Asaba et al., 2022; Tekeş and Uluşen, 2023; Nukunu et al., 2024) have shown that improving midwifery training through digital methods and platforms can enhance access to information on evidence-based care, guidelines and best practices; facilitate real-time communication and collaboration among healthcare workers; enable remote monitoring and prompt response to expectant mothers; and provide flexible but effective learning options for midwives to update knowledge and skills. By using such methods, the wide gap between needed and available skilled healthcare workers in underserved regions can be significantly closed, contributing to the reduction of maternal and infant mortality, and accelerating progress toward the attainment of the SDG 3’s target 1 of significantly improving reproductive, maternal, and child health outcomes.
Midwifery training plays a critical role in ensuring safe childbirth, and reducing maternal and neonatal mortality. Studies from India, Ghana, Afghanistan and Tanzania (Muke et al., 2020; Speciale, 2016; Essel et al., 2020) have shown the feasibility, acceptability, and effectiveness of fully remote digital training for health workers in low-resource rural settings. During the acute phase of the COVID-19 pandemic, critical training interventions for frontline healthcare workers, including midwives were successfully delivered using remote and digital methods (Reljic et al., 2023).
Benue State, located in North-Central Nigeria, faces significant challenges in maternal and neonatal healthcare. Limited access to trained midwives contributes to high maternal and neonatal mortality (Bola et al., 2022; Ujoh et al., 2021; Bola et al., 2022). Conventional face-to-face, instructor-led midwifery training has been the standard approach used. However, such methods pose important challenges, notably high costs, geographical limitations, and insufficient human resources. Digital training platforms offer a promising solution, providing flexible, cost-effective, and scalable alternatives. In low-income regions like Benue State where access to quality healthcare and midwives/skilled birth attendants is limited, effective midwifery training is desperately needed but unavailable at the needed scale. With advances in technology, digital training platforms have emerged as potential alternatives or supplements to conventional instructor-led training methods, for at least some aspects of training.
The WHO framework for action on “Strengthening Quality Midwifery Education for Universal Health Coverage 2030” proposes that transformative and innovative teaching strategies—including technology-based approaches—are necessary to engage midwifery students as active learners and teach them clinical competencies aligning with international standards (WHO, 2019). Providing quality training to midwives, using such methods, could contribute to significant reductions in maternal mortality. Over 50 outcomes have been shown to be improved by quality midwifery education (WHO, 2019).
Consistent with the WHO framework, the Canadian Network for International Surgery (CNIS) has been seeking to contribute to the reduction of poor outcomes among women and newborns. In this work, we have drawn on the Whistler Principles to Accelerate Development, including: promoting inclusive innovation, focus on the poor and the vulnerable, taking intelligent risks, and experimentation while doing no harm (G7 Charlevoix, 2018).
Since 1995, CNIS has trained over 60,000 African health professionals using structured clinical training courses that include Socratic questioning, case studies and hands-on learning. In 2008, CNIS introduced its course, “Fundamental Interventions, Referral and Safe Transfer (FIRST) for Midwives” in Tanzania, using small group teaching methodology. FIRST has been successfully used for training midwifery students but the methodology used has significant human resources and infrastructure requirements. In CNIS’s experience, the use of small group teaching is an improvement over standard teaching in African midwifery colleges where the usual method of instruction has been large-group teaching. Due to increasing demand for healthcare services, more students are enrolling in midwifery training programs, making the currently accepted gold standard methodology, small group teaching, less feasible as there has not been a commensurate increase in the number of institutions or instructors (Bvumbe and Mtshali, 2018; Odongo and Talbert-Slagle, 2019).
Digital teaching has several important potential advantages for instructors and students. For instructors, these include the ability to pre-record lectures, monitor students’ progress digitally, and integrate other relevant learning technologies to support the delivery of the curriculum. For students, the most notable advantages are the ability to watch and replay lectures on demand as well as monitor their own progress using the digital platform. This individualized learning is consistent with general principles of small group learning, but is not necessarily intended to fully replace it.
In response to the increase in those seeking midwifery education in low-income countries where CNIS is active (Tanzania, Nigeria, and Ethiopia), CNIS has developed the Midwifery Active Digitization Empowerment Initiative (MADE-I), the main strategy of which is to deliver the didactic portion of FIRST using digital methods. With increasingly widespread use of digital learning platforms and virtual communication technologies, building knowledge and skills through use of such platforms is a promising area for clinical instruction (Wilcha, 2020). Delivery of the FIRST-for-Midwives course using digital methods (through MADE-I) is intended to enable a larger number of midwifery students to receive good quality training.
We have previously demonstrated that digital delivery of the FIRST course to clinical officer students in Tanga, Tanzania was well-received and, when supplemented with standard training materials and in-person instruction, students performed better than those who received just the standard training (Bola et al., 2021). However, it is unknown whether students who receive only digital delivery of the didactic material perform similarly to students who are exposed to the same material through standard small-group methods. To our knowledge, no previous study has investigated the effectiveness of digital midwifery training compared to instructor-led small-group training, utilizing a non-inferior randomized trial design.
Further understanding is needed on the effectiveness of digital versus small-group methods for midwifery education in resource-constrained settings like Benue State. Therefore, the primary objective of this study is to determine whether digital midwifery training is non-inferior to the accepted gold standard of conventional instructor-led small-group training for knowledge acquisition, skills development, and clinical competency, assessed using a randomized non-inferiority trial design. The primary outcome is performance on the post-intervention OSCE, with other measures including students’ knowledge and thinking skills, including analysis disaggregated by modules and gender.
We sought to determine whether digital delivery of the FIRST course is at least as effective as the conventional instructor-led training of this material. While digital delivery can be expected to be more efficient, we must ensure that use of such an approach does not compromise training effectiveness. If the digital delivery is demonstrated to be equally or more effective, it would be the preferred method as it can reach a larger number of students with fewer resources. The study therefore, seeks to answer the following research question:
Is digital delivery of the FIRST course for midwifery students at least non-inferior to conventional instructor-led methods with regard to key learning outcomes, given the technology infrastructure in a setting such as Benue State?
In our study, a non-inferiority margin of 15% was used, considering the feasibly, available sample size and the proportion expected to achieve a clear pass, i.e., meeting a predefined cut-off score on post-intervention OSCE performance (our main outcome measure). Given the challenges and the increasing burden on health care systems in Nigeria particularly due to stagnating national income in the presence of rising population and increasing population displacements due to conflicts and natural disasters, the need to prioritize investments for increased manpower in the healthcare sector cannot be over-emphasized. We consider this study an important first step.
To our knowledge, no previous study has investigated the effectiveness of digital midwifery training compared to instructor-led small-group training utilizing a non-inferior randomized trial design.
