 Ana Célia Nunes1
Ana Célia Nunes1 Daniela Bitencourt Santos2
Daniela Bitencourt Santos2 Márcio Fernandes Alves Leite3
Márcio Fernandes Alves Leite3 Marta Gràcia2
Marta Gràcia2 Patricia Carla de Souza Della Barba1*
Patricia Carla de Souza Della Barba1*- 1Postgraduate Program in Occupational Therapy at the Federal University of São Carlos, São Carlos, Brazil
- 2Department of Cognition, Development and Educational Psychology of the University of Barcelona, Barcelona, Spain
- 3Netherlands Institute of Ecology - NIOO, Wageningen, Gelderland, Netherlands
Introduction: In Brazil, there are few studies that investigate the support needs of families that have handicap children in their daily context. This study aims to adapt and validate the Family Needs Assessment (FNA) scale for use with families of children and adolescents with disabilities in Brazil.
Method: Two studies were conducted. The first study involved the cross-cultural adaptation of the scale, resulting in the Brazilian version of the FNA, which is called Avaliação das Necessidades da Família (ANF). The FNA comprises 49 items with high internal consistency (α = 0.98). The second study validated the FNA using a sample of 151 families with children and adolescents with disabilities.
Results: The structure of the scale was confirmed using Structural Equation Modeling (SEM), which grouped 46 items into seven dimensions. The scale demonstrated good fit (RMSEA = 0.041, SRMR = 0.063), satisfactory convergent validity (rs = −0.27, p < 0.001), and high levels of reliability (α = 0.92, ω = 0.94) and test–retest consistency (R1F = 0.98).
Discussion: The FNA is a valid, reliable, and accurate measure for assessing the needs of Brazilian families with children and adolescents with disabilities under 18 years of age.
1. Introduction
Living with a child’s disability can present various challenges for families. The scientific literature has shown that families with children or adolescents with disabilities often face difficulties that can affect family dynamics (Batista and França, 2007; Oliveira and Poletto, 2015).
The family is a social system within various contexts, including the immediate community and broader social systems. This family structure is characterized by interdependence among its members, which means that variables affecting one family member impact each of the other individuals individually and on the functioning of the family unit (Giné, 2000; Buscaglia, 2006; Fiamenghi and Messa, 2007; Hechet et al., 2011; Baqués, 2017).
Each family member has their own understanding and assigns meanings to family relationships based on their personal resources. Furthermore, each child experiences the dynamics of their parents based on their expectations, emotions, and the level of emotional availability within the family (Fiamenghi and Messa, 2007).
Several studies have explored the effects of having a family member with a disability in Brazilian families. These studies have revealed that families dealing with disability often face challenges such as overwhelming caregiving responsibilities, adapting to a new reality, needing emotional and financial support, and encountering barriers to accessing quality healthcare and education services (Tomaz et al., 2017).
The siblings of children with disabilities are also affected by this unique family dynamic. They commonly develop maturity and independence at an early age, as their parents’ attention and energy are intensely focused on the child with a disability (Matsukura and Cid, 2004).
Mothers of children with disabilities, such as those with autism, report difficulties accessing appropriate educational placements and ensuring their children’s rights are upheld. They face situations of inadequate inclusion, lack of preparation of schools to receive children, and experiences of prejudice and discrimination (Minatel and Matsukura, 2015).
Stress is a reality for caregivers of these children as well. Studies have shown that parents of children with Down syndrome and intellectual disabilities experience higher stress levels than those with typical development (Minetto et al., 2012).
The Brazilian scientific literature has identified several challenges that families of individuals with disabilities encounter. These difficulties include negative perceptions about the quality of life of the primary caregiver, the impact on the marital relationship, the greater burden of responsibility assigned to women, obstacles in accessing health and education information and services, financial difficulties arising from giving up work to care for the child with a disability, and restrictions in transportation, health, inclusive education, social life, and leisure. All of these difficulties stem from a social structure that is not inclusive enough (Oliveira et al., 2008; Barbosa and Fernandes, 2009; Favero-Nunes and dos Santos, 2010; Tomaz et al., 2017).
In this context, it is crucial for service providers to recognize the families of individuals with disabilities as a primary focus and to develop approaches that value the family as a support system in the child’s life. When families have access to the necessary resources and support, they become a driving force for their children’s optimal development. It is essential to understand that families of children and adolescents with disabilities do not hinder their development but are their primary providers (Allen and Petr, 1996; Franco, 2015).
Family-centered practices have emerged as a recent approach based on bioecological and systemic human development perspectives. They broaden their understanding of the interactions between human development and the contexts in which they occur. These practices consider the developing individual’s biological, psychological, and behavioral characteristics, including the hierarchical and interrelated contexts in which they are situated (Carvalho et al., 2016).
The instruments developed from family-centered practices to assess the family’s needs for support and quality of life are essential for strengthening and empowering families to overcome their challenges. Understanding the support needs of a family that has a member with a disability and how these needs influence the perceived quality of life of the family group is essential for developing effective family-centered practices. The balance of these variables is crucial, as an increase or decrease in one will directly affect the other.
“Family needs” refers to the lack of support in performing essential activities for the well-being of the entire family group. This impacts all members’ functionality and quality of life, including those with disabilities. Therefore, it is crucial to prioritize the identification of these needs in the process of developing action plans. This will enable effective planning of interventions that meet the real demands of the family (Giné, 2000; Thompson et al., 2009; McWilliam, 2010; Verdugo et al., 2012; Chiu et al., 2013).
In Brazil, the approach based on family needs is not yet a common practice in the work routines of professionals in the Early Intervention services field. This is due to a shortage of specific instruments, inadequate professional training, and the predominance of assistance based exclusively on the expertise of the professional, usually in healthcare institutions. Moreover, the intersection between different sectors is weak, resulting in a neglect of evidence indicating that support needs affecting all family members have a significant impact on the quality of life of the entire family group, including the quality of life of the child with a disability (McWilliam, 2010; Hechet et al., 2011; Santos, 2018; Nunes, 2019).
