 Nashreen Behardien
Nashreen Behardien Simone Titus
Simone Titus Nicolette V. Roman
Nicolette V. Roman- 1Department of Maxillofacial and Oral Surgery, Faculty of Dentistry, University of the Western Cape, Cape Town, South Africa
- 2Department of Health Professions Education, Stellenbosch University, Stellenbosch, South Africa
- 3Faculty of Community and Health Sciences, University of the Western Cape, Bellville, South Africa
- 4South African Research Chair in Family Studies, Centre for Interdisciplinary Studies of Children, Families and Society, Faculty of Community and Health Sciences, University of the Western Cape, Bellville, South Africa
Introduction: Curriculum review is crucial for ensuring health professions education programs remain responsive and relevant. Teaching and learning (T&L) strategies facilitate knowledge acquisition, with traditional methods being supplemented by innovative techniques in a blended curriculum. This study evaluated an Exodontia Block Course (EBC) focused on tooth extraction skills, utilizing a blended-learning approach across three learning environments: classroom, preclinical skills laboratory, and clinical training platform.
Methods: A qualitative study employed appreciative inquiry for data collection and analysis. Focus group discussions were conducted with 30 participants: 13 undergraduate students, 10 clinical teachers, and 7 dental practitioners. Data underwent coding and thematic analysis.
Results: Two main themes relevant to this paper emerged: “Block course structure” and “Recommendations for improvement.” Participants affirmed the blended-learning approach, highlighting strengths like demonstrations, videos, activity workbooks, and assessments that supported learning. Recommendations included integrating more visual technologies, simulated patients, peer-learning, debriefing, case reviews, community-based learning, and dedicated skills laboratories.
Discussion: While the traditional course adequately achieved its objectives, opportunities for enhancement were identified. Incorporating advanced educational technologies, simulation-based activities, and structured feedback mechanisms could optimize skills development. Real-world clinical experiences and peer-assisted learning may reinforce knowledge and foster competencies like clinical reasoning. Continued curriculum refinement through stakeholder feedback is essential for delivering effective, student-centered dental education, and by inference, improved patient care.
1 Introduction
Curriculum review is an important and necessary feature of health professions education (HPE), ensuring that academic programs remain reflexive, responsive, and relevant. Teaching and learning (T&L) strategies, also known as instructional methods, are techniques used to deliver the content required to achieve the learning outcomes or course objectives. Furthermore, they are utilized to support student learning through diverse approaches aimed at fostering knowledge acquisition. Given the constant changes in technology and shift to a learner-centered approach, HPE has had to adapt. Traditional teaching methods are now being supplemented or replaced by more sophisticated techniques in a blended curriculum (Timothy et al., 2016; Baig, 2020; O’Doherty et al., 2018). Several methods for disseminating information have emerged in recent years. The term ‘educational media’, as described by Baig (2020), encompasses any method of communication used to relay information to learners or students. These may include presentations, handouts, podcasts, virtual reality or computer technology, and mobile technologies (Baig, 2020). A plethora of effective methods using educational technologies exist to enhance student learning and success. Thus, educators need to design innovative ways of T&L using technology. Charlton et al. (2012) presents a range of conventional digital educational strategies designed for acquisition, collaboration, discussion, investigation, production, and practice. Moreover, it is important to emphasize that students are key stakeholders, and their learning preferences, combined with the evolving technological landscape, should guide the selection of instructional methods. Therefore, incorporating innovative teaching strategies into every health educator’s toolkit is imperative.
At a dental school in the Western Cape Province in South Africa, the module coordinator (principal investigator [PI]) of an Exodontia Block Course (EBC) embarked on an evaluation of a 4-day course as part of a curriculum renewal initiative. The course focused on imparting skills in injection techniques and tooth extraction (exodontia). Exodontia, a dental procedure primarily used for treating dental pain and infection, is considered an essential skill for dentistry students as a basic competency before graduating, applicable to all dentists and dental therapists worldwide (Manogue et al., 2011; Health Professions Council of South Africa, 2014). The EBC is offered in the sixth semester (Semester 2 of the 3rd year) using a blended-learning format. This approach integrates various instructional tools, including PowerPoint lectures presented in a didactic mode, video clips demonstrating relevant clinical procedures, activity workbooks focusing on exodontia instruments, an online quiz for reviewing content from previously passed modules, live demonstrations, clinical practice rotations, and a preclinical assessment to gauge students’ readiness for clinical training. The blended-learning approach has been successfully employed in HPE (Coyne et al., 2018), including exodontia skills development (Omar, 2017). Within dentistry education, students have identified opportunities such as research relevance, health connections and flexible scheduling as a result of improved blended online learning provision (Punzalan and Roberto, 2023). Some students in medical education held favorable views toward a blended learning environment due to the key advantages and affordances relating to flexibility and convenience for the end user. In their study, students showed a preference for well-organized content on easily accessible platforms and they expressed a desire for interactive elements in each study unit, believing these would optimize their learning process and improve overall outcomes (Zubair et al., 2024). Furthermore, Li et al. (2024) found that the online components of a blended learning curriculum strengthened the analysis and discussion of actual clinical cases and students were better enabled to solve practical clinical problem.
In this course, the development of exodontia skills is facilitated across three physical learning environments: (i) the classroom, (ii) the preclinical skills laboratory, and (iii) the clinical teaching and training platform. These learning environments are defined as physical or virtual spaces specifically designed and tailored to the content being taught, ensuring they are fit for purpose, such as a chemistry laboratory and a computer laboratory, among others (Leijon et al., 2024; Ralph et al., 2022). The interplay of these environments enables scaffolding, integration, and transfer of knowledge, supporting students’ progression from novice to competent. Figure 1 illustrates the learning spaces, along with the T&L strategies employed during the presentation of the course.
