 Lauren Haire
Lauren Haire Jennifer Symonds1*
Jennifer Symonds1*- 1School of Education, University College Dublin, Dublin, Ireland
- 2University of Reggio Calabria, Reggio Calabria, Italy
The construct of pathological demand avoidance (PDA) is relatively new and contested. Clinical reports indicate a population who obsessively resist everyday demands and have an extreme need for control. Children and adolescents who might experience PDA, and their families, struggle significantly in their daily lives, creating a need for more research into the phenomenon. To assist the developing research field, this scoping review focuses on the methodologies used to study PDA in children and adolescents. A systematic search of six databases and grey literature uncovered 57 unique records after duplicates were removed. 21 documents containing 22 studies were retained for analysis. Of the 22 studies, 21 were from the UK and one was from the Faroe Islands. There were 18 quantitative analyses and 11 qualitative analyses. Half of the studies were cross-sectional and quantitative and almost half used mixed methods. Samples were non-representative and studies often used comparison groups of children with and without PDA. Researcher’s conceptualizations of PDA were coded into categories of emotional, socio-cognitive, and neurological differences. Studies of PDA focused mostly on PDA symptoms, mechanisms, and precipitants, with fewer studies of PDA origins and problems resulting from PDA or possible supports for individuals. The EDA-Q and the DISCO were the main measures used to identify PDA. Quantitative data were often analyzed using inferential statistics, and qualitative data were analyzed using thematic analysis, content analysis, and narrative summaries. Implications for future research are discussed.
Introduction
The construct of Pathological Demand Avoidance (PDA) reflects a presentation characterized by extreme avoidance of everyday and ordinary demands firstly conceptualized as a distinct developmental disorder and since primarily studied in autistic children and adolescents. The construct is controversial and does not exist in diagnostic manuals such as the DSM-V or ICD-11 upon which clinicians rely. No consensus exists as to the diagnostic validity of PDA, its features, or its relationship with other known constructs in childhood disability. Nevertheless, the experience of living with those who present demand avoidant behaviors appears to present as problematic for children and their families, meaning families seek support. However, the level of debate that exists around PDA means information on robust research methods is lacking, as is evidence-based clinical guidance. To date, interest and research in PDA has been predominantly confined to the UK.
Origin of PDA
The concept of PDA emerged in the 1970s when a clinician, Elizabeth Newson found children referred to her clinic for autism assessment resembled autistic children but were different from them and similar to each other. Newson and colleagues developed a set of criteria describing these children, the central feature being a need to avoid everyday demands to reduce anxiety, using social manipulation as a key strategy (Newson et al., 2003). If avoidance strategies failed, extreme emotional responses were observed, understood by clinicians as akin to a panic attack. Additional characteristics comprised a reserved nature during the initial year, leading to subsequent disparities in communication, especially in language comprehension. Individuals displayed a sociable demeanor yet lacked a strong sense of self-identity, pride, or shame. They exhibited rapid mood swings driven by a desire for control, showed ease in engaging in role-playing activities, and frequently demonstrated obsessive behaviors, often centered around social interactions. Additionally, neurological traits such as clumsiness were frequently observed. Not all features were said to be required for identification of PDA. Because of the differences with autistic children, e.g., higher sociability and differences in play and language profiles, Newson felt autism, based on DSM-IV criteria was contraindicated. Instead, she conceptualized PDA as a potential subgroup within her own version of pervasive developmental disorders.
Newson’s work carried important clinical and social implications. Newson noted that children meeting the PDA criteria would have previously been identified as atypically autistic, a category from the ICD-10 which she deemed as unhelpful in accessing appropriate support. Importantly, Newson reported that children with PDA needed different supports to autistic children, going as far as to say ‘if [PDA is] perceived as autism, the wrong advice will be given’ (Newson et al., 2003, p. 596). Newson advocated for approaches based on novelty, humor, and variety and not on compliance.
Aligned with Newson’s observations that children exhibit challenging features even within autism services, Gore Langton and Frederickson (2016) assert that success in schools is contingent upon staff flexibility rather than access to more specialized provisions, such as autism classes. Contrary to the structured and repetitive approaches rooted in the principles of Lovaas (1987) and Kunce and Mesibov (1998), which have historically dominated education for autistic individuals (Moore, 2020), Newson advocates for a different approach. Recent research (e.g., Gore Langton and Frederickson, 2018; Ozsivadjian, 2020) and practitioner insights (e.g., Fidler and Christie, 2019) support Newson’s approach, which places anxiety as a central driver (O'Nions and Eaton, 2020). For parents whose children do not thrive under traditional autism interventions, Pathological Demand Avoidance (PDA) offers a significant recognition factor and a roadmap for more tailored support (Gore Langton and Frederickson, 2018). Despite similarities noted between PDA and conduct disorder, children continue to struggle even in schools designed to address emotional and behavioral difficulties (Gore Langton and Frederickson, 2016). Moreover, Newson’s conceptualization has been criticized for including criteria that are conceptually very different, ranging from observable behaviors, assumptions about behavioral intentionality, and assumed causes (i.e., neurological involvement; cf. Kildahl et al., 2021).
Rationale for identified PDA
Regardless of approach used, the presentation as described by Newson means children are very likely to find educational settings challenging. Avoidance of typical demands alongside a lack of identity, pride or shame coupled with extremes of mood and need to be in control (Newson et al., 2003) may be met with unsympathetic approaches in schools. In this context, “identity” refers to a sense of self-awareness and understanding of one’s own traits, characteristics, and individuality. When discussing the lack of identity in individuals with PDA it implies a difficulty in forming a cohesive sense of self or a distinct personal identity. This lack of identity can manifest as an uncertainty about one’s own preferences, interests, or values. Schools also have been primarily compliance-based systems where compliance in PDA may be perceived as giving up control likely to provoke anxiety. Thus, features of compliance-based systems such as use of rewards are reportedly unhelpful in PDA (Eaton and Weaver, 2020). Families of and individuals with PDA report a lack of understanding and lack of appropriate support in education resulting in high rates of exclusion and placement moves, high professional involvement and poor mental health for parents and children (Gore Langton and Frederickson, 2016; Truman et al., 2021; Doyle and Kenny, 2023).
Parental blame and reference to poor parenting skills is often associated with school-related demand avoidance (Doyle and Kenny, 2023), with Gore Langton and Frederickson (2018) likening this to blame parents of autistic children have experienced (e.g., Jacobs et al., 2018). Such experiences mean parents are likely forced to seek any available supports for their children. National and regional societies for autistic people in the UK have supported parents (O'Nions et al., 2014a), many of whom seek identification of PDA (Green et al., 2020; Truman et al., 2021) as a path to appropriate support (Gore Langton and Frederickson, 2018). However, authors highlight that clinicians differ in their willingness to identify PDA (O’Nions et al., 2014b). Researchers reveal the resulting power imbalance at play. Since diagnostic practices vary significantly, Woods (2017) highlights the role of private providers in addressing the diagnostic gap for identifying PDA, noting that they often charge families in crisis substantial amounts of money. This practice exacerbates the financial burden on families already facing difficulties, further underscoring the challenges associated with accessing timely and affordable diagnostic services (Moore, 2020). Moreover, a different perspective is that vulnerable individuals are unjustly placed in situations where their support packages may be disregarded due to the contested nature of PDA. This occurs because there are various clinical approaches to addressing PDA, rather than attributing it directly to individuals (Green et al., 2018a). Anecdotal reports indicate at least some instances where children have been excluded from educational plans due to PDA attribution. This raises questions about diagnostic practices and implications for access to support services, underscoring the need for a more nuanced and contextual approach in the assessment and intervention for those who may be affected by this condition.
Empirical and conceptual issues
Despite the social interest and utility of PDA for families, there remains no consensus on the validity of PDA which likely further impacts upon children who evidently struggle to access education. There is also no agreement as to what constitutes as PDA, what the features are or its relationship with other known constructs. Several debates exist in the literature.
PDA within autism
In the time since Newson’s work, the DSM has progressed to its fifth version, within which, the category of pervasive developmental disorder is no longer used. Thus, some now see pervasive developmental disorder and autism as synonymous, understanding the features of PDA as fitting within the widened DSM-V criteria for autism (Christie, 2007). Woods (2021b) highlights that some features of PDA originally described by Newson were removed in keeping with this narrative (O’Nions et al., 2016).
Many studies have examined PDA within autistic individuals. Gillberg et al. (2015) prevalence study suggests up to one in five autistic people may experience PDA. Aligned with autism, children with PDA appear to have differences in social communication and specific and intense interests and preferences but differ on some counts, children with PDA show higher emotionality, resist demands, control others using manipulation, engage in more imaginative play and prefer novelty, spontaneity, and humor (O’Nions et al., 2014b; O'Nions et al., 2018b; Eaton and Weaver, 2020; Stuart et al., 2020). Eaton and Weaver (2020) demonstrated that differences between autism and PDA can be observed via the Autism Diagnostic Observation Schedule second version. In samples of autistic children, international scholars have also observed children avoiding ordinary tasks experienced as aversive (e.g., Lucyshyn et al., 2015).
Certain UK national charities support PDA as a feature of autism, with many conferences oversubscribed (Trundle et al., 2017). Recent guidance published outlines how to identify and assess for PDA within autism, according to a group of 12 clinicians (PDA Society UK, 2022). Calls exist for PDA to be included in diagnostic manuals. Fidler and Christie (2019) note that attention needs to be paid to the utility of diagnostic classifications for practitioners, which Astle et al. (2019) note are relatively ineffective in predicting how a child presents. While there is no indication that PDA will be included in future diagnostic manuals, Grahame et al. (2020) seek to provide information for clinicians, noting classification systems are of their time and thus PDA may yet earn a place. The authors highlight the collaboration of clinical populations with clinicians is not an unusual method by which phenomena go from being first considered to eventually formalized as categories in the DSM or ICD, thus dispelling concerns regarding the circularity of PDA research (Green, 2020).
Moreover, some authors query the position of PDA as being confined to autism. They argue the need for control evident in PDA cannot explained by theories of autism (O'Nions, 2013, chapter 4). Awareness of others mental states to ‘manipulate’ is also noted to conflict with understanding of autism. Woods (2022a) queries if it is helpful to have features such as manipulation attributable to autism. O’Nions et al. (2016) and O'Nions et al. (2018a) since found that the spontaneity and increased imaginative play hypothesized by Newson to exist in PDA could not be replicated. Woods (2022a) notes that since there are key features of PDA which do not exist in the criteria for autism, e.g., anxiety, PDA cannot be considered as representing autism. Others point to evidence that PDA features have been shown to exist outside of autism (e.g., Gillberg et al., 2015). Authors point to the differing gender balance apparent in autism compared to in PDA. Newson and O’Nions et al. (2021) describe PDA occurring in a similar number of females to males, while the ratio of autism is understood to be one female to three males (Loomes et al., 2017). However, this may be an underestimation as it is acknowledged females have been at risk of not being identified as autistic (Hull et al., 2020). Some query if PDA is a female presentation of autism (O'Nions, 2013, chapter 4). Clearly, the positioning of PDA within autism is not without difficulty.
The need for different approaches in PDA and autism has been used as justification for a new category. Woods (2019), refutes this position, instead, highlighting that the approaches described as helpful in PDA are likely to be useful in all neurodivergent populations. Mols and Danckaerts (2022) support Woods, noting PDA approaches are likely common practice and highlight that differential treatment approaches appear to be based solely on clinical impression. Authors point to what they perceive as the misinterpretation of the avoidance of demands. Kildahl et al. (2021) notes that importantly, what we know about autistic people avoiding demands is based on the report of others, who may not be autistic themselves. Using the lens of critical autism scholars, Milton (2013) recognizes that what are perceived as non-threatening demands to neurotypical people, may be experienced that way by autistic people who have different experiences. Similarly, the terms rational demand avoidance (Milton, 2017; Woods, 2018; Moore, 2020) or pervasive drive for autonomy (Wilding and Griffey, 2015) have been used, reflecting the avoidance of demands as rational for autistic people, who need autonomy to feel safe in a world which may not be set up for them.
O'Nions and Eaton (2020) highlight a misinterpretation of the need to avoid demands is reflected in the language used to describe children. The authors note what was previously described as ‘manipulation’ by individuals experiencing demand avoidance, could be reframed with more compassion as the use of a social strategy, to maintain much needed autonomy. Supporting Milton’s view, Moore (2020) highlights further the PDA label makes autistic people vulnerable to be pathologised when avoiding demands which are overwhelming to them. The misinterpretation reflects a lack of attention given to the subjective perspective, and to the transaction between children and the context in which they seek to avoid demands (Milton, 2017; Green et al., 2018b; Woods, 2022a). Aligned with the social model of disability, a transactional model explores explanatory factors in the child’s environment when demands exceed coping ability, rather than a deficit within the child.
Critical of the supporting evidence underpinning PDA, Kildahl et al. (2021) query the potential of using existing categories, e.g., anxiety disorders to convey experience of high anxiety or trauma in autistic people. The authors highlight that if different labels, e.g., PDA are used to describe similar experiences such as anxiety in autistic, and non-autistic people then this may ‘obscure the commonality of experience’ (p. 2173). The authors point out that this is not likely to result in a more inclusive community or reduce the impact of the double empathy problem (Milton, 2012). Similarly, Woods (2020) highlights that significant work was undertaken by autism advocates to remove subtypes in the revision of the DSM, aiming to unite autistic individuals rather than separate them (Happé, 2011).