These statements are supported by two systematic literature review studies conducted in Brazil. In their systematic review, the Santos et al. (2017) identified a gap in Brazilian research on family quality of life. They pointed out that all studies selected for analysis focused solely on understanding the quality of life of individuals with disabilities, their caregivers, or parents, without considering the family’s and environment’s needs. These findings were confirmed by another systematic review conducted by the Nunes et al. (2021) on the quality of life of families with children and adolescents with disabilities. The authors noted the scarcity of studies on the topic, the prevalent use of individual constructs of quality of life, and the lack of measurement instruments to comprehend the quality of life of the family group. Nunes et al. (2021) further pointed out that the few studies addressed high formal and informal support needs as a barrier to family well-being and quality of life.
Given the above, this study aims to outline the process of cross-cultural adaptation and validation of the Family Needs Assessment scale for use in Brazil.
2. Materials and method
This multicenter, cross-sectional, descriptive, and methodological study aims to cross-culturally adapt and validate the Family Needs Assessment (FNA version 0–18 years) for use in Brazil. To conduct this study, researchers from the Graduate Program in Occupational Therapy at the Federal University of São Carlos (UFSCar) in Brazil established a partnership with the Spanish authors of the instrument. Additionally, collaborations have been established with faculty researchers from Brazilian public universities (federal and state) offering undergraduate Occupational Therapy programs. These universities include the Federal University of São Paulo (UNIFESP), the Federal University of Pelotas (UFPel), the Federal University of Sergipe (UFS), and the Alagoas State University of Health Sciences (UNCISAL).
2.1. Instruments
The Family Needs Assessment (FNA) was initially developed to gather information about the needs of families with children with developmental disabilities or delays to create individualized support plans that promote the quality of life for the entire family group (Chiu et al., 2013). The scale was initially developed in two official languages, English and Spanish (Avaliación de las Necesidades Familiares - FNA), and comprises 77 items distributed across 11 domains: family relationships, emotional health, physical health, finances, social relationships, leisure time, spirituality, daily care, education, access to services, and life changes. Response options are provided on a five-point Likert scale, ranging from 1 (no need) to 5 (very high need). This study used the Spanish version of the scale because of its proximity to Brazilian Portuguese compared to English (Chiu et al., 2013).
The QdVF Brazil scale, the cross-culturally adapted version of the Beach Center Family Quality of Life scale for the Brazilian population, was used to obtain concurrent criterion validity. This adaptation was conducted by Bitencourt, Gràcia, and Beltran in 2015. The Brazil FQoL questionnaire comprises 25 questions that measure satisfaction with a range of family activities over the past 12 months. Respondents rate their satisfaction on a five-point Likert scale, ranging from 1 (very dissatisfied) to 5 (very satisfied).
Additionally, the authors designed a questionnaire to gather socioeconomic and demographic information from the families who participated in the study.
2.2. Data collection procedures
This study was approved by the Research Ethics Committee (REC) for human participants at UFSCar under opinion number 2,278,628 on September 15, 2017. It also obtained approval from all the RECs of the participating centers. Data were collected by undergraduate and graduate Occupational Therapy students from the study’s partner universities in both the cross-cultural adaptation and validation phases. These students were previously trained by the main researcher of the coordinating center (UFSCar) through virtual meetings and with the support of a booklet prepared by the researchers exclusively for this purpose.
Data collection for the pre-test (cross-cultural adaptation phase) took place between April and June 2018. Data collection for the validation study occurred between September and December 2018, and test–retest data collection was conducted between June and August 2019.
2.3. Participants, inclusion criteria, and data collection sites
The final sample for the study comprised 189 participants recruited at different stages and phases of the research. During the pre-test stage, 38 families participated in the cross-cultural adaptation study. In the validation study of the scale, 130 families were involved. As part of the validation process, a test and retest study was conducted with the participation of 21 families.
The study’s inclusion criteria encompassed individuals who were family members (parents, siblings over the age of 18, grandparents, and primary family caregivers) of children and adolescents between the ages of 0 and 17 years, 11 months, and 29 days who had already received a diagnosis of disability or developmental delay.
The data were collected in various Brazilian cities at different stages of the study. During the pre-test phase, data were collected from early childhood education schools and institutions that serve children with autism in the cities of São Paulo and Santos (in the state of São Paulo), Lagarto (in the state of Sergipe), and Maceió (in the state of Alagoas). Furthermore, data for the main validation study and test–retest study of the scale were collected from rehabilitation institutions for individuals with physical and motor disabilities, institutions for individuals with autism and other intellectual disabilities, and early childhood education schools in the cities of São Paulo, Santos, Maceió, and Pelotas (in the state of Rio Grande do Sul).
2.4. Procedures adopted in the cross-cultural adaptation of the scale
The process of translating and cross-culturally adapting the Spanish version of the FNA scale was conducted in various stages, following the recommendations of Wild et al. (2005) and Beaton et al. (2007).
In Stage I, a formal request was made to the Spanish authors of the FNA scale for authorization to adapt it for use in Brazil. In Stage II, two independent translations of the FNA from Spanish to Brazilian Portuguese were done (translation A by a clinical professional working in physical disability rehabilitation and translation B by a document translation company.) Both translations were done by bilingual translators whose first language was Portuguese. None of the translators had prior knowledge of the scale and its concepts. Next, the coordinating team responsible for the adaptation process reconciled the two translations.
In Stage III, the translations were reconciled following the recommendations of Koller et al. (2012). Koller et al. (2012) present nine reconciled translation options. The option chosen as the most appropriate way to merge the A and B translations, with the B translation adapted to A. This stage resulted in the Brazilian instrument’s first version (V1). In Stage IV, the V1 was back-translated into Spanish by two bilingual native Colombian translators proficient in Portuguese and had no prior contact with the original Spanish scale.