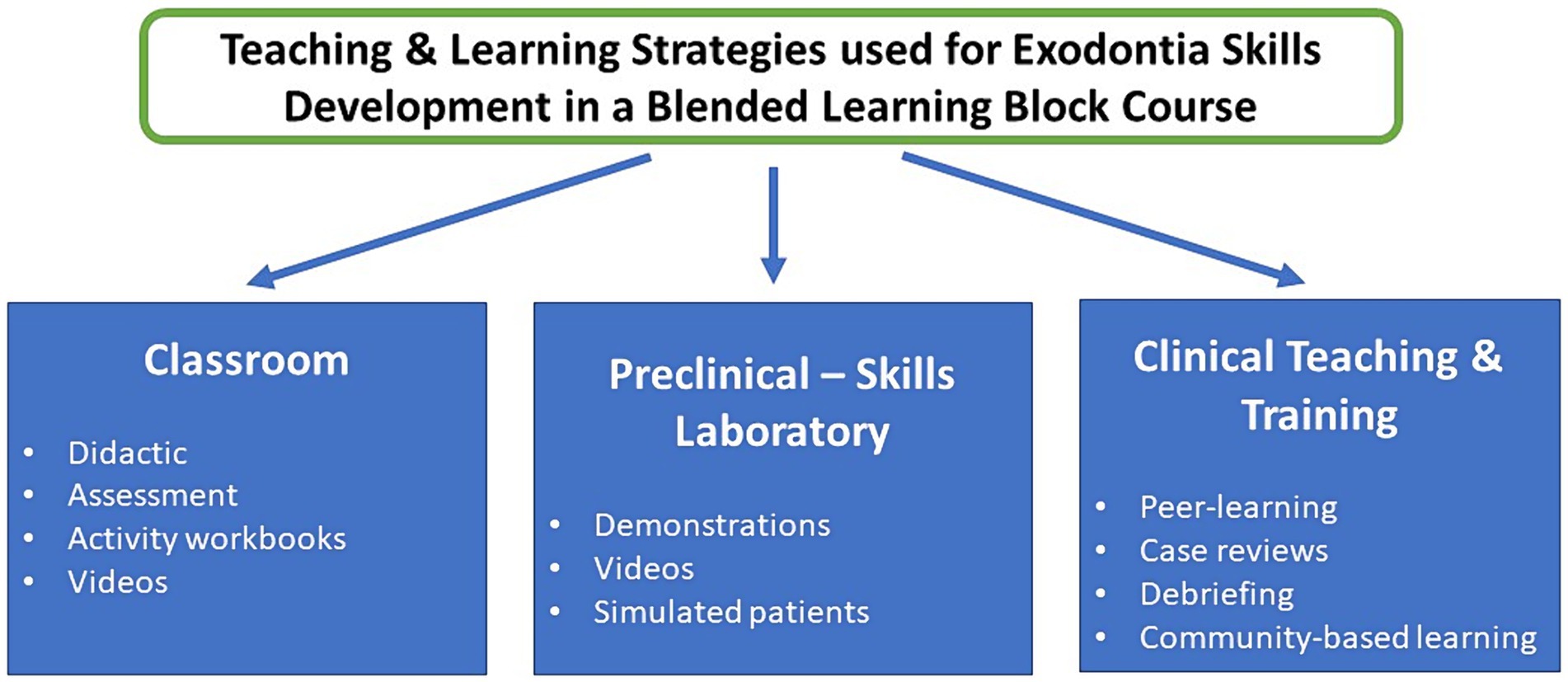
Figure 1. Teaching environments highlighting the strategies employed and explored in this study.
In this course, the classroom environment served as an in-person, face-to-face space where didactic teaching and video presentations were the primary modes of content delivery. Conversely, the preclinical skills laboratory furnished the infrastructure and opportunity for hands-on practice of technical skills related to tooth removal, encompassing aspects such as clinician and patient positioning. Subsequently, the practical application of these skills was undertaken in a clinical setting with real-life patients, fostering the development of clinical reasoning. However, owing to resource constraints, the preclinical skills laboratory consisted of a modified classroom, or the clinic was used as a skills laboratory for student practice with simulated patients. Therefore, this study set out to evaluate the existing T&L strategies of the existing exodontia block course in order to enhance exodontia skills through curriculum redesign.
This evaluation aimed to gain insight into T&L strategies employed to enhance exodontia skills. Hence, this paper reports on the T&L strategies identified by the participants in the evaluative study of the EBC.
2 Materials and methods
2.1 Study design
This qualitative research employed appreciative inquiry (AI) as a guiding framework for data collection and analysis.
2.2 Participants
The research was conducted at a South African dentistry school and involved participants from various groups. These included clinical teachers (CTs) in the Maxillofacial and Oral Surgery Department, undergraduate dentistry students who completed the EBC, and dental practitioners (DPs) who completed the EBC as undergraduates. Participants from the 3rd to 5th year classes were invited to participate in the study through class representatives using the institutional learning management system (LMS). DPs from both private and public settings were recruited through invitations. The PI invited three practitioners and asked them to share the invitation with colleagues who may be interested in participating. The interested parties contacted the PI and formed part of the sample. Consent was obtained through Google Forms after sharing detailed information about the study.
In total, the study comprised 30 participants. The student sample consisted of four (4) third-year students, four (4) fourth-year students, and five (5) fifth-year students. The total number of students eligible to participate in this study was 261 (90 third-years, 85 fourth-years and 86 fifth-years). Among the student sample, there were 13 participants, with seven (7) males and six (6) females. The CT sample included 10 participants, with an equal distribution of five (5) male and five (5) female participants. The DP sample consisted of seven (7) dentists, comprising four (4) males and three (3) females.
2.3 Ethical considerations
The study received approval from the institution’s Review Committee (BM19/10/23). Participants were invited to provide informed consent, and research assistants were briefed on data protection protocols. Data were securely stored both on Google Drive and a laptop. To maintain confidentiality, participants were assigned codes (e.g., SIII1) rather than being identified by name. Participation was voluntary, without any incentives offered, and participants had the option to withdraw from the study at any time without facing any penalties.
2.4 Data collection and analysis
Data collection took place from July 2020 to March 2021. Demographic information was gathered using Google Forms. The PI facilitated the first two focus group discussions (FDGs), one with a group of two students and another with a group of six CTs. These initial FGDs were conducted in-person and served as a pilot study. Following this, to mitigate potential bias, an external facilitator conducted the remaining five FGDs, each involving between four and seven participants. An external facilitator, an experienced qualitative researcher in the field of health professions education with an excellent understanding the principles of FGDs and adept at understanding participant responses and identifying areas that require follow up was, was selected to facilitate the discussions.
Due to the COVID-19 pandemic, the FGDs were conducted using Google Meet. Data from the pilot study were analyzed to evaluate the clarity of the questions in accordance with the AI framework and to evaluate the duration of the FGDs. As only two participants were present in one session, it did not meet the criteria to constitute a focus group, and therefore, the data from this session were excluded from the analysis. Torrentira (2020) strongly recommended video-conferencing as an adaptive mechanism to replace in-person focus group discussions (FGDs) introduced during the COVID-19 pandemic, enabling research to continue despite imposed restrictions. The online format for FGDs introduced both advantages and limitations to data collection. Advantages included reduced costs for both participants and researchers. In this study, it allowed for the inclusion of a CT from another continent and approximately three other participants from other South African cities. However, the online format also presented potential limitations. One concern was that participants might not engage equally in the discussion, especially if their webcams were not activated. Throughout the study, only one instance was noted where a participant experienced connectivity issues and had to rejoin the meeting multiple times. A significant drawback of the online format is the potential loss of facial expressions from participants due to inactive webcams from technical issues such as reduced bandwidth. This loss of visual cues can hinder the facilitator’s ability to effectively direct the discussion. Additionally, there may have been the loss of potential participants, but connectivity or data issues may have excluded them. In reviewing the data and findings, it’s crucial to consider these potential limitations of the online FGD format. Despite these challenges, the online approach proved to be a valuable tool for conducting research during the pandemic, balancing safety concerns with the need for the continuation of the research.
The AI framework guided the development of questions for the FGDs. An interview guide (Table 1) was created to allow for flexible exploration of participants’ experiences of the course.
