 Kristel De Groot
Kristel De Groot Sander M. Wieman
Sander M. Wieman Jan W. Van Strien1
Jan W. Van Strien1 Oliver Lindemann
Oliver Lindemann- 1Department of Psychology, Education & Child Studies, Erasmus School of Social and Behavioural Sciences (ESSB), Erasmus University Rotterdam, Rotterdam, Netherlands
- 2Department of Applied Economics, Erasmus School of Economics (ESE), Erasmus University Rotterdam, Rotterdam, Netherlands
- 3Department of Economics and Business, Erasmus University College (EUC), Erasmus University Rotterdam, Rotterdam, Netherlands
Research has demonstrated high rates of mental health problems in university students, and even higher rates in students belonging to historically marginalised populations. However, research on disparities in student mental health has almost exclusively focused on internalising problems (like symptoms of depression and anxiety), overlooking other ways in which individuals experience and express negative emotion. To address this limitation, the present study employed the Brief Problem Monitor to examine three types of mental health problems—internalising, externalising, and attentional problems—across six sociodemographic characteristics: gender (male vs. female), sexual orientation (heterosexual vs. non-heterosexual), ethnicity (Dutch without vs. with migration background), internationality (domestic vs. international), disability (no disabilities vs. disabilities), and parental education (continuing- vs. first-generation). These sociodemographic variables were included in regression models simultaneously, thereby controlling for the effects of the others. Across a sample of 2,256 students, internalising problems were significantly higher in students who were female, non-heterosexual, international, and in those with disabilities. Higher externalising problems were found in female students, students with disabilities, those with a migration background, and first-generation students. Finally, attentional problems were higher in non-heterosexual students and students with disabilities. These findings support the premise that different groups of students experience different types of mental health concerns, emphasising the importance of measuring mental health multidimensionally. As an example, had the present study only examined internalising problems, we would not have found mental health disparities for students with a migration background and first-generation students, which has clear implications for outreach and resources offered to them.
1 Introduction
Despite university students generally being considered a socially advantaged and privileged population, research indicates that many of them meet the diagnostic criteria for a mental health disorder or experience non-clinical but nonetheless high psychological distress. For example, using data from the Healthy Minds Study, Lipson et al. (2016) found that about one in three American undergraduates and one in four graduate students met the criteria for at least one mental health problem. A similarly high prevalence was reported in a nationwide Canadian study, detailing that one in three undergraduate students experienced elevated psychological distress (Adlaf et al., 2001). Likewise, European data from students in Belgium showed that one-third of undergraduates reported to have had mental health problems in the past year (Bruffaerts et al., 2018). The consequences of experiencing such problems are significant to students, with research for example demonstrating a negative impact on day-to-day functioning (Stallman, 2010), academic performance (Bruffaerts et al., 2018; Stallman, 2010), and ability to complete a degree (Breslau et al., 2008).
The high rates of mental health problems in students can in part be explained by psychosocial changes and stressors that are inherent to student life and that negatively impact wellbeing. Compared to their peers who do not attend university, students are more likely to move away from home, resulting in a loss of their familiar surroundings and usual support network, and requiring them to adapt to a new environment and form new relationships (Farrer et al., 2016; Hurst et al., 2013; Reisbig et al., 2012). In addition to these transitional stressors, students face obvious academic ones, including a heavy workload, pressure from deadlines and examinations, and a resulting lack of respite (Linden et al., 2022; Reisbig et al., 2012; Skead and Rogers, 2014). Moreover, they bear high expectations, not only from others, but from themselves as well (Hurst et al., 2013; Linden et al., 2022). Being surrounded by peers whose intellect rivals students' own abilities, they are prone to setting unreasonably high standards and feeling pressure to succeed (Farrer et al., 2016; Hamaideh, 2011; Skead and Rogers, 2014). Finally, many students are subject to financial stressors, as they often live on a limited budget, worry about debt, and balance their studies with work to cover the costs of housing and tuition (Bøe et al., 2021; Linden et al., 2022; Richardson et al., 2017; Stallman, 2010).
However, the prevalence of mental health issues, as well as their causes, are not the same among all students. Research has demonstrated that several—mostly historically marginalised—sociodemographic groups within the student body face specific additional challenges, and as a result are more likely than others to experience mental health concerns. A first disparity in this regard is that based on gender, with female students more often than males reporting a “chilly” campus climate (Hall and Sandler, 1982; Kim and Kim, 2023; Lee and McCabe, 2021) in which they experience microaggressions (subtle exchanges that convey a disparaging attitude; Pierce, 1974; Sue, 2010), like being passed over and interrupted in class conversations; and in addition more overt sexist behaviours, such as jokes involving traditional gender role stereotypes, derogatory remarks about women, and sexual objectification. These experiences have been related to increased feelings of depression and anxiety (Klonoff et al., 2000), and decreased self-esteem (Swim et al., 2001). Furthermore, female students have been shown to be at higher risk than male students of sexual harassment (within and outside educational settings; Klein and Martin, 2021; Parr, 2020), and to worry more about their safety (Etopio et al., 2019; Grinshteyn et al., 2022), both of which again negatively relate to mental health. In line with these findings, a large body of research has found that female students report more mental health problems than male students (e.g., Ibrahim et al., 2013; Steptoe et al., 2007; but see Akhtar et al., 2020), except for some specific concerns, such as conduct problems and alcohol and substance abuse, which seem to be more prevalent in men (Chien et al., 2011; Richardson et al., 2017; Said et al., 2013).
A second mental health disparity that has been studied extensively is that based on gender identity and sexual identity. Consistent with models which postulate that LGBTQ persons have elevated rates of mental health problems because of stressors in their social environment (Meyer, 2003), research on LGBTQ students has highlighted the impact of an unsupportive or unsafe campus climate. Specifically, LGBTQ students are more likely to be deliberately excluded (Rankin et al., 2010); to be targets of offensive remarks or jokes about their sexuality (Alessi et al., 2017); to be verbally threatened (Marx et al., 2022); and to experience sexual harassment (Klein and Martin, 2021), each of which has been shown to negatively impact their mental health (Silverschanz et al., 2008; Woodford et al., 2015). Furthermore, as a result of these experiences, they have been shown to feel less safe at university (Grinshteyn et al., 2022; Marx et al., 2022), and to be cautious about disclosing their gender identity or sexual identity, fostering feelings of isolation and additional distress (Alessi et al., 2017; Leleux-Labarge et al., 2015; Rankin, 2003). These resulting mental health disparities have been corroborated by various large-scale studies, showing that transgender and gender-non-conforming students are more likely to report poor mental health than cisgender students; and that gay, lesbian, bisexual, pansexual, demisexual, asexual, questioning, queer, and unsure students are more likely to do so compared to their heterosexual peers (e.g., Borgogna et al., 2019; Kelders et al., 2019; Liu et al., 2019).
A third mental health disparity that has received considerable attention concerns race and ethnicity. In particular, students of colour in North-American and European universities have been shown to confront various stressors that their White peers do not face and that negatively impact their mental health. One such stressor is racial discrimination, often taking the form of microaggressions, like being treated as lesser (Sue et al., 2007) and being stared at with suspicion as if they do not belong (Swim et al., 2003). More overt racism, like racial slurs, is also reported. Additionally, students of colour have been shown to experience acculturative conflict, being fearful of exhibiting behaviour that may confirm biases about their ethnic group (i.e., stereotype threat), whilst feeling pressure from those within this group to conform to the group's expectations (Ojeda et al., 2012). Together, these ethnicity-related stressors can instil a sense of self-doubt and frustration (Solórzano et al., 2000), and have been shown to negatively impact students' psychological wellbeing beyond the effects attributable to generic student stress (Smedley et al., 1993; Wei et al., 2010). In line with this, various studies have reported poorer mental health in students belonging to ethnic minorities relative to their peers (Eisenberg et al., 2013; Nerdrum et al., 2006; Weitzman, 2004), although some studies have found little to no differences (Eisenberg et al., 2007; Said et al., 2013), possibly due to underreporting related to high stigma and low help-seeking in ethnic minority students (Lipson et al., 2018).
A fourth disparity in mental health is that between domestic students and a group that has been growing steadily: international students (UNESCO Institute for Statistics, 2022). Leaving their home country for an unfamiliar environment, they face more transitional stressors than their domestic peers, like having to adjust to a different culture and educational practices, and are vulnerable to loneliness (Forbes-Mewett and Sawyer, 2016; Mori, 2000). Language barriers may exacerbate this, hindering students in comfortably socialising with others (Smith and Khawaja, 2011). Furthermore, international students are at risk of discrimination based on ethnicity, much like domestic students of colour, worsening feelings of homesickness, and alienation (Poyrazli and Lopez, 2007). However, despite these stressors having a negative impact on international students' mental health (Jung et al., 2007; Shadowen et al., 2019), most research comparing international and domestic students has found no evidence to suggest their mental health differs (Eisenberg et al., 2007; Leahy et al., 2010; Liu et al., 2019; Stallman, 2010), or has in fact found that international students do better than their domestic peers (Farrer et al., 2016; Said et al., 2013). However, the geographical scope of this research is limited, as the vast majority of studies on international students' mental health are Australia- or USA-based. Thus, their findings do not automatically translate to international students in other host countries that have, for instance, a different culture and educational system. As an example, in a recent large-scale Dutch study, international students scored significantly worse than Dutch students on a variety of distress-related variables, including depression, anxiety, stress, and burnout (Kelders et al., 2019).
A fifth disparity in student mental health deals with the difference between students with and without disabilities. Despite legislation aimed at making tertiary education accessible to those with physical, sensory, learning, and psychological conditions, barriers in accessibility persist, and can form a challenge for these students (García-González et al., 2021). Potential practical obstacles include poor accessibility of buildings and learning materials (Borland and James, 1999; Fuller et al., 2004); financial strain from disability-related expenses combined with limited opportunities to work (Fox et al., 2022; Wolanin and Steele, 2004); and problems with arranging accommodations, including bureaucratic processes that place a high burden on students (Goode, 2007; Hong, 2015; Toutain, 2019). Socially, students with disabilities have been shown to suffer more from loneliness, have a lesser sense of belonging (Kelders et al., 2019; McLeod et al., 2019), and to face stigma, fearing that disclosing their disability or using accommodations changes how others view and treat them (Hong, 2015; Kimball et al., 2016; Toutain, 2019). In relation to these stressors, students with disabilities have been shown to report more mental health issues than others, including higher feelings of depression and anxiety and decreased wellbeing (Coduti et al., 2016; Kelders et al., 2019; McLeod et al., 2019; Richardson et al., 2017). This is mirrored in research on specific disabilities, with for example deaf and hard-of-hearing students reporting more suicidal ideation than hearing students do (Fox et al., 2020), and students on the autism spectrum having more mental health difficulties than their neurotypical peers (Kuder et al., 2021). On the other hand, students with disabilities have been shown to score similar to students without disabilities on anger-related problems (Coduti et al., 2016; Fleming et al., 2018), and in fact score better on substance abuse (Coduti et al., 2016; Richardson et al., 2017).