2 Literature review
The global shutdown resulting from the COVID-19 pandemic in 2020 posed major challenges sustaining crucial functions such as the educational, healthcare services and commercial activities. This led to the prominence of virtual events such as conferences, business meetings as well as teaching and learning. Specifically, academic institutions in different parts of the world were mandated by government to use digital/e-learning/online teaching modes in order to limit human contact as a measure for reducing the spread of COVID-19. Institutions of learning all over the world accelerated introduction of digital teaching methods across all levels of education (primary/elementary, secondary and tertiary education) and in different disciplines (including engineering, healthcare, social sciences and humanities; Martín et al., 2021; Navarro et al., 2024; Webster, 2024; Hussein et al., 2020; Wei and Chou, 2020; Chung et al., 2020). It became indisputably advantageous to adopt digital education for several reasons including but not limited to immediate access to the multiple scientific resources in online databases and virtual libraries (including videos and tutorials, articles, etc.); open, interactive and interdisciplinary teaching and learning interaction; developing online communities/groups for a certain field (Dospinescu and Dospinescu, 2020), thereby removing time and geographical location constraints in the teaching and learning process (Nayar and Kumar, 2018).
While it was possible to deploy digital teaching and learning globally, some studies revealed that digital learning and teaching methods come with inherent challenges peculiar to specific regions of the world. For example, in sub-Saharan Africa (including Nigeria), major challenges included unreliability of electricity to power learning devices, lack of teaching equipment, incompatibility of technologies, high cost and weak quality of internet service, and psychological consequences arising from the absence of physical interaction among students and teachers (Navarro et al., 2024; Webster, 2024). Furthermore, several other concerns have been raised including the quality of digital/online teaching; the ability of the online courses to meet the learning needs of students as effectively as the instructor-led method; and the fact that some students may struggle in a digital learning environment (Webster, 2024; Picciano et al., 2012; Shah et al., 2021; Ya Ni, 2013). From a review of 1,496 articles on digital learning, the challenges of these methodd have been succinctly summarized into 3 main categories (Fauzi, 2022): (1) selection of the appropriate learning practices and patterns; (2) mental and physical health of learners and teachers (stress, anxiety and/or depression) due to lack of direct personal interaction; and, (3) discipline-specific issues in medical and engineering education, where in-person clinical, laboratory, onsite and field activities are needed, suggesting that certain learning activities in some disciplines may not perform adequately using digital/online/e-learning approaches. Similarly, another bibliometric study of 8,303 post-COVID pandemic published works revealed that the focus of digital learning had been on ICT and pedagogy, technology-enhanced education, mental health and well-being, student experience and curriculum and professional development (Aristovnik et al., 2023). In another study, an Artificial Intelligence (AI) Ecological Education Policy Framework was proposed to address the complex and multifaceted implications of AI integration in teaching and learning at intsitutions of higher learning. Classified in into three dimensions, (1) “the Pedagogical dimension concentrates on using AI to improve teaching and learning outcomes, while the Governance dimension tackles issues related to privacy, security, and accountability; and finally the Operational dimension addresses matters concerning infrastructure and training (Chan, 2023). The aim of this framework is to address a concern relating to use of text-generating AI in academic environments, considered as cheating and plagiarism.
During the period since the acute pandemic phase, there has been a continued rapid adoption of digital techniques and methods in teaching and learning globally (Fauzi, 2022; Aristovnik et al., 2023). For midwifery, the use of digital teaching, learning and practice is progressively replacing conventional instructor-led methods because of its flexible and accessible student-centric character. Digital teaching and learning methods enhance the speed and ease of knowledge and skills acquisition for healthcare practitioners working in distant and rural locations, away from the critical and knowledgeable resource-persons/instructors who may never be able to visit those remote locations. One study (Geraghty et al., 2019) revealed that online courses provide midwives with flexibility, but may also lead to feelings of loneliness and inadequate support throughout the learning process. One systematic review (Lahti et al., 2014) found no evidence for the superiority of digital learning compared to conventional training with regard to learning outcomes for nursing students and practitioners, but other studies (Eisner et al., 2022; Quinn et al., 2019; Tzitiridou-Chatzopoulou et al., 2024) have found that online training programs significantly enhanced the comprehension of nurses about reproductive concerns affecting cancer and post-partum depression patients.
In Nigeria, academic institutions are increasingly adopting digital teaching and learning methods continue for knowledge transfer (Adeshina, 2023; Nwaokugha and Wogonwu, 2023; Undie et al., 2024). Since the pandemic, midwifery schools have increasingly sought opportunities for digital midwifery training and practice. It is evident that there is a misalignment between international standards for midwifery training and what schools and clinical sites can provide, further reinforcing the need for informed investment decisions in midwifery education (Warren et al., 2023). The adoption of digital education for midwifery training has become increasing necessary given that the 2021 State of the World’s Midwifery Report “puts the midwives shortage in Nigeria at about 30,000 which is 6 midwives per 10,000 people. To close the gap by 2030, about 70,000 more midwives positions are needed but with current estimates, only 40,000 more will be created by 2030” (UNFPA, WHO, and ICM, 2021) but the ratio in Nigeria is 0.62/1000 (World Health Organisation, 2021), ranking among the poorest globally.
Technology is used in midwifery practice as patient education (UNFPA, WHO, and ICM, 2021), empowering midwives to use various digital tools to provide their patients with information on pregnancy, childbirth, and postpartum care especially in locations where midwives are in short supply. Use of the Community Maternal Danger Score (CMDS) App to provide risk information to pregnant women has been tested (Bola et al., 2022; Bola et al., 2022) among practicing midwives in remote areas of Benue State.
From the literature, it is clear that while the adoption of digital methods for training midwifery students is significantly increasing, it remains important to assess technology availability and support resources, suitability to the midwifery profession in terms of practical/clinical exercises, effectiveness for skill acquisition, and mental and physical health consequences for students and instructors.
Importantly, the northern geo-political region of Nigeria (within which Benue State is located) has few nursing and midwifery schools, and even much lesser qualified midwives by a ratio of 1:5 of the 114,168 registered midwives in the Nursing and Midwifery Council of Nigeria (NMCN) database (compared with the geographically smaller and less populated southern region of Nigeria; Nursing and Midwifery Council of Nigeria, NMCN, 2020; Mba et al., 2021). To help meet the need for rapidly expanding quality midwifery education and training in this setting, this study hypothesizes that: “a digital training approach is non-inferior to conventional in-person small-group instruction provided to midwifery students in Benue State, for acquiring knowledge and skills addressed by the FIRST training package.”