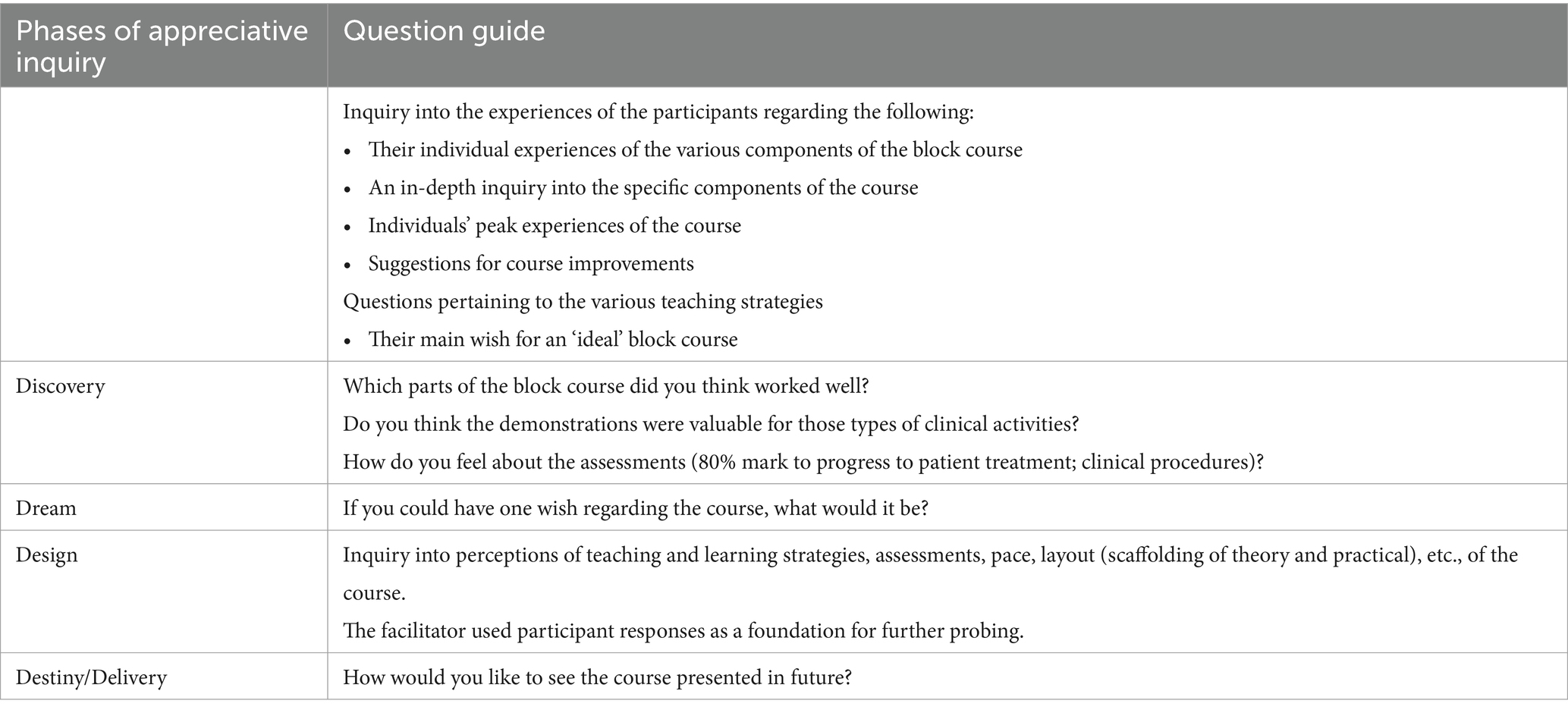
Table 1. Semi-structured topic guide using the AI framework.
The FGDs lasted between 50 and 110 min each, and data collection continued until saturation was achieved or no new information emerged. The time between completing the course and the discussions was 29 months. For third-year students, the interval was approximately 1 month, while for fourth-year students, it was approximately 22 months. The group discussion format was chosen to enhance reliability, particularly with longer intervals, as it aids memory recall and helps mitigate recall bias. The time between the EBC and FGDs varied by year, with fifth-year participants having graduated and completed 2 weeks of mandated public sector service.
All data were transcribed verbatim in English. The latter underwent coding using an open coding method and were analyzed following Tesch’s eight steps. During the analysis, the PI and external coder familiarized themselves with the data and made initial notes about potential patterns and any novel and interesting points raised by the participants (independently). This study used open and inductive coding by systematically working through the entire dataset. The external coder was the primary coder. In the initial phase of open coding, the external coder broke the data down into distinct units of meaning based on the outcomes of the teaching and learning strategies. Each of these units were coded, after which some of the codes were condensed. Coding was also done inductively as the themes were derived directly from the data as no pre-conceived categories were formed. This was useful in the exploration of new ideas as it related to the teaching and learning strategies. The codes were sorted into potential themes and many were combined to form the overarching themes. These themes were reviewed by the PI, who met on numerous occasions in order to reach consensus on, and finalize the themes. The analysis of the data was interpreted through the lens of the AI framework, as outlined by Priest et al. (2013).
AI is recognized as both a theory of organizing and a method for facilitating change within organizations and communities. It shares several core principles with action research methodology (Cooperrider and Whitney, 2000).
The research design was guided by the 4-D AI model (Hammond, 2013). This model comprises four distinct phases: Discovery, Dream, Design, and Destiny/Delivery. The Discovery phase draws on the best of the current situation (Watkins et al., 2019). The Dream phase represents aspirations for what could be, while the Design phase involves consensus on what should be. Finally, the Destiny/Delivery phase is an experiment to achieve what is possible (Watkins et al., 2019). FGDs allowed for rich data collection while reducing potential researcher bias (Barbour, 2005). The AI framework was used to delve and explore the strengths, weaknesses and deficiencies related to the course by application of the AI framework. Figure 2 provides some insight into the application of AI within study. The generated data was themed as described above and presented such to highlight the course strengths, areas for improvements and gaps within the curriculum.
