
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Educ. , 08 April 2024
Sec. Educational Psychology
Volume 9 - 2024 | https://doi.org/10.3389/feduc.2024.1353756
 Juliana Alvares Duarte Bonini Campos1
Juliana Alvares Duarte Bonini Campos1 Lucas Arrais Campos2,3,4*
Lucas Arrais Campos2,3,4* Maria Antonia Ramos Azevedo5
Maria Antonia Ramos Azevedo5 Bianca Gonzalez Martins1
Bianca Gonzalez Martins1 Bianca Núbia Souza Silva3
Bianca Núbia Souza Silva3 João Marôco6,7
João Marôco6,7Introduction: The COVID-19 pandemic brought profound societal changes and disruptions, including in the education system, which underwent swift modifications. It presented unique challenges for both professors and students, contributing to an increase in the prevalence of mental health-related symptoms.
Objective: To determine the prevalence of mental health disorders symptoms, coping strategies, and concerns among students (≥18 years) and professors at different times during the COVID-19 pandemic.
Methods: This was an online cross-sectional study (Student: N = 6,609; Phase 1 = 3,325; Phase 2 = 1,402; Phase 3 = 1,882; Professor: N = 9,096; Phase 1 = 3,924; Phase 2 = 2,223; Phase 3 = 2,949). Depression, Anxiety, and Stress Scale (DASS-21), Impact of Event Scale-revised (IES-R), and BriefCOPE inventory were used. The probability of presenting the symptoms was calculated by multiple logistic regression and odds ratio (OR).
Results: The prevalence of depression, anxiety, stress, and distress symptoms among students and professors was high (≥59.5% and ≥ 33.5%, respectively). Students, women, and those diagnosed with a mental disorder were more likely to have symptoms or distress. In the face of the pandemic, professors used more adaptive coping strategies than students. Health was the focus of professors’ concerns, while for students, future and labor market uncertainty were concerns derived from the health core.
Conclusion: The results point to the need to strengthen psychosocial support for both professors and students.
Santos (2020) and Harari (2020) argue that the COVID-19 pandemic has taught us some lessons about human behavior and its impact on the world. The authors (Harari, 2020; Santos, 2020) point out that the social isolation and quarantine imposed by the health crisis have raised unprecedented social, economic, political, environmental, physical, and emotional issues. As a result, there have been significant changes in several domains of life that have required us to reshape our ways of living.
In Brazil, with the announcement of the pandemic by the World Health Organization (March 11th, 2020), the Ministry of Health decreed lockdowns in several locations across the country, maintaining only essential services, such as hospitals and food establishments. Among the sectors most impacted by the pandemic was the education system, which initially had its activities suspended. However, with the prolongation of the pandemic, it needed to be quickly reorganized into an emergency distance learning system to ensure continuity (Sousa and Coimbra, 2020; Pinho et al., 2021; Telyani et al., 2021; Tri Sakti et al., 2022).
Both professors and students had to adapt to technological and digital resources to make the teaching-learning process viable. This transition demanded proactivity and creativity in implementing synchronous and asynchronous activities. However, there were immediate consequences, such as the expansion of the working hours of professors, the precariousness of working conditions adapted in households, increased spending on work equipment, and a general safety (Bernardo et al., 2020; Azzi et al., 2022; Weibenfels et al., 2022). Although these consequences were initially focused on the configurations of teaching during the pandemic (Bernardo et al., 2020; Azzi et al., 2022; Weibenfels et al., 2022), they can be easily extended to students as well.
The surveys conducted with professors (Bernardo et al., 2020; Ozamiz-Etxebarria et al., 2021; Pinho et al., 2021) show that, regardless of their teaching level and sector (elementary, secondary, or higher education, public or private), many of them encountered an unfamiliar universe, not only in terms of using technology to deliver instruction but also in terms of establishing connections with students and peers in non-face-to-face spaces. Being outside the classroom environment and having family obligations that intersected with course requirements were aggravating elements of the learning process for both professors and students. For students, this experience was perhaps even more remarkable due to the chaotic scenario characterized by a lack of signs of new opportunities and future professional possibilities and chronic inequalities that were constantly and rapidly changing (Kivunja, 2015; Harari, 2018). The limited skills and behavioral repertoire that younger people have to cope with so many challenges indicate the complexity of adapting their routine to the pandemic reality (Campos et al., 2020).
In the dynamic of a teaching-learning process where students are the protagonists, the responsibility of the professor extends beyond the mere transmission of information and the construction of knowledge. It should also involve developing the active participation of students in their learning process, giving them autonomy and freedom to carry out their own construction so that learning becomes significant for them. This, in turn, enables the building of educational spaces and relationships in a historical and multicultural context (Freire, 1996). However, the complexity of teaching and the challenges for the unfolding of student protagonism in this unfavorable scenario of the pandemic, especially for those preparing for and approaching the labor market, can lead to overload and physical and mental illness.
In previous studies, a high prevalence of depression, anxiety, stress, and subjective distress symptoms was found among university students (Chang et al., 2021; Li et al., 2021; Wang et al., 2021; Campos et al., 2021a) and professors (Ozamiz-Etxebarria et al., 2021; Silva et al., 2021). Li et al. (2021) and Silva et al. (2021) indicate that after the onset of the COVID-19 pandemic, this prevalence increased. Some studies also point to a worrisome prevalence of burnout among students (Azzi et al., 2022; Salmela-Aro et al., 2022) and professors (Pressley, 2021; Weibenfels et al., 2022) given the overload caused not only by the health crisis but also by the rapid and massive transformation of the educational process during COVID-19.
Education in times of pandemic therefore becomes a challenging task, and as we witness the renewal of teaching and learning processes in this scenario, we must have a supportive look at how professors and students have experienced, how they have suffered, how they have resigned, and how these experiences have finally revealed fundamental questions about the life and mental health in this context. We cannot but emphasize that the pandemic severely shook the journey of students in the final year of their program and on their way to professional life, as they were not on school campuses and thus felt even more fragile in their professional identity formation, which in the context of the pandemic seems so far removed from concrete reality.
Thus, this study aimed to gather information on the mental health of Brazilian professors and students (over 18 years old) during the COVID-19 pandemic using a large national sample. Self-reported information was collected to identify the prevalence of mental health disorder symptoms, coping strategies, and main concerns at different times during the pandemic. To the best of our knowledge, this is the first study conducted with a large sample of Brazilian professors and students during different periods of the pandemic, providing relevant information to understand the educational scenario during the pandemic from the perspective of its actors. The evidence presented may also be useful for developing programs and actions aimed at promoting mental health and well-being in the educational environment.
Despite numerous studies conducted during the COVID-19 pandemic, to the best of our knowledge, no research has provided data on coping mechanisms and symptoms across multiple stages of the pandemic or simultaneously collected data from both teachers and students. Thus, the present study is also justified by the scarcity of such information in existing literature. This information could deepen understanding of global transformations in education and their impact on the mental health of teachers and students. This knowledge could better equip practitioners and researchers to develop strategies to handle future crises and support the educational population.
Three main theoretical frameworks were used in the conduction of the present study: one for assessing and interpreting coping strategies; another for identifying symptoms of depression, anxiety, and stress; and a third for recognizing subjective distress in response to the pandemic. To assess coping strategies, the cognitive and behavioral perspective described by Carver et al. (1989) was applied in the present study. These authors developed a model based on the study of Folkman and Lazarus (1980) and on the studies of their own research group, which presented a behavioral model of self-regulation (Carver and Scheier, 1981, 1983, 1985; Scheier and Carver, 1988). Folkman and Lazarus (1980) proposed a model that divides coping into two functional categories: 1. problem-focused coping and 2. emotion-focused coping. Additionally, it is considered that the coping strategy employed, regardless of its functional category, should not be inherently labeled as good or bad, adaptive or maladaptive (Folkman and Lazarus, 1980; Carver et al., 1989). Understanding both the nature of the stressor and the individual and social context involved is necessary. From this perspective, coping refers to cognitive and behavioral efforts, which are deliberate actions individuals undertake to deal with specific demands.