3 Methods
3.1 Study design and setting
The study was conducted in the two largest government-registered midwifery schools in Benue State (see map below), in the north central region of Nigeria: Mkar and Makurdi Schools of Midwifery. The Benue State Government Ministry of Health and Human Services entered into a Memorandum of Understanding with CNIS for the delivery of various health interventions, including the FIRST-for-Midwives course through the MADE-I digital method.
Benue State (Figure 1) is one of 36 territories comprising the Federal Republic of Nigeria. According to 2022 projections, Benue State has a population of 6,141,300, with a population density of 199.5 per square kilometer, and 50.7% aged between 15 and 64 years, and 46.1% aged between 0 and 14 years (National Bureau of Statistics, 2023). As at 2022, the State’s gross domestic product (GDP) was Nigerian Naira 4.27 trillion, ranking 12th out of 36 States (BudgIT, 2022). With a landmass of 34,059 square kilometers (Ujoh et al., 2019), the Inhabitants of the State are predominantly Christians and largely engaged in crop farming and other primary economic activities such as fishing, hunting and charcoal production from fuelwood.
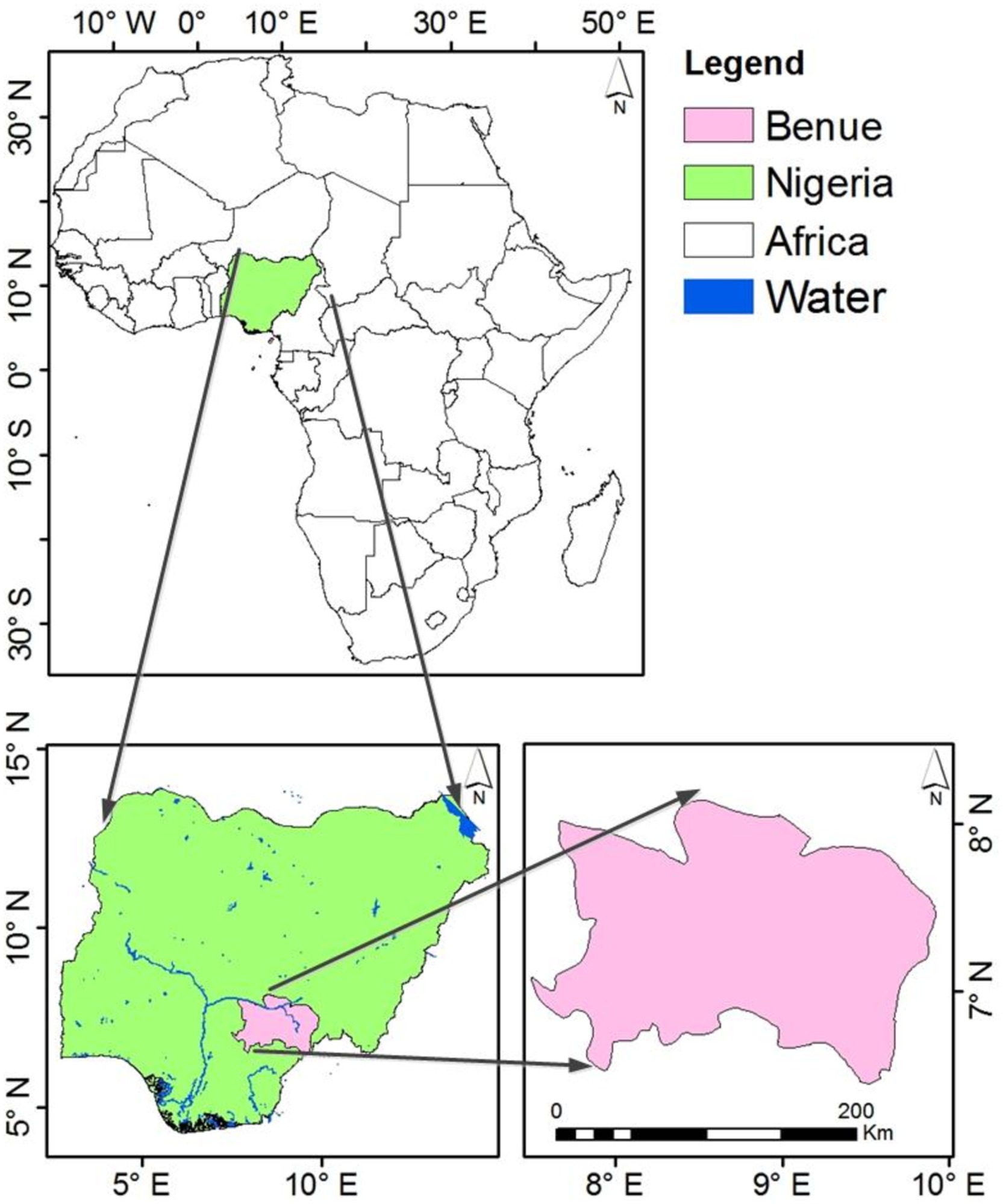
Figure 1. Map of Benue State, the study area (Ujoh et al., 2019).
3.2 Intervention preparation
The process began with the digitization of the four modules of the 2014 FIRST for Midwives course (Patient Risk Management, Wound Management, Basic Obstetrics, and Community Maternal Danger Score) and preparation of 2 additional modules (Respectful Maternal Care, and Impairment at Birth). This required video recording of lectures and skills demonstrations, development of presentations, quiz questions and formative evaluations. Pre- and post- course modules were developed to introduce the students to the course and evaluate their performance, including use of an OSCE. Moodle (ref Home | Moodle.org), an open-source Learning Management System (LMS), was selected as the platform for the course because: (1) it has a Mobile App with some offline capabilities; this was important for the study given that internet access in this setting is unreliable, and (2) because of the flexibility offered by the more than 2,000 available plugins. Efforts were made to ensure that the learning experience was interactive, utilizing H5P plugins for video and slide presentations (ref H5P – Create and Share Rich HTML5 Content and Applications) and providing immediate feedback to the learner when they responded to questions both correctly and incorrectly. Case studies used stock photos to enhance visual interest, and each module concluded with survey questions for the evaluation of students’ understanding of the content of training materials.
3.3 Intervention delivery
For each of the modules, the students were randomized in a cross-over design into digital or standard learning. A print manual was provided, which included directions for use of the Moodle app. For both digital and standard delivery, students completed their modular evaluation exercise on the Moodle app. It was necessary to provide the classrooms in both schools with a wireless router and ensure continuous electrification of the routers (and fans for cooling) with a back-up generator.
3.4 Implementation period and study population
The MADE-I project was implemented from March to October 2021, and comprised three phases:
i. a formative evaluation with students and midwifery instructors,
ii. an evaluation of the effectiveness of the digital approach of the FIRST course, and
iii. a post-intervention evaluation with students and instructors.