A sixth mental health disparity that is examined in student populations is that based on socioeconomic position, often operationalised as one's education, income, or occupation, or in the case of students, that of their parent(s). Using these proxies, research has shown that students who are first-generation or come from low-income or working-class backgrounds (so-called FLoW students) are more likely than others to face challenges from lack of resources, having to navigate university with limited economic, cultural, and social capital. The main economic barrier they face are the costs of education, with FLoW students being more likely to incur large debts and work alongside their studies (House et al., 2020; Soria et al., 2014), and as a result, participate less in social and recreational activities (Martin, 2012). Regarding cultural capital, they experience more difficulty fitting in due to having different values, and are more likely to question their legitimacy as a student (Lippincott and German, 2007). In addition, they experience difficulties navigating the academic system, reporting feeling underprepared and overwhelmed (Bui, 2002; Hsiao, 1992). As for social capital, FloW students' networks often have no experience with higher education and are therefore less able to provide support. In fact, their networks can foster conflict when students take on the “habitus” of university culture, (unintentionally) distancing themselves from their background (Hsiao, 1992; London, 1989). In line with these added stressors, research has shown that lower socioeconomic position in students is associated with poorer mental health, both when examining family income (Eisenberg et al., 2007; Ibrahim et al., 2013; Said et al., 2013; Steptoe et al., 2007) and parental education (Stebleton et al., 2014; Steptoe et al., 2007; Weitzman, 2004), although for the latter some studies have not found an effect (House et al., 2020; Said et al., 2013).
Summarising the available literature on mental health disparities in higher education students, we observe persistent inequalities, with students belonging to historically marginalised populations scoring worse than their peers. However, conclusions drawn from this body of research are limited for two reasons. Primarily, research on student mental health has exclusively focused on internalising problems, such as symptoms of depression and anxiety, overlooking other ways in which individuals might experience and express negative emotion, like directing feelings outwards (i.e., externalising), characterised by undercontrolled, impulsive, or aggressive behaviour. Most inventories available, likewise, exclusively measure internalising symptoms, with for example the short versions of the Depression Anxiety Stress Scale (Lovibond and Lovibond, 1995) and the General Health Questionnaire (Goldberg, 1972; Goldberg and Williams, 1988) being frequently used for measuring students' mental health. The resulting narrow view on mental health problems—particularly regarding students—has been criticised by others, with Bruffaerts et al. (2018) noting that despite externalising problems being present in roughly 20% of students, research is limited to Attention Deficit Hyperactivity Disorder (ADHD) and high-risk financial and health behaviours. With regard to mental health disparities specifically, we argue that the exclusive focus on internalising problems can lead to erroneous conclusions as one may wrongly conclude that certain groups have few psychological problems, while in fact they experience high but non-internalising distress. This could for example be the case for disparities based on gender, as it has been proposed that women tend to internalise mental health problems, whilst men externalise them, which illustrates the importance of measuring mental health in a differentiated and multidimensional way (Dohrenwend and Dohrenwend, 1976).
A second, related limitation of existing research is that most studies have a clinical rather than an epidemiological focus, trying to pinpoint the—internalising—disorders that students might have. This carries the risk of pathologising students, who may have clinical levels of psychological morbidity, but do not inherently represent a clinical group. Also, the inventories used in these studies have often been “designed and validated using clinical populations and may therefore not reflect or be generalisable to the mental health experiences of university students” (Sheldon et al., 2021, p. 289). As for mental health disparities, the use of clinical instruments can again amount to erroneous conclusions, as certain groups of students may be more reluctant than others to disclose mental health problems when these are framed diagnostically, for example because of (cultural) stigma attached to mental health diagnosis (Lipson et al., 2018).
The present study seeks to overcome these constraints by examining the six disparities earlier discussed with the use of an inventory that encompasses a range of mental health problems and is appropriate for use in clinical and non-clinical populations, including young and generally healthy ones, such as students: the Brief Problem Monitor (BPM; Achenbach and Ivanova, 2018). This short inventory assesses emotional and behavioural functioning across three dimensions—internalising, externalising, and attentional functioning—allowing researchers to not only examine group differences in overall mental health, but between different types of mental health problems too.1 Based on the reviewed literature, we hypothesise that students who belong to historically marginalised populations score higher (i.e., worse) on the internalising problems subscale, and on the full BPM. Specifically, in our sample of students attending a Dutch university, we expect worse internalising and overall mental health in (1) female compared to male students; (2) students who do not identity as heterosexual compared to heterosexual students; (3) students of colour compared to White students; (4) international compared to domestic students; (5) students with disabilities compared to students without; and (6) students from lower compared to higher socioeconomic backgrounds. As for externalising problems, we hypothesise that male students report more problems than female students, and that students with disabilities report fewer problems than those without, in both cases based on the available literature on conduct/anger problems and substance abuse. No other hypotheses are formed for the externalising problems subscale, and none at all for attentional problems, given the lack of research on sociodemographic disparities therein.
2 Material and methods
2.1 Participants
The data were collected as part of a larger, longitudinal survey study at Erasmus University Rotterdam on individual differences in student wellbeing for which students were invited to participate if they were 16 years or older; had just started their programme in the fall of 2018; and had not been registered as a student at this university before. In total, N = 7,693 students met these inclusion criteria and were invited. The link to the survey was opened 3,024 times, of which 2,876 times at least one question was answered, and 2,320 times the survey was fully completed. This corresponds to a response rate of (2,320/7,693) * 100 = 30.2%, and a completion rate of (2,320/2,876) *100 = 80.7%.2 After data collection, n = 38 duplicate entries were identified based on student ID and were subsequently removed.
For the present study, we selected all respondents who had completed the Brief Problem Monitor (BPM), and who had provided data on at least one demographic from the hypotheses (i.e., gender, sexual orientation, ethnic background, internationality, disability, or socioeconomic position). This resulted in a sample of n = 2,366. Six participants were excluded due to careless responding, which was determined by examining participants' responses on two consecutive inventories included in the survey: the Autism spectrum Quotient (AQ; Baron-Cohen et al., 2001), which is outside the scope of the present study, and the BPM. Participants were excluded when showing a careless answering pattern on both of these measures, which could either be a high-frequency or a repetitive pattern (for an overview of patterns, see Supplementary material A). In addition, mature students (30 years or above, proxied as those born in 1988 or before) were excluded (n = 104, including one student who did not report their year of birth), as we assumed that they would be in a different stage of their lives.
The final analysis sample consisted of n = 2,256 students, born between 1989 and 2001, with a mean year of birth of 1,997.9 (SD = 2.7), corresponding to a mean age of approximately 20 years. All but 47 students reported their level of study and the faculty they were affiliated with. The majority were new bachelor students (n = 1,697, 76.8%), the others being either new master students (n = 417, 18.9%) or students in a pre-master programme (n = 93, 4.2%). A small percentage (0.1%) reported studying at yet a different level. Students from all faculties were represented: 23.8% reported being affiliated with the management faculty, 18.6% with social sciences, 17.9% economics, 11.6% law, 9.6% humanities, 7.4% medicine, 3.1% health sciences, 1.9% international social studies, and 0.5% philosophy. In addition, 5.7% reported studying at more than one faculty. These numbers were in line with the distribution across the full student body of the university. The study was executed in accordance with the Helsinki declaration, and received ethics approval from the Erasmus Research Institute of Management review board (case number IRB-NE-2017-12). All participants completed an informed consent form approved by the university's Research Data Management team.
2.2 Procedure
The presently used data were gathered as part of the entry survey of a longitudinal project.3 An invitation to participate in this entry survey was sent to eligible students' university email addresses a little over 2 weeks after the start of the academic year (September 2018). In addition, posters advertising the survey were distributed around one of the university's campuses. The survey was also advertised via social media pages of various faculties, via email lists of several others, and through outreach by study associations. Dedicated social media pages for the project were created as well, where the survey was also advertised. Approximately 2 weeks after the initial invitation, a reminder was sent to those students who had not yet responded. A second reminder email was sent circa 3 weeks later, a day before the survey closed. To encourage participation among a broader range of students than those with an intrinsic interest in or concern for wellbeing, students were informed in all communication that every 50th person who finished the survey would receive 50 euros.
Students entered the survey via a hyperlink included in the recruitment and reminder emails that led to a Qualtrics webpage. Here, they were presented with a description of the study, an overview of their rights as participants, and contact details of the lead researcher. Importantly, they were informed that any personal data they provided (like an email address) would be removed and stored separately from the main data. After checking the “I hereby provide my consent” box, students continued to the main part of the survey, where they reported sociodemographic information; filled out two inventories (AQ and BPM); and answered questions about their studies and their social life. The survey was offered in English and Dutch. Students could leave the survey at any point and re-enter later to finish. Most questions were multiple-choice. Given the sensitive nature of some of the questions, these either provided an option “I would rather not say” or could be skipped. At the end of the survey, participants could enter the raffle for the 50 euro reward. The median time spent on the survey was 15.3 minutes, and 15.4 minutes among students who fully completed it. Mean duration was unrepresentative due to some respondents leaving opened surveys unattended for longer periods of time.
2.3 Measures
2.3.1 Socio-demographic information
2.3.1.1 Gender
Participants were asked to select their gender, choosing from three options: “Male”, “Female”, and “Other”, or they could select “I would rather not say”. As we anticipated that the number of transgender and gender-non-conforming students would be too low for use in statistical comparisons, it was decided to not include separate questions on assigned sex and gender identity. For the presently proposed analyses, the “Other” option was disregarded, leaving men and women to be compared.
2.3.1.2 Sexual orientation
Participants were asked to indicate their sexual orientation by selecting one of five options: “Heterosexual”, “Homosexual”, “Bisexual”, “Asexual”, and “Other”, or they could select “I would rather not say”. Because of constraints in sample size, students who selected “Homosexual”, “Bisexual”, “Asexual”, and “Other” were grouped together as “Non-heterosexual”, so that their mental health as a group could be compared to that of heterosexual students.
2.3.1.3 Ethnic background and internationality
Participants' ethnic background and internationality were examined with a question in which students were asked about their “background” and could choose from nine options: “Dutch background”, “Dutch with a migration background”, “International student from an African country”, “… from an Asian country”, “… from a European country”, “… from a North-American country”, “… from a South-American country”, “… from an Oceanian country”, and “Other”.4 Again, the option “I would rather not say” was also available. In the present study, “Other” was disregarded, and the remaining responses were collapsed into three categories: “Dutch”, “Dutch with a migration background”, and “International student”.
2.3.1.4 Disability
Participants could indicate whether they had a disability by selecting those disabilities that applied to them from a list of 53 alphabetically presented options compiled by the first author. In addition, they could enter up to three disabilities that were not on this list. The 53 fixed answer options included disabilities that are thought to be (relatively) common among university students, such as anxiety disorders, asthma, and dyslexia, as well as disabilities that are less common in this group, like diabetes, schizophrenia, and visual impairments. Participants without a disability and those who did not want to disclose any information on this topic could skip the question and continue to the next one. Participants who did report one or more disabilities received additional questions for each disability they reported, including whether or not they had officially been diagnosed. For the present study, students who reported one or more disabilities—regardless of type or diagnosis—were grouped together as “Students with disabilities”. Those who did not report a disability were labelled “Students without disabilities”.