PDA within other known disorders
Outside of autism, similarities have been drawn between PDA and other disorders. Gillberg et al. (2015) notes PDA could occur in language disorders, ADHD, ODD or autism or it may represent a unique phenotype. Overlap exists between conduct disorder (CD) and oppositional defiance disorder (ODD) and PDA (O’Nions et al., 2014b; Green et al., 2018b). However, children with PDA show resistance to demands and need to control others, resorting to what might be construed as embarrassing lengths, in a way that those with CD/ODD do not (O'Nions, 2013, chapter 8). Some authors note that since the approaches in conduct disorder and PDA differ, seeing PDA as a conduct disorder is unlikely to be helpful to children as it may lead to use of reward-consequence approaches, likely to increase anxiety (O'Nions et al., 2018a).
O’Nions et al. (2014b) also compared PDA with those with callous unemotionality. They noted children with PDA experienced higher emotionality. Egan et al. (2020) and Trundle et al. (2017) demonstrate that when using adult self-report, there is a role for personality traits (e.g., antagonism and emotional instability) and ADHD in predicting a PDA presentation. Milton (2017) notes the role of attachment difficulties and trauma; however, Eaton and Weaver (2020) illustrate that when comprehensive developmental histories are taken, PDA can be differentiated from attachment difficulties. Several authors have been concerned with the link between PDA and anxiety (e.g., Stuart et al., 2020) and Soppitt (2021) refers to the role of sensory processing.
PDA as a collection of disorders
Others view PDA as a collection of features occurring across categories, noting the co-occurrence of many other disorders with autism (Green et al., 2018b). Importantly, authors note that co-occurring difficulties may present uniquely in autism (Woods, 2022a). Indeed, the DSM-V recommends that non-autism features should be noted during assessment (American Psychiatric Association [APA], 2013). Authors have described PDA as a double (O'Nions, 2013, chapter 8; Wing et al., 2011), triple (Gore Langton and Frederickson, 2016) or multiple hit (O'Nions, 2013) involving autism, ODD, ADHD, autism, anxiety and/or other emotional problems. O'Nions (2013) cautions that though the phenotype is similar, the underlying mechanisms may be different and thus warrant different approaches.
PDA as a distinct entity
Some still feel PDA represents a standalone entity owing to the key differences observed between it and other disorders. Woods (2022b) notes people without autism who experience demand avoidance also have equal rights to diagnoses, research, and support. He acknowledges there is a clinical need for a standalone entity, using the terminology of demand avoidance phenomena (DAP) (Woods, 2021a). He outlines comprehensively how DAP meets the criteria for inclusion within the obsessive compulsive and related disorders in the DSM-5 (Woods, 2022c). In Green’s analysis from 2020, it’s observed that the reliance on circular reasoning up to the present indicates a dearth of evidence supporting the independent existence of PDA. This suggests that the arguments made so far have been self-referential or circular in nature, rather than providing solid evidence for the standalone existence of PDA.
Methods of studying PDA
Issues to date
A key problem is that Newson’s original study, where the criteria for PDA were first developed, has been highly criticized for use of circular reasoning and overinterpretation. Authors note Newson first defined the groups in her study, and then studied them (Green et al., 2018b). O'Nions and Eaton (2020, p. 411) describe Newson’s sample as having a ‘collider bias’, meaning the important recognition factor for parents reported by Newson represented confirmation bias (Mols and Danckaerts, 2022). The reliance on Newson and colleagues study is problematic when one considers that many subsequent studies (e.g., Gore Langton and Frederickson, 2016; Egan et al., 2020) use measures such as the Extreme Demand Avoidance Questionnaire (EDA-Q) which is based on features described in their seminal paper (O'Nions et al., 2014a). The EDA-Q and the Diagnostic Instrument for Social and Communication Disorder (DISCO), though both shown to be internally reliable, have not yet been further validated. Of note, there are different cut-off values for the DISCO in use across studies (Gillberg et al., 2015; O’Nions et al., 2016). Additionally, the refined EDA-8, containing items shown to be most consistent in PDA, has not yet been tested in clinical settings.
Further difficulties have been raised in relation to the conceptualization of PDA as a developmental disorder which is pervasive in nature. The longevity of the presentation has been called into question, with recent studies demonstrating PDA features decrease in adulthood (Stuart et al., 2020). Additionally, problematic, the category of pervasive developmental disorder, which is said to include PDA, has become synonymous with autism owing to changes in the DSM, thus, many studies investigate PDA within autistic people. Critics argue that automatically subsuming PDA within autism conflicts with Newson et al. (2003) early work which indicated PDA was not autism (Woods, 2022c). Further contributing to bias in the PDA literature, authors note that some studies used overlapping samples recruiting through similar channels, e.g., Newson’s clinic, the PDA Society UK and PDA conferences (Kildahl et al., 2021). No agreement appears to exist regarding the sample for inclusion when studying PDA. Finally, Newson proposed to have biological or genetic origin, however currently, evidence of biological or genetic origin for mental disorders remains lacking.
Variety of methods
Lack of consensus regarding operationalization of PDA, its features, their stability over time, and subsequent validation means methods of studying are inconsistent. An overview of the existing research on PDA indicates quantitative and qualitative methods have been used. Of those studies, some require diagnosis of PDA for inclusion, and many allow parent identification. Some used play-based observation (Eaton and Weaver, 2020).
There are fewer qualitative studies and, as in studies of young autistics (e.g., Fayette and Bond, 2018), few have included the voice of the young person with PDA, despite the benefits of voiced research being well documented (Cunningham, 2022). Egan et al. (2020) showed that inclusion of the PDA voice is challenging even with adults, owing to their difficulty engaging with demands. Communication differences between autistic and non-autistic people, and differences in how emotional experiences are conveyed (Hollocks et al., 2019) may be compounding the difficulty with inclusion of those with PDA in research. Identifying ways to communicate with the PDA population is a worthwhile endeavor to increase research reliability and validity and warrants attention.
The current study
This scoping review which synthesizes existing methods of studying PDA in children and adolescents is needed to inform research and practice on a presentation which lacks formal recognition. The review will help researchers make evidenced-based decisions about how to operationalize and collect information on PDA. The current deliberation in the literature has significant impact on supports for those affected (Gore Langton and Frederickson, 2016). More information on PDA is of clear value to identify “origin, genetics, correlates, developmental course and… interventions… to reduce distress” (Grahame et al., 2020, p. 77). Reliable methodological approaches can be identified through this scoping review.
Objectives
The aim of this scoping review is to synthesize the methods for studying PDA in children and adolescents, to inform educational psychology. The protocol for this scoping review (Haire and Symonds, 2021) was registered on psyarxiv.com. An initial search of the literature determined a scarcity of empirical studies and only two existing systematic reviews of PDA. Kildahl et al. (2021), in their systematic review of 13 studies assessed how PDA is identified, and its relationships with neurodevelopmental disabilities and mental health presentations such as anxiety and trauma. Authors noted the relationship between PDA and neurodevelopmental disabilities and PDA and mental health presentations is unclear and there remains a need for more robust methods to be used to establish these relationships. Mols and Danckaerts (2022) reviewed 26 articles and noted the existence of PDA as a feature of autism, a co-occurrence with autism or a distinct entity is unclear, the authors reveal difficulties in operationalization of the construct and agreement on its criteria as key issues. One additional overview of empirical work was supplied by O'Nions and Eaton (2020) aiming to address the gap in clinical guidance, but the methods used are unclear. A scoping review methodology was selected to provide the field with information on foundational procedures. Scoping reviews support broad topics where many different study designs are applicable and include studies of varying quality suitable for exploratory research questions (Arksey and O'Malley, 2005). Adhering to the scoping review method as defined by Colquhoun et al. (2014), means this review uses systematic search techniques to map key concepts, evidence, and gaps in methodologies.
Research questions
The overarching research question guiding the review is what are the methodologies of studies of PDA in children and adolescents? This was answered by the following secondary research questions:
1. In accordance with Beck’s (1979) case formulation framework, what is the focus of the studies?
2. How is PDA in children and adolescents conceptualized in studies?
3. What type of samples of children and adolescents are used in studies of PDA?
4. What quantitative methods are used to study PDA in children and adolescents?
5. Given the available evidence, how reliable are the quantitative tools used to study PDA in children and adolescents?
6. What qualitative methods are used to study PDA in children and adolescents?
7. Given the available evidence, how trustworthy are the qualitative tools used to study PDA in children and adolescents?
Methods
Arksey and O'Malley’s (2005) framework provides a clear structure to enable an iterative, rigorous, and reproducible process in scoping reviews: (a) identifying the research question, (b) identifying studies, (c) selecting studies, (d) charting and collating data and (e) disseminating and reporting results. The framework was adapted by the Joanna Briggs Institute (Peters et al., 2015) and in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) extension checklist for scoping reviews (PRISMA-ScR) (Tricco et al., 2018). There is no PRISMA-P (protocol) checklist for a scoping review, thus the PRISMA-P for systematic reviews (Moher et al., 2015) was adapted for use.
Selection criteria
Studies of all designs written in English were included if they focused on the construct of PDA in children (2.5 to 9 years) and/or adolescents (10 to 18 years). Non-English language papers were documented (with accurate translations). Published or unpublished studies since the origins of PDA were included. To maintain a high standard of scientific quality, studies must be peer reviewed, thus doctoral dissertations reviewed at viva were included. The age range was selected based on the average age autism is first identified (van’t Hof et al., 2021) and the end of adolescence. Studies focusing on another related and named disorder, e.g., conduct disorder or autism were excluded unless they were also of pathological or extreme demand avoidance.
Search strategy
The first and second author designed the search strategy. The first author comprehensively searched databases to identify studies for inclusion as per Figure 1, documenting details in Microsoft Excel. Results were exported into EndNote and duplicates removed.
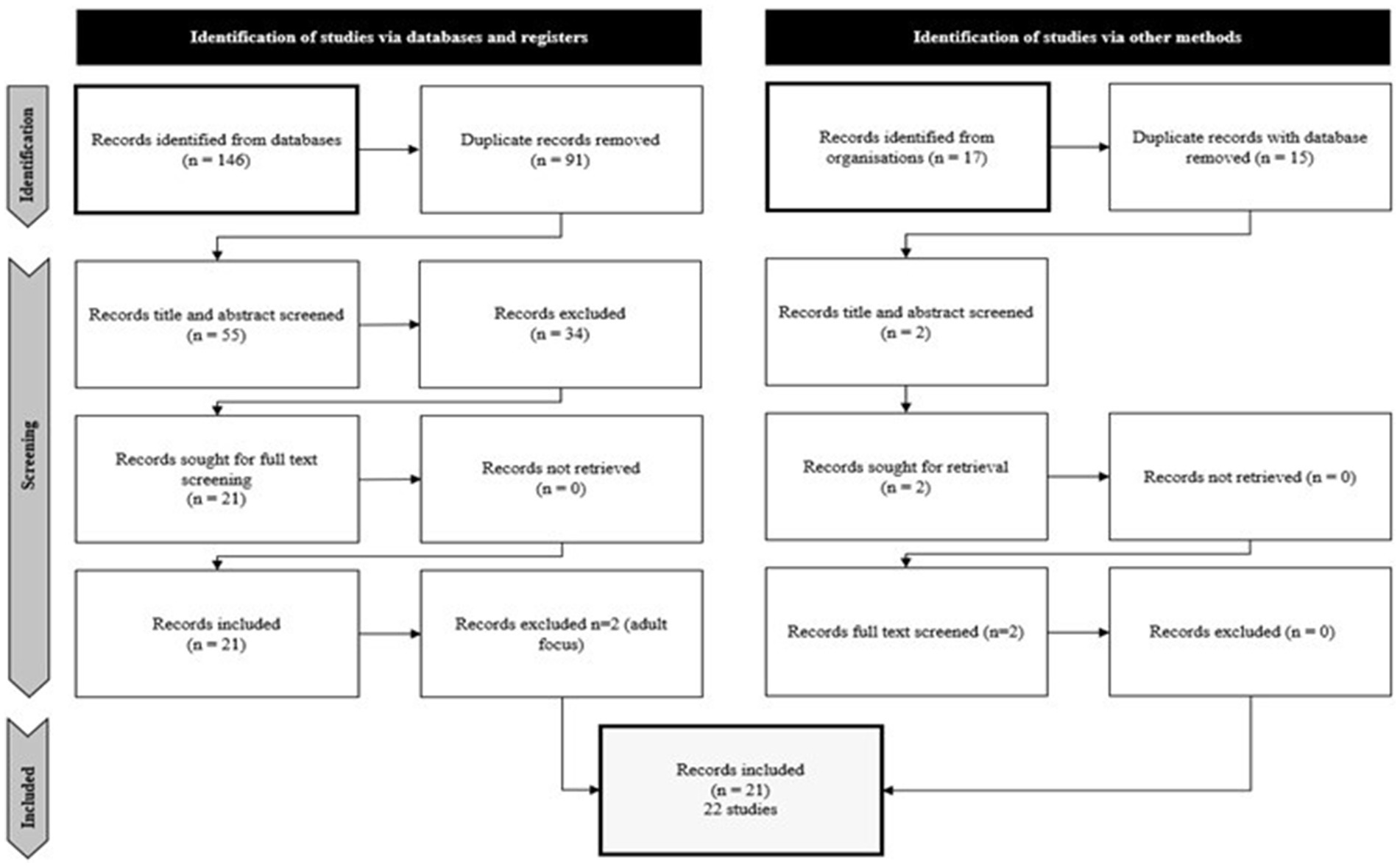
Figure 1. Prisma flowchart.