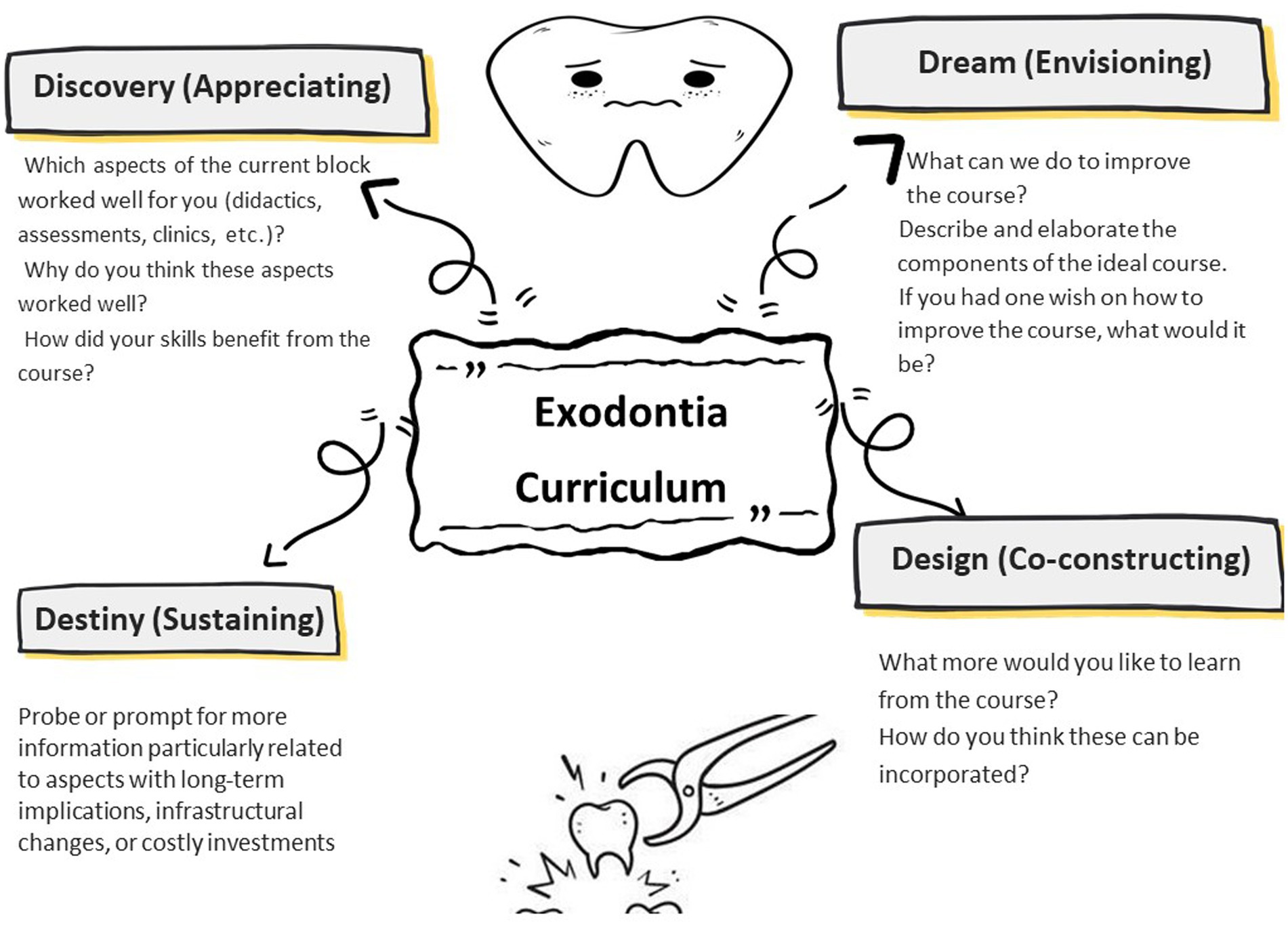
Figure 2. A graphic illustrating the use of appreciative inquiry as a data collection approach with guiding questions used to explore the exodontia course curriculum.
3 Results
This is a third report of the larger study, with comprehensive demographic information reported in a previous paper (Behardien et al., 2023).
3.1 Clinical teachers
Twelve eligible CTs were invited, and 10 participated, resulting in a response rate of 83.3%. Their ages ranged from 27 to 62 years, with a mean age of 36.6. The CTs’ teaching experience varied from 4 to 30 years. Predominantly, they were part-time faculty members, mainly from the private sector, dedicating between 8 to 20 h per week to teaching on the clinical platform. On average, they spent 33.1 h per week practicing as general dentists. The majority (80%) of the CTs held postgraduate qualifications, including oral surgery honors and master’s degrees, oral surgery diplomas, and a law degree. Additionally, two CTs were enrolled in oral surgery diploma programs. Notably, three CTs had left the school: one had emigrated, one had transitioned to the public sector, and one had commenced specialist training in maxillofacial surgery.
3.2 Students
Thirteen students participated in the FGDs, despite the challenges posed by their busy academic schedules and the stress and anxiety associated with the COVID-19 pandemic, which particularly affects healthcare students (Saladino et al., 2022). The student participants requested that the FGDs be held after hours, considering their daytime clinical commitments. The ages of the student participants ranged from 22 to 25 years, with a mean age of 22.87 years.
3.3 Dental practitioners
The seven dental practitioners (DPs) in the study represented various sectors, including private practice, public sector, academia, and the military. Their ages ranged from 23 to 33 years, with a mean age of 28 years. The time since their qualification varied from 1 to 9 years.
3.4 Identified themes and sub-themes
The themes identified from the data represented the strengths, deficiencies, and recommendations for enhancing the traditional course curriculum. Specifically, two prominent themes emerged: Block course structure and Recommendations for improvement, both of which encapsulate insights regarding T&L strategies. These findings are summarized in Table 2.
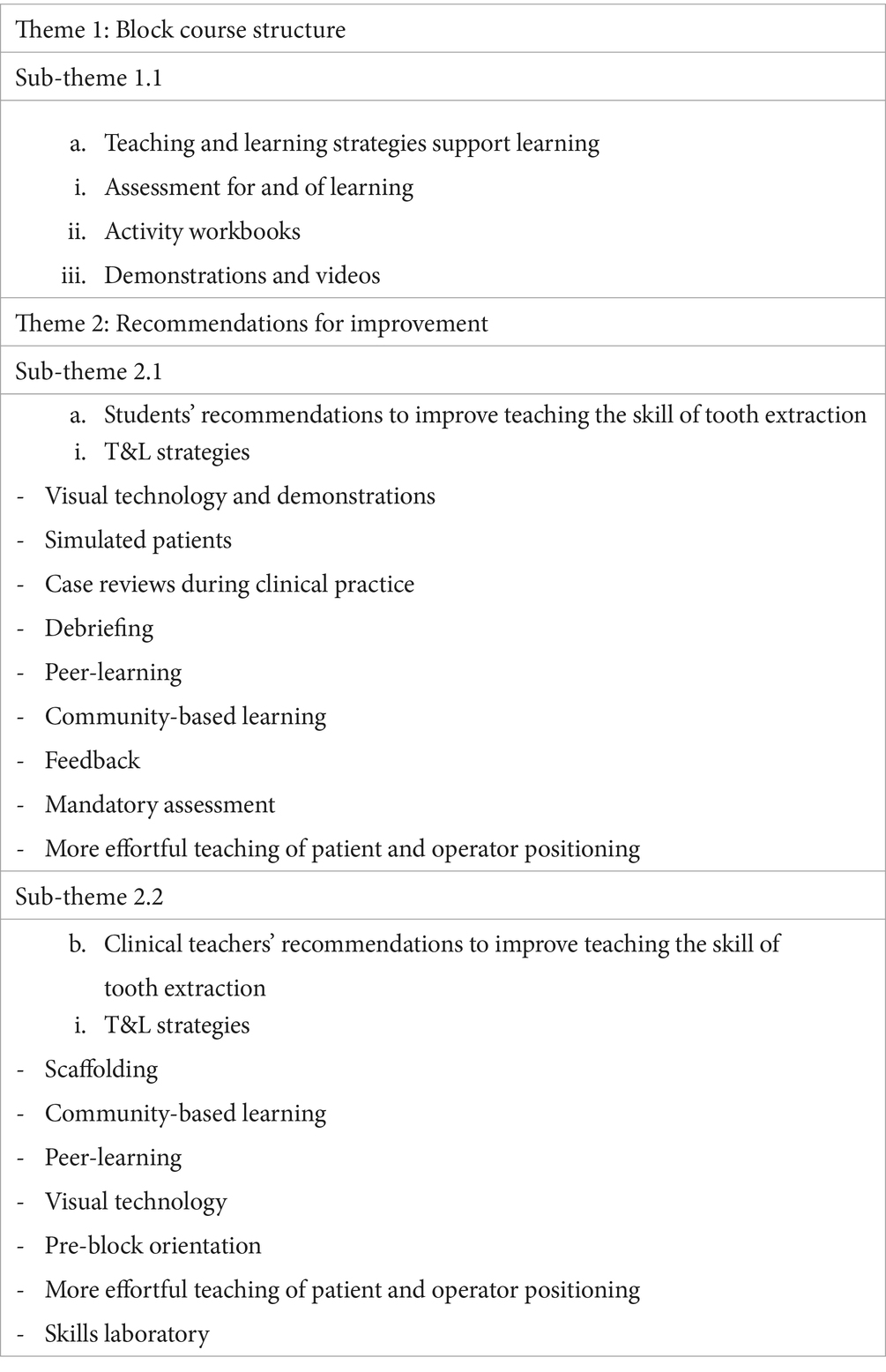
Table 2. Presenting themes and sub-themes encapsulating the findings on T&L strategies described in the study.