Regarding symptoms of depression, anxiety, and stress, the theoretical model employed in the present study was the one that considers a clinical overlap among these concepts (Watson et al., 1995). This proposal is grounded in the tripartite model, in which symptoms of anxiety and depression are grouped into three basic structures: 1. the presence of negative affects, such as depressed mood, insomnia, discomfort, and irritability; 2. factors representing specific symptoms for depression (anhedonia and absence of positive affect); and 3. specific symptoms of anxiety, including somatic tension and hyperactivity (Watson et al., 1995).
For identifying subjective distress, we used a psychometric scale (Caiuby et al., 2012) developed based on the criteria outlined in the third edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-III) (American Psychiatric Association, 1980). We clarify that, when conducting the present study, we did not find other simple and self-administered scales for assessing subjective distress that had been developed following the most current edition of DSM (5th ed., DSM-5) (American Psychiatric Association, 2013). Furthermore, given that the present study was conducted online, we understood that using clinical criteria without a clinical assessment would not be feasible. Therefore, the framework adopted for subjective distress was based on the DSM-III (American Psychiatric Association, 1980).
This cross-sectional study used online data from a larger project approved by the National Commission for Ethics in Research of the Ministry of Health (CONEP). The larger project is a national survey that has collected data at three-time points, 6 months apart since the beginning of the pandemic, using Google Form or Lime Survey platforms.1 The link to the survey was sent by email, WhatsApp, or social networks, and remained accessible for about 40 days. The initial contact was made through publicly accessible information on websites of Brazilian higher education institutions (public and private) using non-probability sampling, and the participants were asked to distribute the link to work and personal contacts (snowball technique).
The inclusion criteria were age ≥ 18 years and being a student or professor. In Brazil, students who are 18 years old may be attending the final years of high school/technical school or the first years of undergraduate studies. However, the present study did not differentiate between these levels, as our interest was solely in identifying the participants’ “professional category,” which in this case, was either student or professor. As educational level varies according to age, we chose to control for the effect of age in our statistical analyses rather than specifying educational categories. Information on the teaching level (elementary, high school, or higher education), the type of institution (public or private) of professors, and the education level of the students was also not available. Despite this being a limitation of the study, we understand that its conduction may provide information and trigger relevant reflections that could serve as a starting point for the development of future studies focused on assessing the mental health of these individuals in the peri and post-pandemic context. A total of 12,196, 6,261, and 7,977 people participated in phases 1, 2, and 3, respectively.
Information on age (years), gender (man, woman, non-binary), Brazil macro-region, monthly family income (by income range, in Brazilian reals), pre-existing diagnosis of mental disorder before the pandemic, perceived safety toward the pandemic (very unsafe, unsafe, safe, very safe), and mental health alterations since the beginning of the pandemic (no, yes) was collected. The dependent variables were symptoms of depression, anxiety, stress, subjective distress, and the coping strategies used by the participants. Additionally, participants were asked to provide three open-ended responses to the question: “What are your top 3 concerns at the moment?”
The minimum sample size was calculated based on the number of items of the longest scale (28 items and 14 correlated factors), the number of parameters to be estimated (119), and 5 to 10 participants per parameter. This resulted in a minimum sample size of 595 to 1,190 participants. This sample size was calculated to ensure that the analytical strategies could be conducted, including the verification of the factorial validity of the scales in the samples.
The Portuguese version of the Depression, Anxiety and Stress Scale (DASS-21) (Martins et al., 2019), the Impact of Event Scale-revised (IES-R) (Caiuby et al., 2012), and the BriefCOPE Inventory (Maroco et al., 2014) were used in the study.
The DASS-21 has 21 items distributed in 3 factors (Factor/item examples - Depression: “I felt I wasn’t worth much as a person,” Anxiety: “I felt scared without any good reason” and Stress: “I felt that I was using a lot of nervous energy”) and a 4-point Likert-type response scale. The scores of each item are added and multiplied by two. The participants were then grouped according to the degree of involvement, following the proposal of Lovibond and Lovibond (1995) (Depression: Normal - 0 to 9, Mild - 10 to 13, Moderate - 14 to 20, Severe - 21 to 27, and Extremely severe ≥28; Anxiety: Normal - 0 to 7, Mild - 8 to 9, Moderate - 10 to 14, Severe - 15 to 19, and Extremely severe ≥20; Stress: Normal - 0 to 14, Mild - 15 to 18, Moderate - 19 to 25, Severe - 26 to 33, and Extremely severe ≥34).
The IES-R has 22 items distributed in 3 factors (Factor/item examples – Avoidance: “I avoid letting myself get upset when I think about it or I am reminded of it,” Intrusion: “Other things keep making me think about it,” and Hyperarousal: “Reminders of it cause me to have physical reactions, such as sweating, trouble breathing, nausea, or a pounding heart”), but a general score for subjective distress can be obtained by the sum of the responses (Normal - 0 to 23, Mild - 24 to 32, Moderate - 33 to 36, Severe - ≥37) (Wang et al., 2020). The items have a 5-point Likert-type response scale.
The BriefCOPE has 28 items arranged in 14 factors (Factor/item examples - Active Coping – AC: “I’ve been taking action to try to make the situation better,” Planning – PL: “I’ve been thinking hard about what steps to take,” Instrumental Support – IS: “I’ve been getting help andadvice from other people,” Emotional Support – ES: “I’ve been getting emotional support from others,” Religion – RE: “I’ve been praying or meditating,” Positive Reinterpretation – PR: “I’ve been looking for something good in what is happening,” Self-Blame – SB: “I’ve been criticizing myself,” Acceptance – AT: “I’ve been learning to live with it,” Venting of Emotions – VE: “I’ve been expressing my negative feelings,” Denial – DN: “I’ve been saying to myself “this is not real,” Self-Distraction – SD: “I’ve been turning to work or other activities to take my mind off things,” Behavioral Disengagement – BD: “I’ve been, Substance Use – SU: “I’ve been using alcohol or other drugs to make myself feel better,” and Humor – HU: “I’ve been making jokes about it”) (Carver, 1997). The scale is answered on a 5-point scale (Maroco et al., 2014) and the participants were grouped considering the average score of each factor into usual strategy (≥3) and non-usual strategy (<3).
The factorial validity of the data was estimated by confirmatory strategy with a robust estimation of weighted least squares means and variances adjusted (WLSMV). The model fit to the data was evaluated using the following indices: Comparative Fit Index (CFI), Tucker-Lewis Index (TLI), and Root Mean Square Error of Approximation (RMSEA) with a 90% confidence interval (Marôco, 2021; Kline, 2023). Data reliability was analyzed to verify the consistency of the obtained information, and it was estimated using the Ordinal Coefficient alpha (α). Values of α ≥ 0.70 were considered indicative of adequate reliability. The analyses were conducted in the R program (R Core Team, 2022) using the “lavaan” (Rosseel, 2012) and “semTools” (Jorgensen et al., 2022) packages.
The factorial validity of the data was confirmed for each sample and phase of data collection separately (Student – DASS-21: CFI = 0.974–0.976, TLI = 0.971–0.973, RMSEA = 0.059–0.064; BriefCOPE: CFI = 0.949–0.985, TLI = 0.926–0.978, RMSEA = 0.050–0.077; IES-R: CFI = 0.951–0.966, TLI = 0.944–0.961, RMSEA = 0.067–0.080; Professor – DASS-21: CFI = 0.971–0.982, TLI = 0.967–0.979, RMSEA = 0.058–0.066; BriefCOPE: CFI = 0.964–0.984, TLI = 0.948–0.977, RMSEA = 0.064–0.082; IES-R: CFI = 0.968–0.976, TLI = 0.963–0.973, RMSEA = 0.062–0.068). Reliability was also confirmed (Student – DASS-21: α = 0.86–0.94; BriefCOPE: α = 0.70–0.97; IES-R: α = 0.85–0.92; Professor – DASS-21: α = 0.88–0.95; BriefCOPE: α = 0.70–0.96; IES-R: α = 0.88–0.94).