In Stage V, a second reconciliation process was conducted to ensure that V1 accurately reflected the content of the items in the original FNA version, as Beaton et al. (2007) recommended. In Stage VI, the scale was evaluated by a committee of eight experts selected by the coordinating team. The committee comprised experts with theoretical and empirical experience working with individuals with disabilities and their families, including translators for stages I and III. Experts in cross-cultural adaptation methodology of assessment scales were also included.
In Stage VII, cognitive debriefing was conducted with 19 individuals from various country regions, including the Northeast, North, Southeast, and South. According to Wild et al. (2005), this is a stage of cross-cultural adaptation of an assessment scale that involves applying the scale to a group of participants to identify potential issues with understanding the items and instructions. This step provides valuable information about the clarity and relevance of the items and helps ensure that participants in the target culture correctly understand the scale.
In Stage VIII, a pre-test (pilot study) was conducted with 38 families of children and adolescents with disabilities from four Brazilian cities (São Paulo, Santos, Lagarto, and Maceió). The study’s objective was to test the application of the scale in a small sample of the target population and assess the clarity, comprehension, and appropriateness of the scale’s items and instructions (Beaton et al., 2007).
2.5. Data analysis procedures
The Content Validity Ratio formula developed by Lawshe (1975) was used to analyze the inter-rater agreement index during the expert evaluation stage, and the scale comprehensibility index in the cognitive debriefing stage was obtained through simple percentage calculations. The minimum CVR value, as stipulated by Lawshe (1975), was adopted as a parameter for a panel of eight raters (CVR ≥ 0.75). The satisfaction parameter for comprehensibility adopted in the cognitive debriefing was a value of ≥80%.
The scale’s psychometric properties were tested in the adaptation and validation studies. During the pre-test stage of the adaptation study, the scale’s internal consistency was evaluated through item-total correlation and Cronbach’s alpha tests.
In the validation study, we began evaluating the psychometric qualities by examining the empirical structure of the scale in the Brazilian context. The normality of the sample was assessed using the Kolmogorov–Smirnov normality test, and the Kaiser-Meyer-Olkin test was used to evaluate the overall consistency of the data and determine whether the factor analysis model used was appropriately fitted to the data. Additionally, Bartlett’s test of sphericity was conducted to confirm the suitability of exploratory factor analysis.
After completing the abovementioned process, we conducted an exploratory factor analysis (EFA) using SEM. The extraction of the factorial model followed two basic principles: parsimony and explanation to achieve a simple factorial response with a reduced number of statistically significant factors or components that could explain the model.
As the EFA did not provide evidence of a good fit to the theoretical model, a subsequent confirmatory factor analysis (CFA) was performed to determine the appropriate structure for the Brazilian socio-cultural context based on latent variable hypotheses. The scale’s reliability was evaluated using Cronbach’s alpha coefficient, McDonald’s omega coefficient, average variance extracted, and composite reliability. Values equal to or greater than 0.7 for alpha, omega, and composite reliability and values equal to or greater than 0.5 for average variance extracted were considered indicative of high internal consistency.
Finally, concurrent validity was estimated by analyzing covariance between the FNA and the Brazil FQoL. Theoretically, family quality of life and family support needs are inversely proportional magnitudes, and this was taken into consideration during the analysis.
3. Results
3.1. Cross-cultural adaptation
The cross-cultural adaptation of the FNA was conducted following the guidelines recommended by international reference publications in the field (Wild et al., 2005; Beaton et al., 2007). During the reconciliation stage (stage III), modifications were made to ensure coherence and harmony between the two translations’ content and the instrument’s original version, resulting in a precise Brazilian version aligned with the original scale.
During the two-stage expert evaluation process, the pre-final version was revised according to feedback from the evaluation committee. In the first phase, 58 out of 78 items (including the initial wording and questionnaire items) showed satisfactory agreement rates (CRV ≥ 0.75) in semantic, idiomatic, cultural, and conceptual equivalences, as suggested by Beaton et al. (2007). Nineteen items were reformulated based on the experts’ suggestions and underwent a second evaluation by the same committee. This time, they obtained satisfactory agreement rates among the evaluators (CRV ≥ 0.75).
Similarly, in the cognitive debriefing stage, the scale underwent further modifications. Although the comprehensibility index obtained was higher than 84%, we considered the evaluators’ suggestions and made minor changes to 12 items on the scale. For example, the word “play” has been replaced with “leisure,” “doctor’s appointment,” with “going to a doctor’s appointment,” and “coordinating medical care” with “organizing medical care.”
During the pre-test stage, Cronbach’s alpha coefficient was 0.98 for the total value. However, during the item-total correlation test, six items from the scale (items 2, 13, 25, 54, 56, and 64) scored below the minimum value recommended by the literature [> 0.3] (Bisquerra et al., 2004), indicating the need to modify or remove these items.
After careful consideration, the coordinating team, in collaboration with the scale’s author, actively engaged in the adaptation process and decided to modify the six items rather than eliminate them. To address the difficulties reported by auxiliary researchers during the protocol application with families (such as extended time for applying the scale, items with similar content, and difficulty understanding certain items by family members), we merged items with similar content and reworded items identified as challenging to understand without losing any content. This approach was considered the most viable solution for reducing the scale, resulting in a Brazilian version of the FNA with 49 items after the cross-cultural adaptation process.
3.2. Demographic and socioeconomic characterization of the participating families
Of the 130 families participating in the main study, a significant number of respondents were mothers (82.44%) or fathers (10.69%) of the child/adolescent, followed by grandparents (3.84%) or individuals with no family connection (1.53%). The average age for mothers was 36.9 years (±8.3 years); for fathers, it was 37 years (±7.97 years); and for grandparents, it was 58.4 years (±5.55 years). There was a higher participation of families with children and adolescents with autism spectrum disorder (39.23%), followed by families with children with Cerebral Palsy or motor disabilities (34.61%). Families with children with Down syndrome, hydrocephalus, myopathies (muscular dystrophies), and visual impairment accounted for 9.24% of the sample (2.31% of each family).