The findings reported in this paper covers all 3 phases but the post-intervention evaluation reported is for students only.
However, the actual student trial was conducted over 3 weeks in September and October 2021. Given the level of the content in the FIRST training curriculum, in discussions with the leadership team of both midwifery schools, it was decided to include only 2nd year midwifery diploma students, 50 from Mkar and 98 from Makurdi.
3.5 Trial design
This study used a non-inferiority design (Honoris et al., 2020) as we were interested in establishing whether the less resource-demanding digital delivery of the material was at least as effective as the standard in-person small-group training. This was a concern given that the human resource requirements of conventional delivery render it less accessible for the increasing numbers of students seeking midwifery education and given insecurity and lack of funding to hire the required numbers of expert trainers to deliver in-person, conventional training in such settings.
Based on the objectives of the project, two modes of delivery were used for lecture material: online delivery using a LMS (Moodle app), and the traditional face-to-face classroom delivery mode. We divided the students into groups using a tool called Cohort model. The Moodle mobile app was used because it allows students to access their courses with or without internet connection.
As the project used a crossover design, all students served as both intervention (here referred to as digital group) and control group (small group). This approach helped minimize the impact of any differences in the allocation between groups, eliminating an important potential source of bias.
Six cohorts were created, each with 22–26 students, 2 in Mkar and 4 in Makurdi, and the students were randomly assigned to one of the cohorts (Figure 2). The study included all second year students officially registered in the three-year midwifery program; no other eligibility criteria were applied. Each week two cohorts participated in the training. As the FIRST course consists of six modules, each cohort alternatingly received half of the material on the Moodle app and the other half through standard conventional small-group teaching.
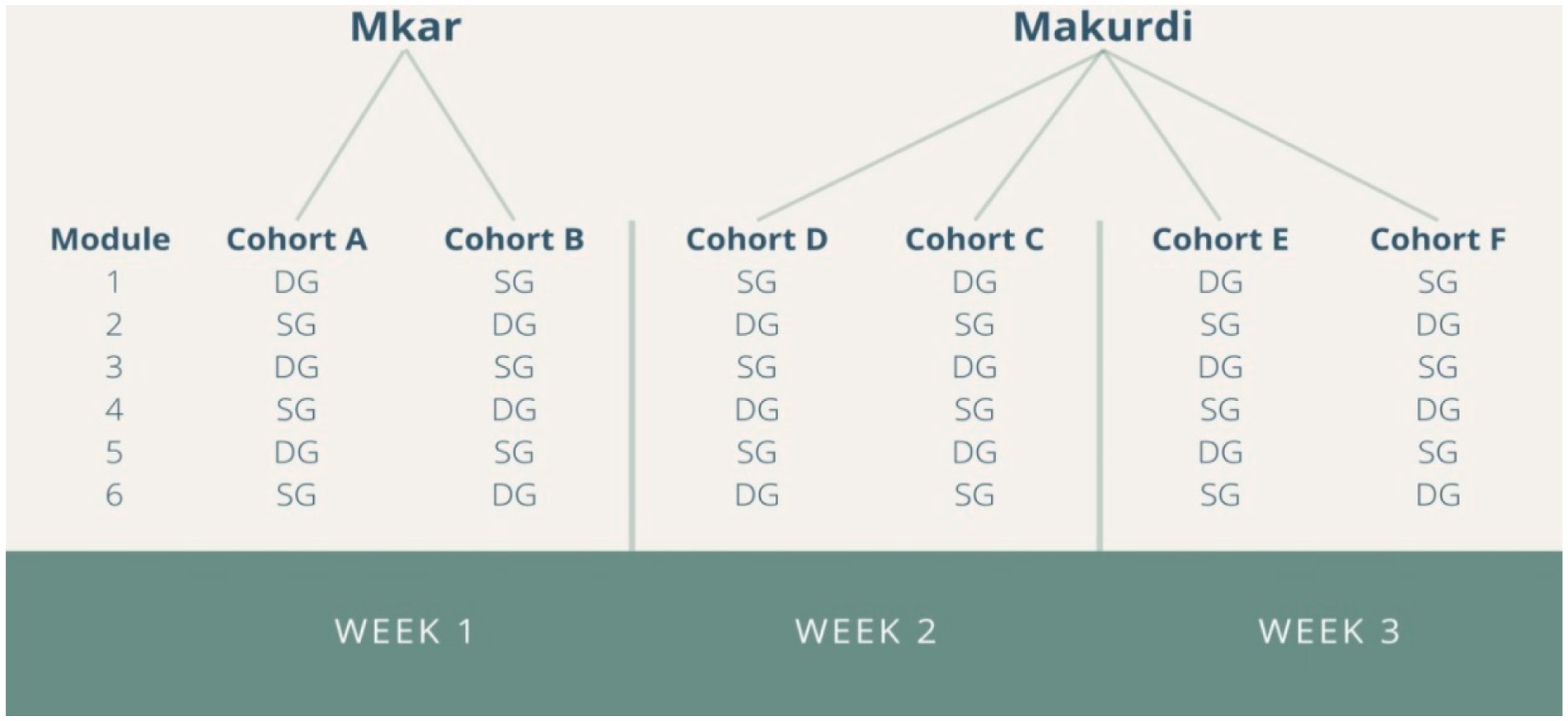
Figure 2. Cohorts and modes of delivery. DG, digital delivery; SG, traditional small-group delivery.
Each of the six modules included four components: (i) theoretical knowledge, (ii) case-based learning, (iii) technical skills practice, and (iv) quizzes. For the standard small group cohort, five midwifery school instructors were assigned to teach the theoretical lessons and to train and monitor students in the case-based learning and technical skills. For the digital delivery cohort, all the components were presented through Moodle: case studies were gamified and video tutorials were used for technical skills. One CNIS staff and one IT instructor supervised the digital cohorts.
In order to assess the effectiveness of digital compared to small-group learning, we employed a pre-test, post-test design and daily modular quizzes to evaluate the performance and skills of students. The pre-test was an online questionnaire consisting of 22 questions meant to assess students’ knowledge, critical thinking, and management skills (see supplementary file). The post-test included a questionnaire with the same 22 questions plus five more and an Objective Structured Clinical Examination (OSCE), which included six technical skills stations. Additionally, we assessed the students’ post-training skills, disaggregated by gender and modules (analysis not included in this paper). We also evaluated student knowledge using modular quizzes administered each day after completing of training.
Note that there were problems with the wording of the questionnaire for module 6 when the pre-test was administered such that we were not able to use changes on this measure in our assessment of non-inferiority. However, we did have valid endline OSCE measures for this module.