The concerns expressed by professors and students underwent qualitative analysis using similarity analysis, a graph-theoretic method for determining the relationships between the reported concerns of each group about the pandemic. This analysis was conducted for the general sample of each occupational category, without separating the different phases of data collection. With this analysis, it was possible to identify the occurrences/co-occurrences and narrow down the relations between the pandemic-related concerns mentioned by the participants. A static Fruchterman Reingold graph was created to present the results using the Interface de R pour les Analyses Multidimensionnelles de Textes et de Questionnaires - Iramuteq software (version 0.7 alpha 2) (Ratinaud, 2008/2023).
The prevalence of depression, anxiety, stress, and subjective distress symptoms was calculated as a point value with a 95% confidence interval (95%CI) and compared between the data collection phases (within each occupational group) using the z test (α =5%). The prevalence of usual (mean ≥ 3) coping strategies was also estimated and compared in the same way as described previously.
For each outcome (depression, anxiety, stress, and subjective distress), a multiple logistic regression model was developed: 0 = normal; 1 = mild, moderate, severe, or extremely severe distress taking into account gender [reference category (ref): man], presence/absence of a previous diagnosis of a mental disorder (ref: absent), occupational group [0 = professor (ref); 1 = student], and age. This analysis was performed separately for each phase of data collection. The odds ratio was estimated by point and 95%CI.
Participants voluntarily accessed the link to the survey and signed the informed consent form. The study followed the ethical guidelines of the National Health Council Decision 466/12 and 510/2016 and the guidelines of resolution No. 1/2021-CONEP/SECNS/MS on research in a virtual environment. This study was approved by the National Research Ethics Committee of the Ministry of Health (CONEP) (CAAE 30604220.4.0000.0008).
A total of 6,609 students (Phase 1 = 3,325; Phase 2 = 1,402; Phase 3 = 1,882) and 9,096 professors (Phase 1 = 3,924; Phase 2 = 2,223; Phase 3 = 2,949) participated in the study. Table 1 shows the characteristics of the sample. Of note is the higher prevalence of a previous diagnosis of a mental disorder reported by students compared to professors. There was also a significant difference in the prevalence of mental health changes reported by the two occupational groups since the onset of the pandemic, with students being more affected.
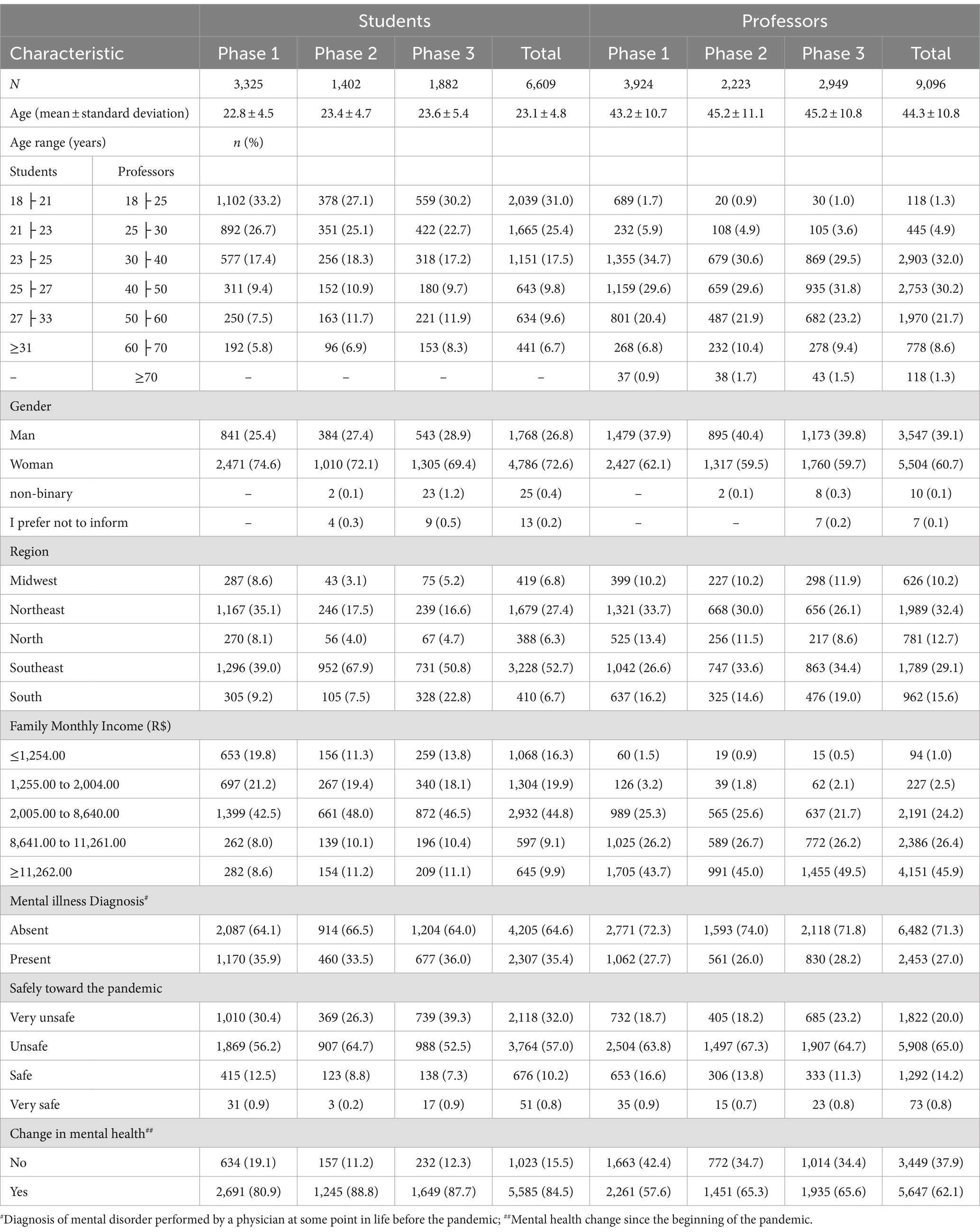
Table 1. Sample characteristics.
Depression, anxiety, and stress symptoms were significantly higher among professors who participated in Phase 3 than among those who participated in Phases 1 and 2, while subjective distress was lower in Phase 2 of the study (Table 2). Among students, the prevalence of depression and stress symptoms was higher in Phases 2 and 3, while anxiety was higher only in Phase 3. The prevalence of symptoms and distress was high in both occupational categories studied, but these were significantly higher among students (see Table 2; Figure 1A). Professors were more likely to use adaptive coping strategies in the face of the pandemic, such as AC, PL, RE, PR, and AT whereas students were more likely than professors to use maladaptive strategies (SD, BD, SU, DN) (Table 2; Figure 1B). The use of problem-oriented strategies such as AC, PL, and IS increased from Phase 1 to Phase 3, for both students and professors. Among professors, the prevalence of acceptance was lower and substance use was higher in Phase 3.