The following bibliographic databases were searched: PsycInfo, Educational Research Information Center, Proquest Premium Social Sciences Collection, Scopus, EBSCO host and JSTOR. Grey literature was identified through Proquest Dissertations, Open Access Theses and Dissertations, Stanford University Libraries (Searchworks), Melvyl, World Cat Dissertations and Theses, Ethos, Cambridge University Library Theses Catalog (Apollo), Oxford University Research Archive, ten pages of Google Scholar, and the professional organizations PDA Society UK, and PDA North America.
Search string
Abstracts, titles, and keywords of the databases were searched using the following search string to capture studies of pathological demand avoidance (“pathological demand avoidance” OR “extreme demand avoidance” OR “demand avoidance phenomena” OR “rational demand avoidance” OR “demand avoidant behavio?r”) and children and adolescents (child* OR “school refus*” OR “high school” OR “secondary school” OR “elementary school” OR “junior school” OR “junior high school” OR “high school” OR “senior high school” OR “middle school” OR adolescen* OR youth OR “young person” OR “young people” OR boys OR girls OR “middle school” OR pre-school OR play-school OR kindergarten OR “special school” OR “pre-school” OR “play-school” OR classroom OR class OR school OR pupil OR student).
Screening and selection process
LH and JS the primary and secondary reviewers screened title and abstracts independently and met regularly to build consensus. The new PRISMA flow diagram for reviews including searches of other sources (Page et al., 2021) was adapted for use as shown in Figure 1. One hundred and forty-six records were obtained from the main databases, e.g., Proquest, Google Scholar and dissertation databases. Ten pages from Google Scholar and all of PDA organization websites records were hand searched and only empirical journal articles included. Reference lists were examined to identify additional articles meeting the inclusion and exclusion criteria. Duplicates were removed and 57 records remained, 55 from databases and 2 from organizations for title and abstract screening. The inter-rater agreement (Cohen’s kappa coefficient (κ) statistic) for study inclusion following title and abstract screen was 96.49. Twenty-three records (21 from databases and 2 records from organizations) remained for full text screening. PDFs of all full texts (23) were obtained and examined by LH. Access to a full text of a doctoral dissertation was sought and obtained. Two records were excluded as the units of interest were not children or adolescents with PDA. Twenty-two studies from 21 records remained for inclusion as shown in Figure 1.
Data extraction and analysis
Data were extracted according to research questions using an extraction tool developed and piloted before use by the authors. Some variables were given numerical codes (e.g., source, 1 = parent 2 = teacher) and others included raw data (e.g., instruments) that were organized thematically after extraction.
Study characteristics
The following study characteristics data were extracted: country, discipline of main author, funding, aims, research design, methods, sampling and recruitment technique, participant inclusion criteria, sample size, participant age, diagnoses, and education setting. In an emerging field, it is important to understand who is researching and where, and how samples are chosen. Study focus (i.e., what the studies were about) was also documented and categorized using Beck’s (1979) case formulation approach (origins, mechanisms, symptoms, problems and/or precipitants of PDA). Study characteristics data were summarized for ease of reporting by collapsing figures for individual groups within samples, e.g., reporting total sample numbers.
Conceptualization of PDA
Introduction sections and short, summary descriptions of PDA were collated to analyze conceptualization of PDA. Mapping how researchers are describing PDA, its indicators, and dimensions and where this knowledge base originates from is important, as the construct is controversial. These data were analyzed using inductive category formation, a form of content analysis (Mayring, 2014) as displayed in Figure 2. The extracted text was read and when an indicator of PDA was found, the first dimension of PDA was constructed. When the next indicator was found, it was examined to consider whether a new dimension could be formed. After examining conceptualization data from 50% of papers, an interim review with the second author was conducted to ensure that categories did not overlap and that the level of abstraction was adequate (Mayring, 2014). Dimensions became more general, and labels were revised to become more neurodiversity affirmative. Three main dimensions with subdimensions were agreed on.
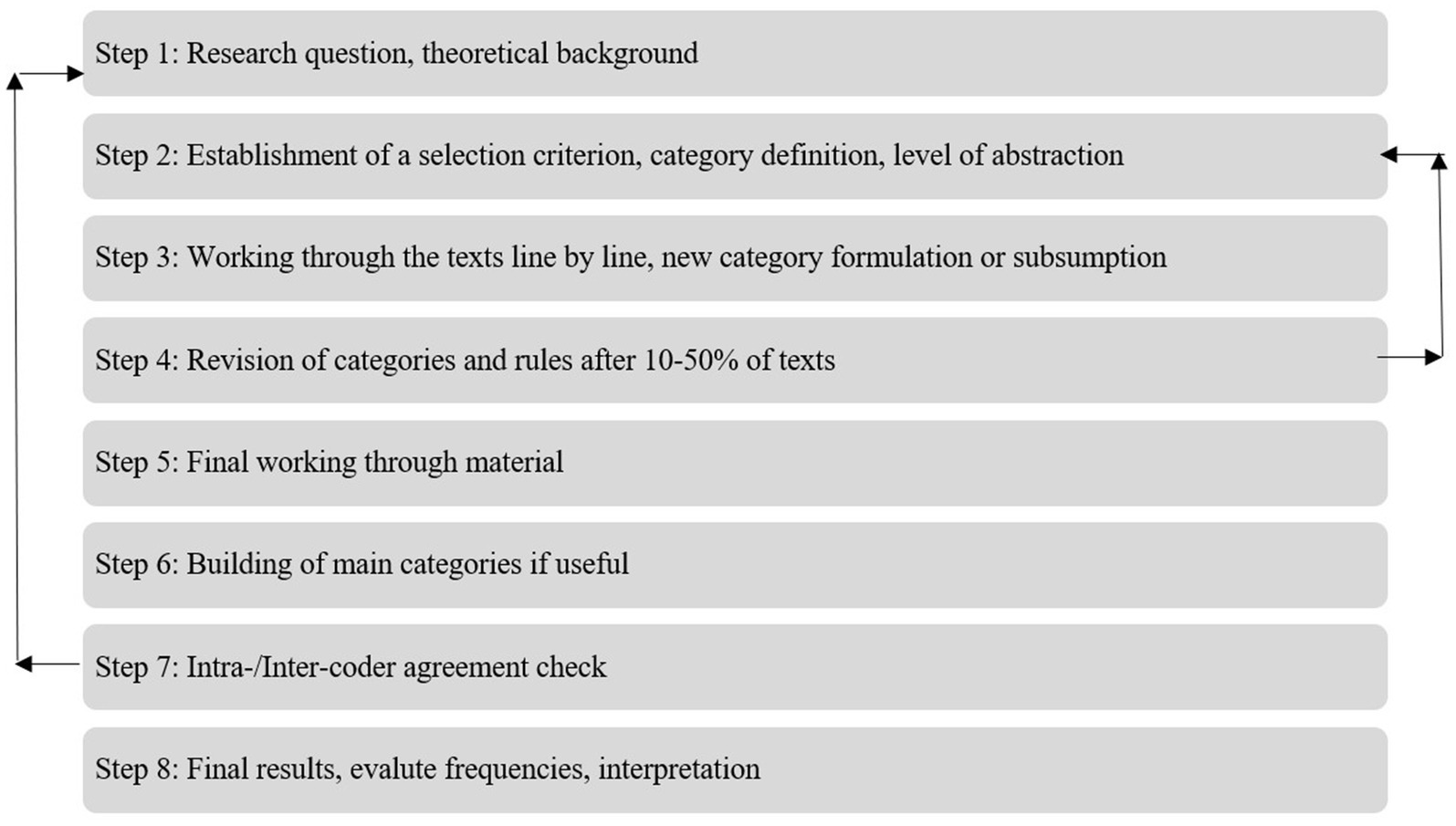
Figure 2. Summary of the steps.
Qualitative methods
Data were extracted regarding interview participants, topic and number of questions, duration and location, information on assent/rapport and how data were recorded and kept confidential as well as analyzed. The clarity and transparency of information on assent/rapport, data recording and confidentiality were used to approximate qualitative trustworthiness. Assent/rapport data were of interest given what the research says regarding engaging a PDA population in agendas set by others, and autistic differences in communication. Confidentiality was also believed to be important, given that PDA is not being identified by all clinicians and the inherent vulnerability in this population. Data on qualitative methods were analyzed using frequencies and with a narrative approach.
Quantitative methods
Regarding quantitative methods, these data were extracted: setting of data collection, measure and reference, age, description, number of items, cut off values, anchor values, validity (discriminative and content) and reliability. The setting is relevant to the preferences this population may have for means of interaction (e.g., online over face to face) or the services they are most comfortable to engage with. Given the sparsity of validated tools, it is of interest which measures authors deemed relevant to explore the presentation described as PDA. Data on quantitative methods were also analyzed using frequencies and with a narrative approach.
Scoping review results
Overview of studies
A total of 22 studies were eligible for this review, the characteristics of which are shown in Table 1. Twenty-one studies contained predominantly UK-based respondents, one study took place in the Faroe Islands1 (Gillberg et al., 2015), and all were conducted between 2003 and 2021. No studies could be found that were conducted published between 2004 and 2012. Seventeen studies were published in peer reviewed journals, which focused either on autism (n = 5), mental health (n = 10), or inclusive education (n = 2). There were four doctoral theses included in the final set of studies. Of the 21 studies, 13 were conducted by clinical psychologists, while the other studies were conducted by educational psychologists, speech and language therapists, mental health clinicians, geneticists, developmental psychologists, and special educators. PDA sample sizes ranged from 1 to 326. In most samples, children were aged between 8 to 12 years. There were a range of presentations and educational settings.

Table 1. Overview of studies included in review.
Study focus
The topics of each study were categorized in line with Beck’s (1979) formulation. Most studies considered multiple aspects relating to PDA. As shown in Table 2, authors focused primarily on symptoms (95%) of PDA, and only in 27% of cases were the origins of PDA considered. The majority of studies also considered the mechanisms of PDA and/or the precipitants of PDA, at 68 and 64%, respectively. Over half of the studies (55%) considered the problems experienced by individuals with PDA.
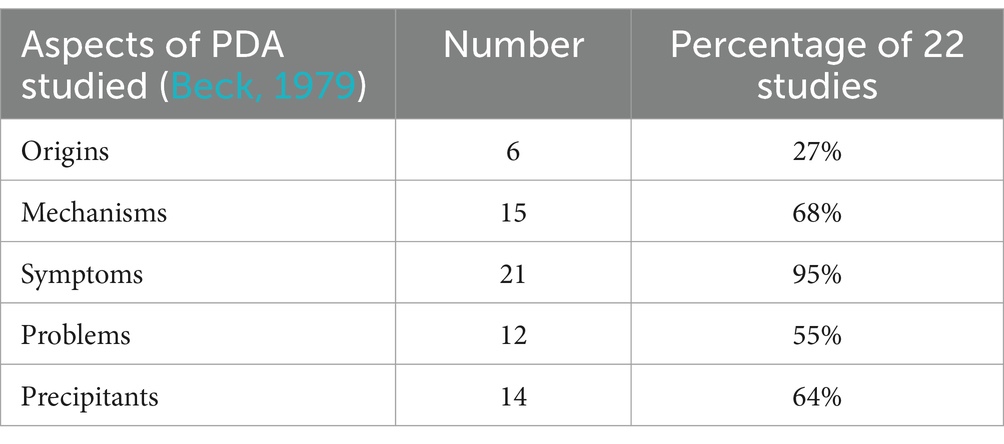
Table 2. Study focus.
Study characteristics
As identified in Table 3, half of the studies (50%) used only quantitative methods, (i.e., questionnaires and diagnostic instruments) of which all were non-experimental and 95% were cross-sectional in design. 45% of studies used a mixed methods approach (e.g., questionnaire and interview). Only one study (O'Nions, 2013) used a purely qualitative approach with a semi-structured interview.