3.6 Statistical analysis
Data were included in the analysis from 130 students who completed all surveys/tests. A difference-in-difference approach was used to analyze the pre- and post-test data because the approach is inherently capable to remove biases in post-intervention comparisons, in this study, between the pre-and post-test data, as well as biases from comparisons between the small group (SG) and digital group (DG) due to other causes of the outcome.
One-sided t-test and z-test (due to the non-inferiority hypothesis) with 95% Confidence Interval (CI) were used to examine whether the changes in the knowledge scores and proportion of clear pass in the OSCE significantly differed between SG and DG. Such analysis allowed for this study to rigorously test the outcome in terms of directional changes, while also providing a clear evidence of the effect of this digital intervention method.
Disaggregated analysis was also performed, by module and student age (and by entrance exam results where relevant). The primary endpoint was proportion achieving a clear pass on the post-intervention OSCE evaluation. Post-intervention tests were combined with equal weighting given to the modular tests, post-test, and the OSCE. All data was analyzed with SPSS.
3.7 Statistical power
With the resources available, the study focused on two midwifery schools in Benue State, in the cities of Mkar and Makurdi. With our total sample of 130 (for which we had complete data), the binary outcome of proportion of students achieving a clear pass on the OSCE assessments, and an expected proportion of students passing in both arms of 85%, we had 80% power to exclude inferiority of greater than 15%, with a one-sided 95% confidence interval.
The formula used for calculating the sample size for the non-inferiority trial was:
,
with πs and πe as the true percent “success” in the standard (conventional small-group) and experimental (digital) learning groups, respectively.
4 Results
Composition of cohorts: the cohorts were similar with regard to gender, age and entrance exam performance (no statistically significant differences observed). Due to lack of Google accounts and smart phones allowing full participation in the trial, 18 students participating in the study were excluded from the analysis, leaving 130 students for whom data were available to analyze all primary and secondary outcomes.
4.1 Pre- to post-test changes in mean scores for knowledge, critical thinking, and management skills
Across all five modules combined, students significantly improved their knowledge, critical thinking, and management skills, as measured on pre- and post-questionnaires. Those in both digital and small group learning arms showed a significant improvement from pre- to post-test (by a mean of 25.03 and 26.39 points, respectively), with no statistically significant difference in gains, overall (p = 0.58). However, on modules 3 and 4, the pre- to post-test improvement was greater in the small-group arm (Table 1).

Table 1. Pre- to post-test changes in mean scores (%, N = 130).
4.2 Endline OSCE performance
On the post-training OSCE evaluation (Table 2), using a clear pass as the outcome (pre-defined as the primary outcome for the study), there was no significant difference in performance between small group and digital arms, overall. However, on the secondary outcome of mean numeric score on the OSCE, small group delivery outperformed digital by approximately 3 percentage points (77.0% vs., 74.1%, p = <0.001) and it appears that most of this difference is accounted for by the results for module 3 (which assessed performance on perineal laceration repair, manual removal of the placenta and intravenous infusion).
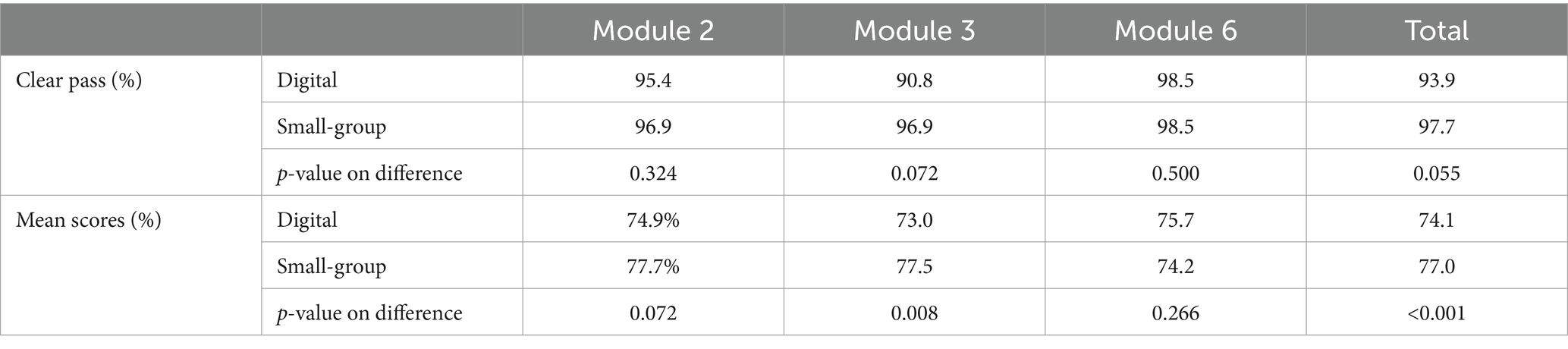
Table 2. Endline OSCE analysis (N = 130).
The OSCE examination included material only from modules 2, 3, and 6 as presented in Table 2.
4.3 Overall endline performance
Overall post-intervention results, which included performance on the daily modular tests, the post-test, and the OSCE, showed very similar results across the 2 arms: digital—75.3%, and small-group—75.0% (p = 0.404).
On analysis of post-test, modular quizzes and OSCE, disaggregated by age and entrance exam scores (not shown), no differences were observed.
On the basis of the overall statistical analysis (p = 0.404), there is no significant difference in learning outcomes between the digital learning group and the small group, instructor-led learning group. Therefore, we accept the null hypothesis statement: “The digital delivery method of FIRST for midwifery students in Benue State is non-inferior to the conventional instructor-led method.”
4.4 Discussion
On most measures, including our primary endpoint—clear pass on the OSCE assessments—digital delivery was found to be non-inferior to small group delivery. However, skills acquisition in module 3 appeared to be lower in the digital arm. Module 3 focused on basic obstetrics. The OSCE assessment of the technical skills taught in this module demonstrated discordance between numeric score and clear pass. On a pass-fail basis, no difference was found between digital learning and small group learning arms but on a numeric basis small group learning showed a trend to better learning. The technical skills assessed by the OSCE on module 3 included perineal laceration repair, manual removal of the placenta and intravenous infusion. These skills required integration of prerequisite skills taught in other modules. We speculate that the digital learning of basic obstetrics needs more time or requires more instruction on skill integration. Further assessment of the methods of digital teaching of the more complex skills is recommended.