2.3.1.5 Socioeconomic position
Participants' socioeconomic position (SEP) was operationalised as parental education, which was preferred over parental income and parental occupation (other common proxies) for two reasons. First, it is the proxy which best informs the research question, since parents who have themselves experienced higher education can support their children with practical knowledge, cultural capital, an understanding of what student life entails, and in many cases also financial support, as education is a strong determinant of income (Oakes and Andrade, 2017). High income or a high-status occupation, on the other hand, predominantly translate into financial support, but do not guarantee practical or emotional assistance. Second, parental education is the easiest of these proxies to measure in our sample, as students are likely to be familiar with this information and willing to disclose it (as opposed to parental income), and since level of education is easier to compare between different societies than income and occupational status, which is particularly relevant given that the sample includes international students. For these reasons, participants were asked to report the highest level of education attended or completed by their parent(s) and/or caregivers(s). For a maximum of four persons, students could select one of six options: “No formal education”, “Primary school”, “Secondary school”, “Vocational education”, “University of applied sciences/polytechnic”, or “Research university”, or they could select “Other/I don't know”. When none of their parents/caregivers had attended or completed a bachelor's programme or higher (i.e., a university of applied sciences or research university programme), students were coded as “first-generation”. Students who reported at least one parent or caregiver who attended or completed a bachelor's programme or higher, were coded as “continuing-generation”. Students who did not provide information on their parents/caregivers or who selected “Other/I don't know” were excluded from analyses involving socioeconomic position.
2.3.2 Brief problem monitor for ages 18–59
Mental health was assessed with the Brief Problem Monitor for ages 18–59 (Achenbach and Ivanova, 2018), a questionnaire consisting of 18 concise statements about how one might feel and act. For each item, participants were asked to indicate how well that item described them over the past week, answering on a 3-point scale with options “0 = not true”, “1 = somewhat true”, and “2 = very true”, resulting in a total score between 0 and 36. The BPM includes three subscales: internalising (INT) problems (e.g., “I lack self-confidence”), externalising (EXT) problems (e.g., “I have a hot temper”), and attentional (ATT) problems (e.g., “I have trouble setting priorities”), each consisting of six items, with a score ranging from 0 to 12. The items that make up the BPM were drawn from the larger Adult Self-Report (ASR) and the Adult Behaviour Checklist (ABCL; Achenbach and Rescorla, 2003) and were selected for loading strongly on their respective subscales, and for discriminating well between people who used mental health services and those who did not (Achenbach and Ivanova, 2018). Good (test-retest) reliabilities were observed for these items (all r's ≥ 0.79; and all α's ≥ 0.75). Further support for the BPM's psychometric properties was offered by De Vries et al. (2020), who found somewhat lower but still acceptable reliabilities (α = 0.79 for the INT subscale; α = 0.63 for EXT; α = 0.71 for ATT; and α = 0.86 for the total scale). The psychometric properties of the BPM for the current sample are examined in the results section. One reason for examining these in more detail is that the BPM is still a rather novel inventory that has not been used and validated often. Second, at the time when the present study was conducted, a formal Dutch translation of the BPM had not been made available yet, resulting in the use of a bespoke translation created using parallel translation and team-based review. Since this bespoke translation, which was used by the majority of the sample (i.e., Dutch-speaking participants), differed slightly from the formal translation that was released later, we thought it important to verify that the psychometric properties of the present data match those from previous studies. Importantly, and in line with our aim to move away from a clinical focus on student mental health, the BPM does not diagnose individuals. It measures emotional and behavioural functioning across three subscales, indicating the level of problems a student is experiencing in each domain.
2.4 Analyses
First, the psychometric properties of the BPM were examined. Specifically, we explored the distribution of the scores; estimated the reliability of the full scale and subscales; and performed an exploratory factor analysis using Principal Axis Factoring, extracting three fixed factors with oblique rotation, as the underlying factors (internalising, externalising, and attentional problems) are expected to correlate. These analyses were repeated using only data from participants who filled out the Dutch BPM to examine whether the psychometric properties of the data resulting from this bespoke translation were similar to those of the full dataset and those found in previous studies.
Second, the BPM total score and subscale scores of the present sample were benchmarked against age-, gender-, and society-specific normative data (Achenbach, 2022). Since previous work has reported that students are at higher risk of experiencing mental health problems than the general population (e.g., Adlaf et al., 2001; Leahy et al., 2010; but see Van der Velden et al., 2019), information on how our student sample scores relative to that population is relevant when interpreting differences that may exist within the student body.
Third, for the main analyses, i.e., comparing the mental health of historically marginalised students to that of their peers, two sets of multiple regression analyses were conducted. A first multiple regression was used to predict the BPM total score, entering all six disparities that were reviewed in the introduction as independent variables: gender, sexual orientation, ethnic background, internationality, disability, and SEP. Since ethnic background and internationality were measured within one question, these were included in the regression by creating two planned contrast variables: one comparing the mental health of Dutch students without a migration background to that of Dutch students with a migration background, and another comparing the mental health of all Dutch students to that of international students (reverse Helmert contrast). The six predictor variables were included in the model concurrently, thereby controlling for the effects of the other sociodemographic variables. Missing values were deleted pairwise. A secondary set of analyses comprising three multiple regressions examined possible mental health differences between students on the BPM subscales (i.e., internalising, externalising, and attentional problems), again by including the six disparities as predictors. Here, the critical p value was set at p = 0.017 to reduce the chance of Type I error (i.e., Bonferroni correction).
Fourth, the data were evaluated for non-response bias, which can occur when persons who do not respond to the survey (non-respondents) differ from those who do respond on variables of interest. This is particularly relevant when examining sensitive topics, like mental health problems, as some persons (e.g., those with serious problems) might be less inclined to take part than others. Since no data were available on the full eligible sample or on non-respondents as a group, possible non-response bias was examined using the Continuum of Resistance Model, which posits that the willingness of individuals to participate can be inferred from the effort that is required to elicit their participation (Bose, 2001; Kypri et al., 2011; Said et al., 2013). From this it follows that late respondents—persons who only participate after considerable effort has been exerted to include them, and who likely would have been non-respondents if the data collection or the efforts of the researcher to include them had ceased earlier—can be used as a proxy for non-respondents. Students were sent reminder emails exactly 16 and 39 days after the initial invitation. For the purpose of studying non-response bias, we assigned students to one of three groups: those who started filling out the survey before the first reminder email were considered “early”; those who started after the first but before the second reminder were considered “late”; and those who started after the second reminder email were considered “very late”. The differences in BPM scores between individuals at each of the three levels of response speed (early, late, and very late) were then examined with one-way ANOVAs. In addition, using chi-square tests, the associations between response speed and the independent variables (gender, sexual orientation, ethnic background, internationality, disability, and socioeconomic position) were examined for those independent variables that were not distributed in line with what we would expect based on previous research or population data.
3 Results
3.1 Psychometric properties of the BPM
The BPM total score ranged from 0 to 34 (two below the maximum), with a mean of M = 8.83 (SD = 6.21). The subscale scores all ranged from 0 to the full 12, with mean scores of M = 2.51 (SD = 2.72) for internalising problems, M = 2.74 (SD = 2.32) for externalising problems, and M = 3.59 (SD = 2.64) for attentional problems. The total score and subscale scores showed a right-skewed distribution, with many students scoring on the low end of the inventory: skewness was 0.89 for the full BPM, 1.22 for the internalising subscale, 0.97 for the externalising subscale, and 0.70 for the attentional subscale (SE = 0.05). Kurtosis was 0.43, 0.94, 0.60, and <0.01 respectively (SE = 0.10), indicating that for all but the attentional subscale the distribution was somewhat heavy-tailed.
Cronbach's alpha was α = 0.86 across all items. The reliability per subscale is shown in Table 1. The results of the exploratory factor analysis are also presented there. Three fixed factors were extracted using Principal Axis Factoring with oblique rotation (δ = 0). The suitability of the analysis was shown by a high Kaiser-Meyer-Olkin value (KMO = 0.90, individual values all >0.82) and a significant result on Bartlett's test of sphericity [ = 11,215.55, p < 0.001]. The three extracted factors explained a total of 37.33% of the variance. The factor pattern matrix showed that all items but one clustered in accordance with the BPM's intended structure: items 2, 4, 5, 10, 15, and 16 loaded strongest on the first factor, together making up the internalising problems subscale; items 1, 6, 7, 8, 9, and 12 loaded strongest on a second factor, comprising the attentional problems subscale; and items 3, 11, 13, 14, and 18 loaded strongest on a third factor, corresponding to the externalising problems subscale. Item 17, “I get upset too easily”, was the only item for which the factor loading did not correspond to the BPM's intended structure, as it loaded stronger on the first (internalising) than the third (externalising) factor. Repeating these analyses using only data from participants who filled out the bespoke, Dutch translation of the BPM (n = 1,456) resulted in similar findings, which are reported in Supplementary material B. The most notable discrepancy was that in the Dutch data items 3 (“I am impulsive or act without thinking”) and 12 (“I have trouble making decisions”), whose loadings were relatively low to begin with, loaded strongest on a different factor than expected (while they loaded correctly in the full sample).
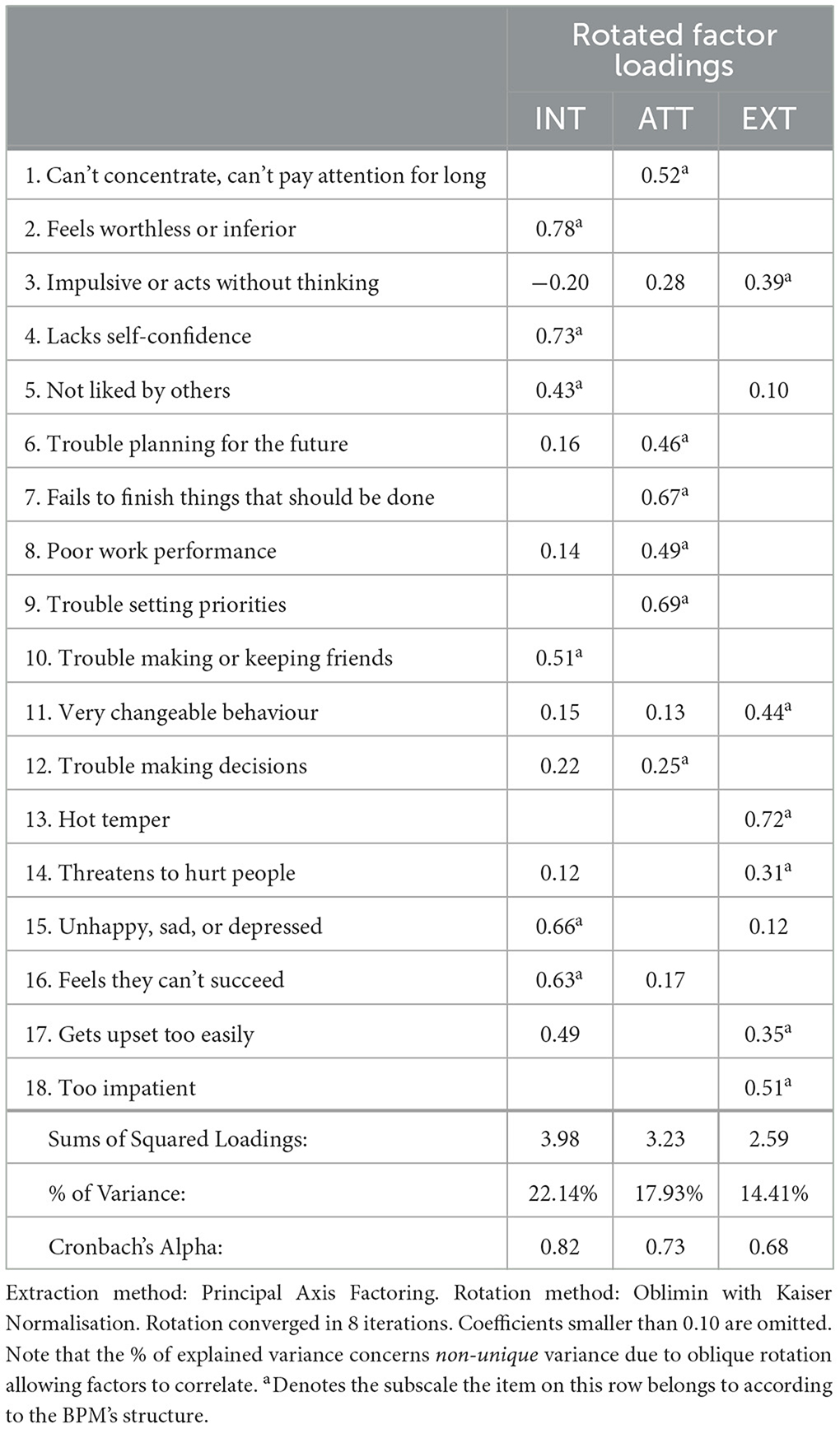
Table 1. Factor pattern loadings, explained variance, and reliability for the BPM subscales.