A total of 53.08% of the respondents perceive the severity of the children’s/adolescents’ disability as moderate, 32.31% perceive it as mild, and only 13.08% perceive it as severe. Only 1.54% of parents did not report the severity of their children’s/adolescents’ disability.
Most participants’ families had three (27.88%), four (31.25%), or five (23.8%) members. A total of 30.29% of the families had an income of up to one Brazilian minimum wage (approximately US$ 214); 23.8% had up to two minimum wages; 26.44% had an income of two to four minimum wages, and only 19.47% of the respondents had a family income above four Brazilian minimum wages.
3.3. Pre-analysis of the data
The Kolmogorov–Smirnov normality test yielded a significant result for all items (p < 0.001), indicating non-normality in the distribution of sample scores. The Kaiser-Meyer-Olkin criterion confirmed that factor analysis was appropriate, with a coefficient of 0.89. Finally, Bartlett’s test of sphericity showed that the data matrix was factorable for factor analysis (X2 = 3776.362; DF = 1,176; p-value < 0.001). To perform the exploratory factor analysis, we used Promax rotation, and to select the appropriate set of dimensions, we performed a comparative analysis of random “parallel” matrices.
3.4. Construct validity
The Scree Plot analysis indicated a five-factor structure as a good configuration, explaining 56% of the total variance in the data. However, the cumulative variance criterion stipulates a percentage > 60% to determine the number of factors that should be extracted. Therefore, even if the first five dimensions had a total variance value greater than 50%, this did not meet the criterion, resulting in a dilemma between parsimony and explanation. Therefore, it was decided to test a different model that would better fit the scale theory and the Brazilian socio-cultural context by combining confirmatory factor analysis and regression analysis through the Structural Equation Model (SEM).
The new model created was composed of seven latent variables: 1) Education [EDU (items 4, 7, 28, 33, 34, 43, 45, 46, 47, and 48); 2) Family life [FL] (items 1, 12. 19, 20, 23, 27, 36, 40, and 49); 3) Community life [CL] (items 10, 18, 24, 32, 39, and 42); 4) Leisure time [LT] (items 2, 13, 17, and 31); 5) Acquisition and Management of Products and Services - AMPS (items 5, 9, 11, 16, 21, 22, 26, 29, 35, 37, 38, and 44); 6) Economics - ECON (items 8, 15, 25, and 30), and 7) Health and Well-Being - HWB (items 3, 6, 14, and 41). This model exhibited acceptable RMSEA (0.049) and SRMR (0.074) values, with highly significant p-values < 0.01.
We continued our search for a model with better data fit by removing items from the scale on each latent variable, one by one, to see if it would improve the model’s fit indices. After removing items 2 (leisure time variable), 35 (acquisition and management of products and services variable), and 48 (education variable), we obtained more robust RMSEA (0.041) and SRMR indices: (0.063) and highly significant p-values < 0.001 (Table 1).
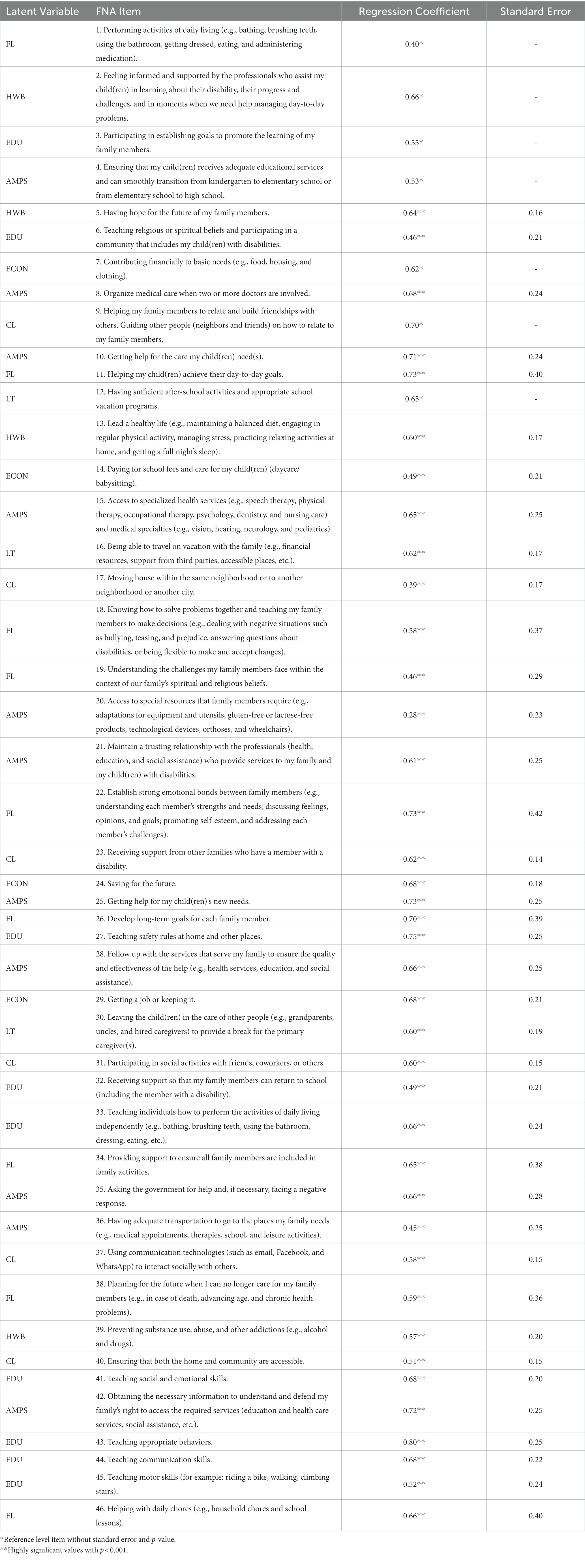
Table 1. Regression coefficients per FNA item (n = 130).