Although, overall the digital delivery modality was found to be non-inferior, small group learning may offer advantages for certain modules (in addition to module 3, as discussed above, we have noted greater pre-to-post-test improvements on module 4 in the small-group arm), potentially due to the more personalized interaction and hands-on guidance provided in such settings. However, the main problem with small-group delivery is that it has heavier human resource requirements, which means there is constraint on scalability. Given this limitation, midwifery schools may opt instead for large group instruction. However, digital group learning offers convenience and flexibility. The lack of significant differences by age and entrance score suggests that both learning methods are equally accessible and effective for students with varying backgrounds and abilities. Overall, these findings highlight the importance of considering various factors, including specific learning objectives, student demographics, and context, when choosing between small group and digital group learning methods for midwifery skills training. Further research with larger and more diverse samples could provide additional insights into the comparative effectiveness of these approaches. As noted, for complex skills requiring integration of more fundamental skills, further research on digital methods is needed.
Based on our results we can conclude that digital delivery of the FIRST course is largely non-inferior, i.e., at least equally efficacious, in teaching knowledge, critical thinking, management, and technical skills as students in both arms scored equally well across all tests, in the aggregate. Also, all students, regardless of age or entrance exam scores, benefitted equally from the digital training. This is consistent with other published evidence (Terry et al., 2019).
Considering the lower number of instructors required for the digital delivery of the FIRST course—2 compared to 5 for the small group delivery—digital delivery approach is more efficient in terms of human resources. Nevertheless, power outages and poor internet connectivity can compromise use of digital approaches. Additionally, there is the need to conduct a separate study to determine the modules that can be better delivered digitally or otherwise by the small group delivery.
In conclusion, digitally delivered training has proven to be an inclusive, scalable, and easily integrated approach for building midwifery skills; and it produces results similar to small group teaching, and clearly superior to large-group teaching, which is the most-often used method in resource-constrained settings. Such effective and efficient training is particularly needed to achieve the targeted 80% reduction in maternal mortality and neonatal mortality in Nigeria.
Assessment needs to be part of an ongoing evaluation cycle (Bola et al., 2024). This is important for ensuring robust and effective training and, ultimately, for the achievement of SDG 3, Target 1: reducing maternal mortality rate to less than 70 per 100,000 live births by year 2030.
4.5 Limitations
The sample size used limited statistical power; this was largely determined by 3 main factors: (1) at the time of this study, these were only two government-licensed midwifery schools in Benue State; (2) the sample retained only 2nd year midwifery students because the material was considered too advanced for 1st year students and 3rd year students are mostly unavailable as they are away on clinical placements; (3) increasing the number of midwifery schools would have required signing additional Memoranda of Understanding with other State Governments, which would not have been feasible given funding and time constraints. However, with a larger sample, tighter confidence intervals for the outcomes of interest would have been possible. Similarly, with a larger number of study sites across more diverse settings, generalizability of the findings would have been enhanced.
5 Conclusion
Overall, we found digital delivery of the FIRST curriculum to be non-inferior to the gold standard of in-person small-group delivery mode.
OSCE Evaluation:
• There was no significant difference in performance between small group and digital arms in the proportions achieving a clear pass (our primary outcome).
• Mean numeric scores pooling in 2 of the 3 OSCE modules were higher in the small group arm than in the digital arm (Table 2), due primarily to differences in performance on module 3 (which tested performance on several technical procedures).
Overall Post-Intervention Results:
• There was comparable performance across the 2 arms: digital—75.3%, small group—75.0%.
Disaggregation by Age and Entrance Score:
• There was no effect modification by age or nursing school entrance exam score, as measured by modular quizzes and OSCE results.
Digital delivery of the FIRST training material was found to be non-inferior to the gold-standard small group approach and is more efficient with regard to human resources required. Digital training platforms could serve as a scalable solution to improve midwifery education in Nigeria and other settings with similar resource constraints.
This study addresses a gap in the literature by comparing the effectiveness of digital versus conventional instructor-led midwifery training. From a theoretical perspective, midwifery training must not be restricted to the conventional instructor-led approach as the study reveals that digital training approach is equally effective, not necessarily superior. This outcome is consistent with the findings of García-Machado et al. (2024) which established two relevant mediators - student intrinsic motivation, and student academic engagement, as an important support for student online learning for superior academic performance. From a practical perspective, it is important to identify and establish the key mediators that serve as effective support for midwifery students engaged in online learning. While this is a context that could be considered for further interrogation at the study area, the current findings of this study are of relevance to policy makers and those responsible for pre-service midwifery education in Benue State.
This study has determined that digital pedagogy for midwifery skills as covered by this curriculum can be delivered with essentially equivalent knowledge/skills transfer to what can be achieved using the more resource-intensive in-person, small-group teaching methodology. In contexts such as Nigeria, where nursing training institutions have high student-to-instructor ratios, adoption of this methodology can produce good learning outcomes, in a more feasible cost-efficient manner. Funding for midwifery education in Benue State is the responsibility of government. It is therefore, expected that digital training methods would be adopted as a strategy for cost-cutting without compromising the quality of midwifery education.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Benue State Ministry of Health and Human Services, Makurdi, Nigeria. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
FU: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing. AD-W: Conceptualization, Data curation, Formal analysis, Methodology, Software, Writing – original draft, Writing – review & editing. RN: Data curation, Software, Writing – original draft, Writing – review & editing. VG: Data curation, Supervision, Writing – original draft. RA-a: Data curation, Supervision, Writing – original draft. IO: Data curation, Software, Writing – original draft. RB: Data curation, Software, Writing – original draft. JC: Conceptualization, Methodology, Writing – original draft. SH: Conceptualization, Methodology, Writing – original draft, Writing – review & editing. RL: Conceptualization, Data curation, Methodology, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. The MADE-I project was funded by the Fund for Innovation and Transformation, the Donner Canadian Foundation, and Mitacs. The views expressed are those of the authors and not necessarily those of the funders.