3.2 Comparison with normative data
Norm data were obtained from the BPM scoring software (version 4.0.280, Achenbach, 2022), which employs T-scores that range from 50 (50th percentile) to 75 (99.4th percentile) for the subscales, and from 50 to 80 (99.9th percentile) for the full scale.5 T-scores ≥ 65 (matching the 93rd percentile in the norm sample) are considered “sufficiently elevated to be of concern” (Achenbach and Ivanova, 2018). Since students aged 30 and older were excluded from the analyses, norm data for ages 18–35 was used. Norms for three “societies” were available: those with low, intermediate (default, represented by US norms), or high problem scores. Since the Netherlands has not been assigned to such a category for the BPM/18–59 yet, and as approximately one-third of the sample consisted of international students, norms for the default category were selected. Separate norms were available for men and women. As five participants did not state their gender, their data were omitted for benchmarking. For male participants (aged 18–35, default society), a T-score ≥ 65 corresponded to a BPM total score of ≥15, an internalising problem score of ≥5, an externalising problem score of ≥8, and an attentional problem score of ≥7. For female participants, these were ≥14, ≥5, ≥7, and ≥6, respectively. Using these cut-off values, 20.3% of students in the present sample had BPM total scores that were sufficiently elevated to be of concern. As for the subscales, 20.8% of students had internalising problem scores that were of concern, 7.0% for externalising problems, and 20.2% for attentional problems.
3.3 Mental health disparities
The overall linear model examining the impact of gender, sexual orientation, ethnic background, internationality, disability, and parental education on the BPM total score was statistically significant, F(6,1991) = 40.31, p < 0.001, = 10.56%. The same was true for the linear models predicting internalising [F(6,1991) = 38.75, p < 0.001, = 10.19%], externalising [F(6,1991) = 21.26, p < 0.001, = 5.74%], and attentional problems [F(6,1991) = 20.77, p < 0.001, = 5.61%]. An overview of the standardised coefficients, t values, and p values of the six predictors in all four models is presented in Table 2; mean BPM scores for each subgroup per (sub)scale are presented in Table 3. Controlling for the effects of the other sociodemographic variables, female students had significantly higher total, internalising, and externalising mental health problems than male students; students who did not identify as heterosexual had higher total, internalising, and attentional problems than heterosexual students; Dutch students with a migration background had higher total and externalising problems compared to those without a migration background; international students had higher total and internalising problems than Dutch students; students with disabilities scored higher on the total BPM and all three subscales relative to students without disabilities; and first-generation students had higher externalising mental health problems than continuing-generation students.
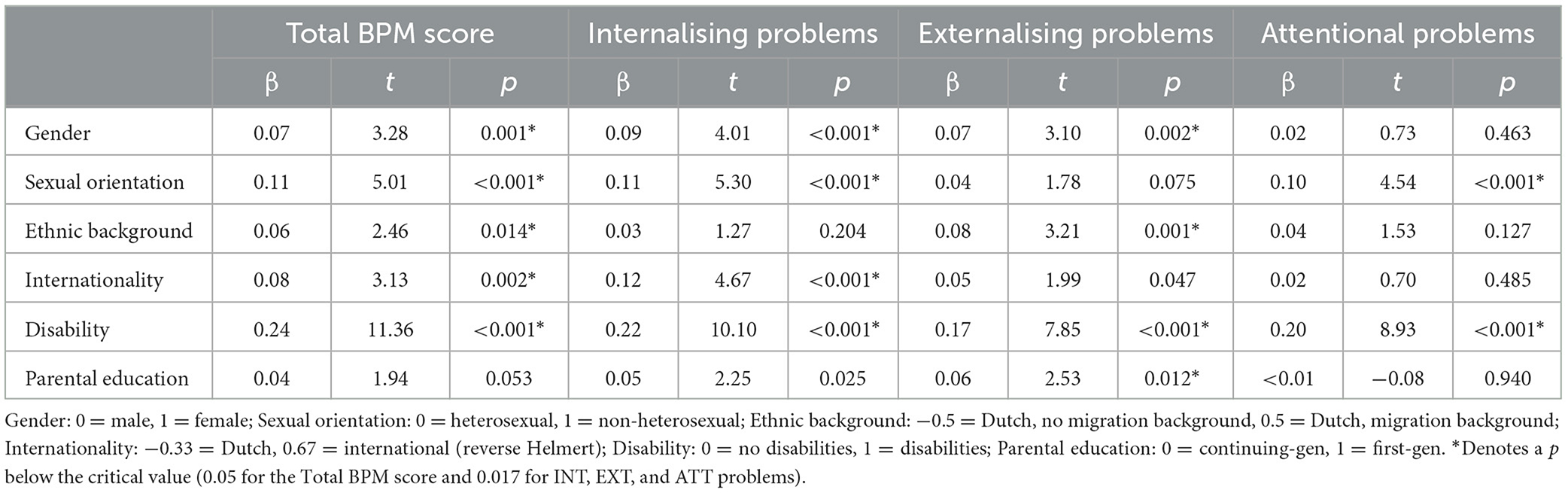
Table 2. Regression coefficients of the four linear models predicting the BPM (sub)scale scores from gender, sexual orientation, ethnic background, internationality, disability, and parental education.
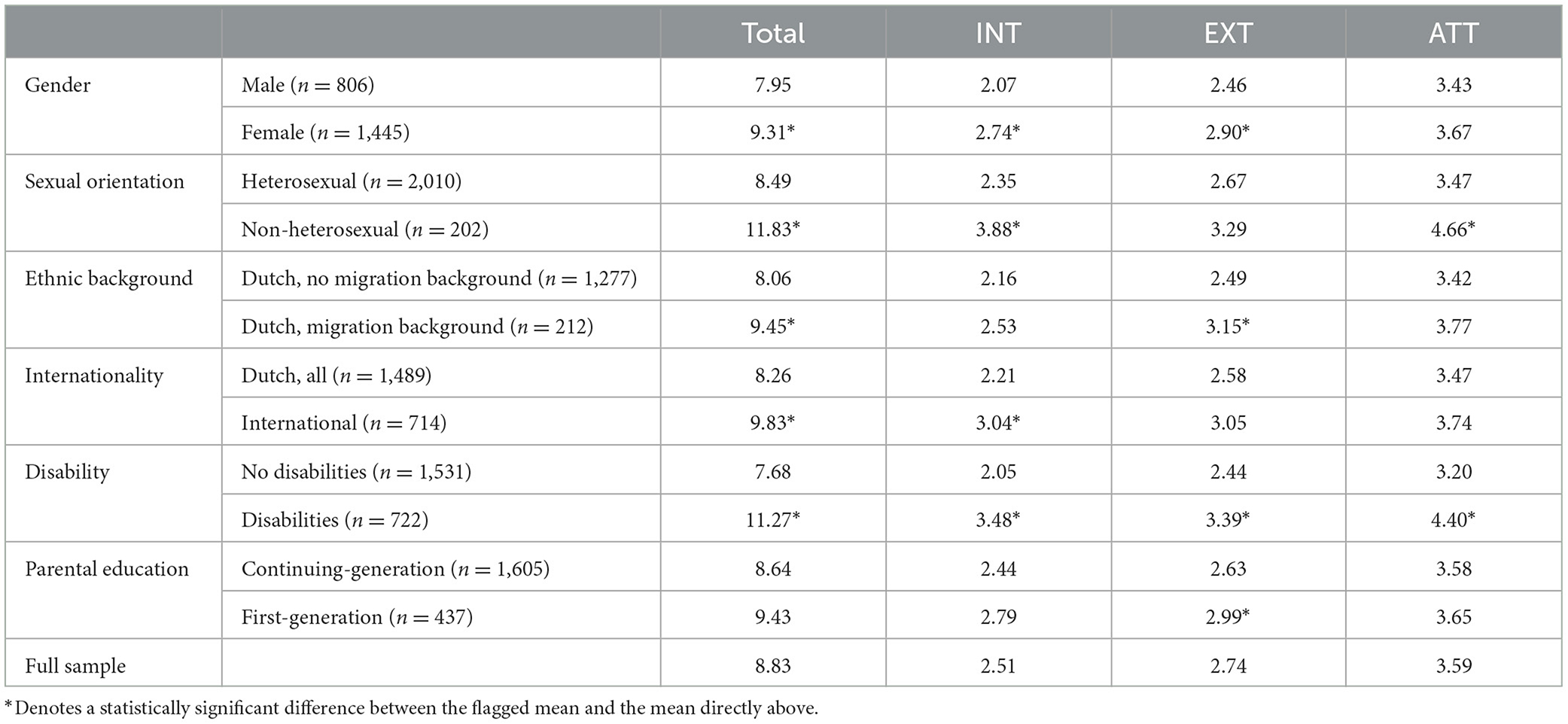
Table 3. Mean BPM (sub)scale scores for each group included in the linear models.
3.4 Response bias analysis
Of the 2,256 participants who started the survey, 55.4% were categorised as “early” respondents, 35.2% as “late”, and 9.4% as “very late”. An analysis of non-response bias in the dependent variables is shown in Table 4. The BPM total score as well as internalising and attentional problems were higher in late compared to early respondents, and slightly lower for very late compared to late ones. Externalising problems were higher in late relative to early respondents, and yet higher in very late ones. However, few of these differences were statistically significant. Levene's test indicated that the variances between the response groups significantly differed for the BPM total score (p = 0.049) and for internalising problems (p = 0.019). Therefore, for these (sub)scales we report the estimates associated with Welch's F. Response speed was significantly associated with the BPM total score [F(2,566) = 3.13, p = 0.044, η2 = 0.003] and with externalising problems [F(2,2253) = 3.39, p = 0.034, η2 = 0.003], but not internalising [F(2,569) = 1.75, p = 0.175, η2 = 0.002] and attentional [F(2,2253) = 1.64, p = 0.195, η2 = 0.001] problems. None of the Games-Howell post-hoc tests was significant at the 0.05 level (p values ranging from 0.078 to 0.996), except for the difference between early and late respondents on the BPM total score (p = 0.045).