A diverse array of T&L strategies was observed across the three learning environments. Under the theme of Block course structure, one sub-theme highlighted the supportive role of T&L strategies. Within the Recommendations for improvement theme, two sub-themes emerged, shedding light on the recommended T&L strategies as perceived by both the student and CT groups. These identified strategies are elaborated upon and discussed more detail in Table 2.
3.4.1 Theme 1: block course structure
The sub-theme Teaching and learning strategies support learning confirms that student learning within the course is augmented by the variety of T&L strategies employed. Assessment tools utilized for active learning activities encompassed the instrumentation workbook, as well as demonstrations and videos. The participants shared the following with regards to ‘assessment for and of learning’ to bolster this sub-theme:
And then realised afterwards [after the assessment] that if I know my stuff, you automatically have that confidence in clinics. SV5.
So, I think for us to know our work, getting the 80% just makes sure that we are doing the job. SIII2.
I think what they did by the workbook where, as (SIII2) said they told us where we can use it, how to use it, and the picture of it as well as actually handling the instruments were very helpful. SIII4.
It did definitely help to have the demo before going to the patient. SIII3.
The blended-learning approach adopted for this course facilitated students’ participation in various T&L strategies. While the didactic component was perceived positively overall in this study, it was also recognized as inadequate for delivering all types of content. The following quotations, drawn from all three participant groups, provide support for these assertions:
I think that, the blended approach is definitely more important for students now, than the didactic approach that we were given, many years ago… we found that blended techniques definitely helped students visualise and also contextualise what they needed. CT7.
…lecturers actually wanted me to do a bit of self-study… So, you kind of have to you get the basics, you get the references, and you kind of have to go into the meat to that end. And that was my style of learning. It wasn’t just to learn what was on the slide and so on. And then you teach yourself, learn it in the clinic, much more in the clinic and from your peers and your colleagues than in your lectures at that point. DP3.
So maybe teaching the emergency med lecture more like practically, or maybe having like a like a, like a someone example fake fainted patient, and then asking the cause the person is fainted. ‘How do you solve the problem now? SV2.
3.4.2 Theme 2: recommendations for improvement
Participants in this study provided several suggestions for enhancing the EBC. Feedback encompassed the utilization of educational technologies, incorporation of simulated patients, peer learning, and debriefing sessions.
Educational technologies, particularly the use of information and communication technologies (ICT) in higher education, featured strongly in the feedback from the student group. Participants expressed that videos demonstrating procedures served as effective tools for supporting student learning of psychomotor skills. The convenience and accessibility of video content were particularly praised, as indicated by the following quote:
So, tutorial videos are my thing, especially now we are into technology and you have it [technology]. So now instead of referring you to that lecture, you can refer to that video. SV6.
ICT represents a diverse array of educational technologies. Within the context of simulation-based medical education (SBME), more advanced technological tools are employed. These technologies facilitate active learning approaches, often utilized within SBME contexts. Primarily, SBME activities occur in preclinical skills laboratories, which serve as crucial transitional spaces bridging theoretical knowledge with practical application. In this study, the student participants advocated for a broader integration of technology. Similarly, the CT and DP samples also recommended the introduction and use of a skills laboratory. The following quotation encapsulates these perspectives:
And I think, that most of us learned more from that, in the clinic [used as a skills laboratory] where they were giving us simulation on a patient as compared to 12 of us around someone in class, so that’s what I personally feel. SIII1.
The clinical teaching and training environment offer students invaluable opportunities to practice psychomotor skills in a real-life context. Clinical training plays a pivotal role in honing clinical skills and reasoning, serving as a crucial bridge between theory and practice. In essence, the clinical platform itself serves as a T&L strategy for fostering the development of psychomotor skills. The following quotations exemplify the perspectives on the benefits of clinical training for skills acquisition:
So you do not expect them, within the block, after three days, to be able to remove, extract any tooth, it’s not realistic. It just acts as a transition of what they have learned in the lecture to the demo, and now into the clinic. CT4.
You can have all the demos [demonstrations] you want; you can play with all the mannequins. But if you need the chair side teaching, and I think that is one area where the programme is good at, at UWC, you get a lot of exposure as a student from early on. CT4.
Both the student and CT groups offered valuable insights into potential enhancements for learning on the clinical platform. Their suggestions encompassed various strategies such as clinical case discussions, peer-learning, debriefing, and feedback. Many of the students’ suggestions pertained to CT contributions. The following quotation outlines the strategies recommended to improve the course:
I think SV3 has an excellent idea with a debriefing thing. I think also that everyone should remember that we are all human beings. I think that we are going to struggle, but we have to learn from that as well. I think a debriefing session is really good. Good idea at the end of the session because anything could happen in the clinic. And anyone can learn from it. SV1.
Senior students demonstrated clinical competence and confidence while sharing perceived shortcuts with junior students. Peer-teaching served to reinforce tutors’ own knowledge, highlighting the effectiveness of peer-learning as a method for formal inclusion to support learning and cultivate core professional competencies.
Being able to show someone as well. And when it works, and you just feel like you actually taught someone something. And it helps you reinforce your mental cues that you use when, when you are going to inject. SIV2.
I advocate for peer-learning. With Oral Surgery, you always get questioned like, during your presentation or afterwards. So, you’ll find us huddled up in some corner. Like, guys, how do you do this? Or this? And I have retained every single piece of information that I picked up from those huddles. So, it works for me, it really does. SIV3.
Within the clinical teaching and training environment, senior students expressed a desire for more case reviews (discussions) during clinical rotations. While this feedback extends beyond the parameters of the 4-day block course, it underscores the ongoing process of learning and the evolution of critical thinking, clinical reasoning, and reflection as students progress through the dentistry program.
As part of the continuum of skills acquisition, dental practitioners stressed the importance of preparing graduates for real-world practice, echoing similar sentiments across different contexts. Senior student participants highlighted the advantages of working in community settings. However, it is worth noting that clinical practice in such settings may not directly relate to the initial development of exodontia skills (EBC). Instead, it reflects the progression of student skills along the continuum toward competency.
4 Discussion
The evaluation of the EBC confirmed that the course adequately addressed the basic requirements outlined in its objectives. Literature on exodontia education is quite limited with the most expansive studies coming from the United Kingdom (MacLuskey et al., 2008; MacLuskey and Durham, 2009) and Europe (Brand et al., 2015). These studies however, do not provide, detailed or comprehensive information on any particular course or curriculum regarding exodontia skills development. However, a significant amount of feedback indicated potential areas for improvement, warranting further academic investigation. The utilization of the 4-D AI model for data collection and analysis played a crucial role in identifying the strengths, deficiencies, and recommendations for improving the course. Despite the significance of exodontia skills in dental practice, there has been a notable imbalance in research attention within the field of dentistry compared to medicine and nursing education. This observation underscores the need for increased research focus and scholarly inquiry in dental education, particularly concerning essential clinical skills like exodontia.