It was confirmed through SEM analysis that the best FNA model for the Brazilian context consists of 46 items distributed across seven latent variables. The new model explained 89.6% of the variance in family needs. The latent variable education was able to model 84.6% of the variability found in the responses to the questions that compose it. The family life dimension models 73%, community life models 92.8%, leisure time models 81.1%, acquisition and management of products and services models 84.9%, economy models 82.8%, and health and well-being models 90.6%.
3.5. Reliability
The scale with 46 items also demonstrated excellent internal consistency, as indicated by the results in Table 2.
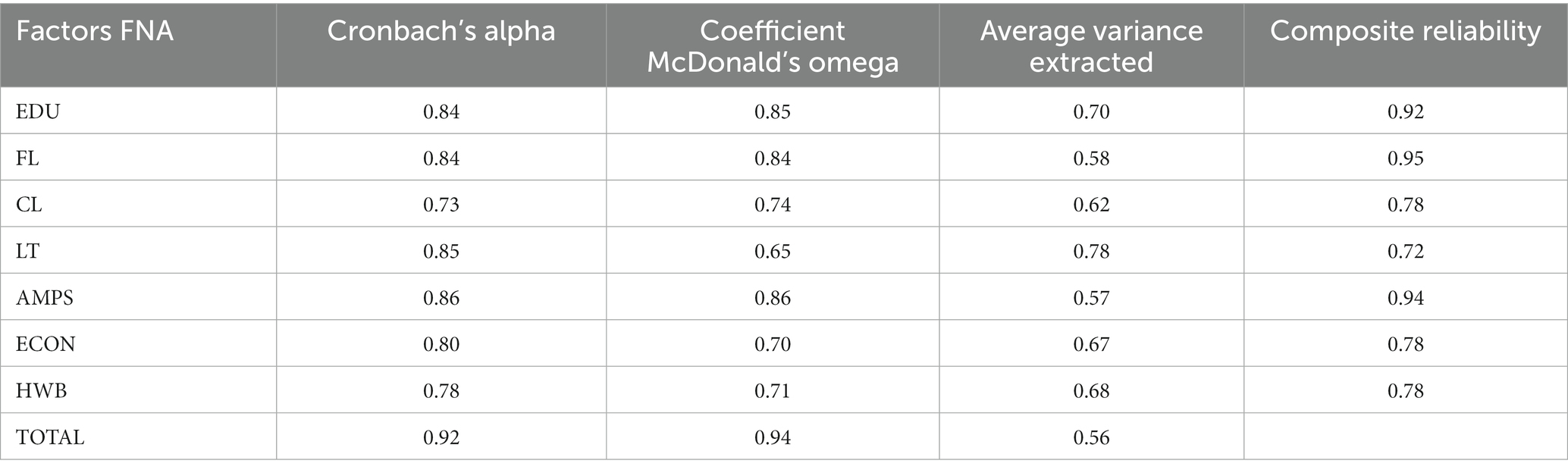
Table 2. Indicators of the accuracy of the latent variables of the FNA (n = 130).
The reliability of the scale was confirmed through the test–retest technique. The Cronbach’s alpha coefficient obtained for the test was 0.96, and for the retest, it was 0.98 (n = 21). The average time between test applications was 43 days, with a standard deviation of 12 and a median of 42 days. The minimum retest interval was 7 days, and the maximum was 63 days. The reliability of the average of all items, with time as the random factor (R1F), showed an excellent reliability index of 0.98, indicating that the reliability of the FNA remains stable over time. In both the initial test and the retest, the following results were obtained: 26% of the variability in responses is due to differences between individuals; 16% is due to the interaction between the subject and the time it takes to apply the FNA; 13% is due to the specific FNA items used; 13% is due to the interaction between application time and FNA items, and the remaining 31% is residual.
3.6. Concurrent criterion validity
Finally, the concurrent criterion validity was examined by assessing the covariance between the regression coefficients obtained with the FNA and the Brazil FQoL. The analysis provided consistent evidence of criterion validity for the FNA, as demonstrated by the negative and significant convergence between the scores obtained from the two scales, with rs (130) = −27, p < 0.01.
4. Discussion
The present study followed international reference guidelines (Wild et al., 2005; Beaton et al., 2007) to ensure the quality of the cross-cultural adaptation process of the scale. The excellent results obtained in the statistical analyses in both stages, the pre-test during the cross-cultural adaptation phase and the validation study, confirmed the quality of the entire cross-cultural adaptation process.
Including diverse participants and socio-cultural contexts in both the expert assessment and cognitive debriefing stages enabled us to achieve the goal outlined in the recommendations made by Beaton et al. (2007) regarding the general level of reading and comprehension of the questionnaire is appropriate for a child who is 12 years old or has a reading level equivalent to the sixth grade of elementary school.
In the transcultural adaptation study of the scale, despite Crombach’s alpha coefficient indicating high overall consistency, the item-total correlation test identified six items with issues, scoring below the recommended minimum value. Instead of removing these items, the team chose to modify them in collaboration with one of the scale’s authors. Additionally, measures were taken to streamline the scale, such as merging similar questions and rewriting certain items. These actions were based on the feedback from families and assisting researchers, who reported difficulties in administering and comprehending the scale items.