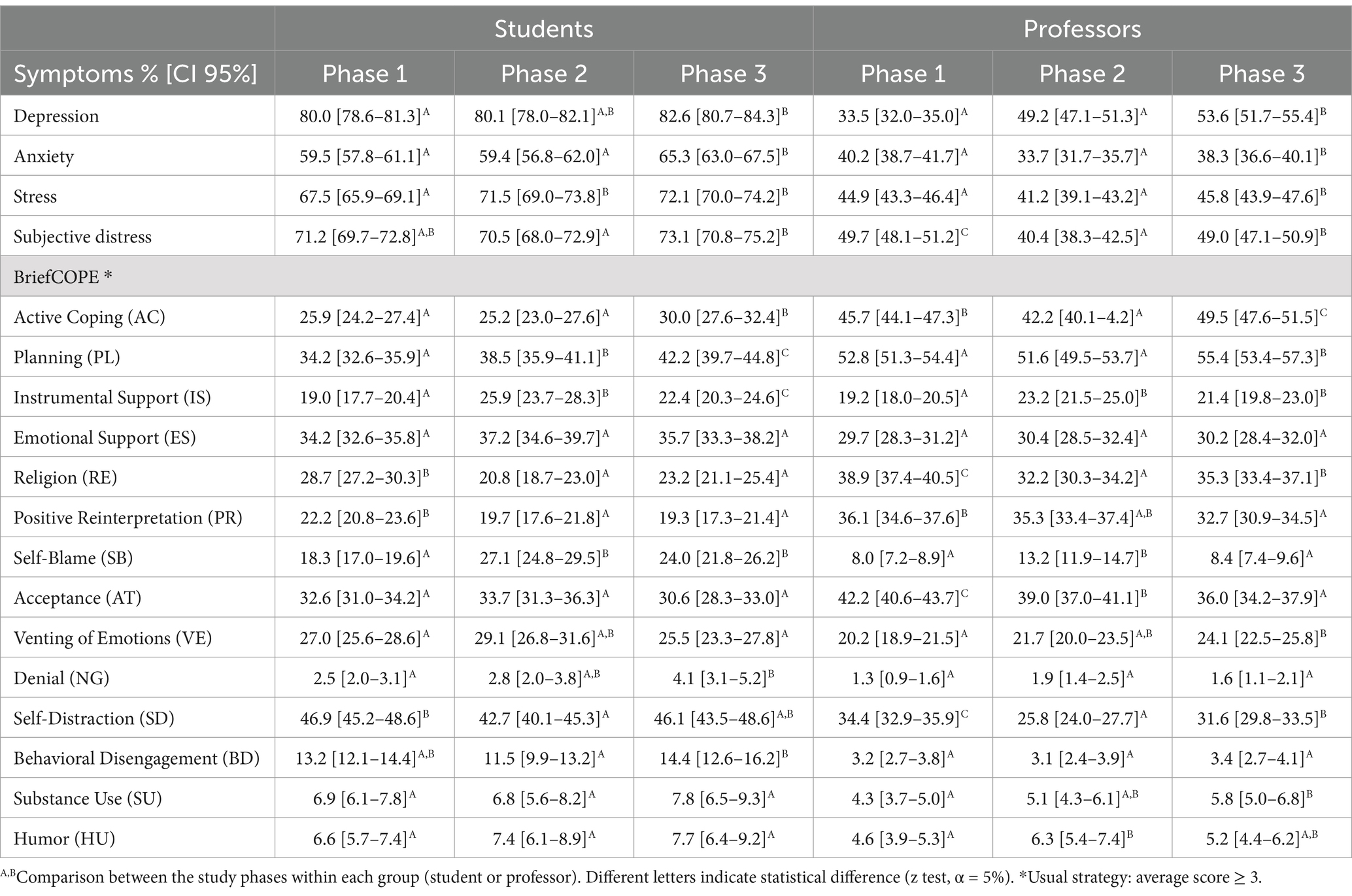
Table 2. Prevalence [p 95% (CI)] of depression, anxiety, stress and subjective distress symptoms, and usual coping strategies mentioned in BriefCOPE by students and professors at the different phases of data collection.
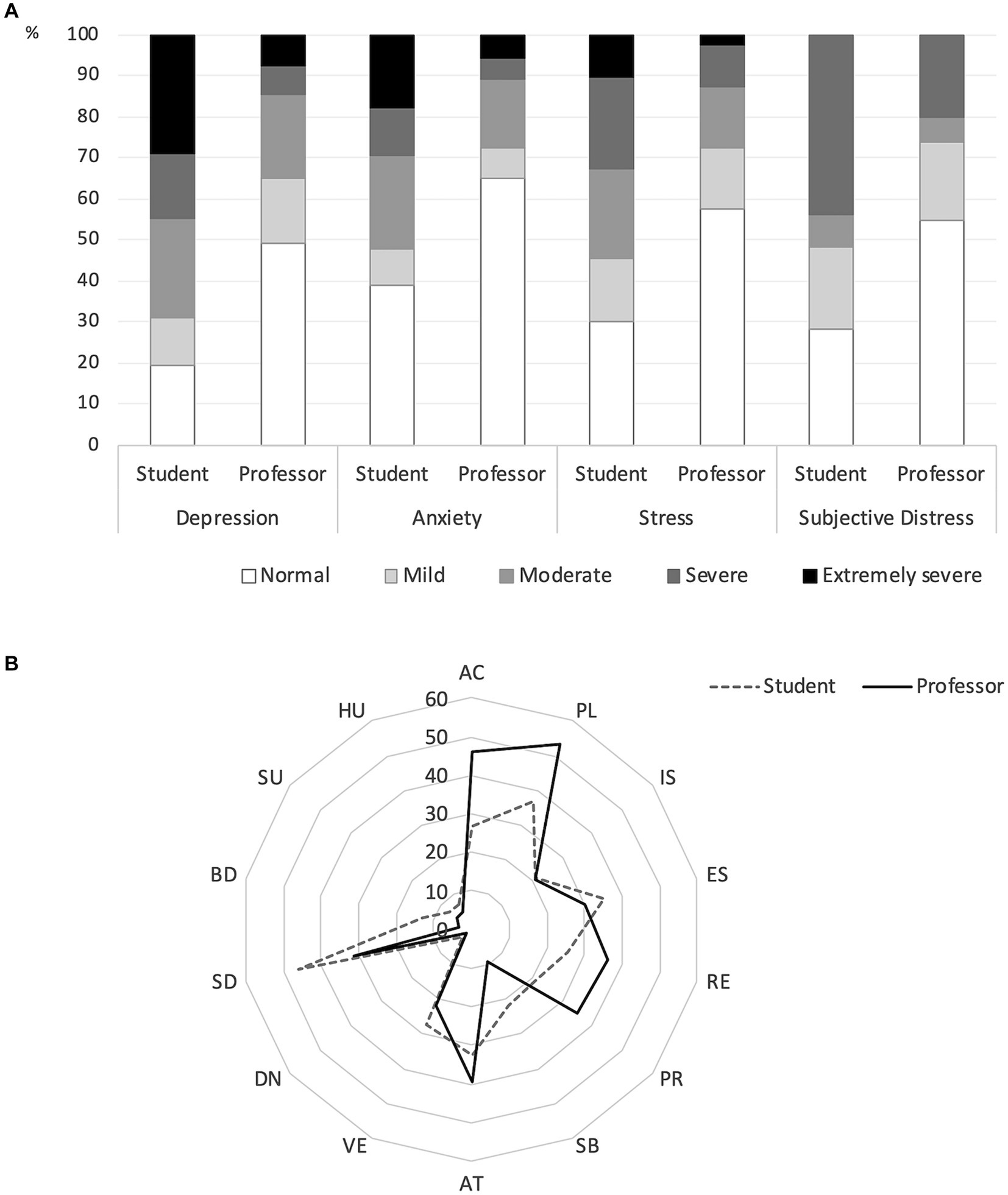
Figure 1. Distribution of students and professors according to the degree of being affected by symptoms of depression, anxiety, stress, and subjective distress (A) and according to the usual (mean ≥ 3) coping strategy (B), considering respondents of the three phases of the study (total sample). Radar radius = % of participants using the coping strategy habitually (mean ≥ 3). AC: Active coping; PL: Planning; IS: Instrumental support; ES: Emotional support; RE: Religion; PR: Positive reinterpretation; SB: Self-Blame; AT: Acceptance; VE: Venting of emotions; DN: Denial; SD: Self-Distraction; BD: Behavioral disengagement; SU: Substance use; HU: Humor.
The likelihood of experiencing symptoms of depression, anxiety, and subjective distress was significantly higher among students, women, and those with a prior mental disorder diagnosis. Age was inversely associated with the likelihood of symptoms/distress in the three study phases (Table 3). We clarify that age was included in the model, as it plays an important role in differentiating occupational categories and should therefore be considered.