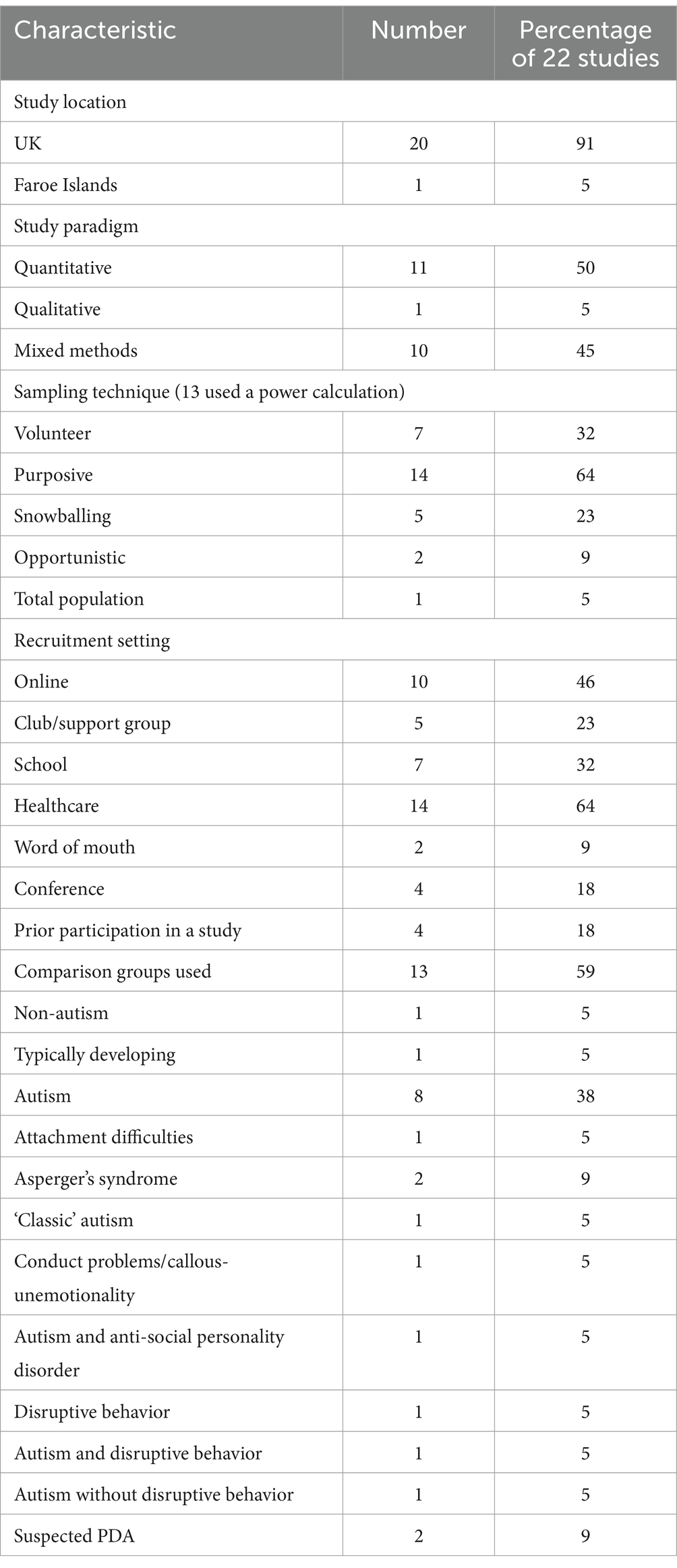
Table 3. Study characteristics.
Fourteen per-cent of studies used a power calculation to determine the size of sample needed to determine an effect. Many studies used a variety of sampling approaches, however purposive sampling was the majority (65%). Other studies used volunteer (32%), snowballing (23%) and opportunistic (9%) methods. Interestingly, one study (Gillberg et al., 2015) conducted a population-based study where all children born were screened. Recruitment for most studies was done through healthcare (64%), 46% online, 32% education, 18% conferences/prior participation in a study or a club or support group and 9% word of mouth.
Fifty-nine per-cent of all studies used a comparison group. Most studies (38%) used autism as a comparison group, and a further 34% used another DSM-IV description of autism, e.g., Asperger’s syndrome, some (10%) with co-occurring presentations, e.g., autism and anti-social personality disorder. O'Nions et al. (2014a) used a neurotypical group, measured by scores on certain scales. Bishop (2018) noted they used a non-autism group, O'Nions (2013) used a group with conduct problems/high callous-unemotionality, while Eaton and Weaver (2020) used attachment difficulties as their comparison group.
Conceptualization of PDA
Both dimensions and summary descriptions of PDA were analyzed. Regarding descriptions, most studies referred to features of PDA described by Newson et al. (2003) as shown in Table 4. Newson et al. (2003) positioned PDA as similar to, but distinct from autism as it was understood at the time, thus much of the features described initially relate to those seen in autism, according to previous versions of the DSM but with key differences. Several studies proposed that the DSM-V criteria signal that PDA exists as a profile for some autistic people then go on to compare the two profiles. Some studies explore PDA as occurring in other groups. Using content analysis of the study descriptions of PDA, three overarching dimensions of PDA were identified: Emotion, Socio-Cognitive, and Neurological Involvement, each with subdimensions shown in Table 5.
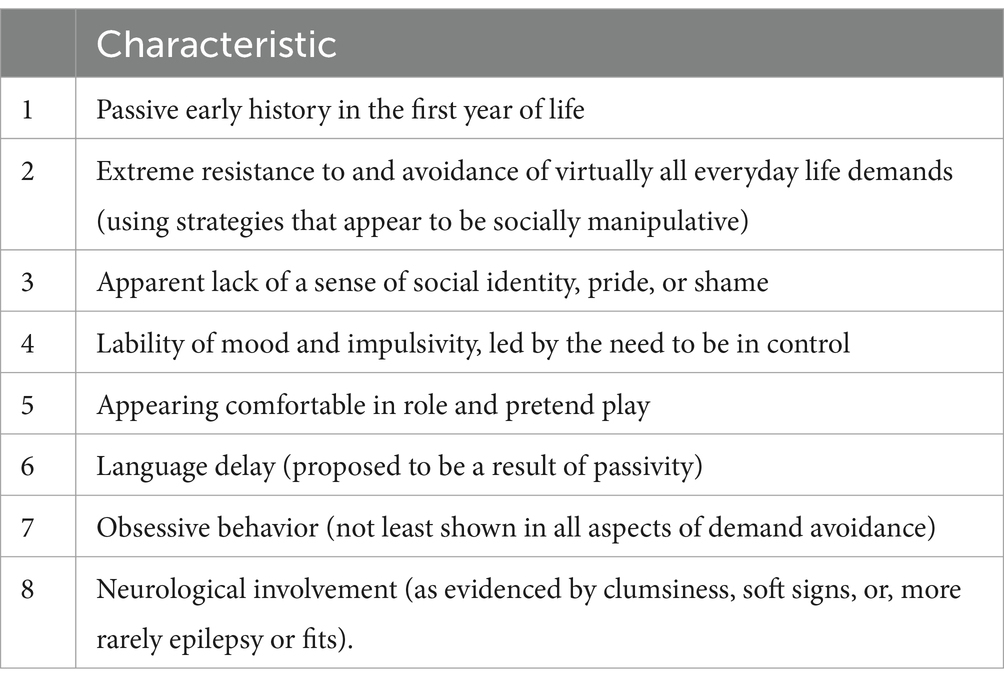
Table 4. Characteristics of PDA according to Newson et al. (2003, p. 597).
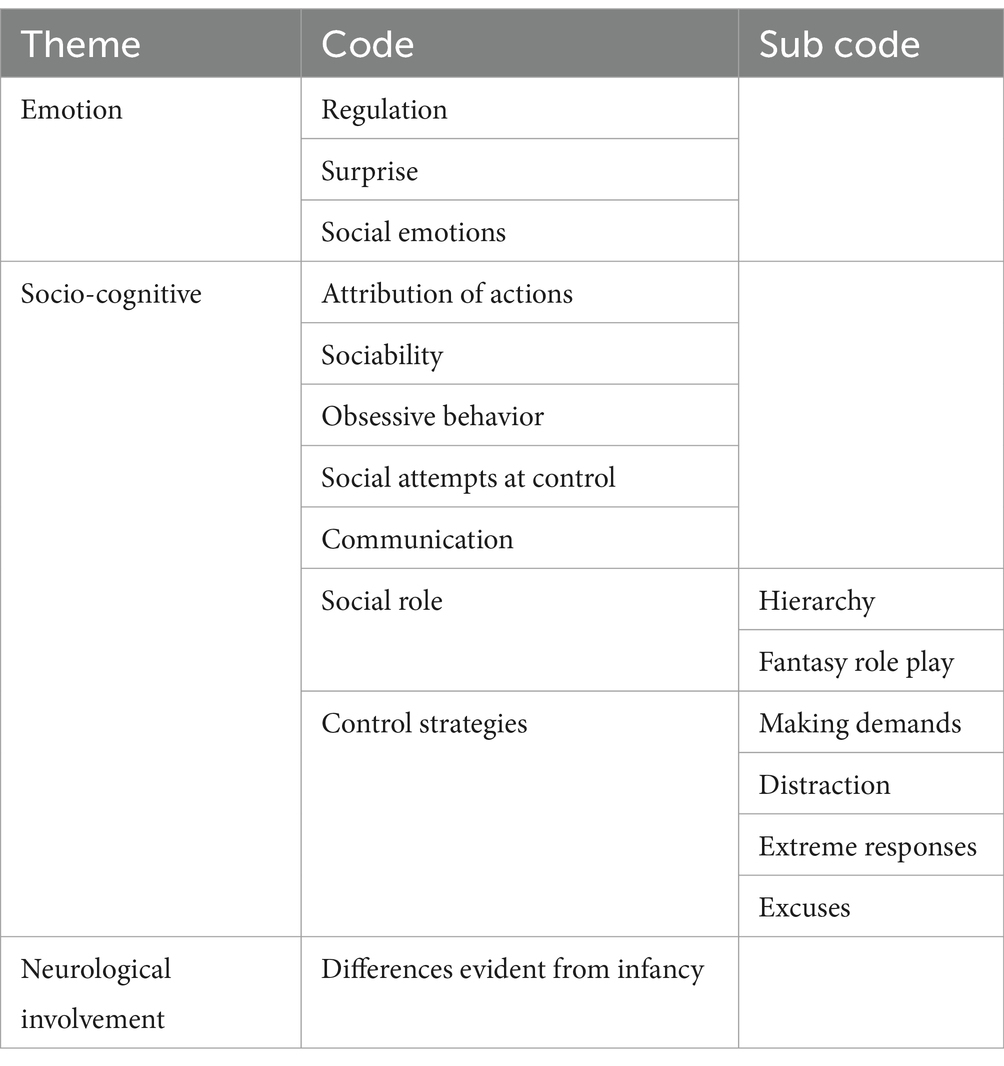
Table 5. Conceptualization of PDA in included studies.
Emotion
The subdimension of Regulation relates to a difference in how individuals with PDA experience change in emotional regulation, this difference is more pronounced than what is experienced by those who are autistic without PDA. The phrase ‘lability of mood’ was used, ‘including sudden changes from loving to aggressive’ (O’Nions et al., 2021, p. 2). A second subdimension, Social Emotions, describes differences in how socially embedded emotions such as identity, pride and shame are understood with authors going as far as to describe such emotions as ‘lacking’ in individuals with PDA (Bishop, 2018, p.78). The final subdimension of Surprise in the dimension of Emotion represents a preference for and responding best to spontaneity, humor, and unpredictability. This is of interest in the context of a traditional view that autistic people benefit from structure and routine (Kunce and Mesibov, 1998).
Socio-cognitive
The subdimension, Attribution of Actions, refers to the description of children not fully grasping or recognizing the impact of their actions on others, which can be explained in a more neurodivergent-positive way as a unique way of processing and interacting with the world (Graham-White, 2015, p. 2). It describes children asking personal questions…[and] behaving in provocative ways (O'Nions et al., 2014a) linked to a need to control the environment, ‘when prompted to comply… socially shocking … behaviour’ (Goodson, 2018, p. 66). The subdimension Sociability relates to individuals apparent seeking social connections, but not in the way others expect, described by Newson et al. (2003, p. 595) as carried out ‘in an odd way’. The concept is often linked with a need to control, ‘an apparent sociability…used to achieve avoidance or control of situations’ (Stuart et al., 2020, p. 60). The subdimension Obsessive Behavior recognizes that experiencing certain strong passions/preferences or interests is a criterion for identification of autism, known as restrictive or repetitive behaviors or interests in the DSM-V (American Psychiatric Association [APA], 2013). In PDA, the social nature of the preference or interest provokes surprise, ‘obsessive behaviour; often focused on …particular people’ (O'Nions, 2013, p. 83).
The subdimension Social Role relates to difference in understanding of roles, including of self and others, likely defined by cultural norms relating to hierarchy, as well as unusual use of fantasy. Children were described as being, ‘oblivious to the fact they were children, identifying more with adults and adopting domineering roles with peers, or even their parents’ (O'Nions, 2013, p. 83). Children are often described as ‘at ease in role play’ (Goodson, 2018, p. 67). The subdimension Social Attempts at Control refers to a need for individuals to control the environment, and avoid demands with the aim of managing anxiety, done through what are described as ‘socially manipulative strategies’ (Goodson, 2018, p. 66). The degree of non-engagement with demands of others captures interest, O'Nions et al. (2014a) note, ‘obsessive, not limited to unpleasant tasks, but at worst, a blanket resistance to accept suggestions, to talk, sit down, take part in fun activities or walk in the same direction’. The understanding of individuals’ need for control of others and ability to cope with demands of others varies across studies. Authors note ‘attempts to control … others’ activities using coercive strategies (e.g., threats), elaborate excuses, sabotaging, and extreme aggression’ (O’Nions et al., 2021, p. 2) while Newson et al. (2003) used the lens of a panic attack, perhaps seeing loss of control as an overwhelmed nervous system.
The subdimension entitled Control Strategies contains four subgroups of indicators with each group signaling a different attempt to maintain control. Making Demands refers to individuals not recognizing the volition of others, e.g., by describing how others should behave, e.g., deciding the clinician could only deliver requests with the door open (Eaton and Weaver, 2020, p. 36). Distraction of Others captures a group of indicators showing how individuals are perceived as distracting from or delaying demands being placed upon them, by ‘asking repetitive questions’ (Eaton and Weaver, 2020, p. 35), ‘adopting a babyish style’ (O'Nions et al., 2014a, p. 758), or ‘offering large amounts of information’ (Eaton and Weaver, 2020, p. 35). Extreme Responses capture bigger responses to attempt control (e.g., meltdown, harming, destruction) to maintain control, understood as a ‘final avoidance strategy, having exhausted all other means’ (Eaton and Weaver, 2020, p. 35). Excuses Used with Others is a group of indicators showing the creativity which individuals employ in their attempt to achieve control, for example, saying they do not know an answer, blaming others, to a very inventive level, such as, “I cannot possibly; I’m Mr. Platypus and platypuses do not talk” (Eaton and Weaver, 2020, p. 35).