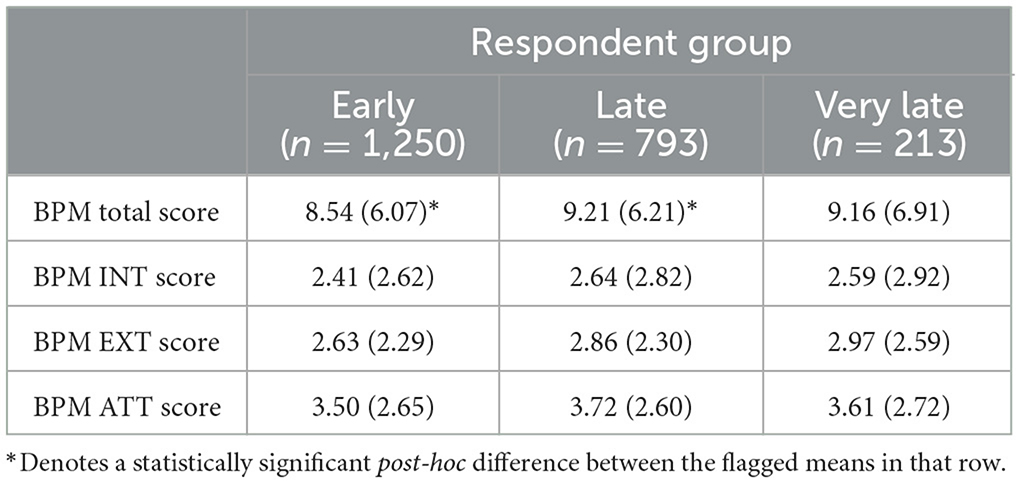
Table 4. Means (standard deviations in brackets) of the BPM (sub)scale scores by respondent group.
For the independent variables, we first examined whether they were distributed in line with previous research or population data. If not, we argued they could be a source of non-response bias. Gender was not distributed evenly in our sample, as more respondents were female (64.1%). The distribution of sexual orientation (9.0% was not heterosexual) was in line with existing data, as it matched recent findings from another Dutch student sample (~10%; Kelders et al., 2019). Students with a migration background were underrepresented in our sample (9.4% vs. estimates of around 20%; Weber, 2016), and international students were overrepresented (31.6% vs. 20.4% according to the university's 2018 annual report, Erasmus University Rotterdam, 2018). The percentage of students with disabilities in our study (32.0%) closely matched a previously reported 34.0% from the Dutch Expert Centre on Inclusive Education (ECIO, 2022). No reliable estimates of the proportion of first-generation students in the Netherlands could be found. Therefore, we examined the association between response speed and four predictors: gender, ethnic background, internationality, and parental education. The overall effect was significant for three: gender [ = 12.83, p = 0.002, V = 0.08], internationality [ = 30.53, p < 0.001, V = 0.12], and parental education [ = 7.16, p = 0.028, V = 0.06], but not for ethnic background [ = 4.73, p = 0.094, V = 0.06]. Post-hoc tests (Bonferroni-corrected z tests for independent proportions; not specified in the pre-registration; Table 5) indicated that, specifically, male students were more likely to respond very late (12.4% of men vs. 7.8% of women); Dutch students with a migration background were less likely to respond early (45.8% of students with vs. 53.7% of students without a migration background); and Dutch students and first-generation students were less likely to respond early (52.6% of Dutch students vs. 62.0% of internationals; and 50.6% of first-gen students vs. 56.8% of continuing-gen students) and more likely to respond late (38.8% vs. 26.9% and 40.5% vs. 33.6%, respectively).
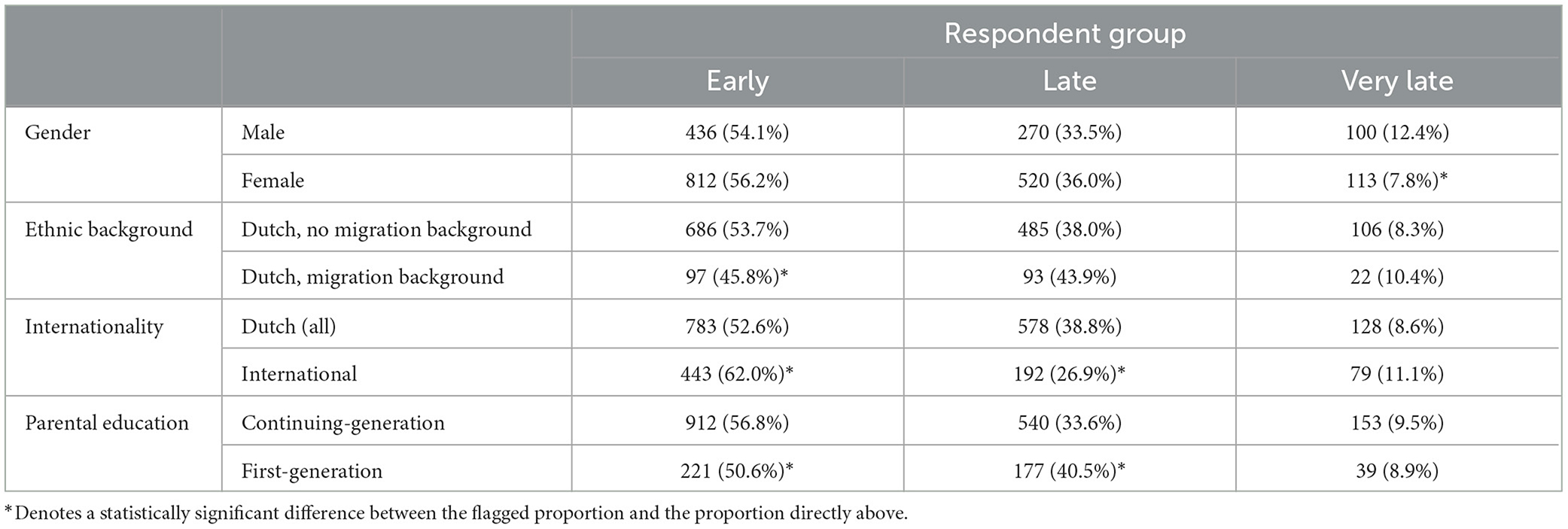
Table 5. Observed frequencies and proportions of response latency in relation to gender, ethnic background, internationality, and parental education.
4 Discussion and conclusion
Using data from a large sample of students at a Dutch university, the present study examined disparities in internalising, externalising, and attentional mental health problems in relation to gender, sexual orientation, ethnicity, internationality, disability, and parental education. In addition to these main analyses, we examined the psychometric qualities of the inventory used for measuring mental health; benchmarked the mental health of our sample to that of a normative population; and performed an elaborate response bias analysis.
Mental health problems were assessed with the Brief Problem Monitor (BPM), for which we found good reliabilities that were similar to those found in another large Dutch sample (De Vries et al., 2020), and moderately high factor loadings that were largely in line with the BPM's intended structure. The only deviation was item 17, “I get upset too easily”, which loaded stronger on the factor comprising the internalising items than it did on the factor comprising the externalising ones. This may have occurred due to participants interpreting being “upset” as directing feelings inwards rather than outwards, as the item was intended. Overall, the psychometric analysis of the BPM data confirmed the instrument as a viable option for measuring emotional and behavioural functioning across multiple domains in contexts that require a brief testing instrument.
Benchmarking our data revealed that our student sample was at higher risk of experiencing mental health problems than the general 18–35 year-old population: approximately 20% of students scored above the “of concern” cut-off for the total BPM, while this cut-off is located at the 93rd percentile of the norm group. The same was observed for the internalising and attentional subscales. This finding is in line with student mental health research in other Western countries (e.g., Adlaf et al., 2001; Leahy et al., 2010; but see Van der Velden et al., 2019), and is further supported by data from the Netherlands Twin Register reported by De Vries et al. (2020), who found that ~11% of non-clinical 18–35 year-old adults score above the total BPM cut-off, ~10% score above the cut-off for internalising problems, and likewise ~10% score above the cut-off for attentional problems. This is slightly more than would be expected based on the BPM's norm data, but far lower than observed for the present sample. Conversely, only 7% of our sample scored above the critical cut-off on externalising problems, which was equivalent to the BPM norm data and lower than the ~10%-rate reported by De Vries et al. (2020), indicating that students are not more likely than the general population to experience externalising mental health problems that are of concern. An alternative explanation may be the composition of our sample combined with the disparities we find: the majority of respondents are continuing-generation students and have no migration background, while in the present study we show that externalising problems are higher in first-generation students and in those with a migration background.
In analysing the main research question, that is, comparing the mental health of students belonging to historically marginalised populations to that of their peers, the significant effect of ethnic background and parental education on externalising mental health problems was one of several findings that stood out. Based on prior research, we expected that students from historically marginalised groups would score higher on internalising mental health problems. In the present study, such an effect was observed for female students, students not identifying as heterosexual, international students, and students with disabilities, but not for students with a migration background or first-generation students. Instead, these students scored higher than their peers on externalising problems. This finding demonstrates the importance of measuring mental health in a multidimensional fashion and illustrates that simply focussing on internalising problems may lead to a masking of existing mental health issues. A relevant observation to add is that ethnic background and parental education are related: previous research has shown that first-generation students are more likely to belong to an ethnic minority (Bui, 2002), and in the present data as well, first-generation students were significantly more likely to have a migration background (and vice versa). Still, both exerted a statistically significant independent effect on externalising problems, indicating that neither “explained away” the other.
A second main finding that stood out was that female students had higher externalising problems than male students. We had hypothesised, based on studies on conduct problems and alcohol/substance abuse in students, that men would be more likely to externalise negative emotions (i.e., show disruptive or anti-social behaviour), and that women would be more likely to internalise them (i.e., feel depressed or insecure). This is also what is found in research on adolescents, an age group for which the internalising-externalising distinction has been studied more (Bartels et al., 2013). Surprisingly however, in our sample, female students scored higher on both internalising and externalising problems. Interestingly, the same outcome has been reported by De Vries et al. (2020), who speculate that this may be the result of some of the BPM's externalising subscale items representing emotionality-related traits (which may apply more to women), while the more physical, aggressive items from the ASR and ABCL (that may apply more to men) were not selected for the BPM. In support of this conjecture, De Vries et al. find that, for the same sample, men score higher than women on the externalising subscale of the ASR. They suggest that if their findings on the BPM replicate—which they do in the present paper—replacing certain items from the externalising subscale with others, like “I argue a lot” or “I get into many fights”, should be considered. In particular, the present paper finds that women score significantly higher than men on items 13, 17, and 18, which De Vries et al. find for items 3, 11, 17, and 18 (L. P. De Vries, personal communication, August 17, 2023). Since item 17 (“I get upset too easily”) also performed relatively poorly in the factor analysis, this may be a sensible candidate for replacement. As the BPM/18–59 is a rather new instrument, recurrent observations like these are important indicators that can help improve the performance of the scale.
A third main finding that stood out was that disability had—by far—the largest impact on mental health of all sociodemographic variables, and was the only predictor to have a statistically significant effect on all (sub)scales of the BPM. Moreover, these effects may represent a lower bound, as students were included regardless of formal diagnosis and of whether they considered their disability to be an obstacle. For the internalising subscale, the observed effects were in line with our hypotheses. For externalising problems, we had expected an opposite effect (i.e., lower problems in those with disabilities). An obvious critique on the present findings—and a possible explanation for the opposing effect found for the externalising subscale—is that the group of students with disabilities includes students with psychological conditions that are inherently characterised by internalising, externalising, or attentional mental health problems. For example, those with depression are by definition more likely to have high internalising problems. Similarly, it is expected that students who have ADHD report high attentional or externalising concerns. This can potentially bias the estimates, especially when such students make up a larger part of the total group of students with disabilities. To examine the extent to which this may have occurred in the present study, we excluded students who reported disabilities that were common and had obvious characteristics of one of the BPM subscales to it, and redid the main regressions. For the regression predicting internalising problems, we excluded students with anxiety and/or depression, who made up more than one-fourth of the disability group. For the regressions predicting externalising and attentional problems, we excluded students with ADD, ADHD, and/or unspecified problems in concentrating, who together represented more than one-fifth of those with disabilities. The resulting standardised coefficients were about half their original sizes (respectively 0.10 and twice 0.11), but remained statistically significant at the 0.001 level. So, part of the effect of disability on internalising, externalising, and attentional problems was driven by students with psychological conditions that by definition involve these problems, but another part was independent of this. Future studies may want to divide heterogeneous groups like students with disabilities into smaller subgroups (like students with physical, learning/developmental, sensory, and psychological conditions) to address the possibility that effects across the larger group may be obscured or inflated.