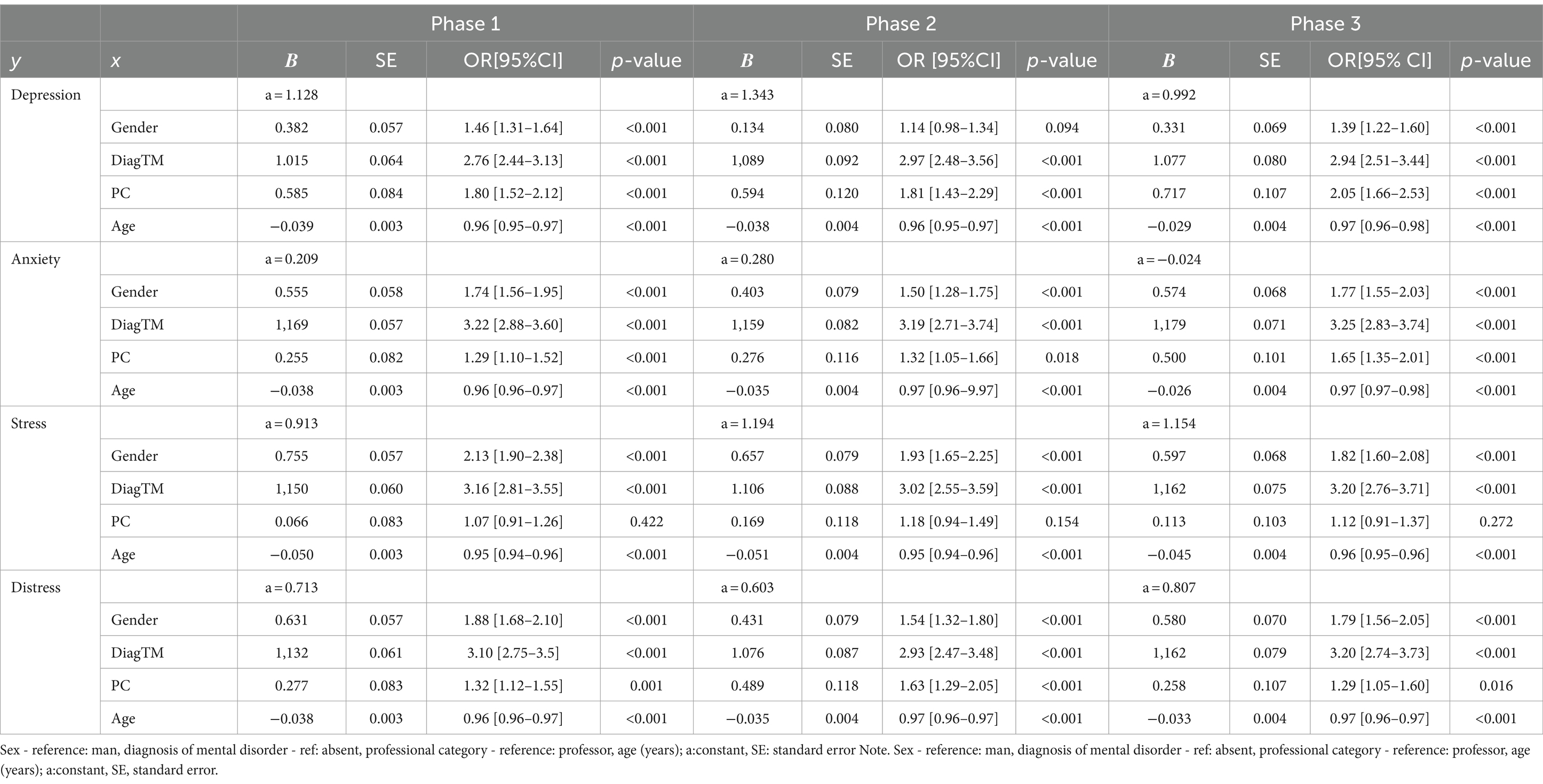
Table 3. Logistic regression model and odds ratio (OR) of symptom occurrence in relation to mental health according to sex, lifetime diagnosis of mental disorder (DiagTM), professional category (PC), and age.
The main concerns reported by students and professors regarding the pandemic suggest that the two occupational groups had distinct experiences. In the case of professors, the concerns originated from a single core, namely health concerns, from which branched out all other concerns from various spheres of life, particularly family (Figure 2). Conversely, we observed 3 cores among students: health, which branched out and two main groupings (see Figures 2A,B), family and COVID-19. From the health concern arose group A, which represents the uncertainty and spread of the pandemic (over time), while B is represented by more pragmatic concerns such as unemployment/employment, graduation/education, and money/finances. The family core (group C) is closely related to the health core and is mainly related to worries about the contagion/illness of a family member. The COVID-19 core (Group D) is closer to family than health and also reflects fear of contracting the virus and anticipation of vaccination.
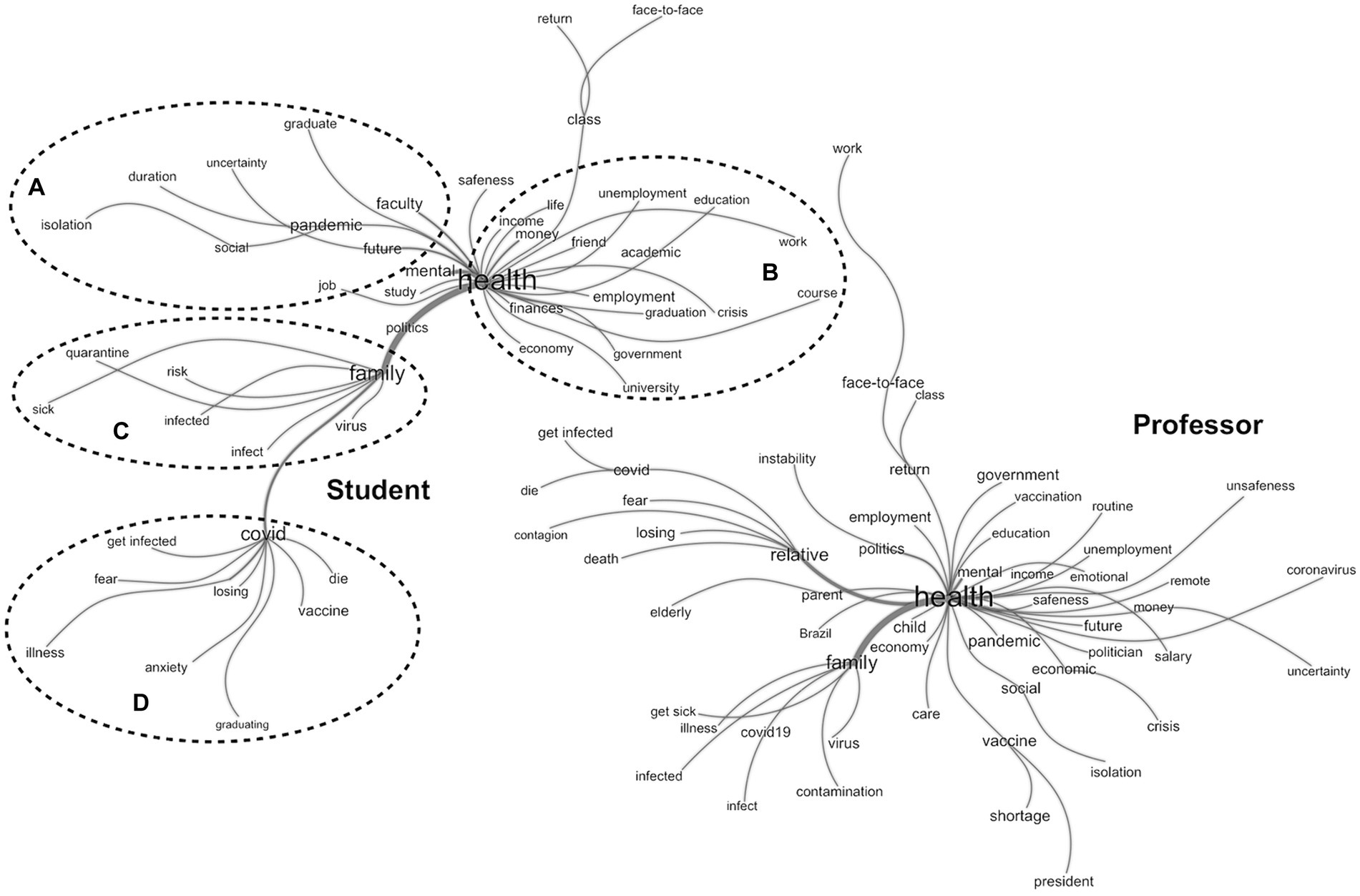
Figure 2. Similitude analysis of the main concerns of students and professors in the face of the pandemic. Student: 3 cores: health, which branched out and two main grouping (A,B), family (C) and COVID-19 (D). Professor: single core: health.