Communication is a subdimension relating to perceived differences in language use, including understanding of metaphorical speech, using, and understanding humor and abnormal speech content (Graham-White, 2015). The studies referenced indicate noticeable communication differences, distinct even from the atypical communication observed in autism and less impaired pragmatically compared to Asperger’s syndrome (Newson et al., 2003, p. 595). These distinctions are believed to be noticeable from infancy, with children initially appearing passive in their early years (Newson et al., 2003).
Neurological involvement
This dimension refers to the role of neurology, evident from infancy in the differences observed in the PDA profile. Many studies cited Newson et al.’s (2003, p. 597) early description of ‘soft neurological signs…clumsiness or physical awkwardness, crawling late or absent in more than half’ as well as ‘absences, fits, episodic dyscontrol, or generalized excitability’. Three studies also noted the presence of seizures (O’Nions et al., 2016) or epilepsy (Reilly et al., 2014; Gillberg et al., 2015). O'Nions (2013, chapter 4) reported ‘floppiness’ as infants, perhaps to refer to low muscle tone.
The research landscape surrounding PDA predominantly revolves around individuals who possess verbal communication skills and do not exhibit intellectual disabilities. Notably, widely-used assessment tools like the EDA-Q lack validation for individuals with intellectual disabilities (ID) (O'Nions et al., 2014a), thus limiting their applicability in this population. Verbal communication is often emphasized as a fundamental aspect in current conceptualizations of PDA, as evident from specific references such as the paragraph cited in lines 527–541 on page 14. However, this emphasis may inadvertently exclude non-verbal individuals or those with intellectual disabilities from comprehensive study. It is imperative for researchers to critically assess the suitability of their chosen research methods for these populations, considering factors such as communication barriers and cognitive abilities. Inclusion of at least one paragraph in the Discussion section addressing the adaptability of research methods for non-verbal individuals or those with intellectual disabilities is crucial. Additionally, explicit recognition of this demographic as a focal point for future research endeavors is necessary to ensure inclusivity and foster a thorough understanding of PDA across diverse populations.
Quantitative methods and reliability
This section relates to the following research questions: ‘What are the quantitative methods used to study PDA in children and adolescents?’ and ‘given the available evidence, how reliable are the quantitative methods used to study PDA in children and adolescents?’
Identification of PDA and autism
Possibly owing to inconsistent practices of identifying PDA, only 9% of studies required a clinical diagnosis in their samples. Twenty-four per-cent involved parent report of the profile (Table 6). The parent-report 26-item Extreme Demand Avoidance Questionnaire (EDA-Q) (O'Nions et al., 2014a) was the most used measure to identify PDA (45%). Authors have also used shorter versions with 11 items (O'Nions et al., 2018a) and 23 items (O’Nions et al., 2021). The EDA-Q contains features of PDA as described by Newson et al. (2003) which indicates the development of PDA criteria based on archival data. Eighteen per-cent of studies used the Diagnostic Interview for Social and Communication Disorders II (DISCO) to identify PDA, in longer and shorter formats of 15 and 11 items (Gillberg et al., 2015; O’Nions et al., 2016; O'Nions et al., 2018a).
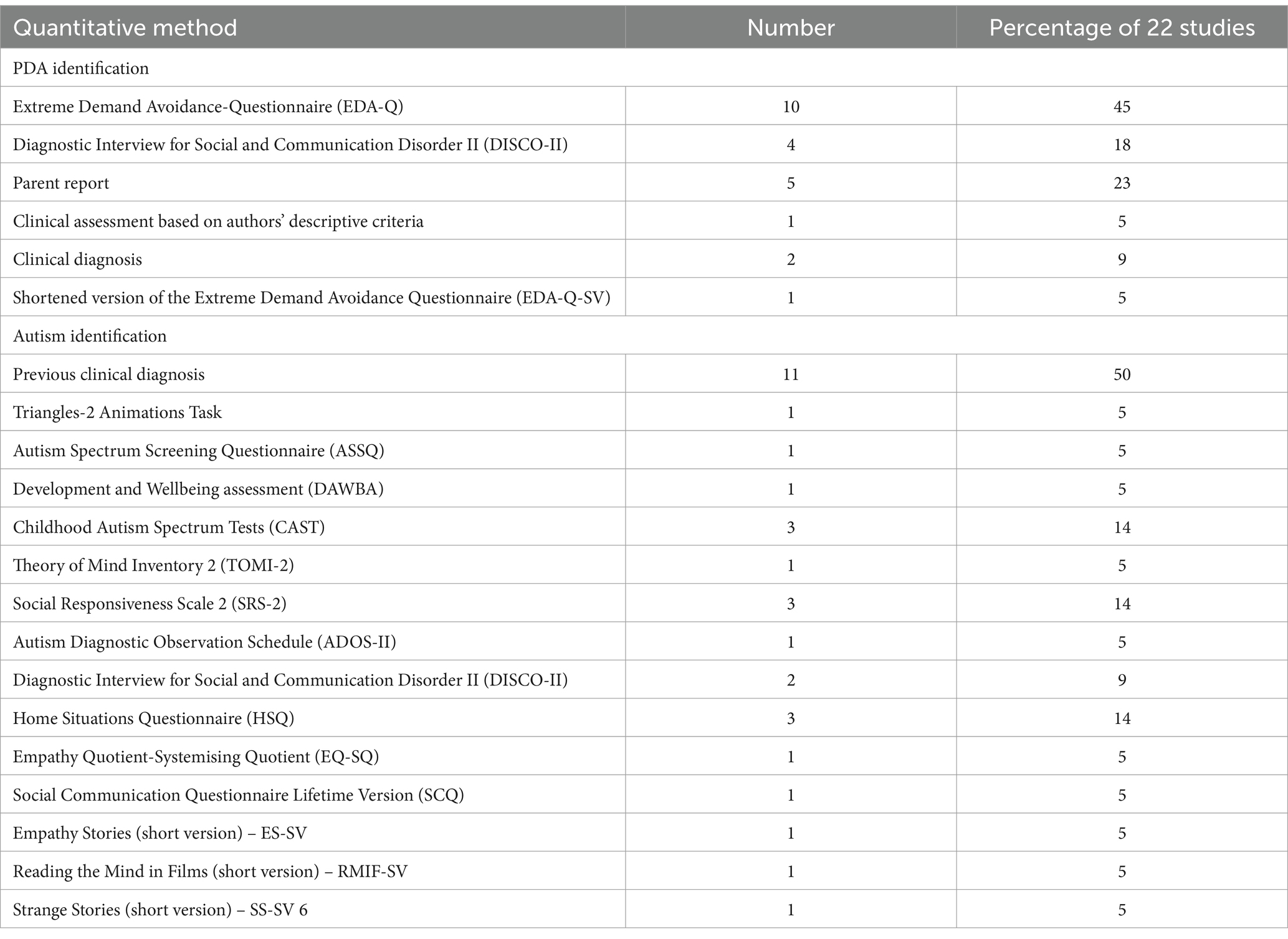
Table 6. Quantitative methods used to identify PDA and autism.
Half of the studies (50%) involved a previous clinical diagnosis of autism. In other studies, a wide variety of tools were used in identifying autism, the most common were, the Childhood Autism Spectrum Test (CAST) (14%), the Social Responsiveness Scale 2 (SRS-2) (14%) and the Home Situations Questionnaire (HSQ) (14%). Measures assessing theory of mind, (e.g., Triangles-2 Animations Task) and empathy (e.g., Reading the Mind in Films (RMIF)) were common. One study (O'Nions et al., 2014a), used the Development and Wellbeing Assessment (DAWBA) (Goodman et al., 2000) which generated information based on common ICD-10 and DSM-IV psychiatric conditions in children, versions of which have since advanced.
Statistical analysis
Within the 22 separate studies, there were 18 analyses of quantitative data, shown in Table 7. All the studies that analyzed quantitative data reported descriptive statistics (N = 18), and in addition, 13 of these studies examined their data using inferential statistics. The most common types of inferential statistic used were t-tests (n = 8) and correlation (n = 7). Fewer studies used regression (n = 4) and ANOVA (n = 3). A few studies (n = 5) used non-parametric statistics: Chi-Square, Mann Whitney U, and Kruskal Wallis. Other types of analyses used (in 3 studies) were MANOVA, Spearman-Brown split-half reliability, principal components analysis, graded response model, and the receiver operating characteristic curve. Of the quantitative studies that used psychometric scales (n = 16), 8 reported their own validity analysis, 2 reported the validity analyses of other studies, and 6 did not include a validity analysis. Overall, most quantitative analyses used relatively simple inferential statistics including correlation and group differences tests. Far fewer studies used regression analyses building on the relationships between variables.
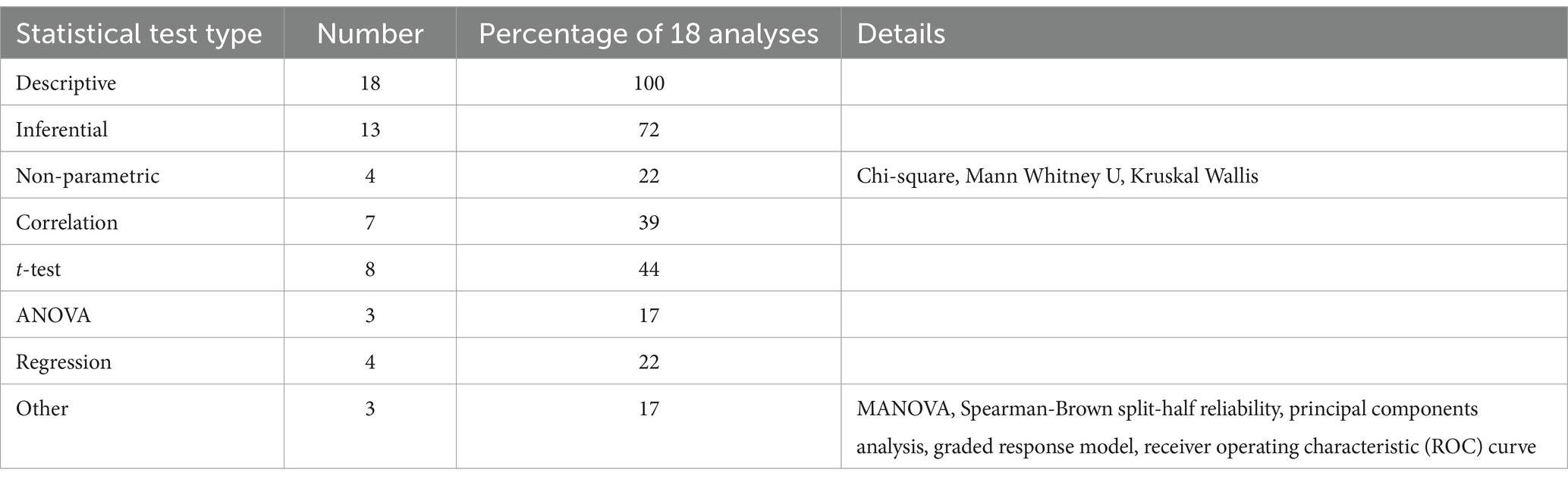
Table 7. Statistical tests used in the analysis of quantitative data.
Qualitative methods and trustworthiness
This section relates to the following research questions: ‘What are the qualitative methods used to study PDA in children and adolescents?’ and ‘Given the available evidence, how trustworthy are the qualitative methods used to study PDA in children and adolescents?’
Methods
Table 8 outlines the qualitative methods used in 50% of studies, all of whom, except O'Nions (2013), also used quantitative methods. The most common method was semi-structured interview (64%) with parents (91%), with the most common topic being their child’s current presentation and school experience (91%). Some interviews were at least partly based on widely used diagnostic interviews such as the Autism Diagnostic Interview- Revised (ADI-R), and the DISCO-II or on Newson’s PDA criteria or on the EDA-Q. Similarly, observations were at least partly based on the ADOS-II, a play-based autism observation assessment. In exploring tolerance of uncertainty through a behavioral presentation, Stuart et al. (2020) employed an Antecedent, Behavior Consequence (ABC) structure during a telephone interview. 18% of studies gained a developmental history, where the focus for Graham-White (2015) in his case file review was on creating communication profiles at different stages.