Acknowledgments
We acknowledge the support of the Benue State Government through its Ministry of Health and Human Services for providing ethical approval and access to the Schools of Midwifery in Mkar and Makurdi for this study. We acknowledge the valuable suggestions of Abraham Ijer, the Director of Nursing Services in Benue State. We thank the Management and Staff of the two Midwifery Schools in Mkar and Makurdi for their support throughout the course of this project. Finally, we acknowledge the efforts of our Research Assistants, Shedrach T. Ujoh (Makurdi) and Benjamin T. Abu (Mkar).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/feduc.2024.1470075/full#supplementary-material
References
Adeshina, A. E. (2023). The transformative role of digital resources in teaching and learning. Open J. Educ. Develop. 5, 1–9. doi: 10.52417/ojed.v5i1.520
Aristovnik, A., Karampelas, K., Umek, L., and Ravšelj, D. (2023). Impact of the COVID-19 pandemic on online learning in higher education: a bibliometric analysis. Front. Educ. 8:1225834. doi: 10.3389/feduc.2023.1225834
Asaba, M., Omolara, T., Ihekwaba, I., and Tella, A. O. (2022). Willingness and readiness to use digital technologies in midwifery practice among midwives at tertiary health facilities in Uganda. A qualitative and phenomenological study. Training and education. Student’s J. Health Res. Africa 3:15. doi: 10.51168/sjhrafrica.v3i12.255
Bola, R., Mushi, B., Kweka, L. E., and Lett, R. (2021). A randomized matched- pairs study evaluating a hybrid, structured skills course for clinical officers in Tanga. Tanzania. East Cent Afr J Surg. 26, 59–64. doi: 10.4314/ecajs.v26i2.3
Bola, R., Ngonzi, J., Ujoh, F., Kihimuro, R. B., and Lett, R. (2024). An evaluation of obstetrical data collection at health institutions in Mbarara region, Uganda and Benue state. Nigeria. Pan African Med. J. 47:109. doi: 10.11604/pamj.2024.47.109.36295
Bola, R., Ujoh, F., and Lett, R. (2022). Identification and mitigation of high-risk pregnancy with the community maternal danger score Mobile application in Gboko, Nigeria. PubMed central. PLoS One 17, 1–8. doi: 10.1371/journal.pone.0275442
Bola, R., Ujoh, F., Ukah, U. V., and Lett, R. (2022). Assessment and validation of the community maternal danger score algorithm. Global Health Res. Policy 7, 1–9. doi: 10.1186/s41256-022-00240-8
BudgIT (2022). State of states: subnational governance reforms for a new era, 2022 edition. Available at: https://yourbudgit.com/wp-content/uploads/2022/10/2022-State-of-States-Report.pdf (Accessed October 7, 2024).
Bvumbe, T., and Mtshali, N. (2018). Nursing education challenges and solutions in sub Saharan Africa: an integrative review. BMC Nurs. 17:3. doi: 10.1186/s12912-018-0272-4
Chan, C. K. Y. (2023). A comprehensive AI policy education framework for university teaching and learning. Int. J. Educ. Technol. High. Educ. 20, 1–25. doi: 10.1186/s41239-023-00408-3
Chung, E., Subramaniam, G., and Dass, L. C. (2020). Online learning readiness among university students in Malaysia amidst Covid-19. AJUE 16:45. doi: 10.24191/ajue.v16i2.10294
Dospinescu, N., and Dospinescu, O. (2020). Information technologies to support education during COVID-19. University scientific notes, Університетські наукові записки 2020, 17–28. doi: 10.37491/UNZ.75-76.2
Eisner, E., Lewis, S., Stockton-Powdrell, C., Agass, R., Whelan, P., and Tower, C. (2022). Digital screening for postnatal depression: mixed methods proof-of-concept study. BMC Pregnancy Childbirth 22:429. doi: 10.1186/s12884-022-04756-2
Essel, H.B., Awuni, T., and Mohammed, S. (2020) Digital Technologies in Nursing and Midwifery Education in Ghana: educators perspective, practice and barriers. Library philosophy and practice (e-journal) 3722. Available at: https://digitalcommons.unl.edu/libphilprac/3722 (Accessed October 3, 2024).
Fauzi, M. A. (2022). E-learning in higher education institutions during COVID-19 pandemic: current and future trends through bibliometric analysis. Heliyon 8:e09433. doi: 10.1016/j.heliyon.2022.e09433
G7 Charlevoix. The Whistler Principles to Accelerate Innovation for Development Impact: Investing in Growth that Works for Everyone. (2018). Available at: https://www.international.gc.ca/world-monde/assets/pdfs/international_relations-relations_internationales/g7/2018-05-31-whistler-development-developpement-en.pdf (Accessed October 7, 2024).
García-Machado, J. J., Ávila, M. M., Dospinescu, N., and Dospinescu, O. (2024). How the support that students receive during online learning infuences their academic performance. Educ. Inf. Technol. 29, 1–25. doi: 10.1007/s10639-024-12639-6
Geraghty, A. C., Gibson, E. M., Ghanem, R. A., Greene, J. J., Ocampo, A., Goldstein, A. K., et al. (2019). Loss of adaptive myelination contributes to methotrexate chemotherapy-related cognitive impairment. Neuron 103, 250–265.e8. doi: 10.1016/j.neuron.2019.04.032
Honoris, H. M., Wang, L., and Rios, D. (2020). Non-inferiority clinical trials: importance and applications in health sciences. Braz. Oral Res. 34:e072. doi: 10.1590/1807-3107bor-2020.vol34.0072
Hussein, E., Daoud, S., Alrabaiah, H., and Badawi, R. (2020). Exploring undergraduate students’attitudes towards emergency online learning during COVID-19: a case from the UAE. Child Youth Serv. Rev. 119:105699. doi: 10.1016/j.childyouth.2020.105699
Lahti, L., Salojärvi, J., Salonen, A., Scheffer, M., and de Vos, W. M. (2014). Tipping elements in the human intestinal ecosystem. Nat. Commun. 5:4344. doi: 10.1038/ncomms5344
Macro Trends (2024) Nigerian maternal mortality rate 2000 – 2024. Available at: https://www.macrotrends.net/countries/NGA/nigeria/maternal-mortality-rate (Accessed October 7, 2024).
Martín, C. T., Acal, C., El Honrani, M., and Mingorance Estrada, Á. C. (2021). Impact on the virtual learning environment due to COVID-19. Sustain. For. 13:582. doi: 10.3390/su13020582
Mba, C. J., Yunusa, U., Ibrahim, A. N., Rajah, A. S., Aliyu, F. M., Ndanusa, F., et al. (2021). Challenges associated with midwifery practice and education in northern Nigeria: way forward. Bayero J. Nurs. Healthcare 3, 906–917.
Muke, S. S., Tugnawat, D., Joshi, U., Anand, A., Khan, A., Shrivastava, R., et al. (2020). Digital training for non-specialist health workers to deliver a brief psychological treatment for depression in primary Care in India: findings from a randomized pilot study. Int. J. Environ. Res. Public Health 17, 1–22. doi: 10.3390/ijerph17176368
National Bureau of Statistics (2023) Demographic statistics bulletin 2022. Available at: https://nigerianstat.gov.ng/pdfuploads/DEMOGRAPHIC_BULLETIN_2022_FINAL.pdf (Accessed October 7, 2024).