This study shows that students and professors experienced symptoms of depression (≥33%), anxiety (≥34%), and subjective distress (≥40%), at different times during the pandemic and used various coping strategies. We also found that students (OR = 1.29–2.05; p ≤ 0.001), women (OR = 1.39–2.13, p < 0.001), and those previously diagnosed with a mental health disorder (OR = 2.76–3.25, p < 0.001) were more likely to experience these symptoms. Additionally, our results indicated that professors are teaching young people who have been seriously impacted by the pandemic and require psychological support (e.g., conducting support or assistance actions, engaging in activities that help release tension, or practicing self-care). However, this is complicated by the fact that professors themselves were also experiencing symptoms and distress. Given these challenges, managers and educators need to focus their attention on the need to support mental health in the educational environment. Thus, the main objective of this study was to draw attention to this critical issue.
Tri Sakti et al. (2022) highlighted in a systematic review that the COVID-19 health crisis has had four main consequences on the school population: the major effects on mental health, the teaching-learning process, people’s quality of life, and physical health. The sudden disruption of the school ecosystem required rapid responses to the almost immediate and urgent application of distance education, which resulted in stress, anxiety, and uncertainty that accompanied the health crisis. This situation placed a significant cognitive burden on individuals across education systems and countries (Keržič et al., 2021). This overload led to increasing emotional exhaustion, triggering more or less severe symptoms depending on individual repertoires, social support, and contextual factors (Hadar et al., 2020; Pressley, 2021; Salmela-Aro et al., 2022).
Students are typically younger and tend to have less life experience and a smaller repertoire of coping strategies than older individuals. Due that, they rely more emotion-focused coping strategies or maladaptive strategies (see Figure 1B), which can contribute to the maintenance or exacerbation of symptoms (Restubog et al., 2020; Panayiotou et al., 2021). In addition, younger individuals were more likely to express their feelings as a coping strategy, which may have contributed to their more frequent reporting of affective symptoms. On the other hand, professors, being older, have a larger cognitive repertoire, which likely contributed to their more frequent use of adaptive coping strategies focused on problem solving, i.e., they used more planning and action skills to eliminate or overcome the daily effects of the pandemic. This leads to better cognitive restructuring of reality, better psychosocial adjustment, and consequently, lower prevalence of symptoms and distress (Lazarus and Folkman, 1984). Better coping and satisfaction with online classes were observed to be strong determinants of academic achievement among students from 10 countries around the world, which serves as a protective factor for health and physical and psychological well-being (Keržič et al., 2021).
The stage of life may be a factor that contributes to the experience of stress and mental health issues for students during the COVID-19 pandemic. The students who participated in the study were over 18 years of age, meaning that they either finished high school or were in various stages of higher education and thus in the process of defining a career and entering the labor market, whereas professors were already in a stable role. Career choice is a complex process and involves expectations and uncertainties. Harari (2018) warned that in the technological era, predictability in the labor market is no longer guaranteed, which increases the need for flexibility and adaptability to constant change. With the advent of the pandemic, the whole scenario of possibilities changed rapidly, and in the context of remote work, uncertainties about their choices and the future increased, which can be observed in our study (Figure 2). While for professors, health was the core of their concerns, which is contextual and to be expected once they were in a stable professional role, for students the core of concerns was divided into the uncertainties about the future on the one hand (Figure 2A Cluster) and the academic situation and employability on the other hand (Figure 2B Cluster). This scenario may have contributed to the higher prevalence of symptoms and distress among students, which is supported by the data in the Organization for Economic Cooperation and Development report (2021).
The sharp decline in spontaneous social interaction and the introduction of distance education are also important factors to be considered. According to Salmela-Aro et al. (2022) and Tonon (2021), the academic/school environment facilitates contacts and social interactions, providing opportunities to build networks and friendships and space for identity and institutional bonds. With the closure of schools/universities, student engagement in extracurricular activities and peer relationships declined significantly. For young people, this meant a disruption of important socialization rituals, a reduction in personal contact, and increased feelings of loneliness, stress, and burnout (Salmela-Aro et al., 2022). Population studies in the United States and New Zealand present data showing that the prevalence of loneliness among young people (18 to 25 years) has more than doubled since the onset of the pandemic (Organisation for Economic Co-Operation and Development, 2021). It is worth noting that distance education professors also report feelings of loneliness. Telyani et al. (2021) highlighted the relationship between professors’ loneliness and their performance, engagement, job satisfaction, and well-being, and showed that keeping students motivated and engaged in distance education was an arduous task for professors. In general, students and professors differ in terms of their social support network (instrumental and emotional), with professors having a more contextualized cognitive repertoire and coping strategies. Khan and Kadoya (2021) also point to the significant relationship between loneliness and depression and caution the need for interventions that can minimize harm to mental health.
As mentioned earlier, despite the lower prevalence of symptoms in professors than in students, this does not mean that they are low; on the contrary, the prevalence found is alarming and deserves attention (Table 2; 33.5–53.6%). Certainly, COVID-19 has profoundly changed the way education is practiced, requiring intense adaptation from those involved, often without institutional support or sufficient training. In addition, there are complicating factors, such as the enormous social and economic inequalities in the Brazilian population, which are even more evident in the face of distance education (Santos, 2020; Sousa and Coimbra, 2020), making the process more difficult. Some studies also suggest that although technological resources have allowed continuity in the communication process, they often create a distance between students and professors that affects social interaction and increases psychological fatigue (technostress: high level of psychophysiological activation; a set of symptoms associated with an excess of information and psychological demands) (Pinho et al., 2021), which can lead to physical and mental illness if not adequately managed. Our results show that the frequency of depression and stress symptoms (Table 2) significantly increased 18 months after the introduction of distance learning compared to the initial phases of the pandemic, both among students (depression: 80.0–82.6%; stress: 67.5–72.1%) and professors (depression: 33.5–53.6%; stress: 44.9–45.8%). Additionally, there was a significant increase in the prevalence of anxiety among students during this period (59.5–65.3%).
Regarding the fact that women (professors or students: OR = 1.39–2.13, p < 0.001) suffer more often from distress, we can support the following arguments: 1. women have more accentuated ruminative reactions than men, which can prolong anxiety and increase the impact of stressors on humor (Almeida and Kessler, 1998; Campos et al., 2020); 2. women take on multiple responsibilities and tasks and society expects them to try harder and make fewer mistakes than men (Foschi, 2000); and/or 3. men are encouraged to limit and hide their emotions (Chaplin, 2015). Certainly, other arguments can be used to explain the differences found between men and women; however, we presented only these three because this study was not designed to identify which of these arguments were involved in these results. Thus, these arguments are only speculation, and the reader should consider them cautiously.
Campos et al. (2021b) highlighted the greater vulnerability of people diagnosed with a mental disorder (the observed values in the results of the present study were OR = 2.76–3.25, p < 0.001), in which they reported that these people (1) may have greater emotional instability, (2) may have greater difficulty adapting quickly to changes in their routines, (3) may also have had a disruption in mental health care due to the pandemic, and (4) may have greater difficulty obtaining social support during isolation. Given the pronounced impact of this condition on symptoms and subjective distress, it is suggested that strategic care interventions be developed, such as support, counseling, intervention, and follow-up involving specialized professionals and promoting healthy lifestyles.