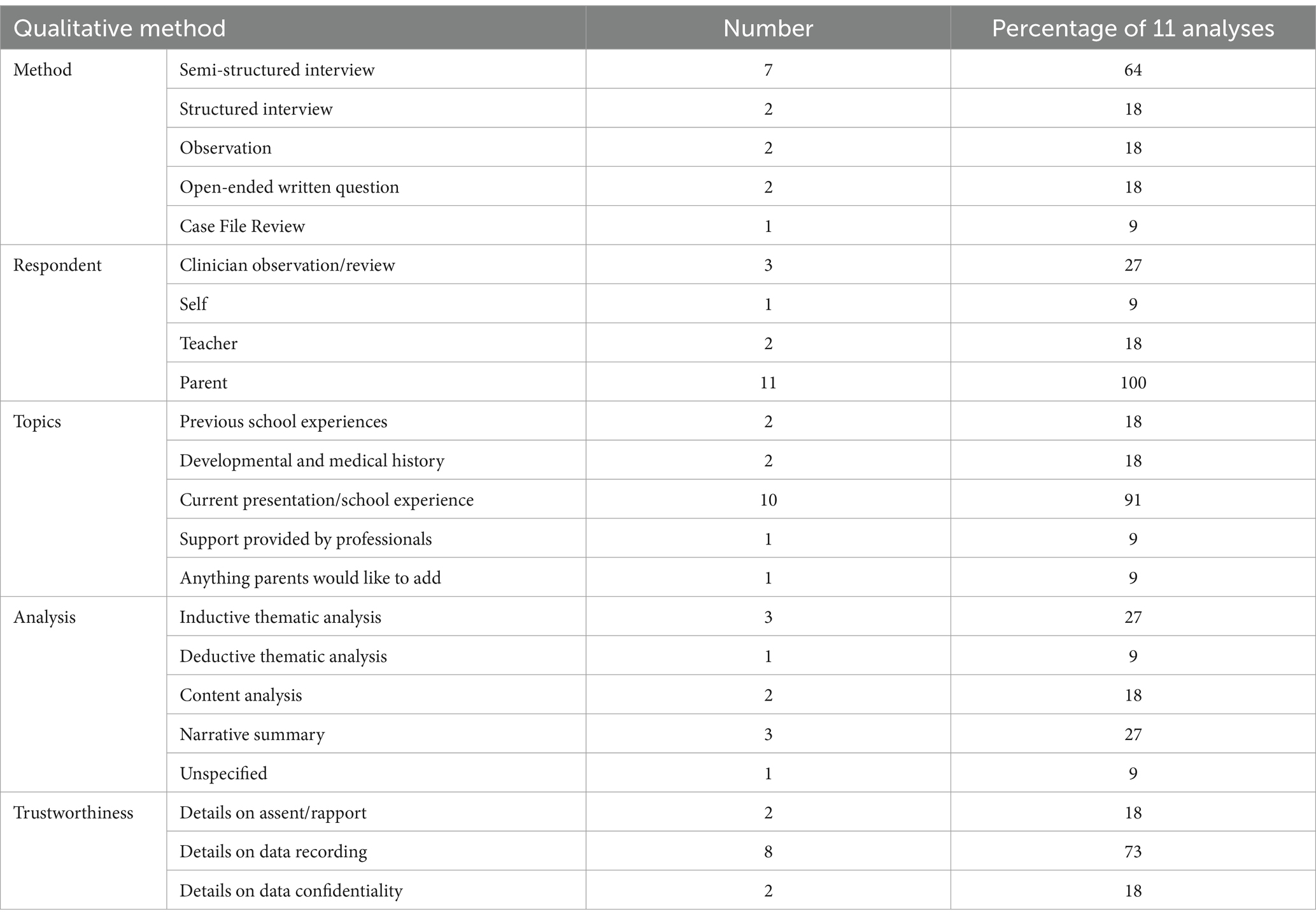
Table 8. Qualitative methods used to study PDA and trustworthiness.
Only one study (Brede et al., 2017), took a true triangulation approach in interviewing young people, parents, and teachers about their experiences in their current and previous schools. Truman et al. (2021) examined support and perceived helpfulness provided by different educationalists via an open-ended written question using some elements of the Educational Experience Questionnaire (Gore Langton and Frederickson, 2016).
Within the 22 separate studies, there were 11 qualitative analyses. Each type of quantitative and qualitative analysis method was logged during data extraction. Of the 11 qualitative analyses, there were 3 inductive thematic analyses (Braun and Clarke, 2006), 3 narrative summaries of clinical case studies and reports, 2 content analyses (Mayring, 2014), and 1 deductive thematic analysis using a questionnaire item framework. One study did not specify the analysis type. These results show a wide spread of types of qualitative analyses, although all were thematic in their approach.
Trustworthiness
Of the 11 qualitative methods employed, all gave information regarding trustworthiness, 57% gave a detailed account, and 43% gave few details. Two studies reported information on data confidentiality and eight on data recording. As the only qualitative study eliciting the voice of adolescents and their teachers, Brede et al. (2017) described how assent and rapport were achieved. Interviews took place in their school and visual supports and choice was incorporated regarding people present and/or order of events (Brede et al., 2017). Researchers met with students several times thus viewing consent as a continuous process (Brede et al., 2017).
Discussion
The attention to PDA is growing but is rife with disagreement. Coherence in the field is needed to move forwards with clarity. Currently, only two systematic reviews of PDA research exist, with no scoping review dedicated to studies of PDA in children and adolescents. Accordingly, this scoping review sought to synthesize the quantitative and qualitative methods for studying PDA in children and adolescents according to Beck’s case formulation framework (Beck, 1979, in Persons, 2008, p. 5). Research in this area is limited; only 21 studies were identified that met broad inclusion criteria suitable for a scoping review methodology. The studies signal there are children and adolescents who show extreme avoidance of everyday demands resulting in difficulties. To date, this presentation has primarily been studied within autistic people and critics highlight this represents circular reasoning. Many methodological gaps exist with implications on study quality. This review provides information on foundational procedures to inform future research.
Study characteristics
Most studies of PDA have taken place in the UK which presents a limitation, given the growing numbers of people identified as autistic across the globe, with 1–20% of autistic people likely to have PDA (Gillberg et al., 2015). Seminal work was completed by Newson and colleagues in 2003, but no study eligible for this review appears to have been undertaken in the following ten years. Since 2013, reignited by O′Nions et al., there has been growth in research in the area, supported by mainstream interest in support groups such as the UK PDA Society. A variety of professionals have studied PDA to date, with most papers published in mental health journals. Almost all studies used quantitative methods and half also used qualitative methods, reflecting an array of methodological approaches. Consistent with findings from previous reviews (Kildahl et al., 2021; Mols and Danckaerts, 2022), the primary focus of most studies were the features associated with PDA and very few on the origins, mechanisms or precipitants, such factors may require a longitudinal approach. Of those studies focusing on origins, most considered those of neurological in nature as first identified by Newson, e.g., epilepsy.
Given the confusion around the conceptualization of PDA, it is evident that choosing a sample for study is likely to have presented a challenge for many researchers. Evidence of possible overlap in samples was apparent, in line with Kildahl et al. (2021). Most studies used purposive sampling to maximize access and information gathering, but this type of sampling raises questions of generalizability (Etikan et al., 2016). Gillberg et al. (2015) conducted a population-based study to glean prevalence data. Regarding comparison groups, autism was the most common choice, perhaps reflecting a common current understanding of PDA as existing in autism. Half of the studies required autism to be previously identified, reflecting exploration as to whether PDA occurs outside of autism. A variety of other comparison groups were also used. This is encouraging as critics have noted a lack of evidence to confine PDA to autism when Newson did not intend it this way, for example, Woods (2022c) notes alternative explanations for this presentation must be sought.
Conceptualizations of PDA
The influence of Newson et al.’s (2003) early PDA criteria continues to have a significant impact on how researchers conceptualize PDA. Previous reviews (Kildahl et al., 2021; Mols and Danckaerts, 2022) have pointed out the challenges stemming from criticisms of these criteria (Green et al., 2018b; Eaton and Weaver, 2020). Newson regarded PDA as resembling autism but not being synonymous with it; instead, she saw it as a separate developmental disorder (Newson et al., 2003). With the broadening of autism criteria in the DSM-V, some now perceive PDA as a feature of autism (Eaton and Weaver, 2020), leading to its often being analyzed and compared within the framework of autism. Studies might observe, for instance, that children exhibit intense interests akin to those in autism, although these interests may be social in nature.
Botha et al. (2024) highlights the evolution of autism understanding since the introduction of DSM-V, coinciding with the rise of the neurodiversity movement pioneered by Judy Singer in the 1990s. This movement advocates for acknowledging brain divergences without framing them solely as deficits, a perspective historically dominated by neurotypical norms. As Kapp (2020) extensively outlines, neurodiversity embraces the idea that diverse cognitive functioning enriches society. Moreover, autistic adults are increasingly becoming active participants in research endeavors, offering invaluable insights into their own experiences (Fletcher-Watson et al., 2019). This inclusion of diverse perspectives fosters a more holistic understanding of autism spectrum conditions (ASCs). Considering the intersection of Pathological Demand Avoidance (PDA) with autism, adopting an autistic perspective may lead to a re-evaluation of certain traits associated with PDA. This approach challenges traditional dichotomies by highlighting the overlap and nuances within the autism spectrum. The imperative for control, a central aspect of Newson’s criteria, might be reinterpreted as a quest for autonomy and safety (Moore, 2020) in a world designed for a different neurotype, often resulting in challenging life experiences (Gore Langton and Frederickson, 2018; Doyle and Kenny, 2023). This interpretation could extend further: for example, Newson’s characterization of ‘surface sociability’ as ‘odd’ and distinct from autism as per DSM-IV criteria may now only be considered odd when compared to neurotypical behavior.
Surface sociability, which can also be referred to as ‘fawn’ or ‘appeasement,’ may represent a stress response mechanism. This behavior is characterized by individuals displaying exaggerated friendliness or submissiveness in order to diffuse potential threats or conflicts. It is a strategic reaction aimed at reducing perceived danger or aggression from others in their environment (Bailey et al., 2023).
Comfort in role-playing, seen as a strategy to avoid demands, might reflect autistic masking using camouflaging techniques, either deliberate (Cook et al., 2021) or automatic (Hull et al., 2017), to navigate a neurotypical world. Similarly, autistic individuals may have different perceptions of social roles and hierarchy, challenging traditional societal expectations based on neurotypical norms. It’s crucial to note that an interest in people and the appearance of social competence should no longer rule out autism, as they could indicate social camouflaging (Hull et al., 2017). Emotions reliant on cultural norms, such as shame or pride, may manifest differently in autism due to alexithymia (Kinnaird et al., 2019).
Considering the timely access to appropriate support for individuals, accepting Pathological Demand Avoidance (PDA) as part of autism poses unique challenges, potentially risking the integrity of autism itself. If PDA is regarded as a feature of autism but lacks universal recognition, the interplay between the need for control and the presence of traits such as humor, spontaneity, and unpredictability can complicate interventions in autism-focused settings. The need for control, a fundamental human drive, often clashes with traditional approaches to autism, such as TEACCH (Schopler et al., 1995), which emphasize structure, routine, and behavioral strategies (Lovaas, 1987), contrasting with the philosophy embraced by PDA proponents (e.g., Newson et al., 2003; Fidler and Christie, 2019). Moreover, distinct features of PDA, including the avoidance of demands, unique communication profiles, sociability, and imaginative play, may deter individuals from seeking autism assessments, particularly those with limited understanding of their own behaviors. This lack of recognition or misidentification of needs can result in blame, delayed or inadequate support, and negative experiences for families (Gore Langton and Frederickson, 2018; Jacobs et al., 2018; Zener, 2019). Thus, gaining a deeper understanding of the underlying mechanisms behind individuals’ responses is imperative for providing tailored and effective support (Ozsivadjian, 2020).
Woods (2022a) advocates for considering PDA outside the realm of autism and adopting a transdiagnostic approach, rejecting rigid categorizations and highlighting the risk of overlooking the needs of individuals, such as those with high anxiety in autism. Astle et al. (2022) propose a transdiagnostic framework to address the heterogeneity and complexity of neurodivergent individuals, prioritizing early access to support and focusing on underlying mechanisms. Despite the limitations associated with Newson’s work and the challenges in conceptualizing PDA, analyzing existing research underscores the clinical imperative to support children and adolescents exhibiting extreme demand-avoidant behaviors. Across studies, the Emotion, Socio-Cognitive, and Neurological dimensions of PDA present evident day-to-day challenges. Given the focus on children and adolescents, the impact on education is significant. Differences in understanding social roles, including authority and boundaries, may hinder success in compliance-based educational systems. Regardless of the conceptualization of PDA, the pervasive need for control, including over people, may lead to negative perceptions of these individuals and their caregivers in a world governed by neurotypical norms. While understanding of autism improves, distinguishing PDA from anxiety in autism or other conditions remains clinically valuable.
The differentiation between pathological demand avoidance (PDA) and other psychological categories can be complex and influenced by how PDA is defined and measured within studies. For instance, Eaton and Weaver (2020) propose that PDA can be distinguished from trauma; however, some argue that PDA is a manifestation of Attachment Disorder (Christie, 2007; Flackhill et al., 2017). Consequently, if researchers investigate PDA as a form of Attachment Disorder, there may be an inherent overlap with trauma, potentially leading to the interpretation of PDA as trauma-induced. Similarly, O’Nions et al. (2021), in their development of the EDA-8, defined PDA as a subtype of autism and validated it in samples of suspected autistic children and young people (CYP). However, studies such as McFadzen (2020) have shown that the EDA-Q, a questionnaire for assessing PDA traits, can identify significant numbers of non-autistic CYP. This discrepancy suggests that the definition and inclusion criteria for PDA can significantly impact research outcomes. If O’Nions et al. (2021) had adopted a more inclusive approach to defining PDA and included diverse demographic groups such as those with ADHD, they might have produced a different version of the EDA-Q, potentially leading to a different outcome than the EDA-8. Therefore, it is essential for future research to consider the broader context and potential overlaps between PDA and other categories, as well as the implications of different measurement approaches.
Quantitative methods
Most quantitative studies relied on parent report which some argue increases risk of bias as parents may have elected to take part owing to interest in PDA (Green et al., 2018b). In addition, accounts from parents of their children’s experience, and of the demands they face may differ than if the individuals were asked directly (Kalvin et al., 2020). There are only two measures in use for the study of PDA, the EDA-Q and the DISCO.