Navarro, A. L. E. S., Tomas, J. P. Q., and Tomas, M. C. A. (2024). The impact of online learning on students and teachers: a systematic literature review investigating the effects during the COVID-19 pandemic. J. Electrical Syst. 20, 1340–1347. doi: 10.52783/jes.2180
Nayar, K. B., and Kumar, V. (2018). Cost benefit analysis of cloud computing in education. Int. J. Business Info. Syst. 27:205. doi: 10.1504/IJBIS.2018.089112
Nukunu, F., Odoi, P., Oppong-Boateng, V., Donkor, W., Bennin, L., and Addy, A. (2024). The journey to digitalization: the story of nursing and midwifery training colleges in Ghana. Ghana J. Nurs. Midwifery 1, 1–14. doi: 10.69600/z3pyqm13
Nursing and Midwifery Council of Nigeria, NMCN (2020). North should establish more nursing schools. Available at: https://www.sfhnigeria.org/northshould-establish-more-nursingschools-registrar-nmcn/ (Accessed October 9, 2024).
Nwaokugha, D. O., and Wogonwu, H. W. (2023). Prospects of online teaching and learning in Nigeria. Int. J. Educ. Learn. Develop. 11, 1–15.
Odongo, C. O., and Talbert-Slagle, K. (2019). Training the next generation of Africa's doctors: why medical schools should embrace the team-based learning pedagogy. BMC Med. Educ. 19:403. doi: 10.1186/s12909-019-1845-y
Picciano, A., Seaman, J., Shea, P., and Swan, K. (2012). Examining the extent and nature of online learning in American K-12 education: the research initiatives of the Alfred P. Sloan Foundation. Internet High. Educ. 15, 127–135. doi: 10.1016/j.iheduc.2011.07.004
Quinn, G. P., Bowman, C. M., Reich, R. R., Gwede, C. K., and Meade, C. D.ENRICH/ECHO Working Group, et al. (2019). Impact of a web-based reproductive health training program: ENRICH (educating nurses about reproductive issues in Cancer healthcare). Psychooncology 28, 1096–1101. doi: 10.1002/pon.5063
Reljic, N. M., Dolinar, M. D., Štiglic, G., Kmetec, S., Fekonja, Z., and Donik, B. (2023). E-learning in nursing and midwifery during the COVID-19 pandemic. Health 11, 1–14. doi: 10.3390/healthcare11233094
Shah, S., Shah, A., Memon, F., Kemal, A., and Soomro, A. (2021) Online learning during the COVID-19pandemic: Applying the self-determination theory in the “new normal” Revista de Psicodidáctica (English ed.), 26:168–177
Speciale, A.M. (2016). Midwifery in low resource environments: challenges and opportunities in maternal and reproductive health service provision. Doctoral thesis in demography, Department of Geography, Centre for Demographic Studies, Universitat autonomous da Barcelona, Spain.
Tekeş, H., and Uluşen, M. (2023). How effective digital technologies in midwifery education. European journal of. Midwifery 7. doi: 10.18332/ejm/172484
Terry, J., Davies, A., Williams, C., Tait, S., and Condon, L. (2019). Improving the digital literacy competence of nursing and midwifery students: a qualitative study of the experiences of NICE student champions. Nurse Educ. Pract. 34, 192–198. doi: 10.1016/j.nepr.2018.11.016
Tzitiridou-Chatzopoulou, M., Orovou, E., and Zournatzidou, G. (2024). Digital training for nurses and midwives to improve treatment for women with postpartum depression and protect neonates: a dynamic bibliometric review analysis. Healthcare (Basel) 12:1015. doi: 10.3390/healthcare12101015
Ujoh, F., Bola, R., and Lett, R. (2021). Stillbirths among pregnant women in Otukpo local government area, Benue state, North-Central Nigeria. Nigerian Health J. 21, 123–134.
Ujoh, F., Igbawua, T., and Paul, M. O. (2019). Suitability mapping for Rice cultivation in Benue state, Nigeria using satellite data. Geo-spat. Inf. Sci. 22, 332–344. doi: 10.1080/10095020.2019.1637075
Undie, S. B., Ojini, R. A., Udo, S. D., Effiong, A. A., Nkebem, U. B., Bisong, A. E., et al. (2024). Digital learning technology usage and teaching effectiveness of business educators in Nigeria’s south-south universities. J. Curriculum Teach. 12, 89–106.
UNFPA, WHO, and ICM (2021). The state of the World's midwifery 2021. Available at: https://www.unfpa.org/publications/sowmy-2021 (Accessed October 6, 2024).
Warren, N., Gresh, A., Mkhonta, N. R., Kazembe, A., Engelbrecht, S., Feraud, J., et al. (2023). Pre-service midwifery education in sub-Saharan Africa: a scoping review. Nurse Educ. Pract. 71:103678. doi: 10.1016/j.nepr.2023.103678
Webster, K. (2024). The impact of online learning during the Covid-19 pandemic on academic outcomes for newly-struggling high school Students. Online Learn. 28, 427–444. doi: 10.24059/olj.v28i3.3680
Wei, H., and Chou, C. (2020). Online learning performance and satisfaction: do perceptions and readiness matter? Distance Educ. 41, 48–69. doi: 10.1080/01587919.2020.1724768
WHO (2019). Framework for action: Strengthening quality midwifery education for universal health coverage 2030. Switzerland: WHO.
WHO, UNICEF, UNFPA, World Bank Group, and United Nations Population Division (2017). Trends in maternal mortality: 2000 to 2017. WHO, UNICEF, UNFPA, World Bank Group and the United Nations population division. Available at: https://data.unicef.org/resources/trends-maternal-mortality-2000-2017/ (Accessed March 25, 2021).
Wilcha, R. J. (2020). Effectiveness of virtual medical teaching during the COVID-19 crisis: systematic review. JMIR Med Educ. 6:e20963. doi: 10.2196/20963
World Health Organisation (2021). Global Health Observatory data repository: nursing and midwifery personnel. Available at: https://apps.who.int/gho/data/node.main.HWFGRP_0040?lang=en (Accessed November 19, 2022).
Keywords: RCT, non-inferiority test, digital training, midwifery education, MADE-I, FIRST
Citation: Ujoh F, Dzunic-Wachilonga A, Noor R, Gusa V, Ape-aii R, Ohene I, Bola R, Christilaw J, Hodgins S and Lett R (2024) Digital vs. conventional instructor-led midwifery training in Benue State, Nigeria: a randomized non-inferiority trial. Front. Educ. 9:1470075. doi: 10.3389/feduc.2024.1470075
Edited by:
Octavian Dospinescu, Alexandru Ioan Cuza University, RomaniaReviewed by:
Utkarsh Bansal, Hind Institute of Medical Sciences, IndiaVíctor Hugo Fernández-Bedoya, Cesar Vallejo University, Peru
Copyright © 2024 Ujoh, Dzunic-Wachilonga, Noor, Gusa, Ape-aii, Ohene, Bola, Christilaw, Hodgins and Lett. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fanan Ujoh, ZmFuYW4udWpvaEBjbmlzLmNh