To determine the number of factors in the adapted scale, a correlation matrix analysis was conducted using the successive eigenvalue scree plot (Parallel Analysis Scree Plots). The scree plot test indicated that five factors were the ideal number, but further analyses revealed that this model did not meet all the desired fit criteria. In light of this, new analyses were performed, leading to the identification of a 12-dimensional model that exhibited better fit. However, the proportion of explained variance beyond the first five dimensions was notably low. This discovery created a dilemma between parsimony and explanation. As none of the scenarios fully satisfied the established criteria, a decision was made to test a new model using confirmatory factor analysis and regression analysis through the Structural Equation Modeling framework. The new model demonstrated acceptable fit indices and was further improved by removing three specific items (item 2 from the free time variable, item 35 from the acquisition and management of products and services variable, and item 48 from the education variable), resulting in more robust fit indices.
The rationale behind these modifications was to enhance the quality and utility of the scale, as well as to seek a model that better aligned with the underlying theory of the scale and the Brazilian context, ensuring a more reliable and valid measurement instrument.
Thus, compared to the original scale, the version adapted to the Brazilian context was reduced to 7 factors and 46 items. It is important to emphasize that the item content was retained, and the factor categories are similar.
Structural Equation Modeling (SEM) was chosen to test the hypothesis of this study due to the non-normal nature of the data and its measurement form. The scale questions do not generate fractional responses, and the items are interrelated, grouping into macro variables (latent variables) that represent the construct under analysis (family support needs). SEM is a confirmatory technique that requires the formulation of the model prior to data collection, with its main objective being to verify whether the data confirm or refute the formulated hypothesis.
In this convergent validation study of the FNA scale, the postulated hypothesis was that an increase in family support needs would be associated with a decrease in perceived quality of life among families. This hypothesis was confirmed through a significance test of the correlation coefficient, which indicated a significant negative relationship between the variables. In addressing the reviewer’s comment regarding the non-normal distribution of the sample scores, it was considered in the data analysis by employing appropriate statistical techniques that account for non-normality. These techniques allow for robust estimation and inference, mitigating any potential impacts that non-normality might have on the results.
Regarding reliability, the results of the present study showed excellent internal consistency values for both the total scale and the seven dimensions of the FNA. According to the literature, values of α > 0.70 are considered satisfactory and indicative of high internal consistency (Field, 2009).
In addition to Cronbach’s alpha coefficient, alternative measures were used to highlight the scale’s reliability, such as McDonald’s omega coefficient. The results obtained with McDonald’s omega also reinforced the reliability of the FNA, demonstrating adequate internal consistency to measure what it intends to measure. This reliability was confirmed by the composite reliability and average variance extracted indices, which are robust measures of internal consistency (Campo-Arias et al., 2013; Valentini and Damásio, 2016; Ventura-León and Caycho-Rodríguez, 2017; Ventura-León, 2018).
The test–retest results showed high internal consistency values for both the test measure and the retest measure confirming that the FNA has a high safety coefficient and a low margin of error, even when there are possible modifications in the environment. Furthermore, the FNA demonstrated an excellent reliability index when the time was considered a random factor, with only 13% variability observed when comparing application time and scale items. This indicates consistency and accuracy, as the scale consistently produced the same result in similar and successive situations under the same environmental conditions as the first measurement conducted with the same participants.
The cross-cultural adaptation of the FNA in different international socio-cultural contexts resulted in changes to the number of items and dimensions compared to the original scale. The excellent validity and reliability indices obtained in this study align with previous FNA validation studies conducted in various countries, which also reported similar results in terms of item and dimension reduction, as well as satisfactory validity and reliability indices (Aya-Gómez et al., 2017; Baqués, 2017; Cordero-Huertas, 2018; Santos, 2018).
The study results indicate that the FNA scale’s cross-cultural adaptation was conducted per international guidelines, ensuring its quality. The scale demonstrated good criterion validity, internal reliability, and test–retest reliability. These results confirm the usefulness of the FNA as a reliable tool for evaluating family support needs and its correlation with families’ perceived quality of life in diverse socio-cultural contexts.
The importance of the FNA for Brazil lies in its ability to provide relevant information about the needs of families, which can then be used to create personalized support plans to promote the family group’s quality of life (Chiu et al., 2013). However, the scientific research on family quality of life in Brazil, particularly for families with members who have disabilities, is still limited. Only a few studies have explored this topic, and they mainly focus on individual aspects. This contrasts with the increasing importance placed on the quality of family life globally.
In this context, the FNA stands out as a tool that can help professionals and families adopt a family-centered approach, recognizing their real needs. It enables the joint identification of supports that benefit both professionals/services and families, promoting effective problem-solving in various areas such as education, family life, community life, leisure time, acquisition and management of products and services, economy, and emotional health and well-being.
By assessing these different areas, the FNA considers both the individual support needs and the needs of the family group as a whole, contributing to practices that result in a better quality of life for all family members. In the context of Brazilian families with children and adolescents with disabilities, the FNA can empower them. Specifically, by allowing them to become the primary decision-makers in choosing which demands should be addressed by professionals and services based on their own priorities and urgencies.
Furthermore, the FNA provides services and professionals with a reliable foundation for initiating a logical dialogue, with qualified listening and meaningful participation from the family. It can also be used to measure the effectiveness of therapeutic interventions, as the quality of life of each family member is interconnected and directly impacts the quality of life of the entire family.
The FNA instrument was originally developed for clinical and research purposes. In clinical practice, the interpretation of the FNA is straightforward: items indicated by families as having high or very high support needs, as well as items selected as top priority, require special attention from professionals and services.
However, categorizing individuals into specific categories poses a challenge when using assessment instruments in scientific research. Therefore, in this study, a latent variable model was employed to classify family needs, taking into account item scores and their specific weights. However, calculating actual scores for each item and dimension is complex and time-consuming, particularly in studies with numerous participants. To simplify this process, the authors developed a simple software that performs the necessary calculations to classify family needs more efficiently. This approach aimed to facilitate the application of the ANF scale and expedite the analysis of results [comment 4 from reviewer 1].
The FNA is an effective tool for assessing and analyzing human activity in daily life, gathering information about family members’ performance in basic and instrumental activities, education, economy, leisure, and other relevant dimensions. As a result, it contributes to a more comprehensive and family-centered approach in Early Intervention in Brazil, considering that this instrument should not be the sole means of gathering information about family needs.