The EDA-Q, validated by O'Nions et al. (2014a) which demonstrated strong psychometric properties and discriminatory capacity is the most common measure. Gore Langton and Frederickson (2016) and Stuart et al. (2020) also noted the EDA-Q shows high internal consistency. The EDA-Q is also primarily based on PDA as described by Newson, thus, is not without its difficulties (Green et al., 2018b). This is important if it is upon which our knowledge base lies (O’Nions et al., 2021). A principal component analysis was carried out on the EDA-Q resulting in the 23 item EDA-8 (O’Nions et al., 2021) and on the DISCO, demonstrating good discriminatory power (O’Nions et al., 2016). However, the different thresholds values in use to indicate PDA across studies based on the DISCO, (Gillberg et al., 2015; O’Nions et al., 2016; O'Nions et al., 2018a) further highlights the difficulty with defining the PDA construct. Perhaps reflecting a more established field of study, many different measures are in use in assessment of characteristics of autism.
Descriptive statistics were used in all quantitative studies, often accompanied by simple inferential analysis. Many studies used psychometric scales but reporting of validity scores was inconsistent. The lack of complex statistical analyses may be explained by the relatively smaller samples in use in studies, the largest study had 326.
Qualitative methods
Predominantly, qualitative methods have been used alongside quantitative methods in the study of PDA. In using qualitative approaches, most papers did not address researcher positionality. Like the quantitative methods, to date the source of information has heavily relied on parents who, in semi-structured interview report on children’s current and previous experience. In line with Beck’s framework, the focus in qualitative work has thus been on symptoms and problems associated with PDA. More than half of papers reported trustworthiness data, but given the vulnerability of the population, there is a low number reporting confidentiality information.
Only one study (Brede et al., 2017) interviewed parents, teachers, and adolescents. Of note, given the increasing attention being paid to the impact of the autistic voice in research and in neurodiverse movements and the idea of ‘nothing about us without us’ (Milton, 2019), Brede et al. (2017) were the only authors to interview adolescents. The voices of teachers, children, and psychologists are relatively absent. Information on how assent and rapport was achieved in the Brede et al. (2017) study is important and reflects a possible platform for future researchers to build upon. The study indicates consideration needs to be paid to setting, number of sessions, who present, use of choice and visual supports.
Limitations
A strength of this review is that it is one of the first to focus on the foundational processes involved in the study of PDA. This is important given that the landscape regarding PDA is particularly unclear and rife with criticism with implications on clinical practice and thus vulnerable families. A weakness of the review is that it profiles only studies of children and adolescents and does not address methodologies in use in the study of PDA in adults. Accordingly, it is possible that some methodologies exist for the study of PDA in children and adolescents which are not documented here. Secondly, content analysis was chosen to address how studies were conceptualizing PDA, content analysis can be reductive which may be problematic given the overlapping nature of features of PDA with other neurodevelopmental differences. Moreover, the studies have used clinical, strategic, or convenience samples. This makes it highly likely that those having a clinical picture in line with existing descriptions of PDA may be overrepresented in the studies. Sampling bias is a problem across these studies, and limits also what conclusions may be drawn in this review.
Conclusion
Research in this area is limited; only 21 studies were identified that met broad inclusion criteria suitable for a scoping review methodology. The studies signal there are children and adolescents who show extreme avoidance of everyday demands resulting in difficulties. To date, this presentation has primarily been studied within autistic people and critics highlight this represents circular reasoning. Many methodological gaps exist with implications on study quality. This review provides information on foundational procedures to inform future research. It is important to acknowledge the widely recognized limitations of most PDA studies, especially in the context of this dataset. The studies reviewed vary significantly in their methodologies; while some incorporate control groups, others do not, leading to potential biases and challenges in generalizability. For example, the study by Gillberg et al. (2015) employed a population-based approach to glean prevalence data, whereas other studies relied heavily on purposive sampling (Etikan et al., 2016). The lack of standardized control groups and inconsistent methodological rigor across studies pose significant challenges in drawing definitive conclusions. Additionally, the reliance on parent-reported measures, such as the EDA-Q and DISCO, can introduce bias, as parents may have a vested interest in the outcomes (Green et al., 2018b; Kalvin et al., 2020). Future research must prioritize robust quality appraisal methods to ensure the reliability and validity of findings. It is imperative that future datasets undergo thorough quality assessment to establish the credibility of the data produced. Moreover, the reliability of tools does not necessarily equate to the validity of the data regarding PDA characteristics. This highlights the need for continual refinement and critical evaluation in the study of PDA to enhance the overall understanding and support for this population.
This review explored the methods used to study PDA in children and adolescents. Few reviews of methods exist, in a research field rife with disagreement with impacts on clinical practice with children and adolescents presenting as experiencing extreme challenges. The review examined the methods used in previous research employing a scoping review methodology suitable for the research question. The findings suggest that there is a range of methodological approaches being utilized. However, there is a noticeable absence of socio-cultural reflection in these studies. While most studies concentrate on the symptoms and issues related to PDA, there is less focus on understanding its origins, mechanisms, triggers, and effective support systems. Moreover, current studies lack the incorporation of subjective experiences, which are now recognized to hold significant value, and instead heavily rely on parental reports. Additionally, both studies and assessment measures tend to rely excessively on criteria that are over two decades old and may not adequately reflect the complexities of the condition in contemporary contexts. Work needs to be done to further develop measures to conceptualize PDA clearly as distinct from other neurodevelopmental differences where avoidance is also experienced and also to figure out what PDA is, rather than attempting to establish it as a distinct entity, as we do not really know whether this is warranted. It is surprising that few studies included a clinical diagnosis, as there are no formal criteria for diagnosing PDA. Regardless of its developmental trajectory, there is a clear clinical need to address challenges people face. Future research warrants attention to be paid to the neurodiversity movement and double empathy problem, wherein avoidance is viewed through an autistic lens. The review findings outline some useful foundational procedures for the study of PDA in children and adolescents, but many methodological gaps remain with impact on the reliability of research and clinical practice. It is surprising that few studies included a clinical diagnosis, as there are no formal criteria for diagnosing PDA. This omission is notable because the lack of standardized diagnostic criteria makes it difficult to ensure consistency and reliability in the identification and study of PDA. The variability in how PDA is recognized and understood can lead to discrepancies in research findings and clinical interventions, highlighting the need for more rigorous and uniform diagnostic guidelines. Addressing this gap would contribute significantly to improving the reliability of research and the effectiveness of clinical practices related to PDA.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
LH: conceptualization, methodology, data extraction, formal analysis, writing—original draft, and writing—review and editing. JeS: and GD conceptualization, methodology, supervision, and writing—review and editing. JoS: conceptualization, supervision, and review. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
1. ^The population of the Faroe Islands was 53,090 in 2022, and the number of individuals identified with PDA was very few.
References
American Psychiatric Association [APA] (2013). Diagnostic and statistical manual of mental disorders. 5th Edn. Washington, DC: American Psychiatric Association.
Arksey, H., and O'Malley, L. (2005). Scoping studies: towards a methodological framework. Int. J. Soc. Res. Methodol. 8, 19–32. doi: 10.1080/1364557032000119616
Astle, D. E., Bathelt, J., and Holmes, J. (2019). Remapping the cognitive and neural profiles of children who struggle at school. Dev. Sci. 22:12747. doi: 10.1111/desc.12747
Astle, D. E., Holmes, J., Kievit, R., and Gathercole, S. E. (2022). Annual research review: the transdiagnostic revolution in neurodevelopmental disorders. J. Child Psychol. Psychiatry 63, 397–417. doi: 10.1111/jcpp.13481
Bailey, R., Dugard, J., Smith, S. F., and Porges, S. W. (2023). Appeasement: replacing Stockholm syndrome as a definition of a survival strategy. Eur. J. Psychotraumatol. 14:2161038.
Bishop, E. (2018). The relationship between theory of mind and traits associated with autism Spectrum condition and pathological demand avoidance presentations (Doctoral dissertation). London: University College London.
Botha, M., Chapman, R., Giwa Onaiwu, M., Kapp, S. K., Stannard Ashley, A., and Walker, N. (2024). The neurodiversity concept was developed collectively: an overdue correction on the origins of neurodiversity theory. Autism 28, 1591–1594. doi: 10.1177/13623613241237871
Braun, V., and Clarke, V. (2006). Using thematic analysis in psychology. Qual. Res. Psychol. 3, 77–101.
Brede, J., Remington, A., Kenny, L., Warren, K., and Pellicano, E. (2017). Excluded from school: autistic students’ experiences of school exclusion and subsequent re-integration into school. Autism Dev. Lang. Impairment. 2:2396941517737511. doi: 10.1177/2396941517737511
Christie, P. (2007). The distinctive clinical and educational needs of children with pathological demand avoidance syndrome: guidelines for good practice. Good Autism Practice 8, 3–11.
Colquhoun, H. L., Levac, D., O'Brien, K. K., Straus, S., Tricco, A. C., Perrier, L., et al. (2014). Scoping reviews: time for clarity in definition, methods, and reporting. J. Clin. Epidemiol. 67, 1291–1294. doi: 10.1016/j.jclinepi.2014.03.013
Cook, J., Hull, L., Crane, L., and Mandy, W. (2021). Camouflaging in autism: a systematic review. Clin. Psychol. Rev. 89:102080. doi: 10.1016/j.cpr.2021.102080
Cunningham, M. (2022). ‘This school is 100% not autistic friendly!‘listening to the voices of primary-aged autistic children to understand what an autistic friendly primary school should be like. Int. J. Incl. Educ. 26, 1211–1225. doi: 10.1080/13603116.2020.1789767
Doyle, A., and Kenny, N. (2023). Mapping experiences of pathological demand avoidance in Ireland. J. Res. Spec. Educ. Needs 23, 52–61. doi: 10.1111/1471-3802.12579
Eaton, J., and Weaver, K. (2020). An exploration of the pathological (or extreme) demand avoidant profile in children referred for an autism diagnostic assessment using data from ADOS-2 assessments and their developmental histories. Good Autism Practice 21, 33–51.
Egan, V., Bull, E., and Trundle, G. (2020). Individual differences, ADHD, adult pathological demand avoidance, and delinquency. Res. Dev. Disabil. 105:103733. doi: 10.1016/j.ridd.2020.103733
Etikan, I., Musa, S. A., and Alkassim, R. S. (2016). Comparison of convenience sampling and purposive sampling. Am. J. Theor. Appl. Stat. 5, 1–4.
Fayette, R., and Bond, C. (2018). A systematic literature review of qualitative research methods for eliciting the views of young people with ASD about their educational experiences. Eur. J. Spec. Needs Educ. 33, 349–365. doi: 10.1080/08856257.2017.1314111
Fidler, R., and Christie, P. (2019). Collaborative approaches to learning for pupils with PDA: Strategies for education professionals. London: Jessica Kingsley Publishers.
Flackhill, C., James, S., Soppitt, R., and Milton, K. (2017). The Coventry grid interview (CGI): exploring autism and attachment difficulties. Good Autism Practice 18, 62–80.
Fletcher-Watson, S., Adams, J., Brook, K., Charman, T., Crane, L., Cusack, J., et al. (2019). Making the future together: shaping autism research through meaningful participation. Autism 23, 943–953.
Gillberg, C., Gillberg, I. C., Thompson, L., Biskupsto, R., and Billstedt, E. (2015). Extreme (“pathological”) demand avoidance in autism: a general population study in the Faroe Islands. Eur. Child Adolesc. Psychiatry 24, 979–984. doi: 10.1007/s00787-014-0647-3
Goodman, R., Ford, T., Richards, H., Gatward, R., and Meltzer, H. (2000). The development and well-being assessment: description and initial validation of an integrated assessment of child and adolescent psychopathology. J. Child Psychol. Psychiatry 41, 645–655.
Goodson, A. (2018). Emotion regulation and executive function in children and adolescents with autism Spectrum disorder and pathological demand avoidance traits (Doctoral dissertation). London: University College London.
Gore Langton, E., and Frederickson, N. (2016). Mapping the educational experiences of children with pathological demand avoidance. J. Res. Spec. Educ. Needs 16, 254–263. doi: 10.1111/1471-3802.12081
Gore Langton, E., and Frederickson, N. (2018). Parents’ experiences of professionals’ involvement for children with extreme demand avoidance. Int. J. Dev. Disabil. 64, 16–24. doi: 10.1080/20473869.2016.1204743
Grahame, V., Stuart, L., Honey, E., and Freeston, M. (2020). Response: anxiety and behaviour in and beyond ASD; does the idea of ‘PDA’really help?–a response to Green (2020). Child Adolesc. Mental Health 25, 77–78. doi: 10.1111/camh.12383
Graham-White, C. (2015). An investigation into the communication development and general communication of children with pathological demand avoidance syndrome. Available at: https://www.autismeastmidlands.org.uk/wp-content/uploads/2016/10/Communication-development-of-Children-with-pathological-Demand-Avoidance-Syndrome.pdf
Green, J. (2020). Commentary: anxiety and behaviour in and beyond ASD; does the idea of ‘PDA’really help?–a commentary on Stuart et al.(2020). Child Adolesc. Mental Health 25, 74–76. doi: 10.1111/camh.12379
Green, J., Absoud, M., Grahame, V., Malik, O., Simonoff, E., Le Couteur, A., et al. (2018b). Pathological demand avoidance: symptoms but not a syndrome. Lancet Child Adolescent Health 2, 455–464. doi: 10.1016/S2352-4642(18)30044-0
Green, J., Aldred, C., Charman, T., Le Couteur, A., Emsley, R. A., Grahame, V., et al. (2018a). Paediatric autism communication therapy-generalised (PACT-G) against treatment as usual for reducing symptom severity in young children with autism spectrum disorder: study protocol for a randomised controlled trial. Trials 19, 1–13.