Specifically in the context of mental health disparities, examining subgroups is relevant for some of the other sociodemographic variables we included as well. For example, studies have found bisexual students to have poorer mental health than gay and lesbian students (Liu et al., 2019), and have reported differences between the mental health of students of various non-White ethnicities (Eisenberg et al., 2013). This suggests that our comparisons of heterosexual vs. non-heterosexual students and students with vs. those without a migration background may be too coarse. Moreover, instead of merely comparing Dutch with international students, future research would do well to further divide the latter into those coming from countries that have a larger vs. smaller cultural distance to the Netherlands (for example, China vs. Germany), as having to navigate a larger cross-cultural transition has been related to worse mental health (Babiker et al., 1980; Demes and Geeraert, 2014). Finally, recent studies have called for more research into how the intersectionality of students' identities affects their functioning (House et al., 2020; Lipson et al., 2018). In the present paper, we examined the influence of for instance gender while controlling for the impact of other sociodemographic variables. While findings on these unique effects do contribute valuable information to the student mental health literature, students' experiential reality is shaped by their combined sociodemographic characteristics. Thus, it may be more meaningful to examine how these characteristics interact. Such interactions may “create specific, unique conditions of disadvantage (or privilege)” (Smith et al., 2007, p. 553) that subsequently can cause disparities in mental health. As an example, Marx et al. (2022) show that non-binary students have higher feelings of unsafety and poorer mental health than cisgender students, and that these effects are stronger for Black compared to White students, demonstrating an interaction between sexual orientation and ethnic background.
In designing the present study, we took various measures to minimise selective (non)response, such as providing a monetary incentive to counter the impact of potentially biasing motivations to partake (like out of concern for one's mental health). However, since fully negating selective responding is not feasible, we also examined the possible impact of non-response bias on the main findings. Specifically, we tested if differences were present between early, late, and very late respondents under the premise that the data of late(r) respondents resembled that of the—non-observed—non-respondents. On the full BPM scale, late respondents had significantly higher mental health problems than early respondents. Thus, those with higher problems were more hesitant to participate. If non-respondents' behaviour is similar to this or more extreme, we underestimated the total BPM score and possibly the number of students with scores that are of concern (which was already high compared to normative data). With regard to the predictor variables, stronger hesitation to respond (i.e., late(r) responding) was observed in men, students with a migration background, Dutch students, and first-generation students. Since late respondents had higher mental health problems, it is possible that the disparities in mental health between men and women, and between Dutch and international students, are smaller than reported earlier, as male and Dutch students with high problems may be underrepresented in our sample. On the other hand, the mental health disparities between students with vs. those without a migration background, and between first- and continuing-generation students, may be larger than reported, as first-generation students and those with a migration background with high problems may be underrepresented. However, the effect sizes of the differences were rather small, and for the dependent variables, only the effect for the total BPM scale—not the subscales—was statistically significant. Therefore, the impact of selective non-response on the present findings may be minimal.
In conclusion, the present study provides support for disparities in student mental health based on sociodemographic characteristics: using a brief, non-clinical inventory, higher mental health problems were found in female students, students who do not identify as heterosexual, students with a migration background, international students, students with disabilities, and first-generation students. These findings make an important contribution to the student mental health literature, as there have been “few studies of large, diverse university samples that (…) enable comparison between subgroups” (Stallman, 2010, p. 249, also see Liu et al., 2019). In particular, there have been very few large-scale comparisons of the mental health of international vs. domestic students, students with vs. those without disabilities, and first-generation vs. continuing-generation students. A second critical contribution our study makes is demonstrating the need to take into account different types of mental health—not only measuring internalising symptoms, as most prior research does, but also looking at externalising problems. Most notably, we find that first-generation students and students with a migration background do not differ from their continuing-generation, no migration background peers on internalising mental health problems. However, they do have higher externalising problems. Findings like these have strong implications for how we conceptualise and understand mental health, and additionally have significant implications for practice: if we fail to recognise that different (groups of) students experience different types of mental health concerns, the resources we offer to students are likely to be biased towards internalising mental health problems, and to not fit all students' needs. This is particularly troublesome given that many historically marginalised groups already make less use of mental health services (Hunt and Eisenberg, 2010). If we instead recognise the variations in mental health across sociodemographic groups, policies and services can be appropriately targeted. As university education is characterised by increasingly diverse enrolment, it is necessary to understand how these diverse groups fare in our existing educational system, and whether adjustments are required for these students to reach their full potential.
Data availability statement
The preregistration of the study can be found at https://aspredicted.org/qk7xw.pdf, and the materials can be found at https://osf.io/ntx6k/. The dataset presented in this article is not readily available because anonymity of participants cannot be guaranteed. Requests to access the dataset should be directed to ay5kZWdyb290QGVzc2IuZXVyLm5s.
Ethics statement
The studies involving humans were approved by the Erasmus Research Institute of Management review board (case number IRB-NE-2017-12). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
KDG: Conceptualisation, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Visualisation, Writing – original draught. SW: Data curation, Investigation, Writing – review & editing. JVS: Conceptualisation, Funding acquisition, Writing – review & editing. OL: Methodology, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. Kristel De Groot was supported by a Research Talent Grant from the Dutch Research Council (406.17.505) and a grant from the Community for Learning & Innovation (CLI).
Acknowledgments
The authors thank all students who participated in the study and all staff who helped distribute the survey, including study advisors, diversity officers, study associations, and teaching staff. They also thank students and staff who participated in the pilot and gave feedback on the draft survey. They thank Nayana Satpathy for her role in participant recruitment and data processing.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/feduc.2024.1391067/full#supplementary-material
Footnotes
1. ^Another inventory that fit the criteria for our research purposes is the Global Appraisal of Individual Needs Short Screener (GAIN-SS; Dennis et al., 2006), which, like the BPM, is short, differentiates between various types of mental health problems, and is suitable for clinical and non-clinical populations. Preference was given to the BPM since the subscale that it offers in addition to internalising and externalising problems (attentional problems) has more relevance for students than those offered in the GAIN-SS (substance disorders and crime/violence, which were not common in Bruffaerts et al., 2018 student sample).
2. ^Since a few (~20, exact number not catalogued) email addresses returned an error, the actual number of students that received an invitation was slightly lower than the number used for computing the response rate. Therefore, the response rate as reported here represents a lower bound.
3. ^Students were invited to participate in follow-up surveys in January 2019, June 2019, October 2019, October 2020, October 2021, and November 2023. The current paper only presents data from the entry survey (September 2018).
4. ^The term ‘migration background' formally refers to Dutch citizens who were born abroad (first-generation migration background) or who have at least one parent who was born abroad (second-generation migration background). While the term is not commonly used outside of the Netherlands and is current being phased out of formal publications on Dutch demographics (Statistics Netherlands, 2022), the term is well-known to our sample population, and is a good proxy for students of colour, since the majority of persons with a migration background in the Netherlands (mostly persons of Turkish, Moroccan, Surinamese, or Indonesian descent) are persons of colour (Statistics Netherlands, 2021).
5. ^BPM T-scores are truncated at 50 to prevent overinterpretation of differences between low scores (i.e., scores that are all indicative of minor problems). The maximum T-score for the total BPM is higher than that for the subscales, as the total BPM warrants greater differentiation among high scores (Achenbach and Ivanova, 2018).
References
Achenbach, T. M., and Ivanova, M. Y. (2018). Manual for the ASEBA brief problem monitor for ages 18-59 (BPM/18-59). University of Vermont Research Center for Children, Youth, and Families.
Achenbach, T. M., and Rescorla, L. A. (2003). Manual for the ASEBA adult forms and profiles. University of Vermont Research Center for Children, Youth, and Families.
Adlaf, E. M., Gliksman, L., Demers, A., and Newton-Taylor, B. (2001). The prevalence of elevated psychological distress among Canadian undergraduates: findings from the 1998 Canadian campus survey. J. Am. College Health 50, 67–72. doi: 10.1080/07448480109596009
Akhtar, P., Ma, L., Waqas, A., Naveed, S., Li, Y., Rahman, A., et al. (2020). Prevalence of depression among university students in low and middle income countries (LMICs): a systematic review and meta-analysis. J. Affect. Disord. 274, 911–919. doi: 10.1016/j.jad.2020.03.183
Alessi, E. J., Sapiro, B., Kahn, S., and Craig, S. L. (2017). The first-year university experience for sexual minority students: a grounded theory exploration. J. LGBT Youth 14, 71–92. doi: 10.1080/19361653.2016.1256013
Babiker, I. E., Cox, J. L., and Miller, P. M. (1980). The measurement of cultural distance and its relationship to medical consultations, symptomatology and examination performance of overseas students at Edinburgh university. Soc. Psychiat. 15, 109–116. doi: 10.1007/BF00578141
Baron-Cohen, S., Wheelwright, S., Skinner, R., Martin, J., and Clubley, E. (2001). The autism-spectrum quotient (AQ): Evidence from Asperger syndrome/high-functioning autism, males and females, scientists and mathematicians. J. Autism Dev. Disord. 31, 5–17. doi: 10.1023/A:1005653411471
Bartels, M., Cacioppo, J. T., Van Beijsterveldt, T. C., and Boomsma, D. I. (2013). Exploring the association between well-being and psychopathology in adolescents. Behav. Genet. 43, 177–190. doi: 10.1007/s10519-013-9589-7
Bøe, T., Hysing, M., Lønning, K. J., and Sivertsen, B. (2021). Financial difficulties and student health: results from a national cross-sectional survey of Norwegian college and university students. Mental Health Prev. 21:200196. doi: 10.1016/j.mhp.2020.200196
Borgogna, N. C., McDermott, R. C., Aita, S. L., and Kridel, M. M. (2019). Anxiety and depression across gender and sexual minorities: implications for transgender, gender nonconforming, pansexual, demisexual, asexual, queer, and questioning individuals. Psychol. Sexual Orient. Gender Diver. 6, 54–63. doi: 10.1037/sgd0000306
Borland, J., and James, S. (1999). The learning experience of students with disabilities in higher education. A case study of a UK university. Disab. Soc. 14, 85–101. doi: 10.1080/09687599926398
Bose, J. (2001). “Nonresponse bias analyses at the national center for education statistics,” in Proceedings of Statistics Canada Symposium. Available at: https://nces.ed.gov/FCSM/pdf/IHSNG_StatsCan2_JB.pdf (accessed June 28, 2022).
Breslau, J., Lane, M., Sampson, N., and Kessler, R. C. (2008). Mental disorders and subsequent educational attainment in a US national sample. J. Psychiatr. Res. 42, 708–716. doi: 10.1016/j.jpsychires.2008.01.016
Bruffaerts, R., Mortier, P., Kiekens, G., Auerbach, R. P., Cuijpers, P., Demyttenaere, K., et al. (2018). Mental health problems in college freshmen: prevalence and academic functioning. J. Affect. Disord. 225, 97–103. doi: 10.1016/j.jad.2017.07.044
Bui, K. V. T. (2002). First-generation college students at a four-year university: background characteristics, reasons for pursuing higher education, and first-year experiences. Coll. Stud. J. 36, 3–11.