As limitations of the study, we mention the sample size and selection, which were recruited through non-probabilistic convenience sampling, and the inability to recruit participants from all regions of the country due to its continental dimensions, both in the adaptation study and in the scale validation. Another limitation of the study is the short time interval between test and retest administrations.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: https://repositorio.ufscar.br/handle/ufscar/12279.
Ethics statement
The studies involving human participants were reviewed and approved by CEP Humanos UFSCar. The patients/participants provided their written informed consent to participate in this study.
Author contributions
AN contributed to the research conduct, from the study conception to the data collection and analysis. They also contributed to manuscript writing and the development of key results, conclusions, existing literature review, and interpretation of findings. DS provided methodological guidance, contributed to manuscript writing and final manuscript review. ML contributed to the statistical analysis of the study. MG contributed to the study conception, methodological guidance, manuscript writing, and final manuscript review. PDB contributed to the research conduct and guidance, from the study conception to the data collection and analysis. They also contributed to manuscript writing, data analysis, conclusions, discussions, and final manuscript review. All authors contributed to the article and approved the submitted version.
Acknowledgments
We would like to express our sincere gratitude to Carla Cilene Baptista and Andrea Jurdi from Unifesp Campus Baixada Santista, Nicole Guarani from UFPel, Flavia Calheiros and Emanuelle Santos from Uncisal, and Taís Bracher from UFS, as well as all the students involved, for their invaluable support and contribution to the completion of this study. We would also like to extend our appreciation to the Association of Friends of Autistic Individuals in São Paulo (AMA), the Autism Vila Mariana Project, and the Association for Assistance to Disabled Children in São Paulo (AACD) for believing in and supporting this research. We sincerely thank them for welcoming us with open arms and allowing us to work collaboratively with the families they serve to produce the results of this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Allen, R. I., and Petr, C. G. (1996) in Toward developing standards and measurements for family-centered practice in family support programs, in redefining family support: Innovations in public-private partnerships. eds. G. H. S. Singer, L. E. Powers, and A. L. Olson (Baltimore, Maryland, United States: Paul H. Brookes Publishing), 57–85.
Aya-Gómez, V. L., Ovalle Parra, A. A., Cabrera-Garcia, V., Muñoz-Gómez, D. S., and Duque Romero, C. A. (2017). Validation of the family needs assessment scale for Colombian families with children with intellectual disability. Int. J. Disabil. Hum. Dev. 16, 233–336. doi: 10.1515/ijdhd-2016-0033
Baqués, N. A. (2017). La valoración de las necesidades de apoio de las familias con un hijo/a con discapacidad intelectual: validación de una escala [doctoral dissertation]. [Spain]: Universitat Ramon Llull.
Barbosa, M. R. P., and Fernandes, F. D. M. (2009). Qualidade de vida dos cuidadores de crianças com transtorno do espectro autístico. Rev. soc bras fonoaudiol. 14, 482–486. doi: 10.1590/S1516-80342009000400009
Batista, S. M., and França, R. M. (2007). Família de pessoas com deficiência: desafios e superação. J. Tech. Sci. Dissemination ICPG. 3, 117–121.
Beaton, D., Bombardier, C., and Guillemin, F. (2007). Recommendations for the cross-cultural adaptation of the DASH & QuickDASH outcome measures (Institute for Work and Health). 1, 1–45.
Bisquerra, R., Sarriera, J., and Martinez, F. (2004). Introdução à Estatística – Enfoque Informático Com Pacote Estatístico SPSS (Porto Alegre: Artmed), 256 p.
Buscaglia, L. O. (2006). “Papel da família” in Os Deficientes e Seus Pais: um Desafio Ao Aconselhamento. ed. L. Buscaglia (Rio de Janeiro: Record), 77–90.
Campo-Arias, A., Villamil-Vargas, M., and Herazo, E. (2013). Reliability and dimensionality of the alcohol use disorders identification test (AUDIT) in university students from Tunja (Colombia). Psciol Caribe. 30, sp. Available at: http://rcientificas.uninorte.edu.co/index.php/psicologia/article/view/4377/6769 [Accessed November 19, 2019].
Carvalho, L., Almeida, I., Felgueiras, I., and Franco, V. (2016). Práticas Recomendadas em Intervenção Precoce na Infância: um Guia para Profissionais (Coimbra: National Association for Early Intervention), 355.
Chiu, C.-Y., Turnbull, A. P., and Summers, J. A. (2013). What families need: validation of the family needs assessment for Taiwanese families of children with intellectual disability and developmental delay. Res. Pract. Pers. Severe Disabil. 38, 247–258. doi: 10.1177/154079691303800404
Cordero-Huertas, B. (2018). Calidad de Vida y Necesidades de Apoyo de las Familias de Personas con Discapacidad en Edades Tempranas en Costa Rica [dissertation] (Doctorate in Psychology) (Universitat Ramon Llull).
Favero-Nunes, M. Â., and dos Santos, M. A. (2010). Depressão e qualidade de vida em mães de crianças com transtornos invasivos do desenvolvimento Rev. Latino-Am. Enfermagem, Ribeirão Preto. 18, 33–40. doi: 10.1590/S0104-11692010000100006
Fiamenghi, G. A., and Messa, A. A. (2007). Pais, filhos e deficiência: estudos sobre as relações familiares. Psicol. Cien. Prof. 27, 236–245. doi: 10.1590/S1414-98932007000200006
Franco, V. (2015). Introdução à Intervenção Precoce no desenvolvimento das crianças: com a família, na comunidade, em equipe Aloendro Editions.
Giné, C. (2000). “Las necesidades de las familias a lo largo del ciclo vital” in collection, in Familias y Discapacidad Intelectual. ed. M. A. Verdugo (Madrid, Spain: FEAPS), 19–40.