Given the data and arguments presented, we understand that educational systems need to strengthen their psychosocial support network and, in this direction, Hadar et al. (2020) recommend that professor education curricula, based on the COVID-19 experience, include the training and development of socio-emotional skills that they can use for themselves and students and others in the educational process for overall well-being. Among the possible techniques for developing these skills, the authors cite conducting case studies and teamwork on problems and challenges encountered in education during the pandemic, training in digital platforms and tools, presentation and familiarization with the topic of crisis management, and stress management techniques.
The first limitation of this study was the fact that it was part of a larger study, which made it impossible to obtain more detailed information about respondents’ job performance (e.g., for professors: number of hours/week worked, work experience, type of institution, and level of education in which they work; for students: course, period and level of the course, full-or part-time studies, screen time used in remote activities, among others), and therefore we recommend conducting future studies. Another limitation is the study design used (non-probability sample and online data collection), which may have limited access to the research for populations with lower levels of education and/or economic status, making it difficult to generalize the data.
A further limitation is that we conducted three independent and anonymous phases in the study, meaning that we cannot determine whether participants took part in just one phase or two or all three. We can also mention the significant decrease in the number of participants from the first to the subsequent phases. This may have occurred due to the increased online demands placed on people during the pandemic, which may have discouraged their participation after 6 and 12 months. However, given the pandemic scenario, this online strategy was feasible to collect information that would directly identify subjective distress in the population. Despite these limitations, we emphasize that there are still few studies in the literature that present data from students and professors at different times during the COVID-19 pandemic and that use large samples.
The prevalence of depression, anxiety, stress, and subjective distress symptoms was high among students and professors. Students, women, and those previously diagnosed with a mental disorder were more likely to have mental health symptoms or distress. During the pandemic, professors used more adaptive coping strategies than students. Health was the focus of professors’ concerns, while for students, future and labor market uncertainty were concerns derived from the health core. The results point to the need to strengthen psychosocial support for both professors and students.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by the National Research Ethics Committee of the Ministry of Health (CONEP) (CAAE 30604220.4.0000.0008). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
JC: Conceptualization, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Software, Supervision, Writing – original draft. LC: Conceptualization, Data curation, Funding acquisition, Investigation, Methodology, Validation, Visualization, Writing – original draft, Writing – review & editing. MA: Conceptualization, Investigation, Methodology, Writing – review & editing. BM: Conceptualization, Data curation, Funding acquisition, Investigation, Methodology, Writing – review & editing. BS: Conceptualization, Data curation, Funding acquisition, Investigation, Methodology, Writing – review & editing. JM: Conceptualization, Investigation, Software, Supervision, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was supported by grants #2020/08239-6 and #2021/03775-0, São Paulo Research Foundation (FAPESP); and the National Council for Scientific and Technological Development – CNPQ (#303118/2021-0).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. ^Phase 1: May 18 to June 23, 2020, COVID-19 total (n) cases: 1,228,114, total (n) deaths: 54,971; mean number of cases/day: 25,308.6, mean number of deaths/day: 996.2; phase 2: November 18 to December 23, 2020, n cases: 7,448,560, n deaths: 190,488, mean number of cases/day: 40,442.2, mean number of deaths/day: 626.0; phase 3: May 18 to June 23, 2021, n cases: 18,322,760, n deaths: 511,142, average cases/day: 68,342.8, average deaths/day: 1,912.9.
Almeida, D. M., and Kessler, R. C. (1998). Everyday stressors and gender differences in daily distress. J. Pers. Soc. Psychol. 75, 670–680. doi: 10.1037/0022-3514.75.3.670
American Psychiatric Association. (1980). Diagnostic and statistical manual of mental disorders: DSM-III. 3rd Edn. Washington, DC: American Psychiatric Publishing.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders: DSM-5. 5th edn. Washington, D.C.: American Psychiatric Publishing.
Azzi, D. V., Melo, J., Neto, A. A. C., Castelo, P. M., Andrade, E. F., and Pereira, L. J. (2022). Quality of life, physical activity and burnout syndrome during online learning period in Brazilian university students during the COVID-19 pandemic: a cluster analysis. Psychol. Health Med. 27, 466–480. doi: 10.1080/13548506.2021.1944656
Bernardo, K. A. S., Maia, F. L., and Bridi, M. A. (2020). As configurações do trabalho remoto da categoria docente no contexto da pandemia covid-19. Novos Rumos Sociol. 8, 8–39. doi: 10.15210/NORUS.V8I14.19908
Caiuby, A. V. S., Lacerda, S. S., Quintana, M. I., Torii, T. S., and Andreoli, S. B. (2012). Cross-cultural adaptation of the Brazilian version of the impact of events scale-revised (IES-R). Cad Saúde Pública 28, 597–603. doi: 10.1590/S0102-311X2012000300019
Campos, J. A. D., Campos, L. A., Bueno, J. L., and Martins, B. G. (2021a). Emotions and mood swings of pharmacy students in the context of the coronavirus disease of 2019 pandemic. Curr. Pharm. Teach. Learn. 13, 635–642. doi: 10.1016/j.cptl.2021.01.034
Campos, J. A. D., Campos, L. A., Martins, B. G., Valadao Dias, F., Ruano, R., and Maroco, J. (2021b). The psychological impact of COVID-19 on individuals with and without mental health disorders. Psychol. Rep. 125, 2435–2455. doi: 10.1177/00332941211026850
Campos, J. A. D. B., Martins, B. G., Campos, L. A., Marôco, J., Saasiq, R. A., and Ruano, R. (2020). Early psychological impact of the COVID-19 pandemic in Brazil: a national survey. J. Clin. Med. 9:2976. doi: 10.3390/jcm9092976
Carver, C. S. (1997). You want to measure coping but your protocol's too long: consider the brief COPE. Int. J. Behav. Med. 4, 92–100. doi: 10.1207/s15327558ijbm0401_6
Carver, C. S., and Scheier, M. F. (1981). Attention and self-regulation: A control-theory approach to human. New York: Springer-Verlag.
Carver, C. S., and Scheier, M. F. (1983). “A control-theory approach to human behavior, and implications for problems in self-management” in Advances in cognitive-behavioral research and therapy. ed. P. C. Kendal (New York: Academic Press), 127–194.
Carver, C. S., and Scheier, M. F. (1985). “Self-consciousness, expectancies, and the coping process” in Stress and coping. eds. T. Field, P. M. McCabe, N. Schneiderman, and T. M. Field (New York: Psychology Press), 305–330.
Carver, C. S., Scheier, M. F., and Weintraub, J. K. (1989). Assessing coping strategies: a theoretically based approach. J. Pers. Soc. Psychol. 56, 267–283. doi: 10.1037/0022-3514.56.2.267
Chang, J. J., Ji, Y., Li, Y. H., Pan, H. F., and Su, P. Y. (2021). Prevalence of anxiety symptom and depressive symptom among college students during COVID-19 pandemic: a meta-analysis. J. Affect. Disord. 292, 242–254. doi: 10.1016/j.jad.2021.05.109
Chaplin, T. M. (2015). Gender and emotion expression: a developmental contextual perpective. Emot. Rev. 7, 14–21. doi: 10.1177/1754073914544408
Folkman, S., and Lazarus, R. S. (1980). An analysis of coping in a middle-aged community sample. J. Health Soc. Behav. 21, 219–239. doi: 10.2307/2136617
Foschi, M. (2000). Double standards for competence: theory and research. Annu. Rev. Sociol. 26, 21–42. doi: 10.1146/annurev.soc.26.1.21
Hadar, L. L., Ergas, O., Alpert, B., and Ariav, T. (2020). Rethinking teacher education in a VUCA world: student teachers’ social-emotional competencies during the Covid-19 crisis. Eur. J. Teach. Educ. 43, 573–586. doi: 10.1080/02619768.2020.1807513
Harari, Y. N. (2020). Notas sobre a pandemia e breves lições para o mundo pós-coronavírus. São Paulo: Companhia das Letras.