Chien, Y., Gau, S. S., and Gadow, K. D. (2011). Sex difference in the rates and co-occurring conditions of psychiatric symptoms in incoming college students in Taiwan. Compr. Psychiatry 52, 195–207. doi: 10.1016/j.comppsych.2010.03.009
Coduti, W. A., Hayes, J. A., Locke, B. D., and Youn, S. J. (2016). Mental health and professional help-seeking among college students with disabilities. Rehabil. Psychol. 61, 288–296. doi: 10.1037/rep0000101
De Vries, L. P., Van de Weijer, M. P., Ligthart, L., Willemsen, G., Dolan, C. V., Boomsma, D. I., et al. (2020). A comparison of the ASEBA adult self report (ASR) and the brief problem monitor (BPM/18-59). Behav. Genet. 50, 363–373. doi: 10.1007/s10519-020-10001-3
Demes, K. A., and Geeraert, N. (2014). Measures matter: scales for adaptation, cultural distance, and acculturation orientation revisited. J. Cross Cult. Psychol. 45, 91–109. doi: 10.1177/0022022113487590
Dennis, M. L., Feeney, T., and Stevens, L. H. (2006). Global Appraisal of Individual Needs - Short Screener (GAIN-SS): Administration and Scoring Manual Version 2.0.1. Bloomington, IL: Chestnut Health Systems. doi: 10.1037/t21457-000
Dohrenwend, B. P., and Dohrenwend, B. S. (1976). Sex differences and psychiatric disorders. Am. J. Sociol. 81, 1447–1454. doi: 10.1086/226229
ECIO (2022). Analyse monitor beleidsmaatregelen hoger onderwijs 2021-2022 [Analysis monitor policy measures higher education 2021-2022]. Available at: https://ecio.nl/wp-content/uploads/sites/2/2022/09/ECIO_095_Factsheet_Monitor-Beleidsmaatregelen_tg_2022.pdf (accessed September 23, 2022).
Eisenberg, D., Gollust, S. E., Golberstein, E., and Hefner, J. L. (2007). Prevalence and correlates of depression, anxiety, and suicidality among university students. Am. J. Orthopsychiat. 77, 534–542. doi: 10.1037/0002-9432.77.4.534
Eisenberg, D., Hunt, J., and Speer, N. (2013). Mental health in American colleges and universities: variation across student subgroups and across campuses. J. Nerv. Ment. Dis. 201, 60–67. doi: 10.1097/NMD.0b013e31827ab077
Erasmus University Rotterdam (2018). Jaarverslag 2018 [Annual report 2018]. Available at: https://www.eur.nl/media/2019-07-30808jaarverslag2018opmaak16 (accessed September 23, 2022).
Etopio, A. L., Devereux, P., and Crowder, M. (2019). Perceived campus safety as a mediator of the link between gender and mental health in a national US college sample. Women Health 59, 703–717. doi: 10.1080/03630242.2018.1549646
Farrer, L. M., Gulliver, A., Bennett, K., Fassnacht, D. B., and Griffiths, K. M. (2016). Demographic and psychosocial predictors of major depression and generalised anxiety disorder in Australian university students. BMC Psychiatry 16:241. doi: 10.1186/s12888-016-0961-z
Fleming, A. R., Edwin, M., Hayes, J. A., Locke, B. D., and Lockard, A. J. (2018). Treatment-seeking college students with disabilities: Presenting concerns, protective factors, and academic distress. Rehabil. Psychol. 63, 55–67. doi: 10.1037/rep0000193
Forbes-Mewett, H., and Sawyer, A. (2016). International students and mental health. J. Int. Students 6, 661–677. doi: 10.32674/jis.v6i3.348
Fox, A., Hedayet, M., Mansour, K. E., Kommers, S., and Wells, R. (2022). College students with disabilities experiences with financial, social, and emotional costs on campus in the United States. Int. J. Disab. Dev. Educ. 69, 106–120. doi: 10.1080/1034912X.2021.1966758
Fox, M. L., James, T. G., and Barnett, S. L. (2020). Suicidal behaviors and help-seeking attitudes among deaf and hard-of-hearing college students. Suicide Life-Threat. Behav. 50, 387–396. doi: 10.1111/sltb.12595
Fuller, M., Healey, M., Bradley, A., and Hall, T. (2004). Barriers to learning: a systematic study of the experience of disabled students in one university. Stud. High. Educ. 29, 303–318. doi: 10.1080/03075070410001682592
García-González, J. M., Gutiérrez Gómez-Calcerrada, S., Solera Hernández, E., and Ríos-Aguilar, S. (2021). Barriers in higher education: perceptions and discourse analysis of students with disabilities in Spain. Disab. Soc. 36, 579–595. doi: 10.1080/09687599.2020.1749565
Goldberg, D. P. (1972). The Detection of Psychiatric Illness by Questionnaire: A Technique for the Identification and Assessment of Non-Psychotic Psychiatric Illness. Oxford: Oxford University Press.
Goldberg, D. P., and Williams, P. (1988). A User's Guide to the General Health Questionnaire. Berkshire: NFER, Nelson.
Goode, J. (2007). ‘Managing' disability: early experiences of university students with disabilities. Disab. Soc. 22, 35–48. doi: 10.1080/09687590601056204
Grinshteyn, E., Whaley, R., and Couture, M. (2022). High fear of discriminatory violence among racial, gender, and sexual minority college students and its association with anxiety and depression. Int. J. Environ. Res. Public Health 19:2117. doi: 10.3390/ijerph19042117
Hall, R. M., and Sandler, B. R. (1982). The classroom climate: A chilly one for women? Education Resources Information Center. Available at: https://files.eric.ed.gov/fulltext/ED215628.pdf (accessed March 7, 2022).
Hamaideh, S. H. (2011). Stressors and reactions to stressors among university students. Int. J. Soc. Psychiat. 57, 69–80. doi: 10.1177/0020764009348442
Hong, B. S. (2015). Qualitative analysis of the barriers college students with disabilities experience in higher education. J. Coll. Stud. Dev. 56, 209–226. doi: 10.1353/csd.2015.0032
House, L. A., Neal, C., and Kolb, J. (2020). Supporting the mental health needs of first generation college students. J. College Stud. Psychother. 34, 157–167. doi: 10.1080/87568225.2019.1578940
Hsiao, K. P. (1992). First-generation college students. Education Resources Information Center. Available at: https://files.eric.ed.gov/fulltext/ED351079.pdf (accessed February 28, 2022).
Hunt, J., and Eisenberg, D. (2010). Mental health problems and help-seeking behavior among college students. J. Adolesc. Health 46, 3–10. doi: 10.1016/j.jadohealth.2009.08.008
Hurst, C. S., Baranik, L. E., and Daniel, F. (2013). College student stressors: a review of the qualitative research. Stress Health 29, 275–285. doi: 10.1002/smi.2465
Ibrahim, A. K., Kelly, S. J., Adams, C. E., and Glazebrook, C. (2013). A systematic review of studies of depression prevalence in university students. J. Psychiatr. Res. 47, 391–400. doi: 10.1016/j.jpsychires.2012.11.015
Jung, E., Hecht, M. L., and Wadsworth, B. C. (2007). The role of identity in international students' psychological well-being in the United States: a model of depression level, identity gaps, discrimination, and acculturation. Int. J. Intercult. Relat. 31, 605–624. doi: 10.1016/j.ijintrel.2007.04.001
Kelders, S., Oberschmidt, K., and Bohlmeijer, E. (2019). Student wellbeing: A cross-sectional survey of mental health of UT-students. Available at: https://ris.utwente.nl/ws/portalfiles/portal/172853563/Student_wellbeing_report_28052019_DEF.pdf (accessed January 14, 2022).
Kim, T., and Kim, D. (2023). Chilly climate perceived by female engineering undergraduates: an exploratory study using concept mapping. Front. Psychol. 14:1145795. doi: 10.3389/fpsyg.2023.1145795
Kimball, E. W., Wells, R. S., Ostiguy, B. J., Manly, C. A., and Lauterbach, A. A. (2016). “Students with disabilities in higher education: a review of the literature and an agenda for future research,” in Higher education: Handbook of theory and research, ed. M. B. Paulsen (Cham: Springer), 91–156. doi: 10.1007/978-3-319-26829-3_3
Klein, L. B., and Martin, S. L. (2021). Sexual harassment of college and university students: a systematic review. Trauma Viol. Abuse 22, 777–792. doi: 10.1177/1524838019881731
Klonoff, E. A., Landrine, H., and Campbell, R. (2000). Sexist discrimination may account for well-known gender differences in psychiatric symptoms. Psychol. Women Q. 24, 93–99. doi: 10.1111/j.1471-6402.2000.tb01025.x
Kuder, S. J., Accardo, A. L., and Bomgardner, E. M. (2021). Mental health and university students on the autism spectrum: a literature review. J. Autism Dev. Disord. 8, 421–435. doi: 10.1007/s40489-020-00222-x
Kypri, K., Samaranayaka, A., Connor, J., Langley, J. D., and Maclennan, B. (2011). Non-response bias in a web-based health behaviour survey of New Zealand tertiary students. Prev. Med. 53, 274–277. doi: 10.1016/j.ypmed.2011.07.017
Leahy, C. M., Peterson, R. F., Wilson, I. G., Newbury, J. W., Tonkin, A. L., and Turnbull, D. (2010). Distress levels and self-reported treatment rates for medicine, law, psychology and mechanical engineering tertiary students: cross-sectional study. Austr. New Zeal. J. Psychiat. 44, 608–615. doi: 10.3109/00048671003649052
Lee, J. J., and McCabe, J. M. (2021). Who speaks and who listens: revisiting the chilly climate in college classrooms. Gender Soc. 35, 32–60. doi: 10.1177/0891243220977141
Leleux-Labarge, K., Hatton, A. T., Goodnight, B. L., and Masuda, A. (2015). Psychological distress in sexual minorities: examining the roles of self-concealment and psychological inflexibility. J. Gay Lesbian Mental Health 19, 40–54. doi: 10.1080/19359705.2014.944738
Linden, B., Boyes, R., and Stuart, H. (2022). The post-secondary student stressors index: proof of concept and implications for use. J. Am. College Health 70, 469–477. doi: 10.1080/07448481.2020.1754222
Lippincott, J. A., and German, N. (2007). “From blue collar to ivory tower: counseling first-generation, working-class students,” in Special populations in college counseling: A handbook for mental health professionals, eds. J. A. Lippincott, and R. B. Lippincott (New York: American Counseling Association), 89–98.