Hechet, E., Reynolds, M., Agosta, J., McGinley, K., and Moseley, C. (2011). Building a national agenda for supporting families with a member with intellectual and developmental disabilities. Final report of the Wingspread Conference on building a family support agenda, March 6–8, 2011. Racine, WI (Johnson Foundation).
Koller, M., Kantzer, V., Mear, I., Zarzar, K., Martin, M., Greimel, E., et al. (2012). The process of reconciliation: evaluation of guidelines for translating quality-of-life questionnaires. Expert Rev. Pharmacoecon. Outcomes Res. 12, 189–197. doi: 10.1586/erp.11.102
Lawshe, C. H. (1975). A quantitative approach to content validity. Pers. Psychol. 28, 563–575. doi: 10.1111/j.1744-6570.1975.tb01393.x
Matsukura, T. S., and Cid, M. F. B. (2004). Irmãos de crianças com necessidades especiais: buscando conhecer a realidade do outro. Rev. Bras. Educ. Especial. 10, 355–370.
Mcwilliam, R. A. ed. (2010). Routines-based early intervention – Supporting young children and their families (New York/London: The Guilford Press).
Minatel, M. M., and Matsukura, T. S. (2015). Familiares de crianças e adolescentes com autismo: percepções do contexto escolar. Rev. Educ. Espec. 28, 429–442. doi: 10.5902/1984686X14708
Minetto, M. F., Crepaldi, M. A., Bigras, M., and Moreira, I. C. (2012). Educational practices and parental stress of parents of young children with typical and atypical development. Educ. Rev. Curitiba. 43, 117–132. doi: 10.1590/S0104-40602012000100009
Nunes, A. C. (2019). Adaptação transcultural e validação da escala evaluación de las necesidades familiares para uso com famílias brasileiras de crianças e adolescentes com deficiência [doctoral dissertation]. Brazil: Universidade Federal de São Carlos.
Nunes, A. C., Luiz, E. A. M., and Della Barba, P. C. S. (2021). Family quality of life: An integrative review on the family of people with disabilities. Ciência & Saúde Coletiva 26, 2873–2888. doi: 10.1590/1413-81232021267.06962019
Oliveira, S., Fatima, M., Silva, M. B. M., Frota, M. A., Pinto, J. M., Md, L., et al. (2008). Qualidade de vida do cuidador de crianças com paralisia cerebral. RBPS 2008, 275–280. doi: 10.5020/18061230.2008.p275
Oliveira, I. G., and Poletto, M. (2015). Emotional experiences of mothers and fathers of children with disabilities. Rev. SPAGESP. 16, 102–119.
Santos, D. B. (2018). Evaluación de las necesidades de apoyo de las familias de personas con Discapacidad Intelectual y/o del Desarrollo en Brasil [doctoral dissertation]. Spain: Universitat di Barcelona.
Santos, D. B., Garcia, M. G., and Della Barba, P. C. D. S. (2017). Qualidade de vida das pessoas com deficiência: revisão sistemática no âmbito de trabalhos brasileiros publicados em bases de dados. Revista Brasileira de Qualidade de Vida 9, 45–62. doi: 10.3895/rbqv.v9n1.4655
Thompson, J. R., Bradley, V. J., Buntinx, W. H., Schalock, R. L., Shogren, K. A., Snell, M. E., et al. (2009). Conceptualizing supports and the support needs of people with intellectual disability. Intellect. Dev. Disabil. 47, 135–146. doi: 10.1352/1934-9556-47.2.135
Tomaz, R. V. V., Santos, V. A., Silva de Avó, L. R. D., Germano, C. M. R., and Melo, D. G. (2017). Impact of moderate intellectual disability on the dynamics and quality of family life: a qualitative clinical study. Cad. Saude Publica 33:e00096016. doi: 10.1590/0102-311X00096016
Valentini, F., and Damásio, B. F. (2016). Variância média extraída e confiabilidade composta: indicadores de precisão. Psic.: Teor. e Pesq. 32, 1–7. doi: 10.1590/0102-3772e322225
Ventura-León, J. L. (2018). Confidence intervals for omega coefficient: proposal for Calculus. Adicciones 30, 77–78. doi: 10.20882/adicciones.962
Ventura-León, J. L., and Caycho-Rodríguez, T. (2017). El coeficiente Omega: un método alternativo para la estimación de la confiabilidad. Rev. Latinoam. Cienc. Soc. Niñez Juv. 15, 625–627.
Verdugo, M. Á., Rodríguez, A., and Sainz, F. (2012). Escala de Calidad de Vida Familiar: Manual de Aplicación (Salamanca: Universidad de Salamanca), INICO.
Wild, D., Grove, A., Martin, M., Eremenco, S., McElroy, S., Verjee-Lorenz, A., et al. (2005). Principles of good practice for the translation and cultural adaptation process for patient-reported outcomes (PRO) measures: report of the ISPOR task force for translation and cultural adaptation. Value Health 8, 94–104. doi: 10.1111/j.1524-4733.2005.04054.x
Keywords: test validity, family, disability, support needs, Brazil
Citation: Nunes AC, Santos DB, Leite MFA, Gràcia M and Della Barba PCS (2023) Cross-cultural adaptation and validation of the family needs assessment scale for Brazilian families of children and adolescents with disabilities. Front. Educ. 8:1241018. doi: 10.3389/feduc.2023.1241018
Edited by:
Gabriel Martínez-Rico, Catholic University of Valencia San Vicente Mártir, SpainReviewed by:
Cláudia Cristina Fukuda, Catholic University of Brasilia (UCB), BrazilAntonio Luque, University of Almeria, Spain
Copyright © 2023 Nunes, Santos, Leite, Gràcia and Della Barba. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Patricia Carla de Souza Della Barba, cGF0cmljaWFiYXJiYUB1ZnNjYXIuYnI=