Jorgensen, T. D., Pornprasertmanit Schoemann, S. A. M., and Rosseel, Y. (2022). semTools: useful tools for structural equation Modeling. Available at: https://cran.r-project.org/web/packages/semTools/index.html (Accessed February 08, 2022).
Keržič, D., Alex, J. K., Pamela Balbontín Alvarado, R., Bezerra, D. D. S., Cheraghi, M., Dobrowolska, B., et al. (2021). Academic student satisfaction and perceived performance in the e-learning environment during the COVID-19 pandemic: evidence across ten countries. PLoS One 16:e0258807. doi: 10.1371/journal.pone.0258807
Khan, M. S. R., and Kadoya, Y. (2021). Loneliness during the COVID-19 pandemic: a comparison between older and younger people. Int. J. Environ. Res. Public Health 18:7871. doi: 10.3390/ijerph18157871
Kivunja, C. (2015). Teaching students to learn and to work well with 21st century skills: unpacking the career and life skills domain of the new learning paradigm. Int J High Educ 4, 1–12. doi: 10.5430/ijhe.v4n1p1
Kline, R. B. (2023). Principles and practice of structural equation Modeling. 5th Edn New York: The Guilford Press.
Lazarus, R. S., and Folkman, S. (1984). Stress, appraisal and. New York: Springer Publishing Company.
Li, Y., Wang, A., Wu, Y., Han, N., and Huang, H. (2021). Impact of the COVID-19 pandemic on the mental health of college students: a systematic review and meta-analysis. Front. Psychol. 12:669119. doi: 10.3389/fpsyg.2021.669119
Lovibond, S. H., and Lovibond, P. F. (1995). Manual for the depression, anxiety, stress scales. Australia: Psychology Foundation Monograph.
Maroco, J., Campos, J. A. D. B., Bonafé, F. S. S., Vinagre, M. G., and Pais-Ribeiro, J. L. (2014). Adaptação transcultural Brasil-Portugal da Escala Brief COPE para estudantes do ensino superior. Psicol. Saúde Doenças 15, 300–313. doi: 10.15309/14psd150201
Martins, B. G., Silva, W. R., Maroco, J., and Campos, J. A. D. B. (2019). Depression, anxiety, and stress scale: psychometric properties and affectivity prevalence. J. Bras. Psiquiatr. 68, 32–41. doi: 10.1590/0047-2085000000222
Organisation for Economic Co-Operation and Development. (2021). Supporting young people’s mental health through the COVID-19 crisis. In: Tackling coronavirus (COVID-19) contributing to a global effort, Paris.
Ozamiz-Etxebarria, N., Idoiaga Mondragon, N., Bueno-Notivol, J., Perez-Moreno, M., and Santabarbara, J. (2021). Prevalence of anxiety, depression, and stress among teachers during the COVID-19 pandemic: a rapid systematic review with meta-analysis. Brain Sci. 11:1172. doi: 10.3390/brainsci11091172
Panayiotou, G., Panteli, M., and Leonidou, C. (2021). Coping with the invisible enemy: the role of emotion regulation and awareness in quality of life during the COVID-19 pandemic. J. Contextual Behav. Sci. 19, 17–27. doi: 10.1016/j.jcbs.2020.11.002
Pinho, P. S., Freitas, A. M. C., Cardoso, M. C. B., Silva, J. S., Reis, L. F., Muniz, C. F. D., et al. (2021). Remote teaching work and health: repercussions of new requirements in the context of the Covid-19 pandemic. Trabalho Educ Saúde 19:e00325157. doi: 10.1590/1981-7746-sol00325
Pressley, T. (2021). Factors contributing to teacher burnout during covid-19. Educ. Res. 50, 325–327. doi: 10.3102/0013189X211004138
R Core Team. (2022). R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria. Available online at: https://www.R-project.org/ (Accessed March 30, 2024).
Ratinaud, P. (2008/2023). IRAMUTEQ: Interface de R pour les Analyses Multidimensionnelles de Textes et de Questionnaires.
Restubog, S. L., Ocampo, A. C., and Wang, L. (2020). Taking control amidst the chaos: emotion regulation during the COVID-19. J. Vocat. Behav. 119:103440. doi: 10.1016/j.jvb.2020.103440
Rosseel, Y. (2012). Lavaan: an R package for structural equation modeling and more. J. Stat. Softw. 48, 1–36. doi: 10.18637/jss.v048.i02
Salmela-Aro, K., Upadyaya, K., Ronkainen, I., and Hietajarvi, L. (2022). Study burnout and engagement during COVID-19 among university students: the role of demands, resources, and psychological needs. J. Happiness Stud. 23, 2685–2702. doi: 10.1007/s10902-022-00518-1
Scheier, M. F., and Carver, C. S. (1988). “A model of behavioral self-regulation: translating intention into action” in Advances in experimental social psychology. ed. L. Berkowits (New York: Academic Press), 303–346.
Silva, D. F. O., Cobucci, R. N., Lima, S., and de Andrade, F. B. (2021). Prevalence of anxiety, depression, and stress among teachers during the COVID-19 pandemic: a PRISMA-compliant systematic review. Medicine (Baltimore) 100:e27684. doi: 10.1097/MD.0000000000027684
Sousa, A. P. R., and Coimbra, L. J. P. (2020). A educação e as novas tecnologias de informação e comunicação no contexto da pandemia do novo coronavírus: o professor "R" e o esvaziamento do ato de ensinar. Rev. Pedag. Cotidiano Ressign. 1, 53–72.
Telyani, A., Farmanesh, P., and Zargar, P. (2021). The impact of covid-19 investigated changes on loneliness of teachers and motivation-engagement of students: a psychological analysis of education sector. Front. Psychol. 12, 1–6. doi: 10.3389/fpsyg.2021.765180
Tonon, G. H. (2021). Student’s quality of life at the university: a qualitative study. Appl. Res. Qual. Life 16, 1517–1535. doi: 10.1007/s11482-020-09827-0
Tri Sakti, A. M., Mohd Ajis, S. Z., Azlan, A. A., Kim, H. J., Wong, E., and Mohamad, E. (2022). Impact of COVID-19 on school populations and associated factors: a systematic review. Int. J. Environ. Res. Public Health 19:4024. doi: 10.3390/ijerph19074024
Wang, C., Pan, R., Wan, X., Tan, Y., Xu, L., Ho, C. S., et al. (2020). Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 17:1729. doi: 10.3390/ijerph17051729
Wang, C., Wen, W., Zhang, H., Ni, J., Jiang, J., Cheng, Y., et al. (2021). Anxiety, depression, and stress prevalence among college students during the COVID-19 pandemic: a systematic review and meta-analysis. J. Am. Coll. Heal. 71, 2123–2130. doi: 10.1080/07448481.2021.1960849
Watson, D., Weber, K., Assenheimer, J. S., Clark, L. A., Strauss, M. E., and McCormick, R. A. (1995). Testing a tripartite model: I. Evaluating the convergent and discriminant validity of anxiety and depression symptom scales. J. Abnorm. Psychol. 104, 3–14. doi: 10.1037/0021-843X.104.1.3
Keywords: mental health, university, students, professors, pandemics
Citation: Campos JADB, Campos LA, Azevedo MAR, Martins BG, Silva BNS and Marôco J (2024) Mental health in times of pandemic from the perspective of professors and students. Front. Educ. 9:1353756. doi: 10.3389/feduc.2024.1353756
Edited by:
Laisa Liane Paineiras-Domingos, Federal University of Bahia (UFBA), BrazilReviewed by:
Anna Parola, Department of Humanities, University of Naples Federico II, ItalyCopyright © 2024 Campos, Campos, Azevedo, Martins, Silva and Marôco. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lucas Arrais Campos, bHVjYXMuYXJyYWlzZGVjYW1wb3NAdHVuaS5maQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.