Lipson, S. K., Kern, A., Eisenberg, D., and Breland-Noble, A. M. (2018). Mental health disparities among college students of color. J. Adolesc. Health 63, 348–356. doi: 10.1016/j.jadohealth.2018.04.014
Lipson, S. K., Zhou, S., Wagner, I. I. I. B., Beck, K., and Eisenberg, D. (2016). Major differences: variations in undergraduate and graduate student mental health and treatment utilization across academic disciplines. J. College Stud. Psychother. 30, 23–41. doi: 10.1080/87568225.2016.1105657
Liu, C. H., Stevens, C., Wong, S. H., Yasui, M., and Chen, J. A. (2019). The prevalence and predictors of mental health diagnoses and suicide among US college students: implications for addressing disparities in service use. Depress. Anxiety 36, 8–17. doi: 10.1002/da.22830
London, H. B. (1989). Breaking away: a study of first-generation college students and their families. Am. J. Educ. 97, 144–170. doi: 10.1086/443919
Lovibond, P. F., and Lovibond, S. H. (1995). The structure of negative emotional states: comparison of the depression anxiety stress scales (DASS) with the Beck depression and anxiety inventories. Behav. Res. Ther. 33, 335–343. doi: 10.1016/0005-7967(94)00075-U
Martin, N. D. (2012). The privilege of ease: social class and campus life at highly selective, private universities. Res. High. Educ. 53, 426–452. doi: 10.1007/s11162-011-9234-3
Marx, R. A., Maffini, C. S., and Peña, F. J. (2022). Understanding nonbinary college students' experiences on college campuses: An exploratory study of mental health, campus involvement, victimization, and safety. J. Diver. High. Educ. 17:330. doi: 10.1037/dhe0000422
McLeod, J. D., Meanwell, E., and Hawbaker, A. (2019). The experiences of college students on the autism spectrum: a comparison to their neurotypical peers. J. Autism Dev. Disord. 49, 2320–2336. doi: 10.1007/s10803-019-03910-8
Meyer, I. H. (2003). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: conceptual issues and research evidence. Psychol. Bull. 129, 674–697. doi: 10.1037/0033-2909.129.5.674
Mori, S. C. (2000). Addressing the mental health concerns of international students. J. Couns. Dev. 78, 137–144. doi: 10.1002/j.1556-6676.2000.tb02571.x
Nerdrum, P., Rustøen, T., and Rønnestad, M. H. (2006). Student psychological distress: a psychometric study of 1750 Norwegian 1st-year undergraduate students. Scandinav. J. Educ. Res. 50, 95–109. doi: 10.1080/00313830500372075
Oakes, J. M., and Andrade, K. E. (2017). “The measurement of socioeconomic status,” in Methods in social epidemiology, eds. J. M. Oakes, and J. S. Kaufman (San Francisco, CA: Jossey-Bass), 23–42.
Ojeda, L., Navarro, R. L., Meza, R. R., and Arbona, C. (2012). Too Latino and not Latino enough: the role of ethnicity-related stressors on Latino college students' life satisfaction. J. Hispanic High. Educ. 11, 14–28. doi: 10.1177/1538192711435553
Parr, N. J. (2020). Sexual assault and co-occurrence of mental health outcomes among cisgender female, cisgender male, and gender minority US college students. J. Adoles. Health 67, 722–726. doi: 10.1016/j.jadohealth.2020.03.040
Pierce, C. M. (1974). “Psychiatric problems of the black minority,” in American handbook of psychiatry, ed. S. Arieti (New York: Basic Books), 512–523.
Poyrazli, S., and Lopez, M. D. (2007). An exploratory study of perceived discrimination and homesickness: a comparison of international students and American students. J. Psychol. 141, 263–280. doi: 10.3200/JRLP.141.3.263-280
Rankin, S. R. (2003). Campus climate for gay, lesbian, bisexual, and transgender people: A national perspective. The Policy Institute of the National Gay and Lesbian Task Force. Available at: https://www.whoi.edu/cms/files/CampusClimate_23425.pdf (accessed February 4, 2022).
Rankin, S. R., Weber, G. N., Blumenfeld, W. J., and Frazer, S. (2010). 2010 State of Higher Education for Lesbian, Gay, Bisexual and Transgender People. Charlotte, NC: Campus Pride.
Reisbig, A. M., Danielson, J. A., Wu, T., Hafen Jr, M., Krienert, A., Girard, D., et al. (2012). A study of depression and anxiety, general health, and academic performance in three cohorts of veterinary medical students across the first three semesters of veterinary school. J. Vet. Med. Educ. 39, 341–358. doi: 10.3138/jvme.0712-065R
Richardson, T., Elliott, P., Roberts, R., and Jansen, M. (2017). A longitudinal study of financial difficulties and mental health in a national sample of British undergraduate students. Commun. Ment. Health J. 53, 344–352. doi: 10.1007/s10597-016-0052-0
Said, D., Kypri, K., and Bowman, J. (2013). Risk factors for mental disorder among university students in Australia: findings from a web-based cross-sectional survey. Soc. Psychiatry Psychiatr. Epidemiol. 48, 935–944. doi: 10.1007/s00127-012-0574-x
Shadowen, N. L., Williamson, A. A., Guerra, N. G., Ammigan, R., and Drexler, M. L. (2019). Prevalence and correlates of depressive symptoms among international students: implications for university support offices. J. Int. Stud. 9, 129–148. doi: 10.32674/jis.v9i1.277
Sheldon, E., Simmonds-Buckley, M., Bone, C., Mascarenhas, T., Chan, N., Wincott, M., et al. (2021). Prevalence and risk factors for mental health problems in university undergraduate students: a systematic review with meta-analysis. J. Affect. Disord. 287, 282–292. doi: 10.1016/j.jad.2021.03.054
Silverschanz, P., Cortina, L. M., Konik, J., and Magley, V. J. (2008). Slurs, snubs, and queer jokes: incidence and impact of heterosexist harassment in academia. Sex Roles 58, 179–191. doi: 10.1007/s11199-007-9329-7
Skead, N., and Rogers, S. L. (2014). Stress, anxiety and depression in law students: how student behaviors affect student wellbeing. Monash Univ. Law Rev. 40, 564–587. doi: 10.2139/ssrn.2392131
Smedley, B. D., Myers, H. F., and Harrell, S. P. (1993). Minority-status stresses and the college adjustment of ethnic minority freshmen. J. Higher Educ. 64, 434–452. doi: 10.1080/00221546.1993.11778438
Smith, R. A., and Khawaja, N. G. (2011). A review of the acculturation experiences of international students. Int. J. Interc. Relat. 35, 699–713. doi: 10.1016/j.ijintrel.2011.08.004
Smith, W. A., Allen, W. R., and Danley, L. L. (2007). “Assume the position... you fit the description.” Psychosocial experiences and racial battle fatigue among African American male college students. Am. Behav. Sci. 51, 551–578. doi: 10.1177/0002764207307742
Solórzano, D., Ceja, M., and Yosso, T. (2000). Critical race theory, racial microaggressions, and campus racial climate: the experiences of African American college students. J. Negro Educ. 69, 60–73.
Soria, K. M., Weiner, B., and Lu, E. C. (2014). Financial decisions among undergraduate students from low-income and working-class social class backgrounds. J. Stud. Financ. Aid 44:2. doi: 10.55504/0884-9153.1037
Stallman, H. M. (2010). Psychological distress in university students: a comparison with general population data. Aust. Psychol. 45, 249–257. doi: 10.1080/00050067.2010.482109
Statistics Netherlands (2021). Bevolking; geslacht, leeftijd, generatie en migratieachtergrond [Population; gender, age, generation, and migration background]. Available at: https://opendata.cbs.nl/statline/#/CBS/nl/dataset/37325/table?ts=1653915950728 (accessed May 30, 2022).
Statistics Netherlands (2022). CBS introducing new population classification by origin. Available at: https://www.cbs.nl/en-gb/news/2022/07/cbs-introducing-new-population-classification-by-origin (accessed March 18, 2022).
Stebleton, M. J., Soria, K. M., and Huesman Jr, R. L. (2014). First-generation students' sense of belonging, mental health, and use of counseling services at public research universities. J. College Counsel. 17, 6–20. doi: 10.1002/j.2161-1882.2014.00044.x
Steptoe, A., Tsuda, A., and Tanaka, Y. (2007). Depressive symptoms, socio-economic background, sense of control, and cultural factors in university students from 23 countries. Int. J. Behav. Med. 14, 97–107. doi: 10.1007/BF03004175
Sue, D. W. (2010). Microaggressions in Everyday Life: Race, Gender, and Sexual Orientation. New York: John Wiley and Sons.
Sue, D. W., Bucceri, J., Lin, A. I., Nadal, K. L., and Torino, G. C. (2007). Racial microaggressions and the Asian American experience. Cult. Diver. Ethnic Minority Psychol. 13, 72–81. doi: 10.1037/1099-9809.13.1.72
Swim, J. K., Hyers, L. L., Cohen, L. L., and Ferguson, M. J. (2001). Everyday sexism: evidence for its incidence, nature, and psychological impact from three daily diary studies. J. Soc. Issues 57, 31–53. doi: 10.1111/0022-4537.00200
Swim, J. K., Hyers, L. L., Cohen, L. L., Fitzgerald, D. C., and Bylsma, W. H. (2003). African American college students' experiences with everyday racism: characteristics of and responses to these incidents. J. Black Psychol. 29, 38–67. doi: 10.1177/0095798402239228
Toutain, C. (2019). Barriers to accommodations for students with disabilities in higher education: a literature review. J. Postsecondary Educ. Disab. 32, 297–310.
UNESCO Institute for Statistics (2022). Inbound internationally mobile students by continent of origin. Available at: http://data.uis.unesco.org/index.aspx?queryid=3804# (accessed February 18, 2022).
Van der Velden, P. G., Das, M., and Muffels, R. (2019). The stability and latent profiles of mental health problems among Dutch young adults in the past decade: a comparison of three cohorts from a national sample. Psychiatry Res. 282:112622. doi: 10.1016/j.psychres.2019.112622
Weber, S. (2016). Folia checkt: ‘Qua instroom van niet-westerse allochtonen is UvA tweede van Nederland' [Folia checks: ‘In terms of influx of non-Western immigrants, UvA comes second in the Netherlands']. Available at: https://www.folia.nl/actueel/101511/folia-checkt-qua-instroom-van-niet-westerse-allochtonen-is-uva-tweede-van-nederland (accessed September 23, 2022).
Wei, M., Liao, K. Y., Chao, R. C., Mallinckrodt, B., Tsai, P., and Botello-Zamarron, R. (2010). Minority stress, perceived bicultural competence, and depressive symptoms among ethnic minority college students. J. Couns. Psychol. 57, 411–422. doi: 10.1037/a0020790
Weitzman, E. R. (2004). Poor mental health, depression, and associations with alcohol consumption, harm, and abuse in a national sample of young adults in college. J. Nerv. Ment. Dis. 192, 269–277. doi: 10.1097/01.nmd.0000120885.17362.94
Wolanin, T. R., and Steele, P. (2004). Higher education opportunities for students with disabilities: A primer for policymakers. The Institute for Higher Education Policy. Available at: https://vtechworks.lib.vt.edu/server/api/core/bitstreams/ae855738-78e3-4128-8c47-5d0bcd40d164/content (accessed April 20, 2022).
Keywords: university students, mental health, minority groups, diversity, higher education
Citation: De Groot K, Wieman SM, Van Strien JW and Lindemann O (2024) To each their own: sociodemographic disparities in student mental health. Front. Educ. 9:1391067. doi: 10.3389/feduc.2024.1391067
Received: 29 February 2024; Accepted: 09 September 2024;
Published: 27 September 2024.
Edited by:
Valerie Sotardi, University of Canterbury, New ZealandReviewed by:
Mark Vicars, Victoria University, AustraliaSimon Benham-Clarke, University of Exeter, United Kingdom
Copyright © 2024 De Groot, Wieman, Van Strien and Lindemann. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kristel De Groot, ay5kZWdyb290QGVzc2IuZXVyLm5s