Many of the T&L strategies employed were active learning strategies, while passive learning strategies were primarily observed in in-person, didactic PowerPoint presentations delivering course content, along with certain types of ICT. This study indicates that more effective T&L strategies can be utilized in preclinical oral surgery, particularly when an ample amount of content is delivered through active learning strategies, as highlighted in previous research (Omar, 2017).
4.1 Passive strategies
4.1.1 Didactics
Some healthcare programs overemphasize didactic theory at the expense of psychomotor skills instruction (DeBourgh and Prion, 2017). Zou et al. (2011) suggest that didactic teaching is advantageous for conveying substantial amounts of information to sizeable classes during the preclinical years of medical school, with students often passively listening as the lecturer presents the topic. Innovative pedagogical strategies, including videos and simulations, can better prepare students for the complex challenges of their future roles, such as providing culturally appropriate care (Forbes et al., 2016; Sivarajah et al., 2019) They advocate for the integration of videos and simulation incorporating problem-solving skills, as these methods better equip health students for the multifaceted challenges inherent in their future professional roles, such as providing culturally appropriate care.
4.1.2 ICT
In this study, the student group expressed a positive reception toward video clips showcasing clinical procedures. Videos offer the advantage of allowing learning to occur at an individual pace, enabling learners to take control of information reception. This flexibility is manifested through unlimited viewing opportunities and the ability to access content independently, irrespective of time and location. Moreover, video-based learning incorporates images, graphics, on-screen text, and audio to deliver a multi-sensory learning experience, accommodating various learning styles. This holistic approach fosters engagement with the content, consequently enhancing learning outcomes and facilitating knowledge retention (Kosterelioglu, 2016). According to Dale (1969), the more senses that are involved in the learning process, the more meaningful the learning experience becomes. Additionally, Berk (2009) asserts that videos utilized for educational purposes have both a cognitive and affective impact.
4.1.3 Active learning strategies
Active learning strategies enhance knowledge retention, critical thinking, motivation, and interpersonal skills while reducing course failure rates (Shin et al., 2015; Skene et al., n.d.). Tools like simulated patients and activity workbooks facilitate this approach. Additionally, scaffolding the learning process is beneficial in refining psychomotor skills development.
Simulation-based medical education–Preclinical skills laboratories and clinical training platforms play a crucial role in refining clinical skills. The introduction of skills laboratories or clinical skills centers for clinical skills development has gained traction since the 1990s. In the field of dentistry, Raina et al. (2021) and Omar (2017) have explored and delineated the benefits of simulation education offered within clinical skills centers. These centers, also referred to as clinical skills laboratories or clinics, provide students with opportunities to practice clinical tasks in a simulated real-world environment, devoid of actual patients. Programs are increasingly incorporating clinical simulation to furnish students with a realistic, safe, and low-pressure environment conducive to the development of clinical skills and reasoning. To prevent any potential compromise to patient care during student training in a clinical setting, various simulations are accessible to provide dentistry students with opportunities to practice oral assessments, examination techniques, and clinical procedures. However, it is worth noting that this study may have fallen short in fully assessing the true value of a skills laboratory. The institution lacked a dedicated skills laboratory for oral surgery procedures, resorting instead to a modified classroom and clinical area as makeshift laboratories. This limitation could have potentially hindered participants from fully grasping the value or benefits of such facilities, thereby compromising the feedback’s accuracy on this topic.
4.1.4 Clinical teaching and training
Clinical teaching and training, a necessary component of HPE, is required for students to gain the maximum benefit from the clinical platform. Various T&L factors contribute to this process, including an optimal student/CT ratio (Shoaib et al., 2018), appropriate and functional instruments and equipment (Bauer et al., 2020), and ideal patient case selection (Bauer et al., 2020). Procedural skills are imparted through diverse methods, incorporating an array of tools and techniques (Houghton et al., 2013; Coyne et al., 2018). With evidence supporting the association of increased complications for patients treated in the traditional apprenticeship model (Stather et al., 2013), skills clinics or surgical skills laboratories provide guided practice for learning psychomotor skills. These facilities are designed to embed opportunities for students to develop the following skill sets: safety awareness and proactive actions to minimize risk and harm to providers and patients; the associated clinical reasoning to enable sound decision-making and problem-solving abilities related to the performance of specific skills; and flexible, nimble practice in responding to dynamic practice environments, including variation in patient clinical conditions and equipment requiring principal-based procedure modifications (DeBourgh and Prion, 2017).
In this study, the student group highlighted clinical case discussion (problem-based learning) as a valuable tool for learning, particularly in enhancing critical thinking and retaining information. Notably, senior students advocated for increased opportunities for case discussions on the clinical platform. This underscores the notion that skills development occurs along a continuum, extending beyond the parameters of the EBC. While medical schools have integrated problem-based learning into the preclinical years to promote more active learning, a criticism is that although students retain information better through problem-based learning, the breadth of knowledge covered may not be as extensive as with didactic teaching (Zou et al., 2011). Thus, carefully designed scaffolded curricula are crucial for maximizing learning outcomes. The clinical practicum provides a platform for deploying various T&L strategies.
Debriefing, or after-action review, a strategy recommended to improve the course, originated in the military, where servicemen would review a mission to enhance its outcomes. For the purpose of this paper, the concepts of ‘debriefing’ and ‘feedback’ are discussed as one. In a clinical context, feedback is defined as ‘specific information about the comparison between a trainee’s observed performance and a standard, given with the intent to improve the trainee’s performance’ (Van De Ridder et al., 2008). According to Ende (1983), feedback in medical education is a key step in the acquisition of clinical skills. It is integral to the experiential learning theory (Kolb and Kolb, 2005) and is considered the cornerstone of effective clinical teaching, essential to medical education (Cantillon and Sargeant, 2008). Gauthier et al. (2015) emphasize the importance of quality feedback in endocrinology education. The findings of this study recommend increased opportunities for debriefing on adverse clinical events as learning opportunities for a larger group than merely the student involved in the event. Additionally, an increase in feedback from clinical sessions was identified as a strategy needing enhancement.
Peer-learning was regarded as a strength of the program, and there was a suggestion for more opportunities in this regard. Stelzle et al. (2011) specifically mention senior students serving as peer-tutors for juniors. Student–student interaction, overall, offers advantages over solely faculty instruction, including relatability and straightforward communication. Formal peer-tutoring programs enable senior students to consolidate their expertise while empowering juniors through competence modeling and sharing valuable insights and tips (Stelzle et al., 2011). This study discovered that peer-learning among students, both within the same year and across different years of study, yielded significant benefits. Peer-learners emphasized the importance of identifying with peers and found ease of communication crucial when seeking advice from fellow students rather than CTs. Sharing information was the most common reason for peer interaction.