Haire, L., and Symonds, J. E. (2021). Methods of studying pathological demand avoidance in children and adolescents: A scoping review protocol.
Happé, F. (2011). Criteria, categories, and continua: autism and related disorders in DSM-5. J. Am. Acad. Child Adolesc. Psychiatry 50, 540–542.
Hollocks, M. J., Lerh, J. W., Magiati, I., Meiser-Stedman, R., and Brugha, T. S. (2019). Anxiety and depression in adults with autism spectrum disorder: a systematic review and meta-analysis. Psychol. Med. 49, 559–572. doi: 10.1017/S0033291718002283
Hull, L., Petrides, K. V., Allison, C., Smith, P., Baron-Cohen, S., Lai, M. C., et al. (2017). “Putting on my best normal”: social camouflaging in adults with autism spectrum conditions. J. Autism Dev. Disord. 47, 2519–2534. doi: 10.1007/s10803-017-3166-5
Hull, L., Petrides, K. V., and Mandy, W. (2020). The female autism phenotype and camouflaging: a narrative review. Rev. J. Autism Dev. Disord. 7, 306–317. doi: 10.1007/s40489-020-00197-9
Jacobs, D., Steyaert, J., Dierickx, K., and Hens, K. (2018). Implications of an autism Spectrum disorder diagnosis: an interview study of how physicians experience the diagnosis in a young child. J. Clin. Med. 7:348. doi: 10.3390/jcm7100348
Kalvin, C. B., Marsh, C. L., Ibrahim, K., Gladstone, T. R., Woodward, D., Grantz, H., et al. (2020). Discrepancies between parent and child ratings of anxiety in children with autism spectrum disorder. Autism Res. 13, 93–103. doi: 10.1002/aur.2220
Kanani, F., and Balasubramanian, M. (2018). SHANK3 variant as a cause of nonsyndromal autism in an 11-year-old boy and a review of published literature. Clin. Dysmorphol. 27, 113–115. doi: 10.1097/MCD.0000000000000232
Kapp, S. K. (2020). Autistic community and the neurodiversity movement: Stories from the frontline. Berlin: Springer Nature, 330.
Kildahl, A. N., Helverschou, S. B., Rysstad, A. L., Wigaard, E., Hellerud, J. M., Ludvigsen, L. B., et al. (2021). Pathological demand avoidance in children and adolescents: a systematic review. Autism 25, 2162–2176. doi: 10.1177/13623613211034382
Kinnaird, E., Stewart, C., and Tchanturia, K. (2019). Investigating alexithymia in autism: a systematic review and meta-analysis. Eur. Psychiatry 55, 80–89.
Kunce, L., and Mesibov, G. B. (1998). “Educational approaches to high-functioning autism and asperger syndrome” in Asperger syndrome or high-functioning autism? (New York: Springer), 227–261.
Loomes, R., Hull, L., and Mandy, W. P. L. (2017). What is the male-to-female ratio in autism spectrum disorder? A systematic review and meta-analysis. J. Am. Acad. Child Adolesc. Psychiatry 56, 466–474. doi: 10.1016/j.jaac.2017.03.013
Lovaas, O. I. (1987). Behavioral treatment and normal educational and intellectual functioning in young autistic children. J. Consult. Clin. Psychol. 55, 3–9. doi: 10.1037/0022-006X.55.1.3
Lucyshyn, J. M., Fossett, B., Bakeman, R., Cheremshynski, C., Miller, L., Lohrmann, S., et al. (2015). Transforming parent–child interaction in family routines: longitudinal analysis with families of children with developmental disabilities. J. Child Fam. Stud. 24, 3526–3541.
Mayring, P. (2014). Qualitative content analysis: Theoretical foundation, basic procedures and software solution. Klagenfurt: Austria. Available at: http://nbn-resolving.de/urn:nbn:de:0168-ssoar-395173
McFadzen, C. (2020). Exploring the presence of pathological demand avoidance in school aged children.
Milton, D. (2012). On the ontological status of autism: the ‘double empathy problem’. Disabil. Soc. 27, 883–887. doi: 10.1080/09687599.2012.710008
Milton, D. (2013). 'Natures answer to over-conformity': deconstructing pathological demand avoidance. Natures.
Milton, D. (2017). A mismatch of salience: Explorations of the nature of autism from theory to practice. London: Pavilion Press.
Moher, D., Shamseer, L., Clarke, M., Ghersi, D., Liberati, A., Petticrew, M., et al. (2015). Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 4, 1–9. doi: 10.1186/2046-4053-4-1
Mols, D., and Danckaerts, M. (2022). Diagnostische validiteit van het concept Pathological Demand Avoidance: een systematische literatuurreview. Tijdschrift voor Geneeskunde. doi: 10.47671/tvg.78.22.077
Moore, A. (2020). Pathological demand avoidance: what and who are being pathologised and in whose interests? Global Stud. Childhood 10, 39–52. doi: 10.1177/2043610619890070
Newson, E. L. M. K., Le Marechal, K., and David, C. (2003). Pathological demand avoidance syndrome: a necessary distinction within the pervasive developmental disorders. Arch. Dis. Child. 88, 595–600.
O’Nions, E., Gould, J., Christie, P., Gillberg, C., Viding, E., and Happé, F. (2016). Identifying features of ‘pathological demand avoidance’using the diagnostic interview for social and communication disorders (DISCO). Eur. Child Adolesc. Psychiatry 25, 407–419. doi: 10.1007/s00787-015-0740-2
O’Nions, E., Happé, F., Viding, E., and Noens, I. (2021). Extreme demand avoidance in children with autism Spectrum disorder: refinement of a caregiver-report measure. Adv. Neurodev. Disord., 1–13. doi: 10.1007/s41252-021-00203-z
O’Nions, E., Viding, E., Greven, C. U., Ronald, A., and Happé, F. (2014b). Pathological demand avoidance: exploring the behavioural profile. Autism 18, 538–544. doi: 10.1177/1362361313481861
O'Nions, E. (2013). Understanding thoughts and responding to emotions: exploring similarities and differences between autism spectrum disorders, conduct problems with callous-unemotional traits, and pathological demand avoidance (Doctoral dissertation, King's College London (University of London)). Available at: https://ethos.bl.uk/OrderDetails.do?uin=uk.bl.ethos.814002
O'Nions, E., Christie, P., Gould, J., Viding, E., and Happé, F. (2014a). Development of the ‘extreme demand avoidance questionnaire’(EDA-Q): preliminary observations on a trait measure for pathological demand avoidance. J. Child Psychol. Psychiatry 55, 758–768.
O'Nions, E., and Eaton, J. (2020). Extreme/‘pathological’demand avoidance: an overview. Paediatr. Child Health 30, 411–415. doi: 10.1016/j.paed.2020.09.002
O'Nions, E., Happé, F., Viding, E., Gould, J., and Noens, I. (2018a). Demand avoidance is not necessarily defiance. Lancet Child Adolescent Health 2:e14. doi: 10.1016/S2352-4642(18)30171-8
O'Nions, E., Viding, E., Floyd, C., Quinlan, E., Pidgeon, C., Gould, J., et al. (2018b). Dimensions of difficulty in children reported to have an autism spectrum diagnosis and features of extreme/‘pathological’demand avoidance. Child Adolesc. Mental Health 23, 220–227. doi: 10.1111/camh.12242
Ozsivadjian, A. (2020). Demand avoidance—pathological, extreme or oppositional? Child Adolesc. Mental Health 25, 57–58. doi: 10.1111/camh.12388
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., et al. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int. J. Surg. 88, 1–9. doi: 10.1016/j.ijsu.2021.105906
PDA Society UK. (2022). Identifying & Assessing a PDA profile – Practice Guidance ID guide draft. Available at: pdasociety.org.uk
Persons, J. B. (2008). The case formulation approach to cognitive-behavior therapy. New York: Guilford Press.
Peters, M., Godfrey, C., McInerney, P., Soares, C. B., Khalil, H., and Parker, D. (2015). “Methodology for JBI scoping reviews” in The Joanna Briggs institute reviewers manual 2015 (Adelaide, SA: Joanna Briggs Institute), 3–24.
Reilly, C., Atkinson, P., Menlove, L., Gillberg, C., O’Nions, E., Happé, F., et al. (2014). Pathological demand avoidance in a population-based cohort of children with epilepsy: four case studies. Res. Dev. Disabil. 35, 3236–3244. doi: 10.1016/j.ridd.2014.08.005
Schopler, E., Mesibov, G. B., and Hearsey, K. (1995). Structured teaching in the TEACCH system. Learn. Cogn. Autism, 243–268.
Soppitt, R. (2021). “Pathological/extreme demand avoidance (PDA/EDA)” in Special educational needs: A guide for inclusive practice, 296–314.
Stuart, L., Grahame, V., Honey, E., and Freeston, M. (2020). Intolerance of uncertainty and anxiety as explanatory frameworks for extreme demand avoidance in children and adolescents. Child Adolesc. Mental Health 25, 59–67. doi: 10.1111/camh.12336
Tollerfield, I., Chapman, H. M., and Lovell, A. (2021). Underlying thinking pattern profiles predict parent-reported distress responses in autism Spectrum disorder. J. Autism Dev. Disord. 1-20. doi: 10.1007/s10803-021-05092-8
Tricco, A. C., Lillie, E., Zarin, W., O'Brien, K. K., Colquhoun, H., and Levac, D. (2018). PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann. Intern. Med. 169, 467–473. doi: 10.7326/m18-0850
Truman, C., Crane, L., Howlin, P., and Pellicano, E. (2021). The educational experiences of autistic children with and without extreme demand avoidance behaviours. Int. J. Incl. Educ., 1–21. doi: 10.1080/13603116.2021.1916108
Trundle, G., Craig, L. A., and Stringer, I. (2017). Differentiating between pathological demand avoidance and antisocial personality disorder: a case study. J. Intell. Disabil. Offending Behav. doi: 10.1108/JIDOB-07-2016-0013
van’t Hof, M., Tisseur, C., van Berckelear-Onnes, I., van Nieuwenhuyzen, A., Daniels, A. M., Deen, M., et al. (2021). Age at autism spectrum disorder diagnosis: a systematic review and meta-analysis from 2012 to 2019. Autism 25, 862–873. doi: 10.1177/1362361320971107
Wilding, L., and Griffey, S. (2015). The strength-based approach to educational psychology practice: a critique from social constructionist and systemic perspectives. Educ. Psychol. Pract. 31, 43–55.
Wing, L., Gould, J., and Gillberg, C. (2011). Autism spectrum disorders in the DSM-V: better or worse than the DSM-IV? Res. Dev. Disabil. 32, 768–773.
Woods, R. (2017). Pathological demand avoidance: my thoughts on looping effects and commodification of autism. Disabil. Soc. 32, 753–758. doi: 10.1080/09687599.2017.1308705
Woods, R. (2018). “Rational (pathological) demand avoidance: what it is not, what it could be & what it does” in Critical perspectives on pathological demand avoidance (PDA) (London: Participatory Autism Research Collective, London South Bank University).
Woods, R. (2019). Demand avoidance phenomena: circularity, integrity and validity–a commentary on the 2018 National Autistic Society PDA conference. Good Autism Practice 20, 28–40.
Woods, R. (2020). Pathological demand avoidance and the DSM-5: a rebuttal to Judy Eaton’s response. Good Autism Practice 21, 74–76.
Woods, R. (2021a). Demand avoidance phenomena (“pathological”/“extreme” demand avoidance): Is it a disorder at a lower diagnostic threshold?.[paper presentation] Online Participatory Research Collective: Understanding PDA, London South Bank University. PowerPoint Presentation. Available at: researchgate.net
Woods, R. (2021b). Pathological demand avoidance (DAP): its four schools of thought. Neurodevelopmental Psychology Forum 94, 10–14. doi: 10.53841/bpsdev.2021.1.94.10
Woods, R. (2022a). Pathological”/“Extreme” Demand-Avoidance: How do you build a Demand-Avoidance Disorder? [Video]. Youtube. “Pathological”/“Extreme” Demand-Avoidance: How do you build a Demand-Avoidance Disorder? – YouTube
Woods, R. (2022b). Demand avoidance phenomena (“pathological extreme” demand avoidance): what if it is a neurodevelopmental disorder?. [conference session]. Disability research forum event 3. Demand avoidance phenomena (pathological extreme demand avoidance): what if it is a neurodevelopmental disorder?: LSBU open research. Sheffield: Sheffield Hallam University.
Woods, R. (2022c). “Rational (pathological) demand avoidance: as a mental disorder and an evolving social construct” in The Routledge international handbook of critical autism studies (Abingdon: Routledge), 56–75.
Keywords: adolescence, autism, childhood, pathological demand avoidance, scoping review
Citation: Haire L, Symonds J, Senior J and D’Urso G (2024) Methods of studying pathological demand avoidance in children and adolescents: a scoping review. Front. Educ. 9:1230011. doi: 10.3389/feduc.2024.1230011
Edited by:
Richard Woods, London South Bank University, United KingdomReviewed by:
Wenn Lawson, Curtin University, AustraliaNicola Yuill, University of Sussex, United Kingdom
Copyright © 2024 Haire, Symonds, Senior and D’Urso. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lauren Haire, bGF1cmVuLmhhaXJlQHVjZGNvbm5lY3QuaWU=; Jennifer Symonds, SmVubmlmZXIuU3ltb25kc0B1Y2QuaWU=