Community-based clinical practice was strongly supported by senior students and DP participants, viewing it as an opportunity to enhance clinical speed, understand patient context, and develop critical thinking and clinical reasoning skills. This aligns with the broader goal of preparing graduates for real-world practice. Morris (2012) advocates for immersing students in the professional community, integrating T&L into daily activities. This “learning by doing” approach makes learning more explicit, especially in clinical settings compared to traditional classrooms. However, the value of community-based oral surgery skill development is subject to debate. MacLuskey and Durham (2009) discovered that outreach activities can detract from oral surgery teaching by removing students from that specific environment. In summary, community and workplace-based learning offer opportunities for authentic professional immersion, bridging classroom lessons with integrated clinical practice. However, their effectiveness in developing specific skills such as oral surgery is a topic of debate. While some view workplace participation as conducive to contextual learning-by-doing, others argue it may divert attention from targeted competencies. Further research is warranted to evaluate the efficacy of real-world training for particular skill sets.
The data from this study suggest that while the strategies employed in the course are sufficient for achieving the course outcomes, there is still room for improvement. It is noteworthy that some of the feedback pertains to clinical practice occurring beyond the scope of the EBC. Nonetheless, these suggestions may be considered for future integration into a revised course, as clinical skill acquisition occurs along a continuum of learning. Medical education has evolved from passive, knowledge accumulation to more engaging, student-centered learning approaches (Adefuye et al., 2018). Skills laboratories, which have gained momentum since the 1990s, allow students to practice clinical skills without the involvement of real patients (Raina et al., 2021; Omar, 2017). Simulations provided in these laboratories foster the safe development of skills and clinical reasoning. Guided practice within these environments builds capacities such as risk minimization, which may otherwise be compromised in traditional apprenticeship models (Stather et al., 2013; DeBourgh and Prion, 2017). Integrating technology into these laboratories offers opportunities to transform 2D workbook instrumentation into multidimensional, rotatable representations. Having appropriate staff facilitate dedicated labs enables valuable hands-on participation that is impossible in makeshift classrooms.
5 Conclusion
This paper provided insights into an EBC and the pedagogical value of the T&L strategies used in developing skills for tooth extraction. Due to the paucity of literature on comprehensive evaluations of exodontia education, there is limited information to compare the findings of this study to. By considering the perspectives of multiple stakeholders with varying levels of training, this evaluation offered in-depth and comprehensive information regarding the epistemological and ontological outcomes of the course. The study highlighted that while the didactic approach may have limited appeal to students, it can be effectively enhanced within a blended learning environment. Additionally, while the overall structure, pace, and sequencing of the EBC components were positively affirmed, insightful student-centered recommendations have been made for future improvement and practice.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Biomedical Research Ethics Committee of the University of the Western Cape. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
NB: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Writing – original draft, Writing – review & editing. ST: Conceptualization, Data curation, Writing – review & editing. NR: Conceptualization, Methodology, Supervision, Writing – review & editing.
Acknowledgments
We thank the participants (students, clinical teachers, and dental practitioners) for taking the time and sharing their experiences and opinions in this study. We also thank Andisiwe Mjacu for graphic assistance.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Adefuye, A., Adeola, H. A., and Bezuidenhout, J. (2018). Medical education units: a necessity for quality assurance in health professions education in Nigeria. Afr. J. Health Prof. Educ. 10:5. doi: 10.7196/AJHPE.2018.V10I1.966
Barbour, R. S. (2005). Making sense of focus groups. Med. Educ. 39, 742–750. doi: 10.1111/j.1365-2929.2005.02200.x
Bauer, D., Lahner, F. M., Huwendiek, S., Schmitz, F. M., and Guttormsen, S. (2020). An overview of and approach to selecting appropriate patient representations in teaching and summative assessment in medical education. Swiss Med. Wkly. 150:w20382. doi: 10.4414/smw.2020.20382
Behardien, N., Brijlal, P., and Roman, N. V. (2023). Exodontia skills acquisition: Focusing on clinical teaching and training. PloS One 18:e0286737. doi: 10.1371/journal.pone.0286737
Berk, R. A. (2009). Multimedia teaching with video clips: TV, movies, YouTube, and mtvU in the college classroom. Int. J. Technol. Teach. Learn. 5, 1–21. doi: 10.1016/j.sbspro.2010.12.326
Brand, H. S., van der Cammen, C. C. J., Roorda, S. M. E., and Baart, J. A. (2015). Tooth extraction education at dental schools across Europe. BDJ Open 1:15002. doi: 10.1038/bdjopen.2015.2
Cantillon, P., and Sargeant, J. (2008). Giving feedback in clinical settings. BMJ 337, a1961–a1294. doi: 10.1136/bmj.a1961
Charlton, P., Magoulas, G., and Laurillard, D. (2012). Enabling creative learning design through semantic technologies. Technol. Pedagogy Educ. 21, 231–253.
Cooperrider, D. L., and Whitney, D. (2000). A positive revolution in change: appreciative inquiry. Handbook of organizational behavior, revised and expanded. Available online at: https://www.researchgate.net/publication/237404587
Coyne, E., Rands, H., Frommolt, V., Kain, V., Plugge, M., and Mitchell, M. (2018). Investigation of blended learning video resources to teach health students clinical skills: an integrative review. Nurse Educ. Today 63, 101–107. doi: 10.1016/j.nedt.2018.01.021
Dale, E. (1969). The cone of experience. Chapter 4 in Audiovisual methods in teaching, 3rd ed. Hinsdale, IL: The Dryden Press, 107–135.
DeBourgh, G. A., and Prion, S. K. (2017). Student-directed video validation of psychomotor skills performance: a strategy to facilitate deliberate practice, peer review, and team skill sets. Int. J. Nurs. Educ. Scholarship 14:20. doi: 10.1515/ijnes-2016-0020
Forbes, H., Oprescu, F. I., Downer, T., Phillips, N. M., McTier, L., Lord, B., et al. (2016). Use of videos to support teaching and learning of clinical skills in nursing education: a review. Nurse Educ. Today 42, 53–56. doi: 10.1016/j.nedt.2016.04.010
Gauthier, S., Cavalcanti, R., Goguen, J., and Sibbald, M. (2015). Deliberate practice as a framework for evaluating feedback in residency training. Med. Teach. 37, 551–557.
Hammond, S. A. (2013). The thin book of appreciative inquiry [Internet]. 3rd ed. Bend, ORE: Thin Book Publishing Company, 1–40. Available from: https://www.readpbn.com/pdf/The-Thin-Book-of-Appreciative-Inquiry-Sample-Pages.pdf
Health Professions Council of South Africa . (2014). Core Competencies for Undergraduate Students in the Clinical Associate, Dentistry and Medical Teaching and Learning Programmes in South Africa Developed by the Undergraduate Education and Training Subcommittee of the Medical and Dental Professi, Hpcsa, (February), pp. 1–14. Available online at: http://www.hpcsa.co.za/uploads/editor/UserFiles/downloads/medical_dental/MDBCoreCompetencies-ENGLISH-FINAL2014.pdf
Houghton, C. E., Casey, D., Shaw, D., and Murphy, K. (2013). Students’ experiences of implementing clinical skills in the real world of practice. J. Clin. Nurs. 22, 1961–1969. doi: 10.1111/jocn.12014
Kolb, A. Y., and Kolb, D. A. (2005). The Kolb learning style inventory — version 3.1 2005 technical specifications. Exp. Based Learn. Syst., 1–72.
Kosterelioglu, I. (2016). Student views on learning environments enriched by video clips. Univ. J. Educ. Res. 4, 359–369. doi: 10.13189/ujer.2016.040207
Leijon, M., Nordmo, I., Tieva, Å., and Troelsen, R. (2024). Formal learning spaces in higher education - a systematic review. Teach. High. Educ. 29, 1460–1481. doi: 10.1080/13562517.2022.2066469
Li, S., Su, L., Lou, R., Liu, Y., Zhang, H., Jiang, L., et al. (2024). Blended teaching mode based on small private online course and case-based learning in analgesia and sedation education in China: a comparison with an offline mode. BMC Med. Educ. 24:28. doi: 10.1186/s12909-023-04839-4
MacLuskey, M., and Durham, J. (2009). Oral surgery undergraduate teaching and experience in the United Kingdom: a national survey. Eur. J. Dent. Educ. 13, 52–57. doi: 10.1111/j.1600-0579.2008.00537.x
Macluskey, M., Durham, J., Cowan, G., Cowpe, J., Evans, A., Freeman, C., et al. (2008). UK national curriculum for undergraduate oral surgery subgroup for teaching of the association of British academic oral and maxillofacial surgeons. Eur. J. Dent. Educ. 12, 48–58. doi: 10.1111/j.1600-0579.2007.00467.x
Manogue, M., McLoughlin, J., Christersson, C., Delap, E., Lindh, C., Schoonheim-Klein, M., et al. (2011). Curriculum structure, content, learning and assessment in European undergraduate dental education – update 2010. Eur J Dent Educ 15, 133–141. doi: 10.1111/j.1600-0579.2011.00699.x
Morris, C. (2012). “Reimagining ‘The Firm’,” in Workbased learning in clinical settings. eds. V. Cook, C. Daly, and M. Newman (London: Radcliffe), 1–25.
O’Doherty, D., Dromey, M., Lougheed, J., Hannigan, A., Last, J., and McGrath, D. (2018). Barriers and solutions to online learning in medical education – an integrative review. BMC Med. Educ. 18:130. doi: 10.1186/s12909-018-1240-0
Omar, E. (2017). Perceptions of teaching methods for preclinical Oral surgery: a comparison with learning styles. Open Dent. J. 11, 109–119. doi: 10.2174/1874210601711010109
Priest, K. L., Kaufman, E. K., Brunton, K., and Seibel, M. (2013). Appreciative inquiry: A tool for organizational, programmatic, and project-focused change. J. Leadersh. Educ. 12, 18–33.
Punzalan, C. H., and Roberto, L. R. (2023). Online biochemistry distance learning: dentistry students’ perceived opportunities and challenges. Turk. Online J. Dist. Educ. 24, 280–292. doi: 10.17718/tojde.1126780
Raina, K., Poojary, D., Shetty, P., Khalid, I., Rashmi, K. S., and Chandana, R. D. K. (2021). Simulation based training in dental education-a review. Multicult. Educ. 7, 238–43.
Ralph, V. R., Scharlott, L. J., Schwarz, C. E., Becker, N. M., and Stowe, R. L. (2022). Beyond instructional practices: characterizing learning environments that support students in explaining chemical phenomena. J. Res. Sci. Teach. 59, 841–875. doi: 10.1002/tea.21746
Saladino, V., Auriemma, V., and Campinoti, V. (2022). Healthcare professionals, post-traumatic stress disorder, and COVID-19: A review of the literature. Front. Psychol. 12, 1–9. doi: 10.3389/fpsyt.2021.795221
Shin, H., Sok, S., Hyun, K. S., and Kim, M. J. (2015). Competency and an active learning program in undergraduate nursing education. J. Adv. Nurs. 71, 591–598.
Shoaib, L. A., Safii, S. H., Naimie, Z., Ahmad, N. A., Sukumaran, P., and Yunus, R. M. (2018). Dental students’ perceptions on the contribution and impact role of a clinical teacher. Eur. J. Dent. Educ. 22, e26–e34. doi: 10.1111/eje.12252
Sivarajah, R. T., Curci, N. E., Johnson, E. M., Lam, D. L., Lee, J. T., and Richardson, M. L. (2019). A review of innovative teaching methods. Acad. Radiol. 26, 101–113. doi: 10.1016/J.ACRA.2018.03.025
Skene, A., Paziuk, G., and Hamilton, B. (n.d.). Effective practices in course redesign. Available at: https://www.uwindsor.ca/ctl/sites/uwindsor.ca.ctl/files/effective_practices_in_course_redesign.pdf
Stather, D. R., MacEachern, P., Chee, A., Dumoulin, E., and Tremblay, A. (2013). Trainee impact on procedural complications: an analysis of 967 consecutive flexible bronchoscopy procedures in an interventional pulmonology practice. Respiration 85, 422–428. doi: 10.1159/000346650
Stelzle, F., Farhoumand, D., Neukam, F. W., and Nkenke, E. (2011). Implementation and validation of an extraction course using mannequin models for undergraduate dental students. Acta. Odontologica. Scandinavica. 69, 80–87. doi: 10.3109/00016357.2010.517560
Timothy, P. G., Jeffrey, B., Kaitlyn, L., and Margarita, V. D. V. (2016). Delivery of educational content via Instagram®. Med. Educ. 50, 575–576. doi: 10.1111/medu.13009
Torrentira, M. C. (2020). Online data collection as adaptation in conducting quantitative and qualitative research during the Covid-19 pandemic. European J. Educ. Stud. 7, 78–87. doi: 10.46827/ejes.v7i11.3336
van de Ridder, J. M. M., Stokking, K. M., McGaghie, W. C., and ten Cate, O. T. J. (2008). What is feedback in clinical education? Med. Educ. 42, 189–197. doi: 10.1111/j.1365-2923.2007.02973.x
Watkins, K. E., Marsick, V. J., and Wasserman, I. (2019). Action research, action learning, and appreciative inquiry. 76–92. doi: 10.4018/978-1-5225-6155-2.ch004
Zou, L., King, A., Soman, S., Lischuk, A., Schneider, B., Walor, D., et al. (2011). Medical students’ preferences in radiology education. A comparison between the socratic and didactic methods utilizing PowerPoint features in radiology education. Acad. Radiol. 18, 253–256. doi: 10.1016/j.acra.2010.09.005
Keywords: exodontia, curriculum evaluation, didactic, preclinical, teaching and learning strategies, blended-learning
Citation: Behardien N, Titus S and Roman NV (2024) Exodontia curriculum evaluation: fit for purpose teaching and learning strategies. Front. Educ. 9:1398699. doi: 10.3389/feduc.2024.1398699
Edited by:
Rhythm Bains, King George’s Medical University, IndiaReviewed by:
Ransome Vanzil Van Der Hoeven, The University of Iowa, United StatesShalini Aggarwal, Dr. D. Y. Patil Vidyapeeth, India
Mai Khalaf, Kuwait University, Kuwait
Shyam Sundar Sarkar, Islamic University, Bangladesh
Copyright © 2024 Behardien, Titus and Roman. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nashreen Behardien, bmJlaGFyZGllbkB1d2MuYWMuemE=
†ORCID: Nashreen Behardien, https://orcid.org/0000-0003-2881-7891
Simone Titus, https://orcid.org/0000-0003-3599-8918
Nicolette V. Roman, https://orcid.org/0000-0002-4506-437X